
988368
Thu, Apr 25, 2024

Volume 17, Issue 2 (June 2019)
Iranian Rehabilitation Journal 2019, 17(2): 97-104 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammad-Aminzadeh D, Sharifi M, Younesi S J, Movallali G, Asmari Y. Mental Rehabilitation Based on Emotion Regulation Training to Reduce Depression in Students With Physical Disability. Iranian Rehabilitation Journal 2019; 17 (2) :97-104
URL: http://irj.uswr.ac.ir/article-1-856-en.html
URL: http://irj.uswr.ac.ir/article-1-856-en.html
Dana Mohammad-Aminzadeh1 
 , Mehdi Sharifi2 , Seyed Jalal Younesi *
, Mehdi Sharifi2 , Seyed Jalal Younesi *  2, Giuta Movallali3 , Yousef Asmari4
2, Giuta Movallali3 , Yousef Asmari4
, Mehdi Sharifi2 , Seyed Jalal Younesi * 2, Giuta Movallali3 , Yousef Asmari4
1- Department of Counseling, Faculty of Psychology and Educational Sciences, Allameh Tabataba'i University, Tehran, Iran; Student Research Committee, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
2- Department of Counseling, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychology and Exceptional Children Education, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran; Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Counseling, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychology and Exceptional Children Education, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran; Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 570 kb]
(1459 Downloads)
| Abstract (HTML) (3625 Views)

Full-Text: (982 Views)
Highlights
● Poor emotional regulation in depression, students with disabilities, is effective.
Plain Language Summary
Emotion regulation training in the experimental group showed that emotion regulation could be effective in reducing depression in students with disabilities.
1. Introduction
Disability is an umbrella term covering impairments, activity limitations, and participation restrictions as defined by the World Health Organization (WHO) relying on the International Classification of Functioning, Disability, and Health Disability [1]. Disability refers to impaired physical functioning [2] and deprives the individual from daily activities, the opportunity of independent living, and personal and social relationships [3].
Physical disability is a type of disability. It is defined as an impairment that restricts one or more major life activities in an individual [4]. According to World Health Statistics, nearly 1 billion people in the world live with physical disability [5], more than two-thirds of them live in the developing countries [6].
Findings of several studies reflect psychological and emotional consequences of physical disability in the affected students. Overall, these studies show that physical disability can reduce self-esteem [7] and cause mental distress and depression [8]. On the other hand, people with physically disabilities and impairment in the development of motor coordination and abnormal growth are more vulnerable to emotional problems and less capable to control and regulate their emotional reactions [9].
Evidence suggests the relapse of depression or even the incidence of a chronic depression after discontinuation of depression therapies [10]. In this regard, emotion regulation skills can be a promising therapy to improve depression [11]. Given this hypothesis, empirical studies show that people with depression cannot easily use emotion regulation strategies [12]. In addition, cross sectional, self-examination studies show that the intensity of depression can be attributed to difficulties in recognizing and describing emotions [13]. Various researchers also showed that difficulty in applying emotion regulation strategies increases the risk of often recurrent and chronic disorders [14].
Emotion regulation refers to those skills used to recognize and assess emotions, regulate those emotions, and use adaptive emotions [15]. The Gross model of emotion regulation encompasses all conscious and unconscious strategies for decreasing, maintaining, and increasing emotional, behavioral, and cognitive components of an emotional response [16]. It refers to the ability to understand emotions, modify an experience, and express emotions [17]. In other words, emotion regulation refers to controlling emotions in current conditions [18].
It is defined as “how emotions affect people, what emotions should they express, and when they should experience and express their emotions” [19, 20]. It aims to regulate emotional reactions using the right strategies [21]. Emotion regulation skill plays a critical role in welfare and well-being of individuals [22]. It serves in mental health, interpersonal relationships, and academic achievement [16]. On the other hand, difficulty in applying emotion regulation is correlated with such psychiatric disorders as depression and anxiety [23].
Berking et al. showed that impaired emotion regulation leads to the incidence of depression. On the contrary, systematic strengthening of emotion regulation skills can prevent and improve symptoms of depression [24]. Diedrich et al. found out that emotion regulation training can significantly improve depression, especially in people with higher degrees of depression [25].
Considering the important role of emotions in determining health status and successful social functioning [19], and the prominent role of emotions in all mental and emotional disorders [22]. e.g. depression, anxiety, and interpersonal sensitivity [23], emotion regulation training can be an effective strategy to reduce the symptoms of depression [26], increase personal capability to perform daily activities and enjoy life [15], and improve mental health in the affected individuals [22].
To the best of authors’ knowledge, there is limited research on emotion regulation training in students with physical disabilities from Iran. This type of therapy for such chronic disorders, such as depression is neglected in Iran. Accordingly, the present study aimed at investigating the efficacy of group emotion regulation training in reducing depression in students with physical disabilities.
2. Methods
The current pre-test and post-test, quasi-experimental study was designed with the intervention and control groups. The statistical population consisted of all male students in high schools serving children with physical disabilities in Tehran, Iran in the academic year 2016-2017. The sample size was determined as 26. Accordingly, 26 male students with physical disabilities were selected using purposive sampling method based on inclusion criteria.
The selected individuals were randomly divided into two intervention and control groups, each had 13 subjects. The sample size was determined based on the Kori theory. He believed that the members of six-member and 15-member with a leader have abundant opportunity to interact with each other in the least time. They had also the possibility for individual activities. They also sensed their significant role in the group [27].
Inclusion criteria were having normal IQ (90 to 110) based on school records, physical disability in the secondary school students, no history of psychiatric or other disorders, and no history of hospitalization in psychiatric hospitals, based on medical records available at the school, and no history of attending therapeutic programs except for emotion regulation training. The only exclusion criterion was unwillingness to participate in the project.
