
988368
Sat, Aug 1, 2026

Volume 20, Issue 3 (September 2022)
Iranian Rehabilitation Journal 2022, 20(3): 363-368 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rostampourgonbaki M, Deghanpour N, Kiakojouri K, Dehghan M, Gholinia H. Acoustic Voice Measures in Benign Mass Lesions. Iranian Rehabilitation Journal 2022; 20 (3) :363-368
URL: http://irj.uswr.ac.ir/article-1-1537-en.html
URL: http://irj.uswr.ac.ir/article-1-1537-en.html
Mohaddeseh Rostampourgonbaki1 

 , Niloofar Deghanpour1 , Keivan Kiakojouri2 , Mehdi Dehghan *3 , Hemmat Gholinia4
, Niloofar Deghanpour1 , Keivan Kiakojouri2 , Mehdi Dehghan *3 , Hemmat Gholinia4
, Niloofar Deghanpour1 , Keivan Kiakojouri2 , Mehdi Dehghan *3 , Hemmat Gholinia4
1- Faculty of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
2- Faculty of Medicine, Babol University of Medical Sciences, Babol, Iran.
3- Ayatollah Rouhani Clinical Research Center, Movement Disorders Research Center, Faculty of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
4- Clinical Research Center of Ayatollah Rouhani Hospital, Babol University of Medical Sciences, Babol, Iran.
2- Faculty of Medicine, Babol University of Medical Sciences, Babol, Iran.
3- Ayatollah Rouhani Clinical Research Center, Movement Disorders Research Center, Faculty of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
4- Clinical Research Center of Ayatollah Rouhani Hospital, Babol University of Medical Sciences, Babol, Iran.
Keywords: Vocal fold polyps, Vocal nodule, Acoustic parameters, Voice analysis, Multi-dimensional voice program
Full-Text [PDF 460 kb]
(1835 Downloads)
| Abstract (HTML) (3736 Views)
Full-Text: (1569 Views)
1. Introduction
Polyps and nodules are identified as the most common benign lesions [1] of vocal cords caused by vocal disturbances [2, 3]. The most common clinical symptoms are different degrees of roughness and feeling of a foreign body [4]. These voice pathologies are not life-threatening disorders but may limit communication activities and consequently, voice disorders can affect the quality of life [5]. Therefore, an assessment of different dimensions of voice in these pathologies seems necessary.
The use of specific instruments to investigate voice and its physical parameters is known as acoustic analysis, which comprises an assessment procedure for patients suffering from mass lesions, including polyps and nodules [6]. Acoustic analysis of voice is a non-invasive, quantitative, economical, convenient, and rapid procedure compared to other assessment methods, such as electroglottographic [7] and video-laryngostroboscopic evaluations [8, 9].
The computerized multidimensional acoustic voice analysis enables visual and numerical analysis of the voice samples. Such analysis programs provide objective data and support subjective voice evaluation [2], which helps monitor clinical procedures and compare the results pre and post-intervention in experimental studies. The acoustic parameters measured in the most of studies are fundamental frequency (F0), amplitude perturbation or shimmer, frequency perturbation or jitter, and noise-to-harmonic ratio (NHR).
In terms of physiological characteristics of vocal folds, F0 as one of the most important voice parameters for the acoustic voice measures shows the number of vocal cords’ cover layer vibrations per second [10]. The intensity corresponding to loudness is the other acoustic voice measure frequently reported in the literature. Jitter and shimmer have been designed to measure two important aspects of acoustic voice parameters in a signal, frequency, and amplitude perturbation, respectively. In terms of physiological characteristics, the rate of perturbation increases with advancing the disturbances of the vocal folds. A close relationship exists between the increase in perturbation and the change in voice quality, such as breathiness and hoarseness [11].
It appears that the existence of vocal cord polyps and nodules contributes to changes in voice quality and acoustic voice parameters. Petrovic-Lazic et al. studied the acoustic voice parameters of patients with vocal fold polyps and healthy individuals using MDVP software. They reported that jitter (%), shimmer (%), and NHR values significantly differentiated the patients with vocal fold polyps from the vocally healthy group [2]. Kandogan and Ozuer also observed the values of jitter and shimmer increased in people with vocal folds lesions, such as vocal cord polyps, nodules, Reinke edema, and cysts using MDVP. They investigated 25 patients with vocal nodules, 29 patients with vocal cord polyps, 15 patients with Reinke edema, and 8 patients with vocal cord cysts [12]. Two studies demonstrated that NHR values in patients with vocal cord nodules were not statistically different from the control group [6, 13].
