
988368
Wed, May 8, 2024

Volume 20, Issue 2 (June 2022)
Iranian Rehabilitation Journal 2022, 20(2): 171-184 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shori G, Raghava S. Effects of Right Sidelying Respiratory Left Adductor Pull Back Exercise on Improving Hip Biomechanics in Participants With a Tendency to Stand on Right Side. Iranian Rehabilitation Journal 2022; 20 (2) :171-184
URL: http://irj.uswr.ac.ir/article-1-1250-en.html
URL: http://irj.uswr.ac.ir/article-1-1250-en.html



1- Rehabilitation Services, Health Care at Home India Pvt Ltd, Noida, Uttar Pradesh, India.
2- Department of Physiotherapy, Jaypee Hospital Noida, India.
2- Department of Physiotherapy, Jaypee Hospital Noida, India.
Full-Text [PDF 3590 kb]
(546 Downloads)
| Abstract (HTML) (1658 Views)
Full-Text: (875 Views)
1. Introduction
Succinct functional patterns govern and produce many systems, and posture is a symbol of their role. These forms reflect our inclination and incapability to spin and rest evenly with the left and right hemispheres of our axial structures [1].
Individuals with a tendency to change their body weight or center of gravity linked with the pelvis and lumbar vertebrae rotate on one side while the upper thoracic and the pubic symphysis rotate on the opposite, have been discussed in the literature as the left anterior interior chain (Left AIC) pattern [2, 3, 4, 5]. These uneven patterns have been linked to a muscle chain that stretches numerous joints and overlaps without a break in continuity, generating an imbalance [6, 7, 8, 9].
The above-mentioned pattern is demonstrated with imbalances in muscles and associated soft tissues, resulting in compensation in areas of the trunk, and connected limbs [10]. The biomechanics of the linked pelvic position also changes and influences the motion and potential arthrokinematics of the hip joint, as well as creating a functional impingement [11, 12, 13].
If not addressed timely, these abnormal positional patterns may lead to movement dysfunctions, structural changes, and distorted movement [14, 15]. These subsequent abnormal alignments may result in the decline of the individual’s participation in activities of daily living [4].
An intense rehabilitative exercise that corrects postural asymmetry and helps to restore normal bone and soft tissue posture of the trunk and pelvis is beneficial to patients. Although physical therapists use the right sidelying respiratory left adductor pull back exercise for a variety of musculoskeletal conditions [16, 17], there is a paucity of research on this technique’s efficacy. Therefore, this research aims to explore the effect of right sidelying respiratory left adductor pull back exercise on improving hip biomechanics in participants with a tendency to stand on the right side.
2. Materials and Methods
Study participants
A total of 30 participants (6 females and 24 males) with Mean±SD age of 28.53±2.62 years, Mean±SD weight of 63.83±3.89 kg, and Mean±SD height of 165.8±3.97 cm were recruited and randomly divided into experimental (n=15) and control groups (n=15). The potential candidates were screened using a standardized procedure. Posters, standees, and electronic notice boards were used to invite potential participation. A certified assessor visually assessed the posture. The person was examined in their regular relaxed position. The inclusion criteria comprised the following items: age range of 25 to 40 years, both sexes, and a tendency to stand on the right side given their affirmative answer on the self-declaration form indicating that they spend the majority of their time in this position. The exclusion criteria comprised the following items: having musculoskeletal injuries or other neurological and systemic illness as diagnosed by a physician, receiving any other training or intervention, having limb length discrepancy, inability to follow the commands (patients with cognitive impairment and inability to understand the language and or instructions), having a tendency to stand on the left side. The participants were excluded based on the self-reported form. Before collecting the data, all participants signed an informed consent form. Experimental procedure was also clarified to the participants using standard process. The study protocol was approved by the Institutional Ethics Committee (Code: ITS.COP.REC.1025.775).
Study procedure
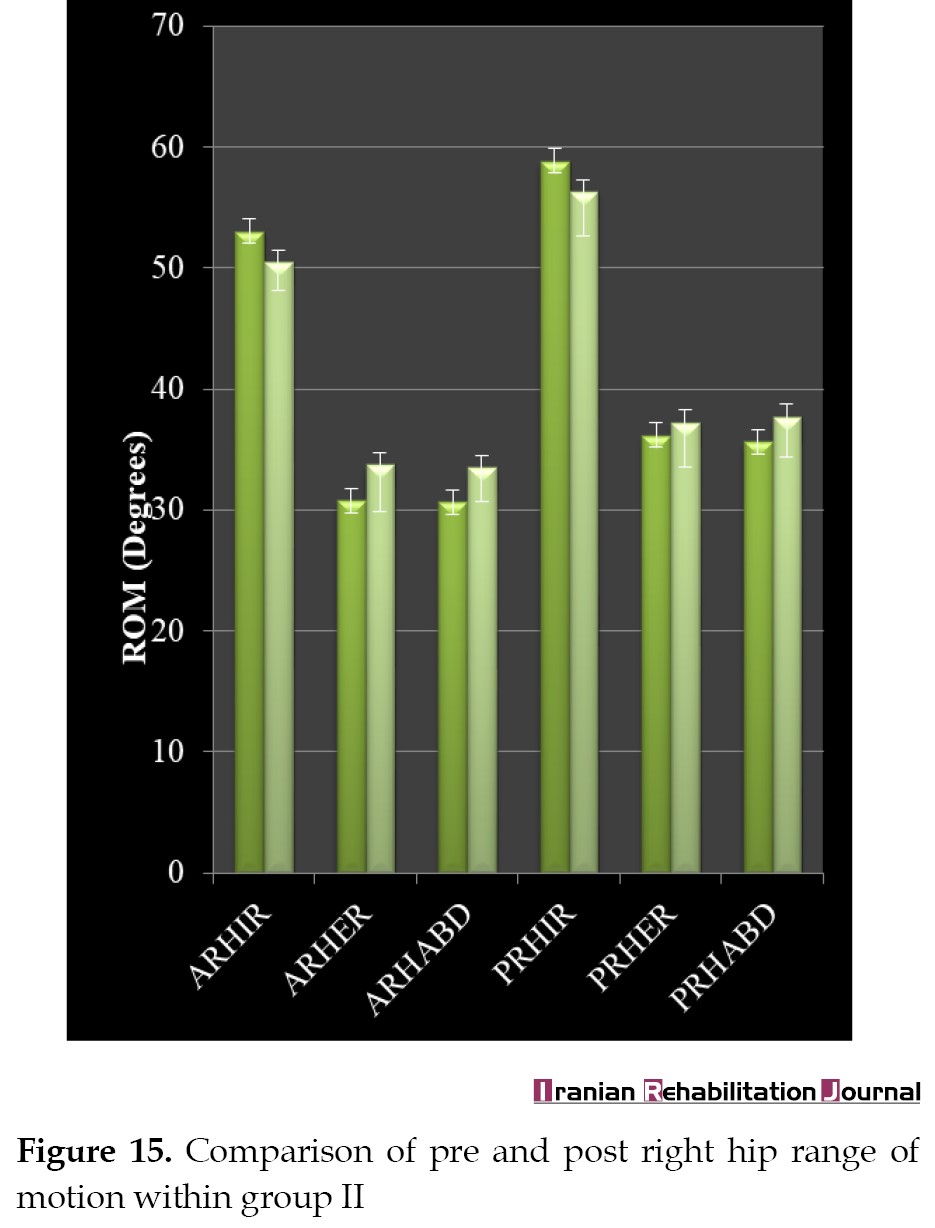
This was a double-blinded randomized control trial. All assessments took place in the physiotherapy clinic of the institution (ITS College of Physiotherapy). Pre and posttest active and passive range of motion (ROM) measurements of right and left hip internal rotation, external rotation, abduction as well as active right and left hip shift were recorded. All assessments were evaluated by another examiner, who was skilled in performing the assessments. The participants were randomly divided into two groups via concealed allocation method using the sequential numbering of opaque, sealed envelopes. The participants draw the next number in the sequence. The participants’ baseline data and details were printed on the envelope before it was opened. The envelope was then opened to disclose the treatment allocation. The researcher and participants were blind in the study in terms of grouping and the received treatment. All the exercises were performed by the same examiner who did the assessment. The participants of both groups received all the exercises twice a day for 3 weeks. Group I (experimental group) received stretching (left external rotators, abductors, right internal rotators and adductors), strengthening (left adductors, internal rotators, medial hamstrings and abdominals, right external rotators and abductors), postural re-education, and right sidelying respiratory left adductor pull back exercise. Group II (control group) received only stretching (left external rotators, abductors, right internal rotators and adductors), strengthening (left adductors, internal rotators, medial hamstrings and abdominals, right external rotators and abductors), and posture re-education.
