
988368
Fri, Apr 19, 2024

Volume 15, Issue 1 (March 2017 2017)
Iranian Rehabilitation Journal 2017, 15(1): 43-48 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rastogi S, Hamdani N. Comparison of Effects of Bilateral Versus Unilateral Quadriceps Training on Balance, Functional Mobility and Functional Gait in Patients With Stroke. Iranian Rehabilitation Journal 2017; 15 (1) :43-48
URL: http://irj.uswr.ac.ir/article-1-552-en.html
URL: http://irj.uswr.ac.ir/article-1-552-en.html


1- Department of Rehabilitation Sciences, Neurology and Sleep Center, New Delhi, India.
2- Department of Rehabilitation Sciences, Hamdard Institute of Medical Sciences and Research, New Delhi, India.
2- Department of Rehabilitation Sciences, Hamdard Institute of Medical Sciences and Research, New Delhi, India.
Full-Text [PDF 490 kb]
(1921 Downloads)
| Abstract (HTML) (4272 Views)
Full-Text: (938 Views)
1. Introduction
Studies have been conducted on the relationship between whole lower extremity muscle strength, balance, functional gait and functional mobility [1-3]. However, only a few studies have focused on knee extensor muscle strength correlation with functional performances like balance, mobility and gait. The knee extensor muscle is an important contributor to human locomotor efficiency and stability and is crucial to a variety of other ADL too. So, the extension of the leg is an important movement involved in daily life [4-6] .
Few researches have been conducted on the effects of unilateral quadriceps training on balance, functional mobility, and functional gait in patients with stroke [7, 8].
Specifically, deficits are well recognized in both paretic and non-paretic limbs. Bilateral training in which the patient practices identical activities with both of the limbs has been proposed to improve hemiplegic limb control and function. Regulation of bilateral, identical, and synchronous movements appears to be coordinated centrally through bilaterally distributed neural networks connected via the corpus callosum, involving cortical and subcortical areas. These networks stipulate a shared facilitatory drive to both motor cortices, contributing to a sound spatial coupling of limb movement noticed during bilateral, identical, synchronous, and voluntary movements.
Hence, the beneficial effects of bilateral training in stroke are assumed to arise from this coupling effect in which the nonparetic limb provides a template for the paretic limb in terms of movement characteristics, facilitating restoration of movement [9, 10]. This study is aimed to find out the effect of bilateral quadriceps training compared to the unilateral quadriceps training on balance, functional mobility, and functional gait in patients with stroke.
2. Methods
A total of 30 subjects were selected by random sampling based on inclusion and exclusion criteria. All the patients were recruited from the inpatient and outpatient department of HAHCH, Jamia Hamdard New Delhi.
Subjects
Inclusion criteria: Male/female between 40-60 years of age; hemiparetic patients with post-stroke of 1-6 months; patients having ischemic stroke or hemorrhagic stroke (Unilateral stroke); patients who were able to follow verbal commands or demonstrated directions, which ensured that each patient was trainable (MMSE>=24); Berg balance scale less than 45/56; motricity index of score as 25 points, i.e. movement against gravity was taken into account.
Exclusion criteria: Brain tumors associated with CVA; patients having another mobility limiting neurological condition (e.g. dementia or Parkinson’s disease) or any etiology of trauma or any identified orthopedic condition (Osteoporosis, RA, OA); and patient having serious uncontrolled medical complications.
Procedure
Subjects were selected according to the inclusion and exclusion criteria. Informed consent was obtained from each patient before confirming their participation in the study. On the first visit, data in the form of scores was obtained through Berg balance scale, dynamic gait index, timed up and go test, and strain gauge. Then data was obtained with the help of the above-mentioned scales and strain gauge 6 weeks after providing the patient with strength training. Group A consisted of patients who got unilateral training, and Group B consisted of patients who got bilateral training. Firstly, the isometric muscle strength was measured with strain gauge.