Considering contradictory results for NHR, we decided to conduct this study. Additionally, the acoustic voice parameters of patients with vocal cord nodules and polyps and healthy controls were compared in terms of sex.
2. Materials and Methods
Study design
The present project was a cross-sectional case-control study. Sixty-eight patients with vocal cord nodules and polyps who visited the speech therapy clinic of Ayatollah Rouhani Hospital in Babol City, Iran, in 2016-2017 were recruited in the current research.
Participants
A total of 110 participants in three groups, including patients with nodules, patients with polyps, and healthy subjects were recruited in the current research. Table 1 presents the distribution of the subjects in terms of sex. The video-laryngostrobosspic examination was performed by the experienced speech and language pathologist (SLP) by corresponding author and the diagnosis of vocal nodules and polyps was confirmed by an otolaryngologist. In the healthy group, individuals who had no history of voice disorders and had intact larynx were included based on video-laryngostroboscopic examination. The exclusion criteria for all groups included other structural disorders, such as Reinke’s edema, cysts, sulcus vocalis, granuloma, neurological disorders, such as vocal cord paralysis, multiple sclerosis, Parkinson’s disease, psychological problems, and history of cold and flu before 2 weeks ago.
.jpg)
Ethical approval
The current study was approved by the Ethics Committee of Babol University of Medical Sciences (MUBABOL.HRI.REC.1396.60). The participants were given the signed consent form and requested to complete it before the sampling procedure.
Procedure
The participants’ demographic data were gathered via an interview and a questionnaire containing demographic information and the medical history of the subjects. We asked the participants to sit in an upright posture and produce prolonged /â/ vowel (at least 5 seconds) with habitual intensity and pitch three times. The procedure was conducted in the sound-attenuated room. MDVP software (MDVP, Elemetrics K. Kay Elemetrics Visi-Pitch IV model 3950 instruction manual) was utilized to measure the traditional acoustic voice parameters. The recorder (Model: Lincoln Park, NJ) was applied to record the voice samples of the participants using the microphone (model: SM48, assembled in Mexico) with a 20 cm constant distance [14].
In case of any unwanted sampling error, the test was repeated. In this step, the clearest voice sample of each subject was chosen for analysis. We removed the onset and offset of each segment and the middle part of the segment was exposed to measure the acoustic voice parameters. Then, the acoustic voice parameters (jitter, shimmer, fundamental frequency, and NHR) were analyzed.
Measures and analyses
The SPSS software v. 18.0 (SPSS, Inc., Chicago, Illinois) was applied for the statistical analysis of data. Descriptive statistics were used to report the age, group, and sex of the participants. After investigating the normality of the distribution of the data by Kolmogorov Smirnov test, we used 1-way analysis of variance (ANOVA) test to compare each variable (jitter, shimmer, fundamental frequency, and NHR) in three groups. Moreover, 1-way analysis of variance (ANOVA) test was applied to compare the acoustic voice parameters among three groups in males and females. The significance level was considered (P<0.05).
3. Results
As provided in Table 2, three groups showed a significant difference in the fundamental frequency (P<0.001). Women had a significant difference in the fundamental frequency in the three groups (P<0.001), but the difference was not statistically evident in men (P=0.93).
.jpg)
In Table 3, the two groups had statistically significant differences for the jitter (P<0.001). Also, for jitter measurement, men (P<0.001) and women (P<0.001) had a significant difference in the three groups.
.jpg)
Table 4 presents the mean and standard deviation values of shimmer in three groups. As found in Table 4, they had a statistical difference for the shimmer (P<0.001). In addition, men had a significant difference in shimmer (P=0.001). Evident differences were observed for the shimmer in the women (P<0.001) and men (P=0.001).
