
988368
Fri, Apr 19, 2024

Volume 19, Issue 3 (September 2021)
Iranian Rehabilitation Journal 2021, 19(3): 221-230 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dabiri Golchin M, Mirzaie H, Hosseini S A. Effects of Occupational Therapy Interventions on Improving Play Performance in Children With Attention-Deficit/Hyperactivity Disorder (ADHD): A Systematic Review. Iranian Rehabilitation Journal 2021; 19 (3) :221-230
URL: http://irj.uswr.ac.ir/article-1-1243-en.html
URL: http://irj.uswr.ac.ir/article-1-1243-en.html



1- Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Keywords: Systematic review, Attention-Deficit/Hyperactivity Disorder, Play, Playthings, Occupational therapy
Full-Text [PDF 633 kb]
(2595 Downloads)
| Abstract (HTML) (2935 Views)
Full-Text: (1942 Views)
1. Introduction
Attention-deficit/hyperactivity disorder (ADHD) is highly prevalent among childhood behavioral disorders worldwide [1, 2]. This illness is a neurodevelopmental disorder diagnosed by three main characteristics: Inattention, hyperactivity, and impulsivity. These characteristics are the core symptoms of this neurodevelopmental disorder [3]. This disorder is not confined to childhood, and its impairments can last through life with an effect on educational performance [4], work [5], and other life domains [6]. It also leads to a lower quality of life than other peers [7, 8]. Children with ADHD also have difficulties in their playing patterns, especially their social play [9, 10, 11].
Play is a primary occupation for a child that is not only necessary for academic learning and cognitive skills but also is crucial for the child’s development [12, 13]. The play has enormous benefits for a child’s development [14, 15]. It relates to all developmental dimensions such as cognitive [16], emotional [17], language [18], social [19], and motor skills [20]. It is common to use play as an intervention to improve other skills such as executive functions, learning, or social skills [21, 22, 23]. Couch and Deitz reported that most occupational therapists address play as an essential concept in a child’s life, but they rarely put objectives and goals to improve one’s play. Instead, they usually benefit from play as a means and medium to do their interventions or used it as a reinforcement for a child [24]. Although this paper was published in 1998, the concept of “play for the sake of play” did not enter much literature, as we can see in the NICE (the National Institute for Health and Care Excellence) newest guideline for ADHD [25].
Children with ADHD have severe problems in their social participation, especially in their playing [26]. “Social play” is greatly affected in these children [27]. About 56% of children with ADHD have no friend, as 32% of typically developed children do not have a friend [9], while “pretend play” is a building block for making personal interactions and communications [28]. Although sometimes play therapy improves ADHD signs like hyperactivity and attention deficit [29], there are some problems in play patterns for children with ADHD, and interventions are needed to improve this area [30, 31, 32].
Play interventions have a fixed position in occupational therapy interventions for children with ADHD [31, 33]. The play has been reviewed as an outcome in other studies, and a systematic review was done in children with autism spectrum disorder children to check the effective interventions which can facilitate and improve social play in the children [34]. Having a review of the ADHD population will help the occupational therapist to access better evidence and will improve their evidence-based practice [35]. As mentioned earlier, play may be used to improve other skills, but in this study, we see play as the primary outcome.
2. Materials and Methods
Search strategy
These four databases were searched from inception to March 2020: PubMed, Web of Science, Scopus, and Elsevier. The used keywords in MeSH terms were “occupational therapy,” “play and playthings,” and “child mental disorders.” Based on MeSH definitions, ADHD is a subcategory of mental disorders, the wider concept (child mental disorders) searched not to miss any studies. The search was done among English and Persian written articles (peer-reviews) only. No other limitation was made in the search process. The article’s references were reviewed to find potential studies to include in the study. The whole process of searching and sampling took four months.
Study selection
The mentioned databases were searched by all authors independently. All search results were imported to the Rayyan QCRI online application. The first and second authors reviewed titles and abstracts in the application independently while the blind mode was on, so the other authors could not see the first one’s decisions. Where disagreement was seen for including an article, the third author made the decision. The inclusion criteria were as follows: 1) participants should be aged 2-12 years (MeSH term definition of a child, PubMed), 2) diagnosis of ADHD, 3) play should be mentioned as the outcome of the study and be a dependent variable using an assessment tool to be measured, 4) any occupational therapy intervention is included, 5) articles should be in English or Persian only, 6) non-full-text and non-peer-reviewed articles are not included, 6) all experimental studies are welcomed. Non-experimental studies will not enter the study because they cannot show the effect of interventions.
After reviewing articles and deciding about their inclusion, the full text of the articles was studied. Then, some of the articles were excluded. All authors extracted the final included articles. A form was made to organize articles data regarding the participants’ information like their diagnosis, age, and gender, the intervention features like the frequency, duration, and follow-up, and the used assessment tools for playing.
Quality assessment
Firstly, the level of evidence was estimated based on the Centre of Evidence-Based Medicine (2009) definition, which is related to the study design. We also used the research pyramid. This new research pyramid critics the traditional single-hierarchy evidence model (Arbesman-2008).
Preferred Reporting Item for Systematic Review and A meta-analysis (PRISMA) statement (Appendix A) was used in the next step. A protocol was registered on the Prospero database (CRD42020172447).
3. Results
First, we extracted 103 articles. One extra article was added from other sources. After removing duplicates, 83 remained that 2 of which were not English or Persian. Fifty-one studies were excluded based on their titles and abstracts. Thirty articles were selected to be read in their full text which 6 of them remained because of meeting the mentioned inclusion and exclusion criteria. Figure 1 demonstrates the process that we passed to get these 6 articles.

The included articles are shown in Table 1.