Procedure
To conduct the current research, the required permissions were obtained from the Research and Development Department in Allameh Tabataba'i University. The Special Education Organization in Tehran was visited.
Districts 2, 4, and 16 were selected purposively out of 22 districts of Tehran, since the schools serving students with physical disabilities were only found in these districts. The school located in District 4 was considered as the sample due to adequate number of students with physical disabilities. First, the Beck Depression Inventory (BDI) was distributed among the students.
In the next step, 26 students with higher depression scores were determined as the sample size out of total number of the students who completed the inventory (n=67). They were randomly divided into two intervention and control groups. The emotion regulation training protocol was implemented in the intervention group, while the control group did not receive any training during this period. Post-test was taken from both groups after the training completion. Finally, the emotion regulation skills were also explained for the control group in a separate session.
The emotion regulation intervention was implemented within eight 60-minute sessions twice a week in the intervention group. Statistical package for social science version 23.0, SPSS V. 23 was used for statistical analysis.
The informed consent was obtained from the students before enrollment in the research. The subjects were assured about the confidentiality of their information and it was explained to them that they can withdraw from the study at any stage.
The Beck Depression inventory consists of 21 items to measure the feedback and symptoms in patients with depression. The items were designed based on observing and summarizing common attitudes and symptoms in patients with depression. The content of this inventory comprehensively encompasses symptomatology of depression, but it puts more emphasis on cognitive content [28].
The items cover various symptoms of depression. The items are scored based on a five-point Likert scale (from 0 to 4). The scale measures the intensity of depression from mild to very severe. Total score of the instrument range 0 to 63. Beck et al. reviewed the studies in which this scale was employed.
Test-retest reliability of BDI varied from 0.48 to 0.86 based on the interval consistency of test-retest results and the population type and sample size. Beck et al., Measured reliability of BDI at one-week interval (0.93) [29]. In the reviews performed by Beck et al. On the second edition of the scale, the intensity of depression was highlighted in both healthy and patient groups. They reported the reliability and internal consistency by Cronbach’s alpha of 0.86 and 0.81, respectively. In a study from Iran, the reliability and internal consistency of BDI were 0.70 to 0.90, respectively. Validity of the scale was also acceptable according to various studies.
Intervention method
Summary of the training sessions is given as follows:
Session 1: Pre-test implementation, communication and conceptualization, and explanation of the need to use emotion regulation skills; Session 2: Teach how to be aware of positive emotions and their various types (happiness, interest, and love) and teach how to pay attention to positive emotions and the need to use them with an example relying on mental visualization. Homework: Write down major positive emotions in the provided form; Session 3: Teach how to be aware of negative emotions; encompass a brief overview of the previous session; teach how to be aware of negative emotions and their types (anxiety, sadness, anger, and hatred), and teach how to pay attention to negative emotions and the need to use them with an example relying on mental visualization. Homework: write down major negative emotions in the provided form; Session 4: Teach how to accept positive emotions; cover a brief overview of the previous session; teach how to accept without judging the rate and number (high or low) of positive emotions and positive and negative outcomes of using these emotions. Homework: ask opinions of the spouse or a close friend about how low or high his/her positive emotions were and write them down in the provided form; Session 5: Teach the contents of the 4th session with regard to negative emotions and the same homework; Session 6: Teach reassessment and expression of positive emotions encompassing a brief overview of the previous session; teach mental experience of positive emotions relying on mental visualization and mental inhibition, and teach who to properly express such emotions; Session 7: Teach reassessment and expression of negative emotions covering a brief overview of the previous session; teach mental experience of negative emotions; inappropriate expression and inhibition of inappropriate expression of these emotions; Session 8: Summarize training sessions and implement post-test.
3. Results
The mean age of the participants was 15.8±3.47 years. ANCOVA was used to investigate the efficacy of intervention. First, assumptions of homogeneity of variances, homogeneity of regression slopes and normal distribution were tested. The Levene test was used to test homogeneity of variances in the two groups at post-test. The result of applied statistics was not statistically significant for the studied variable (post-test: depression index, P=0.2). Therefore, the assumption of homogeneity of variances was accepted at the post-test. Homogeneity of regression coefficients was tested using interaction of pre-test depression with treatment method as an independent variable at post-test.
The interaction of the pre-test with treatment method was not significant, which indicated the homogeneity of regression coefficients. Therefore, the assumption of homogeneity of regression coefficients was accepted at post-test (post-test depression, P=0.69, F=0.6). The Kolmogorov-Smirnov test results showed normal data distribution since the difference between the results of statistics was not significant (P>0.05). The null hypothesis was accepted and data distribution was normal. Then, ANCOVA was performed.
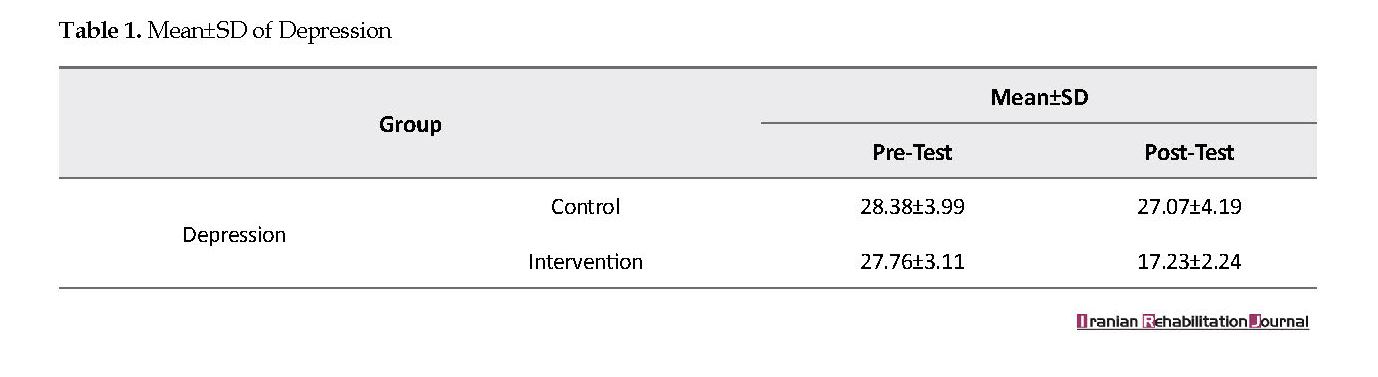
Table 1 shows mean and standard deviation of depression in the intervention and control groups at pre-test and post-test. Mean comparison showed that the mean value of the intervention group was lower than that of the group at post-test. Table 2 shows that the effect of group or intervention was statistically significant by deleting and neutralizing the pre-test variable (P<0.001). It can be concluded that group emotion regulation training made a difference between the intervention and control groups.