Stretching of right hip internal rotators and adductors method
The participant was asked to lie supine with both knees bent to 90 degrees. Then, they were asked to bring the right knee to fall all the way to the left as far as it goes toward the floor by rotating the upper legs inward at the hip joint and the therapist gave the overpressure in the end. The stretch was held for 30 sec and was repeated 5 times [18, 19].
Stretching of left hip external rotators and abductors method
The participants were asked to sit with their back straight and against the back of a chair. The participants held the right foot firmly on the floor and rested the left ankle on the right thigh. Then, they were asked to lean forward. The therapist gave the overpressure in the end. The stretch was held for 30 sec and was repeated 5 times [18, 19].
Strengthening of right hip abductors and external rotators method
The participants were asked to lie on their side with backs against a wall and both hips externally rotated, with knees extended and an ankle weight on the top leg. The top leg was raised, and then lowered toward the starting position with a 3 to 5-sec hold. The exercise was repeated 5 times [18, 19].
Strengthening of left hip adductors method
The participants were asked to lie in the left sidelying position with both legs extended, the top right leg on the seat of a chair, and an ankle weight on the lower left leg. The left lower leg was raised, and returned to the starting position with a 3 to 5-sec hold. This exercise was repeated 5 times [18, 19].
Strengthening of left hip internal rotators method
The participants were asked to lie in a prone position with knees bent to 90 degrees and straps placed around the foot. The exercise started with the hip slightly externally rotated and then internally rotated from the hip such that the knee faces inward and the foot of the bent knee moved away from the extended knee. The participant was then asked to return to the starting position following a 3 to 5-sec hold. This exercise was repeated 5 times [18, 19].