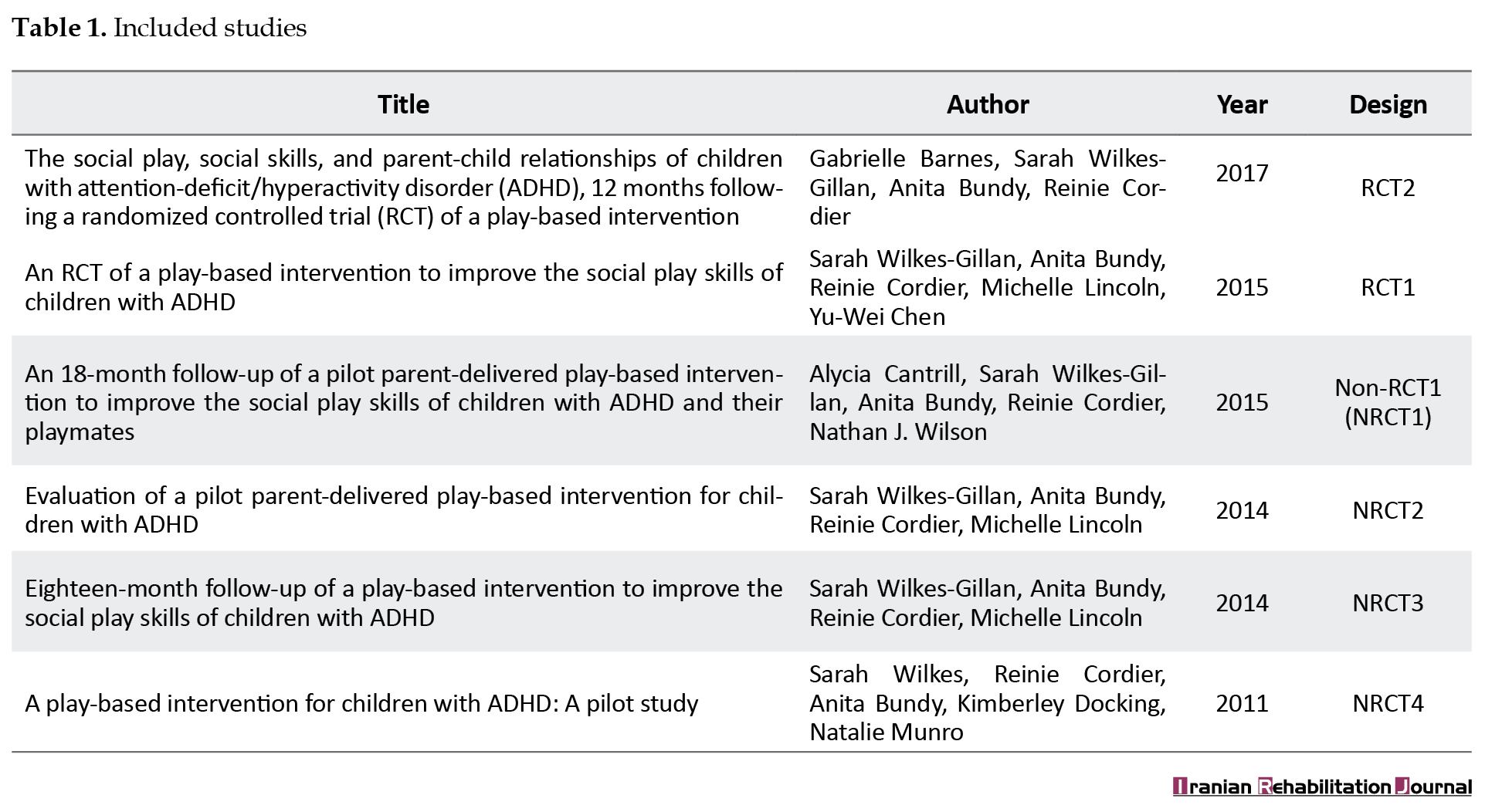
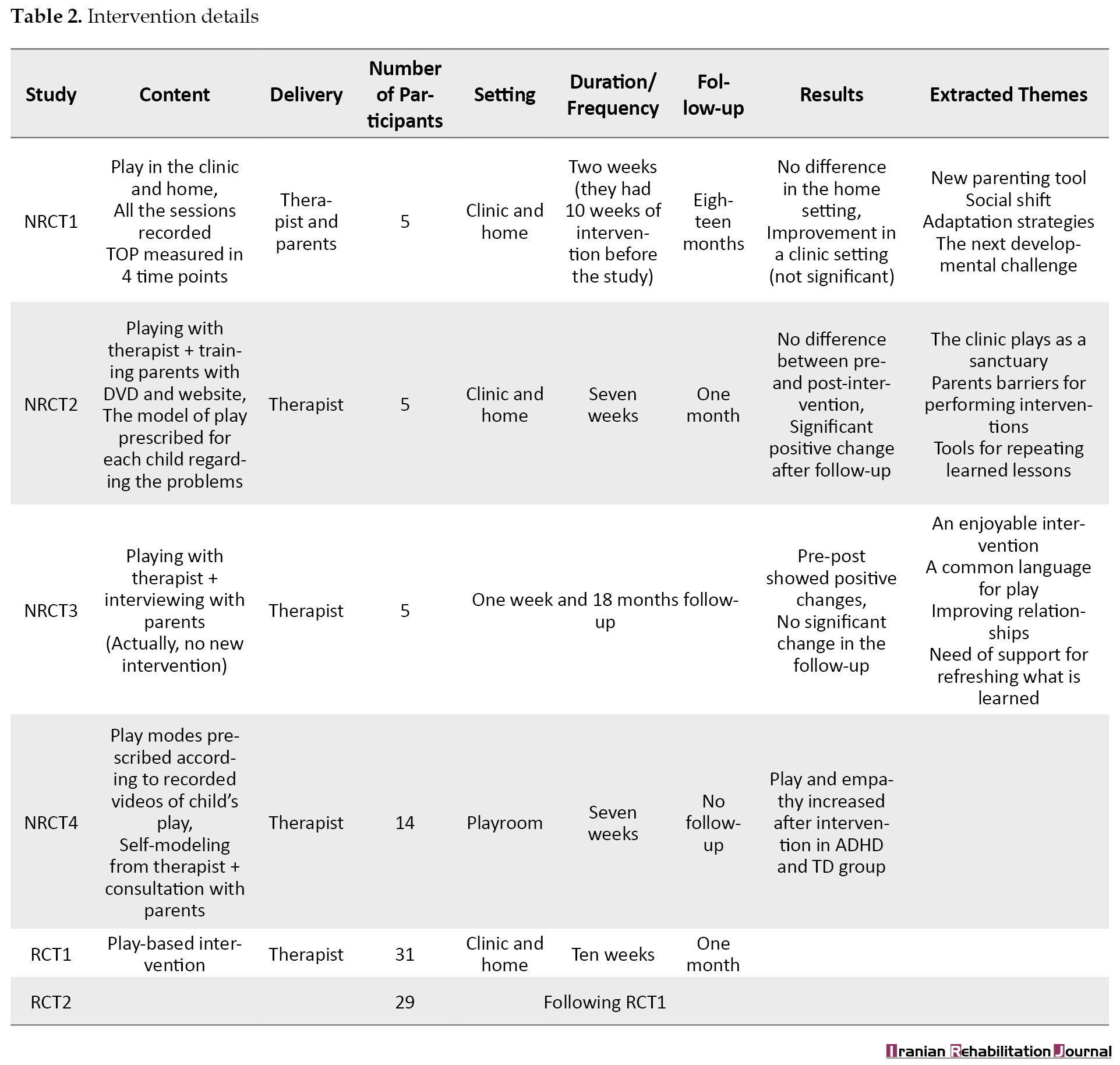
We coded all the studies in Table 1 to ease mentioning them in this paper. More details of play intervention efficiencies are illustrated in Table 2.