4. Discussion
The present study aimed at investigating the efficacy of mental rehabilitation based on group emotion regulation training to reduce depression in students with physical disabilities. The intervention program of emotion regulation training was implemented within eight sessions. Research findings showed a decrease in the depression score of the intervention group students.
● Poor emotional regulation in depression, students with disabilities, is effective.
Plain Language Summary
Emotion regulation training in the experimental group showed that emotion regulation could be effective in reducing depression in students with disabilities.
1. Introduction
Disability is an umbrella term covering impairments, activity limitations, and participation restrictions as defined by the World Health Organization (WHO) relying on the International Classification of Functioning, Disability, and Health Disability [1]. Disability refers to impaired physical functioning [2] and deprives the individual from daily activities, the opportunity of independent living, and personal and social relationships [3].
Physical disability is a type of disability. It is defined as an impairment that restricts one or more major life activities in an individual [4]. According to World Health Statistics, nearly 1 billion people in the world live with physical disability [5], more than two-thirds of them live in the developing countries [6].
Findings of several studies reflect psychological and emotional consequences of physical disability in the affected students. Overall, these studies show that physical disability can reduce self-esteem [7] and cause mental distress and depression [8]. On the other hand, people with physically disabilities and impairment in the development of motor coordination and abnormal growth are more vulnerable to emotional problems and less capable to control and regulate their emotional reactions [9].
Evidence suggests the relapse of depression or even the incidence of a chronic depression after discontinuation of depression therapies [10]. In this regard, emotion regulation skills can be a promising therapy to improve depression [11]. Given this hypothesis, empirical studies show that people with depression cannot easily use emotion regulation strategies [12]. In addition, cross sectional, self-examination studies show that the intensity of depression can be attributed to difficulties in recognizing and describing emotions [13]. Various researchers also showed that difficulty in applying emotion regulation strategies increases the risk of often recurrent and chronic disorders [14].
Emotion regulation refers to those skills used to recognize and assess emotions, regulate those emotions, and use adaptive emotions [15]. The Gross model of emotion regulation encompasses all conscious and unconscious strategies for decreasing, maintaining, and increasing emotional, behavioral, and cognitive components of an emotional response [16]. It refers to the ability to understand emotions, modify an experience, and express emotions [17]. In other words, emotion regulation refers to controlling emotions in current conditions [18].
It is defined as “how emotions affect people, what emotions should they express, and when they should experience and express their emotions” [19, 20]. It aims to regulate emotional reactions using the right strategies [21]. Emotion regulation skill plays a critical role in welfare and well-being of individuals [22]. It serves in mental health, interpersonal relationships, and academic achievement [16]. On the other hand, difficulty in applying emotion regulation is correlated with such psychiatric disorders as depression and anxiety [23].
Berking et al. showed that impaired emotion regulation leads to the incidence of depression. On the contrary, systematic strengthening of emotion regulation skills can prevent and improve symptoms of depression [24]. Diedrich et al. found out that emotion regulation training can significantly improve depression, especially in people with higher degrees of depression [25].
Considering the important role of emotions in determining health status and successful social functioning [19], and the prominent role of emotions in all mental and emotional disorders [22]. e.g. depression, anxiety, and interpersonal sensitivity [23], emotion regulation training can be an effective strategy to reduce the symptoms of depression [26], increase personal capability to perform daily activities and enjoy life [15], and improve mental health in the affected individuals [22].
To the best of authors’ knowledge, there is limited research on emotion regulation training in students with physical disabilities from Iran. This type of therapy for such chronic disorders, such as depression is neglected in Iran. Accordingly, the present study aimed at investigating the efficacy of group emotion regulation training in reducing depression in students with physical disabilities.
2. Methods
The current pre-test and post-test, quasi-experimental study was designed with the intervention and control groups. The statistical population consisted of all male students in high schools serving children with physical disabilities in Tehran, Iran in the academic year 2016-2017. The sample size was determined as 26. Accordingly, 26 male students with physical disabilities were selected using purposive sampling method based on inclusion criteria.
The selected individuals were randomly divided into two intervention and control groups, each had 13 subjects. The sample size was determined based on the Kori theory. He believed that the members of six-member and 15-member with a leader have abundant opportunity to interact with each other in the least time. They had also the possibility for individual activities. They also sensed their significant role in the group [27].
Inclusion criteria were having normal IQ (90 to 110) based on school records, physical disability in the secondary school students, no history of psychiatric or other disorders, and no history of hospitalization in psychiatric hospitals, based on medical records available at the school, and no history of attending therapeutic programs except for emotion regulation training. The only exclusion criterion was unwillingness to participate in the project.
Procedure
To conduct the current research, the required permissions were obtained from the Research and Development Department in Allameh Tabataba'i University. The Special Education Organization in Tehran was visited.
