
988368
Sat, Apr 20, 2024

Volume 18, Issue 4 (December 2020)
Iranian Rehabilitation Journal 2020, 18(4): 485-496 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shaikhul Hasan M, Anusaksathien K, Siripornpibul T, Narattharaksa K. Assessing Post-stroke Outpatients’ Rehabilitation Service Quality Gaps in Bangladesh. Iranian Rehabilitation Journal 2020; 18 (4) :485-496
URL: http://irj.uswr.ac.ir/article-1-1159-en.html
URL: http://irj.uswr.ac.ir/article-1-1159-en.html
Mohammad Shaikhul Hasan * 

 1, Kantabhat Anusaksathien1 , Taweesak Siripornpibul1 , Kanida Narattharaksa1
1, Kantabhat Anusaksathien1 , Taweesak Siripornpibul1 , Kanida Narattharaksa1
1, Kantabhat Anusaksathien1 , Taweesak Siripornpibul1 , Kanida Narattharaksa1
1- Health Systems Management, Faculty of Social Science, Naresuan University, Phitsanulok, Thailand.
Keywords: Patient expectation, Patient perception, Post-stroke, Rehabilitation service quality, Service Quality model
Full-Text [PDF 626 kb]
(1150 Downloads)
| Abstract (HTML) (2154 Views)
Full-Text: (690 Views)
1. Introduction
atients’ have a right to receive quality healthcare services. Furthermore, healthcare providers should ensure committed services to obtain better patient perceptions through sound healthcare service delivery [1]. The developing countries’ residents have become aware of different disease conditions where patient expectations must be considered before providing them with healthcare services. As a developing country, the healthcare service systems of Bangladesh have been facing challenges to prevent life-threatening diseases [2]. Among those conditions, such Non-Communicable Diseases (NCDs) as stroke shape the second leading NCD on the causes of death and long-term disability in Bangladesh.
A stroke is a medical emergency, characterized by a neurological deficit. Stroke is a major cause of disability and death worldwide [3]. Globally, 4.46 million individuals have died due to stroke per year; 1.2 million in developed countries and approximately 3.2 million in developing ones. For instance, stroke was the fourth leading cause of death in US citizens [4]. In 2012, Australia projected that 377000 individuals experienced a stroke some-time in their lives [5, 6]. Approximately 3.7 million South-East Asian individuals died from stroke. Besides, in Bangladesh, the prevalence rate of stroke equals 0.3%, and approximately 485 per 10000 disability-adjusted life-years are lost due to stroke [7]. In terms of disability, the majority (80%) of stroke survivors live with either minor or major physical, emotional, and cognitive disabilities [4]. The National Stroke Association [8] claimed that they could get back to their functional life through comprehensive rehabilitation services. Rehabilitation services is defined as the approach aimed at enabling individuals with disabilities by ensuring the provision of all required healthcare services during treatment [7].
However, the rehabilitation Service Quality (SQ) measurement and the relevant assessment tools are limited and developing worldwide [9]. Eventually, in Bangladesh, few studies have examined healthcare quality measurement; however, no study explored rehabilitation SQ. Post-stroke disability and rehabilitation are major concerns worldwide. Therefore, it is important to ensure the provision of quality services to develop stronger integrated health systems [7, 8, 9]. Particularly, not-for-profit Non-Government Organizations (NGOs) provide rehabilitation services throughout Bangladesh [10]. Several studies have examined the healthcare sector of Bangladesh; they found that the patients are dissatisfied with the quality of healthcare services provided to them [10, 11]. Accordingly, patients lost faith and participation in rehabilitation care, i.e. a significant challenge for the citizens of Bangladesh. Consequently, such shortcomings increase the burden of stroke disability [2]. Thus, it is essential to assess gaps in rehabilitation SQ to implement continuous quality improvement monitoring systems in Bangladesh.
In measuring the quality gap of services, this is respectful and responsive to individual patient preferences to manage and enhance the quality of healthcare services [12]. Parasuraman et al. [13] studied patient’s preferences (expectations and perceptions) and claimed that a positive patient experience intends better health outcomes with sufficient patient engagement in the healthcare services. Therefore, they preferred to assess the quality of healthcare services through patients’ preferences and proposed a mostly accepted and valid Five-Dimensional (5D) model. This is also called the gap theory or Service Quality (SERVQUAL) model for measuring various SQ types. Andaleeb et al. [14] conducted a study in Bangladesh and introduced the cost and availability of medical professionals as the important indicators for poor patients’ perceptions concerning healthcare services. Lee [15] studied the 5D model of HEALTHQUAL, i.e. using specifically for healthcare SQ and it’s quite similar to the SERVQUAL. Saha, Harries, and Gilhooly [16] investigated post-stroke patients’ conditions. They reported that the patient’s illness was the main factor for the poor perception of the rehabilitation services. Al Fraihi and Latif [12] as well as Güllü, Tekindal, Tekindal [17] studied outpatient services and presented a significant association between gaps in SQ and patient’s age, gender, educational level, socioeconomic status, distance from home to the hospital, and the intensity of the hospital visit factors. Particularly, numerous tools are available for measuring healthcare SQ; however, a limited number of tools are valid to measure rehabilitation SQ.
Swaine et al. [18] measured the quality of rehabilitation services using a 5D Perceptions of the Quality of Rehabilitation Services-Montreal (PQRS-Montreal) model. They claimed that this tool is valid to measure the patient’s perceptions of rehabilitation services. Kingsley and Patel [19] explored Patient-reported Outcome Measures (PROMs) and Patient-Reported Experience Measures (PREMs). PROMs are relatively used for measuring the health status. PREMs are also employed for measuring the patients’ experiences of SQ. Perhaps, both tools provide valid data regarding patients’ perceptions; these tools are quite new and might be challenging for implementation [20]. However, the SERVQUAL has provided data regarding patients’ expectations and perceptions as well as the gaps in the quality of rehabilitation services. Moreover, this scale is the most valid and reliable tool to evaluate the quality gaps in rehabilitation services [17, 20, 21]. Therefore, this study applied SERVQUAL to address the following points: we aimed to measure post-stroke outpatient rehabilitation SQ gaps in Bangladesh through SERVQUAL; we aimed to determine the patient-related factors concerning these gaps.