All of these 6 studies had mentioned “play” as their primary outcome; however, some of them had other outcomes as well. The assessment tool used for monitoring play was the test of playfulness (TOP) in all of the included studies [36]. There are other tools for the evaluation of play in children, such as child-initiated pretend play assessment (ChIPPA) [37], play history [38], Knox play scale [39], and other scales. These scales could be used for play, but they have some variations in their age group and the area of play that can assess.
For eligibility to attend the study, all studies should have an ADHD diagnosis based on a pediatric physician, but they also used other scales to check if children have common ADHD difficulties. All studies used Conner’s Comprehensive Behavior Rating Scales (CCBRS) to allow children included in the study. Only one study did not use this scale, although, in that study, two other tools were used. Conner’s Parent Rating Scale-the third edition (CPRS-3) and the child Behavior Checklist (CBCL) were used in that study [33].
The core theory of all the studies, regardless of their design, was Cordier’s theory. Cordier published his model of play-based intervention for ADHD children in 2009. Cordier mentioned three main features that should be addressed in play-based interventions for ADHD children. Children’s motivation, lack of empathy in this population, and including playmates in the interventional process are these three main cores [40].
These studies used play-based interventions to improve play, but only two had Randomized Control Trial (RCT) design [41, 42]. The other four studies had not randomized sampling, and all of them mentioned it as a limitation to their studies. The quality assessment of non-randomized studies was done by the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) statement checklist. TREND statement is a checklist for non-randomized trial control studies that claim to evaluate behavioral and public health interventions [43]. This checklist has been used to review articles in the rehabilitation context before [44, 45, 46] the RCT studies were appraised by the CONSORT (CONsolidated Standards Of Reporting Trials) checklist (Table 1). CONSORT statement was established to guide randomized control trial studies to enable researchers to report these studies in a useful way [47].
Study design and methodological quality
Two included studies used the RCT design. The other four studies had a non-randomized control trial design. One of the studies met all the CONSORT criteria [42], and the others had somehow blur descriptions in criteria such as blinding and the whole protocol [41]. In this study, the researcher used the same sample as their past study. Therefore, by referring to that paper, some details on allocation and sampling were not mentioned. The CONSORT table is filled for these two studies. The four residual studies have a lower rate of value according to the center of evidence-based medicine.
Used interventions
The interventions varied in their protocol and the settings; however, they were play-based interventions to improve social play. These interventions were parallel to some instructions and interviews with parents in 3 studies out of these 6. These three studies were not randomized control studies (Not RCTs [NRCTs]) that had an interview part that followed a thematic analysis and grounded theory based on Straus and Corbin’s view. The extracted themes from these parts of the studies are presented in Table 1. Play-based intervention details are prepared in this table, too.
Study participants
The age range of the participants was 5 to 13 years. None of the participants had other major disorders like Autism Spectrum Disorder (ASD), but some related minor disorders like language difficulties were not excluded from the study. The sample size is shown in Table 2. In addition, all studies had typically developed children as match groups who were invited by the ADHD sample group. This action was done to decrease the problem of social interactions with an unknown peer. All studies had ADHD’s parents in the process of study, as well.
4. Discussion
The main purpose of this review was to find out whether different studies have used occupational therapy interventions for improving play. We did not find any prior review study with this purpose. Overall findings indicated play-based intervention effects on social play skills in ADHD children. The level of accessible evidence is almost low (Centre of Evidence-Based Medicine). However, the newest research pyramid for evidence-based practices lacks a hierarchical process like what was common before. According to this pyramid, the included studies in the current review have higher internal validity.
In this review, two studies used RCT designs while the others had NRCT designs. A common limitation in all NRCTs is the small non-randomized sample size which has decreased the generalization of the results to the other ADHD populations. For decreasing bias, all studies tried to be blinded in their designs, whereas the TOP rater was unaware of the study purpose in all studies except one (NRCT 4). In this study, the authors claim that this is a limitation that they could not prevent. One of the studies (NRCT1) claims that they obviously cannot omit the influence of maturity from their samples. This fact is mentioned because no comparison was made after the intervention between Typically Developed (TD) children and ADHD groups. In NRCT4, we can see that TOP had an increase not only in the ADHD group but also in TD. It may show that play-based intervention has a noticeable influence on social play skills in children, even if they do not have difficulty in this area. As most studies show, a play-based intervention can be effective in children’s play skills; however, because of the small sample size, it is hard to confirm this result so far.