Districts 2, 4, and 16 were selected purposively out of 22 districts of Tehran, since the schools serving students with physical disabilities were only found in these districts. The school located in District 4 was considered as the sample due to adequate number of students with physical disabilities. First, the Beck Depression Inventory (BDI) was distributed among the students.
In the next step, 26 students with higher depression scores were determined as the sample size out of total number of the students who completed the inventory (n=67). They were randomly divided into two intervention and control groups. The emotion regulation training protocol was implemented in the intervention group, while the control group did not receive any training during this period. Post-test was taken from both groups after the training completion. Finally, the emotion regulation skills were also explained for the control group in a separate session.
The emotion regulation intervention was implemented within eight 60-minute sessions twice a week in the intervention group. Statistical package for social science version 23.0, SPSS V. 23 was used for statistical analysis.
The informed consent was obtained from the students before enrollment in the research. The subjects were assured about the confidentiality of their information and it was explained to them that they can withdraw from the study at any stage.
The Beck Depression inventory consists of 21 items to measure the feedback and symptoms in patients with depression. The items were designed based on observing and summarizing common attitudes and symptoms in patients with depression. The content of this inventory comprehensively encompasses symptomatology of depression, but it puts more emphasis on cognitive content [28].
The items cover various symptoms of depression. The items are scored based on a five-point Likert scale (from 0 to 4). The scale measures the intensity of depression from mild to very severe. Total score of the instrument range 0 to 63. Beck et al. reviewed the studies in which this scale was employed.
Test-retest reliability of BDI varied from 0.48 to 0.86 based on the interval consistency of test-retest results and the population type and sample size. Beck et al., Measured reliability of BDI at one-week interval (0.93) [29]. In the reviews performed by Beck et al. On the second edition of the scale, the intensity of depression was highlighted in both healthy and patient groups. They reported the reliability and internal consistency by Cronbach’s alpha of 0.86 and 0.81, respectively. In a study from Iran, the reliability and internal consistency of BDI were 0.70 to 0.90, respectively. Validity of the scale was also acceptable according to various studies.
Intervention method
Summary of the training sessions is given as follows:
Session 1: Pre-test implementation, communication and conceptualization, and explanation of the need to use emotion regulation skills; Session 2: Teach how to be aware of positive emotions and their various types (happiness, interest, and love) and teach how to pay attention to positive emotions and the need to use them with an example relying on mental visualization. Homework: Write down major positive emotions in the provided form; Session 3: Teach how to be aware of negative emotions; encompass a brief overview of the previous session; teach how to be aware of negative emotions and their types (anxiety, sadness, anger, and hatred), and teach how to pay attention to negative emotions and the need to use them with an example relying on mental visualization. Homework: write down major negative emotions in the provided form; Session 4: Teach how to accept positive emotions; cover a brief overview of the previous session; teach how to accept without judging the rate and number (high or low) of positive emotions and positive and negative outcomes of using these emotions. Homework: ask opinions of the spouse or a close friend about how low or high his/her positive emotions were and write them down in the provided form; Session 5: Teach the contents of the 4th session with regard to negative emotions and the same homework; Session 6: Teach reassessment and expression of positive emotions encompassing a brief overview of the previous session; teach mental experience of positive emotions relying on mental visualization and mental inhibition, and teach who to properly express such emotions; Session 7: Teach reassessment and expression of negative emotions covering a brief overview of the previous session; teach mental experience of negative emotions; inappropriate expression and inhibition of inappropriate expression of these emotions; Session 8: Summarize training sessions and implement post-test.
3. Results
The mean age of the participants was 15.8±3.47 years. ANCOVA was used to investigate the efficacy of intervention. First, assumptions of homogeneity of variances, homogeneity of regression slopes and normal distribution were tested. The Levene test was used to test homogeneity of variances in the two groups at post-test. The result of applied statistics was not statistically significant for the studied variable (post-test: depression index, P=0.2). Therefore, the assumption of homogeneity of variances was accepted at the post-test. Homogeneity of regression coefficients was tested using interaction of pre-test depression with treatment method as an independent variable at post-test.
The interaction of the pre-test with treatment method was not significant, which indicated the homogeneity of regression coefficients. Therefore, the assumption of homogeneity of regression coefficients was accepted at post-test (post-test depression, P=0.69, F=0.6). The Kolmogorov-Smirnov test results showed normal data distribution since the difference between the results of statistics was not significant (P>0.05). The null hypothesis was accepted and data distribution was normal. Then, ANCOVA was performed.
Table 1 shows mean and standard deviation of depression in the intervention and control groups at pre-test and post-test. Mean comparison showed that the mean value of the intervention group was lower than that of the group at post-test. Table 2 shows that the effect of group or intervention was statistically significant by deleting and neutralizing the pre-test variable (P<0.001). It can be concluded that group emotion regulation training made a difference between the intervention and control groups.
4. Discussion
The present study aimed at investigating the efficacy of mental rehabilitation based on group emotion regulation training to reduce depression in students with physical disabilities. The intervention program of emotion regulation training was implemented within eight sessions. Research findings showed a decrease in the depression score of the intervention group students.
With regard to neutralizing the effect of depression score at pre-test, it can be stated that the difference caused by the effect of the independent variable. In other words, the training program led to reduction of depression in the students with physical disabilities in the intervention group, since the intervention program was only implemented in this group and the control group received no training.
The research hypothesis tested the effect of emotion regulation training in reducing depression on students with physical disabilities. Since to the best of authors’ knowledge, no similar study was conducted so far, the results of rather similar studies were compared with those of the current study. The results of the present study were consistent with those of the studies by Berking et al.; Diedrich et al.; Gratz and Gunderson; Beck, Steer and Carbin [25-27, 30].