Postural re-education method
Each participant received 15 minutes of gentle and gradual therapeutically sustained postural stretching [20]. To lengthen the posterior muscle chain, the participants laid supine with the occipital, lumbar, and sacral spines supported.
To stretch the anterior chain, the participants laid supine with their arms abducted at 30 degrees and the forearms in supination. The hips were flexed, abducted, and laterally rotated while the legs were gradually extended as far as possible while sustaining the 90-degree angle, and respecting the participants’ limits.
Right sidelying respiratory left adductor pull back exercise method
The participants laid on the right side with feet toward the wall, hip and knees at 90 degrees with ankles in line. While keeping the subject’s head, neck, and back comfortable, a towel was placed between the feet and knees, while the subject’s left knee was lowered. The participant was advised to press their right foot onto the wall and inhale through their nose while dragging their left leg back. While pushing their left knee into the towel, the individual exhaled through their mouth for 3 sec. Subsequently, they were advised to tug again from the left leg on inhalation and squeeze down from the left knee on expiration. The training changed into repeated till the affected person had inhaled and exhaled 4 to 5 instances in a row. For 3 weeks, this exercise was performed twice a day, with each repetition consisting of 3 inhalations and 3 exhalations. One set was completed in a single session [21] (Figure 1).
.jpg) Outcome measures
Outcome measures
