
988368
Thu, Jul 30, 2026

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 695-702 |
Back to browse issues page


Ethics code: DYPCPT/574-B(28)/2021)
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Deshmukh M, Pokle S, Baxi G, Palekar T, Gopiyani I. The Effect of Quadratus Lumborum Muscle Energy Technique on Low Back Pain and Diaphragmatic Electrophysiological Outcomes. Iranian Rehabilitation Journal 2023; 21 (4) :695-702
URL: http://irj.uswr.ac.ir/article-1-1699-en.html
URL: http://irj.uswr.ac.ir/article-1-1699-en.html



1- Dr DY Patil College of Physiotherapy, Dr DY Patil Vidyapeeth Pune, Pimpri, India.
Keywords: Diaphragm, Electromyography, Low back pain, Muscle energy technique (MET) of quadratus lumborum (QL)
Full-Text [PDF 1252 kb]
(4629 Downloads)
| Abstract (HTML) (6333 Views)
Full-Text: (1815 Views)
Introduction
Pain is defined as an unpleasant sensory and emotional experience with or without actual tissue damage. Low back pain localizes from the 12th rib and the inferior gluteal folds, with or without radiation to the legs [1].
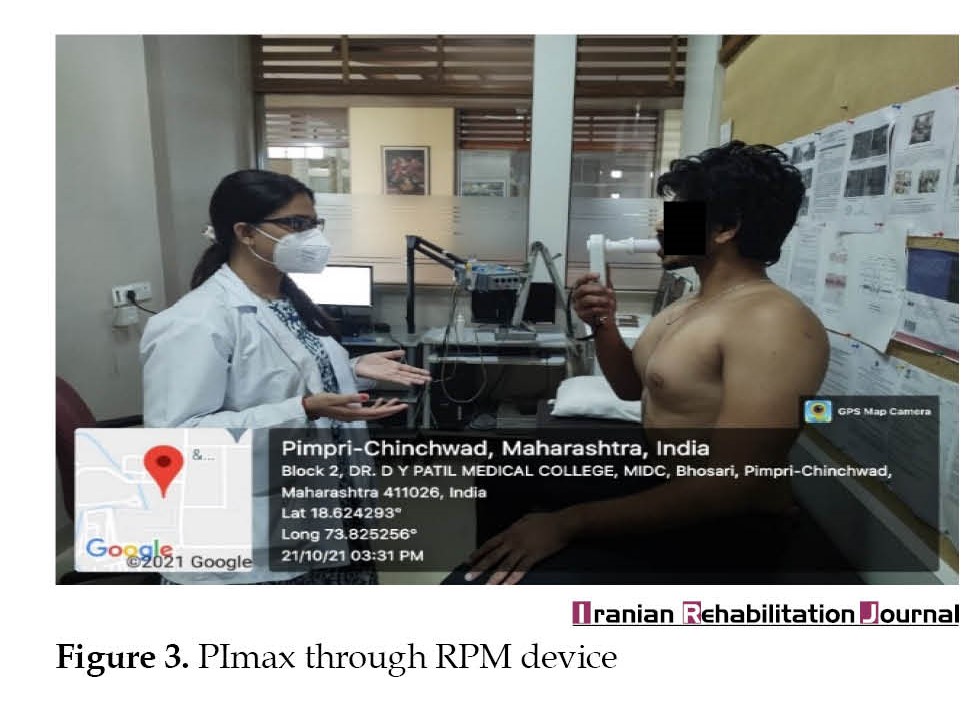
As shown in Figure 1, 2, and 3, the quadratus lumborum (QL) muscle is the deepest muscle situated in the posterior aspect of the abdominal wall, dorsal to the ilopsoas, and is often mistakenly referred to as the back muscle [2, 3].


 Its shape is irregular but quadrangular, hence called ‘QL’. QL is a neglected yet vital muscle that is usually overpowered by the psoas major. It is a hardworking core stabilizer and has a strong influence on respiration and even digestion. QL is included in the list of accessory muscles of expiration due to its insertion to the 12th rib along with fibers of the diaphragm [3]. Barr, Griggs, and Cadby proved that the superior attachments of muscles are the serratus posterior and inferior, which also are attached to the ribs [4]. These muscles contact in combination with QL to depress the ribs. Since rib depression is a feature of expiration, QL assists in expiration, it also stabilizes the diaphragm for functions that require eccentric diaphragmatic actions, such as singing, speaking, etc [3]. Hence, any abnormality in QL can affect the normal breathing pattern [4, 5]. Muscle energy technique (MET) is a manual technique that has a significant effect on muscle functions and has a sustained effect [4, 6]. QL is selected in the present study due to its significant contribution to core stabilization and breathing. Hence, a quasi-experimental study was designed and conducted to prove our hypothesis on whether MET of QL affects pain and lung function in patients with low back pain. Though breathing is the most vital and affected function in any musculoskeletal condition, it is always overlooked in the treatment, if the effect of MET on QL is proven, it will be a new innovative method in the management of low back pain and breathing dysfunction.
Its shape is irregular but quadrangular, hence called ‘QL’. QL is a neglected yet vital muscle that is usually overpowered by the psoas major. It is a hardworking core stabilizer and has a strong influence on respiration and even digestion. QL is included in the list of accessory muscles of expiration due to its insertion to the 12th rib along with fibers of the diaphragm [3]. Barr, Griggs, and Cadby proved that the superior attachments of muscles are the serratus posterior and inferior, which also are attached to the ribs [4]. These muscles contact in combination with QL to depress the ribs. Since rib depression is a feature of expiration, QL assists in expiration, it also stabilizes the diaphragm for functions that require eccentric diaphragmatic actions, such as singing, speaking, etc [3]. Hence, any abnormality in QL can affect the normal breathing pattern [4, 5]. Muscle energy technique (MET) is a manual technique that has a significant effect on muscle functions and has a sustained effect [4, 6]. QL is selected in the present study due to its significant contribution to core stabilization and breathing. Hence, a quasi-experimental study was designed and conducted to prove our hypothesis on whether MET of QL affects pain and lung function in patients with low back pain. Though breathing is the most vital and affected function in any musculoskeletal condition, it is always overlooked in the treatment, if the effect of MET on QL is proven, it will be a new innovative method in the management of low back pain and breathing dysfunction.
