
988368
Tue, Jul 15, 2025

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 623-632 |
Back to browse issues page



Ethics code: Amputation, intact limb, osteoarthritis, risk factors.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rasool A, Aftab A, Saifullah H, Kamran M, Saqulain G. Prevalence and Associated Risk Factors of Knee Osteoarthritis in Contra-lateral Limb After Limb Amputation. Iranian Rehabilitation Journal 2023; 21 (4) :623-632
URL: http://irj.uswr.ac.ir/article-1-1770-en.html
URL: http://irj.uswr.ac.ir/article-1-1770-en.html



1- Institute of Physical Medicine and Rehabilitation, Khyber Medical University, Peshawar, Pakistan.
2- Department of Allied Health Sciences, Faculty of Pharmacy & Allied Health Sciences, University of Sialkot, Sialkot, Pakistan.
3- Department of Prosthetic & Orthotics, Secure Logic Tech Malaysia, Selangor, Malaysia.
4- Department of Prosthetics and Orthotics, Chal Foundation Bacha Khan Medical Complex KPK, Peshawar, Pakistan.
5- Department of Otorhinolaryngology, Capital Hospital PGMI, Islamabad, Pakistan.
2- Department of Allied Health Sciences, Faculty of Pharmacy & Allied Health Sciences, University of Sialkot, Sialkot, Pakistan.
3- Department of Prosthetic & Orthotics, Secure Logic Tech Malaysia, Selangor, Malaysia.
4- Department of Prosthetics and Orthotics, Chal Foundation Bacha Khan Medical Complex KPK, Peshawar, Pakistan.
5- Department of Otorhinolaryngology, Capital Hospital PGMI, Islamabad, Pakistan.
Full-Text [PDF 567 kb]
(705 Downloads)
| Abstract (HTML) (1993 Views)
Full-Text: (345 Views)
Introduction
Osteoarthritis (OA)
OA is a degenerative condition that affects the tissues of the joints, resulting in changes in the structure of joint tissue in terms of metabolism and functioning [1], since this is associated with damage to articular cartilage; formation of osteophytes, subchondral sclerosis and inflammation of synovial lining resulting in loss of function [2] is the leading cause of disability [3]. It can be caused by several factors that contribute to its causation [1].
Prevalence of knee OA
Knee OA is one of the most common conditions in the elderly population with a high global prevalence of 16% in people older than 15 years and 22% in people older than 22 years [4]. A very high prevalence of 28% in urban and 25% in rural areas of Pakistan has been reported for the population older than 18 years [5] and an even higher prevalence of 56.7% in middle-aged adults [6] with a higher prevalence in women [4]. Moreover, the prevalence of knee OA is likely to increase due to the population aging and obesity [7]. A study conducted by Farrokhi et al. revealed an increased prevalence of knee OA and its risk factors in the military population with lower limb amputation [8].
Types of OA
OA can be classified into primary and secondary varieties. Primary OA occurs without a history of disease or predisposing traumatic injury due to risk factors, such as higher age, female gender, increased body mass index (BMI), structural factors, including weakness of muscles, and injury to joints [9]. The secondary variety arises in cases with pre-existing abnormality of the joint [9], such as abnormalities of articular cartilages occurring due to lesions, such as rheumatoid arthritis, or abnormal focus of forces at the joint, such as in post-injury cases [10].
OA involving sound limb
Lower limb amputees also face long-term issues resulting from amputation, including an increased risk of developing OA of the knee and hip on the sound side, which may be due to gait changes due to the use of a prosthesis, which can increase the load on the normal side [11]. Literature also suggests that lower extremity amputation exposes the healthy limb to a increased risk of OA [12]. A recent study conducted by Welke et al. contradicts this issue which may be because of mechanical factors etc. [13].
Risk factors of OA
Several risk factors are incriminated, including age, weight, injury during squatting kneeling, etc, cytokines, leptins, [14] female gender, weak leg muscles, reduced or excessive physical activity, obesity, trauma (accidental or surgical), chronic knee pain [15] as well as some biomechanical factors [16].
As compared to all other large joints of the body, the knee joint is a significant load-bearing joint, in which soft tissues are the main stabilizing factors. With a force 2-3 times body weight being transmitted through it during walking, these forces are crucial in OA [17]; hence, the knee joint is most commonly affected and affected by daily activities, such as climbing stairs, rising from a chair, prolonged standing, and walking.
Research gap and current study
Several risk factors can put the healthy knee at risk of developing OA, thus identifying and controlling such factors is essential to prevent knee OA [15]. Hence, with a research gap in the literature [1], research into knee OA risk factors for the intact limb in amputated individuals requires an hour to preserve the intact limb [8].
Therefore, after these keen observations, in a developing country, it is essential to research into prevalence of knee OA and its associated risk factors for the contralateral limb after lower limb amputation to avoid such risk factors and bring awareness among the public or plan preventive strategies.