Measurement of hip rotation range of motion
The participants were asked to sit on a supportive surface with their knees flexed to 90 degrees over the edge of the surface, their hips in 0 degrees of abduction and adduction, and flexion at 90 degrees. To keep the femur in a horizontal plane, a rolled towel was put under the distal end. The goniometer’s fulcrum was positioned over the anterior aspect of the patella, with the proximal arm parallel to the supporting surface and the distal arm aligned with the lower leg’s anterior midline. The standard procedure was used to calculate both active and passive external and internal ROM. [22, 23] (Figure 2).
.jpg) Measurement of hip abduction range of motion
Measurement of hip abduction range of motion
The participants were instructed to lie supine with their knees extended and their hips in 0 degrees of flexion, extension, and rotation. The goniometer’s fulcrum was positioned over the anterior superior iliac spine, the proximal arm with an imaginary horizontal line stretching from one anterior superior iliac spine to the other, and the distal arm with the anterior midline of the femur, using the patella’s midline as a guide. By laterally sliding the lower extremity, the participants were asked to abduct the hip [22, 23] (Figure 3).
.jpg) Measurement of active hip shift
Measurement of active hip shift
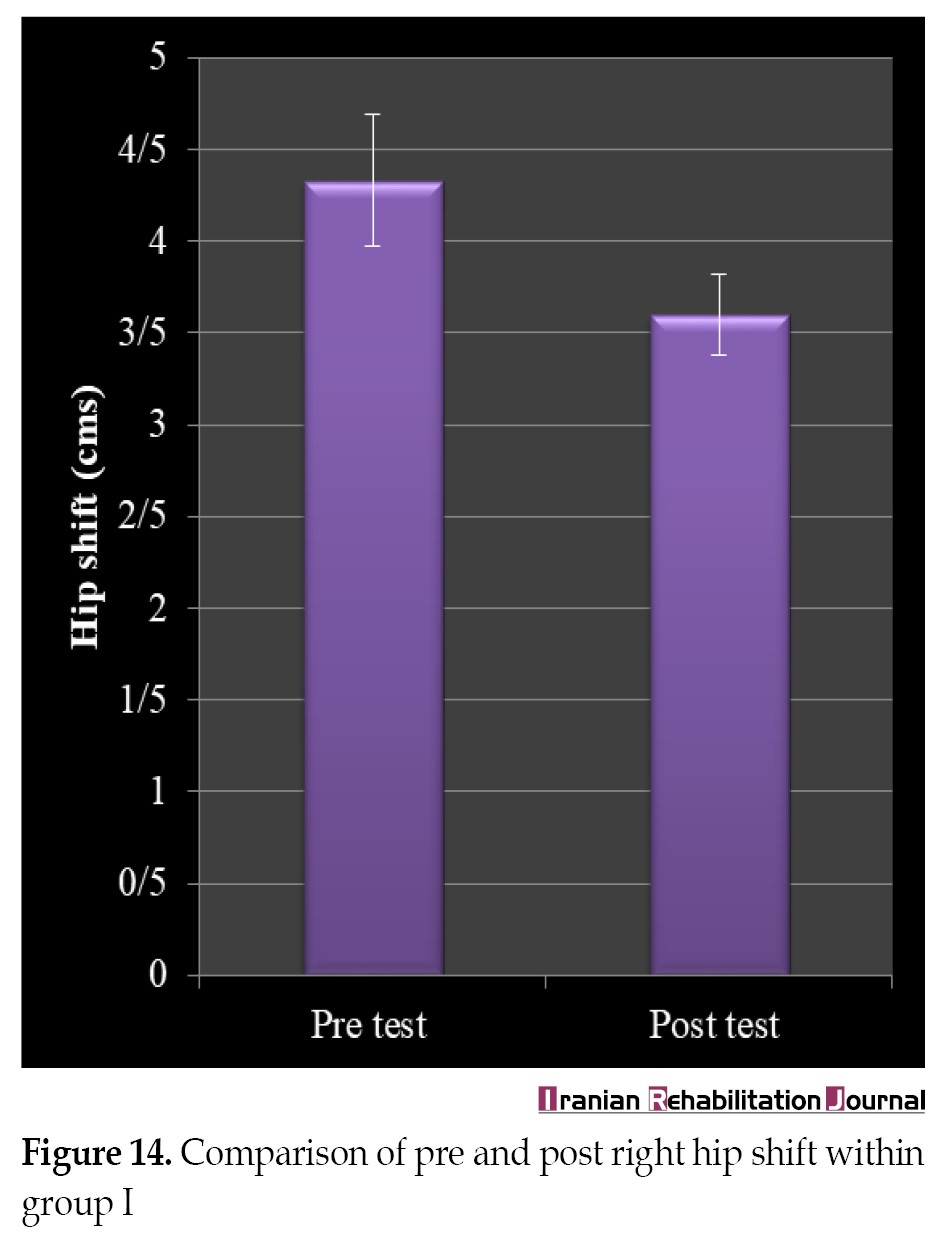
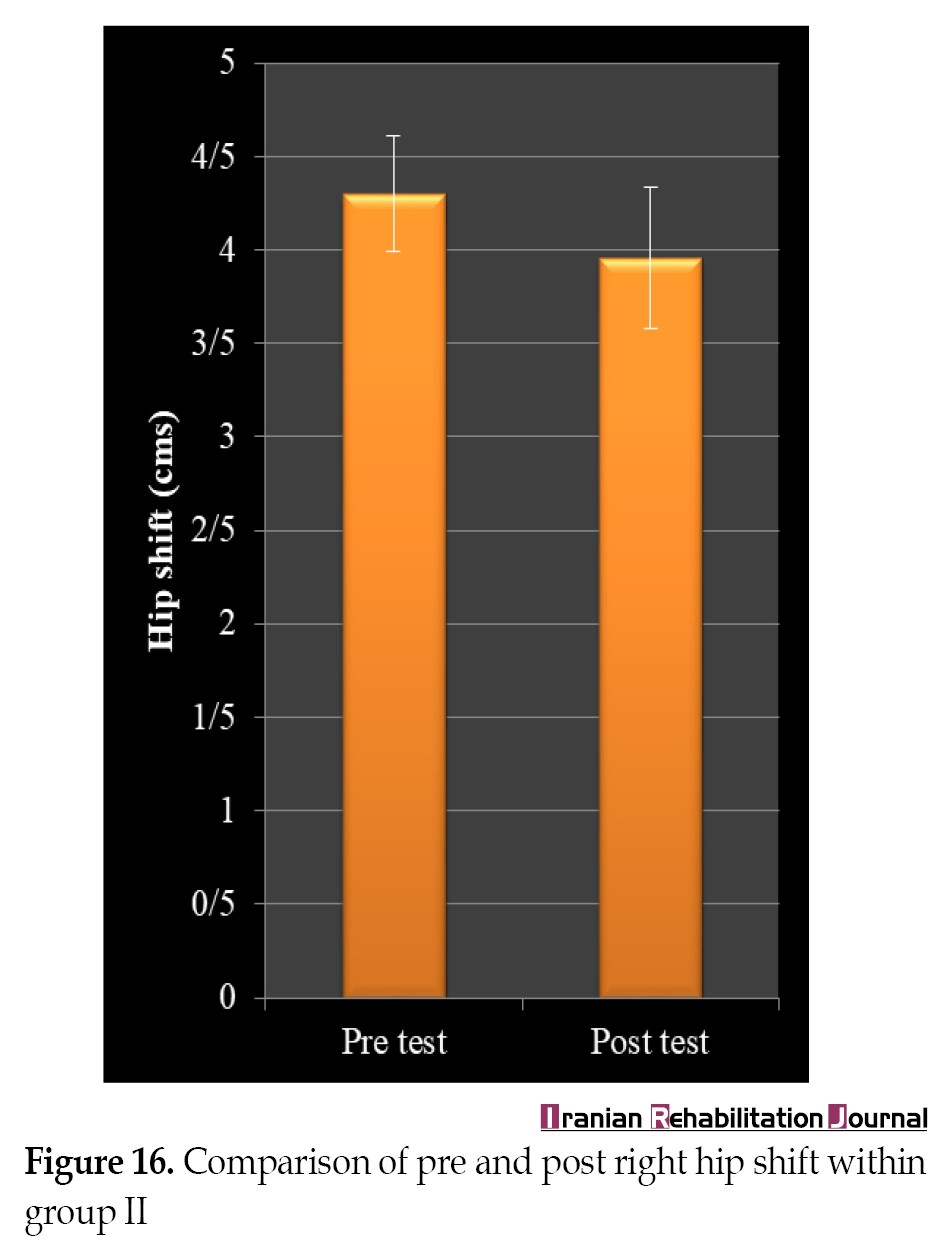
The participants were asked to sit comfortably on a chair. The examiner placed a pad or card in front of the anterior aspect of both knees. This was considered to be the starting position. The participants were then asked to pull the femur (right and left) back one by one, as much as possible. The examiner measured the exact distance in cm through a scale from the starting position to the end position [21] (Figure 4).