2. methods
This was a cross-sectional study [17]. The not-for-profit Centre for the Rehabilitation of the Paralyzed (CRP) hospital (including its 5 divisional centers; Dhaka, Sylhet, Barishal, Rajshahi, and Chittagong) was selected to recruit the study participants [9]. Post-stroke patients were the target population of this study.
A stratified sampling technique was applied to select the study samples covering the 5 divisional centers for post-stroke patients from the outpatient stroke rehabilitation services. Besides, the inclusion criteria of the study included receiving ≥1 outpatient rehabilitation services (i.e. physical, occupational, speech, and speech therapy); the age of ≥20 years; being post-stroke patients; not visiting other CRP branches for rehabilitation services, and having communication abilities. Considering the statistical formula of Charan and Biswas [22], we selected 311 recipients of post-stroke rehabilitation services, as the study sample.

The statistical formula for sample calculation is presented as follows:
According to the formula, n= sample size, Z=1.96, the percentile of the standard normal distribution, p= the highest proportion of the total population, q= 1-p, and d= margin of error means the expected level of precision. The sampling process lasted 3 months, from June to August 2018.
A modified SERVQUAL questionnaire was applied as the research instrument. This study added extra two dimensions along with the 5D SERVQUAL model. These two dimensions were therapy service cost and the availability of the professionals. Cronbach’s alpha coefficient () was applied to check the reliability of the proposed questionnaire. Besides, the Pearson correlation coefficient (Pearson’s r) was employed to examine the correlation between patients’ perceptions and expectations scores per dimension. In total, 27 paired questions and a five-point Likert-type scale were implemented to determine the best answers [23]. Points one and 5 were referred to strongly disagree and strongly agree, respectively. The rehabilitation SQ was measured by assessing the gap between patients’ Perceptions (P) and Expectations (E) by Paired Samples t-test.
Gap= P – E
Wherein, Gap= 0 if patient perception value met with the expectation. Gap= positive if the patient’s perceived value was higher than the expectation. Gap= negative if the patient’s perceived value was lower than the expectation of rehabilitation SQ.
The descriptive statistics were applied for measuring the mean, frequency, and standard deviation values. Eta-statistic (δ) of Analysis of Variance (ANOVA) was applied to examine the relationship between patient-related factors and gaps in rehabilitation SQ.
3. Results
The Cronbach’s coefficient calculated that all the constructs of the questionnaire indicated >0.70 threshold values for patients’ expectations and the perceptions questions. Pearson’s r revealed significant correlation coefficient values at 0.01 level between the expectations and perceptions scores of each sub-scale of the proposed questionnaire (Table 1).
.jpg)
Table 2 indicated that the majority (35.7%) of the respondents were in the age range of 46-60 years and more than half (66.6%) of the respondents of this study were men.


Secondary education was the highest educational level in half (50.5%) of the study respondents. Interestingly, 36% of the respondents indicated others as their occupation, whether, 81.25% of respondents in other occupations signified housewife as their occupation. Furthermore, due to the low educational level, the majority of the respondents maintained a low family status (27%); the majority of the respondents in others occupation indicated housewife as their occupation; that might be why they preferred to perform culinary activities (33.8%) before experiencing a stroke.
Table 3 demonstrated that the Mean±SD values of patients’ expectations (3.99±0.178) were higher than those of the perceptions (3.53±0.291) of rehabilitation SQ.
.jpg)
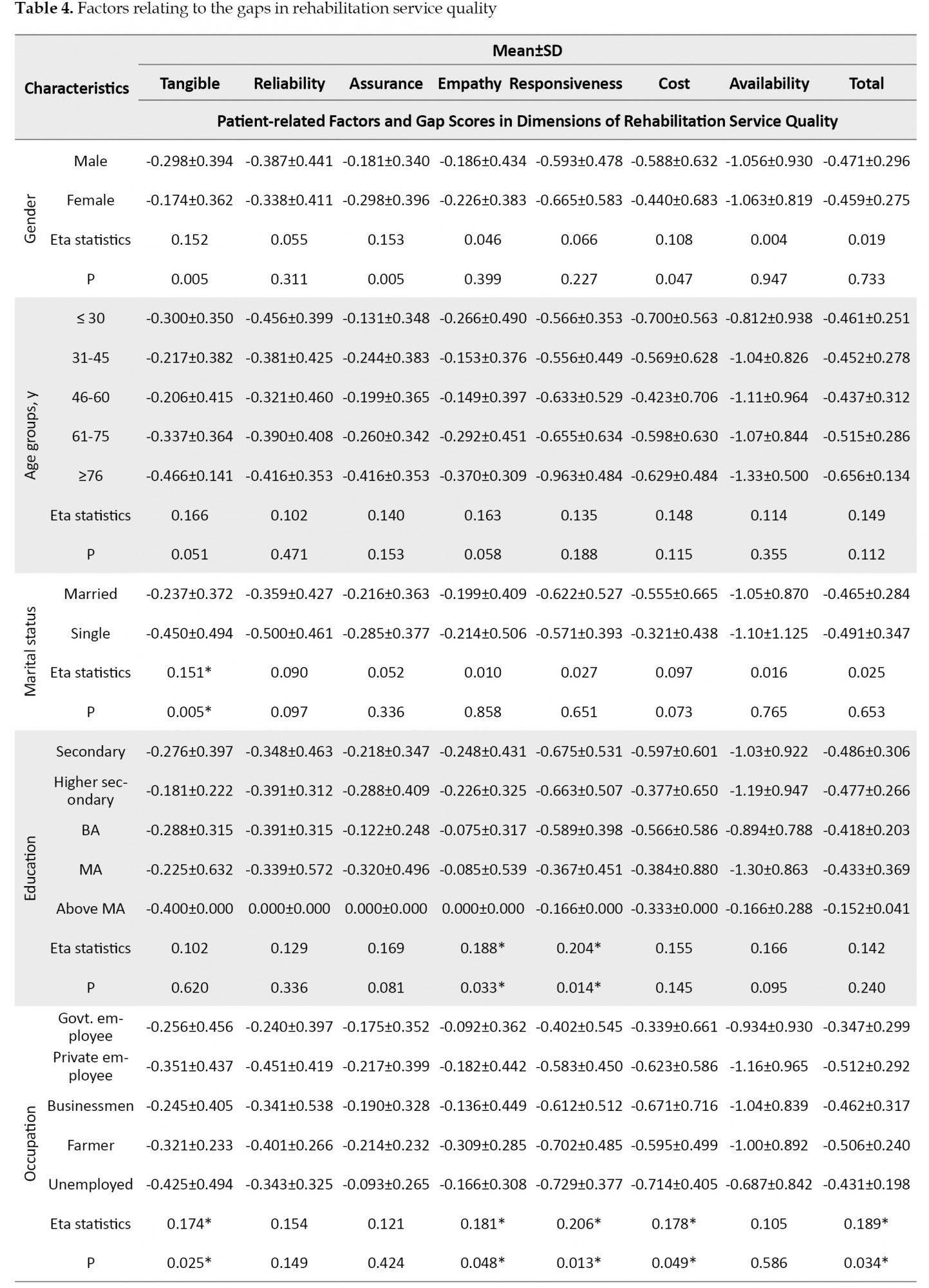