The patients were made to sit in a high sitting position on quadriceps table and made to push one side of distal arm of quadriceps table in the forward direction (extension of leg). The other side of the distal arm of quadriceps table was attached to the ring of chain. The chain was attached to strain gauge’s ring through a hook. Finally, the strain gauge’s other ring was attached to a hook, which was further attached by a chain to the rod that was tied to the posterior legs of quadriceps table. The subject was allowed 5 seconds to develop the maximum contraction. This was done to prevent a sudden snatching effort and also prevent a prolonged effort of more than 5 seconds at the end of which the subject merely would maintain his maximum effort rather than increase it. The average of three successive measurements was taken at intervals of one minute and again after 6 weeks of successful completion of the treatment protocol. Three other successive measurements were also taken accordingly.
Training program
The subjects were made to participate in a supervised strength training three times a week for 6 weeks. In each training session, the knee extension progressive resistance exercises were performed. In one-half of the subjects, bilateral training was performed while in another group, exercises were performed unilaterally. In bilateral training, the affected one was first trained followed by training of the unaffected one.
During the first 2 weeks of the training, the subjects were trained with the loads of 50% of 1 RM. Twelve repetitions were performed per set and total sets were four. During the second two weeks of training, the subjects were trained with the loads of 70% of 1 RM. Eight repetitions were performed per set, and the total sets were five. During the last two weeks of the training, the subjects were trained with the loads of 80% of 1RM. Six repetitions were performed per set, and the total sets were six [11].
Data Analysis
Statistical analysis was done using SPSS Software. Independent t-test was used to compare the impacts of bilateral against unilateral quadriceps training on balance, functional mobility, and functional gait of the patients with stroke. Student’s t-test was used to compare isometric strength, Berg balance scale, dynamic gait index and timed up and go test values in both of the groups after training of 6 weeks. A significance level of 0.05 was used for all statistical comparisons.
3. Results
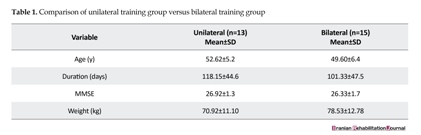
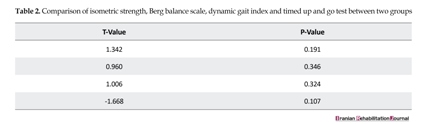
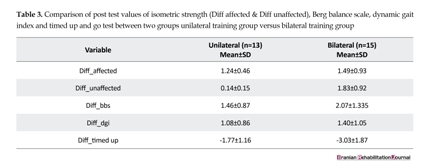
The study consisted of two groups. Group 1 comprised of unilateral training patients, which had 10 males and 3 females with a mean age of 52.62 years while group 2 had 12 males and 3 females with a mean age of 49.60 years. Each patient’s age, duration since onset, MMSE, and weight was recorded. Table 1, 2 gives the details of the mean and standard deviations of these scores. These variables had no significant difference between the two groups. Increase in pre values to post values for isometric strength of affected side, Berg balance scale and dynamic gait index showed no significant difference while timed up and go test and isometric strength of unaffected side showed a significant difference (Table 3 and 4).
4. Discussion
Every parameter in the demographic data like age, gender, duration since onset, MMSE, and weight in both the group’s analysis showed homogeneity.
Age
Age showed non-significant results. The mean age was 52.62 years with a standard deviation of 5.2 in the unilateral training group, and the mean age was 49.60 years with a standard deviation of 6.4 in the bilateral training group (Table 1). In the present study, the age for both the groups was homogeneous, indicating there was no difference in both the groups (the distribution was equal in both of them) (Table 1).
Duration since onset
Duration since onset showed non-significant results. The mean duration was 118.15 with a standard deviation of 44.6 in the unilateral training group, and the mean duration was 101.33 with a standard deviation of 47.5 in the bilateral training group (Table 1). The duration since onset for both of the groups came out to be of equal means with no difference in their distribution.