.jpg) Data analysis
Data analysis
The SPSS software, version 16 was used to analyze the results. To find variations between the demographic and baseline statistics of the subjects, an independent t test was used. The independent t test was used to examine between-group differences, while the paired t-test was employed to examine within-group differences. For P<0.05, the differences were considered statistically significant.
3. Results
General characteristics of the participants
At the start of the study, there were no significant variations in age, height, weight, or baseline readings (Tables 1, 2, 3, 4).
.jpg)
.jpg)
.jpg)
.jpg)
Between-group analysis
The difference was determined by subtracting the post-mean and pre-mean values and expressing the result as mean±SD. All the variables, including right and left hip active and passive internal and external rotation, external rotation, abduction, and right and left hip change, showed statistically significant differences between the mean values of groups I and II. (Tables 5, 6, 7) (Figures 5, 6, 7, 8).
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg) In comparison, the experimental (group I) showed greater changes compared to the control group (group II).
In comparison, the experimental (group I) showed greater changes compared to the control group (group II).
Within-group analysis
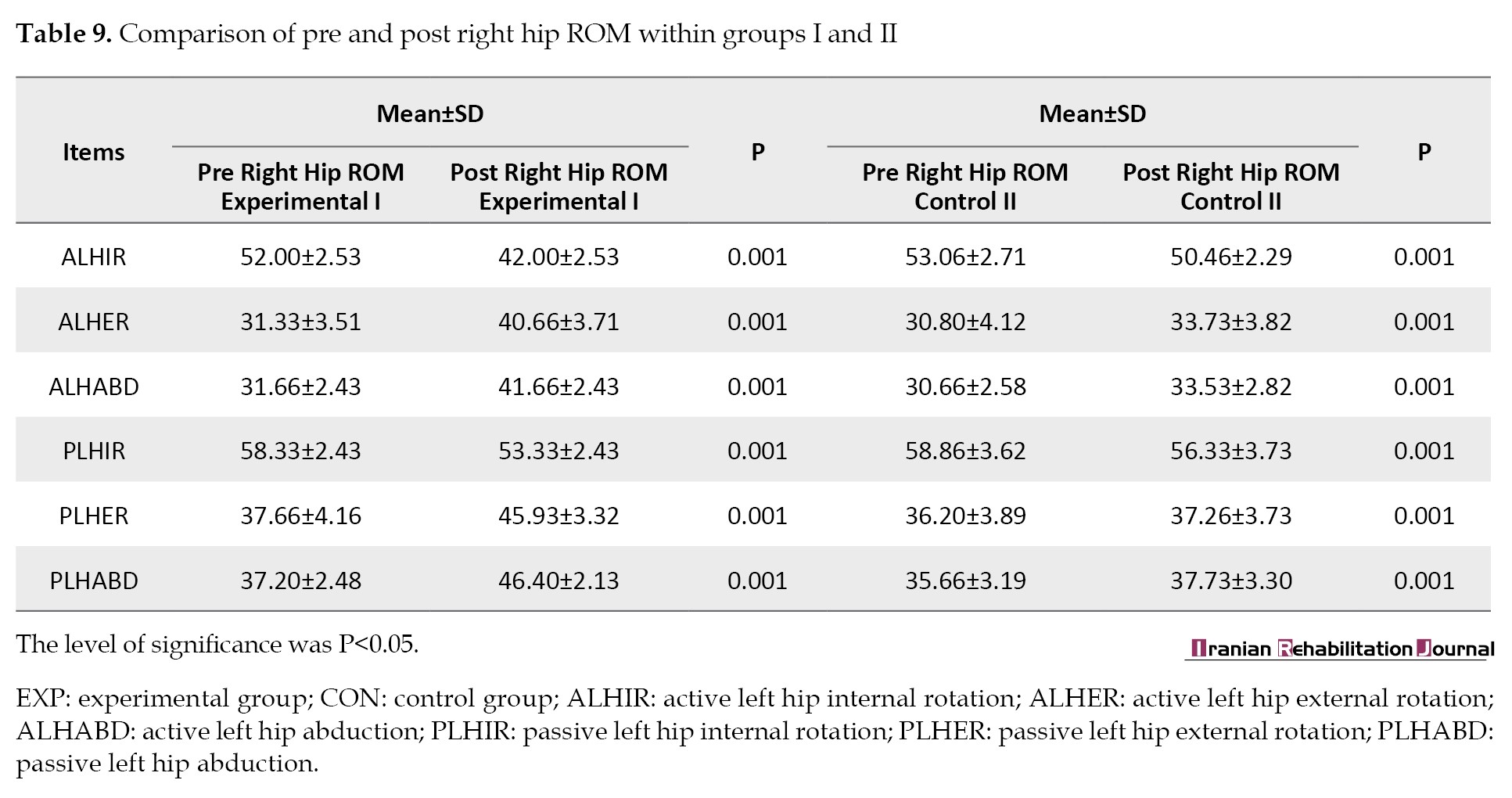
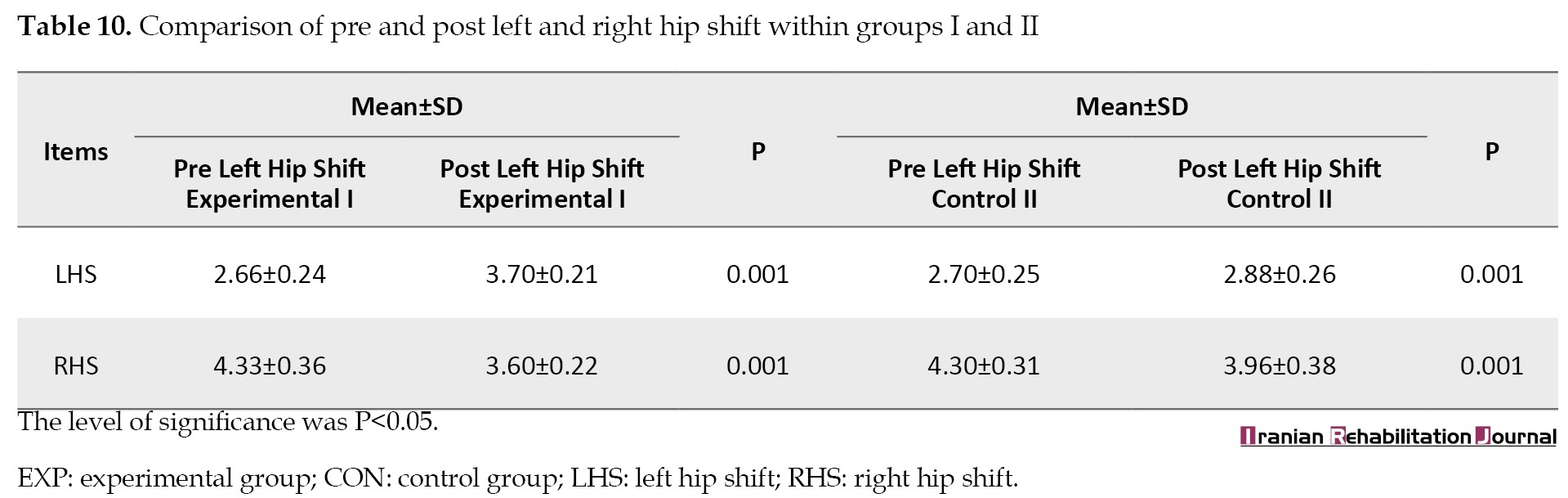
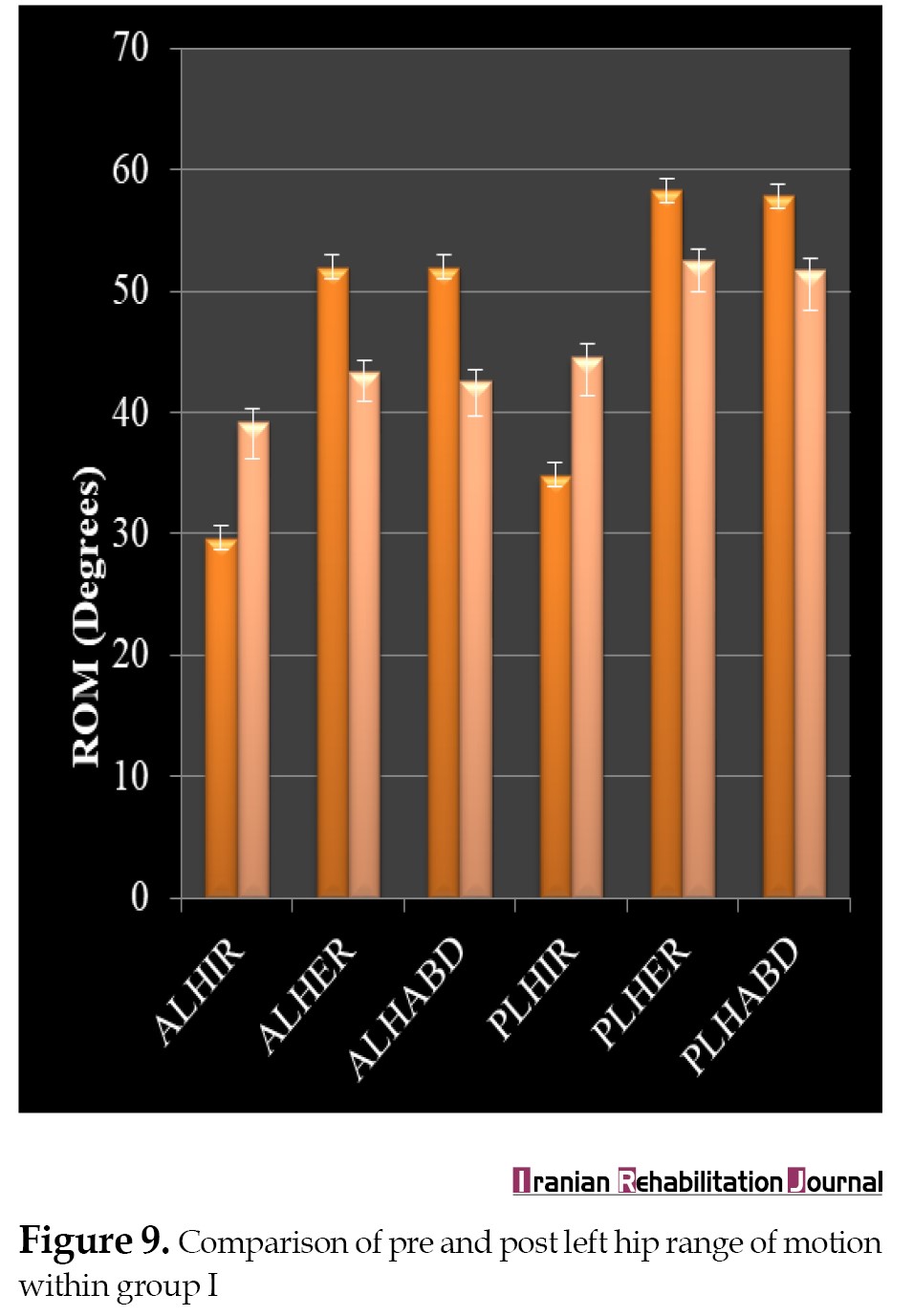
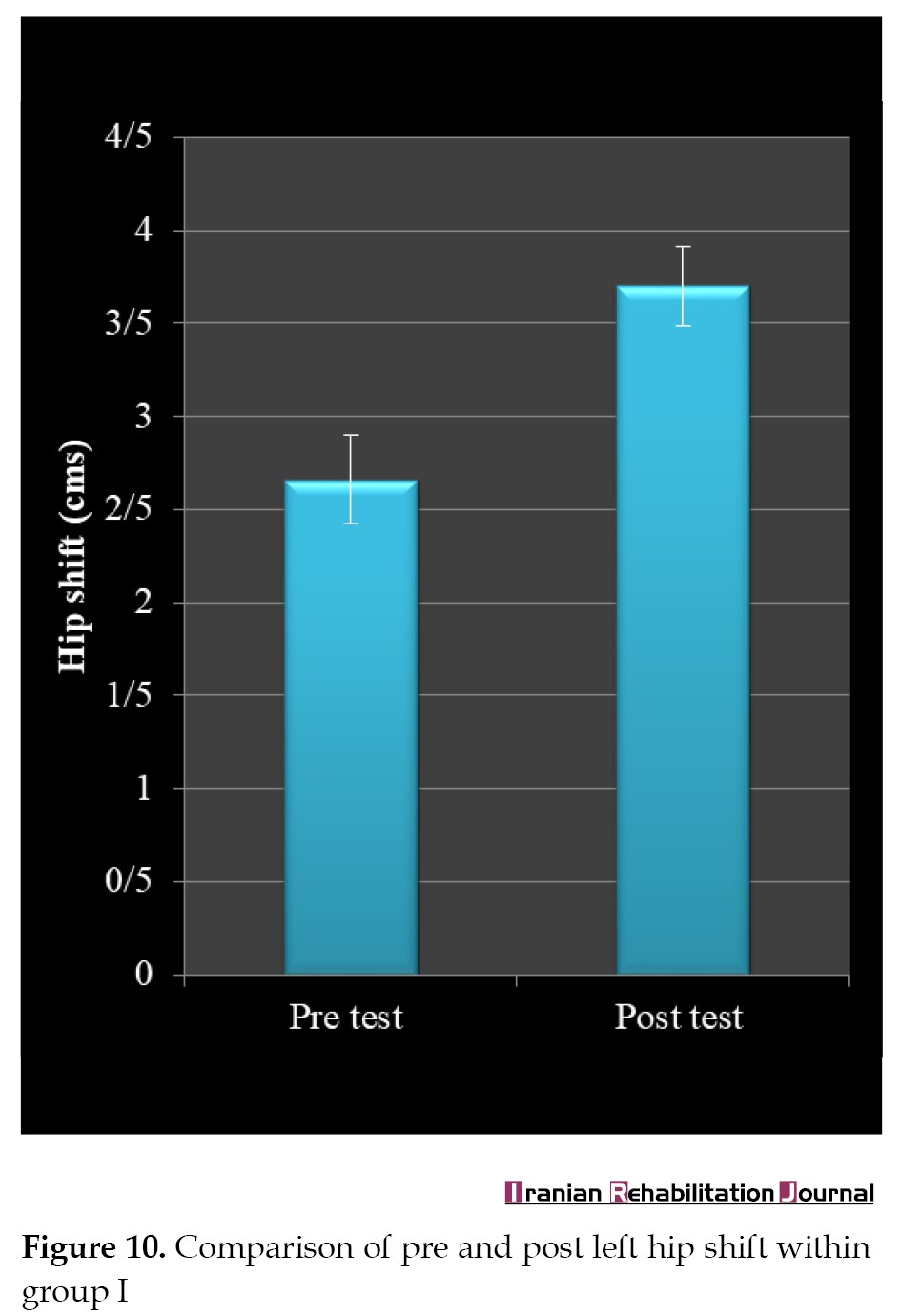
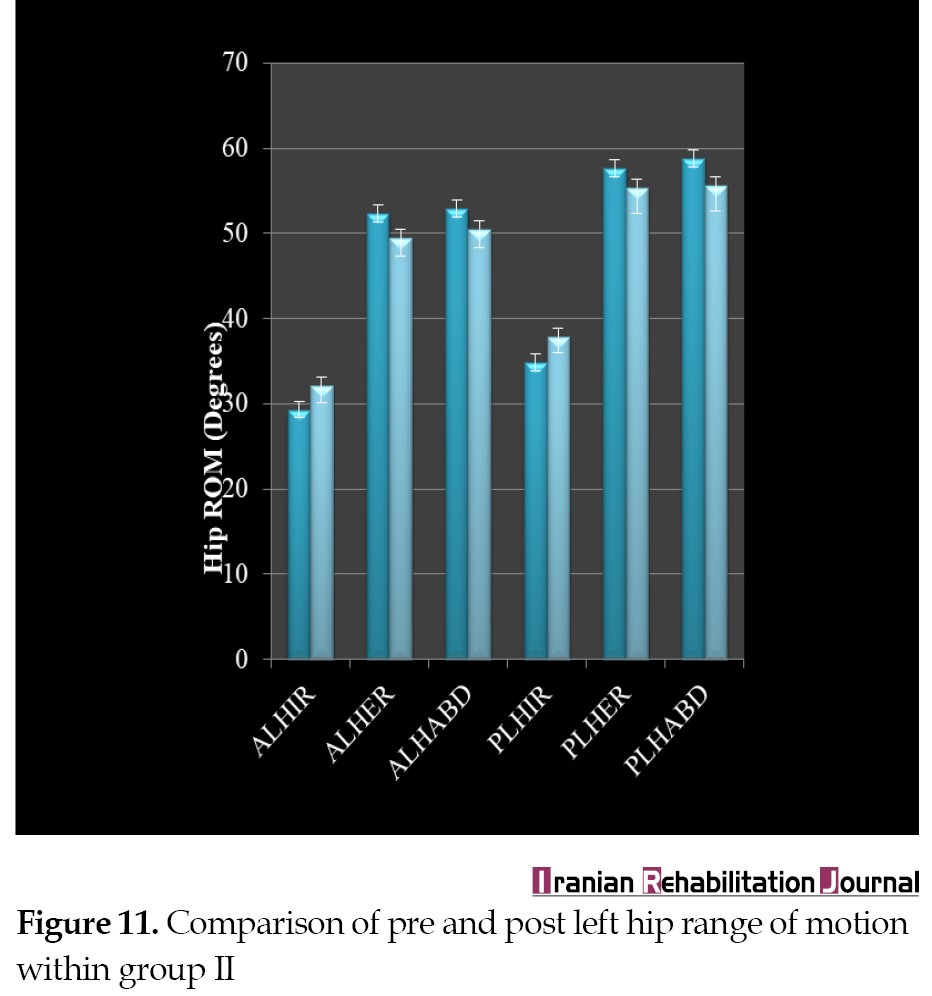
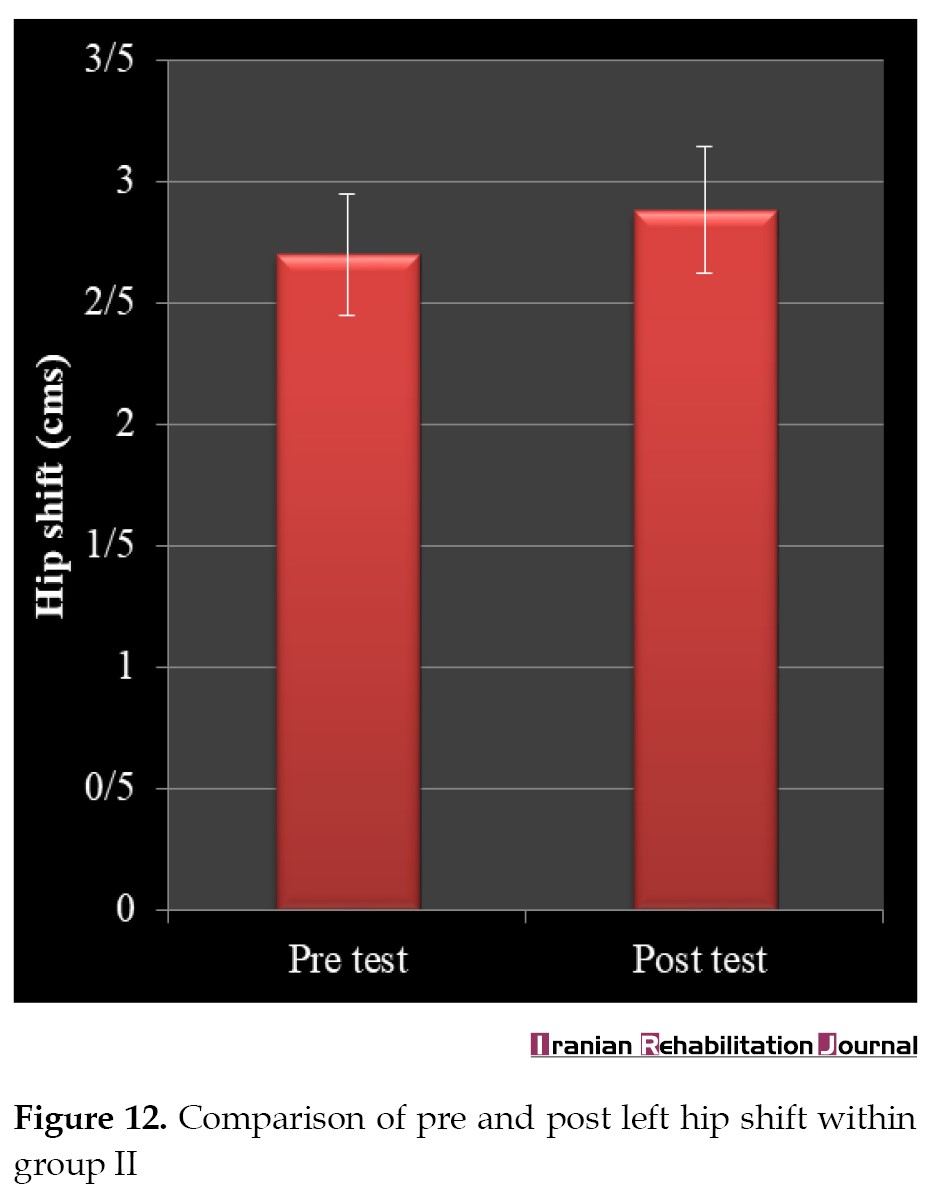
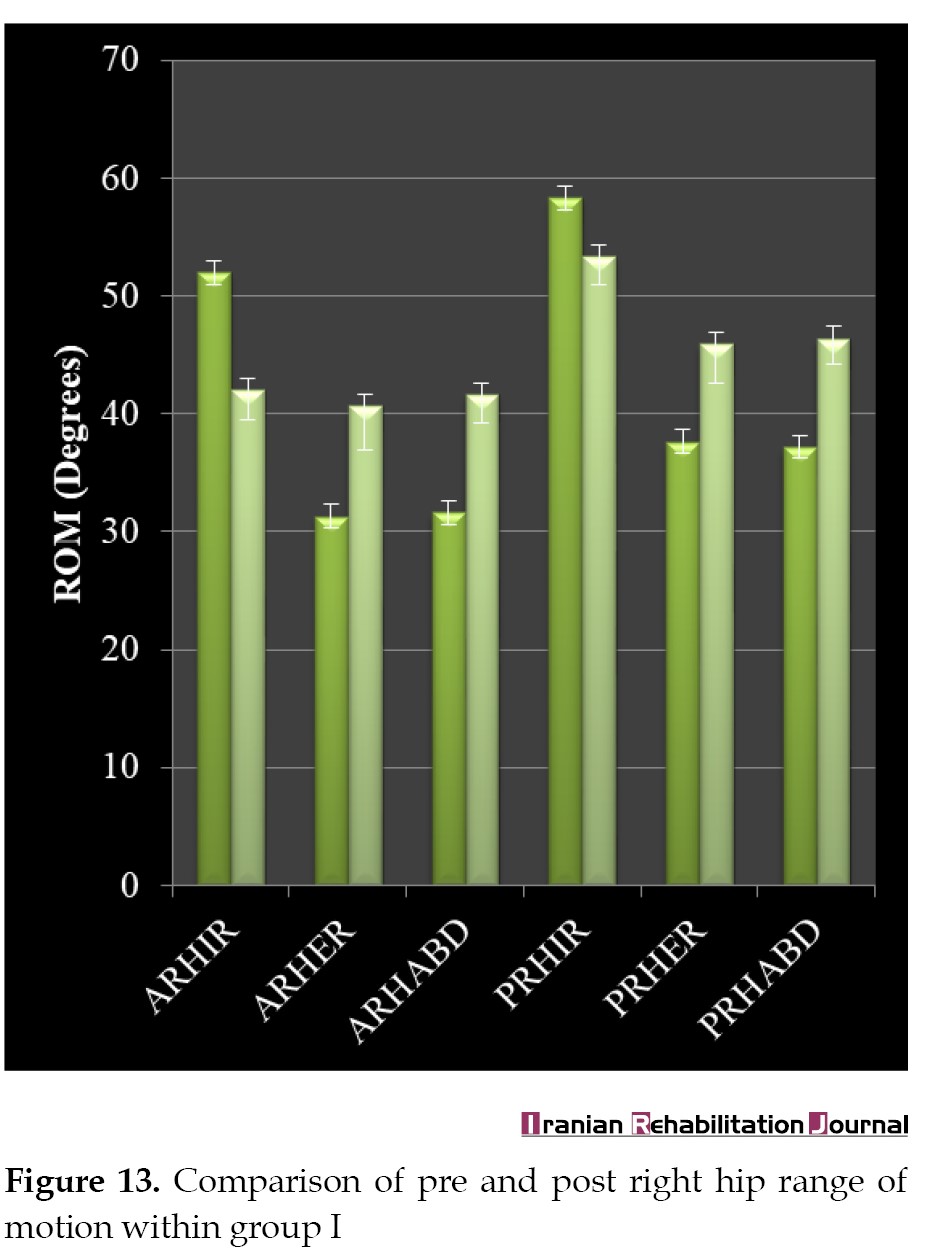
Significant improvement was also found in all the pre- and post-intervention mean values within groups I and II (Tables 8, 9, 10) (Figures 9, 10, 11, 12, 13, 14, 15, 16).
