
988368
Fri, Apr 19, 2024

Volume 15, Issue 3 (September 2017)
Iranian Rehabilitation Journal 2017, 15(3): 193-198 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Massah O, Effatpanah M, Shishehgar S. Matrix Model for Methamphetamine Dependence Among Iranian Female Methadone Patients: The First Report From the Most Populated Persian Gulf Country. Iranian Rehabilitation Journal 2017; 15 (3) :193-198
URL: http://irj.uswr.ac.ir/article-1-768-en.html
URL: http://irj.uswr.ac.ir/article-1-768-en.html


1- Substance Abuse and Dependence Research Center, University of Social Welfare & Rehabilitation Sciences, Tehran, Iran
2- Department of Medicine, School of Medicine, Ziaeian Hospital, International Campus, Tehran University of Medical Sciences, Tehran, Iran.
3- Faculty of Health, University of Technology Sydney, Sydney, Australia.
2- Department of Medicine, School of Medicine, Ziaeian Hospital, International Campus, Tehran University of Medical Sciences, Tehran, Iran.
3- Faculty of Health, University of Technology Sydney, Sydney, Australia.
Full-Text [PDF 513 kb]
(2502 Downloads)
| Abstract (HTML) (6805 Views)

Full-Text: (1687 Views)
1. Introduction
After cannabis, Methamphetamine (MA) is the most widely used illicit drug in the world [1]. Globally, in 2012, between 162 million (3.5%) and 324 million (7%) people aged 15–64 reported using an illicit drug, mainly cannabis, heroin, cocaine or MA at least once in the previous year [2]. Iran (Persia) is a vast Persian-speaking country in Western Asia. Drug-dependent people in Iran are the traditional users of opium [3, 4]. This is because of Afghanistan, the former part of Iran which produces opium and smuggles opium to Iran on a large scale [3, 4].
As the most populous Persian Gulf country, in Iran, MA dependence has recently become a new health problem among methadone patients [5, 6]. Because of stimulant effects, MA is abused to increase sexual desire and physical energy among methadone patients [7]. MA dependence is associated with physical and psychological harms among methadone patients [8, 9].
There is no pharmacological treatment [10]. Psychosocial treatments such as the Matrix Model are the main treatment modality [11]. The Matrix Model is a sixteen week psychosocial treatment that provides a framework for engaging MA-dependent patients in treatment and helping them achieve abstinence. Patients learn about issues critical to dependence and relapse, receive direction and support from a well-trained psychotherapist, and become familiar with self-help programs. Clients are monitored for MA dependence through taking urine testing [12].
The psychotherapist functions simultaneously as teacher and direct, fostering a positive, encouraging relationship with the MA-dependent patient and using that relationship to reinforce positive behavior change. The interaction between the psychotherapist and the client is authentic and direct but not confrontational. Psychotherapists are well-trained to direct treatment sessions in a way that increases the patient’s self-esteem, dignity, and self-worth. A positive relationship between client and psychotherapist is important to patient retention [13].
Treatment materials draw heavily on other evaluated treatment interventions and, thus, include elements of relapse prevention, drug education, family and group therapies, and self-help participation. Detailed treatment manuals include worksheets for individual sessions; other components include social support groups, 12-step programs, family education groups, relapse prevention groups, early recovery skills groups, combined sessions, urine tests, and relapse analysis [14].
A number of research studies have shown that participants treated using the Matrix Model have statistically significant reductions in drug dependence, improvements in psychological status, and reduced risky sexual behaviors associated with HIV problem [12-14]. However, when it comes to Iran, to date, there are no studies of the Matrix Model and MA dependence. The current research is the first study that aimed to explore the self-perceived problems associated with the Matrix Model among a group of Persian women with MA dependence in methadone treatment.
2. Methods
Study settings and design
The qualitative methodology was selected for conducting this study because of the lack of research on the Matrix Model in Iran. The whole study procedure was conducted based on the Grounded Theory of Strauss and Corbin [15]. The study settings were 12 large methadone treatment services in Tehran, Iran. Four study sites were women-only services. All clinics were situated in middle class areas of Tehran.
Participants and the inclusion criteria
All women were eligible to participate in the study if they 1) were at least 18 years old and 2) were dependent on MA in methadone treatment based on the DSM-IV.TR criteria. Self-report of MA dependence by each participant was re-checked with the manager of each study site. Participants needed to be in methadone treatment for at least one months and report receiving the Matrix Model for MA dependence at the time of recruitment. Exclusion criteria included reporting severe drug-related symptoms and/or psychiatric problems which were likely to impact on interviewing procedures.
This qualitative study recruited a group of 42 women enrolled in methadone treatment in October 2015. Interviews with a range of ten health professionals involved in methadone or the Matrix Model were conducted. Based on the Ground Theory of Strauss and Corbin, sample taking continued until no new theme emerged in four consecutive interviews [15, 16]. The ten health professionals who participated in the study included three clinical psychologists, two medical doctors, three site managers and two social workers. All health professionals had at least seven years of experience in working with women with MA dependence in methadone treatment services.Study procedures
In-depth and face-to-face interviews were conducted after the purpose of the study was fully explained. Interviews were conducted in private interview rooms at the methadone centres in October 2015. Interviews took 45-60 minutes and were audio-taped with prior permission from each interviewee. Semi-structured interviews were constructed around a set of core issues. All participants (women and health professionals) were asked about their self-perceived experiences with the Matrix Model, the most important problems that they had and suggestions to manage the problems.