MMSE
MMSE showed non-significant results while the mean cognitive values for unilateral training group was 26.92 with a standard deviation of 1.3 and for the bilateral training group was 26.33 with a standard deviation of 1.7. MMSE values for both the groups were equally distributed (Table 1).
Studies have been conducted on the relationship between whole lower extremity muscle strength, balance, functional gait and functional mobility [1-3]. However, only a few studies have focused on knee extensor muscle strength correlation with functional performances like balance, mobility and gait. The knee extensor muscle is an important contributor to human locomotor efficiency and stability and is crucial to a variety of other ADL too. So, the extension of the leg is an important movement involved in daily life [4-6] .
Few researches have been conducted on the effects of unilateral quadriceps training on balance, functional mobility, and functional gait in patients with stroke [7, 8].
Specifically, deficits are well recognized in both paretic and non-paretic limbs. Bilateral training in which the patient practices identical activities with both of the limbs has been proposed to improve hemiplegic limb control and function. Regulation of bilateral, identical, and synchronous movements appears to be coordinated centrally through bilaterally distributed neural networks connected via the corpus callosum, involving cortical and subcortical areas. These networks stipulate a shared facilitatory drive to both motor cortices, contributing to a sound spatial coupling of limb movement noticed during bilateral, identical, synchronous, and voluntary movements.
Hence, the beneficial effects of bilateral training in stroke are assumed to arise from this coupling effect in which the nonparetic limb provides a template for the paretic limb in terms of movement characteristics, facilitating restoration of movement [9, 10]. This study is aimed to find out the effect of bilateral quadriceps training compared to the unilateral quadriceps training on balance, functional mobility, and functional gait in patients with stroke.
2. Methods
A total of 30 subjects were selected by random sampling based on inclusion and exclusion criteria. All the patients were recruited from the inpatient and outpatient department of HAHCH, Jamia Hamdard New Delhi.
Subjects
Inclusion criteria: Male/female between 40-60 years of age; hemiparetic patients with post-stroke of 1-6 months; patients having ischemic stroke or hemorrhagic stroke (Unilateral stroke); patients who were able to follow verbal commands or demonstrated directions, which ensured that each patient was trainable (MMSE>=24); Berg balance scale less than 45/56; motricity index of score as 25 points, i.e. movement against gravity was taken into account.
Exclusion criteria: Brain tumors associated with CVA; patients having another mobility limiting neurological condition (e.g. dementia or Parkinson’s disease) or any etiology of trauma or any identified orthopedic condition (Osteoporosis, RA, OA); and patient having serious uncontrolled medical complications.
Procedure
Subjects were selected according to the inclusion and exclusion criteria. Informed consent was obtained from each patient before confirming their participation in the study. On the first visit, data in the form of scores was obtained through Berg balance scale, dynamic gait index, timed up and go test, and strain gauge. Then data was obtained with the help of the above-mentioned scales and strain gauge 6 weeks after providing the patient with strength training. Group A consisted of patients who got unilateral training, and Group B consisted of patients who got bilateral training. Firstly, the isometric muscle strength was measured with strain gauge.
The patients were made to sit in a high sitting position on quadriceps table and made to push one side of distal arm of quadriceps table in the forward direction (extension of leg). The other side of the distal arm of quadriceps table was attached to the ring of chain. The chain was attached to strain gauge’s ring through a hook. Finally, the strain gauge’s other ring was attached to a hook, which was further attached by a chain to the rod that was tied to the posterior legs of quadriceps table. The subject was allowed 5 seconds to develop the maximum contraction. This was done to prevent a sudden snatching effort and also prevent a prolonged effort of more than 5 seconds at the end of which the subject merely would maintain his maximum effort rather than increase it. The average of three successive measurements was taken at intervals of one minute and again after 6 weeks of successful completion of the treatment protocol. Three other successive measurements were also taken accordingly.
