
988368
Thu, Apr 25, 2024

Volume 15, Issue 2 (June 2017)
Iranian Rehabilitation Journal 2017, 15(2): 173-180 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khalaji M, Kalantari M, Shafiee Z, Hosseini M A. The Effect of Hydrotherapy on Health of Cerebral Palsy Patients: An Integrative Review. Iranian Rehabilitation Journal 2017; 15 (2) :173-180
URL: http://irj.uswr.ac.ir/article-1-703-en.html
URL: http://irj.uswr.ac.ir/article-1-703-en.html


1- Department of Occupational Therapy, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Rehabmanagment, University of Social Welfare and Rehabilitation Science, Tehran, Iran.
2- Department of Rehabmanagment, University of Social Welfare and Rehabilitation Science, Tehran, Iran.
Full-Text [PDF 582 kb]
(6603 Downloads)
| Abstract (HTML) (17052 Views)
Full-Text: (7303 Views)
1. Introduction
Hydrotherapy is one of the most popular forms of complementary therapies that help in the treatment of children with cerebral palsy and motor neuron disorders. It is known to provide an opportunity to the patients of cerebral palsy to do easier exercises. Hydrotherapy is also known to have useful implications in the treatment of children with neurodevelopmental disorders by improving their physiological and psychological state of being [1]. In addition, it also provides them the ability to do body movements, especially among children who enjoy doing training activities witch moving on the ground is difficult for them. Hence, hydrotherapy is proposed as an immune and complementary therapy in children with cerebral palsy, even those who are diagnosed with low levels of GMFCS [2].
The benefits of water based treatment methods rely on its anti-gravity position and buoyancy. It can thus help in weight loss and reduce compressive forces on joints. As a result, the therapy promotes active and easier movements for children who are not able to do certain ground activities. Finally, owing to the hydrostatic pressure effects of water, hydrotherapy can reduce muscular spasticity and improve endurance to multi-sensory stimulants, and increase blood circulation [3].
Varied applications of hydrotherapy have been displayed in the persisting literature. The most common applications of the therapy included include strength, aerobic and anaerobic training or swimming and playing in the water [4-8]. While some of these studies employed specific techniques, such as “Halliwick”, “Watsu” and “Bad Ragaz”. Halliwick hydrotherapy is a specially designed holistic and task-based approach which is based on the International Classification of Functioning, disability and health structure, including postural control, reducing muscle stiffness and facilitating the movement to achieve performance goals on the ground. Most Halliwick treatment methods are active and designed to facilitate the movement and sensory input. It also has a passive component, which is applied by the therapist for selective activation of muscles and stabilization of specific joints. First, the disabled person learns how to maintain their balance in a stable position and then they learn how to keep their balance on an unstable position while moving in the water [9]. Watsu is a gentle and quiet form of body therapy, which is usually performed in warm water (35°C). It is essentially a combination of massage, joint movements, shiatsu, muscle stretching and dance. The patient is continually supported while floating, swinging in the water and stretching [10]. On the other hand, Bad Ragaz is a special type of individualistic hydrotherapy which is based on the principles of PNF. In this type of therapy, the patient is supported by specific tools for floating, and the therapist applies resistance against the active movements of the patient [11].
Despite the evidences on the positive effects of hydrotherapy on children with cerebral palsy, it is still not standardized for use in Iran. It is expected that review and representation of the related resources may help in creation of a clinical guideline for its implementation in the said country. Due to the presence of a wide variety of hydrotherapy based methods and multifactorial investigation of its results on various types of cerebral palsy, it was thought that an integrative review of the varieties of hydrotherapy and their application on ICF of children with spastic diplegia cerebral palsy. The present study encompassed the analysis of the related manuscripts published between 2000 and 2016.
2. Methods
In this study, integrative review method was used. Integrative studies are the most extensive review studies that simultaneously allow empirical and non-empirical studies so as to achieve a full understanding of a phenomenon. Integrative studies can also combine data from theoretical studies as well as experimental studies with each other. In addition, integrative studies combine a wide range of purposes, including the definition of concepts, review of theories, review of the evidence and methodological analysis of a specific title [12]. For this study, Cooper’s strategy in the integrated review was used. The strategy includes the following: 1. Formulation of the problem, 2. Reviewing the evidences and providing required resources, 3. Evaluating the data, 4. Data analysis and 5. Publication of results. In this regard, Hosseini and colleagues have written an article on such integrated reviews [12]. Given the type of study and pyramid of evidence, the level of evidence was determined.
Formulation of the problem
Hydrotherapy is one of the most useful therapies applicable for the rehabilitation of children with neurodevelopmental disorders and improving their physiological and psychological achievements [1]. However, previous studies based on growth levels of children with cerebral palsy showed that there exist many doubts regarding the effectiveness of hydrotherapy. Therefore, before the use of hydrotherapy as a treatment measure among children with cerebral palsy is promoted, it is essential to answer the prevailing question “which hydrotherapy method, in what conditions, for which group of children and with what function level shall be used?” Therefore, the aim of this study was to investigate the effects of hydrotherapy on spastic diplegia cerebral palsy patients.
The main question of the study included the following: 1) How is the method of hydrotherapy for children with spastic diplegia cerebral palsy in the available literature?; 2) What are the specified effects of hydrotherapy on spastic diplegia cerebral palsy patients with different levels of motor development?; 3) What are the results of hydrotherapy based on the ICF?; and 4) What are the most important factors that influence the effectiveness of hydrotherapy in children with cerebral palsy?
Review of the literature and providing the required evidence
The present study encompassed a search for the information and theoretical foundations related to the application of hydrotherapy in children with cerebral palsy. It also involved the identification of effective conditions and factors that influence the outcome of the therapy and how they were dependent on the growth levels and types of hydrotherapy. This information was identified from the related sites, internet search as well as manual search in databases and reference books.
All articles related to the effects of hydrotherapy on patients with spastic diplegia cerebral palsy were investigated in following Iranian and foreign databases: OTDBASE Occupational Therapy Journal Literature Search Service; PEDRO; OT SEARCH (FORMERLY OT BIBSYS; CINAHL Database; Science Direct; Pub med; Elsevier; Scientific Information Database (SID); Magiran; and Google scholar.