Materials and Methods
This study was conducted using a quasi-experimental study from June 2021 to January 2022. The sample size was calculated 65 individuals by considering the 95% CI using Winpepi software, version 11.65. The inclusion criteria included individuals between the age group of 21 to 45 years with low back pain and individuals with non-specific low back pain without any radiculopathy and other diagnosed conditions. The exclusion criteria included individuals with any other musculoskeletal or neurological involvements. Ethical consideration and COVID-19 precautions were considered and every participant was provided with a separate mouthpiece. Self-evaluation of breathing questionnaire (SEBQ) with high test re-test reproducibility was given to the individuals and were asked to tick the questions and score [7, 8]. Based on scoring, the individuals with or without breathing pattern abnormalities were considered and were divided into two groups. Group A and group B included participants with SEBQ scoreless and >11, respectively [7, 8, 9]. Pre and post-intervention assessment of outcome measures was done by assessing the numerical pain rating scale (NPRS), surface electromyography (EMG) of the diaphragm using a new wave EMG machine, and maximum inspiratory pressure (PIMAX) using respiratory pressure manometer (RPM) with high test re-test reliability of both types of the equipment [10, 11, 12]. The intervention included post-isometric relaxation of QL for 30 s on both sides [13].
MET was performed on QL, followed by readings of pain, and diaphragm activity via surface EMG and maximum inspiratory pressure and chest expansion. The patient was made to lie down in a side-lying position. The therapist stood behind the patient’s waist. The patient was asked to extend his arm over the head level to attempt to hold the upper part of the plinth. The patient was asked to inhale and simultaneously abduct the leg facing the ceiling till the strongly contracting quadratus muscle activity was palpated by the therapist. The individual held the leg against gravity for 10 s and then took his leg behind and let it hang at the back of the plinth. Then the therapist held the crest of the pelvis posteriorly from behind. The patient was asked to exhale and simultaneously the therapist pulled the pelvis away from the lower ribs. The pull was maintained for 10-30 s and the position was released [14, 15].
Statistical analysis
The results were analyzed using Medcalc software, version 22.017. Normal distribution of data was checked using the Shapiro-Wilk test and appropriate tests were used based on the acceptance and rejection of normality. A paired t-test was used to check the significance in the case of normal data distribution. Wilcoxon’s rank sum test was used if the data was not distributed normally.
Results
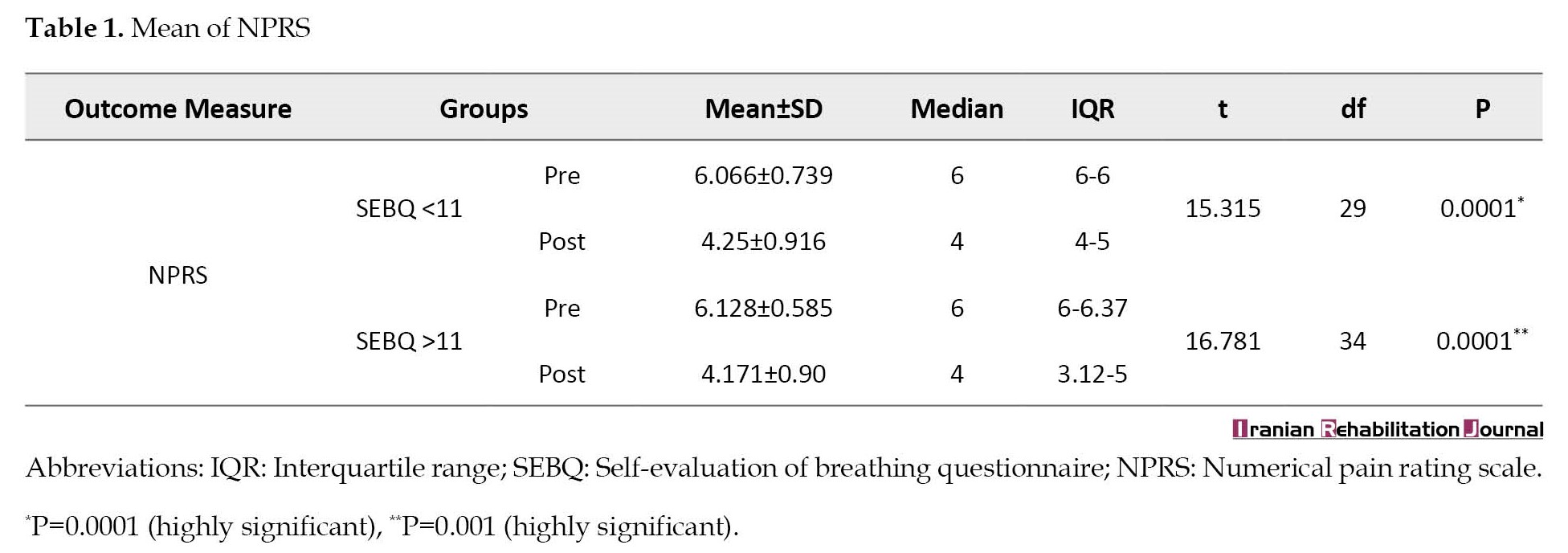
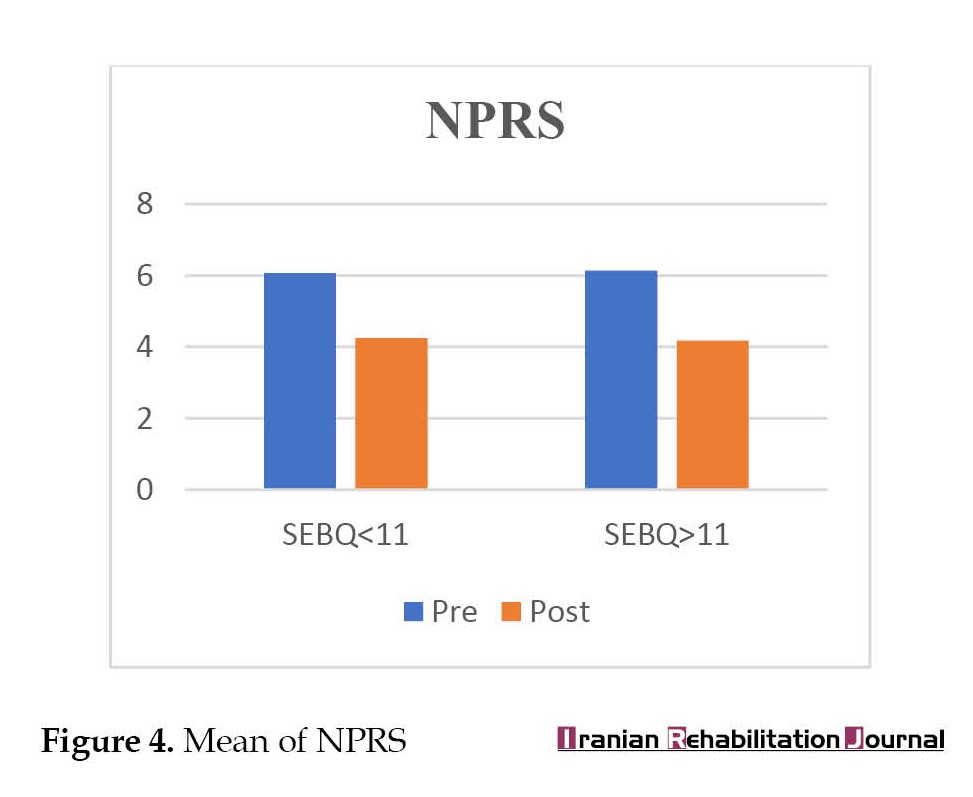
This study showed a significant difference in pain in both groups (P=0.0001) (Table 1, Figure 4).