Because of the small size of samples, researchers had to use Wilcoxon single rank for their statistics in NRCT1, NRCT2, and NRCT3. In NRCT4 and RCT2, paired sample t-test was used. RCT1 used repeated-measures ANOVA for its analysis.
Study duration was between 6 to 10 weeks in these studies, except for those with a follow-up design from previous studies. NRCT1 and NRCT2 did not show a significant change in the post-intervention TOP scale, but the follow-up in NRCT2 showed a significant positive change. All other studies showed an increase in the TOP scale after the intervention. Since all participants were 5 to 13 years old with no extra analysis in their age sub-groups, we cannot conclude any age-related statement in this review [48, 49].
The delivery method of interventions indicates that when therapists delivered interventions, they were more helpful than when parents delivered them. Although the authors’ justification is that parent-delivered intervention lacked an immediate influence, it showed a rise of TOP scores in the follow-up, which means that educating parents may have long-term effects on children’s social play. Again, the small sample size makes it impossible to generalize this statement to the whole population (NRCT1). Other studies suggest that parent-delivered interventions are effective (NRCT2, NRCT3, NRCT1). The feasibility of interventions was questioned in NRCT3 while it was proved in NRCT2 [32, 48, 49].
All the studies used valid and reliable tools and suitable designs for their aim. In this study, we suggest that play-based interventions in different protocols based on Cordier Model (focusing on peer playing, empathy, and motivation) are feasible and effective, especially when carried out by a therapist [27]. For parent-delivered interventions, training with different strategies should be addressed, and long-term results might be expected.
According to Cordier, all studies should focus on enhancing empathy, motivation, and playing with others as these three factors are affected in children’s playing and the main reason for the poor performance of playing in children with ADHD [31]. In one of these studies, children could reach the normal scores (like their peers within an appropriate range regards to their developmental stage) after receiving interventions (RCT2) [27]. Also, RCT1 shows improvement in playing skills and TOP scores not only after intervention but also after follow-up comparing to pretest evaluations [50]. All other studies showed relative improvement in social play; however, it was not sometimes significant (Table 2).
One limitation of this review article is that four studies out of these six used samples from a previous study. We can assume that not many studies are done to improve play for the sake of play. In all studies we talked about, the play was an outcome, a representation of social skills rather than a prior occupation for a child that needs to be improved. The majority of these studies have the same research group that reveals that few researchers have done studies in this area. In addition, this may create a bias in choosing assessment tools and theoretical frameworks. However, these factors made this review easier because the comparison between studies seems more feasible and tangible. While the thing that makes the comparing process difficult is that all studies did not follow the same design in intervention duration, frequency, or even research design. As there is no prior review in this area, we cannot compare our study to others. The only studies about play for the sake of play for children with ADHD are these six articles discussed. This finding might be an essential concept of this paper. There is a wide gap in the study of children with ADHD play skills for the value of play. More focus on this area is needed.
5. Conclusion
There is a limited number of studies arguing the value of play interventions for the sake of play. Play-based interventions are not only appropriate to enhance developmental skills in children but also influential in improving their play skills. Although play-based interventions for improving play skills are not used in many studies, these interventions could improve social play in children with ADHD, according to what was reviewed. The cognitive aspect of play is not focused on and studied in any of the research studies. Play-based intervention could be delivered either by parents or therapists; however, it was more effective when delivered by a therapist. For parent-delivered interventions, more studies with larger sample sizes are required. A wide gap is seen in studies assessing play-based intervention to improve play skills in both (social and cognitive) dimensions.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank the University of Social Welfare and Rehabilitation Sciences, Department of Occupational Therapy for their kind support.
References
Attention-deficit/hyperactivity disorder (ADHD) is highly prevalent among childhood behavioral disorders worldwide [1, 2]. This illness is a neurodevelopmental disorder diagnosed by three main characteristics: Inattention, hyperactivity, and impulsivity. These characteristics are the core symptoms of this neurodevelopmental disorder [3]. This disorder is not confined to childhood, and its impairments can last through life with an effect on educational performance [4], work [5], and other life domains [6]. It also leads to a lower quality of life than other peers [7, 8]. Children with ADHD also have difficulties in their playing patterns, especially their social play [9, 10, 11].
Play is a primary occupation for a child that is not only necessary for academic learning and cognitive skills but also is crucial for the child’s development [12, 13]. The play has enormous benefits for a child’s development [14, 15]. It relates to all developmental dimensions such as cognitive [16], emotional [17], language [18], social [19], and motor skills [20]. It is common to use play as an intervention to improve other skills such as executive functions, learning, or social skills [21, 22, 23]. Couch and Deitz reported that most occupational therapists address play as an essential concept in a child’s life, but they rarely put objectives and goals to improve one’s play. Instead, they usually benefit from play as a means and medium to do their interventions or used it as a reinforcement for a child [24]. Although this paper was published in 1998, the concept of “play for the sake of play” did not enter much literature, as we can see in the NICE (the National Institute for Health and Care Excellence) newest guideline for ADHD [25].
Children with ADHD have severe problems in their social participation, especially in their playing [26]. “Social play” is greatly affected in these children [27]. About 56% of children with ADHD have no friend, as 32% of typically developed children do not have a friend [9], while “pretend play” is a building block for making personal interactions and communications [28]. Although sometimes play therapy improves ADHD signs like hyperactivity and attention deficit [29], there are some problems in play patterns for children with ADHD, and interventions are needed to improve this area [30, 31, 32].
Play interventions have a fixed position in occupational therapy interventions for children with ADHD [31, 33]. The play has been reviewed as an outcome in other studies, and a systematic review was done in children with autism spectrum disorder children to check the effective interventions which can facilitate and improve social play in the children [34]. Having a review of the ADHD population will help the occupational therapist to access better evidence and will improve their evidence-based practice [35]. As mentioned earlier, play may be used to improve other skills, but in this study, we see play as the primary outcome.