Qualitative data analyses
The qualitative content analysis and thematic approach were used to analyze the data. Interviews were transcribed verbatim. Interview transcripts were primary sources and were translated from the Persian language to the English language for further analysis. The methodological approach was inductive in which themes were derived from empirical data, impacted by discourse analysis and grounded theory [15]. We classified the problems associated with the Matrix Model in methadone clinics into this framework to present the hierarchy and interrelatedness of the findings. All data were reviewed for accuracy. Data summaries were presented to each author for discussing. Data interpretation was done until consensus was reached. Data were imported into Atlas-ti software (version 9) for qualitative management and coding.
Ethical approvals
All women signed consent forms. Both women and staff were informed that participation was confidential and voluntary. The study was approved by the Human Research Ethic Committee of the Tehran University of Medical Sciences. Women were reimbursed $ 12 for time and study participation. Both women and health professionals were informed that the lack of participants would not have any impact on either their methadone treatment or their professional relationships.
3. Results
Baseline characteristics
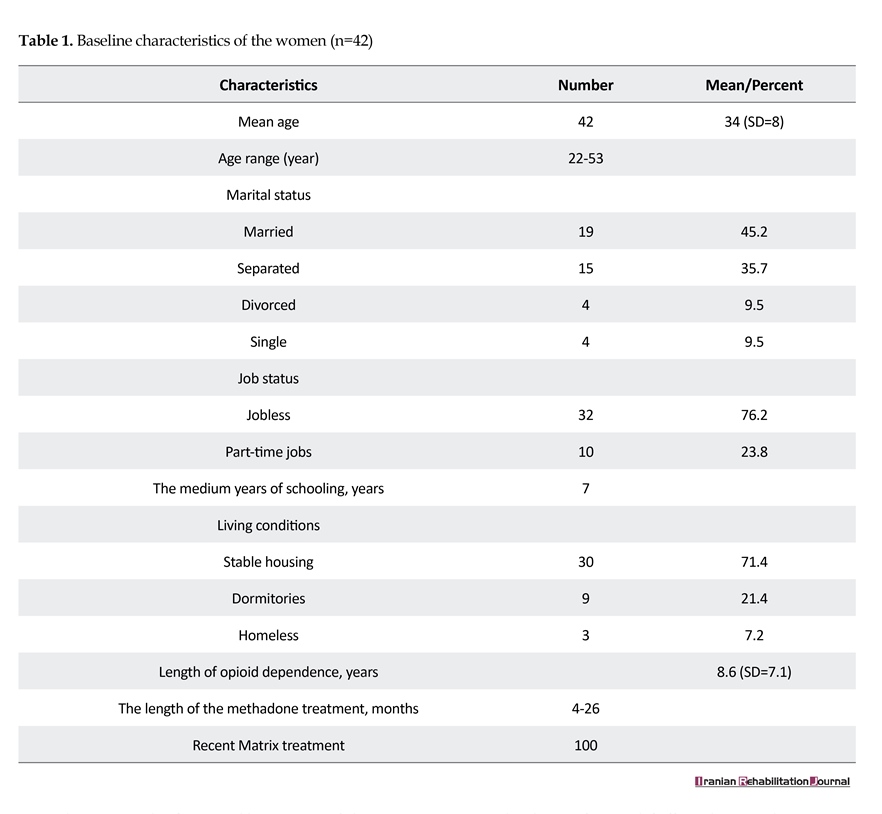
Forty two women participated in the study. The mean age of the women was 34 (SD=8) years (age range: 22-53 years). Most women (n=19) were married and the remaining women were separated (n=15), divorced (n=4) or single (n=4) at the time of interviewing. Overall, 32 participants were jobless and 10 participants had part-time jobs. The medium years of schooling were seven years. Overall, 30 participants reported stable housing while the remaining participants reported living in dormitories (n=9) or being homeless (n=3) at the time of interviewing. Length of opioid dependence was 8.6 (SD=7.1) years. The length of the methadone treatment ranged between 4 and 26 months. All participants were in the Matrix Model at the time of interviewing (Table 1).
Problems associated with the Matrix Model in methadone treatment
The problems associated with the provision of the Matrix Model have been listed below as emerged in the narratives of the women and health professionals.
The long length of the Matrix Model
A theme that gradually emerged from the narratives indicated that the Matrix Model is long. All participants believed that the Matrix Model was able to manage MA craving and relapse in them. However, the long length of the treatment made some women felt tired or disappointed. Therefore, they did not have enough motivation to continue the treatment. More than half of the women and more than half of the health professionals reported this problem. The quotes below can explain this issue better:
ʻ... I like the Matrix Model because it reduces my craving and relapse but sometime I feel I can’t continue the treatment because it is very long…ʼ (a 33 year-old woman).
ʻ… The Matrix Model is a very good intervention but it is very long so some women feel tired and bored. We need to make the treatment shorter or bring brief interventions to the clinic ...ʼ (a clinical psychologist).
Lack of cost-effectiveness
A theme that gradually emerged from the narratives indicated that the Matrix Model was not cost-effective. Participants frequently explained that the treatment was at least 16 weekly sessions and the cost was a main problem. Participants reported that the Matrix Model can successfully manage MA craving and relapse. However, the price was the problem. Half of the women and half of health professionals reported this problem. The quotes below can explain this issue better:
ʻ... The Matrix Model can manage MA craving and relapse in me but it is expensive. I can’t pay for that. Most women can’t pay ...ʼ (a 28 year-old woman).