Materials and Methods
This cross-sectional survey was conducted in six months from July 1, 2019, to December 31, 2019, utilizing non-probability convenience sampling. The study included a sample of 500 patients with unilateral lower limb amputation (131 trans-femoral amputees [TFA] [26.2%], 26 knee disarticulation [5.2%], 314 trans-tibial amputees (TTA) [62.8%] and 29 partial foot amputees [5.8%]) using prosthesis for at least 1 year and registered in Pakistan Institute of Prosthetic and Orthotic Sciences (PIPOS), Peshawar City, Pakistan rehabilitation services program (PRSP) and its satellite centers across Khyber Pakhtunkhwa. The inclusion criteria included either gender aged 20 to 80 years. The exclusion criteria included cases with bilateral lower limb amputation, Polio, club foot, or any other deformity, people who used orthotics on the contralateral side, and congenital amputees. A sample of 500 people was calculated using the Rao soft online calculator with a 99% confidence interval, 5.69% error margin, a population of 20000, and 50% response distribution.
Initially, the records were obtained from the Punjab Rural Support Program (PRSP) center’s reception/front desk. Unilateral lower limb amputees were filtered from those data by quoting their medical record numbers. Data search was further advanced by studying individual case files. All case files of unilateral lower limb amputees who were fitted with prostheses at least one year before and aged between 20 and 80 years were segregated. Files that revealed that the patient had a history of polio, club foot, or other such deformities, or used or were prescribed orthotics on the contralateral side and those who were congenital amputees were removed. Contacts of those cases who seemed to meet the selection criteria as per their record were noted. Then, they were contacted and interviewed by phone utilizing voice as well as video telephony and, their selection criteria were confirmed. They were explained the study and consent was obtained. Hence, 500 cases who met the selection criteria and consented to be included in the study were taken as a sample for the study. Following this, patients were individually contacted through phone calls to participate in the study. A basic demographic sheet, an invalid risk factor questionnaire [18], and American college of rheumatology (ACR) guidelines for diagnostic knee OA were used to collect data. The validity of these criteria has a sensitivity of >90% and specificity ranging from 60% to 84% [19]. The criteria included a history of pain in the knee and one of the following findings, age above 50 years, morning stiffness of less than half an hour duration, crepitus during active movement, and osteophyte formation. For this purpose, plain radiographs were considered. Most patients brought with them radiographs, which were taken at facilities near their residence for pain, while some were subjected to plain radiography for their clinical needs by the concerned orthopedics doctors who also reported the findings and included them in the study by the researchers.
Data were analyzed using SPSS software, version 21. Descriptive statistics were utilized, including frequency, percentage, and odd ratio calculated for risk factors. Chi-square statistics were utilized to observe the relationship with P<0.05 as significant.
Results
The current study revealed the prevalence of OA in 131 subjects (26.2%) (Figure 1).
 In terms of gender, no significant difference (P=0.446) was observed in 86 women (65.6%) suffering from OA, while in terms of age group, 75 participants (57.3%) in the age group of 51-80 years had OA (P=0.000) (Table 1).
In terms of gender, no significant difference (P=0.446) was observed in 86 women (65.6%) suffering from OA, while in terms of age group, 75 participants (57.3%) in the age group of 51-80 years had OA (P=0.000) (Table 1).

Also, in terms of marital status, significantly (P=0.000) 99 married individuals (75.6%) had OA. In addition, significantly (P=0.000) 87 TTA (66.4%) followed by 33 TFA (25.2%) using a trans-tibial and trans-femoral prosthesis, respectively had OA.
Of the total number of OA cases i.e. 131, the prevalence of risk factors was in 129 cases (98.5%) for occupation, followed by 127(96.9%) for sustained knee bending, 117(89.3%) for the history of a painful knee injury, 106(80.9%) for sitting on the floor for home activities, 86(65.5%) for the female gender, 81(61.8%) for overweight, 72(55%) for barefoot walking, 71(54.2%) for stair climbing, 43(32.8%) for prolonged standing and family history of knee or other joint diseases, 23(17.6%) for use of high heeled shoes and 21(16%) for >4 hour heavy activities (Table 2).