Keywords used in the search process included the following: Cerebral palsy, diplegic spastic, rehabilitation, occupational therapy, hydrotherapy, aquatic therapy, water treatment and water exercises.
The obtained articles were examined on the basis of multidimensional factors, such as: purpose statements, inclusion criteria, characteristics of the research, citation of previous reviews, criticism of previous reviews, presentation of preliminary research findings, methods of analysis of the results, discussion of methodological problems, effective systematic searches, interpretation of results and tables. To interpret the collected data, cases based on the following specifications were used: study type, used models and tools, number of samples, date of publication and the number of papers used in this article.
Samples
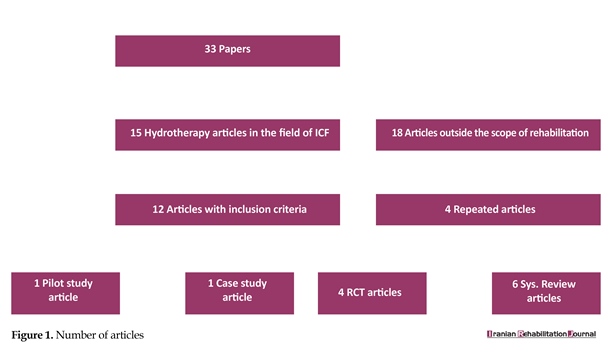
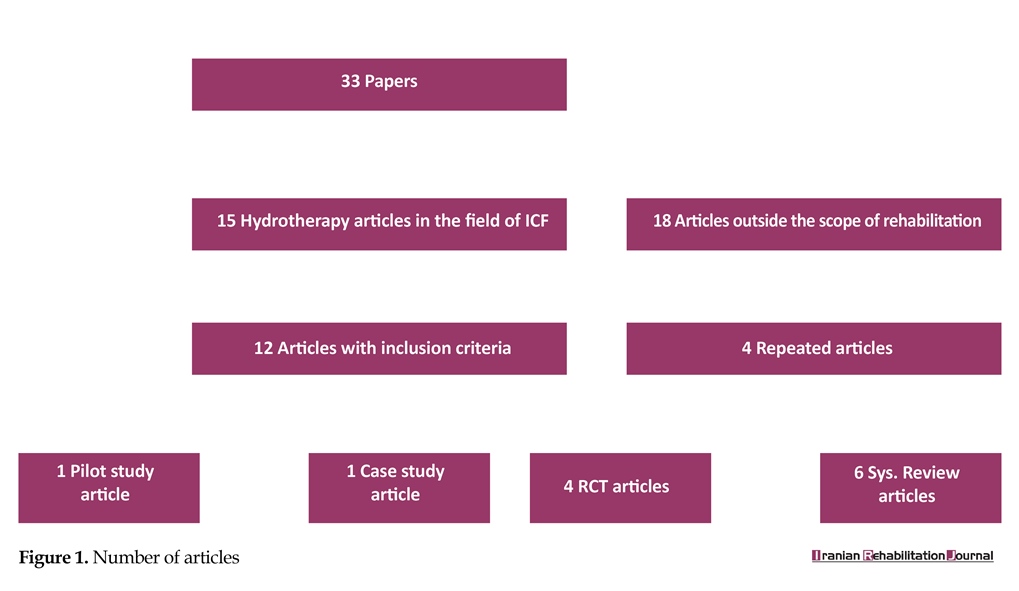
A total of 33 papers based on the effects of hydrotherapy in patients with cerebral palsy were selected for this study. After careful examination of the title, abstract and full-text of articles, and the methods of study employed, 22 articles were excluded from the study due to non-relevance to the subject, being repeated in two or several databases, and poor or unrelated relevance to study aims. Finally, 11 articles were found to suffice the inclusion criteria and were hence included in the present study. Finally, the full-text of the articles were reviewed by the researchers.
Inclusion criteria were: 1) Articles based on spastic diplegia cerebral palsy in children in the age group of 4 to 21 years; 2) Summary or the full-text content of the article in Farsi and English languages; 3) Being published within the period 2000 to 2016; 4) Based on the evaluation of the effect of hydrotherapy in the domain of ICF; and 5) Investigation of hydrotherapy interventions alone or in addition to routine treatment methods.
Exclusion criteria were: 1) Articles that do not include a description of the intervention in full detail; and 2) Articles that investigated hydrotherapy with other non-occupational therapy and physiotherapy.
Data evaluation
The extracted data were prioritized according to the type and methods of study. The review section included descriptive content analysis of the collected data and was formulated based on the type and purpose of the study, the number and profile of participants, type and performing the intervention in terms of the time and number of sessions, assessment tools and the results. The findings were gathered without personal judgment and were arranged according to the order in which they were provided to the experts. Articles that met the inclusion criteria on the basis of the pyramid of evidence included systematic reviews (6 articles), randomized clinical trials (4 papers), pilot study (1 article) and case report (1 article).
Data analysis
At this point, the results of all reviewed articles were summed up and classified based on the ICF domains.
Body function and structure
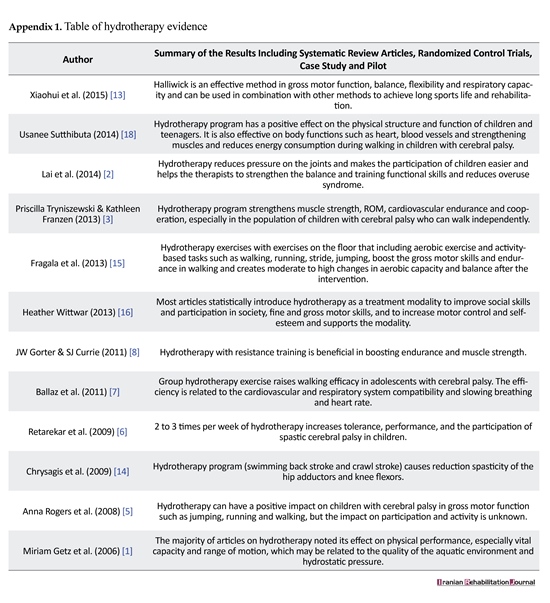
In this area of the ICF, ten articles were found, and their results were related to the structure and function of the body. They investigated the effect of hydrotherapy on variables such as gross motor function, flexibility, balance, respiratory capacity, the function of heart, vessels and muscles, energy expenditure during walking and range of motion, the results of which are provided separately. The Halliwick method is an effective method for the analysis of gross motor function, balance, flexibility and respiratory capacity of children with cerebral palsy (evidence Level II) [13].