After cannabis, Methamphetamine (MA) is the most widely used illicit drug in the world [1]. Globally, in 2012, between 162 million (3.5%) and 324 million (7%) people aged 15–64 reported using an illicit drug, mainly cannabis, heroin, cocaine or MA at least once in the previous year [2]. Iran (Persia) is a vast Persian-speaking country in Western Asia. Drug-dependent people in Iran are the traditional users of opium [3, 4]. This is because of Afghanistan, the former part of Iran which produces opium and smuggles opium to Iran on a large scale [3, 4].
As the most populous Persian Gulf country, in Iran, MA dependence has recently become a new health problem among methadone patients [5, 6]. Because of stimulant effects, MA is abused to increase sexual desire and physical energy among methadone patients [7]. MA dependence is associated with physical and psychological harms among methadone patients [8, 9].
There is no pharmacological treatment [10]. Psychosocial treatments such as the Matrix Model are the main treatment modality [11]. The Matrix Model is a sixteen week psychosocial treatment that provides a framework for engaging MA-dependent patients in treatment and helping them achieve abstinence. Patients learn about issues critical to dependence and relapse, receive direction and support from a well-trained psychotherapist, and become familiar with self-help programs. Clients are monitored for MA dependence through taking urine testing [12].
The psychotherapist functions simultaneously as teacher and direct, fostering a positive, encouraging relationship with the MA-dependent patient and using that relationship to reinforce positive behavior change. The interaction between the psychotherapist and the client is authentic and direct but not confrontational. Psychotherapists are well-trained to direct treatment sessions in a way that increases the patient’s self-esteem, dignity, and self-worth. A positive relationship between client and psychotherapist is important to patient retention [13].
Treatment materials draw heavily on other evaluated treatment interventions and, thus, include elements of relapse prevention, drug education, family and group therapies, and self-help participation. Detailed treatment manuals include worksheets for individual sessions; other components include social support groups, 12-step programs, family education groups, relapse prevention groups, early recovery skills groups, combined sessions, urine tests, and relapse analysis [14].
A number of research studies have shown that participants treated using the Matrix Model have statistically significant reductions in drug dependence, improvements in psychological status, and reduced risky sexual behaviors associated with HIV problem [12-14]. However, when it comes to Iran, to date, there are no studies of the Matrix Model and MA dependence. The current research is the first study that aimed to explore the self-perceived problems associated with the Matrix Model among a group of Persian women with MA dependence in methadone treatment.
2. Methods
Study settings and design
The qualitative methodology was selected for conducting this study because of the lack of research on the Matrix Model in Iran. The whole study procedure was conducted based on the Grounded Theory of Strauss and Corbin [15]. The study settings were 12 large methadone treatment services in Tehran, Iran. Four study sites were women-only services. All clinics were situated in middle class areas of Tehran.
Participants and the inclusion criteria
All women were eligible to participate in the study if they 1) were at least 18 years old and 2) were dependent on MA in methadone treatment based on the DSM-IV.TR criteria. Self-report of MA dependence by each participant was re-checked with the manager of each study site. Participants needed to be in methadone treatment for at least one months and report receiving the Matrix Model for MA dependence at the time of recruitment. Exclusion criteria included reporting severe drug-related symptoms and/or psychiatric problems which were likely to impact on interviewing procedures.
This qualitative study recruited a group of 42 women enrolled in methadone treatment in October 2015. Interviews with a range of ten health professionals involved in methadone or the Matrix Model were conducted. Based on the Ground Theory of Strauss and Corbin, sample taking continued until no new theme emerged in four consecutive interviews [15, 16]. The ten health professionals who participated in the study included three clinical psychologists, two medical doctors, three site managers and two social workers. All health professionals had at least seven years of experience in working with women with MA dependence in methadone treatment services.Study procedures
In-depth and face-to-face interviews were conducted after the purpose of the study was fully explained. Interviews were conducted in private interview rooms at the methadone centres in October 2015. Interviews took 45-60 minutes and were audio-taped with prior permission from each interviewee. Semi-structured interviews were constructed around a set of core issues. All participants (women and health professionals) were asked about their self-perceived experiences with the Matrix Model, the most important problems that they had and suggestions to manage the problems.
Qualitative data analyses
The qualitative content analysis and thematic approach were used to analyze the data. Interviews were transcribed verbatim. Interview transcripts were primary sources and were translated from the Persian language to the English language for further analysis. The methodological approach was inductive in which themes were derived from empirical data, impacted by discourse analysis and grounded theory [15]. We classified the problems associated with the Matrix Model in methadone clinics into this framework to present the hierarchy and interrelatedness of the findings. All data were reviewed for accuracy. Data summaries were presented to each author for discussing. Data interpretation was done until consensus was reached. Data were imported into Atlas-ti software (version 9) for qualitative management and coding.
Ethical approvals
All women signed consent forms. Both women and staff were informed that participation was confidential and voluntary. The study was approved by the Human Research Ethic Committee of the Tehran University of Medical Sciences. Women were reimbursed $ 12 for time and study participation. Both women and health professionals were informed that the lack of participants would not have any impact on either their methadone treatment or their professional relationships.