.jpg)
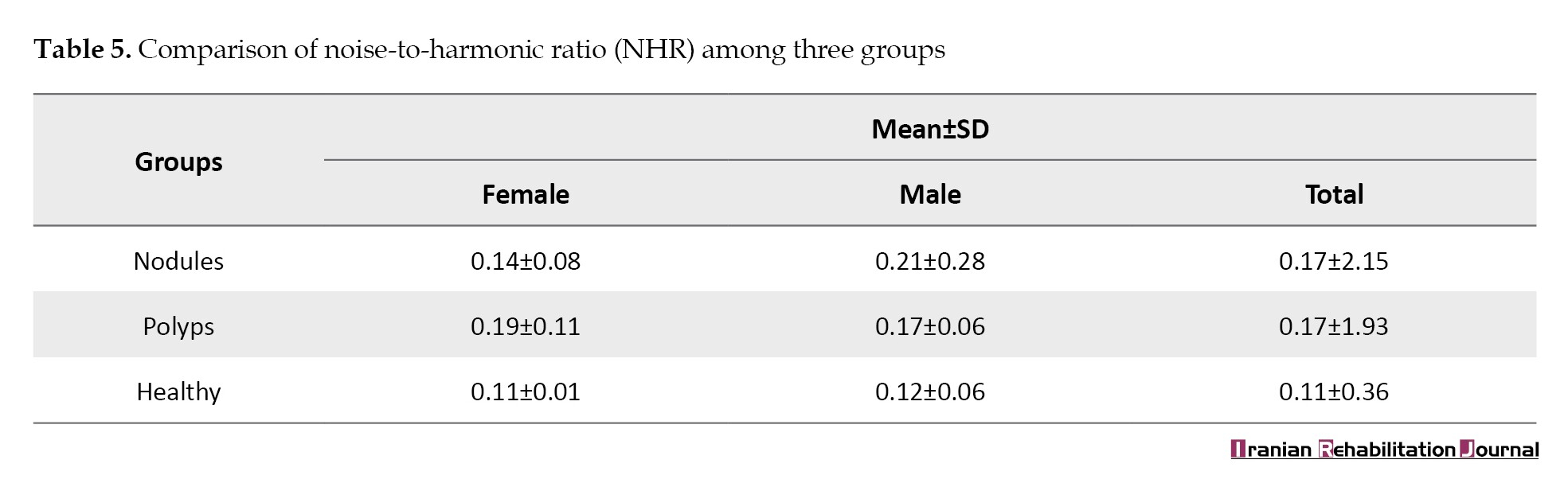
Moreover, according to Table 5, the NHR was significantly different among the three groups. Men did not have a significant difference in NHR (P=0.24), but women showed substantial differences (P=0.01).
4. Discussion
In the current study, four acoustic voice parameters were analyzed, such as F0, jitter, shimmer, and NHR which are the most common acoustic voice measures in most studies.
The mean value of fundamental frequency is defined as the overall mean of all extracted period-to-period fundamental frequency measures in the voice sample [15]. In our study, the F0 was lower in men than in women, as expected, according to the differences in vocal fold characteristics between men and women [16, 17]. Similar to Halawa et al work, our result showed that F0 decreased in patients with vocal cord nodules and polyps. It can be attributed to the existence of extra mass on the surface of vocal folds thickening them [18]. Furthermore, the F0 of female patients was significantly lower than in the control group.
Jitter is defined as the short-term and cycle-to-cycle perturbation in the F0 of the voice [15]. The mean values of jitter showed a significant increase in both patient groups rather than the healthy group similar to some existing research [6]. Also, jitter increased in both females and males with nodules compared to the control group. This finding is consistent with some studies [3] but is not consistent with the result obtained by Chhetri et al. [6]. This significant increase can be caused by small growth on the surface of the vocal folds in mass lesions, such as polyps and nodules [2]. Even very minimal growths on vocal folds may impact the jitter, and larger pathologies may result in more increased jitter [15]. It appears that increasing in jitter correlates with the number of active motor neurons and the increase in decreasing the control of muscle tone in the larynx [2].
Shimmer refers to the cycle-to-cycle, short-term perturbation in the amplitude of voice [15]. The mean values of shimmer showed a significant increase in the patients’ group than the control one. In addition, the mean value of shimmer was significantly higher in both sexes of both case groups rather than the control group. This finding is consistent with several studies [2, 6]. This significant difference would be probably related to incompatible and weak contact of vocal fold edges due to glottis closure deficiency [15].