Thus, this study indicated a significant negative gap (t=-29.604, P<0.001) between patients’ perceptions and expectations of rehabilitation SQ. Even all dimensions of rehabilitation SQ indicated a higher mean value of patients’ expectations, compared to the perceptions. From the individual statements of the 7 dimensions, the statement of ‘explanation about patient’s problem’ counted the highest Mean±SD score (4.10±0.340) of patients’ expectations; this might be because of the dependency of therapy services, where this study indicated the lowest Mean±SD score (3.48±0.529) of patients’ expectations in the statement of ‘medicine fee’. The patients’ perceived the highest Mean±SD score (4.07±0.411) in the statement of ‘safe or confident feeling’ and may be due to shortage of available rehabilitation professionals in Bangladesh; the statement of ‘the availability of therapist appointment’ considered the lowest Mean±SD score (2.88±0.989) of patients’ perceptions in the rehabilitation SQ. The current study considered 10 patient-related factors; of these, the occupation factor presented a significant relationship (0.189, P=0.034) with the gaps in rehabilitation services. The same was followed by the family status (0.289, P=0.026), pre-stroke daily activity (0.235, P=0.013), and post-stroke disability (0.286, P=0.001) that demonstrated significant relationships with the gaps in rehabilitation SQ (Table 4).

4. Discussion
This study addressed the rehabilitation SQ gaps in 7 attributes. We also defined the relationship between factors and gaps in post-stroke outpatients’ rehabilitation SQ after recording the opinions of post-stroke outpatients on what they experienced during visits to the stroke rehabilitation services in the CRP Hospital, Bangladesh. The proposed questionnaire of this study suggested significantly valid and reliable coefficient scores in two separate scales; patient expectations and the perceptions of rehabilitation SQ [12, 15, 17, 20, 21]. The present study extended the SERVQUAL model by adding 2 extra dimensions. Besides, these dimensions demonstrated significant validity and reliability coefficient scores in line with the study of Andaleeb and associates [11].
The present study findings suggested that the explored post-stroke patients were affected physically, functionally, communicably, and cognitively. For cognitive impairment or due to their poor understanding, several studies applied PROMs and PREMs to assess the health status and quality of healthcare services [19]. The number of cognitive impairment respondents was limited; thus, the current study allowed the regular caregiver of the patients to answer the questionnaire instead of the patients. The majority of the respondents’ age ranged between 46-60 years. At this age range, individuals spend their maximum time on their jobs for earning money. Mamin et al. [24] reported that nearly 77% of stroke survivors were public- or private- or self-employed individuals in Bangladesh. Thus, it greatly impacts the economy of this country. Torabipour et al. [20] conducted a study in a physical therapy and rehabilitation center in Iran; they revealed that 21-30-year-olds visited the rehabilitation services for maximum times, i.e. opposing the present study participants group. Contrary to the study of Torabipour et al. [20], the present study revealed that men, in comparison with women are mostly affected by stroke; they also participated in post-stroke rehabilitation services to retain back to their independent and healthy life.
Patient expectations or desired healthcare facilities are continuous processes and patients always expect an ever-increasing improvement in healthcare services [12]. Generally, patients visit hospitals with high hopes of meeting desired services and health outcomes. They expected high-quality rehabilitation care and being consistently consulted with the rehabilitation professionals to fulfill their expectations. The patient always prefers a better outlook of the rehabilitation hospital and its responsible professionals to assure competent management of the rehabilitation service quality. This is because a highly-decorated physical environment with quality therapeutic equipment assists to enhance patients’ participation due to their appropriate mood [25]. They also prefer a responsive professional in the rehabilitation service systems to provide practical therapy services at reasonable service charges. In other words, the SQ depends on the performance of rehabilitation professionals. The better the performance of the rehabilitation professionals, the more it contributes to higher patient perceptions in rehabilitation SQ. Most importantly, patients were expected to receive regular appointments with the therapist; however, due to the shortage of therapists and receptionists, the receptionists often failed to assist the patients when encountering difficulties; often mentioning that they were busy.
