
988368
Tue, Jul 1, 2025

Volume 21, Issue 1 (March 2023)
Iranian Rehabilitation Journal 2023, 21(1): 157-166 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohan M, Deb R. Factors Associated With Resilience Among People With Spinal Cord Injury in the Community Setting. Iranian Rehabilitation Journal 2023; 21 (1) :157-166
URL: http://irj.uswr.ac.ir/article-1-1682-en.html
URL: http://irj.uswr.ac.ir/article-1-1682-en.html



1- Amity Institute of Anthropology, Amity University, Noida, India.
Full-Text [PDF 1204 kb]
(954 Downloads)
| Abstract (HTML) (2257 Views)
Full-Text: (502 Views)
1. Introduction
Spinal cord injury (SCI) has a tremendous impact on survivors, their families, and society at large and has been linked to serious outcomes, including morbidity, mortality, poor quality of life (QoL), and not being able to fully integrate into the community. It is a long-term disabling condition, which poses a major public health challenge [1]. In India, the average annual incidence of SCI is 15,000 with a prevalence of 0.15 million [2]. The World Health Organization (WHO) reports that SCI is becoming more common in developing nations, like India. SCI is a leading cause of paralysis. The injury can be complete or incomplete, which leads to functional impairment below the level of the lesion. Besides, people with SCI tend to experience a higher prevalence of emotional distress, substance abuse, and secondary health conditions/ multi-morbidities (such as chronic pain, pressure ulcer, spasticity, urinary tract infection, gastrointestinal issues, deep vein thrombosis, etc.), which has a substantial impact on person's QoL and worsens rehabilitation [3, 4]. In contrast, positive outcomes are associated with continuing rehabilitation and involvement in meaningful activities, which help SCI individuals to reintegrate well into the community and overcome the trauma. Recent studies have investigated resilience in SCI people who are living with challenging and potentially distressing injuries. Resilience is a complex process that varies according to circumstances, time, age, gender, employment, social participation as well as cultural origin, and it involves qualities that enable one to cope and adapt to the consequences of chronic health conditions, such as SCI [4, 5]. Connor and Davidson defined resilience as basically an individual’s capacity to survive after any trauma, or hardship or overcome the stressful and catastrophic life changes/challenges, which arise from the consequences of SCI. People having resilience are better able to adjust to or adapt to new circumstances, overcome challenges, or safeguard their mental and physical well-being [6].
Resilience can vary due to the presence of different factors, such as demographic and injury-related variables, time since injury, QoL, and social participation in people with SCI [4, 5, 7, 8]. Patients who are found to be resilient have more content, a better QoL, are very well integrated into the community, have greater acceptance, and less behavioral disengagement and these characteristics are positively associated with life satisfaction, optimism, and self-efficacy for individuals experiencing more than one year after their injury. Individuals having old age exhibited higher resilience [5, 9]. It was seen that in terms of level of resilience, resilience varied among professionals (employed and unemployed). Further, it depended on the marital status of the person.
Very few studies have been done on resilience among people with SCI in India. As a developing county, the cultural context, geography, resources, opportunities, and availability of the healthcare system are completely different from the western world. Therefore, the present study was carried out to evaluate the qualitative quantum of resilience among people who sustained SCI and study its association with QoL, community integration, and injury-related variables.
2. Material and Methods
Study design, study area, and subjects
This cross-sectional study was carried out between January 2021 and October 2021. The SCI participants were recruited from the Kusum spine and neuro rehabilitation (KSNR) in Vasant Kunj Delhi. In the present study, the participants aged 18 years or older, with sustained SCI (both traumatic and non-traumatic), living in the community for at least one year after injury, admitted/visited the KSNR for rehabilitation who were able to read, speak, understand Hindi or English and conscious with no cognitive disability (this was checked with the information provided and mentioned in the medical records and history) were approached for data collection. Participants who did not give consent and had co-morbidities, like cognitive dysfunction and vulnerable participant groups were excluded as they were unable to cooperate in the study.
Study tools/techniques
The data were collected using a structured schedule with demographic and injury-related variables. The injury-related data comprised injury level, injury cause, comorbidities related to SCI, and time since injury. The injury-related variables were cross-checked from the medical records of each participant and confirmed during the interview.
Three standardized research tools were used for data collection.
The Connor-Davidson resilience scale (CD-RISC) is a tool to assess resilience after any adversity or stressful event. It majorly comprises five dimensions: Tenacity and competency, tolerance of negative affect, trust in one’s instincts; positive acceptance of change and secure relationships, control, and spiritual impacts. There are only three versions, which are authorized by the developer to use academically, i.e. CD-RISC-2, CD-RISC-10, and CD-RISC-25. In the present study, CDRISC 10 was applied. It consists of ten items and scores ranged from 0 (not true at all) to 4 (true nearly all of the time) on a 5-point Likert scale. There are a total of 0 to 40 possible scores; higher values denote stronger resilience6. The tool has proven its validity and reliability in persons with SCI [10, 11, 12, 13, 14].
The World Health Organization-Quality of life Brief (WHO-QoL Brief) is a brief version of WHOQOL-100. The scale is used to measure the QoL of individuals and populations. WHOQOL-BREF is a 26-item version of the WHOQOL-100. The WHOQOL-BREF questionnaire was developed by WHO in the context of four domains (physical, psychological, social, and environmental) and two items based on the overall QoL. A higher score indicates better QoL and a positive inclination towards life satisfaction. The domain scores were transformed into a linear scale between 0 and 100 following the scoring guidelines [15]. The WHOQOL-BREF has proved suitable for measuring the QoL in patients with SCI and has shown significant results and proven content validity, internal consistency, and test-retest reliability [16, 17]. population through the following methods, i.e. in person, by telephone, or can be self-administered [15, 18].