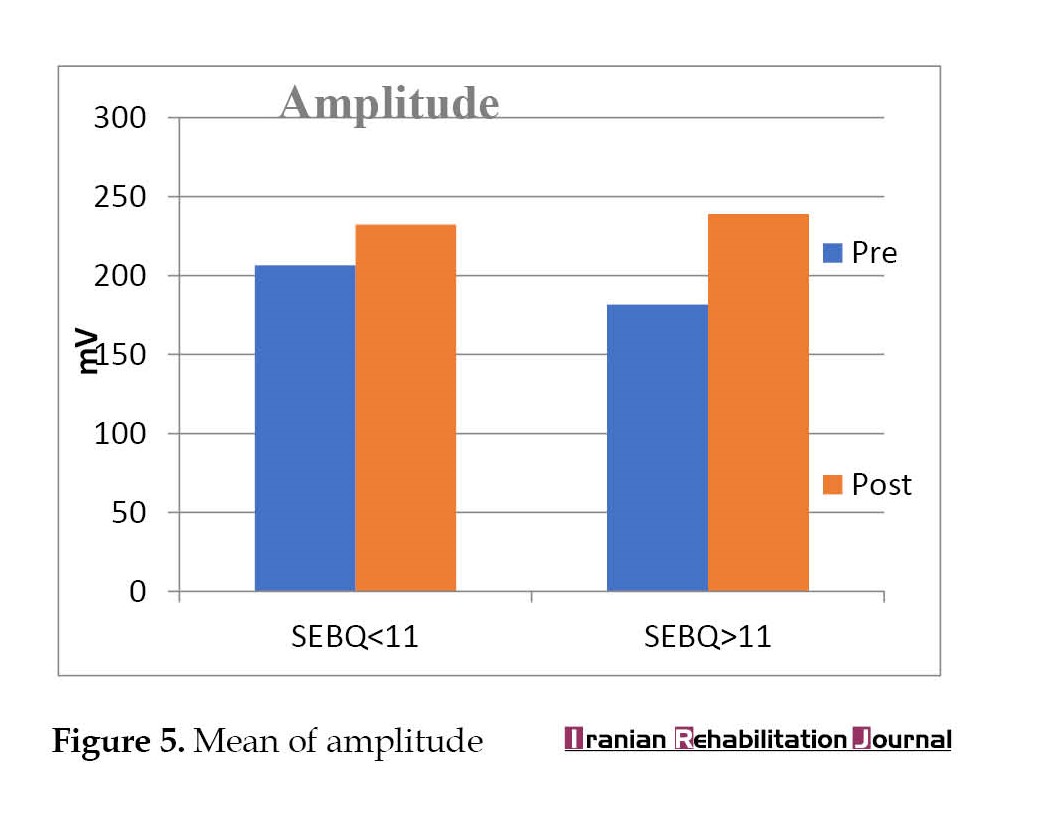
 A statistical significance was observed in the amplitude of motor unit potentials in group B with SEBQ score >11 (P=0.0005) while in group A, the P was not significant (P=0.1505) (Table 2, Figure 5).
A statistical significance was observed in the amplitude of motor unit potentials in group B with SEBQ score >11 (P=0.0005) while in group A, the P was not significant (P=0.1505) (Table 2, Figure 5).
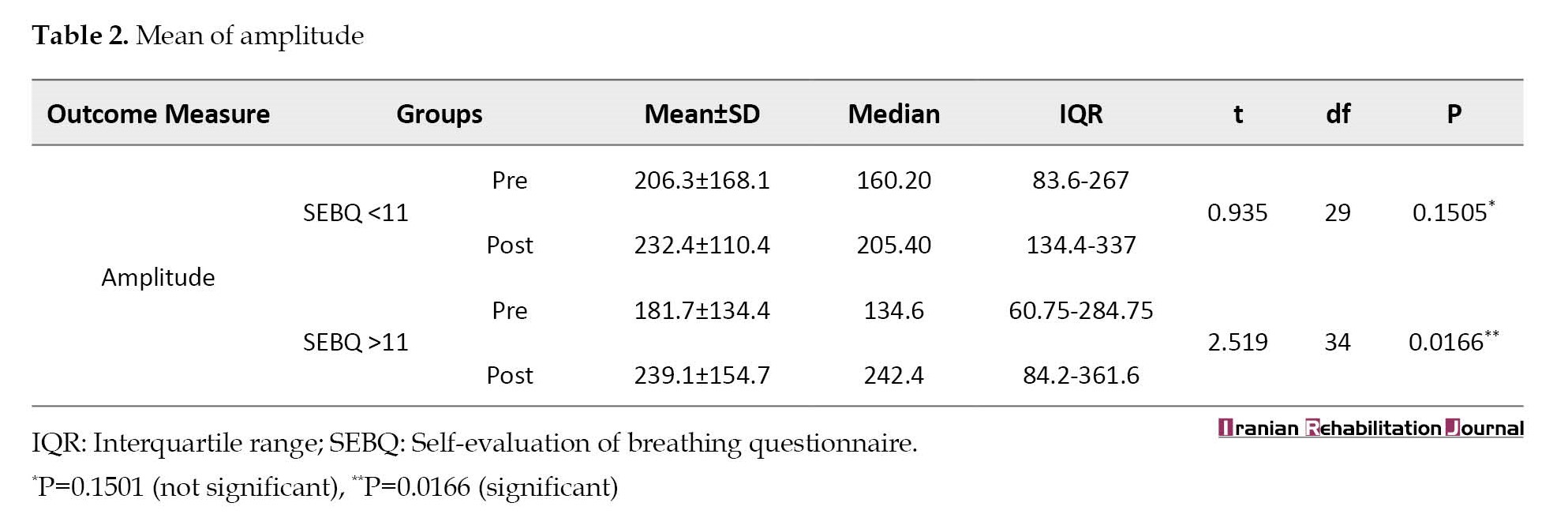
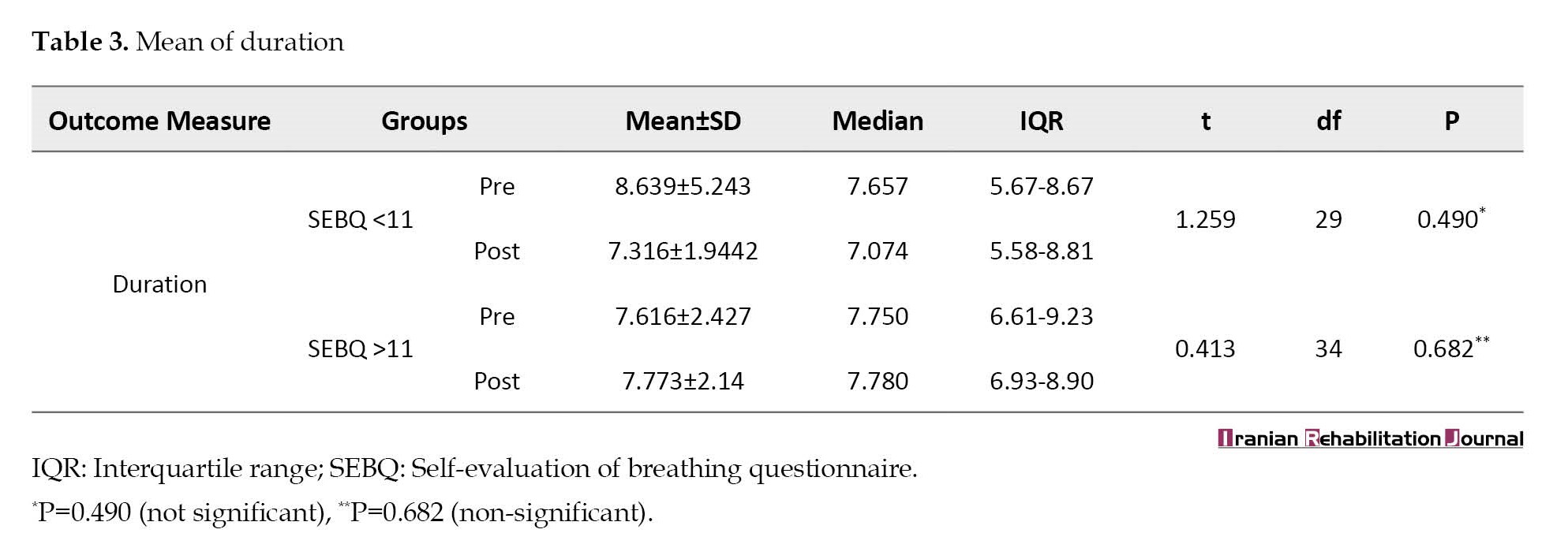
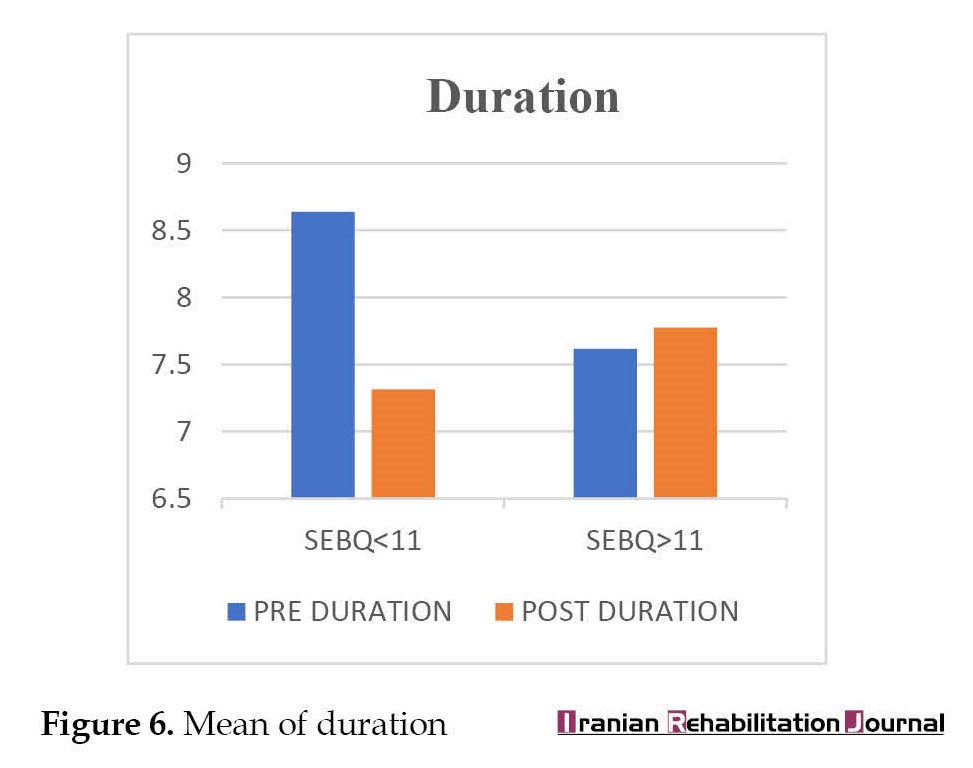
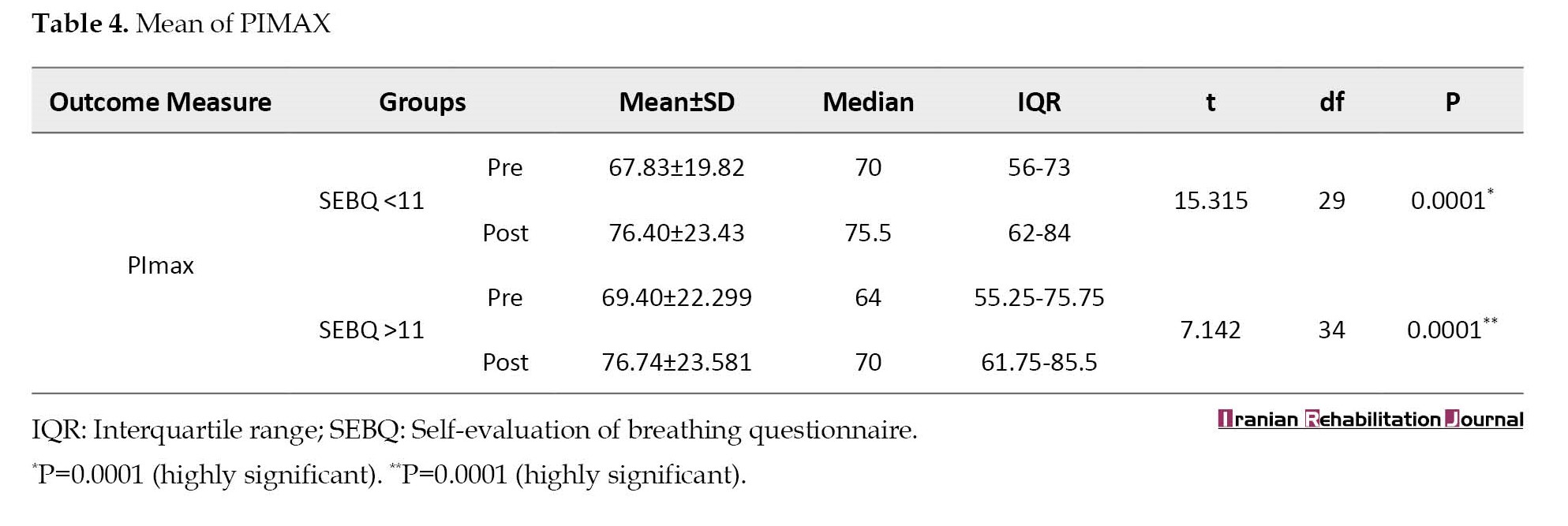
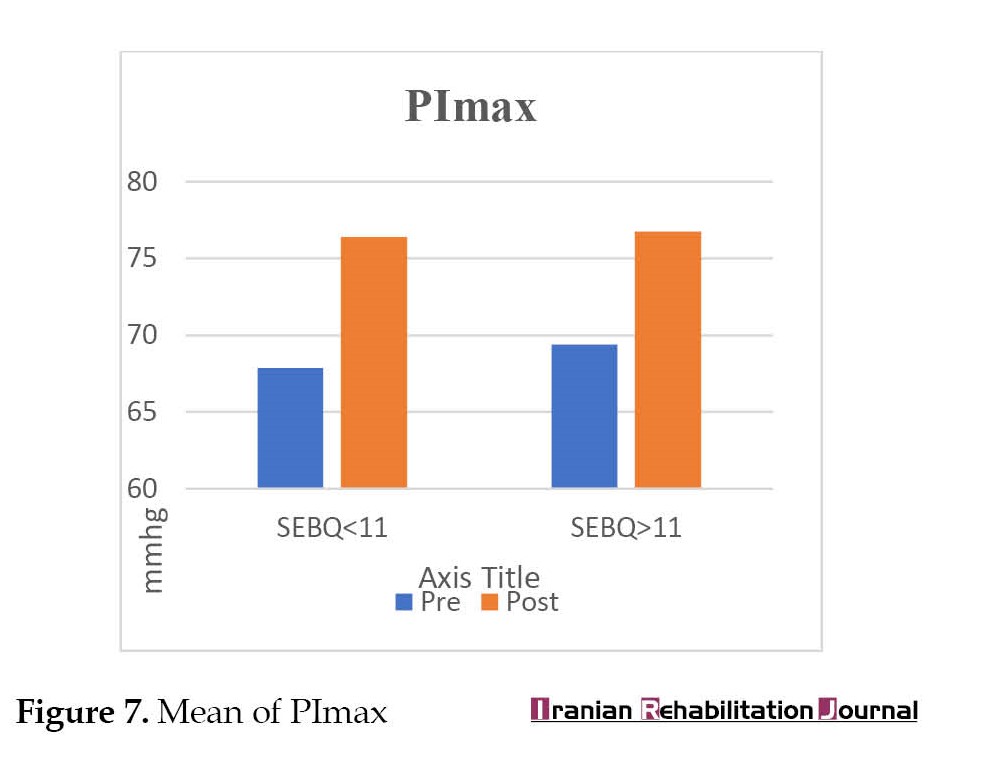
 A statistical insignificance was observed in duration in both groups (P=0.4908) and (P=0.682). (Table 3, Figure 6) and a highly significant result was observed in Pimax in both groups (P=0.0001), respectively (Table 4, Figure 7).
A statistical insignificance was observed in duration in both groups (P=0.4908) and (P=0.682). (Table 3, Figure 6) and a highly significant result was observed in Pimax in both groups (P=0.0001), respectively (Table 4, Figure 7).