Hydrotherapy program was found to have positive effects on the body function and structure of children and teenagers with cerebral palsy. It can also strengthen the function of heart, vessels and muscles and reduce energy consumption during walking (evidence level I) [3]. Hydrotherapy program (swimming back stroke and crawl stroke) causes a reduction in spasticity of the hip adductors and knee flexors (evidence level II) [14].
Hydrotherapy program was also found to cause significant growth in GMFM, and other parameters relating to walking speed and step length. It was also found to increase strength, range of motion and cardiovascular endurance in children with cerebral palsy who can walk independently (evidence level I) [3]. It was also found that when administered in combination with occupational therapy, hydrotherapy program can help in improvement of gross motor function, particularly at GMFCS level 2 and spastic diplegia type. Hence, it can be used as a substitutional yet safe method of treatment even in children with cerebral palsy or GMFCS level 4 patients whose abilities in performing ground training are limited (evidence level II) [2].
Water aerobics program helps in improving motor skills in children with mild to moderate physical disorders, but it was not found to have any significant effects on the functional strength, balance and aerobic capacity of the patients (level III evidence) [15].
Group hydrotherapy exercises help in improving walking capabilities in cerebral palsy teenagers by establishing compatibility of functions between heart and respiratory system and reducing the rate and number of heartbeat (level II evidence) [7]. The most significant effects of hydrotherapy on cerebral palsy patients include increased focus, muscle strength, balance, increased threshold of touch, starting and keeping eye contact (level I evidence) [16]. Furthermore, hydrotherapy also imposes positive effects on gross motor functions, such as jumping, running and walking (level I evidence) [5]. Application of hydrotherapy exercises along with resistance training was also found to be beneficial in boosting endurance and muscle strength (level I evidence) [8].
Hydrotherapy program leads to growth at all levels of ICF and increases children’s motivation levels (level III evidence) [6]. It was also found to have a positive effect on physical performance and vital capacity and range of motion (level I evidence) [1].
Activity
In this area of the ICF, the results of three articles dealt with the different activities of spastic cerebral palsy children, such as ADL, work performance and consciousness. Group hydrotherapy program was found to have positive impacts on the quality of life of patients with cerebral palsy. It allows them to walk farther distances with less fatigue (level II evidence) [7].
The beneficial effects of hydrotherapy on motor functions cannot be attributed to growth in Activity Daily Living (ADL) and the quality of health of life. (Level III evidence) [6]. Hydrotherapy also impacts the work performance, but they were not found to be more effective than conventional treatments. However, children seem to really enjoy this intervention, it should not be eliminated from occupational therapy interventions. (Level A evidence) [16].
The effect of hydrotherapy on the participation of spastic cerebral palsy children was confirmed in only two papers- (Level I evidence) [3], (level III evidence) [6] and it was further remarked that there is need for further research in this area (level A evidence) [5, 8, 18] (Figure 1).
3. Discussion
This study aimed to investigate various methods of hydrotherapy in children with spastic diplegia cerebral palsy and its impact on their GMFCS performance levels. The study also aimed to implement the results of integrative review and the experts’ critiques for the determination of effects of hydrotherapy on the improvement of various aspects of ICF. Interestingly no relevant evidences of the same were found in articles published
Hydrotherapy is one of the most popular forms of complementary therapies that help in the treatment of children with cerebral palsy and motor neuron disorders. It is known to provide an opportunity to the patients of cerebral palsy to do easier exercises. Hydrotherapy is also known to have useful implications in the treatment of children with neurodevelopmental disorders by improving their physiological and psychological state of being [1]. In addition, it also provides them the ability to do body movements, especially among children who enjoy doing training activities witch moving on the ground is difficult for them. Hence, hydrotherapy is proposed as an immune and complementary therapy in children with cerebral palsy, even those who are diagnosed with low levels of GMFCS [2].
The benefits of water based treatment methods rely on its anti-gravity position and buoyancy. It can thus help in weight loss and reduce compressive forces on joints. As a result, the therapy promotes active and easier movements for children who are not able to do certain ground activities. Finally, owing to the hydrostatic pressure effects of water, hydrotherapy can reduce muscular spasticity and improve endurance to multi-sensory stimulants, and increase blood circulation [3].
Varied applications of hydrotherapy have been displayed in the persisting literature. The most common applications of the therapy included include strength, aerobic and anaerobic training or swimming and playing in the water [4-8]. While some of these studies employed specific techniques, such as “Halliwick”, “Watsu” and “Bad Ragaz”. Halliwick hydrotherapy is a specially designed holistic and task-based approach which is based on the International Classification of Functioning, disability and health structure, including postural control, reducing muscle stiffness and facilitating the movement to achieve performance goals on the ground. Most Halliwick treatment methods are active and designed to facilitate the movement and sensory input. It also has a passive component, which is applied by the therapist for selective activation of muscles and stabilization of specific joints. First, the disabled person learns how to maintain their balance in a stable position and then they learn how to keep their balance on an unstable position while moving in the water [9]. Watsu is a gentle and quiet form of body therapy, which is usually performed in warm water (35°C). It is essentially a combination of massage, joint movements, shiatsu, muscle stretching and dance. The patient is continually supported while floating, swinging in the water and stretching [10]. On the other hand, Bad Ragaz is a special type of individualistic hydrotherapy which is based on the principles of PNF. In this type of therapy, the patient is supported by specific tools for floating, and the therapist applies resistance against the active movements of the patient [11].