Training program
The subjects were made to participate in a supervised strength training three times a week for 6 weeks. In each training session, the knee extension progressive resistance exercises were performed. In one-half of the subjects, bilateral training was performed while in another group, exercises were performed unilaterally. In bilateral training, the affected one was first trained followed by training of the unaffected one.
During the first 2 weeks of the training, the subjects were trained with the loads of 50% of 1 RM. Twelve repetitions were performed per set and total sets were four. During the second two weeks of training, the subjects were trained with the loads of 70% of 1 RM. Eight repetitions were performed per set, and the total sets were five. During the last two weeks of the training, the subjects were trained with the loads of 80% of 1RM. Six repetitions were performed per set, and the total sets were six [11].
Data Analysis
Statistical analysis was done using SPSS Software. Independent t-test was used to compare the impacts of bilateral against unilateral quadriceps training on balance, functional mobility, and functional gait of the patients with stroke. Student’s t-test was used to compare isometric strength, Berg balance scale, dynamic gait index and timed up and go test values in both of the groups after training of 6 weeks. A significance level of 0.05 was used for all statistical comparisons.
3. Results
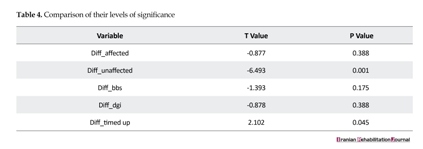
The study consisted of two groups. Group 1 comprised of unilateral training patients, which had 10 males and 3 females with a mean age of 52.62 years while group 2 had 12 males and 3 females with a mean age of 49.60 years. Each patient’s age, duration since onset, MMSE, and weight was recorded. Table 1, 2 gives the details of the mean and standard deviations of these scores. These variables had no significant difference between the two groups. Increase in pre values to post values for isometric strength of affected side, Berg balance scale and dynamic gait index showed no significant difference while timed up and go test and isometric strength of unaffected side showed a significant difference (Table 3 and 4).
4. Discussion
Every parameter in the demographic data like age, gender, duration since onset, MMSE, and weight in both the group’s analysis showed homogeneity.
Age
Age showed non-significant results. The mean age was 52.62 years with a standard deviation of 5.2 in the unilateral training group, and the mean age was 49.60 years with a standard deviation of 6.4 in the bilateral training group (Table 1). In the present study, the age for both the groups was homogeneous, indicating there was no difference in both the groups (the distribution was equal in both of them) (Table 1).
Duration since onset
Duration since onset showed non-significant results. The mean duration was 118.15 with a standard deviation of 44.6 in the unilateral training group, and the mean duration was 101.33 with a standard deviation of 47.5 in the bilateral training group (Table 1). The duration since onset for both of the groups came out to be of equal means with no difference in their distribution.
MMSE
MMSE showed non-significant results while the mean cognitive values for unilateral training group was 26.92 with a standard deviation of 1.3 and for the bilateral training group was 26.33 with a standard deviation of 1.7. MMSE values for both the groups were equally distributed (Table 1).




Weight
Weight also showed non-significant results. The unilateral training group showed a mean of 70.92 kg with a standard deviation of 11.10, and the bilateral training group showed a mean of 78.53 kg with a standard deviation of 12.78. The weight of the patients was in uniformity in both the groups. An increase in particular variables from pre values to post values was observed (Table 1 and 2).
Isometric strength on the affected side showed non-significant results. Isometric strength on affected side after bilateral training was not much improved as compared to after unilateral training (Table 3 and 4). Previous studies have also shown significant gains in the strength of affected side after 6 weeks of intervention by isokinetic strength training. Others have shown significant gains in the strength of paretic limb knee extensors when PRT was applied [5, 6, 9].