Discussion
This study was conducted to assess the effect of MET of QL on pain and diaphragm activity in individuals with non-specific low back pain.
It was found that the pain was significantly reduced in both groups with P=0.0001 in both groups with 29 and 34 degrees of freedom (df), respectively. The Mean±SD were 1.817±0.6497 and 1.957±0.69, respectively. The amplitude was significantly increased in the group with SEBQ >11 with P<0.0005 with 29 df and Mean±SD of -57.43±2.241. PImax increased strongly in both groups with P<0.0001 with 29 and 34 df. This showed that the application of MET affected parameters, such as pain, surface electromyography, and PImax.
A study presented that breathing pattern disorders (BPD) and musculoskeletal pain showed a correlation between BPD and musculoskeletal pain. The study results showed that musculoskeletal pain can lead to BPD and osteopathic manual therapy techniques can be used and were beneficial for a person suffering from BPD [14, 16].
The above study is supported by the study conducted by Deshmukh et al., [16] in which they included the use of SEBQ and Nijmegen questionnaire to evaluate the breathing dysfunction in patients with musculoskeletal pain and concluded the presence of breathing dysfunction with musculoskeletal complaints. The BPD may be due to the imbalance between the parasympathetic and sympathetic nervous systems leading to the causation of pain due to the activation of the flight and fright mechanism [16]. Another reason is the pain and biomechanical factors. Low back pain leads to tightening of structures, especially QL, which is the deepest muscle, and may lead to altered biomechanics of the back and thorax because the descent of the diaphragm and the 12th rib is reduced and limited due to tightness of QL. This may lead to faulty breathing habits, and if left untreated, may cause a vicious cycle of adaptive breathing pattern disorder with persistent low back pain [14, 15].