Disability is a lifelong impairment associated with psychosocial consequences. In other words, people with disabilities have a false perception of themselves (think they cannot be like normal people) and are more vulnerable to emotional problems, since they have impairments in motor development and abnormal growth. Various aspects of their lives are under the influence of disability. Thereby, they are not satisfied with their lives.
They do not enjoy life as they should be. Mental, emotional, and social health of the individual is affected by disability. As a result, students with physical disabilities are less capable to regulate and control emotional reactions; this reduces their well-being. In other words, the students with physical-motor disabilities may not be aware of their negative and positive emotions due to physical and motor impairments.
They cannot involve their emotions in daily life activities, because they assess themselves negatively in different situations due to physical and psychological problems. They also less participate in social activities. Negative effects of this issue cause feelings of worthlessness, restlessness and irritability, despair, and distress. On the other hand, emotion regulation strategies strengthen balance in emotional experiences [15], decrease negative emotions, increase positive emotions, and adjust behavior [31, 32].
In other words, emotion regulation training makes people with disabilities aware of their negative emotions and the impact of these emotions on self-awareness [33]. They try to maintain a healthy emotional life by reassessment of their emotions in different situations. Thereby, they can reduce their physical and mental health problems and control their emotions [33]. On the other hand, dysfunction and impairment in effective regulation of emotions is related to vulnerability to depression [34]. This increases mental problems in people [35], underlies many personal and social problems emerge in crisis.
Emotion regulation training could improve the capability of people with physical disabilities in terms of proper control and management of emotions in different situations. They can properly express their emotions in a timely manner. They can use effective coping strategies to overcome barriers and problems in life. As a result, their social relationships and psychological health are improved and they can assess their life positively and enjoy it. They can keep a balance between positive and negative emotions and feel satisfied with their lives. Ultimately, their positive emotions increase. Consequently, the level of depression reduces.
5. Conclusion
Emotions are crucial in life. Emotion regulation as a therapeutic approach modulates emotions, enhances self-esteem and positive social interactions in personal relationships, strengthens effective coping with stressful situations, and increases the opportunity to participate in social activities. As a result, emotion regulation training makes students with physical-motor disabilities aware of positive and negative emotions, timely acceptance and expression of such emotions. This training can also increase awareness on emotions, and teach how to control and overcome negative emotions resulting from interpersonal relationships, which consequently improves mental health.
The most important limitations were the purposive sampling method and consequently the quasi-experimental design of the study that reduced the possibility of generalizing the results to the whole population. It is suggested to evaluate the effect of teaching emotion regulation skills on other mental health variables in individuals with physical disabilities.
Ethical Considerations
Compliance with ethical guidelines
The informed consent was obtained from the students before enrollment in the research. The subjects were assured about the confidentiality of their information and it was explained to them that they can withdraw from the study at any stage.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Designing the treatment protocol, performing on patients and information, collecting the data: Dana Mohammad-Aminzadeh, Yousef Asamari, Seyed Jalal Younesi; Analyzing the data, writing the results: Mehdi Sharifi, Giuta Movallali; and Writing the basics of theory and background: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Lucas-Carrasco R, Eser E, Hao Y, McPherson KM, Green A, Kullmann L, et al. The Quality of Care and Support (QOCS) for people with disability scale: Development and psychometric properties. Research in Developmental Disabilities. 2011; 32(3):1212-25. [DOI:10.1016/j.ridd.2010.12.030] [PMID]
Aurora U. Study for determining laterality in children with motor disabilities in adapted physical activities. Procedia-Social and Behavioral Sciences. 2014; 117:646-52. [DOI:10.1016/j.sbspro.2014.02.276]
Salehi M, Tavakol HK, Shabani M, Ziaei T. The relationship between self-esteem and sexual self-concept in people with physical-motor disabilities. Iranian Red Crescent Medical Journal. 2015; 17(1):e25359. [DOI:10.5812/ircmj.25359] [PMID] [PMCID]
Brown RL, Turner RJ. Physical limitation and anger: Stress exposure and assessing the role of psychosocial resources. Society and Mental Health. 2012; 2(2):69-84. [DOI:10.1177/2156869312444441]
World Health Organization. World report on disability. Geneva: World Health Organization; 2011.
Bahrampour O, Ghamari M, Amiri Majd M. The effectiveness of cognitive behavioral group therapy on self-esteem and psychological well-being of young people with physical-motor disabilities. Society for Simulation in Healthcare. 2014; 2:2345-633.
Nosek MA, Hughes RB, Swedlund N, Taylor HB, Swank P. Self-esteem and women with disabilities. Social Science & Medicine. 2003; 56(8):1737-47. [DOI:10.1016/S0277-9536(02)00169-7]
Trani JF, Bakhshi P. Challenges for assessing disability prevalence: The case of Afghanistan. Journal of Disability Research. 2008; 2(1):44-64. [DOI:10.1016/j.alter.2007.10.003]
Scotland JL, McKenzie K, Cossar J, Murray A, Michie A. Recognition of facial expressions of emotion by adults with intellectual disability: Is there evidence for the emotion specificity hypothesis? Research in Developmental Disabilities. 2016; 48:69-78. [DOI:10.1016/j.ridd.2015.10.018] [PMID]
Casacalenda N, Perry JC, Looper K. Remission in major depressive disorder: A comparison of pharmacotherapy, psychotherapy, and control conditions. American Journal of Psychiatry. 2002; 159(8):1354-60. [DOI:10.1176/appi.ajp.159.8.1354] [PMID]
Berking M, Poppe C, Luhmann M, Wuppermann P, Jaggi V, Seifritz E. Is the association between various emotion-regulation skills and mental health mediated by the ability to modify emotions? Results from two cross-sectional studies. Journal of Behavior Therapy and Experimental Psychiatry. 2012; 43:931-7.