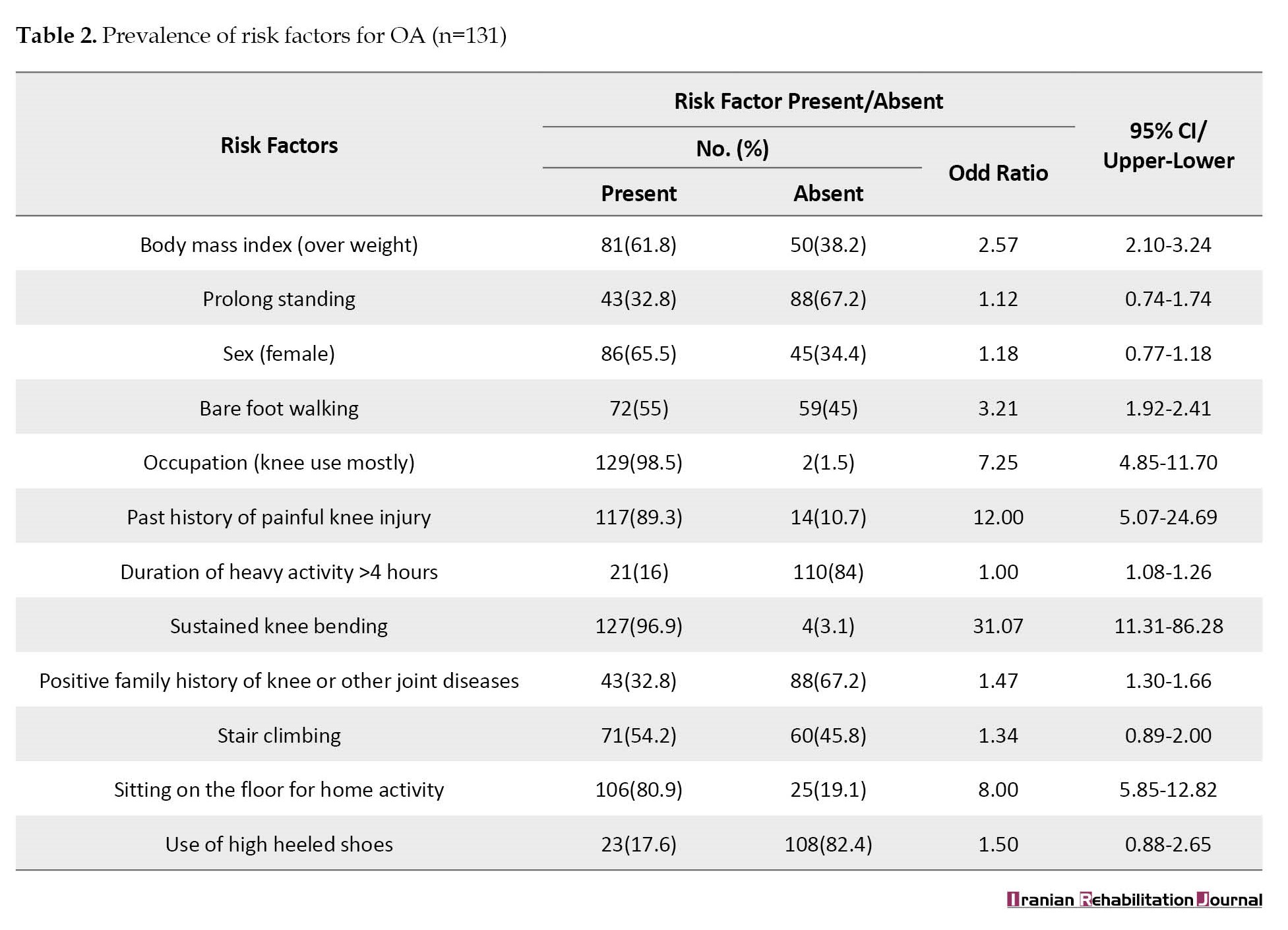
No significant (P>0.05) correlation was observed between sustained knee bending as the most prevalent risk factor in 127 affected subjects (96.9%) (31.07) (Table 2) with other risk factors and the risk factor of sustained knee bending showed no significant relationship with age of the patient, marital status, and amputation level, and prosthesis type (Table 3).

A significant negative correlation (r=-0.360, P=0.000) (Table 4) was observed between the history of a painful knee injury as the second commonest factor in 117 affected subjects (89.3%, 12.00) with occupation commonly associated with knee use and no relationship was observed with other factors (P>0.05).
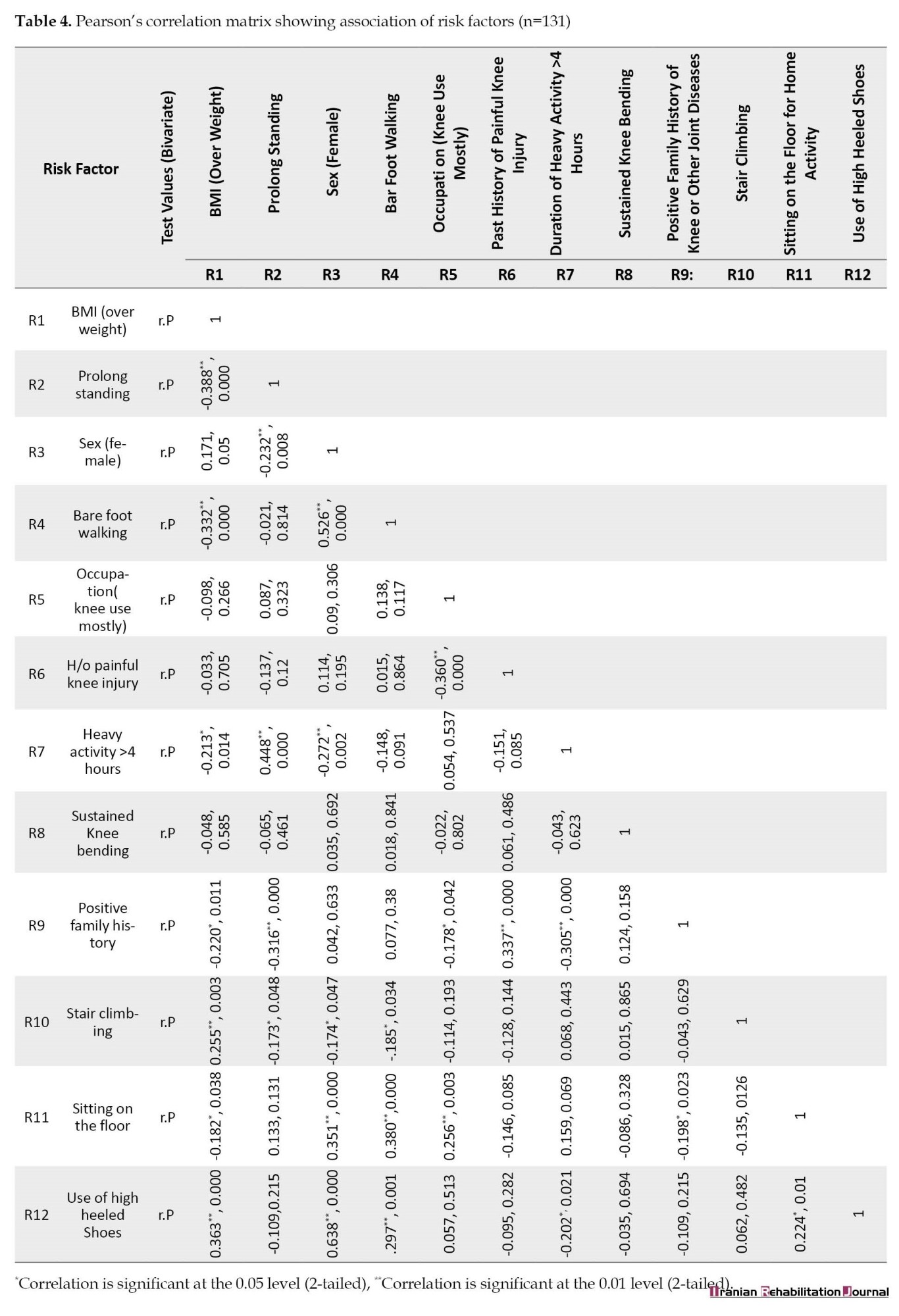
This factor also showed no significant relationship with age, marital status, and amputation level, and prosthesis type.
A significant (P<0.05) negative correlation was observed between sitting on the floor for home activities in 106 affected subjects (80.9%, 8.00) with BMI (overweight), a history of a painful knee injury, positive family history of knee or other joint disease, stair climbing and a positive correlation was observed with female gender, barefoot walking, and occupation with knee usage. However, this factor showed no significant relationship with age, marital status, and amputation level, and prosthesis type.
A significant (P<0.05) negative correlation was observed between the risk factor of occupation with knee use in 129 affected subjects (98.5%, 7.25) with a history of a painful knee injury, sustained knee bending, positive family history, and a positive correlation was observed with sitting on the floor, and no relationship was observed with age, marital status, amputation level, and prosthesis type.
Thus, the current study indicates that sustained knee bending is an independent and most prevalent risk factor that is not dependent on other factors. Hence, this is an easily avoidable factor. The second most common factor is the history of a painful knee injury, which has a significant negative correlation with occupation; hence, occupations in which the chance of knee injury is less are crucial. The third most common factor is sitting on the floor for home activities which has a significant negative correlation with BMI (overweight), a history of a painful knee injury, a positive family history of knee or other joint diseases, stair climbing, and a positive correlation is observed with female gender, barefoot walking, and occupation with knee usage, hence, weight reduction can result in a significant reduction in the risk factor of knee OA. The risk factor of occupation with knee use has a significant negative correlation with the history of a painful knee injury, sustained knee bending, positive family history, and a positive correlation with sitting on the floor, indicating that these factors are interrelated and avoidance can significantly reduce the chances of knee OA.