Based on the findings of the present research, the mean value of NHR in the group of patients with nodules increased significantly. While NHR values were increased in vocal polyps and nodules in both genders of patient groups, this increase was only significant in women with vocal polyps. These results were consistent with some studies [6, 13]. It can be caused by an incomplete closure of the glottis due to polyps leading to an air leakage [15] acoustically characterized as a noisy voice. The relative values of additional noise in the voice signal are quantified by NHR arising from the air-flow turbulence produced at the glottis during the phonation process. Insufficient closure of vocal cords causes exceeding values of airflow in the glottis, resulting in turbulent airflow [19].
5. Conclusion
Every small variation of the mass, biochemical and biomechanical characteristics of vocal folds, can easily lead to rapid disturbances and cyclic changes in the intensity and frequency of voice resulting from the vibration of the vocal folds’ cover layer. According to the findings of this study, it can be concluded that the weak and unstable closure of the glottis, resulting from the vocal fold nodules and or polyp, causes lower fundamental frequency and higher jitter, shimmer, and NHR values. Finally, by the computerized voice analysis procedures, one can provide an objective, accurate, and reliable examination of the vocal performance and quantitatively represent the voice quality.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects. principles of the Helsinki Convention was also observed.
Funding
This study was financially supported by Babol University of Medical Sciences.
Authors' contributions
Conceptualization and Supervision: Mehdi Dehghan, Keivan Kiakojouri; Methodology: Mehdi Dehghan and Hemmat Gholinia; Investigation: Mehdi Dehghan and Mohaddeseh Rostampourgonbaki; Writing–original draft: Mohaddeseh Rostampourgonbaki and Niloofar Dehghanpour; Writing–review & editing: Mehdi dehghan, Mohaddeseh Rostampourgonbaki.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Research Vice-chancellor at the Babol University of Medical Sciences, the Clinical Research Development Center of Ayatollah Rouhani Hospital in Babol, and Mohammad Ali Shams for their material and spiritual support in the implementation of the study.
References
Polyps and nodules are identified as the most common benign lesions [1] of vocal cords caused by vocal disturbances [2, 3]. The most common clinical symptoms are different degrees of roughness and feeling of a foreign body [4]. These voice pathologies are not life-threatening disorders but may limit communication activities and consequently, voice disorders can affect the quality of life [5]. Therefore, an assessment of different dimensions of voice in these pathologies seems necessary.
The use of specific instruments to investigate voice and its physical parameters is known as acoustic analysis, which comprises an assessment procedure for patients suffering from mass lesions, including polyps and nodules [6]. Acoustic analysis of voice is a non-invasive, quantitative, economical, convenient, and rapid procedure compared to other assessment methods, such as electroglottographic [7] and video-laryngostroboscopic evaluations [8, 9].
The computerized multidimensional acoustic voice analysis enables visual and numerical analysis of the voice samples. Such analysis programs provide objective data and support subjective voice evaluation [2], which helps monitor clinical procedures and compare the results pre and post-intervention in experimental studies. The acoustic parameters measured in the most of studies are fundamental frequency (F0), amplitude perturbation or shimmer, frequency perturbation or jitter, and noise-to-harmonic ratio (NHR).
In terms of physiological characteristics of vocal folds, F0 as one of the most important voice parameters for the acoustic voice measures shows the number of vocal cords’ cover layer vibrations per second [10]. The intensity corresponding to loudness is the other acoustic voice measure frequently reported in the literature. Jitter and shimmer have been designed to measure two important aspects of acoustic voice parameters in a signal, frequency, and amplitude perturbation, respectively. In terms of physiological characteristics, the rate of perturbation increases with advancing the disturbances of the vocal folds. A close relationship exists between the increase in perturbation and the change in voice quality, such as breathiness and hoarseness [11].