3. Results
Baseline characteristics
Forty two women participated in the study. The mean age of the women was 34 (SD=8) years (age range: 22-53 years). Most women (n=19) were married and the remaining women were separated (n=15), divorced (n=4) or single (n=4) at the time of interviewing. Overall, 32 participants were jobless and 10 participants had part-time jobs. The medium years of schooling were seven years. Overall, 30 participants reported stable housing while the remaining participants reported living in dormitories (n=9) or being homeless (n=3) at the time of interviewing. Length of opioid dependence was 8.6 (SD=7.1) years. The length of the methadone treatment ranged between 4 and 26 months. All participants were in the Matrix Model at the time of interviewing (Table 1).
Problems associated with the Matrix Model in methadone treatment
The problems associated with the provision of the Matrix Model have been listed below as emerged in the narratives of the women and health professionals.
The long length of the Matrix Model
A theme that gradually emerged from the narratives indicated that the Matrix Model is long. All participants believed that the Matrix Model was able to manage MA craving and relapse in them. However, the long length of the treatment made some women felt tired or disappointed. Therefore, they did not have enough motivation to continue the treatment. More than half of the women and more than half of the health professionals reported this problem. The quotes below can explain this issue better:
ʻ... I like the Matrix Model because it reduces my craving and relapse but sometime I feel I can’t continue the treatment because it is very long…ʼ (a 33 year-old woman).
ʻ… The Matrix Model is a very good intervention but it is very long so some women feel tired and bored. We need to make the treatment shorter or bring brief interventions to the clinic ...ʼ (a clinical psychologist).
Lack of cost-effectiveness
A theme that gradually emerged from the narratives indicated that the Matrix Model was not cost-effective. Participants frequently explained that the treatment was at least 16 weekly sessions and the cost was a main problem. Participants reported that the Matrix Model can successfully manage MA craving and relapse. However, the price was the problem. Half of the women and half of health professionals reported this problem. The quotes below can explain this issue better:
ʻ... The Matrix Model can manage MA craving and relapse in me but it is expensive. I can’t pay for that. Most women can’t pay ...ʼ (a 28 year-old woman).
ʻ... There are at least 16 weekly sessions of the Matrix Model. We need to pay a lot to our psychologist so patients should be able to pay ... . I believe we should also provide brief interventions to reduce the cost …ʼ (a methadone clinic manager).
Intensive staff training
A theme that gradually emerged from the narratives indicated that the Matrix Model needed intensive staff training. Participants frequently reported that the Matrix Model plays an important role in the treatment of MA dependence. However, it is manaulised and professional so psychologists who provide the treatment should be professional. A quarter of women and half of the health professionals reported that intensive staff training was a main problem in methadone clinics. The quotes below can explain this issue better:
ʻ... My psychologist plays an important role in my recovery because she is professional. But the Matrix Model is manualized so professional staff are the main the points …ʼ (a 36-year old woman).
ʻ... The Matrix Model needs intensive staff training because it is a professional and manualized treatment so your staff should be well-trained and experienced ... . Brief intervention do not have this problem …ʼ (a medical doctor).
An inadequate coverage of the Matrix Model
A theme that gradually emerged from the narratives indicated that the Matrix Model was not widely available every patient in methadone treatment services. Participants frequently reported that clinical psychologists in the methadone clinics did not have enough time for each patient. Therefore, the coverage of the treatment was inadequate for many women preventing treating MA dependence among them. A quarter of women and quarter of health professionals reported that the coverage of the Matrix Model was inadequate. The quotes below can explain this issue better:
ʻ... The Matrix Model is manualized and everybody cannot use this treatment. The psychologists in the methadone clinics cannot spend time on each patient. They are lots of patients who are dependent on MA …ʼ (a 38-year old woman).
ʻ... The Matrix Model is a very good treatment but psychologists do not have enough time for each patient because the Matrix Model is very comprehensive so everybody cannot benefit from the treatment. We need brief interventions ...ʼ (a methadone clinic manager).
4. Discussion
MA dependence is a health problem among female methadone patients in Iran [7]. However, there are few studies of this group in Iran. In recent years, the Matrix Model of Intensive Outpatient Treatment has been provided in methadone treatment services to treat MA dependence [7]. However, to date, it is not documented what problems are associated with the provision of the Matrix Model. This issue is important because MA dependence needs an immediate treatment [5, 7].
The study results indicated that the Matrix Model was long. Studies indicate that the length of the treatment is a concern for many drug-dependent patients [17]. Women should be informed that the duration of the Matrix Model is needed for their treatment and recovery procedure is not a short issue. Women should be informed that the Matrix Model can lead to craving management and relapse prevention [11]. Furthermore, brief interventions should be evaluated to address this problem. Further studies are suggested to assess the relationship between the length of the treatment and treating MA dependence among this group.
The study results indicated that the Matrix Model was not cost-effective for many participants in the study. This is consistent with some studies which indicate that psychosocial treatments are not often cost-effective for people with drug dependence [17, 18]. Methadone clinics should consider discount for those women who cannot pay for the Matrix Model. Women should be encouraged to participate in the treatment despite high costs. Brief interventions should be evaluated and compared with the Matrix Model in terms of cost-effectiveness
The study results indicated that the Matrix Model needed intensive staff training. Furthermore, it was clear that most women need individual treatment services which were not possible because of inadequate treatment coverage. This issue means that the Matrix Model may not be available for every women in methadone treatment. This is consistent with a study which indicated that intensive staff training is a significant barrier to providing psychological treatments [17]. Psychologists should be trained to provide the Matrix Model in a flexible way. Health policy makers should consider this issue in designing and implementing psychological treatments for MA dependence in methadone treatment services.