2. Materials and Methods
Search strategy
These four databases were searched from inception to March 2020: PubMed, Web of Science, Scopus, and Elsevier. The used keywords in MeSH terms were “occupational therapy,” “play and playthings,” and “child mental disorders.” Based on MeSH definitions, ADHD is a subcategory of mental disorders, the wider concept (child mental disorders) searched not to miss any studies. The search was done among English and Persian written articles (peer-reviews) only. No other limitation was made in the search process. The article’s references were reviewed to find potential studies to include in the study. The whole process of searching and sampling took four months.
Study selection
The mentioned databases were searched by all authors independently. All search results were imported to the Rayyan QCRI online application. The first and second authors reviewed titles and abstracts in the application independently while the blind mode was on, so the other authors could not see the first one’s decisions. Where disagreement was seen for including an article, the third author made the decision. The inclusion criteria were as follows: 1) participants should be aged 2-12 years (MeSH term definition of a child, PubMed), 2) diagnosis of ADHD, 3) play should be mentioned as the outcome of the study and be a dependent variable using an assessment tool to be measured, 4) any occupational therapy intervention is included, 5) articles should be in English or Persian only, 6) non-full-text and non-peer-reviewed articles are not included, 6) all experimental studies are welcomed. Non-experimental studies will not enter the study because they cannot show the effect of interventions.
After reviewing articles and deciding about their inclusion, the full text of the articles was studied. Then, some of the articles were excluded. All authors extracted the final included articles. A form was made to organize articles data regarding the participants’ information like their diagnosis, age, and gender, the intervention features like the frequency, duration, and follow-up, and the used assessment tools for playing.
Quality assessment
Firstly, the level of evidence was estimated based on the Centre of Evidence-Based Medicine (2009) definition, which is related to the study design. We also used the research pyramid. This new research pyramid critics the traditional single-hierarchy evidence model (Arbesman-2008).
Preferred Reporting Item for Systematic Review and A meta-analysis (PRISMA) statement (Appendix A) was used in the next step. A protocol was registered on the Prospero database (CRD42020172447).
3. Results
First, we extracted 103 articles. One extra article was added from other sources. After removing duplicates, 83 remained that 2 of which were not English or Persian. Fifty-one studies were excluded based on their titles and abstracts. Thirty articles were selected to be read in their full text which 6 of them remained because of meeting the mentioned inclusion and exclusion criteria. Figure 1 demonstrates the process that we passed to get these 6 articles.
The included articles are shown in Table 1.
We coded all the studies in Table 1 to ease mentioning them in this paper. More details of play intervention efficiencies are illustrated in Table 2.
All of these 6 studies had mentioned “play” as their primary outcome; however, some of them had other outcomes as well. The assessment tool used for monitoring play was the test of playfulness (TOP) in all of the included studies [36]. There are other tools for the evaluation of play in children, such as child-initiated pretend play assessment (ChIPPA) [37], play history [38], Knox play scale [39], and other scales. These scales could be used for play, but they have some variations in their age group and the area of play that can assess.
For eligibility to attend the study, all studies should have an ADHD diagnosis based on a pediatric physician, but they also used other scales to check if children have common ADHD difficulties. All studies used Conner’s Comprehensive Behavior Rating Scales (CCBRS) to allow children included in the study. Only one study did not use this scale, although, in that study, two other tools were used. Conner’s Parent Rating Scale-the third edition (CPRS-3) and the child Behavior Checklist (CBCL) were used in that study [33].
The core theory of all the studies, regardless of their design, was Cordier’s theory. Cordier published his model of play-based intervention for ADHD children in 2009. Cordier mentioned three main features that should be addressed in play-based interventions for ADHD children. Children’s motivation, lack of empathy in this population, and including playmates in the interventional process are these three main cores [40].
These studies used play-based interventions to improve play, but only two had Randomized Control Trial (RCT) design [41, 42]. The other four studies had not randomized sampling, and all of them mentioned it as a limitation to their studies. The quality assessment of non-randomized studies was done by the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) statement checklist. TREND statement is a checklist for non-randomized trial control studies that claim to evaluate behavioral and public health interventions [43]. This checklist has been used to review articles in the rehabilitation context before [44, 45, 46] the RCT studies were appraised by the CONSORT (CONsolidated Standards Of Reporting Trials) checklist (Table 1). CONSORT statement was established to guide randomized control trial studies to enable researchers to report these studies in a useful way [47].
Study design and methodological quality
Two included studies used the RCT design. The other four studies had a non-randomized control trial design. One of the studies met all the CONSORT criteria [42], and the others had somehow blur descriptions in criteria such as blinding and the whole protocol [41]. In this study, the researcher used the same sample as their past study. Therefore, by referring to that paper, some details on allocation and sampling were not mentioned. The CONSORT table is filled for these two studies. The four residual studies have a lower rate of value according to the center of evidence-based medicine.
Used interventions
The interventions varied in their protocol and the settings; however, they were play-based interventions to improve social play. These interventions were parallel to some instructions and interviews with parents in 3 studies out of these 6. These three studies were not randomized control studies (Not RCTs [NRCTs]) that had an interview part that followed a thematic analysis and grounded theory based on Straus and Corbin’s view. The extracted themes from these parts of the studies are presented in Table 1. Play-based intervention details are prepared in this table, too.
Study participants
The age range of the participants was 5 to 13 years. None of the participants had other major disorders like Autism Spectrum Disorder (ASD), but some related minor disorders like language difficulties were not excluded from the study. The sample size is shown in Table 2. In addition, all studies had typically developed children as match groups who were invited by the ADHD sample group. This action was done to decrease the problem of social interactions with an unknown peer. All studies had ADHD’s parents in the process of study, as well.
4. Discussion
The main purpose of this review was to find out whether different studies have used occupational therapy interventions for improving play. We did not find any prior review study with this purpose. Overall findings indicated play-based intervention effects on social play skills in ADHD children. The level of accessible evidence is almost low (Centre of Evidence-Based Medicine). However, the newest research pyramid for evidence-based practices lacks a hierarchical process like what was common before. According to this pyramid, the included studies in the current review have higher internal validity.
