
988368
Wed, Apr 17, 2024

Volume 19, Issue 4 (December 2021)
Iranian Rehabilitation Journal 2021, 19(4): 343-350 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hajmohammadi F, Hosseinifar M, Akbari A, Ghiasi F, Namvar H, Askari Ashtiani A. The Effect of Aquatic and Non-aquatic Balance Training on the Fall Risk of Patients With Grade 2 and 3 Knee Osteoarthritis: A Randomized Clinical Trial. Iranian Rehabilitation Journal 2021; 19 (4) :343-350
URL: http://irj.uswr.ac.ir/article-1-1196-en.html
URL: http://irj.uswr.ac.ir/article-1-1196-en.html
Farzaneh Hajmohammadi1 

 , Mohammad Hosseinifar * 1, Asghar Akbari1 , Fatemeh Ghiasi1 , Hassan Namvar1 , Ahmadreza Askari Ashtiani1
, Mohammad Hosseinifar * 1, Asghar Akbari1 , Fatemeh Ghiasi1 , Hassan Namvar1 , Ahmadreza Askari Ashtiani1
, Mohammad Hosseinifar * 1, Asghar Akbari1 , Fatemeh Ghiasi1 , Hassan Namvar1 , Ahmadreza Askari Ashtiani1
1- Deptment of Physical Therapy, Zahedan University of Medical Sciences, Zahedan, Iran.
Full-Text [PDF 613 kb]
(1194 Downloads)
| Abstract (HTML) (3577 Views)
Full-Text: (921 Views)
1. Introduction
The most common joint disease is osteoarthritis (OA) [1]. The knee joint is known as a common joint to be affected [1]. OA causes destructive changes in the articular cartilage, bone formation, subchondral bone sclerosis, and subchondral cysts in advanced forms [2]. This disease affects approximately 38% of the population aged over 65 years [3]. The symptoms of the disease are pain, swelling [4], muscle weakness [5], reduced range of motion, joint instability [6], decreased balance [7], joint stiffness, and functional disability [8].
Many intrinsic and extrinsic risk factors are responsible for falls in patients with knee OA. Intrinsic risk factors consist of biomechanical factors, such as balance, strength, instability, and proprioception, symptomatic knee osteoarthritis (symptoms such as pain, number of affected joints), and presence of comorbidities. Extrinsic risk factor includes the use of walking aids [9]. The balance disorder is one of the most critical risk factors for falls in people with knee OA [10]. However, other risk factors such as muscle weakness, medications, cognitive impairments, cardiovascular disorder, visual impairment, and environmental factors have been reported for falls, too [11]. Falling in the elderly results in physical injuries such as bone fracture and subchondral hematoma. It also has psychological consequences such as fear of falling and depression [12]. The primary reason for the low quality of life is fear of falling [13].
Several studies have been conducted on improving balance and reducing the risk of falls [14-17]. Hall et al. concluded that water-based exercise did not reduce falling risk compared with the control group that received computer skill training [16]. Arnold et al. found that combined water-based exercise and education were more effective than water-based exercise alone [17].
We conducted this study because of the critical role of the balance in reducing the risk of falls in patients with knee OA. No study has compared the effects of balance exercises on the risk of falls in two different environments. This study aimed to investigate the effect of balance exercises in aquatic and Non-aquatic environments. The center of gravity rises higher in the water environment, so the balance becomes more challenging. We hypothesized that balance exercises in the aquatic environment would further challenge the balance and subsequently improve it and decrease fall risk.
2. Materials and Methods
Study design
The study was a single-blind, randomized controlled trial. No changes were made to the trial design after it started.
Sampling method
Recruitment began in August 2019, and baseline testing and intervention were implemented in 3 groups from October to December 2019. Women with primary knee OA were recruited from the Razmjoo Moghaddam Clinic, general practitioners, physiotherapists’ offices, and public advertisement in Zahedan City, Iran. Volunteers contacted the researcher, and their eligibility was checked through a standardized telephone-administered checklist.
Women were selected based on the following inclusion criteria: being 45 to 65 years old, having grade 2 or 3 knee osteoarthritis according to Kellgren-Lawrence scale determined by radiological findings [18], having self-reported OA in the knee by asking the patient’s symptoms such as having pain in last month, and morning stiffness. The participants would not enter into this study if they had urinary incontinence, open wound, skin diseases, heart disease or uncontrolled hypertension, uncontrolled diabetes, any neurological diseases such as epilepsy, dizziness, stroke, or Parkinson disease. In addition, they would not enter if they used protective equipment, walking aid like a cane, had a joint injection in the last three months, lower extremity traumatic surgery, any recent knee injury, lower limb arthroplasty, participated in any physiotherapy or hydrotherapy treatment over the past three months [19-26]. The exclusion criteria were worsening the patient’s symptoms during treatment sessions and failure to complete treatment sessions by the patient.