Marzban et al. [26] conducted a study on stroke rehabilitation. They reported that its prudent urges to increase the number of therapeutic and administrative professionals for offering quality services with patient satisfaction. Continuous quality improvement monitoring systems are also essential to the regular monitoring of the overall service delivery systems and patients’ preference on the services [11]. Relatively, the appointment system of the hospital was more complex for the patients; therefore, the patients had to wait for a long queue to get an appointment with the therapist. The present study data indicated that the explored patients’ expectations level was higher than the value of patients’ perceptions; such findings revealed a significant negative gap between patients’ perceptions and expectations of rehabilitation SQ. A similar negative SQ gap was delivered in the studies of Al Fraihi and Latif [12], Torabipour et al. [20], Ludviga and Tambora [21], and Marzban et al. [26].
Moreover, the patient’s occupation exposed a significant relationship with the gaps in rehabilitation SQ. Government employees reported better therapy services experience, compared to other patient groups. The government employee experienced better physical environments with reliable rehabilitation professionals and therapy services. The government employee also perceived higher levels of respect and responsive services from rehabilitation professionals with realistic therapy services charge; accordingly, their preference was also the low-cost therapy services of the center. This result was inconsistent with the study of Girmay et al. [25], who found no significant relationship between occupation and patient’s experience.
The family status of the patients presented a significant relationship with the gaps in rehabilitation SQ. Individuals from upper-middle-class families were perceived to have the highest level of empathy from the rehabilitation professionals, compared with other social classes. The upper-middle-class patients also experienced a practical therapy service charge. This is because they have adequate financial sources, compared with other family classes. They did not care about the charges; they required quality services for returning to their independent and functional life. The findings were consistent with those of the study by Güllü, Tekindal, and Tekindal [17]. Accordingly, the upper-class family expected better hospital responsiveness concerning responsive rehabilitation professionals and their services. This finding was not in line with the study of Torabipour et al. [20].
The present study considered some pre-stroke daily activities, including attending sports, physical exercise, traveling, and culinary activities. These pre-stroke functions assisted the investigated patients to recover early from stroke-induced disabilities with better perceptions of hospital services [27]. Thus, the pre-stroke daily activities affected the SQ gaps. Besides, this study found a significant relationship between daily activities before the stroke and the gaps of rehabilitation SQ. Particularly, the patient’s expectation was influenced by the severity of illness and expertise of pre-stroke functions [16]. The present study indicated that the majority of the respondents preferred to perform culinary activities before experiencing stroke; therefore, they had not much idea about the healthcare services. As a result, after encountering disabilities, they expected high-quality rehabilitation services to become healthy soon. Wherein their perceived experience did not meet with their expectations and suggested significant gaps in rehabilitation SQ.
The patients with physical disabilities considered better perceptions in the tangibility, reliability, empathy, responsiveness, and therapy charges of the rehabilitation SQ. Similarly, the patients with cognitive disabilities reported a better perception of the tangibility and responsiveness of rehabilitation SQ. That is why post-stroke disability was significantly associated with the gaps of rehabilitation SQ. Saha et al. [16] reported that post-stroke disability negatively affected patients’ perceptions. Besides, after a stroke, the patients with physical disabilities expected a desirable physical environment with reliable professionals and their services. They expected to feel safe and to be treated with respect and provide rehabilitation services at a reasonable service charge. The present study only examined the specific conditions based on outpatients’ rehabilitation SQ gaps; thus, it limits the information regarding in-patient and other condition-based rehabilitation SQ. Therefore, conducting a future study on providers’ perspectives on rehabilitation SQ is recommended to evaluate the exact scenario of rehabilitation SQ gaps.
5. Conclusion
The quality of rehabilitation care was not up to the mark of the study patients’ expectations. Particularly, the number of rehabilitation professionals is inadequate to fulfill the vast needs of therapeutic services for post-stroke patients. As a result, therapists were concentrated on the number of therapeutic sessions rather than ensuring quality services. The rehabilitation center was also concentrated on providing therapeutic sessions to cover a huge number of patients requiring therapeutic services. This issue is very common in Bangladesh and could gradually increase the burden of stroke disability. The better quality of healthcare service intends better health outcomes; thus, the rehabilitation center must improve its quality in considering all aspects of rehabilitation services. The rehabilitation center must also develop a continuous quality improvement monitoring system to address these gaps by prioritizing ranks and the associated factors.
Ethical Considerations
Compliance with ethical guidelines
This study received approval from Naresuan University Institutional Review Board (NU-IRB) (IRB No. 0139/61) and the Centre for the Rehabilitation of the Paralysed (CRP) Ethical clearance (No. CRP-R&E-0401-225). All participants of this study were guaranteed on the privacy of their information.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
References
atients’ have a right to receive quality healthcare services. Furthermore, healthcare providers should ensure committed services to obtain better patient perceptions through sound healthcare service delivery [1]. The developing countries’ residents have become aware of different disease conditions where patient expectations must be considered before providing them with healthcare services. As a developing country, the healthcare service systems of Bangladesh have been facing challenges to prevent life-threatening diseases [2]. Among those conditions, such Non-Communicable Diseases (NCDs) as stroke shape the second leading NCD on the causes of death and long-term disability in Bangladesh.
A stroke is a medical emergency, characterized by a neurological deficit. Stroke is a major cause of disability and death worldwide [3]. Globally, 4.46 million individuals have died due to stroke per year; 1.2 million in developed countries and approximately 3.2 million in developing ones. For instance, stroke was the fourth leading cause of death in US citizens [4]. In 2012, Australia projected that 377000 individuals experienced a stroke some-time in their lives [5, 6]. Approximately 3.7 million South-East Asian individuals died from stroke. Besides, in Bangladesh, the prevalence rate of stroke equals 0.3%, and approximately 485 per 10000 disability-adjusted life-years are lost due to stroke [7]. In terms of disability, the majority (80%) of stroke survivors live with either minor or major physical, emotional, and cognitive disabilities [4]. The National Stroke Association [8] claimed that they could get back to their functional life through comprehensive rehabilitation services. Rehabilitation services is defined as the approach aimed at enabling individuals with disabilities by ensuring the provision of all required healthcare services during treatment [7].