Discussion
The present study revealed the prevalence of knee OA for lower extremity amputees in the intact or sound limb of 131 people (26.2%). Similarly, a small study conducted by Struyf et al. reported a prevalence of 27% [20]. While in contrast, Welke et al. in a large study reported a much lower prevalence of knee OA in 261 people (16.6%) in TFA compared to non-amputees, the lower prevalence may be due to reduced physical activity and heavy work [21] due to a higher level of amputation, while the current study included mostly TTA and revealed a higher prevalence of knee OA. Similarly, Norvell et al. also reported a prevalence (16.1%) of OA in amputees compared to non-amputees (11.7%) [22]; however, these studies are quite different from the current study because the current study did not include non-amputees.
The literature reveals obesity, female gender [23], sedentary lifestyle, and age as significant risk factors for knee OA without focusing on amputation cases [24]. However, in the current study, the female gender revealed a higher prevalence in 86 subjects (65.6%) with OA; however, the difference was not significant (P=0.446) and the odd ratio revealed a lower value (1.18). A reason behind this finding may be the sedentary lifestyle of women who are culturally expected to stay at home. Consistent with our study, a similarly higher prevalence in women has been reported in a Saudi study involving non-amputees probably due to variations in anatomy, female hormones, and genetic makeup [23]. This is consistent with the international literature [25]. Similarly, in the current study, obesity revealed a higher prevalence in 81 subjects (61.8%) with OA indicating that it is a risk factor (2.57) of OA, which is by the available literature [26]. However, another local study involving non-amputated cases reported BMI (overweight) with an odd ratio of 11.636 as the number one risk factor [18], indicating that though it was a risk factor of OA, its impact on the sound limb in amputees was less, possibly because in amputees, the mobility was restricted due to amputation and the additional impact of obesity on the sound limb was less.
In the present study, OA was significantly (P=0.000) more common in 75 subjects (57.3%) in the age group of 51-80 years. Similarly, a study conducted by Welke et al. revealed that most cases (39%) of knee OA in amputees occurred in subjects aged 70-79 years, followed by 20.3% in subjects aged 60-69 years followed by 16.2% each in the age group of 50-59 and 80-89 years [21]. A Saudi study also revealed the relationship of OA with age; however, more severe OA was reported to affect non-amputee elderly [23], indicating that aging was a risk factor for OA, which is consistent with the literature [21].