Regardless of the resistance training mode employed, the resistance exercise should focus on other impairments like non-paretic limb.11 Interestingly, in the contra lateral side, both changes in intrinsic muscle characteristics and impaired neural activation seemed responsible. In the unilateral side, reduced rate of torque development seemed primarily related to neural activation changes. Hence, strengthening regimens of the paretic as well as non-paretic limbs are important [12-14].
Isometric strengthening of the unaffected side showed significant results. Isometric strength on the unaffected side for bilateral training was more effective than unilateral training (Table 3 and 4). Previous studies have also shown significant improvement on the non-paretic side strength after stroke by stating that beneficial effects in bilateral training given on unaffected side in stroke also gave a coupling effect. The non-paretic limb provided a template for paretic limb in terms of movement characteristics, facilitating restoration of movement [9].
According to this study, functional performances were found to be correlated with both of the limbs and served as indicators of impairment. Berg balance scale for bilateral training was no more effective than unilateral training. Dynamic Gait Index (DGI) showed non-significant results in both unilateral and bilateral training groups, suggesting that DGI for bilateral training was no more effective compared to unilateral training. Timed up and go test showed significant results, suggesting its effectiveness for bilateral training than for unilateral training.
According to the results obtained in this study, two parameters, i.e., isometric strength of unaffected side and timed up and go test showed significant results in which bilateral training showed to be good. The other three parameters, i.e., isometric strength of affected side, Berg balance scale and dynamic gait index, showed insignificant results (Table 3 and 4). This proved that bilateral quadriceps training is not much effective than unilateral quadriceps training.
5. Conclusion
The findings of the present study suggested that bilateral quadriceps training is good for improving functional performance like timed up and go test and isometric strength on the unaffected side. For further improvement, the Berg balance scale, dynamic gait index and isometric strength scores of affected side, both for the bilateral quadriceps or unilateral quadriceps training, have been proved to be equally effective.
Acknowledgments
We appreciate all the financial support provided by Hamdard Institute of Medical Sciences and Research, New Delhi.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Akbari A, Karimi H. The relationship between lower extremity muscle strength and functional performance in hemiparetic patients. Journal of Medical Sciences. 2006; 6(3):327-331. doi: 10.3923/jms.2006.327.331
[2]Kligyte I, Lundy-Ekman L, Medeiros JM. Relationship between lower extremity muscle strength and dynamic balance in people post stroke. Medicina. 2003; 39(2): 122-8. PMID: 12626864
[3]Daubney ME, Culham EG. Lower extremity muscle force and balance performance in adults aged 65 years and older. Physical Therapy. 1999; 79(12):1177-85. PMID: 10630286
[4]Fukagawa NK, Wolfson L, Judge J, Whipple R, King M. Strength is a major factor in balance, gait, and the occurrence of falls. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 1995; 50A(Special):64–7. doi: 10.1093/gerona/50a.special_issue.64
[5]Ada L, Dorsch S, Canning CG. Strengthening interventions increase strength and improve activity after stroke: A systematic review. Australian Journal of Physiotherapy. 2006; 52(4):241-8. doi: 10.1016/s0004-9514(06)70003-4
[6]Teixeira-Salmela LF, Olney SJ, Nadeau S, Brouwer B. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Archives of Physical Medicine and Rehabilitation. 1999; 80(10):1211–8. doi: 10.1016/s0003-9993(99)90018-7
[7]Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee: Effects on function and spasticity. Archives of Physical Medicine and Rehabilitation. 1997; 78(11):1231–6. doi: 10.1016/s0003-9993(97)90337-3
[8]Flansbjer U, Miller M, Downham D, Lexell J. Progressive resistance training after stroke: Effects on muscle strength, muscle tone, gait performance and perceived participation. Journal of Rehabilitation Medicine. 2008; 40(1):42–8. doi: 10.2340/16501977-0129
[9]Ouellette MM, LeBrasseur NK, Bean JF, Phillips E, Stein J, Frontera WR, et al. High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors. stroke. Ovid Technologies. 2004; 35(6):1404-9. doi: 10.1161/01.str.0000127785.73065.34