Our study is consistent with a study conducted by Tawrej, Kaur, and Ghodey, which concluded that a subsequent reduction in agonist muscle tone was observed [17]. Due to the stretch of the Golgi tendon organs, a reduction in pain and an increase in lumbar mobility was observed with the application of a hot pack. Table 1 and Figure 1 show that both groups A and B with SEBQ <11 and SEBQ >11 have P=0.0001, respectively. It was statistically significant and after the application of MET of QL, the pain was reduced in both groups. The possible reason for pain reduction can be the subsequent reduction in agonist muscle tone due to post-isometric relaxation. As per the study mentioned above, the stretch of Golgi tendon organs may lead to pain reduction in the present study as well [18].
This study is supported by another study conducted by Rishi and Arora, which concluded that an improvement in pain and functional disability was observed in both groups, which received MET and MET with a supervised exercise program. It concluded that stimulation of the Golgi tendon organ in the tendon of a muscle inhibits the muscle fibres. It occurs when the application of MET stretches the shortened structures or muscles and strengthens the weakened ones. The isometric contraction of an agonist inhibits the antagonist and promotes its relaxation [17, 19].
A study proposed by Espinosa-López et al. [13] proved that the application of MET on QL muscle improved its performance and increased respiratory muscle strength. Along with the increased range and mobility of the muscle, PImax and maximum expiratory pressure (PEmax) increased from 41% to 69% and 33% to 57%, respectively, which further improved the efficacy of its role in ventilation and impacted the segmental and intersegmental restriction and led to increased expansion of thorax [13, 20, 21].
Table 4 and Figure 4 show that in both groups with SEBQ <11 and SEBQ >11, the P<0.0001 with 29 and 34 df, respectively which showed a significant increase in the values of PImax and proved its statistical significance.
Another study conducted by Uysal et al. applied MET to scalene, upper trapezius, and sternocleidomastoid after a superficial heat application and concluded that the application of MET to the accessory muscles of respiration increased the respiratory muscle strength and endurance, improved flexibility, and reduced pain and disability in patients with fibromyalgia. It stated that the application of MET improved tolerance against stretching and reduced the sensation of pain because it stimulated the muscle and joint receptors. The reduction of pain in the present study can also be due to the improved tolerance to stretching and stimulation of muscle and joint receptors [14].
According to the results of Vaseghnia, a significant reduction was observed in pain and disability on the visual analog scale after applying MET in cases of sacroiliac joint dysfunction in daily activities and lumbar stiffness in women [15].
A study conducted by Gutiérrez et al. on breathing dysfunction investigated the electromyographic activities of the primary and accessory muscles of respiration, such as the diaphragm, external intercostals, scalene, latissimus dorsi, sternocleidomastoid with different types of breathing, such as normal quiet breathing, maximal voluntary clenching in intercuspal position and proved that different or altered breathing type had an effect or significant change in the electromyographic activities of respiratory muscles, especially in the diaphragm [11, 18]. This result supports our present study with reduced amplitude and increased duration in patients with SEBQ scores of more than 11 before treatment and improvement was observed after the intervention [12, 18]. From the above-mentioned studies and the present study, it has been proven that due to the presence of persistent low back pain, breathing dysfunction may develop, leading to adaptive faulty breathing patterns. After the application of MET to QL, pain reduction, improvement in amplitudes, and duration of surface electromyography of diaphragm and PImax were observed. From Table 1, Table 2, Table 3, Table 4, and Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, it can be correlated that due to the application of MET, a pain reduction was observed, which further led to increased PImax values. Along with back pain treatment, breathing dysfunction should be emphasized and intervention should also be provided. This can be the new perspective of treating not only back pain but also breathing dysfunction in the rehabilitation process.
Conclusion
From the above study, we conclude that an effect of MET of QL on pain and electrophysiological activity of the diaphragm is observed in individuals with non-specific low back pain.
Study limitations
This study was limited to the effect of MET to QL
Future scope of the study
Further research can be done on the MET to different muscles and pulmonary characteristics in distinct populations.
Ethical Considerations
Compliance with ethical guidelines
The Ethical Approval was obtained from the Institutional Ethics Committee of Dr. D. Y. Patil Vidyapeeth Pune (Code: CTRI/2021/09/036591). Informed consent was obtained from all the study participants (Ref No.: DYPCPT/574-B(28)/2021).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and manuscript preparation: Mayura Deshmukh; Investigations: Siddhi Pokle; Data collection: Siddhi Pokle and Ishani Gopiyani; Data analysis: Mayura Deshmukh and Gaurang Baxi; Review and finalizing manuscript: Gaurang Baxi and Tushar Palekar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the participants who participated in the study.
References
Pain is defined as an unpleasant sensory and emotional experience with or without actual tissue damage. Low back pain localizes from the 12th rib and the inferior gluteal folds, with or without radiation to the legs [1].
As shown in Figure 1, 2, and 3, the quadratus lumborum (QL) muscle is the deepest muscle situated in the posterior aspect of the abdominal wall, dorsal to the ilopsoas, and is often mistakenly referred to as the back muscle [2, 3].
Materials and Methods
This study was conducted using a quasi-experimental study from June 2021 to January 2022. The sample size was calculated 65 individuals by considering the 95% CI using Winpepi software, version 11.65. The inclusion criteria included individuals between the age group of 21 to 45 years with low back pain and individuals with non-specific low back pain without any radiculopathy and other diagnosed conditions. The exclusion criteria included individuals with any other musculoskeletal or neurological involvements. Ethical consideration and COVID-19 precautions were considered and every participant was provided with a separate mouthpiece. Self-evaluation of breathing questionnaire (SEBQ) with high test re-test reproducibility was given to the individuals and were asked to tick the questions and score [7, 8]. Based on scoring, the individuals with or without breathing pattern abnormalities were considered and were divided into two groups. Group A and group B included participants with SEBQ scoreless and >11, respectively [7, 8, 9]. Pre and post-intervention assessment of outcome measures was done by assessing the numerical pain rating scale (NPRS), surface electromyography (EMG) of the diaphragm using a new wave EMG machine, and maximum inspiratory pressure (PIMAX) using respiratory pressure manometer (RPM) with high test re-test reliability of both types of the equipment [10, 11, 12]. The intervention included post-isometric relaxation of QL for 30 s on both sides [13].
MET was performed on QL, followed by readings of pain, and diaphragm activity via surface EMG and maximum inspiratory pressure and chest expansion. The patient was made to lie down in a side-lying position. The therapist stood behind the patient’s waist. The patient was asked to extend his arm over the head level to attempt to hold the upper part of the plinth. The patient was asked to inhale and simultaneously abduct the leg facing the ceiling till the strongly contracting quadratus muscle activity was palpated by the therapist. The individual held the leg against gravity for 10 s and then took his leg behind and let it hang at the back of the plinth. Then the therapist held the crest of the pelvis posteriorly from behind. The patient was asked to exhale and simultaneously the therapist pulled the pelvis away from the lower ribs. The pull was maintained for 10-30 s and the position was released [14, 15].