Despite the evidences on the positive effects of hydrotherapy on children with cerebral palsy, it is still not standardized for use in Iran. It is expected that review and representation of the related resources may help in creation of a clinical guideline for its implementation in the said country. Due to the presence of a wide variety of hydrotherapy based methods and multifactorial investigation of its results on various types of cerebral palsy, it was thought that an integrative review of the varieties of hydrotherapy and their application on ICF of children with spastic diplegia cerebral palsy. The present study encompassed the analysis of the related manuscripts published between 2000 and 2016.
2. Methods
In this study, integrative review method was used. Integrative studies are the most extensive review studies that simultaneously allow empirical and non-empirical studies so as to achieve a full understanding of a phenomenon. Integrative studies can also combine data from theoretical studies as well as experimental studies with each other. In addition, integrative studies combine a wide range of purposes, including the definition of concepts, review of theories, review of the evidence and methodological analysis of a specific title [12]. For this study, Cooper’s strategy in the integrated review was used. The strategy includes the following: 1. Formulation of the problem, 2. Reviewing the evidences and providing required resources, 3. Evaluating the data, 4. Data analysis and 5. Publication of results. In this regard, Hosseini and colleagues have written an article on such integrated reviews [12]. Given the type of study and pyramid of evidence, the level of evidence was determined.
Formulation of the problem
Hydrotherapy is one of the most useful therapies applicable for the rehabilitation of children with neurodevelopmental disorders and improving their physiological and psychological achievements [1]. However, previous studies based on growth levels of children with cerebral palsy showed that there exist many doubts regarding the effectiveness of hydrotherapy. Therefore, before the use of hydrotherapy as a treatment measure among children with cerebral palsy is promoted, it is essential to answer the prevailing question “which hydrotherapy method, in what conditions, for which group of children and with what function level shall be used?” Therefore, the aim of this study was to investigate the effects of hydrotherapy on spastic diplegia cerebral palsy patients.
The main question of the study included the following: 1) How is the method of hydrotherapy for children with spastic diplegia cerebral palsy in the available literature?; 2) What are the specified effects of hydrotherapy on spastic diplegia cerebral palsy patients with different levels of motor development?; 3) What are the results of hydrotherapy based on the ICF?; and 4) What are the most important factors that influence the effectiveness of hydrotherapy in children with cerebral palsy?
Review of the literature and providing the required evidence
The present study encompassed a search for the information and theoretical foundations related to the application of hydrotherapy in children with cerebral palsy. It also involved the identification of effective conditions and factors that influence the outcome of the therapy and how they were dependent on the growth levels and types of hydrotherapy. This information was identified from the related sites, internet search as well as manual search in databases and reference books.
All articles related to the effects of hydrotherapy on patients with spastic diplegia cerebral palsy were investigated in following Iranian and foreign databases: OTDBASE Occupational Therapy Journal Literature Search Service; PEDRO; OT SEARCH (FORMERLY OT BIBSYS; CINAHL Database; Science Direct; Pub med; Elsevier; Scientific Information Database (SID); Magiran; and Google scholar.
Keywords used in the search process included the following: Cerebral palsy, diplegic spastic, rehabilitation, occupational therapy, hydrotherapy, aquatic therapy, water treatment and water exercises.
The obtained articles were examined on the basis of multidimensional factors, such as: purpose statements, inclusion criteria, characteristics of the research, citation of previous reviews, criticism of previous reviews, presentation of preliminary research findings, methods of analysis of the results, discussion of methodological problems, effective systematic searches, interpretation of results and tables. To interpret the collected data, cases based on the following specifications were used: study type, used models and tools, number of samples, date of publication and the number of papers used in this article.
Samples
A total of 33 papers based on the effects of hydrotherapy in patients with cerebral palsy were selected for this study. After careful examination of the title, abstract and full-text of articles, and the methods of study employed, 22 articles were excluded from the study due to non-relevance to the subject, being repeated in two or several databases, and poor or unrelated relevance to study aims. Finally, 11 articles were found to suffice the inclusion criteria and were hence included in the present study. Finally, the full-text of the articles were reviewed by the researchers.
Inclusion criteria were: 1) Articles based on spastic diplegia cerebral palsy in children in the age group of 4 to 21 years; 2) Summary or the full-text content of the article in Farsi and English languages; 3) Being published within the period 2000 to 2016; 4) Based on the evaluation of the effect of hydrotherapy in the domain of ICF; and 5) Investigation of hydrotherapy interventions alone or in addition to routine treatment methods.
Exclusion criteria were: 1) Articles that do not include a description of the intervention in full detail; and 2) Articles that investigated hydrotherapy with other non-occupational therapy and physiotherapy.
Data evaluation
The extracted data were prioritized according to the type and methods of study. The review section included descriptive content analysis of the collected data and was formulated based on the type and purpose of the study, the number and profile of participants, type and performing the intervention in terms of the time and number of sessions, assessment tools and the results. The findings were gathered without personal judgment and were arranged according to the order in which they were provided to the experts. Articles that met the inclusion criteria on the basis of the pyramid of evidence included systematic reviews (6 articles), randomized clinical trials (4 papers), pilot study (1 article) and case report (1 article).
Data analysis
At this point, the results of all reviewed articles were summed up and classified based on the ICF domains.
Body function and structure
In this area of the ICF, ten articles were found, and their results were related to the structure and function of the body. They investigated the effect of hydrotherapy on variables such as gross motor function, flexibility, balance, respiratory capacity, the function of heart, vessels and muscles, energy expenditure during walking and range of motion, the results of which are provided separately. The Halliwick method is an effective method for the analysis of gross motor function, balance, flexibility and respiratory capacity of children with cerebral palsy (evidence Level II) [13].
Hydrotherapy program was found to have positive effects on the body function and structure of children and teenagers with cerebral palsy. It can also strengthen the function of heart, vessels and muscles and reduce energy consumption during walking (evidence level I) [3]. Hydrotherapy program (swimming back stroke and crawl stroke) causes a reduction in spasticity of the hip adductors and knee flexors (evidence level II) [14].