The community integration questionnaire-revised (CIQ-R) is used to gather information about how connected people are to their communities. The CIQ-R is an 18-item questionnaire, which has four subscales: Home integration–how actively the person is involved in house chores, Social Integration–how well the participant is socially active and interactive, Productivity–this part explains the participant’s current employment status, education as well as any participation in volunteer activities, and electronic social networking (ESN) – this helps find out how well the participant involves in social networking through electronic devices [19, 20, 21]. Although the scale was originally developed for brain injury patients to measure their extent of participation in the community; now, it can be used for people with SCI. Also, the instrument was found to be precise, feasible, and easy to administer [11, 22]. It takes approximately 10-15 minutes to complete (in one participant). Researchers can collect the data on this instrument via telephone, or face-to-face, or it can be self-administered by the participant. Its validity and reliability (in SCI population) have been already approved [11, 20, 21].
Data collection
All data were collected via telephone interviews within 10 months. The sample size was calculated through online software i.e. nMaster 2.0. Of 150 patients with SCI admitted to the KSNR in the past few years, the contact information of 120 individuals was obtained from the center. Out of 120 SCI individuals, only 108 met the inclusion/exclusion criteria. Therefore, the convenience sampling method was used to employ 108 participants and they all were contacted via telephone. Participation was entirely voluntary. No further calls were made to case study participants or care providers who declined to take part. Before the study began, informed consent was obtained from each participant.
Data analysis
SPSS software, version 23.0 was used to perform statistical analysis. Demographic and injury-related data were examined using descriptive statistics. All continuous variables were expressed as Mean±SD or median with the interquartile range as per the distribution of data. Categorical variables are shown in terms of number and their respective percentage. Shiparo-Wilk test was applied to determine the normality of the data. All the variables were observed to follow a normal distribution. Independent t-tests and ANOVA were used to determine the significant difference in the CDRIDC score among patients of different categories. The extent of the linear relationship between resilience and independent variables was determined by Pearson’s correlation and Point-Biserial correlation, which depended on the level of measurement of each variable. Univariate and multivariate linear regression analyses were used to identify the influence of demographic and injury-related factors on resilience. Variables meeting the assumptions of normality, linearity, homo-scedasticity, and multicollinearity were included in the linear regression. All the calculated P were two-sided and P<0.05 were considered to be statistically significant.
3. Results
Participants consisted of 24 females with a mean age of 30.24±8.50 years and 84 males with a mean age of 31.59±10.61. It was observed that 88% of participants (n=95) had comorbidities related to SCI where spasticity (n=60, 55.5%) was the most common comorbidity followed by pain (n=45, 41.6%) and urological complications (n=31, 28.7%). Respiratory issues (n=8, 7.4%) were the least common comorbidity. The mean time elapsed since injury was found to be 64.6 months.
The etiology of injuries consisted of 96 cases of traumatic SCI and 12 cases of non-traumatic SCI. The most common etiology of traumatic SCI was found to be transport-related injuries (n=56, 51.9%), followed by falls (n=32, 29.6%). The etiology of non-traumatic SCI varied considerably, including tumors, infections, etc. Seventy-eight percent (n=84) of the participants reported moderate-to-high scores on the CD-RISC 10 (that is, score range 20–35), indicating that resilient qualities and behaviors were present to some extent. However, the average CD-RISC score of the participants was 27.06±6.87. Descriptive statistics for WHO-QoL were as follows: Physical domain (53.67±19.2, actual score range=15-94), psychological (53.88±23.70, actual score range=6-94), social relationships domain (48.73±25.00, actual score range=2-100), environment domain (58.97±20.90, actual score range=18-100) and community participation (CIQ-R) (16.21±5.44, actual score range=4-28.25).
Point-Biserial correlation analysis indicated a mild, however, significant negative correlation between marital status and resilience (r=-0.247, P=0.010). However, a significant positive correlation was found between time since injury and resilience (r=0.2, P=0.038) (Figure 1).
.jpg)
In addition, QoL and community integration among the participants were also found to be positively correlated with resilience (overall health; r=0.317, P=0.001, physical health; r=0.31, P=0.001, psychological; r=0.48, P=0.000, environment; r=0.184, P=0.057) and are presented through scatter plot in Figure 2.
.jpg)
Similarly, a non-significant strong positive association was found between resilience and QoL and social relationships (r=0.178, P=0.065). While resilience and other demographic factors (such as age, gender, family type, and family income) were not found to be significantly associated. Independent t-test and ANOVA were used to determine the significant difference in the resilience score and demographics/injury-related variables among the study participants. Demographic and injury-related variables, such as marital status and frequency of going out from home were found to be significant.
It was found that unmarried participants (28.39±5.70) were more resilient as compared to married individuals (25.39±8.35) (P=0.029). Similarly, those visiting daily outside their homes (28.12±6.59) and participating in community activities were more resilient compared to those who do not prefer to go out regularly (P=0.051). However, a non-significant association was found among the variables, such as gender, place of residence, geographical area, family type, employment after injury, education, religion, monthly family income, and type of floor (Table 1).