Statistical analysis
The results were analyzed using Medcalc software, version 22.017. Normal distribution of data was checked using the Shapiro-Wilk test and appropriate tests were used based on the acceptance and rejection of normality. A paired t-test was used to check the significance in the case of normal data distribution. Wilcoxon’s rank sum test was used if the data was not distributed normally.
Results
This study showed a significant difference in pain in both groups (P=0.0001) (Table 1, Figure 4).
Discussion
This study was conducted to assess the effect of MET of QL on pain and diaphragm activity in individuals with non-specific low back pain.
It was found that the pain was significantly reduced in both groups with P=0.0001 in both groups with 29 and 34 degrees of freedom (df), respectively. The Mean±SD were 1.817±0.6497 and 1.957±0.69, respectively. The amplitude was significantly increased in the group with SEBQ >11 with P<0.0005 with 29 df and Mean±SD of -57.43±2.241. PImax increased strongly in both groups with P<0.0001 with 29 and 34 df. This showed that the application of MET affected parameters, such as pain, surface electromyography, and PImax.
A study presented that breathing pattern disorders (BPD) and musculoskeletal pain showed a correlation between BPD and musculoskeletal pain. The study results showed that musculoskeletal pain can lead to BPD and osteopathic manual therapy techniques can be used and were beneficial for a person suffering from BPD [14, 16].
The above study is supported by the study conducted by Deshmukh et al., [16] in which they included the use of SEBQ and Nijmegen questionnaire to evaluate the breathing dysfunction in patients with musculoskeletal pain and concluded the presence of breathing dysfunction with musculoskeletal complaints. The BPD may be due to the imbalance between the parasympathetic and sympathetic nervous systems leading to the causation of pain due to the activation of the flight and fright mechanism [16]. Another reason is the pain and biomechanical factors. Low back pain leads to tightening of structures, especially QL, which is the deepest muscle, and may lead to altered biomechanics of the back and thorax because the descent of the diaphragm and the 12th rib is reduced and limited due to tightness of QL. This may lead to faulty breathing habits, and if left untreated, may cause a vicious cycle of adaptive breathing pattern disorder with persistent low back pain [14, 15].
Our study is consistent with a study conducted by Tawrej, Kaur, and Ghodey, which concluded that a subsequent reduction in agonist muscle tone was observed [17]. Due to the stretch of the Golgi tendon organs, a reduction in pain and an increase in lumbar mobility was observed with the application of a hot pack. Table 1 and Figure 1 show that both groups A and B with SEBQ <11 and SEBQ >11 have P=0.0001, respectively. It was statistically significant and after the application of MET of QL, the pain was reduced in both groups. The possible reason for pain reduction can be the subsequent reduction in agonist muscle tone due to post-isometric relaxation. As per the study mentioned above, the stretch of Golgi tendon organs may lead to pain reduction in the present study as well [18].
This study is supported by another study conducted by Rishi and Arora, which concluded that an improvement in pain and functional disability was observed in both groups, which received MET and MET with a supervised exercise program. It concluded that stimulation of the Golgi tendon organ in the tendon of a muscle inhibits the muscle fibres. It occurs when the application of MET stretches the shortened structures or muscles and strengthens the weakened ones. The isometric contraction of an agonist inhibits the antagonist and promotes its relaxation [17, 19].
A study proposed by Espinosa-López et al. [13] proved that the application of MET on QL muscle improved its performance and increased respiratory muscle strength. Along with the increased range and mobility of the muscle, PImax and maximum expiratory pressure (PEmax) increased from 41% to 69% and 33% to 57%, respectively, which further improved the efficacy of its role in ventilation and impacted the segmental and intersegmental restriction and led to increased expansion of thorax [13, 20, 21].
Table 4 and Figure 4 show that in both groups with SEBQ <11 and SEBQ >11, the P<0.0001 with 29 and 34 df, respectively which showed a significant increase in the values of PImax and proved its statistical significance.
Another study conducted by Uysal et al. applied MET to scalene, upper trapezius, and sternocleidomastoid after a superficial heat application and concluded that the application of MET to the accessory muscles of respiration increased the respiratory muscle strength and endurance, improved flexibility, and reduced pain and disability in patients with fibromyalgia. It stated that the application of MET improved tolerance against stretching and reduced the sensation of pain because it stimulated the muscle and joint receptors. The reduction of pain in the present study can also be due to the improved tolerance to stretching and stimulation of muscle and joint receptors [14].
According to the results of Vaseghnia, a significant reduction was observed in pain and disability on the visual analog scale after applying MET in cases of sacroiliac joint dysfunction in daily activities and lumbar stiffness in women [15].
A study conducted by Gutiérrez et al. on breathing dysfunction investigated the electromyographic activities of the primary and accessory muscles of respiration, such as the diaphragm, external intercostals, scalene, latissimus dorsi, sternocleidomastoid with different types of breathing, such as normal quiet breathing, maximal voluntary clenching in intercuspal position and proved that different or altered breathing type had an effect or significant change in the electromyographic activities of respiratory muscles, especially in the diaphragm [11, 18]. This result supports our present study with reduced amplitude and increased duration in patients with SEBQ scores of more than 11 before treatment and improvement was observed after the intervention [12, 18]. From the above-mentioned studies and the present study, it has been proven that due to the presence of persistent low back pain, breathing dysfunction may develop, leading to adaptive faulty breathing patterns. After the application of MET to QL, pain reduction, improvement in amplitudes, and duration of surface electromyography of diaphragm and PImax were observed. From Table 1, Table 2, Table 3, Table 4, and Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, it can be correlated that due to the application of MET, a pain reduction was observed, which further led to increased PImax values. Along with back pain treatment, breathing dysfunction should be emphasized and intervention should also be provided. This can be the new perspective of treating not only back pain but also breathing dysfunction in the rehabilitation process.
Conclusion
From the above study, we conclude that an effect of MET of QL on pain and electrophysiological activity of the diaphragm is observed in individuals with non-specific low back pain.
Study limitations
This study was limited to the effect of MET to QL
Future scope of the study
Further research can be done on the MET to different muscles and pulmonary characteristics in distinct populations.