The Matrix Model is an approved intervention for MA dependence [11]. Nonetheless, evaluating other treatments such as brief cognitive-behavioral treatment is suggested. Because of no internationally approved pharmacotherapy [17, 18], MA treatment depends on long-term psychosocial interventions such as the Matrix Model. Implementing long-term psychosocial interventions may not be cost-effective. Therefore, MA education and prevention programs should be provided in methadone clinics. Further studies are suggested to assess the relationship between treatment cost-effectiveness, treatment participation and retention among this group.
Gender differences have been documented in terms of MA dependence in western countries [19, 20]. It is still a need for further research in Iran to investigate the treatment success in the Matrix Model in terms of gender differences. This issue should be evaluated among men and women with MA dependence in methadone treatment services.
5. Conclusion
As MA dependence continues on the methadone programme, it is necessary to ensure that the adequate resources are allocated to treatment. Efforts should be strengthened towards education, prevention and strengthening the provision of the Matrix Model in methadone clinics. Cost-effectiveness, staff training and longevity of the Matrix Model are important problems which may impact on positive methadone treatment outcomes. Further studies are suggested.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors thank all women and health professionals who participated in this study.
Conflict of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]United Nations Office on Drugs and Crime. World drug report 2013. Vienna: United Nations Publications; 2013.
[2]United Nations Office on Drugs and Crime. World drug report 2014. Vienna: United Nations Publications; 2014.
[3]Mehrjerdi ZA. Crystal in Iran: Methamphetamine or heroin kerack. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):22. doi: 10.1186/2008-2231-21-22
[4]Alam mehrjerdi Z, Barr AM, Noroozi A. Methamphetamine-associated psychosis: A new health challenge in Iran. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):30. doi: 10.1186/2008-2231-21-30
[5]Alam Mehrjerdi Z, Abarashi Z, Noroozi A, Arshad L, Zarghami M. Correlates of shared methamphetamine injection among methamphetamine injecting treatment seekers: The first report from Iran. International Journal of STD & AIDS. 2013; 25(6):420–7. doi: 10.1177/0956462413512806
[6]Yoonessi A, Ekhtiari H. Text messages as a tool for assessing public concern about drug problems. International Journal of Drug Policy. 2013; 24(6):624–7. doi: 10.1016/j.drugpo.2013.06.002
[7]Shariatirad S, Maarefvand M, Ekhtiari H. Methamphetamine use and methadone maintenance treatment: An emerging problem in the drug addiction treatment network in Iran. International Journal of Drug Policy. 2013; 24(6):115–6. doi: 10.1016/j.drugpo.2013.05.003
[8]Alaee A, Zarghami M, Farnia S, Khademloo M, Khoddad T. Comparison of brain white matter hyperintensities in methamphetamine and methadone dependent patients and healthy controls. Iranian Journal of Radiology. 2014; 11(2):14275.. doi: 10.5812/iranjradiol.14275
[9]Ahmadi Jouibari T, Fattahi N, Shamsipur M. Rapid extraction and determination of amphetamines in human urine samples using dispersive liquid liquid microextraction and solidification of floating organic drop followed by high performance liquid chromatography. Journal of Pharmaceutical and Biomedical Analysis. 2014; 94(6):145–51. doi: 10.1016/j.jpba.2014.01.044
[10]Phillips KA, Epstein DH, Preston KL. Psychostimulant addiction treatment. Neuropharmacology. 2014; 87:150–60. doi: 10.1016/j.neuropharm.2014.04.002
[11]Lee N, Rawson R. A systematic review of cognitive and behavioural therapies for methamphetamine dependence. Drug and Alcohol Review. 2008; 27(3):309–17. doi: 10.1080/09595230801919494
[12]Huber A, Ling W, Shoptaw S, Gulati V, Brethen P, Rawson R. Integrating treatments for methamphetamine abuse: A psychosocial perspective. Journal of Addictive Diseases. 1997; 16(4):41–50. doi: 10.1080/10550889709511142
[13]Rawson RA, Shoptaw SJ, Obert JL, McCann MJ, Hasson AL, Marinelli Casey PJ, et al. An intensive outpatient approach for cocaine abuse treatment. Journal of Substance Abuse Treatment. 1995; 12(2):117–27. doi: 10.1016/0740-5472(94)00080-b
[14]Rawson RA, Huber A, McCann M, Shoptaw S, Farabee D, Reiber C, et al. A comparison of contingency management and cognitive behavioral approaches during methadone maintenance treatment for cocaine dependence. Archives of General Psychiatry. 2002; 59(9):817. doi: 10.1001/archpsyc.59.9.817
[15]Strauss A, Corbin J. Basics of qualitative research: Grounded theory procedures and techniques. California: Sage Publications; 1991.