However, the rehabilitation Service Quality (SQ) measurement and the relevant assessment tools are limited and developing worldwide [9]. Eventually, in Bangladesh, few studies have examined healthcare quality measurement; however, no study explored rehabilitation SQ. Post-stroke disability and rehabilitation are major concerns worldwide. Therefore, it is important to ensure the provision of quality services to develop stronger integrated health systems [7, 8, 9]. Particularly, not-for-profit Non-Government Organizations (NGOs) provide rehabilitation services throughout Bangladesh [10]. Several studies have examined the healthcare sector of Bangladesh; they found that the patients are dissatisfied with the quality of healthcare services provided to them [10, 11]. Accordingly, patients lost faith and participation in rehabilitation care, i.e. a significant challenge for the citizens of Bangladesh. Consequently, such shortcomings increase the burden of stroke disability [2]. Thus, it is essential to assess gaps in rehabilitation SQ to implement continuous quality improvement monitoring systems in Bangladesh.
In measuring the quality gap of services, this is respectful and responsive to individual patient preferences to manage and enhance the quality of healthcare services [12]. Parasuraman et al. [13] studied patient’s preferences (expectations and perceptions) and claimed that a positive patient experience intends better health outcomes with sufficient patient engagement in the healthcare services. Therefore, they preferred to assess the quality of healthcare services through patients’ preferences and proposed a mostly accepted and valid Five-Dimensional (5D) model. This is also called the gap theory or Service Quality (SERVQUAL) model for measuring various SQ types. Andaleeb et al. [14] conducted a study in Bangladesh and introduced the cost and availability of medical professionals as the important indicators for poor patients’ perceptions concerning healthcare services. Lee [15] studied the 5D model of HEALTHQUAL, i.e. using specifically for healthcare SQ and it’s quite similar to the SERVQUAL. Saha, Harries, and Gilhooly [16] investigated post-stroke patients’ conditions. They reported that the patient’s illness was the main factor for the poor perception of the rehabilitation services. Al Fraihi and Latif [12] as well as Güllü, Tekindal, Tekindal [17] studied outpatient services and presented a significant association between gaps in SQ and patient’s age, gender, educational level, socioeconomic status, distance from home to the hospital, and the intensity of the hospital visit factors. Particularly, numerous tools are available for measuring healthcare SQ; however, a limited number of tools are valid to measure rehabilitation SQ.
Swaine et al. [18] measured the quality of rehabilitation services using a 5D Perceptions of the Quality of Rehabilitation Services-Montreal (PQRS-Montreal) model. They claimed that this tool is valid to measure the patient’s perceptions of rehabilitation services. Kingsley and Patel [19] explored Patient-reported Outcome Measures (PROMs) and Patient-Reported Experience Measures (PREMs). PROMs are relatively used for measuring the health status. PREMs are also employed for measuring the patients’ experiences of SQ. Perhaps, both tools provide valid data regarding patients’ perceptions; these tools are quite new and might be challenging for implementation [20]. However, the SERVQUAL has provided data regarding patients’ expectations and perceptions as well as the gaps in the quality of rehabilitation services. Moreover, this scale is the most valid and reliable tool to evaluate the quality gaps in rehabilitation services [17, 20, 21]. Therefore, this study applied SERVQUAL to address the following points: we aimed to measure post-stroke outpatient rehabilitation SQ gaps in Bangladesh through SERVQUAL; we aimed to determine the patient-related factors concerning these gaps.
2. methods
This was a cross-sectional study [17]. The not-for-profit Centre for the Rehabilitation of the Paralyzed (CRP) hospital (including its 5 divisional centers; Dhaka, Sylhet, Barishal, Rajshahi, and Chittagong) was selected to recruit the study participants [9]. Post-stroke patients were the target population of this study.
A stratified sampling technique was applied to select the study samples covering the 5 divisional centers for post-stroke patients from the outpatient stroke rehabilitation services. Besides, the inclusion criteria of the study included receiving ≥1 outpatient rehabilitation services (i.e. physical, occupational, speech, and speech therapy); the age of ≥20 years; being post-stroke patients; not visiting other CRP branches for rehabilitation services, and having communication abilities. Considering the statistical formula of Charan and Biswas [22], we selected 311 recipients of post-stroke rehabilitation services, as the study sample.
The statistical formula for sample calculation is presented as follows:
According to the formula, n= sample size, Z=1.96, the percentile of the standard normal distribution, p= the highest proportion of the total population, q= 1-p, and d= margin of error means the expected level of precision. The sampling process lasted 3 months, from June to August 2018.
A modified SERVQUAL questionnaire was applied as the research instrument. This study added extra two dimensions along with the 5D SERVQUAL model. These two dimensions were therapy service cost and the availability of the professionals. Cronbach’s alpha coefficient () was applied to check the reliability of the proposed questionnaire. Besides, the Pearson correlation coefficient (Pearson’s r) was employed to examine the correlation between patients’ perceptions and expectations scores per dimension. In total, 27 paired questions and a five-point Likert-type scale were implemented to determine the best answers [23]. Points one and 5 were referred to strongly disagree and strongly agree, respectively. The rehabilitation SQ was measured by assessing the gap between patients’ Perceptions (P) and Expectations (E) by Paired Samples t-test.
Gap= P – E
Wherein, Gap= 0 if patient perception value met with the expectation. Gap= positive if the patient’s perceived value was higher than the expectation. Gap= negative if the patient’s perceived value was lower than the expectation of rehabilitation SQ.
The descriptive statistics were applied for measuring the mean, frequency, and standard deviation values. Eta-statistic (δ) of Analysis of Variance (ANOVA) was applied to examine the relationship between patient-related factors and gaps in rehabilitation SQ.