.jpg)
 4. Discussion
4. Discussion
Our findings showed how hip biomechanics, as measured by the ROM and hip change, can be influenced by a novel exercise that addresses postural deviations and irregular chain forms. After 3 weeks of adductor pull back exercise, participants demonstrated significant progress in all variables.
Sai et al. observed comparable results in a study that combined 2 weeks of adductor pull back exercise with standard training; this improved pain and functional impairment in persons with sacroiliac joint dysfunction [17].
The findings of this research are in line with the study conducted by Shori G. and Joshi A. Their study revealed that 3 weeks of right sidelying left adductor pull back training improves hip adduction angle and corrects postural asymmetry induced by iliotibial band tightness [16].
The adductor pull back exercise was suggested by the Postural Restoration Institute to transpose the lumbar and pelvic areas of the body [7]. When the large padding is placed between the ankle and the foot, it relaxes, inhibits, or lengthens the paraspinals, and induces left femoral internal rotation. The left posterior hip capsule and the ischiofemoral ligament are pushed even more into a lengthened position as a result of compensating for a left anterior internal chain arrangement [12, 24, 25, 26]. This active technique also guides the respiratory structures and pushes them into a mechanical advantage so that they can work efficiently. This innovative technique also promotes relaxation via parasympathetic activation [3].
The findings of this research were consistent with 4 previously published case studies that illustrated related techniques or exercises. The authors of these case studies have discussed postural asymmetry impairments, reporting significant improvements in function and pain severity. A case study was reported by Kyndall L. Boyle on managing a female patient with left low back pain and sacroiliac joint pain with therapeutic exercise [3]. For the previous 10 months, the patient, a 65-year-old woman, had been suffering from pain in her back and leg. She was treated 6 times with exercises to correct a pelvic malalignment. The patient’s examination was negative and she was out of pain.
Another case report, “Management of a Female With Chronic Sciatica and Low Back Pain,” was written by Boyle KL and Demske JR. [27]. The patient was a 61-year-old woman with chronic right sciatica and low back discomfort. She had a 9-point pain scale, a 45-degree straight leg raise, and a positive Ober test on initial inspection. The Oswestry disability index stood at 40%. For the first 6 weeks, the patient was taught spinal flexion and stabilization exercises (5 visits). Muscle stimulation of the specific group of muscles, stretching of the left posterior hip capsule, and muscle inhibition for the paraspinals were added to the intervention schedule for an additional 13 weeks (10 visits) to reposition and stabilize the pelvis. The patient was discharged with no pain, a negative Ober test, and an Oswestry disability index of 0%.
In a case study, “Bilateral Functional Thoracic Outlet Syndrome in a College Football Player,” by Jason H. Robey and Kyndall L. Boyle [28], a college football player was diagnosed with chronic cervical traction neuropraxia and functional thoracic outlet syndrome. The athlete’s problems remained unresolved despite 4 weeks of shoulder strengthening and stretching. Four doctors recommended surgery for his problem and retirement from football. By activating and inhibiting muscles, the Postural Restoration Institute’s unique therapy exercises were employed to enhance breathing and posture. After 6 weeks, the player was asymptomatic and returned to football.
Holly Spence in his study, “Postural Restoration: An Effective Physical Therapy Approach to Patient Treatment” [29], reported a 40-year-old woman who has discomfort in her neck, back, left leg, left hip, right glenohumeral joint, and temporomandibular joint and medical history of acid reflux, and renal colic spring. The patient has had right foot surgery, right rotator cuff surgery, heart catheterization, and 2 vehicle accidents in his past. Over 6 months, this patient received manual and non-manual training procedures as well as a home regimen. After 6 weeks, she had no discomfort and was able to ski 3 days in a row and perform activities of daily living without pain.
Study limitations
Regarding the study limitations, the sample size was wide and the age range of the sample size was narrow. The statistical analysis provided enough power for the study to detect the differences. To evaluate the long-term effects of this intervention on various groups and outcomes, further research is needed.
5. Conclusion
The results showed that the specific form of exercise used in this study improves hip biomechanics in participants who prefer to stand on their right side. This exercise corrects related postural asymmetry, while also assisting in the establishment of a natural respiratory pattern and easing the individual’s involvement in activities of daily living.
Ethical Considerations
Compliance with ethical guidelines
The present research was conducted in full accordance with ethical principles. Experiments were undertaken with the understanding and written consent of each participant. The study has been reviewed and approved by the Institutional Ethics Committee (Code: ITS.COP.REC.1025.775).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to acknowledge, Ruchika Gupta, for extending help in data analysis and interpretation.
References
Succinct functional patterns govern and produce many systems, and posture is a symbol of their role. These forms reflect our inclination and incapability to spin and rest evenly with the left and right hemispheres of our axial structures [1].
Individuals with a tendency to change their body weight or center of gravity linked with the pelvis and lumbar vertebrae rotate on one side while the upper thoracic and the pubic symphysis rotate on the opposite, have been discussed in the literature as the left anterior interior chain (Left AIC) pattern [2, 3, 4, 5]. These uneven patterns have been linked to a muscle chain that stretches numerous joints and overlaps without a break in continuity, generating an imbalance [6, 7, 8, 9].
The above-mentioned pattern is demonstrated with imbalances in muscles and associated soft tissues, resulting in compensation in areas of the trunk, and connected limbs [10]. The biomechanics of the linked pelvic position also changes and influences the motion and potential arthrokinematics of the hip joint, as well as creating a functional impingement [11, 12, 13].
If not addressed timely, these abnormal positional patterns may lead to movement dysfunctions, structural changes, and distorted movement [14, 15]. These subsequent abnormal alignments may result in the decline of the individual’s participation in activities of daily living [4].
An intense rehabilitative exercise that corrects postural asymmetry and helps to restore normal bone and soft tissue posture of the trunk and pelvis is beneficial to patients. Although physical therapists use the right sidelying respiratory left adductor pull back exercise for a variety of musculoskeletal conditions [16, 17], there is a paucity of research on this technique’s efficacy. Therefore, this research aims to explore the effect of right sidelying respiratory left adductor pull back exercise on improving hip biomechanics in participants with a tendency to stand on the right side.
2. Materials and Methods
Study participants
A total of 30 participants (6 females and 24 males) with Mean±SD age of 28.53±2.62 years, Mean±SD weight of 63.83±3.89 kg, and Mean±SD height of 165.8±3.97 cm were recruited and randomly divided into experimental (n=15) and control groups (n=15). The potential candidates were screened using a standardized procedure. Posters, standees, and electronic notice boards were used to invite potential participation. A certified assessor visually assessed the posture. The person was examined in their regular relaxed position. The inclusion criteria comprised the following items: age range of 25 to 40 years, both sexes, and a tendency to stand on the right side given their affirmative answer on the self-declaration form indicating that they spend the majority of their time in this position. The exclusion criteria comprised the following items: having musculoskeletal injuries or other neurological and systemic illness as diagnosed by a physician, receiving any other training or intervention, having limb length discrepancy, inability to follow the commands (patients with cognitive impairment and inability to understand the language and or instructions), having a tendency to stand on the left side. The participants were excluded based on the self-reported form. Before collecting the data, all participants signed an informed consent form. Experimental procedure was also clarified to the participants using standard process. The study protocol was approved by the Institutional Ethics Committee (Code: ITS.COP.REC.1025.775).