[16]Pope C, Mays N. Qualitative research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ. 1995; 311(6996):42–5. doi: 10.1136/bmj.311.6996.42
[17]Baker A, Boggs TG, Lewin TJ. Randomized controlled trial of brief cognitive behavioural interventions among regular users of amphetamine. Addiction. 2001; 96(9):1279–87. doi: 10.1046/j.1360-0443.2001.96912797.x
[18]Baker A, Lee NK, Claire M, Lewin TJ, Grant T, Pohlman S, et al. Brief cognitive behavioural interventions for regular amphetamine users: A step in the right direction. Addiction. 2005; 100(3):367–78. doi: 10.1111/j.1360-0443.2005.01002.x
[19]Simpson JL, Grant KM, Daly PM, Kelley SG, Carlo G, Bevins RA. Psychological burden and gender differences in methamphetamine dependent individuals in treatment. Journal of Psychoactive Drugs. 2016; 48(4):261–9. doi: 10.1080/02791072.2016.1213470
[20]Han Y, Lin V, Wu F, Hser Y-I. Gender comparisons among Asian American and Pacific Islander patients in drug dependency treatment. Substance Use & Misuse. 2016; 51(6):752–62. doi: 10.3109/10826084.2016.1155604
Intensive staff training
A theme that gradually emerged from the narratives indicated that the Matrix Model needed intensive staff training. Participants frequently reported that the Matrix Model plays an important role in the treatment of MA dependence. However, it is manaulised and professional so psychologists who provide the treatment should be professional. A quarter of women and half of the health professionals reported that intensive staff training was a main problem in methadone clinics. The quotes below can explain this issue better:
ʻ... My psychologist plays an important role in my recovery because she is professional. But the Matrix Model is manualized so professional staff are the main the points …ʼ (a 36-year old woman).
ʻ... The Matrix Model needs intensive staff training because it is a professional and manualized treatment so your staff should be well-trained and experienced ... . Brief intervention do not have this problem …ʼ (a medical doctor).
An inadequate coverage of the Matrix Model
A theme that gradually emerged from the narratives indicated that the Matrix Model was not widely available every patient in methadone treatment services. Participants frequently reported that clinical psychologists in the methadone clinics did not have enough time for each patient. Therefore, the coverage of the treatment was inadequate for many women preventing treating MA dependence among them. A quarter of women and quarter of health professionals reported that the coverage of the Matrix Model was inadequate. The quotes below can explain this issue better:
ʻ... The Matrix Model is manualized and everybody cannot use this treatment. The psychologists in the methadone clinics cannot spend time on each patient. They are lots of patients who are dependent on MA …ʼ (a 38-year old woman).
ʻ... The Matrix Model is a very good treatment but psychologists do not have enough time for each patient because the Matrix Model is very comprehensive so everybody cannot benefit from the treatment. We need brief interventions ...ʼ (a methadone clinic manager).
4. Discussion
MA dependence is a health problem among female methadone patients in Iran [7]. However, there are few studies of this group in Iran. In recent years, the Matrix Model of Intensive Outpatient Treatment has been provided in methadone treatment services to treat MA dependence [7]. However, to date, it is not documented what problems are associated with the provision of the Matrix Model. This issue is important because MA dependence needs an immediate treatment [5, 7].
The study results indicated that the Matrix Model was long. Studies indicate that the length of the treatment is a concern for many drug-dependent patients [17]. Women should be informed that the duration of the Matrix Model is needed for their treatment and recovery procedure is not a short issue. Women should be informed that the Matrix Model can lead to craving management and relapse prevention [11]. Furthermore, brief interventions should be evaluated to address this problem. Further studies are suggested to assess the relationship between the length of the treatment and treating MA dependence among this group.
The study results indicated that the Matrix Model was not cost-effective for many participants in the study. This is consistent with some studies which indicate that psychosocial treatments are not often cost-effective for people with drug dependence [17, 18]. Methadone clinics should consider discount for those women who cannot pay for the Matrix Model. Women should be encouraged to participate in the treatment despite high costs. Brief interventions should be evaluated and compared with the Matrix Model in terms of cost-effectiveness
The study results indicated that the Matrix Model needed intensive staff training. Furthermore, it was clear that most women need individual treatment services which were not possible because of inadequate treatment coverage. This issue means that the Matrix Model may not be available for every women in methadone treatment. This is consistent with a study which indicated that intensive staff training is a significant barrier to providing psychological treatments [17]. Psychologists should be trained to provide the Matrix Model in a flexible way. Health policy makers should consider this issue in designing and implementing psychological treatments for MA dependence in methadone treatment services.
The Matrix Model is an approved intervention for MA dependence [11]. Nonetheless, evaluating other treatments such as brief cognitive-behavioral treatment is suggested. Because of no internationally approved pharmacotherapy [17, 18], MA treatment depends on long-term psychosocial interventions such as the Matrix Model. Implementing long-term psychosocial interventions may not be cost-effective. Therefore, MA education and prevention programs should be provided in methadone clinics. Further studies are suggested to assess the relationship between treatment cost-effectiveness, treatment participation and retention among this group.
Gender differences have been documented in terms of MA dependence in western countries [19, 20]. It is still a need for further research in Iran to investigate the treatment success in the Matrix Model in terms of gender differences. This issue should be evaluated among men and women with MA dependence in methadone treatment services.
5. Conclusion
As MA dependence continues on the methadone programme, it is necessary to ensure that the adequate resources are allocated to treatment. Efforts should be strengthened towards education, prevention and strengthening the provision of the Matrix Model in methadone clinics. Cost-effectiveness, staff training and longevity of the Matrix Model are important problems which may impact on positive methadone treatment outcomes. Further studies are suggested.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors thank all women and health professionals who participated in this study.