3. Results
The Cronbach’s coefficient calculated that all the constructs of the questionnaire indicated >0.70 threshold values for patients’ expectations and the perceptions questions. Pearson’s r revealed significant correlation coefficient values at 0.01 level between the expectations and perceptions scores of each sub-scale of the proposed questionnaire (Table 1).
Table 2 indicated that the majority (35.7%) of the respondents were in the age range of 46-60 years and more than half (66.6%) of the respondents of this study were men.
Secondary education was the highest educational level in half (50.5%) of the study respondents. Interestingly, 36% of the respondents indicated others as their occupation, whether, 81.25% of respondents in other occupations signified housewife as their occupation. Furthermore, due to the low educational level, the majority of the respondents maintained a low family status (27%); the majority of the respondents in others occupation indicated housewife as their occupation; that might be why they preferred to perform culinary activities (33.8%) before experiencing a stroke.
Table 3 demonstrated that the Mean±SD values of patients’ expectations (3.99±0.178) were higher than those of the perceptions (3.53±0.291) of rehabilitation SQ.
Thus, this study indicated a significant negative gap (t=-29.604, P<0.001) between patients’ perceptions and expectations of rehabilitation SQ. Even all dimensions of rehabilitation SQ indicated a higher mean value of patients’ expectations, compared to the perceptions. From the individual statements of the 7 dimensions, the statement of ‘explanation about patient’s problem’ counted the highest Mean±SD score (4.10±0.340) of patients’ expectations; this might be because of the dependency of therapy services, where this study indicated the lowest Mean±SD score (3.48±0.529) of patients’ expectations in the statement of ‘medicine fee’. The patients’ perceived the highest Mean±SD score (4.07±0.411) in the statement of ‘safe or confident feeling’ and may be due to shortage of available rehabilitation professionals in Bangladesh; the statement of ‘the availability of therapist appointment’ considered the lowest Mean±SD score (2.88±0.989) of patients’ perceptions in the rehabilitation SQ. The current study considered 10 patient-related factors; of these, the occupation factor presented a significant relationship (0.189, P=0.034) with the gaps in rehabilitation services. The same was followed by the family status (0.289, P=0.026), pre-stroke daily activity (0.235, P=0.013), and post-stroke disability (0.286, P=0.001) that demonstrated significant relationships with the gaps in rehabilitation SQ (Table 4).
4. Discussion
This study addressed the rehabilitation SQ gaps in 7 attributes. We also defined the relationship between factors and gaps in post-stroke outpatients’ rehabilitation SQ after recording the opinions of post-stroke outpatients on what they experienced during visits to the stroke rehabilitation services in the CRP Hospital, Bangladesh. The proposed questionnaire of this study suggested significantly valid and reliable coefficient scores in two separate scales; patient expectations and the perceptions of rehabilitation SQ [12, 15, 17, 20, 21]. The present study extended the SERVQUAL model by adding 2 extra dimensions. Besides, these dimensions demonstrated significant validity and reliability coefficient scores in line with the study of Andaleeb and associates [11].
The present study findings suggested that the explored post-stroke patients were affected physically, functionally, communicably, and cognitively. For cognitive impairment or due to their poor understanding, several studies applied PROMs and PREMs to assess the health status and quality of healthcare services [19]. The number of cognitive impairment respondents was limited; thus, the current study allowed the regular caregiver of the patients to answer the questionnaire instead of the patients. The majority of the respondents’ age ranged between 46-60 years. At this age range, individuals spend their maximum time on their jobs for earning money. Mamin et al. [24] reported that nearly 77% of stroke survivors were public- or private- or self-employed individuals in Bangladesh. Thus, it greatly impacts the economy of this country. Torabipour et al. [20] conducted a study in a physical therapy and rehabilitation center in Iran; they revealed that 21-30-year-olds visited the rehabilitation services for maximum times, i.e. opposing the present study participants group. Contrary to the study of Torabipour et al. [20], the present study revealed that men, in comparison with women are mostly affected by stroke; they also participated in post-stroke rehabilitation services to retain back to their independent and healthy life.
Patient expectations or desired healthcare facilities are continuous processes and patients always expect an ever-increasing improvement in healthcare services [12]. Generally, patients visit hospitals with high hopes of meeting desired services and health outcomes. They expected high-quality rehabilitation care and being consistently consulted with the rehabilitation professionals to fulfill their expectations. The patient always prefers a better outlook of the rehabilitation hospital and its responsible professionals to assure competent management of the rehabilitation service quality. This is because a highly-decorated physical environment with quality therapeutic equipment assists to enhance patients’ participation due to their appropriate mood [25]. They also prefer a responsive professional in the rehabilitation service systems to provide practical therapy services at reasonable service charges. In other words, the SQ depends on the performance of rehabilitation professionals. The better the performance of the rehabilitation professionals, the more it contributes to higher patient perceptions in rehabilitation SQ. Most importantly, patients were expected to receive regular appointments with the therapist; however, due to the shortage of therapists and receptionists, the receptionists often failed to assist the patients when encountering difficulties; often mentioning that they were busy.
Marzban et al. [26] conducted a study on stroke rehabilitation. They reported that its prudent urges to increase the number of therapeutic and administrative professionals for offering quality services with patient satisfaction. Continuous quality improvement monitoring systems are also essential to the regular monitoring of the overall service delivery systems and patients’ preference on the services [11]. Relatively, the appointment system of the hospital was more complex for the patients; therefore, the patients had to wait for a long queue to get an appointment with the therapist. The present study data indicated that the explored patients’ expectations level was higher than the value of patients’ perceptions; such findings revealed a significant negative gap between patients’ perceptions and expectations of rehabilitation SQ. A similar negative SQ gap was delivered in the studies of Al Fraihi and Latif [12], Torabipour et al. [20], Ludviga and Tambora [21], and Marzban et al. [26].