This study also revealed a significantly (P=0.000) higher prevalence of OA in 99 married subjects (75.6%). Consistent with the current study, a study conducted by Jørgensen et al. also revealed that OA risk and admission in hospitals are more common among married men, which may be due to the lifestyle of people with children [27], since married individuals with families have to perform additional tasks to run their families, putting them at additional risk of injury and hence risk of OA.
In the present study, knee OA was more prevalent in 87 TTA (66.4%) followed by 33 TFA (25.2%) with the same percentage using trans-tibial and trans-femoral prostheses, respectively. This seems to be consistent with literature revealing that symmetry for the first peak; stance and impulse vary with amputation level and are related to intact knee OA [28]. However, some prosthetic feet, such as energy storing and return (ESAR) prosthetic feet may not result in any significant difference in joint kinematics and hence may not affect joint contact forces, which may be responsible for OA in other cases on the intact side [29]. According to Ding et al., knee OA of a healthy limb can be prevented by better prosthetic designs and foot control, socket design, and strength of muscles on the amputated side [30].
In the current study, sustained knee bending was the most prevalent risk factor in 127 affected people (96.9%, 31.07) consistent with the literature [31]. In contrast, Dahaghin et al. reported that knee bending had only borderline risk [32] and another local study labeled it as low risk with 2.738 [18]. The results in the current study may be because, in Pakistani culture, women usually sit on the floor for home activity with sustained knee bending, especially while working in kitchens and doing laundry that may be the cause of sustained knee bending, which is the most prevalent risk factor for OA.
Barefoot walking was the second most common risk factor identified in the current study with a prevalence of OA in 72 subjects (55%, 3.21). In contrast, Dahaghin et al. reported that even walking up and down was not a risk factor [32] in non-amputees; while in contrast, our study focused on amputees, in whom reduced physical activity was reported as a possible risk factor [15].
The history of a painful knee injury was in 117 affected people (89.3%, 12.00) in the current study, which is consistent with the available literature according to which, loading injuries, such as injury to the meniscus, joint ligaments, fractures, and dislocations are linked with many fold increased risk of knee OA [26]. Also, the literature reveals that traumatic amputees revealed an increased prevalence of knee OA of uninvolved limbs compared to healthy individuals [33].
Sitting on the floor for home activities is a significant risk factor with a prevalence of 106 (80.9%, 8.00) in the current study, which is in contrast to the literature revealing that sitting on the floor did not qualify for being a risk factor [32]. This difference may be because in developing countries, such as Pakistan, especially in rural suburbs, the population spends a lot of time sitting on the floor as well as in a squatting position since they use Indian latrines, where squatting becomes essential, which can damage the knee structures.
This study revealed that occupation with knee use in 129 cases (98.5%, 7.25) was a significant risk factor, which is consistent with the literature that occupations involving standing for long periods and frequent knee bending is considered a modifiable risk factor [31].
Conclusion
The study concludes that due to a high prevalence of OA in the sound limb in the current study, knee OA should be suspected in amputated cases, especially trans-tibial amputation with risk factors, including male gender, older age group, sustained knee bending, the history of a painful knee injury, sitting on the floor for home activities and occupations with knee use.
Study limitations
Since the study utilized an invalid risk factor questionnaire that was used in another study and a convenience sampling method was used, this can affect the study results and bring potential bias. The study was conducted only in one province of the country and a smaller number of women opted for the study; hence, the results cannot be generalized.
Ethical Considerations
Compliance with ethical guidelines
The study was initiated following ethical approval of the Institutional Research Board of Isra University (No.: 1609-P&O-008), and informed consent of the cases before entering the study.
Funding
This article is extracted from MPhil thesis of Arsalan Rasool, approved by Isra University.
Authors' contributions
Conceptualization and supervision: Anam Aftab and Hassan Saifullah; Methodology, resources and data curation: Arsalan Rasool; Formal analysis and writing-original draft preparation: Muhammad Kamran and Anam Aftab; Supervision, review and editing: Ghulam Saqulain.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are indebted and thankful to the management of Pakistan Institute of Prosthetic and Orthotic Sciences to make this study possible.
References
Osteoarthritis (OA)
OA is a degenerative condition that affects the tissues of the joints, resulting in changes in the structure of joint tissue in terms of metabolism and functioning [1], since this is associated with damage to articular cartilage; formation of osteophytes, subchondral sclerosis and inflammation of synovial lining resulting in loss of function [2] is the leading cause of disability [3]. It can be caused by several factors that contribute to its causation [1].
Prevalence of knee OA
Knee OA is one of the most common conditions in the elderly population with a high global prevalence of 16% in people older than 15 years and 22% in people older than 22 years [4]. A very high prevalence of 28% in urban and 25% in rural areas of Pakistan has been reported for the population older than 18 years [5] and an even higher prevalence of 56.7% in middle-aged adults [6] with a higher prevalence in women [4]. Moreover, the prevalence of knee OA is likely to increase due to the population aging and obesity [7]. A study conducted by Farrokhi et al. revealed an increased prevalence of knee OA and its risk factors in the military population with lower limb amputation [8].