It appears that the existence of vocal cord polyps and nodules contributes to changes in voice quality and acoustic voice parameters. Petrovic-Lazic et al. studied the acoustic voice parameters of patients with vocal fold polyps and healthy individuals using MDVP software. They reported that jitter (%), shimmer (%), and NHR values significantly differentiated the patients with vocal fold polyps from the vocally healthy group [2]. Kandogan and Ozuer also observed the values of jitter and shimmer increased in people with vocal folds lesions, such as vocal cord polyps, nodules, Reinke edema, and cysts using MDVP. They investigated 25 patients with vocal nodules, 29 patients with vocal cord polyps, 15 patients with Reinke edema, and 8 patients with vocal cord cysts [12]. Two studies demonstrated that NHR values in patients with vocal cord nodules were not statistically different from the control group [6, 13].
Considering contradictory results for NHR, we decided to conduct this study. Additionally, the acoustic voice parameters of patients with vocal cord nodules and polyps and healthy controls were compared in terms of sex.
2. Materials and Methods
Study design
The present project was a cross-sectional case-control study. Sixty-eight patients with vocal cord nodules and polyps who visited the speech therapy clinic of Ayatollah Rouhani Hospital in Babol City, Iran, in 2016-2017 were recruited in the current research.
Participants
A total of 110 participants in three groups, including patients with nodules, patients with polyps, and healthy subjects were recruited in the current research. Table 1 presents the distribution of the subjects in terms of sex. The video-laryngostrobosspic examination was performed by the experienced speech and language pathologist (SLP) by corresponding author and the diagnosis of vocal nodules and polyps was confirmed by an otolaryngologist. In the healthy group, individuals who had no history of voice disorders and had intact larynx were included based on video-laryngostroboscopic examination. The exclusion criteria for all groups included other structural disorders, such as Reinke’s edema, cysts, sulcus vocalis, granuloma, neurological disorders, such as vocal cord paralysis, multiple sclerosis, Parkinson’s disease, psychological problems, and history of cold and flu before 2 weeks ago.
Ethical approval
The current study was approved by the Ethics Committee of Babol University of Medical Sciences (MUBABOL.HRI.REC.1396.60). The participants were given the signed consent form and requested to complete it before the sampling procedure.
Procedure
The participants’ demographic data were gathered via an interview and a questionnaire containing demographic information and the medical history of the subjects. We asked the participants to sit in an upright posture and produce prolonged /â/ vowel (at least 5 seconds) with habitual intensity and pitch three times. The procedure was conducted in the sound-attenuated room. MDVP software (MDVP, Elemetrics K. Kay Elemetrics Visi-Pitch IV model 3950 instruction manual) was utilized to measure the traditional acoustic voice parameters. The recorder (Model: Lincoln Park, NJ) was applied to record the voice samples of the participants using the microphone (model: SM48, assembled in Mexico) with a 20 cm constant distance [14].
In case of any unwanted sampling error, the test was repeated. In this step, the clearest voice sample of each subject was chosen for analysis. We removed the onset and offset of each segment and the middle part of the segment was exposed to measure the acoustic voice parameters. Then, the acoustic voice parameters (jitter, shimmer, fundamental frequency, and NHR) were analyzed.
Measures and analyses
The SPSS software v. 18.0 (SPSS, Inc., Chicago, Illinois) was applied for the statistical analysis of data. Descriptive statistics were used to report the age, group, and sex of the participants. After investigating the normality of the distribution of the data by Kolmogorov Smirnov test, we used 1-way analysis of variance (ANOVA) test to compare each variable (jitter, shimmer, fundamental frequency, and NHR) in three groups. Moreover, 1-way analysis of variance (ANOVA) test was applied to compare the acoustic voice parameters among three groups in males and females. The significance level was considered (P<0.05).
3. Results
As provided in Table 2, three groups showed a significant difference in the fundamental frequency (P<0.001). Women had a significant difference in the fundamental frequency in the three groups (P<0.001), but the difference was not statistically evident in men (P=0.93).
In Table 3, the two groups had statistically significant differences for the jitter (P<0.001). Also, for jitter measurement, men (P<0.001) and women (P<0.001) had a significant difference in the three groups.
Table 4 presents the mean and standard deviation values of shimmer in three groups. As found in Table 4, they had a statistical difference for the shimmer (P<0.001). In addition, men had a significant difference in shimmer (P=0.001). Evident differences were observed for the shimmer in the women (P<0.001) and men (P=0.001).