Moreover, the patient’s occupation exposed a significant relationship with the gaps in rehabilitation SQ. Government employees reported better therapy services experience, compared to other patient groups. The government employee experienced better physical environments with reliable rehabilitation professionals and therapy services. The government employee also perceived higher levels of respect and responsive services from rehabilitation professionals with realistic therapy services charge; accordingly, their preference was also the low-cost therapy services of the center. This result was inconsistent with the study of Girmay et al. [25], who found no significant relationship between occupation and patient’s experience.
The family status of the patients presented a significant relationship with the gaps in rehabilitation SQ. Individuals from upper-middle-class families were perceived to have the highest level of empathy from the rehabilitation professionals, compared with other social classes. The upper-middle-class patients also experienced a practical therapy service charge. This is because they have adequate financial sources, compared with other family classes. They did not care about the charges; they required quality services for returning to their independent and functional life. The findings were consistent with those of the study by Güllü, Tekindal, and Tekindal [17]. Accordingly, the upper-class family expected better hospital responsiveness concerning responsive rehabilitation professionals and their services. This finding was not in line with the study of Torabipour et al. [20].
The present study considered some pre-stroke daily activities, including attending sports, physical exercise, traveling, and culinary activities. These pre-stroke functions assisted the investigated patients to recover early from stroke-induced disabilities with better perceptions of hospital services [27]. Thus, the pre-stroke daily activities affected the SQ gaps. Besides, this study found a significant relationship between daily activities before the stroke and the gaps of rehabilitation SQ. Particularly, the patient’s expectation was influenced by the severity of illness and expertise of pre-stroke functions [16]. The present study indicated that the majority of the respondents preferred to perform culinary activities before experiencing stroke; therefore, they had not much idea about the healthcare services. As a result, after encountering disabilities, they expected high-quality rehabilitation services to become healthy soon. Wherein their perceived experience did not meet with their expectations and suggested significant gaps in rehabilitation SQ.
The patients with physical disabilities considered better perceptions in the tangibility, reliability, empathy, responsiveness, and therapy charges of the rehabilitation SQ. Similarly, the patients with cognitive disabilities reported a better perception of the tangibility and responsiveness of rehabilitation SQ. That is why post-stroke disability was significantly associated with the gaps of rehabilitation SQ. Saha et al. [16] reported that post-stroke disability negatively affected patients’ perceptions. Besides, after a stroke, the patients with physical disabilities expected a desirable physical environment with reliable professionals and their services. They expected to feel safe and to be treated with respect and provide rehabilitation services at a reasonable service charge. The present study only examined the specific conditions based on outpatients’ rehabilitation SQ gaps; thus, it limits the information regarding in-patient and other condition-based rehabilitation SQ. Therefore, conducting a future study on providers’ perspectives on rehabilitation SQ is recommended to evaluate the exact scenario of rehabilitation SQ gaps.
5. Conclusion
The quality of rehabilitation care was not up to the mark of the study patients’ expectations. Particularly, the number of rehabilitation professionals is inadequate to fulfill the vast needs of therapeutic services for post-stroke patients. As a result, therapists were concentrated on the number of therapeutic sessions rather than ensuring quality services. The rehabilitation center was also concentrated on providing therapeutic sessions to cover a huge number of patients requiring therapeutic services. This issue is very common in Bangladesh and could gradually increase the burden of stroke disability. The better quality of healthcare service intends better health outcomes; thus, the rehabilitation center must improve its quality in considering all aspects of rehabilitation services. The rehabilitation center must also develop a continuous quality improvement monitoring system to address these gaps by prioritizing ranks and the associated factors.
Ethical Considerations
Compliance with ethical guidelines
This study received approval from Naresuan University Institutional Review Board (NU-IRB) (IRB No. 0139/61) and the Centre for the Rehabilitation of the Paralysed (CRP) Ethical clearance (No. CRP-R&E-0401-225). All participants of this study were guaranteed on the privacy of their information.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
References
- Webster TR, Mantopoulos J, Jackson E, Cole-Lewis H, Kidane L, Kebede S, et al. A brief questionnaire for assessing patient healthcare experiences in low-income settings. International Journal for Quality in Health Care. 2011; 23(3):258-68. [DOI:10.1093/intqhc/mzr019] [PMID]
- Muhammad F, Chowdhury M, Arifuzzaman M, Chowdhury AA. Public health problems in Bangladesh: Issues and challenges. South East Asia Journal of Public Health. 2017; 6(2):11-6. [DOI:10.3329/seajph.v6i2.31830]
- Mohammad QD. Management of stroke-Bangladesh perspective. Bangladesh Medical Journal. 2014; 42(1):34-7. [DOI:10.3329/bmj.v42i1.18979]
- Kobylańska M, Wójcik BM, Szczepaniak R, Śliwiński Z. The rehabilitation of patients after the cerebral stroke including socio-demographic factors. Fizjoterapia Polska. 2016; 16(4):82-97. http://fizjoterapiapolska.pl/en/article/rehabilitacja-pacjentow-po-udarze-mozgu-z-uwzglednieniem-czynnikow-socjo-demograficznych-the-rehabilitation-of-patients-after-the-cerebral-stroke-including-socio-demographic-factors/
- Heart, stroke, and vascular diseases. [Internet]. Australian Government. 2016 [cited 5th April, 2017]. https://www.aihw.gov.au/reports-data/health-conditions-disability-deaths/heart-stroke-vascular-diseases/overview.
- World Health Organization. Noncommunicable diseases country profiles. [Internet]. 2014 [cited 10th March, 2017]. https://www.who.int/nmh/publications/ncd-profiles-2014/en/.