Types of OA
OA can be classified into primary and secondary varieties. Primary OA occurs without a history of disease or predisposing traumatic injury due to risk factors, such as higher age, female gender, increased body mass index (BMI), structural factors, including weakness of muscles, and injury to joints [9]. The secondary variety arises in cases with pre-existing abnormality of the joint [9], such as abnormalities of articular cartilages occurring due to lesions, such as rheumatoid arthritis, or abnormal focus of forces at the joint, such as in post-injury cases [10].
OA involving sound limb
Lower limb amputees also face long-term issues resulting from amputation, including an increased risk of developing OA of the knee and hip on the sound side, which may be due to gait changes due to the use of a prosthesis, which can increase the load on the normal side [11]. Literature also suggests that lower extremity amputation exposes the healthy limb to a increased risk of OA [12]. A recent study conducted by Welke et al. contradicts this issue which may be because of mechanical factors etc. [13].
Risk factors of OA
Several risk factors are incriminated, including age, weight, injury during squatting kneeling, etc, cytokines, leptins, [14] female gender, weak leg muscles, reduced or excessive physical activity, obesity, trauma (accidental or surgical), chronic knee pain [15] as well as some biomechanical factors [16].
As compared to all other large joints of the body, the knee joint is a significant load-bearing joint, in which soft tissues are the main stabilizing factors. With a force 2-3 times body weight being transmitted through it during walking, these forces are crucial in OA [17]; hence, the knee joint is most commonly affected and affected by daily activities, such as climbing stairs, rising from a chair, prolonged standing, and walking.
Research gap and current study
Several risk factors can put the healthy knee at risk of developing OA, thus identifying and controlling such factors is essential to prevent knee OA [15]. Hence, with a research gap in the literature [1], research into knee OA risk factors for the intact limb in amputated individuals requires an hour to preserve the intact limb [8].
Therefore, after these keen observations, in a developing country, it is essential to research into prevalence of knee OA and its associated risk factors for the contralateral limb after lower limb amputation to avoid such risk factors and bring awareness among the public or plan preventive strategies.
Materials and Methods
This cross-sectional survey was conducted in six months from July 1, 2019, to December 31, 2019, utilizing non-probability convenience sampling. The study included a sample of 500 patients with unilateral lower limb amputation (131 trans-femoral amputees [TFA] [26.2%], 26 knee disarticulation [5.2%], 314 trans-tibial amputees (TTA) [62.8%] and 29 partial foot amputees [5.8%]) using prosthesis for at least 1 year and registered in Pakistan Institute of Prosthetic and Orthotic Sciences (PIPOS), Peshawar City, Pakistan rehabilitation services program (PRSP) and its satellite centers across Khyber Pakhtunkhwa. The inclusion criteria included either gender aged 20 to 80 years. The exclusion criteria included cases with bilateral lower limb amputation, Polio, club foot, or any other deformity, people who used orthotics on the contralateral side, and congenital amputees. A sample of 500 people was calculated using the Rao soft online calculator with a 99% confidence interval, 5.69% error margin, a population of 20000, and 50% response distribution.
Initially, the records were obtained from the Punjab Rural Support Program (PRSP) center’s reception/front desk. Unilateral lower limb amputees were filtered from those data by quoting their medical record numbers. Data search was further advanced by studying individual case files. All case files of unilateral lower limb amputees who were fitted with prostheses at least one year before and aged between 20 and 80 years were segregated. Files that revealed that the patient had a history of polio, club foot, or other such deformities, or used or were prescribed orthotics on the contralateral side and those who were congenital amputees were removed. Contacts of those cases who seemed to meet the selection criteria as per their record were noted. Then, they were contacted and interviewed by phone utilizing voice as well as video telephony and, their selection criteria were confirmed. They were explained the study and consent was obtained. Hence, 500 cases who met the selection criteria and consented to be included in the study were taken as a sample for the study. Following this, patients were individually contacted through phone calls to participate in the study. A basic demographic sheet, an invalid risk factor questionnaire [18], and American college of rheumatology (ACR) guidelines for diagnostic knee OA were used to collect data. The validity of these criteria has a sensitivity of >90% and specificity ranging from 60% to 84% [19]. The criteria included a history of pain in the knee and one of the following findings, age above 50 years, morning stiffness of less than half an hour duration, crepitus during active movement, and osteophyte formation. For this purpose, plain radiographs were considered. Most patients brought with them radiographs, which were taken at facilities near their residence for pain, while some were subjected to plain radiography for their clinical needs by the concerned orthopedics doctors who also reported the findings and included them in the study by the researchers.
Data were analyzed using SPSS software, version 21. Descriptive statistics were utilized, including frequency, percentage, and odd ratio calculated for risk factors. Chi-square statistics were utilized to observe the relationship with P<0.05 as significant.
Results
The current study revealed the prevalence of OA in 131 subjects (26.2%) (Figure 1).
Also, in terms of marital status, significantly (P=0.000) 99 married individuals (75.6%) had OA. In addition, significantly (P=0.000) 87 TTA (66.4%) followed by 33 TFA (25.2%) using a trans-tibial and trans-femoral prosthesis, respectively had OA.