.jpg)
Univariate and multivariate linear regression analyses were performed to identify the demographic determinants that contribute to resilience. Gender, geographic area (rural/urban), marital status, and employment were found to be statistically significant factors affecting resilience in univariate analysis. Multivariate analyses were performed using these significant variables. In multivariate analysis, gender, marital status, and profession were found to be significant. Among these predictors, employment presented a higher beta value (β=0.684 P=0.026) signifying that employment (after injury) was the most significant demographic characteristic of resilience. QoL factors were not included in the linear regression as they did not satisfy the assumption of linear regression (Table 2).
.jpg)
Also, resilience was varying among different categories of age groups (Supplementary Table 1).
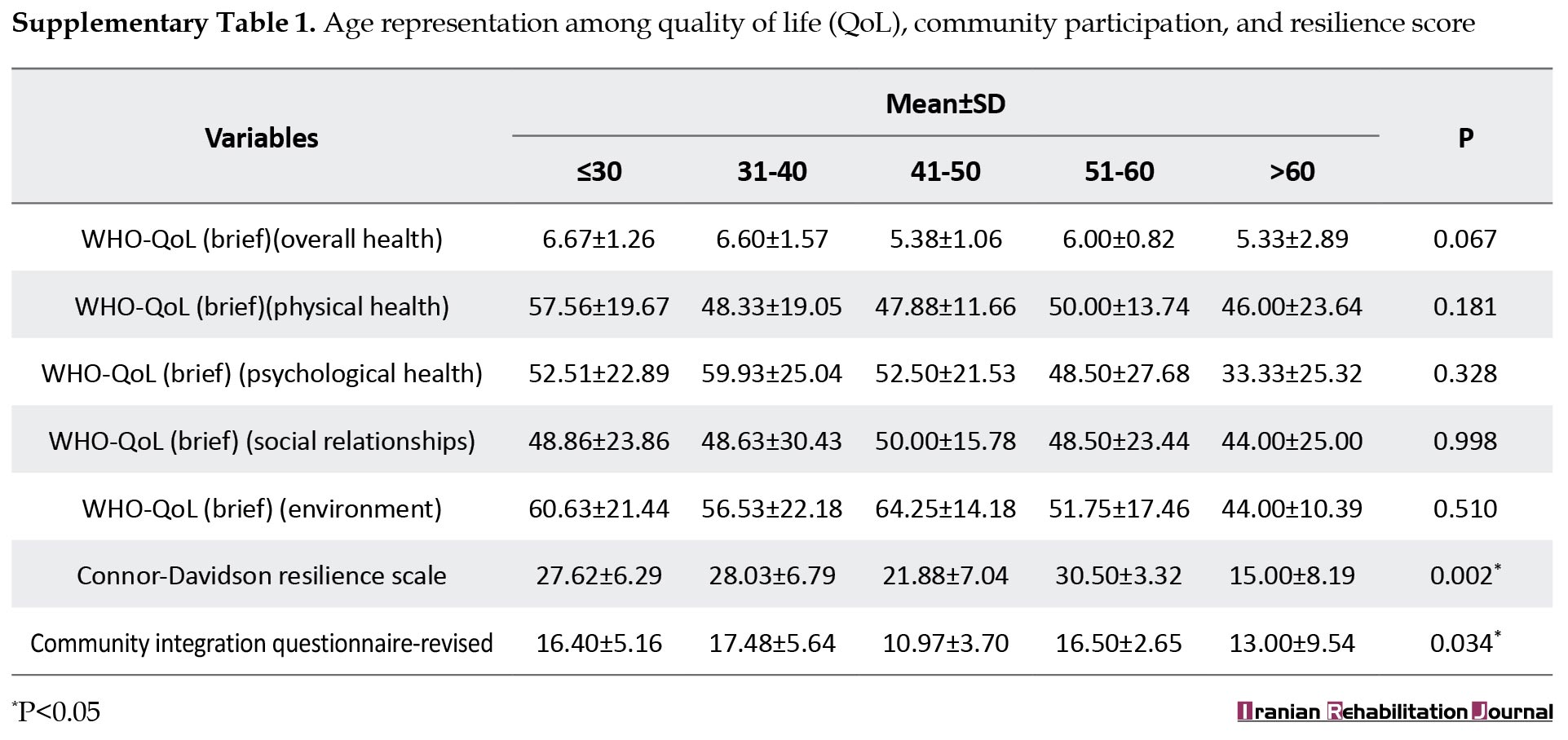
However, other demographic and injury-related variables did not significantly contribute to resilience (P>0.05). CDRISC and CIQ-R were found to vary statistically significantly among participants (P≤0.05). The highest mean CDRISC score was found to be 30.5±3.32 for patients in the age group of 51-60 years followed by a CDRIC score of 28.3±6.79 in the age group of 31-40 years. The lowest CDRISC score was 15±8.19 for elderly patients (>60 years). Furthermore, CIQ-R was found to be highest (17.48±5.64) for patients in the 31-40 age group whereas it was found to be lowest (10.97±3.70) for patients in the age group of 41-50 years.
4. Discussion
This study looked at the level of resilience among SCI individuals living in the community, as well as the relationship between resilience and demographic parameters/injury-related variables, QoL, and community participation. Currently, there is a paucity of published research in low-middle-income countries on resilience among the SCI population post-injury [8]. The participants in the present study were from different backgrounds and places and had been suffering from either traumatic or non-traumatic SCI. Furthermore, SCI is a condition that drastically disrupts a person's life and has a negative impact on physical, psychological, and social aspects, this results in poor participation in the community. Depending on the level and severity of the injury, individuals with SCI may experience complete or incomplete muscle paralysis and loss of sensation, leading to many secondary complications [4, 23]. Because the individuals in this study were exposed to these adversities, they were more likely to suffer from the detrimental effects of spinal cord damage. The findings of the present study are in continuation with the previously published studies and offer some intriguing facts with respect to SCI individuals' resilience, its association with their QoL, and their participation in the community. Physical, psychological, and environmental domains of QoL and level of community participation were significantly associated with resilience among the study participants. Employment was found to be the most significant determinant of resilience in the present study. Participants who were unemployed indicated poor mean resilience, which is consistent with earlier findings [24, 25, 26]. In a postal survey conducted in India with a sample size of 600, no individual had a job living in the community while the employment rate was 41% for those who were working in non-governmental organizations (NGO) or the centers run by armed forces [27].