In this review, two studies used RCT designs while the others had NRCT designs. A common limitation in all NRCTs is the small non-randomized sample size which has decreased the generalization of the results to the other ADHD populations. For decreasing bias, all studies tried to be blinded in their designs, whereas the TOP rater was unaware of the study purpose in all studies except one (NRCT 4). In this study, the authors claim that this is a limitation that they could not prevent. One of the studies (NRCT1) claims that they obviously cannot omit the influence of maturity from their samples. This fact is mentioned because no comparison was made after the intervention between Typically Developed (TD) children and ADHD groups. In NRCT4, we can see that TOP had an increase not only in the ADHD group but also in TD. It may show that play-based intervention has a noticeable influence on social play skills in children, even if they do not have difficulty in this area. As most studies show, a play-based intervention can be effective in children’s play skills; however, because of the small sample size, it is hard to confirm this result so far.
Because of the small size of samples, researchers had to use Wilcoxon single rank for their statistics in NRCT1, NRCT2, and NRCT3. In NRCT4 and RCT2, paired sample t-test was used. RCT1 used repeated-measures ANOVA for its analysis.
Study duration was between 6 to 10 weeks in these studies, except for those with a follow-up design from previous studies. NRCT1 and NRCT2 did not show a significant change in the post-intervention TOP scale, but the follow-up in NRCT2 showed a significant positive change. All other studies showed an increase in the TOP scale after the intervention. Since all participants were 5 to 13 years old with no extra analysis in their age sub-groups, we cannot conclude any age-related statement in this review [48, 49].
The delivery method of interventions indicates that when therapists delivered interventions, they were more helpful than when parents delivered them. Although the authors’ justification is that parent-delivered intervention lacked an immediate influence, it showed a rise of TOP scores in the follow-up, which means that educating parents may have long-term effects on children’s social play. Again, the small sample size makes it impossible to generalize this statement to the whole population (NRCT1). Other studies suggest that parent-delivered interventions are effective (NRCT2, NRCT3, NRCT1). The feasibility of interventions was questioned in NRCT3 while it was proved in NRCT2 [32, 48, 49].
All the studies used valid and reliable tools and suitable designs for their aim. In this study, we suggest that play-based interventions in different protocols based on Cordier Model (focusing on peer playing, empathy, and motivation) are feasible and effective, especially when carried out by a therapist [27]. For parent-delivered interventions, training with different strategies should be addressed, and long-term results might be expected.
According to Cordier, all studies should focus on enhancing empathy, motivation, and playing with others as these three factors are affected in children’s playing and the main reason for the poor performance of playing in children with ADHD [31]. In one of these studies, children could reach the normal scores (like their peers within an appropriate range regards to their developmental stage) after receiving interventions (RCT2) [27]. Also, RCT1 shows improvement in playing skills and TOP scores not only after intervention but also after follow-up comparing to pretest evaluations [50]. All other studies showed relative improvement in social play; however, it was not sometimes significant (Table 2).
One limitation of this review article is that four studies out of these six used samples from a previous study. We can assume that not many studies are done to improve play for the sake of play. In all studies we talked about, the play was an outcome, a representation of social skills rather than a prior occupation for a child that needs to be improved. The majority of these studies have the same research group that reveals that few researchers have done studies in this area. In addition, this may create a bias in choosing assessment tools and theoretical frameworks. However, these factors made this review easier because the comparison between studies seems more feasible and tangible. While the thing that makes the comparing process difficult is that all studies did not follow the same design in intervention duration, frequency, or even research design. As there is no prior review in this area, we cannot compare our study to others. The only studies about play for the sake of play for children with ADHD are these six articles discussed. This finding might be an essential concept of this paper. There is a wide gap in the study of children with ADHD play skills for the value of play. More focus on this area is needed.
5. Conclusion
There is a limited number of studies arguing the value of play interventions for the sake of play. Play-based interventions are not only appropriate to enhance developmental skills in children but also influential in improving their play skills. Although play-based interventions for improving play skills are not used in many studies, these interventions could improve social play in children with ADHD, according to what was reviewed. The cognitive aspect of play is not focused on and studied in any of the research studies. Play-based intervention could be delivered either by parents or therapists; however, it was more effective when delivered by a therapist. For parent-delivered interventions, more studies with larger sample sizes are required. A wide gap is seen in studies assessing play-based intervention to improve play skills in both (social and cognitive) dimensions.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank the University of Social Welfare and Rehabilitation Sciences, Department of Occupational Therapy for their kind support.