Eighty-five women were assessed for eligibility. Twenty of them were not eligible based upon the inclusion and exclusion criteria. Seventeen were excluded following examination and radiography findings (did not have grade 2 or 3 OA). Finally, 48 women met the study criteria. After reading and signing a consent form, the participants were randomly allocated by permutation block method and random number table into three groups: aquatic balance training group (n=16), Non-aquatic balance training group (n=17), and control group (n=15). One subject from the aquatic exercise group, two subjects from the Non-aquatic exercise group, and two subjects from the control group left the study because of personal problems or reasons unrelated to the investigation. Finally, 15 women in the aquatic exercise group, 15 women in the Non-aquatic exercise group, and 13 women in the control group remained. The flowchart of choosing participants in the study is shown in Figure 1.

Outcome measures
The age, height, weight, and body mass index (BMI) of the participants were obtained and recorded. The outcome was fall risk score assessed by using Biodex balance system (BBS) (USA; New York, Biodex medical system; Inc.; SW 45-30 D-E6N: Balance System SD 950-304). BSS is a multi-pivotal device and has an unstable equilibrium platform that-tests postural stability and fall risk. This platform provides more than 20 degrees of deflection in the range of 360 degrees and freely moves in the anterior-posterior and medial-lateral axes [27].
Before the test began, the participants underwent an exercise trial with BSS to introduce the testing process. The participants were asked to stand on a platform with open eyes and bare feet, with hands crossed on the chest. They had to look directly at the device monitor. They were asked to stand up straight and just slightly change their body position when needed, but the position of the legs should remain constant. Legs’ position was recorded and is reused at the final evaluation. Device handles were available for personal safety, but the patient should not use them because contact with the handles will lead to failure in the trial. An instability level of 6 to 2 was used to assess the risk of falls [10].
Intervention
An exercise program of 12 individually-supervised sessions was performed for four weeks, three sessions per week. The control group received routine physiotherapy treatment, including TENS (transcutaneous electrical nerve stimulation) and hot packs (20 min); stretching exercises (10 min: 15 seconds in 3 times repeated) for hamstring, quadriceps, hip adductors, iliopsoas, and ankle plantar flexor muscles; and strengthening exercises (10 min: 10 seconds in 10 times repeated) for dorsiflexors and plantar flexor muscles of the ankle, hamstring muscle, quadriceps muscle, hip adductors, and hip abductors muscles. In addition to receiving routine physiotherapy exercises, the aquatic and Non-aquatic balance training groups performed special balance exercises in the aquatic and Non-aquatic environments, respectively.
Aquatic balance training included walking in the water forward, backward, and sideways, marching, standing on the toes, walking on the toes, single-leg stance with and without the foam pool, tandem stance, tandem walking, two-legged stance on a noodle, and single-leg stance on noodle. Non-aquatic balance training included standing on the tilt board, shifting the trunk forward and backward on the tilt board, standing on the tilt board and rotating the trunk on both sides, tandem stance, tandem walking, reaching training, and single-leg stance. Exercises became more difficult in the third week with the patient’s eyes closed and doing exercises on the softer surface (foam) in this group.
Data analysis
Statistical analysis was done in SPSS v. 16 (SPSS Inc., Chicago, IL, USA). The normality of all data was examined by the Kolmogorov-Simonov test (P>0.05). Between-group comparisons were performed using 1-way ANOVA. Within-group comparisons were performed using paired t-test. Statistical significance was accepted at a Ρ<0.05.
3. Results
Table 1 presents the demographic data of the subjects. The distribution of study data was normal (P>0.05).

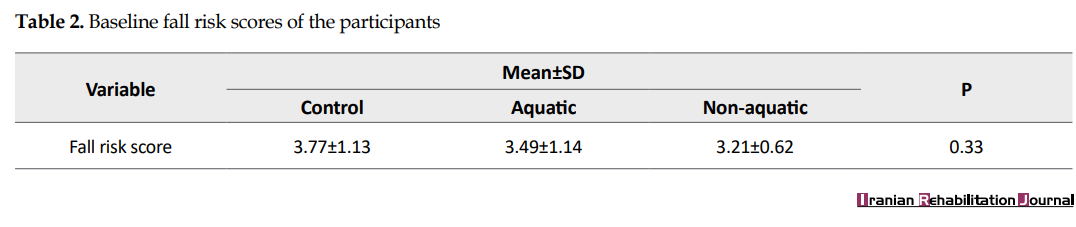
There were no significant differences between the three groups with regard to age, weight, height, and BMI. All data are presented as Mean±SD. Table 2 presents baseline fall risk scores in the aquatic, Non-aquatic balance, and control groups (before the intervention). There were no significant differences between groups, showing that all groups were matched before the intervention.