Conflict of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]United Nations Office on Drugs and Crime. World drug report 2013. Vienna: United Nations Publications; 2013.
[2]United Nations Office on Drugs and Crime. World drug report 2014. Vienna: United Nations Publications; 2014.
[3]Mehrjerdi ZA. Crystal in Iran: Methamphetamine or heroin kerack. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):22. doi: 10.1186/2008-2231-21-22
[4]Alam mehrjerdi Z, Barr AM, Noroozi A. Methamphetamine-associated psychosis: A new health challenge in Iran. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):30. doi: 10.1186/2008-2231-21-30
[5]Alam Mehrjerdi Z, Abarashi Z, Noroozi A, Arshad L, Zarghami M. Correlates of shared methamphetamine injection among methamphetamine injecting treatment seekers: The first report from Iran. International Journal of STD & AIDS. 2013; 25(6):420–7. doi: 10.1177/0956462413512806
[6]Yoonessi A, Ekhtiari H. Text messages as a tool for assessing public concern about drug problems. International Journal of Drug Policy. 2013; 24(6):624–7. doi: 10.1016/j.drugpo.2013.06.002
[7]Shariatirad S, Maarefvand M, Ekhtiari H. Methamphetamine use and methadone maintenance treatment: An emerging problem in the drug addiction treatment network in Iran. International Journal of Drug Policy. 2013; 24(6):115–6. doi: 10.1016/j.drugpo.2013.05.003
[8]Alaee A, Zarghami M, Farnia S, Khademloo M, Khoddad T. Comparison of brain white matter hyperintensities in methamphetamine and methadone dependent patients and healthy controls. Iranian Journal of Radiology. 2014; 11(2):14275.. doi: 10.5812/iranjradiol.14275
[9]Ahmadi Jouibari T, Fattahi N, Shamsipur M. Rapid extraction and determination of amphetamines in human urine samples using dispersive liquid liquid microextraction and solidification of floating organic drop followed by high performance liquid chromatography. Journal of Pharmaceutical and Biomedical Analysis. 2014; 94(6):145–51. doi: 10.1016/j.jpba.2014.01.044
[10]Phillips KA, Epstein DH, Preston KL. Psychostimulant addiction treatment. Neuropharmacology. 2014; 87:150–60. doi: 10.1016/j.neuropharm.2014.04.002
[11]Lee N, Rawson R. A systematic review of cognitive and behavioural therapies for methamphetamine dependence. Drug and Alcohol Review. 2008; 27(3):309–17. doi: 10.1080/09595230801919494
[12]Huber A, Ling W, Shoptaw S, Gulati V, Brethen P, Rawson R. Integrating treatments for methamphetamine abuse: A psychosocial perspective. Journal of Addictive Diseases. 1997; 16(4):41–50. doi: 10.1080/10550889709511142
[13]Rawson RA, Shoptaw SJ, Obert JL, McCann MJ, Hasson AL, Marinelli Casey PJ, et al. An intensive outpatient approach for cocaine abuse treatment. Journal of Substance Abuse Treatment. 1995; 12(2):117–27. doi: 10.1016/0740-5472(94)00080-b
[14]Rawson RA, Huber A, McCann M, Shoptaw S, Farabee D, Reiber C, et al. A comparison of contingency management and cognitive behavioral approaches during methadone maintenance treatment for cocaine dependence. Archives of General Psychiatry. 2002; 59(9):817. doi: 10.1001/archpsyc.59.9.817
[15]Strauss A, Corbin J. Basics of qualitative research: Grounded theory procedures and techniques. California: Sage Publications; 1991.
[16]Pope C, Mays N. Qualitative research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ. 1995; 311(6996):42–5. doi: 10.1136/bmj.311.6996.42
[17]Baker A, Boggs TG, Lewin TJ. Randomized controlled trial of brief cognitive behavioural interventions among regular users of amphetamine. Addiction. 2001; 96(9):1279–87. doi: 10.1046/j.1360-0443.2001.96912797.x
[18]Baker A, Lee NK, Claire M, Lewin TJ, Grant T, Pohlman S, et al. Brief cognitive behavioural interventions for regular amphetamine users: A step in the right direction. Addiction. 2005; 100(3):367–78. doi: 10.1111/j.1360-0443.2005.01002.x
[19]Simpson JL, Grant KM, Daly PM, Kelley SG, Carlo G, Bevins RA. Psychological burden and gender differences in methamphetamine dependent individuals in treatment. Journal of Psychoactive Drugs. 2016; 48(4):261–9. doi: 10.1080/02791072.2016.1213470
[20]Han Y, Lin V, Wu F, Hser Y-I. Gender comparisons among Asian American and Pacific Islander patients in drug dependency treatment. Substance Use & Misuse. 2016; 51(6):752–62. doi: 10.3109/10826084.2016.1155604
Article type: Original Research Articles |
Subject:
Addiction
Received: 2017/02/18 | Accepted: 2017/06/28 | Published: 2017/08/22
Received: 2017/02/18 | Accepted: 2017/06/28 | Published: 2017/08/22
References
1. United Nations Office on Drugs and Crime. World drug report 2013. Vienna: United Nations Publications; 2013.
2. United Nations Office on Drugs and Crime. World drug report 2014. Vienna: United Nations Publications; 2014.
3. Mehrjerdi ZA. Crystal in Iran: Methamphetamine or heroin kerack. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):22. doi: 10.1186/2008-2231-21-22 [DOI:10.1186/2008-2231-21-22]
4. Alam mehrjerdi Z, Barr AM, Noroozi A. Methamphetamine-associated psychosis: A new health challenge in Iran. DARU Journal of Pharmaceutical Sciences. 2013; 21(1):30. doi: 10.1186/2008-2231-21-30 [DOI:10.1186/2008-2231-21-30]
5. Alam Mehrjerdi Z, Abarashi Z, Noroozi A, Arshad L, Zarghami M. Correlates of shared methamphetamine injection among methamphetamine injecting treatment seekers: The first report from Iran. International Journal of STD & AIDS. 2013; 25(6):420–7. doi: 10.1177/0956462413512806 [DOI:10.1177/0956462413512806]
6. Yoonessi A, Ekhtiari H. Text messages as a tool for assessing public concern about drug problems. International Journal of Drug Policy. 2013; 24(6):624–7. doi: 10.1016/j.drugpo.2013.06.002 [DOI:10.1016/j.drugpo.2013.06.002]
7. Shariatirad S, Maarefvand M, Ekhtiari H. Methamphetamine use and methadone maintenance treatment: An emerging problem in the drug addiction treatment network in Iran. International Journal of Drug Policy. 2013; 24(6):115–6. doi: 10.1016/j.drugpo.2013.05.003 [DOI:10.1016/j.drugpo.2013.05.003]
8. Alaee A, Zarghami M, Farnia S, Khademloo M, Khoddad T. Comparison of brain white matter hyperintensities in methamphetamine and methadone dependent patients and healthy controls. Iranian Journal of Radiology. 2014; 11(2):14275.. doi: 10.5812/iranjradiol.14275 [DOI:10.5812/iranjradiol.14275]
9. Ahmadi Jouibari T, Fattahi N, Shamsipur M. Rapid extraction and determination of amphetamines in human urine samples using dispersive liquid liquid microextraction and solidification of floating organic drop followed by high performance liquid chromatography. Journal of Pharmaceutical and Biomedical Analysis. 2014; 94(6):145–51. doi: 10.1016/j.jpba.2014.01.044 [DOI:10.1016/j.jpba.2014.01.044]
10. Phillips KA, Epstein DH, Preston KL. Psychostimulant addiction treatment. Neuropharmacology. 2014; 87:150–60. doi: 10.1016/j.neuropharm.2014.04.002 [DOI:10.1016/j.neuropharm.2014.04.002]
11. Lee N, Rawson R. A systematic review of cognitive and behavioural therapies for methamphetamine dependence. Drug and Alcohol Review. 2008; 27(3):309–17. doi: 10.1080/09595230801919494 [DOI:10.1080/09595230801919494]
12. Huber A, Ling W, Shoptaw S, Gulati V, Brethen P, Rawson R. Integrating treatments for methamphetamine abuse: A psychosocial perspective. Journal of Addictive Diseases. 1997; 16(4):41–50. doi: 10.1080/10550889709511142 [DOI:10.1080/10550889709511142]
13. Rawson RA, Shoptaw SJ, Obert JL, McCann MJ, Hasson AL, Marinelli Casey PJ, et al. An intensive outpatient approach for cocaine abuse treatment. Journal of Substance Abuse Treatment. 1995; 12(2):117–27. doi: 10.1016/0740-5472(94)00080-b [DOI:10.1016/0740-5472(94)00080-B]
14. Rawson RA, Huber A, McCann M, Shoptaw S, Farabee D, Reiber C, et al. A comparison of contingency management and cognitive behavioral approaches during methadone maintenance treatment for cocaine dependence. Archives of General Psychiatry. 2002; 59(9):817. doi: 10.1001/archpsyc.59.9.817 [DOI:10.1001/archpsyc.59.9.817]
15. Strauss A, Corbin J. Basics of qualitative research: Grounded theory procedures and techniques. California: Sage Publications; 1991.
16. Pope C, Mays N. Qualitative research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ. 1995; 311(6996):42–5. doi: 10.1136/bmj.311.6996.42 [DOI:10.1136/bmj.311.6996.42]
17. Baker A, Boggs TG, Lewin TJ. Randomized controlled trial of brief cognitive behavioural interventions among regular users of amphetamine. Addiction. 2001; 96(9):1279–87. doi: 10.1046/j.1360-0443.2001.96912797.x [DOI:10.1046/j.1360-0443.2001.96912797.x]
18. Baker A, Lee NK, Claire M, Lewin TJ, Grant T, Pohlman S, et al. Brief cognitive behavioural interventions for regular amphetamine users: A step in the right direction. Addiction. 2005; 100(3):367–78. doi: 10.1111/j.1360-0443.2005.01002.x [DOI:10.1111/j.1360-0443.2005.01002.x]
19. Simpson JL, Grant KM, Daly PM, Kelley SG, Carlo G, Bevins RA. Psychological burden and gender differences in methamphetamine dependent individuals in treatment. Journal of Psychoactive Drugs. 2016; 48(4):261–9. doi: 10.1080/02791072.2016.1213470 [DOI:10.1080/02791072.2016.1213470]
20. Han Y, Lin V, Wu F, Hser Y-I. Gender comparisons among Asian American and Pacific Islander patients in drug dependency treatment. Substance Use & Misuse. 2016; 51(6):752–62. doi: 10.3109/10826084.2016.1155604 [DOI:10.3109/10826084.2016.1155604]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