Hydrotherapy program was also found to cause significant growth in GMFM, and other parameters relating to walking speed and step length. It was also found to increase strength, range of motion and cardiovascular endurance in children with cerebral palsy who can walk independently (evidence level I) [3]. It was also found that when administered in combination with occupational therapy, hydrotherapy program can help in improvement of gross motor function, particularly at GMFCS level 2 and spastic diplegia type. Hence, it can be used as a substitutional yet safe method of treatment even in children with cerebral palsy or GMFCS level 4 patients whose abilities in performing ground training are limited (evidence level II) [2].
Water aerobics program helps in improving motor skills in children with mild to moderate physical disorders, but it was not found to have any significant effects on the functional strength, balance and aerobic capacity of the patients (level III evidence) [15].
Group hydrotherapy exercises help in improving walking capabilities in cerebral palsy teenagers by establishing compatibility of functions between heart and respiratory system and reducing the rate and number of heartbeat (level II evidence) [7]. The most significant effects of hydrotherapy on cerebral palsy patients include increased focus, muscle strength, balance, increased threshold of touch, starting and keeping eye contact (level I evidence) [16]. Furthermore, hydrotherapy also imposes positive effects on gross motor functions, such as jumping, running and walking (level I evidence) [5]. Application of hydrotherapy exercises along with resistance training was also found to be beneficial in boosting endurance and muscle strength (level I evidence) [8].
Hydrotherapy program leads to growth at all levels of ICF and increases children’s motivation levels (level III evidence) [6]. It was also found to have a positive effect on physical performance and vital capacity and range of motion (level I evidence) [1].
Activity
In this area of the ICF, the results of three articles dealt with the different activities of spastic cerebral palsy children, such as ADL, work performance and consciousness. Group hydrotherapy program was found to have positive impacts on the quality of life of patients with cerebral palsy. It allows them to walk farther distances with less fatigue (level II evidence) [7].
The beneficial effects of hydrotherapy on motor functions cannot be attributed to growth in Activity Daily Living (ADL) and the quality of health of life. (Level III evidence) [6]. Hydrotherapy also impacts the work performance, but they were not found to be more effective than conventional treatments. However, children seem to really enjoy this intervention, it should not be eliminated from occupational therapy interventions. (Level A evidence) [16].
The effect of hydrotherapy on the participation of spastic cerebral palsy children was confirmed in only two papers- (Level I evidence) [3], (level III evidence) [6] and it was further remarked that there is need for further research in this area (level A evidence) [5, 8, 18] (Figure 1).
3. Discussion
This study aimed to investigate various methods of hydrotherapy in children with spastic diplegia cerebral palsy and its impact on their GMFCS performance levels. The study also aimed to implement the results of integrative review and the experts’ critiques for the determination of effects of hydrotherapy on the improvement of various aspects of ICF. Interestingly no relevant evidences of the same were found in articles published
by Iranian researchers. Review of the articles published by foreign researchers indicated the positive impact of water based treatment methods in improving different aspects of ICF in patients with spastic diplegia cerebral palsy. The results so obtained also indicated that the therapeutic effects of the treatment were dependent upon the types of hydrotherapeutic treatment methods. In an effort to find the answer to the question that “which treatment methods and what conditions are more effective for the treatment of various groups of children with spastic diplegia cerebral palsy, the authors integrated the evidences noted with expert opinions.
Environmental factors suitable for implementation
The environmental factors suitable for implementation are water temperature and group/individual practice. In the hydrotherapy program with Halliwick approach, it was indicated that the water temperature should be kept between 33 and 36°C [2]. It was also noted that in water aerobics exercises, water temperature should be between 31 to 32°C [7]. It was observed that group exercises increased the motivation of the children and led to their increased participation. Therefore, group practice provides an attractive environment for relaxation and entertainment during aquatic exercises such as basketball, water polo and volleyball [7].
In addition, group exercising is considered a time efficient method which reduces the duration of treatment and provides better targeted exercises to the children. While doing so, it is essential to ensure that the exercises are in compliance with the standards of the patient such as the ability to perform exercises, level of disability, training experience in hydrotherapy as well as cognitive and social skills [18].
Though group exercising is beneficial, still individual training is recommended for participants who need more practice to perform the tasks and develop problem-solving skills. In addition, simultaneously taking care of groups of children in the water is difficult to manage, especially when there are equipment and work force constraints. Individual practice ensures that the child is properly controlled. Alternatively, the therapist may opt to use both types of the exercises by considering all the above mentioned factors so as to maximize its benefits for the participants [4, 7, 18].
Safety
Ensuring the safety of the participants while doing the hydrotherapy exercises helps in facilitating patient participation and success of training and interventions in children with varying levels of ability to move. Some of the most important safety features that may help in achieving the same include: installation of ramps, lift chairs, stairs and knobs, foam walls, suspension devices and life jackets. Considering the ability of the patient, they must be given glasses, belts and enough swimming equipment to ensure safety [4, 7, 18]. The depth of the pool should be such that the child’s feet should touch the bottom of the pool. It has been observed that large shallow pool encourages the children for running, jumping, walking and enduring other activities [4].
Severity and type of exercises
For cerebral palsy patients, a variety of techniques of hydrotherapy such as Halliwick, aerobic and non-aerobic exercises in water and water games are usually used. They were found to be effective in majority of the articles reviewed in this study and the intensity of each is explained.
The American College of Sports Medicine announced that training session, which involves 8 to 12 times repetition of the exercises that leads the children to the brink of exhaustion, is appropriate for muscle strengthening. Doing aerobic exercise for 30 to 60 minutes every day or most days of the week can help in improving the physical fitness of the children. However, it was suggested by Bar & Row land that the intensity of exercises should be kept between 60 to 70 percent of maximum oxygen uptake, and 70 to 80 percent of heart rate [4]. Furthermore, regular administration of such hydrotherapy interventions for a period of 6-weeks can also improve the gross motor skills of the children [18].