Between-group comparison
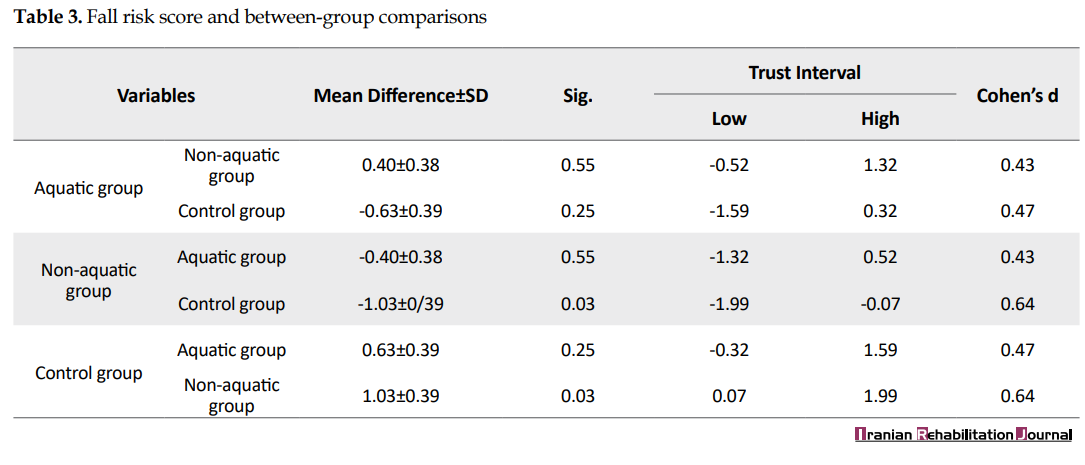
After the intervention, the results of the 1-way ANOVA test showed no significant difference between aquatic and Non-aquatic balance training groups (effect size Cohen’s d=0.43) as well as between aquatic balance training and control groups (P>0.05) (effect size Cohen’s d=0.47). However, the Non-aquatic balance training group had a statistically significant difference with the control (P<0.05) (effect size Cohen’s d=0.64) (Table 3).
Within-group comparison
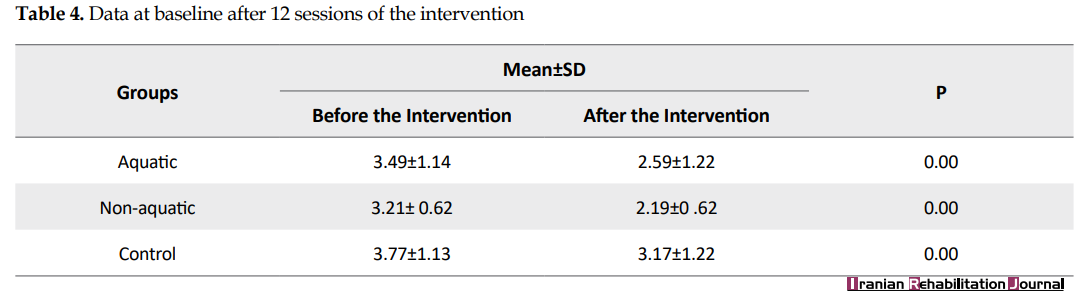
The paired sample t-test showed significant differences between the three groups regarding baseline and after interventions fall risk scores (Table 4).
4. Discussion
All groups improved in the risk of falls compared to before the intervention. This improvement could be due to strengthening and stretching exercises that were included in routine physiotherapy. There was no difference between aquatic and Non-aquatic balance training groups. Although the aquatic balance training group did not differ from the control group, the Non-aquatic balance training group reported an improvement in the fall risk score compared to the control group.
The fall risk score was obtained using a Biodex balance system in this study. Some previous studies also measured the risk of falling using this device [10, 28, 29]. They showed that water-based exercises significantly decreased fall risk scores. These studies compared water-based exercise with the control group [30, 31]. In a study, Nissim et al. divided 42 healthy individuals into three groups. The aquatic physical intervention group was trained based on Tai Chi movements. The second group was the on-land physical intervention group. Subjects in the nonphysical intervention group performed some of the imagery movements used in the Tai Chi method while sitting on a chair. The results showed that the second and third groups improved less than the first group on fall risk score [30]. Nevertheless, it is essential to highlight that our study subjects suffered from knee osteoarthritis, thus differing from that study.
In a study, Zmanian et al. studied the effects of water-based exercises on quadriceps muscle strength and the risk of falls in women with chronic knee OA [31]. There were three groups in this study. The first and second group programs were performed in the shallow and deep water, respectively. The third group did not receive any intervention. This study showed that both intervention groups had significantly different outcomes compared to the control group. The shallow-water exercise group also showed a significantly different outcome from the deep-water exercise group [31]. Both intervention groups achieved significant improvement in the results, which were in line with the results of our study.
Hall et al. studied the effects of water-based exercise to improve fall risks in patients with lower extremity OA. The intervention group performed water exercises for 24 sessions, and the control group performed computer skills during the same period. The risk of falling decreased in both groups. We did not see any significant decrease in fall risk in the water-based group compared to the control group [16]. Although the control group of this study did not have an organized exercise program under the supervision of a physiotherapist, the results were consistent with the results of our research. Another study result similar to ours was the study of Douris et al. They found that using lower extremity exercises in both environments improved balance and reduced the risk of falls. Participants in this study were 11 older people. Balance was measured using the Berg balance scale. It is essential to recognize that the BBS is a sensitive predictor of fall status [32].