Liverant GI, Brown TA, Barlow DH, Roemer L. Emotion regulation in unipolar depression: The effects of acceptance and suppression of subjective emotional experience on the intensity and duration of sadness and negative affect. Behaviour Research and Therapy. 2008; 46(11):1201-9. [DOI:10.1016/j.brat.2008.08.001] [PMID]
Rude S, McCarthy C. Brief report. Cognition & Emotion. 2003; 17(5):799-806. [DOI:10.1080/02699930302283]
Solomon DA, Keller MB, Leon AC, Mueller TI, Lavori PW, Shea MT, et al. Multiple recurrences of major depressive disorder. American Journal of Psychiatry. 2000; 157(2):229-33. [DOI:10.1176/appi.ajp.157.2.229] [PMID]
Susa G, Mone I, Salagean D, Mihalca L, Benga O, Friedlmeier W. The relation between maternal perception of toddler emotion regulation abilities and emotion regulation abilities displayed by children in a frustration inducing task. Procedia-Social and Behavioral Sciences. 2014; 128:493-7. [DOI:10.1016/j.sbspro.2014.03.194]
Gross JJ, John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology. 2003; 85(2):348. [DOI:10.1037/0022-3514.85.2.348] [PMID]
Kingston J, Chadwick P, Meron D, Skinner TC. A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research. 2007; 62(3):297-300. [DOI:10.1016/j.jpsychores.2006.10.007] [PMID]
Koole SL. The psychology of emotion regulation: An integrative review. Cognition and Emotion. 2009; 23(1):4-41. [DOI:10.1080/02699930802619031]
Campos JJ, Walle EA, Dahl A, Main A. Reconceptualizing emotion regulation. Emotion Review. 2011; 3(1):26-35. [DOI:10.1177/1754073910380975]
Joormann J. Cognitive inhibition and emotion regulation in depression. Current Directions in Psychological Science. 2010; 19(3):161-6. [DOI:10.1177/0963721410370293]
Halperin E. Emotion, emotion regulation, and conflict resolution. Emotion Review. 2014; 6(1):3. [DOI:10.1177/1754073913491844]
Cheung EO, Gardner WL, Anderson JF. Emotionships: Examining people’s emotion-regulation relationships and their consequences for well-being. Social Psychological and Personality Science. 2015; 6(4):407-14. [DOI:10.1177/1948550614564223]
Shepherd L, Wild J. Emotion regulation, physiological arousal and PTSD symptoms in trauma-exposed individuals. Journal of Behavior Therapy and Experimental Psychiatry. 2014; 45(3):360-7. [DOI:10.1016/j.jbtep.2014.03.002] [PMID] [PMCID]
Berking M, Wirtz CM, Svaldi J, Hofmann SG. Emotion regulation predicts symptoms of depression over five years. Behaviour Research and Therapy. 2014; 57:13-20. [DOI:10.1016/j.brat.2014.03.003] [PMID]
Diedrich A, Grant M, Hofmann SG, Hiller W, Berking M. Self-compassion as an emotion regulation strategy in major depressive disorder. Behaviour Research and Therapy. 2014; 58:43-51. [DOI:10.1016/j.brat.2014.05.006] [PMID]
Gratz KL, Gunderson JG. Preliminary data on an acceptance-based emotion regulation group intervention for deliberate self-harm among women with borderline personality disorder. Behavior Therapy. 2006; 37(1):25-35. [DOI:10.1016/j.beth.2005.03.002] [PMID]
Corey MS, Corey G, Corey C. Groups: Process and practice. Boston: Cengage Learning; 2013.
Azkhosh M. [Psychological tests and clinical diagnosis (Persian)]. Tehran: Ravan; 2014.
Beck AT, Steer RA, Carbin MG. Psychometric properties of the beck depression inventory: Twenty-five years of evaluation. Clinical Psychology Review. 1988; 8(1):77-100. [DOI:10.1016/0272-7358(88)90050-5]
Berking M, Orth U, Wupperman P, Meier LL, Caspar F. Prospective effects of emotion-regulation skills on emotional adjustment. Journal of Counseling Psychology. 2008; 55(4):485-94. [DOI:10.1037/a0013589] [PMID]
Bardeen JR, Fergus TA. An examination of the incremental contribution of emotion regulation difficulties to health anxiety beyond specific emotion regulation strategies. Journal of Anxiety Disorders. 2014; 28(4):394-401. [DOI:10.1016/j.janxdis.2014.03.002] [PMID]
Isasi CR, Ostrovsky NW, Wills TA. The association of emotion regulation with lifestyle behaviors in inner-city adolescents. Eating Behaviors. 2013; 14(4):518-21. [DOI:10.1016/j.eatbeh.2013.07.009] [PMID] [PMCID]
Oshri A, Sutton TE, Clay-Warner J, Miller JD. Child maltreatment types and risk behaviors: Associations with attachment style and emotion regulation dimensions. Personality and Individual Differences. 2015; 73:127-33. [DOI:10.1016/j.paid.2014.09.015]
Tortella-Feliu M, Balle M, Sesé A. Relationships between negative affectivity, emotion regulation, anxiety, and depressive symptoms in adolescents as examined through structural equation modeling. Journal of Anxiety Disorders. 2010; 24(7):686-93. [DOI:10.1016/j.janxdis.2010.04.012] [PMID]
Rutherford HJ, Wallace NS, Laurent HK, Mayes LC. Emotion regulation in parenthood. Developmental Review. 2015; 36:1-14. [DOI:10.1016/j.dr.2014.12.008] [PMID] [PMCID]
Disability is a lifelong impairment associated with psychosocial consequences. In other words, people with disabilities have a false perception of themselves (think they cannot be like normal people) and are more vulnerable to emotional problems, since they have impairments in motor development and abnormal growth. Various aspects of their lives are under the influence of disability. Thereby, they are not satisfied with their lives.