The consequences of unemployment lead to poor QoL, low resilience status, decreased independence, depression, poor social integration, etc. [27]. When striving to work after SCI, there are facilitators to be explored (e.g. education, transportation, assistive technology) and barriers that need management (e.g. secondary medical complications). There were few studies that examined the association between resilience and employment status [8, 28]. Of the three, two studies found a significant positive correlation between resilience and employment [8, 26]. Employment is a significant variable, which helps an individual to become self-independent and not rely financially on others and also increases the sense of self-worth and satisfaction with life leading to improved resilience [26, 29].
The results of the study also revealed that married patients were less resilient in their lives compared to unmarried patients. Besides, findings interpret that the frequency of divorce was quite high among female patients compared to male sufferers. However, the majority of the participants in the present study were classified as married and were still living with their partners, and most of them were cared for by their partners or other family members. As all the patients studied were living in the community (at least one-year post-injury), the majority of them were not the earning members of their respective families due to their injury. As per the study findings, unmarried people were more resilient and content with their life, but married people were found more dissatisfied and disappointed because of the stress of not functioning normally in the household. The same has been reported in a study conducted on 276 SCI patients to test statistically the experience of fewer marriages and more divorces after the injury [30]. Furthermore, in the present study, the resilience score among the participants was found to be highest in the upper age groups (i.e. 51-60 years) and quite low in the younger and middle-aged cases (18-40 years), which were similar to the other findings [14]. These findings could be explained by managing a life-altering event, such as SCI the young and middle age groups when the individuals were not in a position to accept it, and people of these age groups are quite aggressive and enthusiastic towards their work and family [21]. In addition, secondary health conditions after the tragic events were more taxing. Thus, this could be one of the potential reasons for their poor resilience score. The lowest resilience score was reported amongst elderly participants due to various associated reasons, such as high levels of dependency, secondary health conditions (pain, spasticity), as well as social isolation [14].
5. Conclusion
The results indicated that physical health, psychological health, environmental factors, overall participation in the community as well as demographic variables (such as marital status and frequency of going out of their homes) were strongly associated with resilience. Furthermore, employment was found to be a highly significant determinant of resilience. According to the findings, it is important for healthcare professionals to screen sufferers with fewer resources, such as the unemployed, those from backward places, like rural areas, those emotionally weak cases, cases with poor participation in the community, etc. to provide better care and support through community-based or home-based or telerehabilitation programs, such as vocational rehabilitation support, which includes stress management, focus on independence, optimism, social support, communication and understanding, spousal involvement as well as awareness about the injury to help strengthen the resilience. This will help those who have been traumatized due to SCI and have a low level of resilience. Therefore, this will not only help enhance resilience among SCI people but will also aid in their effective reintegration into society.
Ethical Considerations
Compliance with ethical guidelines
The study got clearance from the Institutional Ethics Committee of the Indian Spinal Injuries Center (Vasant Kunj Reference No.: ISIC/RP/2020/15).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, writing–review & editing: Meenakshi Mohan and Roumi Deb; Methodology, investigation, writing–original draft, data collection and data analysis: Meenakshi Mohan.
Conflict of interest
We certified that there is no actual or potential conflict of interest in relation to this research work.
Acknowledgments
All authors declared no conflict of interest.
References
Spinal cord injury (SCI) has a tremendous impact on survivors, their families, and society at large and has been linked to serious outcomes, including morbidity, mortality, poor quality of life (QoL), and not being able to fully integrate into the community. It is a long-term disabling condition, which poses a major public health challenge [1]. In India, the average annual incidence of SCI is 15,000 with a prevalence of 0.15 million [2]. The World Health Organization (WHO) reports that SCI is becoming more common in developing nations, like India. SCI is a leading cause of paralysis. The injury can be complete or incomplete, which leads to functional impairment below the level of the lesion. Besides, people with SCI tend to experience a higher prevalence of emotional distress, substance abuse, and secondary health conditions/ multi-morbidities (such as chronic pain, pressure ulcer, spasticity, urinary tract infection, gastrointestinal issues, deep vein thrombosis, etc.), which has a substantial impact on person's QoL and worsens rehabilitation [3, 4]. In contrast, positive outcomes are associated with continuing rehabilitation and involvement in meaningful activities, which help SCI individuals to reintegrate well into the community and overcome the trauma. Recent studies have investigated resilience in SCI people who are living with challenging and potentially distressing injuries. Resilience is a complex process that varies according to circumstances, time, age, gender, employment, social participation as well as cultural origin, and it involves qualities that enable one to cope and adapt to the consequences of chronic health conditions, such as SCI [4, 5]. Connor and Davidson defined resilience as basically an individual’s capacity to survive after any trauma, or hardship or overcome the stressful and catastrophic life changes/challenges, which arise from the consequences of SCI. People having resilience are better able to adjust to or adapt to new circumstances, overcome challenges, or safeguard their mental and physical well-being [6].