Of the total number of OA cases i.e. 131, the prevalence of risk factors was in 129 cases (98.5%) for occupation, followed by 127(96.9%) for sustained knee bending, 117(89.3%) for the history of a painful knee injury, 106(80.9%) for sitting on the floor for home activities, 86(65.5%) for the female gender, 81(61.8%) for overweight, 72(55%) for barefoot walking, 71(54.2%) for stair climbing, 43(32.8%) for prolonged standing and family history of knee or other joint diseases, 23(17.6%) for use of high heeled shoes and 21(16%) for >4 hour heavy activities (Table 2).
No significant (P>0.05) correlation was observed between sustained knee bending as the most prevalent risk factor in 127 affected subjects (96.9%) (31.07) (Table 2) with other risk factors and the risk factor of sustained knee bending showed no significant relationship with age of the patient, marital status, and amputation level, and prosthesis type (Table 3).
A significant negative correlation (r=-0.360, P=0.000) (Table 4) was observed between the history of a painful knee injury as the second commonest factor in 117 affected subjects (89.3%, 12.00) with occupation commonly associated with knee use and no relationship was observed with other factors (P>0.05).
This factor also showed no significant relationship with age, marital status, and amputation level, and prosthesis type.
A significant (P<0.05) negative correlation was observed between sitting on the floor for home activities in 106 affected subjects (80.9%, 8.00) with BMI (overweight), a history of a painful knee injury, positive family history of knee or other joint disease, stair climbing and a positive correlation was observed with female gender, barefoot walking, and occupation with knee usage. However, this factor showed no significant relationship with age, marital status, and amputation level, and prosthesis type.
A significant (P<0.05) negative correlation was observed between the risk factor of occupation with knee use in 129 affected subjects (98.5%, 7.25) with a history of a painful knee injury, sustained knee bending, positive family history, and a positive correlation was observed with sitting on the floor, and no relationship was observed with age, marital status, amputation level, and prosthesis type.
Thus, the current study indicates that sustained knee bending is an independent and most prevalent risk factor that is not dependent on other factors. Hence, this is an easily avoidable factor. The second most common factor is the history of a painful knee injury, which has a significant negative correlation with occupation; hence, occupations in which the chance of knee injury is less are crucial. The third most common factor is sitting on the floor for home activities which has a significant negative correlation with BMI (overweight), a history of a painful knee injury, a positive family history of knee or other joint diseases, stair climbing, and a positive correlation is observed with female gender, barefoot walking, and occupation with knee usage, hence, weight reduction can result in a significant reduction in the risk factor of knee OA. The risk factor of occupation with knee use has a significant negative correlation with the history of a painful knee injury, sustained knee bending, positive family history, and a positive correlation with sitting on the floor, indicating that these factors are interrelated and avoidance can significantly reduce the chances of knee OA.
Discussion
The present study revealed the prevalence of knee OA for lower extremity amputees in the intact or sound limb of 131 people (26.2%). Similarly, a small study conducted by Struyf et al. reported a prevalence of 27% [20]. While in contrast, Welke et al. in a large study reported a much lower prevalence of knee OA in 261 people (16.6%) in TFA compared to non-amputees, the lower prevalence may be due to reduced physical activity and heavy work [21] due to a higher level of amputation, while the current study included mostly TTA and revealed a higher prevalence of knee OA. Similarly, Norvell et al. also reported a prevalence (16.1%) of OA in amputees compared to non-amputees (11.7%) [22]; however, these studies are quite different from the current study because the current study did not include non-amputees.
The literature reveals obesity, female gender [23], sedentary lifestyle, and age as significant risk factors for knee OA without focusing on amputation cases [24]. However, in the current study, the female gender revealed a higher prevalence in 86 subjects (65.6%) with OA; however, the difference was not significant (P=0.446) and the odd ratio revealed a lower value (1.18). A reason behind this finding may be the sedentary lifestyle of women who are culturally expected to stay at home. Consistent with our study, a similarly higher prevalence in women has been reported in a Saudi study involving non-amputees probably due to variations in anatomy, female hormones, and genetic makeup [23]. This is consistent with the international literature [25]. Similarly, in the current study, obesity revealed a higher prevalence in 81 subjects (61.8%) with OA indicating that it is a risk factor (2.57) of OA, which is by the available literature [26]. However, another local study involving non-amputated cases reported BMI (overweight) with an odd ratio of 11.636 as the number one risk factor [18], indicating that though it was a risk factor of OA, its impact on the sound limb in amputees was less, possibly because in amputees, the mobility was restricted due to amputation and the additional impact of obesity on the sound limb was less.
In the present study, OA was significantly (P=0.000) more common in 75 subjects (57.3%) in the age group of 51-80 years. Similarly, a study conducted by Welke et al. revealed that most cases (39%) of knee OA in amputees occurred in subjects aged 70-79 years, followed by 20.3% in subjects aged 60-69 years followed by 16.2% each in the age group of 50-59 and 80-89 years [21]. A Saudi study also revealed the relationship of OA with age; however, more severe OA was reported to affect non-amputee elderly [23], indicating that aging was a risk factor for OA, which is consistent with the literature [21].
This study also revealed a significantly (P=0.000) higher prevalence of OA in 99 married subjects (75.6%). Consistent with the current study, a study conducted by Jørgensen et al. also revealed that OA risk and admission in hospitals are more common among married men, which may be due to the lifestyle of people with children [27], since married individuals with families have to perform additional tasks to run their families, putting them at additional risk of injury and hence risk of OA.