According to the Halliwick approach, hydrotherapy programs should include 5 to 10 minutes of warm up, 40 minutes workout exercises in water and 5 to 10 minutes of cooling back down [2].While doing so, it is recommended that the intensity of resistance training and aerobics exercises in children with GMFCS level 1 and 2 should be above 40 percent of heart rate [18]. Hydrotherapy program traditionally takes place 45 minutes every session, 2 to 3 times a week for 10 to 14 weeks. The gap between such therapy sessions helps in the recovery of the patient by strengthening and increasing the strength of cerebral palsy children (level I and II evidence) [1, 4, 6].
Application of hydrotherapy methods according to the GMFCS levels
Hydrotherapy is known to cause the growth of motor functions and delight of children with spastic cerebral palsy. It has been observed that the growth was more than GMFM-88 (level II evidence) in children with level 2 GMFCS [2]. Most studies suggest that hydrotherapy exercises are useful and effective in children with GMFCS levels 1 to 3. Only one of the studies reported the inclusion of a GMFCS level 4 (level I and II evidence) participant in hydrotherapy study [4, 7, 8, 17, 15, 18].
Results of hydrotherapy
Most reviewed papers on hydrotherapy used aerobic exercises with non-aerobic and strength activities. A program including 12 to 14 weeks of aerobic training, 2 to 3 times per week with motor functional activities such as walking, climbing stairs was found to improve the gross motor skills in children with mild to moderate mental disorders (Level II and III evidence) [2, 6, 15].
Halliwick hydrotherapy programs performed 2 to 3 times per week for an average period of 30 minutes for 12 weeks was found to have positive effects on the gross motor function and enjoyment of physical activity, especially in children with spastic diplegia cerebral palsy and GMFCS 2 levels with activity limitations on the ground. (Level II evidence) [2]. It was also found that administration of a combination of aerobic and strength exercises may increase power and endurance of such children (Level II evidence) [8].
Considering the results obtained from studies on the effect of hydrotherapy on different domains of ICF in cerebral palsy spastic diplegia patients, it was suggested that hydrotherapy based interventions should be recommended as a complementary method of treatment and rehabilitation along with other conventional rehabilitation methods. However, it must also be noted that ethical and cultural considerations of the therapy methods necessitate that the intervention protocols are performed by trained therapists only. It is also recommended to consider the conditions (cognitive and motor ability) of the patients in the domains of ICF before recommending a regimen and estimating its impacts. Doing so is extremely important as it helps maintain the patient’s motivation in performing conventional rehabilitation exercises.
In this study, the researchers were faced with the limitation of lack of Persian literature in the field of effects of hydrotherapy in patients with spastic diplegia cerebral palsy. In addition, in the articles dealing with ICF, less attention was paid to the field of collaboration and evaluation tools, which are proposed to be addressed in future studies.
4. Conclusion
The results of this integrative review showed that hydrotherapy when administered with conventional methods of rehabilitation of children with spastic diplegia cerebral palsy, has positive effects on all areas of ICF. It was concluded that hydrotherapy can be used in children and adolescents. The exercises, and their duration and intensity should be decided on the basis of the physical and cognitive conditions of the patients. However, studies in some areas of ICF were found to be limited. Hence, it was proposed that further studies in this field are highly necessary.
Acknowledgments
This article is extracted from the master's thesis of the first author, Department of occupational therapy, Rehabilitation Faculty, Shahid Beheshti University of Medical Sciences.
Conflict of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]Getz M, Hutzler Y, Vermeer A. Effects of aquatic interventions in children with neuromotor impairments: A systematic review of the literature. Clinical Rehabilitation. 2006; 20(11):927–36. doi: 10.1177/0269215506070693
[2]Lai CJ, Liu WY, Yang TF, Chen CL, Wu CY, Chan RC. Pediatric aquatic therapy on motor function and enjoyment in children diagnosed with cerebral palsy of various motor severities. Journal of Child Neurology. 2014; 30(2):200–8. doi: 10.1177/0883073814535491
[3]Franzen K. Effectiveness of aquatic therapy for children with neurodevelopmental disorders: A systematic review of current literature. Philadelphia: Sage; 2013.
[4]Kelly M, Darrah J. Aquatic exercise for children with cerebral palsy. Developmental Medicine & Child Neurology . 2005; 47(12):838. doi: 10.1017/s0012162205001775
[5]Rogers A, Furler BL, Brinks S, Darrah J. A systematic review of the effectiveness of aerobic exercise interventions for children with cerebral palsy: An AACPDM evidence report. Developmental Medicine & Child Neurology. 2008; 50(11):808–14. doi: 10.1111/j.1469-8749.2008.03134.x6
[6]Retarekar R, Fragala-Pinkham MA, Townsend EL. Effects of aquatic aerobic exercise for a child with cerebral palsy: Single-subject design. Pediatric Physical Therapy. 2009; 21(4):336–44. doi: 10.1097/pep.0b013e3181beb039
[7]Ballaz L, Plamondon S, Lemay M. Group aquatic training improves gait efficiency in adolescents with cerebral palsy. Disability and Rehabilitation. 2011; 33(17-18):1616–24. doi: 10.3109/09638288.2010.541544
[8]Gorter JW, Currie SJ. Aquatic exercise programs for children and adolescents with cerebral palsy: What do we know and where do we go? International Journal of Pediatrics. 2011; 2011:1–7. doi: 10.1155/2011/712165
[9]Ainslie T. The concise guide to physiotherapy. Volume 1. Assessment: Elsevier Health Sciences; 2012.
[10]Schoedinger P. Potential risks when utilizing Watsu D. Watsu in aquatic rehabiltiation. In: Cole AJ, Becker BE, editors. Comprehen-sive Aquatic Therapy. Washington: Washington State University Publishing 2011.
[11]Lambeck J, Gamper U. Water Specific Therapy_Halliwick [Internet]. 2016 [Updated 2016 February 4]. Available from: http://www.inertiatherapy.com/wp-content/uploads/2016/02/4.-WST-2015.pdf
[12]Shafiee Z, Hosseini MA, Rassafiani M, Rezaee M. Effects of Constraint-Induced Movement Therapy (CIMT) on improvement of upper-limb and hand function in stroke patients: an integrative review. Journal of Rehabilitation Medicine. 2013; 2(3):52-61.