Resilience can vary due to the presence of different factors, such as demographic and injury-related variables, time since injury, QoL, and social participation in people with SCI [4, 5, 7, 8]. Patients who are found to be resilient have more content, a better QoL, are very well integrated into the community, have greater acceptance, and less behavioral disengagement and these characteristics are positively associated with life satisfaction, optimism, and self-efficacy for individuals experiencing more than one year after their injury. Individuals having old age exhibited higher resilience [5, 9]. It was seen that in terms of level of resilience, resilience varied among professionals (employed and unemployed). Further, it depended on the marital status of the person.
Very few studies have been done on resilience among people with SCI in India. As a developing county, the cultural context, geography, resources, opportunities, and availability of the healthcare system are completely different from the western world. Therefore, the present study was carried out to evaluate the qualitative quantum of resilience among people who sustained SCI and study its association with QoL, community integration, and injury-related variables.
2. Material and Methods
Study design, study area, and subjects
This cross-sectional study was carried out between January 2021 and October 2021. The SCI participants were recruited from the Kusum spine and neuro rehabilitation (KSNR) in Vasant Kunj Delhi. In the present study, the participants aged 18 years or older, with sustained SCI (both traumatic and non-traumatic), living in the community for at least one year after injury, admitted/visited the KSNR for rehabilitation who were able to read, speak, understand Hindi or English and conscious with no cognitive disability (this was checked with the information provided and mentioned in the medical records and history) were approached for data collection. Participants who did not give consent and had co-morbidities, like cognitive dysfunction and vulnerable participant groups were excluded as they were unable to cooperate in the study.
Study tools/techniques
The data were collected using a structured schedule with demographic and injury-related variables. The injury-related data comprised injury level, injury cause, comorbidities related to SCI, and time since injury. The injury-related variables were cross-checked from the medical records of each participant and confirmed during the interview.
Three standardized research tools were used for data collection.
The Connor-Davidson resilience scale (CD-RISC) is a tool to assess resilience after any adversity or stressful event. It majorly comprises five dimensions: Tenacity and competency, tolerance of negative affect, trust in one’s instincts; positive acceptance of change and secure relationships, control, and spiritual impacts. There are only three versions, which are authorized by the developer to use academically, i.e. CD-RISC-2, CD-RISC-10, and CD-RISC-25. In the present study, CDRISC 10 was applied. It consists of ten items and scores ranged from 0 (not true at all) to 4 (true nearly all of the time) on a 5-point Likert scale. There are a total of 0 to 40 possible scores; higher values denote stronger resilience6. The tool has proven its validity and reliability in persons with SCI [10, 11, 12, 13, 14].
The World Health Organization-Quality of life Brief (WHO-QoL Brief) is a brief version of WHOQOL-100. The scale is used to measure the QoL of individuals and populations. WHOQOL-BREF is a 26-item version of the WHOQOL-100. The WHOQOL-BREF questionnaire was developed by WHO in the context of four domains (physical, psychological, social, and environmental) and two items based on the overall QoL. A higher score indicates better QoL and a positive inclination towards life satisfaction. The domain scores were transformed into a linear scale between 0 and 100 following the scoring guidelines [15]. The WHOQOL-BREF has proved suitable for measuring the QoL in patients with SCI and has shown significant results and proven content validity, internal consistency, and test-retest reliability [16, 17]. population through the following methods, i.e. in person, by telephone, or can be self-administered [15, 18].
The community integration questionnaire-revised (CIQ-R) is used to gather information about how connected people are to their communities. The CIQ-R is an 18-item questionnaire, which has four subscales: Home integration–how actively the person is involved in house chores, Social Integration–how well the participant is socially active and interactive, Productivity–this part explains the participant’s current employment status, education as well as any participation in volunteer activities, and electronic social networking (ESN) – this helps find out how well the participant involves in social networking through electronic devices [19, 20, 21]. Although the scale was originally developed for brain injury patients to measure their extent of participation in the community; now, it can be used for people with SCI. Also, the instrument was found to be precise, feasible, and easy to administer [11, 22]. It takes approximately 10-15 minutes to complete (in one participant). Researchers can collect the data on this instrument via telephone, or face-to-face, or it can be self-administered by the participant. Its validity and reliability (in SCI population) have been already approved [11, 20, 21].
Data collection
All data were collected via telephone interviews within 10 months. The sample size was calculated through online software i.e. nMaster 2.0. Of 150 patients with SCI admitted to the KSNR in the past few years, the contact information of 120 individuals was obtained from the center. Out of 120 SCI individuals, only 108 met the inclusion/exclusion criteria. Therefore, the convenience sampling method was used to employ 108 participants and they all were contacted via telephone. Participation was entirely voluntary. No further calls were made to case study participants or care providers who declined to take part. Before the study began, informed consent was obtained from each participant.
Data analysis
SPSS software, version 23.0 was used to perform statistical analysis. Demographic and injury-related data were examined using descriptive statistics. All continuous variables were expressed as Mean±SD or median with the interquartile range as per the distribution of data. Categorical variables are shown in terms of number and their respective percentage. Shiparo-Wilk test was applied to determine the normality of the data. All the variables were observed to follow a normal distribution. Independent t-tests and ANOVA were used to determine the significant difference in the CDRIDC score among patients of different categories. The extent of the linear relationship between resilience and independent variables was determined by Pearson’s correlation and Point-Biserial correlation, which depended on the level of measurement of each variable. Univariate and multivariate linear regression analyses were used to identify the influence of demographic and injury-related factors on resilience. Variables meeting the assumptions of normality, linearity, homo-scedasticity, and multicollinearity were included in the linear regression. All the calculated P were two-sided and P<0.05 were considered to be statistically significant.