References
- Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde L A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry. 2007; 164(6):942-8. [DOI:10.1176/ajp.2007.164.6.942] [PMID]
- Sayal K, Prasad V, Daley D, Ford T, Coghill D. ADHD in children and young people: prevalence, care pathways, and service provision. The Lancet Psychiatry. 2018; 5(2):175-86. [DOI:10.1016/S2215-0366(17)30167-0][PMID]
- Hall CL, Valentine AZ, Groom MJ, Walker GM, Sayal K, Daley D, et al. The clinical utility of the continuous performance test and objective measures of activity for diagnosing and monitoring ADHD in children: A systematic review. European Child & Adolescent Psychiatry. 2016; 25(7):677-99. [DOI:10.1007/s00787-015-0798-x] [PMID]
- Shifrin JG, Proctor BE, Prevatt FF. Work performance differences between college students with and without ADHD. Journal of Attention Disorders. 2010; 13(5):489-96. [DOI:10.1177/1087054709332376] [PMID]
- Nagata M, Nagata T, Inoue A, Mori K. Effect modification by Attention Deficit Hyperactivity Disorder (ADHD) symptoms on the association of psychosocial work environments with psychological distress and work engagement. Frontiers in Psychiatry. 2019; 10:166. [DOI:10.3389/fpsyt.2019.00166] [PMID] [PMCID]
- Ezpeleta L, de la Osa N, Doménech JM. Prevalence of DSM-IV disorders, comorbidity and impairment in 3-year-old Spanish preschoolers. Social Psychiatry and Psychiatric Epidemiology. 2014; 49(1):145-55. [DOI:10.1007/s00127-013-0683-1] [PMID]
- Mulraney M, Coghill D. Quality of life and impairment in ADHD. In: Mulraney M, Coghill D. Oxford Textbook of Attention Deficit Hyperactivity Disorder. Oxford: Oxford University Press; 2018. [DOI:10.1093/med/9780198739258.003.0017]
- Pinho TD, Manz PH, DuPaul GJ, Anastopoulos AD, Weyandt LL. Predictors and moderators of quality of life among college students with ADHD. Journal of Attention Disorders. 2019; 23(14):1736-45. [DOI:10.1177/1087054717734645] [PMID] [PMCID]
- Normand S, Soucisse MM, Melançon MPV, Schneider BH, Lee MD, Maisonneuve M F. Observed free-play patterns of children with ADHD and their real-life friends. Journal of Abnormal Child Psychology. 2019; 47(2):259-71. [DOI:10.1007/s10802-018-0437-3] [PMID]
- Wilkes-Gillan S, Bundy A, Cordier R, Lincoln M, Chen YW. A randomised controlled trial of a play-based intervention to improve the social play skills of children with Attention Deficit Hyperactivity Disorder (ADHD). PloS One. 2016; 11(8):e0160558. [DOI:10.1371/journal.pone.0160558] [PMID] [PMCID]
- Wilkes-Gillan S, Bundy A, Cordier R, Lincoln M. Child outcomes of a pilot parent-delivered intervention for improving the social play skills of children with ADHD and their playmates. Developmental Neurorehabilitation. 2016; 19(4):238-45. [DOI:10.3109/17518423.2014.948639] [PMID]
- Dabiri Golchin M, Mirzakhani N, Stagnitti K, Dabiri Golchin M, Rezaei M. Psychometric properties of Persian version of “child-initiated pretend play assessment” for Iranian children. Iranian Journal of Pediatrics. 2017; 27(1):1-8. [DOI:10.5812/ijp.7053]
- Lynch H, Moore A. Play as an occupation in occupational therapy. London: SAGE Publications; 2016. [DOI:10.1177/0308022616664540]
- Burriss KG, Tsao LL. Review of research: How much do we know about the importance of play in child development? Childhood Education. 2002; 78(4):230-3. [DOI:10.1080/00094056.2002.10522188]
- Piers MW. Play and development. New York: Norton & Company; 1972. https://eric.ed.gov/?q=Konrad+AND+Lorenz&id=ED072864
- Lillard A, Pinkham AM, Smith E. Pretend play and cognitive development. In: Goswami U, editor. The Wiley-Blackwell Handbook of Childhood Cognitive Development. Hobokon: Blackwell Publishing Ltd; 2011. [DOI:10.1002/9781444325485.ch11]
- Erickson RJ. Play contributes to the full emotional development of the child. Education. 1985; 105(3):261-3. https://psycnet.apa.org/record/1986-14119-001
- Quinn S, Donnelly S, Kidd E. The relationship between symbolic play and language acquisition: A meta-analytic review. Developmental Review. 2018; 49:121-35. [DOI:10.1016/j.dr.2018.05.005]
- Szumski G, Smogorzewska J, Karwowski M. Can play develop social skills? The effects of ‘Play Time/Social Time’programme implementation. International Journal of Developmental Disabilities. 2016; 62(1):41-50. [DOI:10.1179/2047387715Y.0000000002]
- Boon B, Rozendaal M, van den Heuvel-Eibrink MM, van der Net J, Stappers PJ. Playscapes: A design perspective on young children’s physical play. Paper presented at: Proceedings of the The 15th International Conference on Interaction Design and Children. 21-24 June 2016; Manchester, England.[DOI:10.1145/2930674.2930713]
- Bergen D. Play as a medium for learning and development: A handbook of theory and practice. New York: Penguin Random House; 1988. https://books.google.com/books?id=3GmdAAAAMAAJ&q
- Tahmores AH. Role of play in social skills and intelligence of children. Procedia-Social and Behavioral Sciences. 2011; 30:2272-9. [DOI:10.1016/j.sbspro.2011.10.444]
- Thibodeau RB, Gilpin A T, Brown MM, Meyer BA. The effects of fantastical pretend-play on the development of executive functions: An intervention study. Journal of Experimental Child Psychology. 2016; 145:120-38. [DOI:10.1016/j.jecp.2016.01.001] [PMID]
- Couch KJ, Deitz JC, Kanny EM. The role of play in pediatric occupational therapy. American Journal of Occupational Therapy. 1998; 52(2):111-7. [DOI:10.5014/ajot.52.2.111] [PMID]
- National Institute for Health and Care Excellence (Great Britain). Attention deficit hyperactivity disorder: Diagnosis and management. London: National Institute for Health and Care Excellence. 2018. https://books.google.com/books?id=hG0izAEACAAJ&dq
- Levanon-Erez N, Kampf-Sherf O, Maeir A. Occupational therapy metacognitive intervention for adolescents with ADHD: Teen Cognitive-Functional (Cog-Fun) feasibility study. British Journal of Occupational Therapy. 2019; 82(10):618-29. [DOI:10.1177/0308022619860978]