To decrease the risk of falls, you need to focus on its risk factors. In our study, we tried to focus on balance improvement and consequently reducing the risk of falling. The important point in our study was the difference in the environment for balance exercises. We hypothesized that the aquatic environment disturbs the balance because the center of gravity is affected. Buoyancy forces unload body weigh 68%±3% at the xiphoid process depth and 39%±4% at the greater trochanter depth [33]. The water level in our study was at xiphoid depth. Thus, the unloading of body weight and the higher whole-body center of gravity [33] disturb the balance. We thought that doing balance exercises in such an environment would further challenge the balance and improve it.
Also, the dynamic characteristic of the water environment (hydrostatic pressure) stimulates sensory inputs through the somatosensory and vestibular systems. This feature of water creates resistance to movement and increases balance [34]. But contrary to what we thought, the Non-aquatic balance exercises group showed more significant improvement than the control group. Perhaps doing balance exercises on the land (because of weight-bearing position) more stimulates joint proprioceptors. In addition, lower limbs muscle activity is greater than that in the aquatic environment. The Non-aquatic treatment program was performed on land, and the risk of falling was also measured on the ground. The aquatic treatment program was performed in the water, and the risk of falling was measured on the land. This factor may affect the final result between the two groups.
Contrary to our hypothesis, the outcome of the aquatic training group did not significantly differ from the control group. Lack of normal muscle strength reduces the ability to return to balance after external disturbances [35]. Therefore, there is an important relationship between neuromuscular factors and postural control in knee OA patients [36]. Patients with muscle weakness have less muscle mass, incomplete muscle activity, decreased muscle spindle sensitivity and decreased sensory units (reduction in the number of mechanoreceptors) [36]. Therefore, it is suggested that improving muscle strength through exercise may lead to improved postural control. Also, the high strength of flexor and extensor muscles reduces the risk of falls [35]. Although we did not measure muscle strength in this study, the results indirectly indicated increased muscle strength in all groups. It is suggested that future studies measure muscle strength objectively. Another limitation of our study was the lack of a follow-up period for patients. It is recommended that future studies consider this component in their studies.
5. Conclusion
The results of our study support that the risk of falls will reduce after exercise in both environments. But the Non-aquatic exercises group had a better result. Therefore, due to the high costs of using the pool and water-based treatments, exercises can be prescribed in a land environment.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Human Ethics Committee of Zahedan University Of Medical Sciences (Code: IR.ZAUMS.REC.1398.222) and was registered with the region’s Clinical Trials Registry (Code: IRCT20160531028186N4).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Refrences:
The most common joint disease is osteoarthritis (OA) [1]. The knee joint is known as a common joint to be affected [1]. OA causes destructive changes in the articular cartilage, bone formation, subchondral bone sclerosis, and subchondral cysts in advanced forms [2]. This disease affects approximately 38% of the population aged over 65 years [3]. The symptoms of the disease are pain, swelling [4], muscle weakness [5], reduced range of motion, joint instability [6], decreased balance [7], joint stiffness, and functional disability [8].
Many intrinsic and extrinsic risk factors are responsible for falls in patients with knee OA. Intrinsic risk factors consist of biomechanical factors, such as balance, strength, instability, and proprioception, symptomatic knee osteoarthritis (symptoms such as pain, number of affected joints), and presence of comorbidities. Extrinsic risk factor includes the use of walking aids [9]. The balance disorder is one of the most critical risk factors for falls in people with knee OA [10]. However, other risk factors such as muscle weakness, medications, cognitive impairments, cardiovascular disorder, visual impairment, and environmental factors have been reported for falls, too [11]. Falling in the elderly results in physical injuries such as bone fracture and subchondral hematoma. It also has psychological consequences such as fear of falling and depression [12]. The primary reason for the low quality of life is fear of falling [13].
Several studies have been conducted on improving balance and reducing the risk of falls [14-17]. Hall et al. concluded that water-based exercise did not reduce falling risk compared with the control group that received computer skill training [16]. Arnold et al. found that combined water-based exercise and education were more effective than water-based exercise alone [17].
We conducted this study because of the critical role of the balance in reducing the risk of falls in patients with knee OA. No study has compared the effects of balance exercises on the risk of falls in two different environments. This study aimed to investigate the effect of balance exercises in aquatic and Non-aquatic environments. The center of gravity rises higher in the water environment, so the balance becomes more challenging. We hypothesized that balance exercises in the aquatic environment would further challenge the balance and subsequently improve it and decrease fall risk.
2. Materials and Methods
Study design
The study was a single-blind, randomized controlled trial. No changes were made to the trial design after it started.
Sampling method
Recruitment began in August 2019, and baseline testing and intervention were implemented in 3 groups from October to December 2019. Women with primary knee OA were recruited from the Razmjoo Moghaddam Clinic, general practitioners, physiotherapists’ offices, and public advertisement in Zahedan City, Iran. Volunteers contacted the researcher, and their eligibility was checked through a standardized telephone-administered checklist.