3. Results
Participants consisted of 24 females with a mean age of 30.24±8.50 years and 84 males with a mean age of 31.59±10.61. It was observed that 88% of participants (n=95) had comorbidities related to SCI where spasticity (n=60, 55.5%) was the most common comorbidity followed by pain (n=45, 41.6%) and urological complications (n=31, 28.7%). Respiratory issues (n=8, 7.4%) were the least common comorbidity. The mean time elapsed since injury was found to be 64.6 months.
The etiology of injuries consisted of 96 cases of traumatic SCI and 12 cases of non-traumatic SCI. The most common etiology of traumatic SCI was found to be transport-related injuries (n=56, 51.9%), followed by falls (n=32, 29.6%). The etiology of non-traumatic SCI varied considerably, including tumors, infections, etc. Seventy-eight percent (n=84) of the participants reported moderate-to-high scores on the CD-RISC 10 (that is, score range 20–35), indicating that resilient qualities and behaviors were present to some extent. However, the average CD-RISC score of the participants was 27.06±6.87. Descriptive statistics for WHO-QoL were as follows: Physical domain (53.67±19.2, actual score range=15-94), psychological (53.88±23.70, actual score range=6-94), social relationships domain (48.73±25.00, actual score range=2-100), environment domain (58.97±20.90, actual score range=18-100) and community participation (CIQ-R) (16.21±5.44, actual score range=4-28.25).
Point-Biserial correlation analysis indicated a mild, however, significant negative correlation between marital status and resilience (r=-0.247, P=0.010). However, a significant positive correlation was found between time since injury and resilience (r=0.2, P=0.038) (Figure 1).
In addition, QoL and community integration among the participants were also found to be positively correlated with resilience (overall health; r=0.317, P=0.001, physical health; r=0.31, P=0.001, psychological; r=0.48, P=0.000, environment; r=0.184, P=0.057) and are presented through scatter plot in Figure 2.
Similarly, a non-significant strong positive association was found between resilience and QoL and social relationships (r=0.178, P=0.065). While resilience and other demographic factors (such as age, gender, family type, and family income) were not found to be significantly associated. Independent t-test and ANOVA were used to determine the significant difference in the resilience score and demographics/injury-related variables among the study participants. Demographic and injury-related variables, such as marital status and frequency of going out from home were found to be significant.
It was found that unmarried participants (28.39±5.70) were more resilient as compared to married individuals (25.39±8.35) (P=0.029). Similarly, those visiting daily outside their homes (28.12±6.59) and participating in community activities were more resilient compared to those who do not prefer to go out regularly (P=0.051). However, a non-significant association was found among the variables, such as gender, place of residence, geographical area, family type, employment after injury, education, religion, monthly family income, and type of floor (Table 1).
Univariate and multivariate linear regression analyses were performed to identify the demographic determinants that contribute to resilience. Gender, geographic area (rural/urban), marital status, and employment were found to be statistically significant factors affecting resilience in univariate analysis. Multivariate analyses were performed using these significant variables. In multivariate analysis, gender, marital status, and profession were found to be significant. Among these predictors, employment presented a higher beta value (β=0.684 P=0.026) signifying that employment (after injury) was the most significant demographic characteristic of resilience. QoL factors were not included in the linear regression as they did not satisfy the assumption of linear regression (Table 2).
Also, resilience was varying among different categories of age groups (Supplementary Table 1).
However, other demographic and injury-related variables did not significantly contribute to resilience (P>0.05). CDRISC and CIQ-R were found to vary statistically significantly among participants (P≤0.05). The highest mean CDRISC score was found to be 30.5±3.32 for patients in the age group of 51-60 years followed by a CDRIC score of 28.3±6.79 in the age group of 31-40 years. The lowest CDRISC score was 15±8.19 for elderly patients (>60 years). Furthermore, CIQ-R was found to be highest (17.48±5.64) for patients in the 31-40 age group whereas it was found to be lowest (10.97±3.70) for patients in the age group of 41-50 years.
4. Discussion
This study looked at the level of resilience among SCI individuals living in the community, as well as the relationship between resilience and demographic parameters/injury-related variables, QoL, and community participation. Currently, there is a paucity of published research in low-middle-income countries on resilience among the SCI population post-injury [8]. The participants in the present study were from different backgrounds and places and had been suffering from either traumatic or non-traumatic SCI. Furthermore, SCI is a condition that drastically disrupts a person's life and has a negative impact on physical, psychological, and social aspects, this results in poor participation in the community. Depending on the level and severity of the injury, individuals with SCI may experience complete or incomplete muscle paralysis and loss of sensation, leading to many secondary complications [4, 23]. Because the individuals in this study were exposed to these adversities, they were more likely to suffer from the detrimental effects of spinal cord damage. The findings of the present study are in continuation with the previously published studies and offer some intriguing facts with respect to SCI individuals' resilience, its association with their QoL, and their participation in the community. Physical, psychological, and environmental domains of QoL and level of community participation were significantly associated with resilience among the study participants. Employment was found to be the most significant determinant of resilience in the present study. Participants who were unemployed indicated poor mean resilience, which is consistent with earlier findings [24, 25, 26]. In a postal survey conducted in India with a sample size of 600, no individual had a job living in the community while the employment rate was 41% for those who were working in non-governmental organizations (NGO) or the centers run by armed forces [27].