Study procedure
This was a double-blinded randomized control trial. All assessments took place in the physiotherapy clinic of the institution (ITS College of Physiotherapy). Pre and posttest active and passive range of motion (ROM) measurements of right and left hip internal rotation, external rotation, abduction as well as active right and left hip shift were recorded. All assessments were evaluated by another examiner, who was skilled in performing the assessments. The participants were randomly divided into two groups via concealed allocation method using the sequential numbering of opaque, sealed envelopes. The participants draw the next number in the sequence. The participants’ baseline data and details were printed on the envelope before it was opened. The envelope was then opened to disclose the treatment allocation. The researcher and participants were blind in the study in terms of grouping and the received treatment. All the exercises were performed by the same examiner who did the assessment. The participants of both groups received all the exercises twice a day for 3 weeks. Group I (experimental group) received stretching (left external rotators, abductors, right internal rotators and adductors), strengthening (left adductors, internal rotators, medial hamstrings and abdominals, right external rotators and abductors), postural re-education, and right sidelying respiratory left adductor pull back exercise. Group II (control group) received only stretching (left external rotators, abductors, right internal rotators and adductors), strengthening (left adductors, internal rotators, medial hamstrings and abdominals, right external rotators and abductors), and posture re-education.
Stretching of right hip internal rotators and adductors method
The participant was asked to lie supine with both knees bent to 90 degrees. Then, they were asked to bring the right knee to fall all the way to the left as far as it goes toward the floor by rotating the upper legs inward at the hip joint and the therapist gave the overpressure in the end. The stretch was held for 30 sec and was repeated 5 times [18, 19].
Stretching of left hip external rotators and abductors method
The participants were asked to sit with their back straight and against the back of a chair. The participants held the right foot firmly on the floor and rested the left ankle on the right thigh. Then, they were asked to lean forward. The therapist gave the overpressure in the end. The stretch was held for 30 sec and was repeated 5 times [18, 19].
Strengthening of right hip abductors and external rotators method
The participants were asked to lie on their side with backs against a wall and both hips externally rotated, with knees extended and an ankle weight on the top leg. The top leg was raised, and then lowered toward the starting position with a 3 to 5-sec hold. The exercise was repeated 5 times [18, 19].
Strengthening of left hip adductors method
The participants were asked to lie in the left sidelying position with both legs extended, the top right leg on the seat of a chair, and an ankle weight on the lower left leg. The left lower leg was raised, and returned to the starting position with a 3 to 5-sec hold. This exercise was repeated 5 times [18, 19].
Strengthening of left hip internal rotators method
The participants were asked to lie in a prone position with knees bent to 90 degrees and straps placed around the foot. The exercise started with the hip slightly externally rotated and then internally rotated from the hip such that the knee faces inward and the foot of the bent knee moved away from the extended knee. The participant was then asked to return to the starting position following a 3 to 5-sec hold. This exercise was repeated 5 times [18, 19].
Postural re-education method
Each participant received 15 minutes of gentle and gradual therapeutically sustained postural stretching [20]. To lengthen the posterior muscle chain, the participants laid supine with the occipital, lumbar, and sacral spines supported.
To stretch the anterior chain, the participants laid supine with their arms abducted at 30 degrees and the forearms in supination. The hips were flexed, abducted, and laterally rotated while the legs were gradually extended as far as possible while sustaining the 90-degree angle, and respecting the participants’ limits.
Right sidelying respiratory left adductor pull back exercise method
The participants laid on the right side with feet toward the wall, hip and knees at 90 degrees with ankles in line. While keeping the subject’s head, neck, and back comfortable, a towel was placed between the feet and knees, while the subject’s left knee was lowered. The participant was advised to press their right foot onto the wall and inhale through their nose while dragging their left leg back. While pushing their left knee into the towel, the individual exhaled through their mouth for 3 sec. Subsequently, they were advised to tug again from the left leg on inhalation and squeeze down from the left knee on expiration. The training changed into repeated till the affected person had inhaled and exhaled 4 to 5 instances in a row. For 3 weeks, this exercise was performed twice a day, with each repetition consisting of 3 inhalations and 3 exhalations. One set was completed in a single session [21] (Figure 1).
Measurement of hip rotation range of motion
The participants were asked to sit on a supportive surface with their knees flexed to 90 degrees over the edge of the surface, their hips in 0 degrees of abduction and adduction, and flexion at 90 degrees. To keep the femur in a horizontal plane, a rolled towel was put under the distal end. The goniometer’s fulcrum was positioned over the anterior aspect of the patella, with the proximal arm parallel to the supporting surface and the distal arm aligned with the lower leg’s anterior midline. The standard procedure was used to calculate both active and passive external and internal ROM. [22, 23] (Figure 2).
The participants were instructed to lie supine with their knees extended and their hips in 0 degrees of flexion, extension, and rotation. The goniometer’s fulcrum was positioned over the anterior superior iliac spine, the proximal arm with an imaginary horizontal line stretching from one anterior superior iliac spine to the other, and the distal arm with the anterior midline of the femur, using the patella’s midline as a guide. By laterally sliding the lower extremity, the participants were asked to abduct the hip [22, 23] (Figure 3).
The participants were asked to sit comfortably on a chair. The examiner placed a pad or card in front of the anterior aspect of both knees. This was considered to be the starting position. The participants were then asked to pull the femur (right and left) back one by one, as much as possible. The examiner measured the exact distance in cm through a scale from the starting position to the end position [21] (Figure 4).
The SPSS software, version 16 was used to analyze the results. To find variations between the demographic and baseline statistics of the subjects, an independent t test was used. The independent t test was used to examine between-group differences, while the paired t-test was employed to examine within-group differences. For P<0.05, the differences were considered statistically significant.
3. Results
General characteristics of the participants
At the start of the study, there were no significant variations in age, height, weight, or baseline readings (Tables 1, 2, 3, 4).
Between-group analysis
The difference was determined by subtracting the post-mean and pre-mean values and expressing the result as mean±SD. All the variables, including right and left hip active and passive internal and external rotation, external rotation, abduction, and right and left hip change, showed statistically significant differences between the mean values of groups I and II. (Tables 5, 6, 7) (Figures 5, 6, 7, 8).
Within-group analysis
Significant improvement was also found in all the pre- and post-intervention mean values within groups I and II (Tables 8, 9, 10) (Figures 9, 10, 11, 12, 13, 14, 15, 16).
Our findings showed how hip biomechanics, as measured by the ROM and hip change, can be influenced by a novel exercise that addresses postural deviations and irregular chain forms. After 3 weeks of adductor pull back exercise, participants demonstrated significant progress in all variables.
Sai et al. observed comparable results in a study that combined 2 weeks of adductor pull back exercise with standard training; this improved pain and functional impairment in persons with sacroiliac joint dysfunction [17].
The findings of this research are in line with the study conducted by Shori G. and Joshi A. Their study revealed that 3 weeks of right sidelying left adductor pull back training improves hip adduction angle and corrects postural asymmetry induced by iliotibial band tightness [16].
The adductor pull back exercise was suggested by the Postural Restoration Institute to transpose the lumbar and pelvic areas of the body [7]. When the large padding is placed between the ankle and the foot, it relaxes, inhibits, or lengthens the paraspinals, and induces left femoral internal rotation. The left posterior hip capsule and the ischiofemoral ligament are pushed even more into a lengthened position as a result of compensating for a left anterior internal chain arrangement [12, 24, 25, 26]. This active technique also guides the respiratory structures and pushes them into a mechanical advantage so that they can work efficiently. This innovative technique also promotes relaxation via parasympathetic activation [3].
The findings of this research were consistent with 4 previously published case studies that illustrated related techniques or exercises. The authors of these case studies have discussed postural asymmetry impairments, reporting significant improvements in function and pain severity. A case study was reported by Kyndall L. Boyle on managing a female patient with left low back pain and sacroiliac joint pain with therapeutic exercise [3]. For the previous 10 months, the patient, a 65-year-old woman, had been suffering from pain in her back and leg. She was treated 6 times with exercises to correct a pelvic malalignment. The patient’s examination was negative and she was out of pain.
Another case report, “Management of a Female With Chronic Sciatica and Low Back Pain,” was written by Boyle KL and Demske JR. [27]. The patient was a 61-year-old woman with chronic right sciatica and low back discomfort. She had a 9-point pain scale, a 45-degree straight leg raise, and a positive Ober test on initial inspection. The Oswestry disability index stood at 40%. For the first 6 weeks, the patient was taught spinal flexion and stabilization exercises (5 visits). Muscle stimulation of the specific group of muscles, stretching of the left posterior hip capsule, and muscle inhibition for the paraspinals were added to the intervention schedule for an additional 13 weeks (10 visits) to reposition and stabilize the pelvis. The patient was discharged with no pain, a negative Ober test, and an Oswestry disability index of 0%.