Ethical Considerations
Compliance with ethical guidelines
The Ethical Approval was obtained from the Institutional Ethics Committee of Dr. D. Y. Patil Vidyapeeth Pune (Code: CTRI/2021/09/036591). Informed consent was obtained from all the study participants (Ref No.: DYPCPT/574-B(28)/2021).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and manuscript preparation: Mayura Deshmukh; Investigations: Siddhi Pokle; Data collection: Siddhi Pokle and Ishani Gopiyani; Data analysis: Mayura Deshmukh and Gaurang Baxi; Review and finalizing manuscript: Gaurang Baxi and Tushar Palekar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the participants who participated in the study.
References
- Sembulingam K, Sembulingam P. Essentials of medical physiology. London: JP Medical Ltd; 2012. [Link]
- Chaitow L, Crenshaw K. Muscle energy techniques. Edinburgh: Elsevier Health Sciences; 2006. [Link]
- Norkin CC, Levangie PK. Joint structure & function: A comprehensive analysis. Philadelphia: F.A. Davis Co; 2005. [Link]
- Barr KP, Griggs M, Cadby T. Lumbar stabilization: A review of core concepts and current literature, part 2. American Journal of Physical Medicine & Rehabilitation. 2007; 86(1):72-80. [DOI:10.1097/01.phm.0000250566.44629.a0] [PMID]
- Ostwal PP, Wani SK. Breathing patterns in patients with low back pain. International Journal of Physiotherapy and Research. 2014; 2(1):347-53. [Link]
- Barr KP, Griggs M, Cadby T. Lumbar stabilization: Core concepts and current literature, Part 1. American Journal of Physical Medicine & Rehabilitation. 2005; 84(6):473-80. [DOI:10.1097/01.phm.0000163709.70471.42] [PMID]
- Mitchell AJ, Bacon CJ, Moran RW. Reliability and determinants of self-evaluation of breathing questionnaire (SEBQ) score: A symptoms-based measure of dysfunctional breathing. Applied Psychophysiology and Biofeedback. 2016; 41(1):111-20. [DOI:10.1007/s10484-015-9316-7] [PMID]
- Courtney R, Greenwood KM. Preliminary investigation of a measure of dysfunctional breathing symptoms: The self evaluation of breathing questionnaire (SEBQ). International Journal of Osteopathic Medicine. 2009; 12(4):121-7. [DOI:10.1016/j.ijosm.2009.02.001]
- Deshmukh, M. P., Palekar, T. J., Manvikar, N., Makker, K. S., & Mali, C. (2022). Prevalence of breathing dysfunction in musculoskeletal complaints: A cross sectional study. Int J Health Sci Res, 12(2), 146-52. [DOI:10.52403/ijhsr.20220220]
- Dionne A, Parkes A, Engler B, Watson BV, Nicolle MW. Determination of the best electrode position for recording of the diaphragm compound muscle action potential. Muscle & Nerve. 2009; 40(1):37-41. [DOI:10.1002/mus.21290] [PMID]
- Glerant JC, Mustfa N, Man WD, Luo YM, Rafferty G, Polkey MI, et al. Diaphragm electromyograms recorded from multiple surface electrodes following magnetic stimulation. The European Respiratory Journal. 2006; 27(2):334-42. [DOI:10.1183/09031936.06.00029005] [PMID]
- Jalan NS, Daftari SS, Retharekar SS, Rairikar SA, Shyam AM, Sancheti PK. Intra- and inter-rater reliability of maximum inspiratory pressure measured using a portable capsule-sensing pressure gauge device in healthy adults. Canadian Journal of Respiratory Therapy. 2015; 51(2):39-42. [PMID] [PMCID]
- Espinosa-López AM, Daza-Arana JE, Pinzón-Sanabria LM, Perdomo-Quiroga Y, Ruiz-Jiménez JP. Effects of muscle energy technique for quadratus lumborum on respiratory muscle strength in patients with breast cancer. Revista de la Facultad de Medicina. 2019; 67(4):469-75. [DOI:10.15446/revfacmed.v67n4.68950]
- Uysal SC, Tüzün EH, Eker L, Angın E. Effectiveness of the muscle energy technique on respiratory muscle strength and endurance in patients with fibromyalgia. Journal of Back and Musculoskeletal Rehabilitation. 2019; 32(3):411-9. [DOI:10.3233/BMR-181287] [PMID]
- Vaseghnia A, Shadmehr A, Moghadam BA, Olyaei G, Hadian MR, Khazaeipour Z. Effects of muscle energy technique on daily activities and lumbar stiffness in women with sacroiliac joint dysfunction: A randomized controlled clinical trial study. Journal of Modern Rehabilitation. 2019; 13(1):23-30. [DOI:10.32598/JMR.13.1.23]
- Deshmukh MP, Patil AN, Baxi G, Palekar TJ. Immediate effect of primal reflex release technique on heart rate variability in chronic neck pain: A case report. International Journal of Health Sciences and Research. 2021; 11(6):157-60. [DOI:10.52403/ijhsr.20210624]
- Tawrej P, Kaur R, Ghodey S. Immediate effect of muscle energy technique on quadratus lumborum muscle in patients with non-specific low back pain. Indian Journal of Physiotherapy & Occupational Therapy. 2020; 14(1):180-4. [DOI:10.5958/0973-5674.2020.00032.5]
- Gutiérrez MF, Valenzuela S, Miralles R, Portus C, Santander H, Fuentes AD, et al. Does breathing type influence electromyographic activity of obligatory and accessory respiratory muscles? Journal of Oral Rehabilitation. 2014; 41(11):801-8. [DOI:10.1111/joor.12209] [PMID]
- Rishi P, Arora B. Impact of muscle energy technique along with supervised. Exercise program over muscle energy technique on quadratus lumborum and iliopsoas on pain and functional disability in chronic non specific low back pain. International Journal of Physiotherapy and Research. 2018; 6(3):2748-53. [DOI:10.16965/ijpr.2018.129]
- Malaguti C, Rondelli RR, de Souza LM, Domingues M, Dal Corso S. Reliability of chest wall mobility and its correlation with pulmonary function in patients with chronic obstructive pulmonary disease. Respiratory care. 2009; 54(12):1703-11. [Link]
- Pagare RS, Pedhambkar RB. Assessment of reference values of chest expansion among healthy adults in Pune, India. International Journal of Physiotherapy and Research. 2017; 5(1):1819-23. [DOI:10.16965/ijpr.2016.197]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2022/06/9 | Accepted: 2023/09/5 | Published: 2023/12/1
Received: 2022/06/9 | Accepted: 2023/09/5 | Published: 2023/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