Moreover, according to Table 5, the NHR was significantly different among the three groups. Men did not have a significant difference in NHR (P=0.24), but women showed substantial differences (P=0.01).
4. Discussion
In the current study, four acoustic voice parameters were analyzed, such as F0, jitter, shimmer, and NHR which are the most common acoustic voice measures in most studies.
The mean value of fundamental frequency is defined as the overall mean of all extracted period-to-period fundamental frequency measures in the voice sample [15]. In our study, the F0 was lower in men than in women, as expected, according to the differences in vocal fold characteristics between men and women [16, 17]. Similar to Halawa et al work, our result showed that F0 decreased in patients with vocal cord nodules and polyps. It can be attributed to the existence of extra mass on the surface of vocal folds thickening them [18]. Furthermore, the F0 of female patients was significantly lower than in the control group.
Jitter is defined as the short-term and cycle-to-cycle perturbation in the F0 of the voice [15]. The mean values of jitter showed a significant increase in both patient groups rather than the healthy group similar to some existing research [6]. Also, jitter increased in both females and males with nodules compared to the control group. This finding is consistent with some studies [3] but is not consistent with the result obtained by Chhetri et al. [6]. This significant increase can be caused by small growth on the surface of the vocal folds in mass lesions, such as polyps and nodules [2]. Even very minimal growths on vocal folds may impact the jitter, and larger pathologies may result in more increased jitter [15]. It appears that increasing in jitter correlates with the number of active motor neurons and the increase in decreasing the control of muscle tone in the larynx [2].
Shimmer refers to the cycle-to-cycle, short-term perturbation in the amplitude of voice [15]. The mean values of shimmer showed a significant increase in the patients’ group than the control one. In addition, the mean value of shimmer was significantly higher in both sexes of both case groups rather than the control group. This finding is consistent with several studies [2, 6]. This significant difference would be probably related to incompatible and weak contact of vocal fold edges due to glottis closure deficiency [15].
Based on the findings of the present research, the mean value of NHR in the group of patients with nodules increased significantly. While NHR values were increased in vocal polyps and nodules in both genders of patient groups, this increase was only significant in women with vocal polyps. These results were consistent with some studies [6, 13]. It can be caused by an incomplete closure of the glottis due to polyps leading to an air leakage [15] acoustically characterized as a noisy voice. The relative values of additional noise in the voice signal are quantified by NHR arising from the air-flow turbulence produced at the glottis during the phonation process. Insufficient closure of vocal cords causes exceeding values of airflow in the glottis, resulting in turbulent airflow [19].
5. Conclusion
Every small variation of the mass, biochemical and biomechanical characteristics of vocal folds, can easily lead to rapid disturbances and cyclic changes in the intensity and frequency of voice resulting from the vibration of the vocal folds’ cover layer. According to the findings of this study, it can be concluded that the weak and unstable closure of the glottis, resulting from the vocal fold nodules and or polyp, causes lower fundamental frequency and higher jitter, shimmer, and NHR values. Finally, by the computerized voice analysis procedures, one can provide an objective, accurate, and reliable examination of the vocal performance and quantitatively represent the voice quality.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects. principles of the Helsinki Convention was also observed.
Funding
This study was financially supported by Babol University of Medical Sciences.
Authors' contributions
Conceptualization and Supervision: Mehdi Dehghan, Keivan Kiakojouri; Methodology: Mehdi Dehghan and Hemmat Gholinia; Investigation: Mehdi Dehghan and Mohaddeseh Rostampourgonbaki; Writing–original draft: Mohaddeseh Rostampourgonbaki and Niloofar Dehghanpour; Writing–review & editing: Mehdi dehghan, Mohaddeseh Rostampourgonbaki.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Research Vice-chancellor at the Babol University of Medical Sciences, the Clinical Research Development Center of Ayatollah Rouhani Hospital in Babol, and Mohammad Ali Shams for their material and spiritual support in the implementation of the study.