The consequences of unemployment lead to poor QoL, low resilience status, decreased independence, depression, poor social integration, etc. [27]. When striving to work after SCI, there are facilitators to be explored (e.g. education, transportation, assistive technology) and barriers that need management (e.g. secondary medical complications). There were few studies that examined the association between resilience and employment status [8, 28]. Of the three, two studies found a significant positive correlation between resilience and employment [8, 26]. Employment is a significant variable, which helps an individual to become self-independent and not rely financially on others and also increases the sense of self-worth and satisfaction with life leading to improved resilience [26, 29].
The results of the study also revealed that married patients were less resilient in their lives compared to unmarried patients. Besides, findings interpret that the frequency of divorce was quite high among female patients compared to male sufferers. However, the majority of the participants in the present study were classified as married and were still living with their partners, and most of them were cared for by their partners or other family members. As all the patients studied were living in the community (at least one-year post-injury), the majority of them were not the earning members of their respective families due to their injury. As per the study findings, unmarried people were more resilient and content with their life, but married people were found more dissatisfied and disappointed because of the stress of not functioning normally in the household. The same has been reported in a study conducted on 276 SCI patients to test statistically the experience of fewer marriages and more divorces after the injury [30]. Furthermore, in the present study, the resilience score among the participants was found to be highest in the upper age groups (i.e. 51-60 years) and quite low in the younger and middle-aged cases (18-40 years), which were similar to the other findings [14]. These findings could be explained by managing a life-altering event, such as SCI the young and middle age groups when the individuals were not in a position to accept it, and people of these age groups are quite aggressive and enthusiastic towards their work and family [21]. In addition, secondary health conditions after the tragic events were more taxing. Thus, this could be one of the potential reasons for their poor resilience score. The lowest resilience score was reported amongst elderly participants due to various associated reasons, such as high levels of dependency, secondary health conditions (pain, spasticity), as well as social isolation [14].
5. Conclusion
The results indicated that physical health, psychological health, environmental factors, overall participation in the community as well as demographic variables (such as marital status and frequency of going out of their homes) were strongly associated with resilience. Furthermore, employment was found to be a highly significant determinant of resilience. According to the findings, it is important for healthcare professionals to screen sufferers with fewer resources, such as the unemployed, those from backward places, like rural areas, those emotionally weak cases, cases with poor participation in the community, etc. to provide better care and support through community-based or home-based or telerehabilitation programs, such as vocational rehabilitation support, which includes stress management, focus on independence, optimism, social support, communication and understanding, spousal involvement as well as awareness about the injury to help strengthen the resilience. This will help those who have been traumatized due to SCI and have a low level of resilience. Therefore, this will not only help enhance resilience among SCI people but will also aid in their effective reintegration into society.
Ethical Considerations
Compliance with ethical guidelines
The study got clearance from the Institutional Ethics Committee of the Indian Spinal Injuries Center (Vasant Kunj Reference No.: ISIC/RP/2020/15).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, writing–review & editing: Meenakshi Mohan and Roumi Deb; Methodology, investigation, writing–original draft, data collection and data analysis: Meenakshi Mohan.
Conflict of interest
We certified that there is no actual or potential conflict of interest in relation to this research work.
Acknowledgments
All authors declared no conflict of interest.
References
- Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bulletin of the World Health Organization. 2003; 81(9):646-56. [Link]
- Singh G, Prakash R, Bhatti V, Mahen A. Spinal cord injury in organizational setup: A hospital based descriptive study. Journal of Marine Medical Society. 2019; 21(1):46. [DOI:10.4103/jmms.jmms_67_18]
- Duggan C, Wilson C, DiPonio L, Trumpower B, Meade MA. Resilience and happiness after spinal cord injury: A qualitative study. Topics in Spinal Cord Injury Rehabilitation. 2016; 22(2):99-110. [DOI:10.1310/sci2202-99] [PMID] [PMCID]
- Bhattarai M, Maneewat K, Sae-Sia W. Determinants of resilience among people who sustained spinal cord injury from the 2015 earthquake in Nepal. Spinal Cord. 2018; 56(1):78-83. [DOI:10.1038/sc.2017.93] [PMID]
- Guest R, Craig A, Tran Y, Middleton J. Factors predicting resilience in people with spinal cord injury during transition from inpatient rehabilitation to the community. Spinal Cord. 2015; 53(9):682-6. [DOI:10.1038/sc.2015.32] [PMID]
- Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depression and Anxiety. 2003; 18(2):76-82.[DOI:10.1002/da.10113] [PMID]