They do not enjoy life as they should be. Mental, emotional, and social health of the individual is affected by disability. As a result, students with physical disabilities are less capable to regulate and control emotional reactions; this reduces their well-being. In other words, the students with physical-motor disabilities may not be aware of their negative and positive emotions due to physical and motor impairments.
They cannot involve their emotions in daily life activities, because they assess themselves negatively in different situations due to physical and psychological problems. They also less participate in social activities. Negative effects of this issue cause feelings of worthlessness, restlessness and irritability, despair, and distress. On the other hand, emotion regulation strategies strengthen balance in emotional experiences [15], decrease negative emotions, increase positive emotions, and adjust behavior [31, 32].
In other words, emotion regulation training makes people with disabilities aware of their negative emotions and the impact of these emotions on self-awareness [33]. They try to maintain a healthy emotional life by reassessment of their emotions in different situations. Thereby, they can reduce their physical and mental health problems and control their emotions [33]. On the other hand, dysfunction and impairment in effective regulation of emotions is related to vulnerability to depression [34]. This increases mental problems in people [35], underlies many personal and social problems emerge in crisis.
Emotion regulation training could improve the capability of people with physical disabilities in terms of proper control and management of emotions in different situations. They can properly express their emotions in a timely manner. They can use effective coping strategies to overcome barriers and problems in life. As a result, their social relationships and psychological health are improved and they can assess their life positively and enjoy it. They can keep a balance between positive and negative emotions and feel satisfied with their lives. Ultimately, their positive emotions increase. Consequently, the level of depression reduces.
5. Conclusion
Emotions are crucial in life. Emotion regulation as a therapeutic approach modulates emotions, enhances self-esteem and positive social interactions in personal relationships, strengthens effective coping with stressful situations, and increases the opportunity to participate in social activities. As a result, emotion regulation training makes students with physical-motor disabilities aware of positive and negative emotions, timely acceptance and expression of such emotions. This training can also increase awareness on emotions, and teach how to control and overcome negative emotions resulting from interpersonal relationships, which consequently improves mental health.
The most important limitations were the purposive sampling method and consequently the quasi-experimental design of the study that reduced the possibility of generalizing the results to the whole population. It is suggested to evaluate the effect of teaching emotion regulation skills on other mental health variables in individuals with physical disabilities.
Ethical Considerations
Compliance with ethical guidelines
The informed consent was obtained from the students before enrollment in the research. The subjects were assured about the confidentiality of their information and it was explained to them that they can withdraw from the study at any stage.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Designing the treatment protocol, performing on patients and information, collecting the data: Dana Mohammad-Aminzadeh, Yousef Asamari, Seyed Jalal Younesi; Analyzing the data, writing the results: Mehdi Sharifi, Giuta Movallali; and Writing the basics of theory and background: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Lucas-Carrasco R, Eser E, Hao Y, McPherson KM, Green A, Kullmann L, et al. The Quality of Care and Support (QOCS) for people with disability scale: Development and psychometric properties. Research in Developmental Disabilities. 2011; 32(3):1212-25. [DOI:10.1016/j.ridd.2010.12.030] [PMID]
Aurora U. Study for determining laterality in children with motor disabilities in adapted physical activities. Procedia-Social and Behavioral Sciences. 2014; 117:646-52. [DOI:10.1016/j.sbspro.2014.02.276]
Salehi M, Tavakol HK, Shabani M, Ziaei T. The relationship between self-esteem and sexual self-concept in people with physical-motor disabilities. Iranian Red Crescent Medical Journal. 2015; 17(1):e25359. [DOI:10.5812/ircmj.25359] [PMID] [PMCID]
Brown RL, Turner RJ. Physical limitation and anger: Stress exposure and assessing the role of psychosocial resources. Society and Mental Health. 2012; 2(2):69-84. [DOI:10.1177/2156869312444441]
World Health Organization. World report on disability. Geneva: World Health Organization; 2011.
Bahrampour O, Ghamari M, Amiri Majd M. The effectiveness of cognitive behavioral group therapy on self-esteem and psychological well-being of young people with physical-motor disabilities. Society for Simulation in Healthcare. 2014; 2:2345-633.
Nosek MA, Hughes RB, Swedlund N, Taylor HB, Swank P. Self-esteem and women with disabilities. Social Science & Medicine. 2003; 56(8):1737-47. [DOI:10.1016/S0277-9536(02)00169-7]
Trani JF, Bakhshi P. Challenges for assessing disability prevalence: The case of Afghanistan. Journal of Disability Research. 2008; 2(1):44-64. [DOI:10.1016/j.alter.2007.10.003]
Scotland JL, McKenzie K, Cossar J, Murray A, Michie A. Recognition of facial expressions of emotion by adults with intellectual disability: Is there evidence for the emotion specificity hypothesis? Research in Developmental Disabilities. 2016; 48:69-78. [DOI:10.1016/j.ridd.2015.10.018] [PMID]
Casacalenda N, Perry JC, Looper K. Remission in major depressive disorder: A comparison of pharmacotherapy, psychotherapy, and control conditions. American Journal of Psychiatry. 2002; 159(8):1354-60. [DOI:10.1176/appi.ajp.159.8.1354] [PMID]
Berking M, Poppe C, Luhmann M, Wuppermann P, Jaggi V, Seifritz E. Is the association between various emotion-regulation skills and mental health mediated by the ability to modify emotions? Results from two cross-sectional studies. Journal of Behavior Therapy and Experimental Psychiatry. 2012; 43:931-7.