[10]Bohannon RW, Andrews AW. Limb muscle strength is impaired bilaterally after stroke. Journal of Physical Therapy Science. 1995; 7(1):1–7. doi: 10.1589/jpts.7.1
[11]Kennedy WR. The development and comparison of an electrical strain gauge dynamometer and a cable tensiometer for objective muscle testing. Archives of Physical Medicine and Rehabilitation. 1965; 46(12):793-803. PMID: 5855041
[12]Horstman AM, Gerrits KH, Beltman MJ, Koppe PA, Janssen TW, De Haan A. Intrinsic properties of the knee extensor muscles after subacute stroke. Archives of Physical Medicine and Rehabilitation. 2010; 91(1):123–8. doi: 10.1016/j.apmr.2009.09.008
[13]Munn J. Contralateral effects of unilateral resistance training: A meta-analysis. Journal of Applied Physiology. 2004; 96(5):1861-6. doi: 10.1152/japplphysiol.00541.2003
[14]Gerrits KH, Beltman MJ, Koppe PA, Konijnenbelt H, Elich PD, de Haan A, et al. Isometric muscle function of knee extensors and the relation with functional performance in patients with stroke. Archives of Physical Medicine and Rehabilitation. 2009; 90(3):480-7. doi: 10.1016/j.apmr.2008.09.562
Weight also showed non-significant results. The unilateral training group showed a mean of 70.92 kg with a standard deviation of 11.10, and the bilateral training group showed a mean of 78.53 kg with a standard deviation of 12.78. The weight of the patients was in uniformity in both the groups. An increase in particular variables from pre values to post values was observed (Table 1 and 2).
Isometric strength on the affected side showed non-significant results. Isometric strength on affected side after bilateral training was not much improved as compared to after unilateral training (Table 3 and 4). Previous studies have also shown significant gains in the strength of affected side after 6 weeks of intervention by isokinetic strength training. Others have shown significant gains in the strength of paretic limb knee extensors when PRT was applied [5, 6, 9].
Regardless of the resistance training mode employed, the resistance exercise should focus on other impairments like non-paretic limb.11 Interestingly, in the contra lateral side, both changes in intrinsic muscle characteristics and impaired neural activation seemed responsible. In the unilateral side, reduced rate of torque development seemed primarily related to neural activation changes. Hence, strengthening regimens of the paretic as well as non-paretic limbs are important [12-14].
Isometric strengthening of the unaffected side showed significant results. Isometric strength on the unaffected side for bilateral training was more effective than unilateral training (Table 3 and 4). Previous studies have also shown significant improvement on the non-paretic side strength after stroke by stating that beneficial effects in bilateral training given on unaffected side in stroke also gave a coupling effect. The non-paretic limb provided a template for paretic limb in terms of movement characteristics, facilitating restoration of movement [9].
According to this study, functional performances were found to be correlated with both of the limbs and served as indicators of impairment. Berg balance scale for bilateral training was no more effective than unilateral training. Dynamic Gait Index (DGI) showed non-significant results in both unilateral and bilateral training groups, suggesting that DGI for bilateral training was no more effective compared to unilateral training. Timed up and go test showed significant results, suggesting its effectiveness for bilateral training than for unilateral training.
According to the results obtained in this study, two parameters, i.e., isometric strength of unaffected side and timed up and go test showed significant results in which bilateral training showed to be good. The other three parameters, i.e., isometric strength of affected side, Berg balance scale and dynamic gait index, showed insignificant results (Table 3 and 4). This proved that bilateral quadriceps training is not much effective than unilateral quadriceps training.
5. Conclusion
The findings of the present study suggested that bilateral quadriceps training is good for improving functional performance like timed up and go test and isometric strength on the unaffected side. For further improvement, the Berg balance scale, dynamic gait index and isometric strength scores of affected side, both for the bilateral quadriceps or unilateral quadriceps training, have been proved to be equally effective.