In a case study, “Bilateral Functional Thoracic Outlet Syndrome in a College Football Player,” by Jason H. Robey and Kyndall L. Boyle [28], a college football player was diagnosed with chronic cervical traction neuropraxia and functional thoracic outlet syndrome. The athlete’s problems remained unresolved despite 4 weeks of shoulder strengthening and stretching. Four doctors recommended surgery for his problem and retirement from football. By activating and inhibiting muscles, the Postural Restoration Institute’s unique therapy exercises were employed to enhance breathing and posture. After 6 weeks, the player was asymptomatic and returned to football.
Holly Spence in his study, “Postural Restoration: An Effective Physical Therapy Approach to Patient Treatment” [29], reported a 40-year-old woman who has discomfort in her neck, back, left leg, left hip, right glenohumeral joint, and temporomandibular joint and medical history of acid reflux, and renal colic spring. The patient has had right foot surgery, right rotator cuff surgery, heart catheterization, and 2 vehicle accidents in his past. Over 6 months, this patient received manual and non-manual training procedures as well as a home regimen. After 6 weeks, she had no discomfort and was able to ski 3 days in a row and perform activities of daily living without pain.
Study limitations
Regarding the study limitations, the sample size was wide and the age range of the sample size was narrow. The statistical analysis provided enough power for the study to detect the differences. To evaluate the long-term effects of this intervention on various groups and outcomes, further research is needed.
5. Conclusion
The results showed that the specific form of exercise used in this study improves hip biomechanics in participants who prefer to stand on their right side. This exercise corrects related postural asymmetry, while also assisting in the establishment of a natural respiratory pattern and easing the individual’s involvement in activities of daily living.
Ethical Considerations
Compliance with ethical guidelines
The present research was conducted in full accordance with ethical principles. Experiments were undertaken with the understanding and written consent of each participant. The study has been reviewed and approved by the Institutional Ethics Committee (Code: ITS.COP.REC.1025.775).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to acknowledge, Ruchika Gupta, for extending help in data analysis and interpretation.
References
- Hruska R. Myokinematic restoration: An integrated approach to treatment of patterned lumbo-pelvic femoral pathomechanics. Lincoln: Postural Restoration Institute; 2006.
- Boyle KL. Management of a female with left low back pain and sacroiliac joint pain with therapeutic exercise: A case report. Physiotherapy Canada. 2011; 63(2):154-63. [DOI:10.3138/ptc.2009-37] [PMID] [PMCID]
- Boyle KL. Conservative management for patients with sacroiliac joint dysfunction. In: Norasteh AA, editor. Low Back Pain. Nordersted: BoD–Books on Demand; 2012. [DOI:10.5772/33878]
- Kouwenhoven JW, Vincken KL, Bartels LW, Castelein RM. Analysis of preexistent vertebral rotation in the normal spine. Spine. 2006; 31(13):1467-72. [DOI:10.1097/01.brs.0000219938.14686.b3] [PMID]
- Boulay C, Tardieu C, Bénaim C, Hecquet J, Marty C, Prat-Pradal D et al. Three dimensional study of pelvic asymmetry on anatomical specimens and its clinical perspectives. Journal of Anatomy. 2006; 208:21-33. [DOI:10.1111/j.1469-7580.2006.00513.x] [PMID] [PMCID]
- Boyle KL. Ethnography of the postural restoration subculture: A posture-based approach to patient/client management [PhD Dissertation]. Florida: Nova Southeastern University; 2006. [Link]
- Tenney HR, Boyle KL, Debord A. Influence of hamstring and abdominal muscle activation on a positive ober’s test in people with lumbopelvic pain. Physiotherapy Canada. 2013; 65(1):4-11. [DOI:10.3138/ptc.2011-33] [PMID] [PMCID]
- Boyle KL, Olinick J, Lewis C. The value of blowing up a balloon. North American Journal of Sports Physical Therapy. 2010; 5(3):179-88. [PMID] [PMCID]
- Kolar P, Sulc J, Kyncl M, Sanda J, Neuwirth J, Bokarius A V, et al. Stabilizing function of the diaphragm: Dynamic MRI and synchronized spirometric assessment. Journal of Applied Physiology. 2009; 109(4):1064-71. [DOI:10.1152/japplphysiol.01216.2009] [PMID]
- Postural Restoration Institute®. Postural Restoration Myokinematic Manual®; 2017.
- Flynn T. The thoracic spine and rib cage: Musculoskeletal evaluation and treatment. Oxford: Butterworth- Heinemann; 2008. [Link]
- Goldman M, Mead J. Mechanical interaction between the diaphragm and the rib cage. Journal of Applied Physiology. 1973; 35(2):197-204. [DOI:10.1152/jappl.1973.35.2.197] [PMID]
- Hodges PW, Gandevia SC, Richardson CA. Contractions of specific abdominal muscles in postural tasks are affected by respiratory maneuvers. Journal of Applied Physiology. 1997; 83(3):753-60. [DOI:10.1152/jappl.1997.83.3.753] [PMID]
- Bussey DM. Does the demand for asymmetric functional lower body postures in lateral sports relate to structural asymmetry of the pelvis? Journal of Science and Medicine in Sport. 2010; 13(3):360-4. [DOI:10.1016/j.jsams.2009.02.010] [PMID]
- Wolpert L. Development of the asymmetric human. European Review. 2005; 13(S2):97-103. [DOI:10.1017/S1062798705000682]
- Shori G, Joshi A. Effect of right sidelying respiratory left adductor pull back exercise in subjects with iliotibial band tightness. Physiotherapy Quarterly. 2017; 25(1):13-6. [DOI:10.1515/physio-2016-0014]
- Kumar SN, Akalwadi A, Babu VK, Wani ZR. Efficacy of adductor pull back exercise on pain and functional disability for scaroiliac joint dysfunction. International Journal of Physiotherapy. 2015; 2(4):667-75. [DOI:10.15621/ijphy/2015/v2i4/67748]
- Clippinger SK. Dance anatomy and kinesiology: Human kinetics; 2007. [Link]
- Donnelly EJ. Joseph Living Anatomy: Champaign: Human Kinetic; 1990. [Link]
- Teodori RM, Negri JR, Cruz MC, Marques AP. Global postural re-education: A literature review. Revista Brasileira de Fisioterapia. 2011; 15(3):185-9. [DOI:10.1590/S1413-35552011000300003] [PMID]
- Boyle K. Clinical application of the right sidelying respiratory left adductor pull back exercise. International Journal of Sports Physical Therapy. 2013; 8(3):349-58. [PMID] [PMCID]
- Greene, W B, Heckman, J D. The clinical measurement of joint motion. Rosemont: American Academy of Orthopaedic Surgeons; 1994. [Link]
- Roach KE, Miles TP. Normal hip and knee active range of motion: The relationship to age. Physical Therapy. 1991; 71(9):656-5. [DOI:10.1093/ptj/71.9.656] [PMID]
- Cassart M, Pettiaux N, Gevenois PA, Paiva M, Estenne M. Effect of chronic hyperinflation on diaphragm length and surface area. American Journal of Respiratory and Critical Care Medicine. 1997; 156(2 Pt 1):504-8. [DOI:10.1164/ajrccm.156.2.9612089] [PMID]
- Clanton TL, Diaz PT. Clinical assessment of the respiratory muscles. Physical Therapy. 1995; 75(11):983-95. [DOI:10.1093/ptj/75.11.983] [PMID]
- Hutt D, Parisi R, Edelman NH, Santiago TV. Responses of diaphragm and external oblique muscles to flow-resistive loads during sleep. American Review of Respiratory Disease. 1991; 144(5):1107-11. [DOI:10.1164/ajrccm/144.5.1107] [PMID]
- Boyle KL, Demske JR. Management of a female with chronic sciatica and low back pain: A case report. Physiotherapy Theory and Practice. 2009; 25(1):44-54. [DOI:10.1080/09593980802622677] [PMID]
- Robey JH, Boyle KL. Bilateral Functional Thoracic Outlet Syndrome in a Collegiate Football Player. North American Journal of Sports Physical Therapy. 2009; 4(4):170-81. [PMID] [PMCID]
- Spence H. Case study report: Postural restoration: An effective physical therapy approach to patient treatment. Techniques in Regional Anesthesia and Pain Management. 2008; 12(2):102-04. [DOI:10.1053/j.trap.2008.01.003]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2020/10/23 | Accepted: 2022/04/16 | Published: 2022/06/1
Received: 2020/10/23 | Accepted: 2022/04/16 | Published: 2022/06/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