- Islam MN, Moniruzzaman M, Khalil MI, Basri R, Alam MK, Loo KW, et al. Burden of stroke in Bangladesh. International journal of stroke: official journal of the International Stroke Society. 2013; 8(3):211-3. [DOI:10.1111/j.1747-4949.2012.00885.x] [PMID]
- Miura S, Miyata R, Matsumoto S, Higashi T, Wakisaka Y, Ago T, et al. Quality management program of stroke rehabilitation using adherence to guidelines: A nationwide initiative in Japan. Journal of Stroke and Cerebrovascular Diseases. 2019; 28(9):2434-41. [DOI:10.1016/j.jstrokecerebrovasdis.2019.06.028] [PMID]
- Ahmed SM, Alam BB, Anwar I, Begum T, Huque R, Khan JA, et al. Bangladesh health system review. Asia pacific observatory on health systems and policies. Health Systems in Transition. 2015; 5(3). https://apps.who.int/iris/handle/10665/208214
- Mohuiddin AK. Patient satisfaction with healthcare services: A Bangladesh scenario. Journal of Biomedical Research & Innovation. 2020; 1(1):101. https://www.yumedtext.com/files/publish/published-pdf--6-JBMRI-101.pdf
- Hussain MM, Raihan MMH. Patients’ satisfaction with public health care services in bangladesh: some critical issues. Malaysian Journal of Medical and Biological Research. 2015; 3(1):51-62. [DOI:10.18034/mjmbr.v3i1.405]
- Al Fraihi KJ, Latif SA. Evaluation of outpatient service quality in Eastern Saudi Arabia. Patient’s expectations and perceptions. Saudi medical journal. 2016; 37(4):420-8. [DOI:10.15537/smj.2016.4.14835] [PMID] [PMCID]
- Parasuraman A, Zeithaml VA, Berry LL. SERVQUAL: A multiple-item scale for measuring customer perceptions of service quality. Journal of Retailing. 1988; 64(1):12-40. https://psycnet.apa.org/record/1989-10632-001
- Andaleeb SS, Siddiqui N, Khandakar S. Patient satisfaction with health services in Bangladesh. Health policy and planning. 2007; 22(4):263-73. [DOI:10.1093/heapol/czm017] [PMID]
- Lee D. HEALTHQUAL: a multi-item scale for assessing healthcare service quality. Service Business. 2017; 11(3):491-516. [DOI: 10.1007/s11628-016-0317-2]
- Saha BK, Harries P, Gilhooly KJ. Living with stroke in Bangladesh: Factors influencing Quality of Life (QoL). World Federation of Occupational Therapists Bulletin. 2016; 72(2):117-25. [DOI:10.1007/s11628-016-0317-2]
- Güllü O, Tekindal M, Tekindal MA, Yazicr AC. Evaluation of expected and perceived of quality of service with the SERVQUAL scale: The case of a private physical therapy and rehabilitation center. Biomedical Research. 2017; 28(2). https://www.biomedres.info/abstract/evaluation-of-expected-and-perceived-of-quality-of-service-with-the-servqual-scale-the-case-of-a-private-physical-therapy-and-reha-6357.html
- Swaine B, Dassa C, Koné A, Dutil É, Demers L, Trempe C. The PQRS-montreal: a measure of patients’ perceptions of the quality of rehabilitation services for persons with a traumatic brain injury. Disability and Rehabilitation. 2017; 39(1):59-72. [DOI:10.3109/09638288.2016.1140828] [PMID]
- Kingsley C, Patel S. Patient-reported outcome measures and patient-reported experience measures. BJA Education. 2017; 17(4):137-44. [DOI:10.1093/bjaed/mkw060]
- Torabipour A, Sayaf R, Salehi R, Ghasemzadeh R. Analyzing the quality gapsin the services of rehabilitation centers using the SERVQUAL technique in Ahvaz, Iran. Jundishapur Journal of Health Sciences. 2016; 8(1):e60320. [DOI:10.17795/jjhs-32560]
- Ludviga I, Tambora I. Development of an assessment tool for rehabilitation service quality: An application to the rehabilitation sectorin latvia. International Journal of Recent Scientific Research. 2017; 8(10):20540-7. [DOI:10.24327/ijrsr.2017.0810.0912]
- Charan J, Biswas T. How to calculate sample size for different study designs in medical research?. Indian Journal of Psychological Medicine. 2013; 35(2):121-6. [DOI:10.4103/0253-7176.116232] [PMID] [PMCID]
- Bowling A, Bowling D. Research methods in health: Investigating health and health services. United States: Open University Press; 1997. https://books.google.com/books/about/Research_Methods_in_Health.html?id=1y8QAQAAMAAJ&source=kp_book_description
- Mamin FA, Islam MS, Rumana FS, Faruqui F. Profile of stroke patients treated at a rehabilitation centre in Bangladesh. BMC research notes. 2017; 10(1):520. [DOI:10.1186/s13104-017-2844-x] [PMID] [PMCID]
- Girmay A, Marye T, Haftu M, G/Her D, Brhanu T, Gerensea H. Patients expectation strongly associated with patients perception to nursing care: hospital based cross sectional study. BMC research notes. 2018; 11(1):310. [DOI:10.1186/s13104-018-3447-x] [PMID] [PMCID]
- Marzban S, Najafi M, Etedal MG, Moradi S, Rajaee R. The evaluation of outpatient quality services in physiotherapy in the teaching health centers of Shahid Beheshti University based on SERVQUAL tools. European Journal of Biology and Medical Science Research. 2015; 3(3):46-53. https://www.eajournals.org/journals/european-journal-of-biology-and-medical-science-research-ejbmsr/vol-3issue-3june-2015/the-evaluation-of-outpatient-quality-services-in-physiotherapy-in-the-teaching-health-centers-of-shahid-beheshti-university-based-on-servqual-tools/
- Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Medicine & Science in Sports & Exercise. 2002; 34(12):1996-2001. [DOI:10.1097/00005768-200212000-00020] [PMID]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2020/04/17 | Accepted: 2021/02/1 | Published: 2020/12/1
Received: 2020/04/17 | Accepted: 2021/02/1 | Published: 2020/12/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