Women were selected based on the following inclusion criteria: being 45 to 65 years old, having grade 2 or 3 knee osteoarthritis according to Kellgren-Lawrence scale determined by radiological findings [18], having self-reported OA in the knee by asking the patient’s symptoms such as having pain in last month, and morning stiffness. The participants would not enter into this study if they had urinary incontinence, open wound, skin diseases, heart disease or uncontrolled hypertension, uncontrolled diabetes, any neurological diseases such as epilepsy, dizziness, stroke, or Parkinson disease. In addition, they would not enter if they used protective equipment, walking aid like a cane, had a joint injection in the last three months, lower extremity traumatic surgery, any recent knee injury, lower limb arthroplasty, participated in any physiotherapy or hydrotherapy treatment over the past three months [19-26]. The exclusion criteria were worsening the patient’s symptoms during treatment sessions and failure to complete treatment sessions by the patient.
Eighty-five women were assessed for eligibility. Twenty of them were not eligible based upon the inclusion and exclusion criteria. Seventeen were excluded following examination and radiography findings (did not have grade 2 or 3 OA). Finally, 48 women met the study criteria. After reading and signing a consent form, the participants were randomly allocated by permutation block method and random number table into three groups: aquatic balance training group (n=16), Non-aquatic balance training group (n=17), and control group (n=15). One subject from the aquatic exercise group, two subjects from the Non-aquatic exercise group, and two subjects from the control group left the study because of personal problems or reasons unrelated to the investigation. Finally, 15 women in the aquatic exercise group, 15 women in the Non-aquatic exercise group, and 13 women in the control group remained. The flowchart of choosing participants in the study is shown in Figure 1.
Outcome measures
The age, height, weight, and body mass index (BMI) of the participants were obtained and recorded. The outcome was fall risk score assessed by using Biodex balance system (BBS) (USA; New York, Biodex medical system; Inc.; SW 45-30 D-E6N: Balance System SD 950-304). BSS is a multi-pivotal device and has an unstable equilibrium platform that-tests postural stability and fall risk. This platform provides more than 20 degrees of deflection in the range of 360 degrees and freely moves in the anterior-posterior and medial-lateral axes [27].
Before the test began, the participants underwent an exercise trial with BSS to introduce the testing process. The participants were asked to stand on a platform with open eyes and bare feet, with hands crossed on the chest. They had to look directly at the device monitor. They were asked to stand up straight and just slightly change their body position when needed, but the position of the legs should remain constant. Legs’ position was recorded and is reused at the final evaluation. Device handles were available for personal safety, but the patient should not use them because contact with the handles will lead to failure in the trial. An instability level of 6 to 2 was used to assess the risk of falls [10].
Intervention
An exercise program of 12 individually-supervised sessions was performed for four weeks, three sessions per week. The control group received routine physiotherapy treatment, including TENS (transcutaneous electrical nerve stimulation) and hot packs (20 min); stretching exercises (10 min: 15 seconds in 3 times repeated) for hamstring, quadriceps, hip adductors, iliopsoas, and ankle plantar flexor muscles; and strengthening exercises (10 min: 10 seconds in 10 times repeated) for dorsiflexors and plantar flexor muscles of the ankle, hamstring muscle, quadriceps muscle, hip adductors, and hip abductors muscles. In addition to receiving routine physiotherapy exercises, the aquatic and Non-aquatic balance training groups performed special balance exercises in the aquatic and Non-aquatic environments, respectively.
Aquatic balance training included walking in the water forward, backward, and sideways, marching, standing on the toes, walking on the toes, single-leg stance with and without the foam pool, tandem stance, tandem walking, two-legged stance on a noodle, and single-leg stance on noodle. Non-aquatic balance training included standing on the tilt board, shifting the trunk forward and backward on the tilt board, standing on the tilt board and rotating the trunk on both sides, tandem stance, tandem walking, reaching training, and single-leg stance. Exercises became more difficult in the third week with the patient’s eyes closed and doing exercises on the softer surface (foam) in this group.
Data analysis
Statistical analysis was done in SPSS v. 16 (SPSS Inc., Chicago, IL, USA). The normality of all data was examined by the Kolmogorov-Simonov test (P>0.05). Between-group comparisons were performed using 1-way ANOVA. Within-group comparisons were performed using paired t-test. Statistical significance was accepted at a Ρ<0.05.
3. Results
Table 1 presents the demographic data of the subjects. The distribution of study data was normal (P>0.05).
There were no significant differences between the three groups with regard to age, weight, height, and BMI. All data are presented as Mean±SD. Table 2 presents baseline fall risk scores in the aquatic, Non-aquatic balance, and control groups (before the intervention). There were no significant differences between groups, showing that all groups were matched before the intervention.
Between-group comparison
After the intervention, the results of the 1-way ANOVA test showed no significant difference between aquatic and Non-aquatic balance training groups (effect size Cohen’s d=0.43) as well as between aquatic balance training and control groups (P>0.05) (effect size Cohen’s d=0.47). However, the Non-aquatic balance training group had a statistically significant difference with the control (P<0.05) (effect size Cohen’s d=0.64) (Table 3).
Within-group comparison
The paired sample t-test showed significant differences between the three groups regarding baseline and after interventions fall risk scores (Table 4).