[13]Hou X, Fen Y, Ma Z, Wu Y, Tian X. The effect of adapted aquatic activity for children with cerebral palsy in school age. Paper Presented at: The International sports science conference in commemoration of Seoul Olympics. 6 October 2015; Seoul, South Korea.
[14]Chrysagis N, Douka A, Nikopoulos M, Apostolopoulou F, Koutsouki D. Effects of an aquatic program on gross motor functionof children with spastic cerebral palsy. Journal Biology of Exercise. 2009; 5(2):13-25 . doi: 10.4127/jbe.2009.0027
[15]Fragala-Pinkham MA, Smith HJ, Lombard KA, Barlow C, O’Neil ME. Aquatic aerobic exercise for children with cerebral palsy: A pilot intervention study. Physiotherapy Theory and Practice. 2013; 30(2):69–78. doi: 10.3109/09593985.2013.825825
[16]Wittmer H, Maki J. Efficacy of aquatic therapy: A systematic literature review [PhD dissertation]. Duluth, Minnesota: College of St. Scholastica; 2013.
[17]Dimitrijević L, Aleksandrović M, Madić D, Okičić T, Radovanović D, Daly D. The effect of aquatic intervention on the gross motor function and aquatic skills in children with cerebral palsy. Journal of Human Kinetics. 2012; 32(1):167-174. doi: 10.2478/v10078-012-0033-5.
[18]Sutthibuta U. Systematic Review of aquatic exercise programming for children and adolescents with cerebral palsy. International Journal of Child Development and Mental Health. 2014; 2(1):49-66.
Environmental factors suitable for implementation
The environmental factors suitable for implementation are water temperature and group/individual practice. In the hydrotherapy program with Halliwick approach, it was indicated that the water temperature should be kept between 33 and 36°C [2]. It was also noted that in water aerobics exercises, water temperature should be between 31 to 32°C [7]. It was observed that group exercises increased the motivation of the children and led to their increased participation. Therefore, group practice provides an attractive environment for relaxation and entertainment during aquatic exercises such as basketball, water polo and volleyball [7].
In addition, group exercising is considered a time efficient method which reduces the duration of treatment and provides better targeted exercises to the children. While doing so, it is essential to ensure that the exercises are in compliance with the standards of the patient such as the ability to perform exercises, level of disability, training experience in hydrotherapy as well as cognitive and social skills [18].
Though group exercising is beneficial, still individual training is recommended for participants who need more practice to perform the tasks and develop problem-solving skills. In addition, simultaneously taking care of groups of children in the water is difficult to manage, especially when there are equipment and work force constraints. Individual practice ensures that the child is properly controlled. Alternatively, the therapist may opt to use both types of the exercises by considering all the above mentioned factors so as to maximize its benefits for the participants [4, 7, 18].
Safety
Ensuring the safety of the participants while doing the hydrotherapy exercises helps in facilitating patient participation and success of training and interventions in children with varying levels of ability to move. Some of the most important safety features that may help in achieving the same include: installation of ramps, lift chairs, stairs and knobs, foam walls, suspension devices and life jackets. Considering the ability of the patient, they must be given glasses, belts and enough swimming equipment to ensure safety [4, 7, 18]. The depth of the pool should be such that the child’s feet should touch the bottom of the pool. It has been observed that large shallow pool encourages the children for running, jumping, walking and enduring other activities [4].
Severity and type of exercises
For cerebral palsy patients, a variety of techniques of hydrotherapy such as Halliwick, aerobic and non-aerobic exercises in water and water games are usually used. They were found to be effective in majority of the articles reviewed in this study and the intensity of each is explained.
The American College of Sports Medicine announced that training session, which involves 8 to 12 times repetition of the exercises that leads the children to the brink of exhaustion, is appropriate for muscle strengthening. Doing aerobic exercise for 30 to 60 minutes every day or most days of the week can help in improving the physical fitness of the children. However, it was suggested by Bar & Row land that the intensity of exercises should be kept between 60 to 70 percent of maximum oxygen uptake, and 70 to 80 percent of heart rate [4]. Furthermore, regular administration of such hydrotherapy interventions for a period of 6-weeks can also improve the gross motor skills of the children [18].
According to the Halliwick approach, hydrotherapy programs should include 5 to 10 minutes of warm up, 40 minutes workout exercises in water and 5 to 10 minutes of cooling back down [2].While doing so, it is recommended that the intensity of resistance training and aerobics exercises in children with GMFCS level 1 and 2 should be above 40 percent of heart rate [18]. Hydrotherapy program traditionally takes place 45 minutes every session, 2 to 3 times a week for 10 to 14 weeks. The gap between such therapy sessions helps in the recovery of the patient by strengthening and increasing the strength of cerebral palsy children (level I and II evidence) [1, 4, 6].
Application of hydrotherapy methods according to the GMFCS levels
Hydrotherapy is known to cause the growth of motor functions and delight of children with spastic cerebral palsy. It has been observed that the growth was more than GMFM-88 (level II evidence) in children with level 2 GMFCS [2]. Most studies suggest that hydrotherapy exercises are useful and effective in children with GMFCS levels 1 to 3. Only one of the studies reported the inclusion of a GMFCS level 4 (level I and II evidence) participant in hydrotherapy study [4, 7, 8, 17, 15, 18].
Results of hydrotherapy
Most reviewed papers on hydrotherapy used aerobic exercises with non-aerobic and strength activities. A program including 12 to 14 weeks of aerobic training, 2 to 3 times per week with motor functional activities such as walking, climbing stairs was found to improve the gross motor skills in children with mild to moderate mental disorders (Level II and III evidence) [2, 6, 15].
Halliwick hydrotherapy programs performed 2 to 3 times per week for an average period of 30 minutes for 12 weeks was found to have positive effects on the gross motor function and enjoyment of physical activity, especially in children with spastic diplegia cerebral palsy and GMFCS 2 levels with activity limitations on the ground. (Level II evidence) [2]. It was also found that administration of a combination of aerobic and strength exercises may increase power and endurance of such children (Level II evidence) [8].