- Barnes G, Wilkes‐Gillan S, Bundy A, Cordier R. The social play, social skills and parent-child relationships of children with ADHD 12 months following a RCT of a play‐based intervention. Australian Occupational Therapy Journal. 2017; 64(6):457-65. [DOI:10.1111/1440-1630.12417] [PMID]
- Wieder S. The power of symbolic play in emotional development through the DIR lens. Topics in Language Disorders. 2017; 37(3):259-81. [DOI:10.1097/TLD.0000000000000126]
- Barzegary L, Zamini S. The effect of play therapy on children with ADHD. Procedia-Social and Behavioral Sciences. 2011; 30:2216-8. [DOI:10.1016/j.sbspro.2011.10.432]
- Alessandri SM. Attention, play, and social behavior in ADHD preschoolers. Journal of Abnormal Child Psychology. 1992; 20(3):289-302. [DOI:10.1007/BF00916693] [PMID]
- Cordier R, Bundy A, Hocking C, Einfeld S. A model for play‐based intervention for children with ADHD. Australian Occupational Therapy Journal. 2009; 56(5):332-40. [DOI:10.1111/j.1440-1630.2009.00796.x] [PMID]
- Wilkes‐Gillan S, Bundy A, Cordier R, Lincoln M. Eighteen‐month follow‐up of a play‐based intervention to improve the social play skills of children with attention deficit hyperactivity disorder. Australian Occupational Therapy Journal. 2014; 61(5):299-307. [DOI:10.1111/1440-1630.12124] [PMID]
- Wilkes S, Cordier R, Bundy A, Docking K, Munro N. A play‐based intervention for children with ADHD: A pilot study. Australian Occupational Therapy Journal. 2011; 58(4):231-40. [DOI:10.1111/j.1440-1630.2011.00928.x] [PMID]
- Tanner K, Hand BN, O’Toole G, Lane A E. Effectiveness of interventions to improve social participation, play, leisure, and restricted and repetitive behaviors in people with autism spectrum disorder: A systematic review. The American Journal of Occupational Therapy. 2015; 69(5):6905180010p1-12. [DOI:10.5014/ajot.2015.017806] [PMID]
- Leung EKH. Evidence-based practice in occupational therapy. Hong Kong Journal of Occupational Therapy. 2002; 12(1):21-32. [DOI:10.1016/S1569-1861(09)70014-2]
- Skard G, Bundy AC. 4 test of playfulness. In: Parham LD, Fazio LS, editors. Play in Occupational Therapy for Children. Maryland Heights: Mosby Elsevier; 2008. pp. 71-93. [DOI:10.1016/B978-032302954-4.10004-2]
- Stagnitti K. The child initiated pretend play assessment (ChIPPA). Brunswick West: Vic; 2007. https://www.worldcat.org/title/child-initiated-pretend-play-assessment-chippa/oclc/586500863
- Takata N. The play history. The American Journal of Occupational Therapy. 1969; 23(4):314-8. [PMID]
- Jankovich M, Mullen J, Rinear E, Tanta K, Deitz J. Revised knox preschool play scale: Interrater agreement and construct validity. The American Journal of Occupational Therapy. 2008; 62(2):221-7. [DOI:10.5014/ajot.62.2.221] [PMID]
- Cordier R, Bundy A, Hocking C, Einfeld S. A model for play‐based intervention for children with ADHD. Australian Occupational Therapy Journal. 2009; 56(5):332-40. [DOI:10.1111/j.1440-1630.2009.00796.x] [PMID]
- Barnes G, Wilkes-Gillan S, Bundy A, Cordier R. The social play, social skills and parent-child relationships of children with ADHD 12 months following a RCT of a play-based intervention. Australian Occupational Therapy Journal. 2017; 64(6):457-65. [DOI:10.1111/1440-1630.12417] [PMID]
- Wilkes-Gillan S, Bundy A, Cordier R, Lincoln M, Chen YW. A randomised controlled trial of a play-based intervention to improve the social play skills of children with attention deficit hyperactivity disorder (ADHD). PLoS One. 2016; 11(8):e0160558. [DOI:10.1371/journal.pone.0160558] [PMID] [PMCID]
- Armstrong R, Waters E, Moore L, Riggs E, Cuervo LG, Lumbiganon P, et al. Improving the reporting of public health intervention research: Advancing TREND and CONSORT. Journal of Public Health. 2008; 30(1):103-9. [DOI:10.1093/pubmed/fdm082] [PMID]
- Bettger JAP, Stineman MG. Effectiveness of multidisciplinary rehabilitation services in postacute care: State-of-the-science. A review. Archives of Physical Medicine and Rehabilitation. 2007; 88(11):1526-34. [DOI:10.1016/j.apmr.2007.06.768] [PMID] [PMCID]
- Grotle M, Klokkerud M, Kjeken I, Bremander A, Hagel S, Strömbeck B, et al. What’s in the black box of arthritis rehabilitation? A comparison of rehabilitation practice for patients with inflammatory arthritis in northern Europe. Journal of Rehabilitation Medicine. 2013; 45(5):458-66. [DOI:10.2340/16501977-1125] [PMID]
- Semrau J, Hentschke C, Buchmann J, Meng K, Vogel H, Faller H, et al. Long-term effects of interprofessional biopsychosocial rehabilitation for adults with chronic non-specific low back pain: A multicentre, quasi-experimental study. PloS one. 2015; 10(3):e0118609. [DOI:10.1371/journal.pone.0118609] [PMID] [PMCID]
- Campbell MK, Elbourne DR, Altman DG, CONSORT group. CONSORT statement: Extension to cluster randomised trials. BMJ. 2004; 328(7441):702-8. [DOI:10.1136/bmj.328.7441.702] [PMID] [PMCID]
- Cantrill A, Wilkes‐Gillan S, Bundy A, Cordier R, Wilson NJ. An eighteen‐month follow‐up of a pilot parent‐delivered play‐based intervention to improve the social play skills of children with attention deficit hyperactivity disorder and their playmates. Australian Occupational Therapy Journal. 2015; 62(3):197-207. [DOI:10.1111/1440-1630.12203] [PMID]
- Wilkes-Gillan S, Bundy A, Cordier R, Lincoln M. Evaluation of a pilot parent-delivered play-based intervention for children with attention deficit hyperactivity disorder. American Journal of Occupational Therapy. 2014; 68(6):700-9. [DOI:10.5014/ajot.2014.012450] [PMID]
- Wilkes-Gillan S, Bundy A, Cordier R, Lincoln M, Chen Y W. A randomised controlled trial of a play-based intervention to improve the social play skills of children with Attention Deficit Hyperactivity Disorder (ADHD). PloS One. 2016; 11(8):e0160558. [DOI:10.1371/journal.pone.0160558] [PMID] [PMCID]
Article type: Reviews |
Subject:
Occupational therapy
Received: 2020/10/16 | Accepted: 2021/08/16 | Published: 2021/09/1
Received: 2020/10/16 | Accepted: 2021/08/16 | Published: 2021/09/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