Liverant GI, Brown TA, Barlow DH, Roemer L. Emotion regulation in unipolar depression: The effects of acceptance and suppression of subjective emotional experience on the intensity and duration of sadness and negative affect. Behaviour Research and Therapy. 2008; 46(11):1201-9. [DOI:10.1016/j.brat.2008.08.001] [PMID]
Rude S, McCarthy C. Brief report. Cognition & Emotion. 2003; 17(5):799-806. [DOI:10.1080/02699930302283]
Solomon DA, Keller MB, Leon AC, Mueller TI, Lavori PW, Shea MT, et al. Multiple recurrences of major depressive disorder. American Journal of Psychiatry. 2000; 157(2):229-33. [DOI:10.1176/appi.ajp.157.2.229] [PMID]
Susa G, Mone I, Salagean D, Mihalca L, Benga O, Friedlmeier W. The relation between maternal perception of toddler emotion regulation abilities and emotion regulation abilities displayed by children in a frustration inducing task. Procedia-Social and Behavioral Sciences. 2014; 128:493-7. [DOI:10.1016/j.sbspro.2014.03.194]
Gross JJ, John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology. 2003; 85(2):348. [DOI:10.1037/0022-3514.85.2.348] [PMID]
Kingston J, Chadwick P, Meron D, Skinner TC. A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research. 2007; 62(3):297-300. [DOI:10.1016/j.jpsychores.2006.10.007] [PMID]
Koole SL. The psychology of emotion regulation: An integrative review. Cognition and Emotion. 2009; 23(1):4-41. [DOI:10.1080/02699930802619031]
Campos JJ, Walle EA, Dahl A, Main A. Reconceptualizing emotion regulation. Emotion Review. 2011; 3(1):26-35. [DOI:10.1177/1754073910380975]
Joormann J. Cognitive inhibition and emotion regulation in depression. Current Directions in Psychological Science. 2010; 19(3):161-6. [DOI:10.1177/0963721410370293]
Halperin E. Emotion, emotion regulation, and conflict resolution. Emotion Review. 2014; 6(1):3. [DOI:10.1177/1754073913491844]
Cheung EO, Gardner WL, Anderson JF. Emotionships: Examining people’s emotion-regulation relationships and their consequences for well-being. Social Psychological and Personality Science. 2015; 6(4):407-14. [DOI:10.1177/1948550614564223]
Shepherd L, Wild J. Emotion regulation, physiological arousal and PTSD symptoms in trauma-exposed individuals. Journal of Behavior Therapy and Experimental Psychiatry. 2014; 45(3):360-7. [DOI:10.1016/j.jbtep.2014.03.002] [PMID] [PMCID]
Berking M, Wirtz CM, Svaldi J, Hofmann SG. Emotion regulation predicts symptoms of depression over five years. Behaviour Research and Therapy. 2014; 57:13-20. [DOI:10.1016/j.brat.2014.03.003] [PMID]
Diedrich A, Grant M, Hofmann SG, Hiller W, Berking M. Self-compassion as an emotion regulation strategy in major depressive disorder. Behaviour Research and Therapy. 2014; 58:43-51. [DOI:10.1016/j.brat.2014.05.006] [PMID]
Gratz KL, Gunderson JG. Preliminary data on an acceptance-based emotion regulation group intervention for deliberate self-harm among women with borderline personality disorder. Behavior Therapy. 2006; 37(1):25-35. [DOI:10.1016/j.beth.2005.03.002] [PMID]
Corey MS, Corey G, Corey C. Groups: Process and practice. Boston: Cengage Learning; 2013.
Azkhosh M. [Psychological tests and clinical diagnosis (Persian)]. Tehran: Ravan; 2014.
Beck AT, Steer RA, Carbin MG. Psychometric properties of the beck depression inventory: Twenty-five years of evaluation. Clinical Psychology Review. 1988; 8(1):77-100. [DOI:10.1016/0272-7358(88)90050-5]
Berking M, Orth U, Wupperman P, Meier LL, Caspar F. Prospective effects of emotion-regulation skills on emotional adjustment. Journal of Counseling Psychology. 2008; 55(4):485-94. [DOI:10.1037/a0013589] [PMID]
Bardeen JR, Fergus TA. An examination of the incremental contribution of emotion regulation difficulties to health anxiety beyond specific emotion regulation strategies. Journal of Anxiety Disorders. 2014; 28(4):394-401. [DOI:10.1016/j.janxdis.2014.03.002] [PMID]
Isasi CR, Ostrovsky NW, Wills TA. The association of emotion regulation with lifestyle behaviors in inner-city adolescents. Eating Behaviors. 2013; 14(4):518-21. [DOI:10.1016/j.eatbeh.2013.07.009] [PMID] [PMCID]
Oshri A, Sutton TE, Clay-Warner J, Miller JD. Child maltreatment types and risk behaviors: Associations with attachment style and emotion regulation dimensions. Personality and Individual Differences. 2015; 73:127-33. [DOI:10.1016/j.paid.2014.09.015]
Tortella-Feliu M, Balle M, Sesé A. Relationships between negative affectivity, emotion regulation, anxiety, and depressive symptoms in adolescents as examined through structural equation modeling. Journal of Anxiety Disorders. 2010; 24(7):686-93. [DOI:10.1016/j.janxdis.2010.04.012] [PMID]
Rutherford HJ, Wallace NS, Laurent HK, Mayes LC. Emotion regulation in parenthood. Developmental Review. 2015; 36:1-14. [DOI:10.1016/j.dr.2014.12.008] [PMID] [PMCID]
Article type: Original Research Articles |
Subject:
Psychology
Received: 2018/10/23 | Accepted: 2019/01/29 | Published: 2019/06/1
Received: 2018/10/23 | Accepted: 2019/01/29 | Published: 2019/06/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