- Kornhaber R, Mclean L, Betihavas V, Cleary M. Resilience and the rehabilitation of adult spinal cord injury survivors: A qualitative systematic review.Journal of Advanced Nursing. 2018; 74(1):23-33. [DOI:10.1111/jan.13396] [PMID]
- Bhattarai M, Maneewat K, Sae-Sia W. Psychosocial factors affecting resilience in Nepalese individuals with earthquake-related spinal cord injury: A cross-sectional study. BMC Psychiatry. 2018; 18(1):1-8. [DOI:10.1186/s12888-018-1640-z] [PMID] [PMCID]
- Kilic SA, Dorstyn DS, Guiver NG. Examining factors that contribute to the process of resilience following spinal cord injury. Spinal Cord. 2013; 51(7):553-7. [DOI:10.1038/sc.2013.25] [PMID]
- Driver S, Warren AM, Reynolds M, Agtarap S, Hamilton R, Trost Z, et al. Identifying predictors of resilience at inpatient and 3-month post-spinal cord injury. The Journal of Spinal Cord Medicine. 2016; 39(1):77-84. [DOI:10.1179/2045772314Y.0000000270] [PMID] [PMCID]
- Ahmed N, Quadir MM, Rahman MA, Alamgir H. Community integration and life satisfaction among individuals with spinal cord injury living in the community after receiving institutional care in Bangladesh. Disability and rehabilitation. 2018; 40(9):1033-40. [DOI:10.1080/09638288.2017.1283713] [PMID]
- Nagle Y, Kalpana Rani E, Masood A, Jrf M. Validation of connor-davidson resilience scale on indian military soldiers. Europe's Journal of Psychology. 2021; 8(1):2021. [Link]
- Rehman U, Shahnawaz M. Factorial validation of Connor Davidson Resilience scale on Indian sample. Delhi Psychiatry Journal. 2019; 22(1):99-103. [Link]
- Terrill AL, Molton IR, Ehde DM, Amtmann D, Bombardier CH, Smith AE, et al. Resilience, age, and perceived symptoms in persons with long-term physical disabilities. Journal of Health Psychology. 2016; 21(5):640-9. [DOI:10.1177/1359105314532973] [PMID]
- World Health Organization. Introduction, administration, scoring and generic version of the assessment: Field trial version December 1996. Geneva: World Health Organization; 1996. [Link]
- Whoqol Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine. 1998; 28(3):551-8. [DOI:10.1017/S0033291798006667] [PMID]
- Shin JC, Goo HR, Yu SJ, Kim DH, Yoon SY. Depression and quality of life in patients within the first 6 months after the spinal cord injury. Annals of Rehabilitation Medicine. 2012; 36(1):119-25. [DOI:10.5535/arm.2012.36.1.119] [PMID] [PMCID]
- Leung KF, Wong WW, Tay MSM, Chu MML, Ng SSW. Development and validation of the interview version of the Hong Kong Chinese WHOQOL-BREF. Quality of Life Research. 2005; 14(5):1413-9. [DOI:10.1007/s11136-004-4772-1] [PMID]
- Ioncoli M, Berardi A, Tofani M, Panuccio F, Servadio A, Valente D, et al. crosscultural validation of the community integration questionnaire–revised in an Italian population. Occupational Therapy International. 2020; 2020.[DOI:10.1155/2020/8916541] [PMID] [PMCID]
- Callaway L, Winkler D, Tippett A, Herd N, Migliorini C, Willer B. The Community Integration Questionnaire - Revised: Australian normative data and measurement of electronic social networking. Australian Occupational Therapy Journal. 2016; 63(3):143-53. [DOI:10.1111/1440-1630.12284] [PMID]
- Callaway L, Enticott J, Farnworth L, McDonald R, Migliorini C, Willer B. Community integration outcomes of people with spinal cord injury and multiple matched controls: A pilot study. Australian Occupational Therapy Journal. 2017; 64(3):226-34. [DOI:10.1111/1440-1630.12350] [PMID]
- Gontkovsky ST, Russum P, Stokic DS. Comparison of the CIQ and chart short form in assessing community integration in individuals with chronic spinal cord injury: A pilot study. NeuroRehabilitation. 2009; 24(2):185-92. [DOI:10.3233/NRE-2009-0467] [PMID]
- Craig A, Perry KN, Guest R, Tran Y, Dezarnaulds A, Hales A, et al. Prospective study of the occurrence of psychological disorders and comorbidities after spinal cord injury. Archives of Physical Medicine and Rehabilitation. 2015; 96(8):1426-34. [DOI:10.1016/j.apmr.2015.02.027] [PMID]
- O’Neill J, Dyson-Hudson TA. Employment after spinal cord injury. Current Physical Medicine and Rehabilitation Reports. 2020; 8(3):141-8. [DOI:10.1007/s40141-020-00266-4]
- Kukihara H, Yamawaki N, Uchiyama K, Arai S, Horikawa E. Trauma, depression, and resilience of earthquake/tsunami/nuclear disaster survivors of Hirono, Fukushima, Japan. Psychiatry and Clinical Neurosciences. 2014; 68(7):524-33. [DOI:10.1111/pcn.12159] [PMID]
- Min JA, Lee CU, Hwang SI, Shin JI, Lee BS, Han SH, et al. The moderation of resilience on the negative effect of pain on depression and post-traumatic growth in individuals with spinal cord injury. Disability and Rehabilitation. 2014; 36(14):1196-202. [DOI:10.3109/09638288.2013.834985] [PMID]
- Gupta N, Solomon J, Raja K. Employment after paraplegia in India: A postal survey. Spinal Cord. 2011; 49(7):806-11. [DOI:10.1038/sc.2011.1] [PMID]
- Hossain MS, Rahman MA, Bowden JL, Quadir MM, Herbert RD, Harvey LA. Psychological and socioeconomic status, complications and quality of life in people with spinal cord injuries after discharge from hospital in Bangladesh: A cohort study. Spinal Cord. 2016; 54(6):483-9. [DOI:10.1038/sc.2015.179] [PMID]
- Peter C, Müller R, Cieza A, Geyh S. Psychological resources in spinal cord injury: A systematic literature review. Spinal Cord. 2012; 50(3):188-201.[DOI:10.1038/sc.2011.125] [PMID]
- DeVivo MJ, Fine PR. Spinal cord injury: Its short-term impact on marital status. Archives of Physical Medicine and Rehabilitation. 1985; 66(8):501-4. [Link]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2022/05/25 | Accepted: 2022/11/28 | Published: 2023/03/1
Received: 2022/05/25 | Accepted: 2022/11/28 | Published: 2023/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