Acknowledgments
We appreciate all the financial support provided by Hamdard Institute of Medical Sciences and Research, New Delhi.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Akbari A, Karimi H. The relationship between lower extremity muscle strength and functional performance in hemiparetic patients. Journal of Medical Sciences. 2006; 6(3):327-331. doi: 10.3923/jms.2006.327.331
[2]Kligyte I, Lundy-Ekman L, Medeiros JM. Relationship between lower extremity muscle strength and dynamic balance in people post stroke. Medicina. 2003; 39(2): 122-8. PMID: 12626864
[3]Daubney ME, Culham EG. Lower extremity muscle force and balance performance in adults aged 65 years and older. Physical Therapy. 1999; 79(12):1177-85. PMID: 10630286
[4]Fukagawa NK, Wolfson L, Judge J, Whipple R, King M. Strength is a major factor in balance, gait, and the occurrence of falls. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 1995; 50A(Special):64–7. doi: 10.1093/gerona/50a.special_issue.64
[5]Ada L, Dorsch S, Canning CG. Strengthening interventions increase strength and improve activity after stroke: A systematic review. Australian Journal of Physiotherapy. 2006; 52(4):241-8. doi: 10.1016/s0004-9514(06)70003-4
[6]Teixeira-Salmela LF, Olney SJ, Nadeau S, Brouwer B. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Archives of Physical Medicine and Rehabilitation. 1999; 80(10):1211–8. doi: 10.1016/s0003-9993(99)90018-7
[7]Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee: Effects on function and spasticity. Archives of Physical Medicine and Rehabilitation. 1997; 78(11):1231–6. doi: 10.1016/s0003-9993(97)90337-3
[8]Flansbjer U, Miller M, Downham D, Lexell J. Progressive resistance training after stroke: Effects on muscle strength, muscle tone, gait performance and perceived participation. Journal of Rehabilitation Medicine. 2008; 40(1):42–8. doi: 10.2340/16501977-0129
[9]Ouellette MM, LeBrasseur NK, Bean JF, Phillips E, Stein J, Frontera WR, et al. High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors. stroke. Ovid Technologies. 2004; 35(6):1404-9. doi: 10.1161/01.str.0000127785.73065.34
[10]Bohannon RW, Andrews AW. Limb muscle strength is impaired bilaterally after stroke. Journal of Physical Therapy Science. 1995; 7(1):1–7. doi: 10.1589/jpts.7.1
[11]Kennedy WR. The development and comparison of an electrical strain gauge dynamometer and a cable tensiometer for objective muscle testing. Archives of Physical Medicine and Rehabilitation. 1965; 46(12):793-803. PMID: 5855041
[12]Horstman AM, Gerrits KH, Beltman MJ, Koppe PA, Janssen TW, De Haan A. Intrinsic properties of the knee extensor muscles after subacute stroke. Archives of Physical Medicine and Rehabilitation. 2010; 91(1):123–8. doi: 10.1016/j.apmr.2009.09.008
[13]Munn J. Contralateral effects of unilateral resistance training: A meta-analysis. Journal of Applied Physiology. 2004; 96(5):1861-6. doi: 10.1152/japplphysiol.00541.2003
[14]Gerrits KH, Beltman MJ, Koppe PA, Konijnenbelt H, Elich PD, de Haan A, et al. Isometric muscle function of knee extensors and the relation with functional performance in patients with stroke. Archives of Physical Medicine and Rehabilitation. 2009; 90(3):480-7. doi: 10.1016/j.apmr.2008.09.562
Article type: Original Research Articles |
Received: 2016/09/10 | Accepted: 2016/12/26 | Published: 2017/03/1
Received: 2016/09/10 | Accepted: 2016/12/26 | Published: 2017/03/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