4. Discussion
All groups improved in the risk of falls compared to before the intervention. This improvement could be due to strengthening and stretching exercises that were included in routine physiotherapy. There was no difference between aquatic and Non-aquatic balance training groups. Although the aquatic balance training group did not differ from the control group, the Non-aquatic balance training group reported an improvement in the fall risk score compared to the control group.
The fall risk score was obtained using a Biodex balance system in this study. Some previous studies also measured the risk of falling using this device [10, 28, 29]. They showed that water-based exercises significantly decreased fall risk scores. These studies compared water-based exercise with the control group [30, 31]. In a study, Nissim et al. divided 42 healthy individuals into three groups. The aquatic physical intervention group was trained based on Tai Chi movements. The second group was the on-land physical intervention group. Subjects in the nonphysical intervention group performed some of the imagery movements used in the Tai Chi method while sitting on a chair. The results showed that the second and third groups improved less than the first group on fall risk score [30]. Nevertheless, it is essential to highlight that our study subjects suffered from knee osteoarthritis, thus differing from that study.
In a study, Zmanian et al. studied the effects of water-based exercises on quadriceps muscle strength and the risk of falls in women with chronic knee OA [31]. There were three groups in this study. The first and second group programs were performed in the shallow and deep water, respectively. The third group did not receive any intervention. This study showed that both intervention groups had significantly different outcomes compared to the control group. The shallow-water exercise group also showed a significantly different outcome from the deep-water exercise group [31]. Both intervention groups achieved significant improvement in the results, which were in line with the results of our study.
Hall et al. studied the effects of water-based exercise to improve fall risks in patients with lower extremity OA. The intervention group performed water exercises for 24 sessions, and the control group performed computer skills during the same period. The risk of falling decreased in both groups. We did not see any significant decrease in fall risk in the water-based group compared to the control group [16]. Although the control group of this study did not have an organized exercise program under the supervision of a physiotherapist, the results were consistent with the results of our research. Another study result similar to ours was the study of Douris et al. They found that using lower extremity exercises in both environments improved balance and reduced the risk of falls. Participants in this study were 11 older people. Balance was measured using the Berg balance scale. It is essential to recognize that the BBS is a sensitive predictor of fall status [32].
To decrease the risk of falls, you need to focus on its risk factors. In our study, we tried to focus on balance improvement and consequently reducing the risk of falling. The important point in our study was the difference in the environment for balance exercises. We hypothesized that the aquatic environment disturbs the balance because the center of gravity is affected. Buoyancy forces unload body weigh 68%±3% at the xiphoid process depth and 39%±4% at the greater trochanter depth [33]. The water level in our study was at xiphoid depth. Thus, the unloading of body weight and the higher whole-body center of gravity [33] disturb the balance. We thought that doing balance exercises in such an environment would further challenge the balance and improve it.
Also, the dynamic characteristic of the water environment (hydrostatic pressure) stimulates sensory inputs through the somatosensory and vestibular systems. This feature of water creates resistance to movement and increases balance [34]. But contrary to what we thought, the Non-aquatic balance exercises group showed more significant improvement than the control group. Perhaps doing balance exercises on the land (because of weight-bearing position) more stimulates joint proprioceptors. In addition, lower limbs muscle activity is greater than that in the aquatic environment. The Non-aquatic treatment program was performed on land, and the risk of falling was also measured on the ground. The aquatic treatment program was performed in the water, and the risk of falling was measured on the land. This factor may affect the final result between the two groups.
Contrary to our hypothesis, the outcome of the aquatic training group did not significantly differ from the control group. Lack of normal muscle strength reduces the ability to return to balance after external disturbances [35]. Therefore, there is an important relationship between neuromuscular factors and postural control in knee OA patients [36]. Patients with muscle weakness have less muscle mass, incomplete muscle activity, decreased muscle spindle sensitivity and decreased sensory units (reduction in the number of mechanoreceptors) [36]. Therefore, it is suggested that improving muscle strength through exercise may lead to improved postural control. Also, the high strength of flexor and extensor muscles reduces the risk of falls [35]. Although we did not measure muscle strength in this study, the results indirectly indicated increased muscle strength in all groups. It is suggested that future studies measure muscle strength objectively. Another limitation of our study was the lack of a follow-up period for patients. It is recommended that future studies consider this component in their studies.