Considering the results obtained from studies on the effect of hydrotherapy on different domains of ICF in cerebral palsy spastic diplegia patients, it was suggested that hydrotherapy based interventions should be recommended as a complementary method of treatment and rehabilitation along with other conventional rehabilitation methods. However, it must also be noted that ethical and cultural considerations of the therapy methods necessitate that the intervention protocols are performed by trained therapists only. It is also recommended to consider the conditions (cognitive and motor ability) of the patients in the domains of ICF before recommending a regimen and estimating its impacts. Doing so is extremely important as it helps maintain the patient’s motivation in performing conventional rehabilitation exercises.
In this study, the researchers were faced with the limitation of lack of Persian literature in the field of effects of hydrotherapy in patients with spastic diplegia cerebral palsy. In addition, in the articles dealing with ICF, less attention was paid to the field of collaboration and evaluation tools, which are proposed to be addressed in future studies.
4. Conclusion
The results of this integrative review showed that hydrotherapy when administered with conventional methods of rehabilitation of children with spastic diplegia cerebral palsy, has positive effects on all areas of ICF. It was concluded that hydrotherapy can be used in children and adolescents. The exercises, and their duration and intensity should be decided on the basis of the physical and cognitive conditions of the patients. However, studies in some areas of ICF were found to be limited. Hence, it was proposed that further studies in this field are highly necessary.
Acknowledgments
This article is extracted from the master's thesis of the first author, Department of occupational therapy, Rehabilitation Faculty, Shahid Beheshti University of Medical Sciences.
Conflict of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]Getz M, Hutzler Y, Vermeer A. Effects of aquatic interventions in children with neuromotor impairments: A systematic review of the literature. Clinical Rehabilitation. 2006; 20(11):927–36. doi: 10.1177/0269215506070693
[2]Lai CJ, Liu WY, Yang TF, Chen CL, Wu CY, Chan RC. Pediatric aquatic therapy on motor function and enjoyment in children diagnosed with cerebral palsy of various motor severities. Journal of Child Neurology. 2014; 30(2):200–8. doi: 10.1177/0883073814535491
[3]Franzen K. Effectiveness of aquatic therapy for children with neurodevelopmental disorders: A systematic review of current literature. Philadelphia: Sage; 2013.
[4]Kelly M, Darrah J. Aquatic exercise for children with cerebral palsy. Developmental Medicine & Child Neurology . 2005; 47(12):838. doi: 10.1017/s0012162205001775
[5]Rogers A, Furler BL, Brinks S, Darrah J. A systematic review of the effectiveness of aerobic exercise interventions for children with cerebral palsy: An AACPDM evidence report. Developmental Medicine & Child Neurology. 2008; 50(11):808–14. doi: 10.1111/j.1469-8749.2008.03134.x6
[6]Retarekar R, Fragala-Pinkham MA, Townsend EL. Effects of aquatic aerobic exercise for a child with cerebral palsy: Single-subject design. Pediatric Physical Therapy. 2009; 21(4):336–44. doi: 10.1097/pep.0b013e3181beb039
[7]Ballaz L, Plamondon S, Lemay M. Group aquatic training improves gait efficiency in adolescents with cerebral palsy. Disability and Rehabilitation. 2011; 33(17-18):1616–24. doi: 10.3109/09638288.2010.541544
[8]Gorter JW, Currie SJ. Aquatic exercise programs for children and adolescents with cerebral palsy: What do we know and where do we go? International Journal of Pediatrics. 2011; 2011:1–7. doi: 10.1155/2011/712165
[9]Ainslie T. The concise guide to physiotherapy. Volume 1. Assessment: Elsevier Health Sciences; 2012.
[10]Schoedinger P. Potential risks when utilizing Watsu D. Watsu in aquatic rehabiltiation. In: Cole AJ, Becker BE, editors. Comprehen-sive Aquatic Therapy. Washington: Washington State University Publishing 2011.
[11]Lambeck J, Gamper U. Water Specific Therapy_Halliwick [Internet]. 2016 [Updated 2016 February 4]. Available from: http://www.inertiatherapy.com/wp-content/uploads/2016/02/4.-WST-2015.pdf
[12]Shafiee Z, Hosseini MA, Rassafiani M, Rezaee M. Effects of Constraint-Induced Movement Therapy (CIMT) on improvement of upper-limb and hand function in stroke patients: an integrative review. Journal of Rehabilitation Medicine. 2013; 2(3):52-61.
[13]Hou X, Fen Y, Ma Z, Wu Y, Tian X. The effect of adapted aquatic activity for children with cerebral palsy in school age. Paper Presented at: The International sports science conference in commemoration of Seoul Olympics. 6 October 2015; Seoul, South Korea.
[14]Chrysagis N, Douka A, Nikopoulos M, Apostolopoulou F, Koutsouki D. Effects of an aquatic program on gross motor functionof children with spastic cerebral palsy. Journal Biology of Exercise. 2009; 5(2):13-25 . doi: 10.4127/jbe.2009.0027
[15]Fragala-Pinkham MA, Smith HJ, Lombard KA, Barlow C, O’Neil ME. Aquatic aerobic exercise for children with cerebral palsy: A pilot intervention study. Physiotherapy Theory and Practice. 2013; 30(2):69–78. doi: 10.3109/09593985.2013.825825
[16]Wittmer H, Maki J. Efficacy of aquatic therapy: A systematic literature review [PhD dissertation]. Duluth, Minnesota: College of St. Scholastica; 2013.
[17]Dimitrijević L, Aleksandrović M, Madić D, Okičić T, Radovanović D, Daly D. The effect of aquatic intervention on the gross motor function and aquatic skills in children with cerebral palsy. Journal of Human Kinetics. 2012; 32(1):167-174. doi: 10.2478/v10078-012-0033-5.
[18]Sutthibuta U. Systematic Review of aquatic exercise programming for children and adolescents with cerebral palsy. International Journal of Child Development and Mental Health. 2014; 2(1):49-66.

Article type: Reviews |
Subject:
Occupational therapy
Received: 2017/02/10 | Accepted: 2017/05/1 | Published: 2017/08/1
Received: 2017/02/10 | Accepted: 2017/05/1 | Published: 2017/08/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