References
- Jiang JJ, Zhang Y, MacCallum J, Sprecher A, Zhou L. Objective acoustic analysis of pathological voices from patients with vocal nodules and polyps. Folia Phoniatrica Et Logopaedica : Official Organ of the International Association of Logopedics and Phoniatrics (IALP. 2009; 61(6)342-9. [PMID] [PMCID]
- Petrović-Lazić M, Babac S, Vuković M, Kosanović R, Ivanković Z. Acoustic voice analysis of patients with vocal fold polyp. Journal of Voice: Official Journal of the Voice Foundation. 2011; 25(1):94-7. [PMID]
- Valadez V, Ysunza A, Ocharan-Hernandez E, Garrido-Bustamante N, Sanchez-Valerio A, Pamplona MC. Voice parameters and videonasolaryngoscopy in children with vocal nodules: A longitudinal study, before and after voice therapy. International Journal of Pediatric Otorhinolaryngology. 2012; 76(9):1361-5. [PMID]
- Sataloff RT. Otolaryngology: Head & neck surgery: Pediatric otolaryngology. New Delhi: Jaypee Brothers Medical Publishers Pvt. Limited; 2015. [Link]
- Schindler A, Mozzanica F, Maruzzi P, Atac M, De Cristofaro V, Ottaviani F. Multidimensional assessment of vocal changes in benign vocal fold lesions after voice therapy. Auris, Nasus, Larynx. 2013; 40(3):291-7. [PMID]
- Chhetri SS, Gautam R. Acoustic analysis before and after voice therapy for laryngeal pathology. Kathmandu University Medical Journal (KUMJ). 2015; 13(52):323–7. [PMID]
- Marasek K. An attempt to classify Lx signals. In: Fourth European Conference on Speech Communication and Technology; 1995. [Link]
- Deliyski D. High-speed videoendoscopy: Recent progress and clinical prospects. Proc. Advances in Quantitative Laryngology (AQL). 2006:1-16. [Link]
- Akbari E, Seifpanahi S, Ghorbani A, Izadi F, Torabinezhad F. The effects of size and type of vocal fold polyp on some acoustic voice parameters. Iranian Journal of Medical Sciences. 2018; 43(2):158-63. [PMID]
- Colton RH, Casper JK, Leonard R. Understanding voice problems: A physiological perspective for diagnosis and treatment. Philadelphia: Lippincott Williams & Wilkins; 2006. [Link]
- Sapienza C, Hoffman B. Voice disorders. California: Plural Publishing, Incorporated; 2016. [Link]
- Kandoğan T, Ozuer MZ. Acoustic difference in voice of the patients with and without organic lesion in functional voice disorders. KBB-Forum. 2007; 6(2):46-8. [Link]
- Campisi P, Tewfik TL, Pelland-Blais E, Husein M, Sadeghi N. MultiDimensional voice program analysis in children with vocal cord nodules. The Journal of Otolaryngology. 2000; 29(5):302-8. [Link]
- Elemetrics K. Kay Elemetrics Visi-Pitch IV, model 3950 instruction manual. Lincoln Park, NJ: Author, 2004. [Link]
- Oguz H, Tarhan E, Korkmaz M, Yilmaz U, Safak MA, Demirci M, et al. Acoustic analysis findings in objective laryngopharyngeal reflux patients. Journal of Voice: Official Journal of the Voice Foundation. 2007; 21(2):203-10. [PMID]
- Demirhan E, Unsal EM, Yilmaz C, Ertan E. Acoustic voice analysis of young Turkish speakers. Journal of Voice: Official Journal of the Voice Foundation. 2016; 30(3):378.e21-5. [PMID]
- Kent RA, Read C. The acoustic analysis of speech. Second edition. Albany, NY: Thomson Learning; 2002. [Link]
- Halawa WE, Rodríguez Fernández Freire A, Muñoz IV, Pérez SS. Assessment of effectiveness of acoustic analysis of voice for monitoring the evolution of vocal nodules after vocal treatment. European Archives of Oto-Rhino-Laryngology. 2014; 271(4):749-56. [PMID]
- Ferrand CT. Harmonics-to-noise ratio: An index of vocal aging. Journal of Voice. 2002; 16(4):480-7. [10.1016/S0892-1997(02)00123-6]
Article type: Original Research Articles |
Subject:
Speech therapy
Received: 2021/12/16 | Accepted: 2022/05/14 | Published: 2022/09/19
Received: 2021/12/16 | Accepted: 2022/05/14 | Published: 2022/09/19
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