5. Conclusion
The results of our study support that the risk of falls will reduce after exercise in both environments. But the Non-aquatic exercises group had a better result. Therefore, due to the high costs of using the pool and water-based treatments, exercises can be prescribed in a land environment.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Human Ethics Committee of Zahedan University Of Medical Sciences (Code: IR.ZAUMS.REC.1398.222) and was registered with the region’s Clinical Trials Registry (Code: IRCT20160531028186N4).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Refrences:
- Michael JW, Schlüter-Brust KU, Eysel P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Deutsches Arzteblatt International. 2010; 107(9):152-62. [DOI:10.3238/arztebl.2010.0152] [PMID] [PMCID]
- Lespasio MJ, Piuzzi NS, Husni ME, Muschler GF, Guarino AJ, Mont MA. Knee osteoarthritis: A primer. The Permanente Journal. 2017; 21:16-183. [DOI:10.7812/TPP/16-183] [PMID] [PMCID]
- Cho HJ, Morey V, Kang JY, Kim KW, Kim TK. Prevalence and risk factors of spine, shoulder, hand, hip, and knee osteoarthritis in community-dwelling Koreans older than age 65 years. Clinical Orthopaedics and Related Research. 2015; 473(10):3307-14. [DOI:10.1007/s11999-015-4450-3] [PMID] [PMCID]
- Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT, Giannini EH, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis & Rheumatism. 1998; 41(5):778-99. [DOI:10.1002/1529-0131(199805)41:53.0.CO;2-V]
- O’Reilly S, Jones A, Doherty M. Muscle weakness in osteoarthritis. Current Opinion in Rheumatology. 1997; 9(3):259-62. [DOI:10.1097/00002281-199705000-00014] [PMID]
- Baker K, McAlindon T. Exercise for knee osteoarthritis. Current Opinion in Rheumatology. 2000; 12(5):456-63. [DOI:10.1097/00002281-200009000-00020] [PMID]
- Hinman RS, Bennell KL, Metcalf BR, Crossley KM. Balance impairments in individuals with symptomatic knee osteoarthritis: A comparison with matched controls using clinical tests. Rheumatology. 2002; 41(12):1388-94. [DOI:10.1093/rheumatology/41.12.1388] [PMID]
- Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Annals of the Rheumatic Diseases. 2014; 73(7):1323-30. [DOI:10.1136/annrheumdis-2013-204627] [PMID]
- Manlapaz DG, Sole G, Jayakaran P, Chapple CM. Risk factors for falls in adults with knee osteoarthritis: A systematic review. PM & R. 2019; 11(7):745-57. [DOI:10.1002/pmrj.12066] [PMID]
- Khalaj N, Abu Osman NA, Mokhtar AH, Mehdikhani M, Wan Abas WA. Balance and risk of fall in individuals with bilateral mild and moderate knee osteoarthritis. PloS One. 2014; 9(3):e92270. [DOI:10.1371/journal.pone.0092270] [PMID] [PMCID]
- Moylan KC, Binder EF. Falls in older adults: Risk assessment, management and prevention. The American Journal of Medicine. 2007; 120(6):493.e1-6. [DOI:10.1016/j.amjmed.2006.07.022] [PMID]
- Ng CT, Tan MP. Osteoarthritis and falls in the older person. Age and Ageing. 2013; 42(5):561-6. [DOI:10.1093/ageing/aft070] [PMID]
- Suzuki M, Ohyama N, Yamada K, Kanamori M. The relationship between fear of falling, activities of daily living and quality of life among elderly individuals. Nursing & Health Sciences. 2002; 4(4):155-61. [DOI:10.1046/j.1442-2018.2002.00123.x] [PMID]
- Avelar NC, Bastone AC, Alcântara MA, Gomes WF. Effectiveness of aquatic and non-aquatic lower limb muscle endurance training in the static and dynamic balance of elderly people. Brazilian Journal of Physical Therapy. 2010; 14(3):229-36. [DOI:10.1590/S1413-35552010000300007] [PMID]
- Devereux K, Robertson D, Briffa NK. Effects of a water-based program on women 65 years and over: a randomised controlled trial. Australian Journal of Physiotherapy. 2005; 51(2):102-8. [DOI:10.1016/S0004-9514(05)70038-6]
- Hale LA, Waters D, Herbison P. A randomized controlled trial to investigate the effects of water-based exercise to improve falls risk and physical function in older adults with lower-extremity osteoarthritis. Archives of Physical Medicine and Rehabilitation. 2012; 93(1):27-34. [DOI:10.1016/j.apmr.2011.08.004] [PMID]
- Arnold CM, Faulkner RA. The effect of aquatic exercise and education on lowering fall risk in older adults with hip osteoarthritis. Journal of Aging and Physical Activity. 2010; 18(3):245-60. [DOI:10.1123/japa.18.3.245] [PMID]
- Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clinical Orthopaedics and Related Research. 2016; 474(8):1886-93. [DOI:10.1007/s11999-016-4732-4] [PMID] [PMCID]
- Dias JM, Cisneros L, Dias R, Fritsch C, Gomes W, Pereira L, et al. Hydrotherapy improves pain and function in older women with knee osteoarthritis: A randomized controlled trial. Brazilian Journal of Physical Therapy. 2017; 21(6):449-56. [DOI:10.1016/j.bjpt.2017.06.012] [PMID] [PMCID]
- Lund H, Weile U, Christensen R, Rostock B, Downey A, Bartels EM, et al. A randomized controlled trial of aquatic and land-based exercise in patients with knee osteoarthritis. Journal of Rehabilitation Medicine. 2008; 40(2):137-44. [DOI:10.2340/16501977-0134] [PMID]
- Barker AL, Talevski J, Morello RT, Nolan GA, De Silva RD, Briggs AM. Jumping into the deep-end: results from a pilot impact evaluation of a community-based aquatic exercise program. Clinical Rheumatology. 2016; 35(6):1593-601. [DOI:10.1007/s10067-015-3096-6] [PMID]
- Bressel E, Wing JE, Miller AI, Dolny DG. High-intensity interval training on an aquatic treadmill in adults with osteoarthritis: Effect on pain, balance, function, and mobility. The Journal of Strength & Conditioning Research. 2014; 28(8):2088-96. [DOI:10.1519/JSC.0000000000000258] [PMID]
- Braghin RD, Libardi EC, Junqueira C, Nogueira–Barbosa MH, de Abreu DC. Exercise on balance and function for knee osteoarthritis: A randomized controlled trial. Journal of Bodywork and Movement Therapies. 2018; 22(1):76-82. [DOI:10.1016/j.jbmt.2017.04.006] [PMID]
- Park HJ, Ko S, Hong HM, Ok E, Lee JI. Factors related to standing balance in patients with knee osteoarthritis. Annals of Rehabilitation Medicine. 2013; 37(3):373-8. [DOI:10.5535/arm.2013.37.3.373] [PMID] [PMCID]
- Tas S, Guneri S, Baki A, Yildirim T, Kaymak B, Erden Z. Effects of severity of osteoarthritis on the temporospatial gait parameters in patients with knee osteoarthritis. Acta Orthopaedica et Traumatologica Turcica. 2014; 48(6):635-41. [DOI:10.3944/AOTT.2014.13.0071] [PMID]
- Reis JG, Gomes MM, Neves TM, Petrella M, Oliveira RD, Abreu DC. Evaluation of postural control and quality of life in elderly women with knee osteoarthritis. Revista Brasileira de Reumatologia. 2014; 54(3):208-12. [DOI:10.1016/j.rbre.2013.11.001]
- Arnold BL, Schmitz RJ. Examination of balance measures produced by the biodex stability system. Journal of Athletic Training. 1998; 33(4):323-7. [PMCIE]
- Lawson T, Morrison A, Blaxland S, Wenman M, Schmidt CG, Hunt MA. Laboratory-based measurement of standing balance in individuals with knee osteoarthritis: A systematic review. Clinical Biomechanics. 2015; 30(4):330-42. [DOI:10.1016/j.clinbiomech.2015.02.011] [PMID]
- Khalaj N, Abu Osman NA, Mokhtar AH, George J, Wan Abas WA. Effect of intra-articular hyaluronic injection on postural stability and risk of fall in patients with bilateral knee osteoarthritis. The Scientific World Journal. 2014; 2014:815184. [DOI:10.1155/2014/815184] [PMID] [PMCID]
- Nissim M, Livny A, Barmatz C, Tsarfaty G, Berner Y, Sacher Y, et al. Effects of aquatic physical intervention on fall risk, working memory and hazard-perception as pedestrians in older people: A pilot trial. BMC Geriatrics. 2020; 20(1):74. [DOI:10.1186/s12877-020-1477-4] [PMID] [PMCID]
- Zamanian F, Sedighi Z, Satar S, Leila Z. The role of aquatic exercise on strength of quadriceps muscle and falling risk in elderly people. Research Journal of Sport Sciences. 2013; 1(1):26-34. https://research.iaun.ac.ir/pd/sattar737/pdfs/PaperM_9212.pdf
- Douris P, Southard V, Varga C, Schauss W, Gennaro C, Reiss A. The effect of land and aquatic exercise on balance scores in older adults. Journal of Geriatric Physical Therapy. 2003; 26(1):3-6. [DOI:10.1519/00139143-200304000-00001]
- Harrison RA, Hillman M, Bulstrode S. Loading of the lower limb when walking partially immersed: Implications for clinical practice. Physiotherapy. 1992; 78(3):164-6. [DOI:10.1016/S0031-9406(10)61377-6]
- Louder T, Bressel E, Baldwin M, Dolny DG, Gordin R, Miller A. Effect of aquatic immersion on static balance. International Journal of Aquatic Research and Education. 2014; 8(1):6. [DOI:10.25035/ijare.08.01.06]
- de Zwart AH, van der Esch M, Pijnappels MA, Hoozemans MJ, van der Leeden M, Roorda LD, et al. Falls associated with muscle strength in patients with knee osteoarthritis and self-reported knee instability. The Journal of Rheumatology. 2015; 42(7):1218-23. [DOI:10.3899/jrheum.140517] [PMID]
- Sanchez-Ramirez DC, van der Leeden M, Knol DL, van der Esch M, Roorda LD, Verschueren S, et al. Association of postural control with muscle strength, proprioception, self-reported knee instability and activity limitations in patients with knee osteoarthritis. Journal of Rehabilitation Medicine. 2013; 45(2):192-7. [DOI:10.2340/16501977-1087] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2020/07/2 | Accepted: 2021/04/28 | Published: 2021/12/1
Received: 2020/07/2 | Accepted: 2021/04/28 | Published: 2021/12/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