In the present study, knee OA was more prevalent in 87 TTA (66.4%) followed by 33 TFA (25.2%) with the same percentage using trans-tibial and trans-femoral prostheses, respectively. This seems to be consistent with literature revealing that symmetry for the first peak; stance and impulse vary with amputation level and are related to intact knee OA [28]. However, some prosthetic feet, such as energy storing and return (ESAR) prosthetic feet may not result in any significant difference in joint kinematics and hence may not affect joint contact forces, which may be responsible for OA in other cases on the intact side [29]. According to Ding et al., knee OA of a healthy limb can be prevented by better prosthetic designs and foot control, socket design, and strength of muscles on the amputated side [30].
In the current study, sustained knee bending was the most prevalent risk factor in 127 affected people (96.9%, 31.07) consistent with the literature [31]. In contrast, Dahaghin et al. reported that knee bending had only borderline risk [32] and another local study labeled it as low risk with 2.738 [18]. The results in the current study may be because, in Pakistani culture, women usually sit on the floor for home activity with sustained knee bending, especially while working in kitchens and doing laundry that may be the cause of sustained knee bending, which is the most prevalent risk factor for OA.
Barefoot walking was the second most common risk factor identified in the current study with a prevalence of OA in 72 subjects (55%, 3.21). In contrast, Dahaghin et al. reported that even walking up and down was not a risk factor [32] in non-amputees; while in contrast, our study focused on amputees, in whom reduced physical activity was reported as a possible risk factor [15].
The history of a painful knee injury was in 117 affected people (89.3%, 12.00) in the current study, which is consistent with the available literature according to which, loading injuries, such as injury to the meniscus, joint ligaments, fractures, and dislocations are linked with many fold increased risk of knee OA [26]. Also, the literature reveals that traumatic amputees revealed an increased prevalence of knee OA of uninvolved limbs compared to healthy individuals [33].
Sitting on the floor for home activities is a significant risk factor with a prevalence of 106 (80.9%, 8.00) in the current study, which is in contrast to the literature revealing that sitting on the floor did not qualify for being a risk factor [32]. This difference may be because in developing countries, such as Pakistan, especially in rural suburbs, the population spends a lot of time sitting on the floor as well as in a squatting position since they use Indian latrines, where squatting becomes essential, which can damage the knee structures.
This study revealed that occupation with knee use in 129 cases (98.5%, 7.25) was a significant risk factor, which is consistent with the literature that occupations involving standing for long periods and frequent knee bending is considered a modifiable risk factor [31].
Conclusion
The study concludes that due to a high prevalence of OA in the sound limb in the current study, knee OA should be suspected in amputated cases, especially trans-tibial amputation with risk factors, including male gender, older age group, sustained knee bending, the history of a painful knee injury, sitting on the floor for home activities and occupations with knee use.
Study limitations
Since the study utilized an invalid risk factor questionnaire that was used in another study and a convenience sampling method was used, this can affect the study results and bring potential bias. The study was conducted only in one province of the country and a smaller number of women opted for the study; hence, the results cannot be generalized.
Ethical Considerations
Compliance with ethical guidelines
The study was initiated following ethical approval of the Institutional Research Board of Isra University (No.: 1609-P&O-008), and informed consent of the cases before entering the study.
Funding
This article is extracted from MPhil thesis of Arsalan Rasool, approved by Isra University.
Authors' contributions
Conceptualization and supervision: Anam Aftab and Hassan Saifullah; Methodology, resources and data curation: Arsalan Rasool; Formal analysis and writing-original draft preparation: Muhammad Kamran and Anam Aftab; Supervision, review and editing: Ghulam Saqulain.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are indebted and thankful to the management of Pakistan Institute of Prosthetic and Orthotic Sciences to make this study possible.
References
- Primorac D, Molnar V, Rod E, Jeleč Ž, Čukelj F, Matišić V, et al. Knee osteoarthritis: A review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes. 2020; 11(8):854. [DOI:10.3390/genes11080854] [PMID]
- Samvelyan HJ, Hughes D, Stevens C, Staines KA. Models of osteoarthritis: Relevance and new insights. Calcified Tissue International. 2021; 109(3):243-56. [DOI:10.1007/s00223-020-00670-x] [PMID]
- Osama M, Babur MN, Siddiqi FA. Walking related performance fatigability in persons with knee osteoarthritis; an important yet neglected outcome. The Journal of the Pakistan Medical Association. 2021; 71(5):1513-4. [DOI:10.47391/JPMA.1166] [PMID]
- Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020; 29-30:100587. [DOI:10.1016/j.eclinm.2020.100587] [PMID]
- Iqbal MN, Haidri FR, Motiani B, Mannan A. Frequency of factors associated with knee osteoarthritis. The Journal of the Pakistan Medical Association. 2011; 61(8):786-9. [PMID]
- Malik FB, Memon AG, Shah S, Latif D, Afzal MF, Memon SA. Prevalence of knee osteoarthritis and quality of life among middle aged adults in of Pakistan. The Rehabilitation Journal. 2022; 6(1):280-3. [DOI:10.52567/trj.v6i01.80]
- Palazzo C, Nguyen C, Lefevre-Colau MM, Rannou F, Poiraudeau S. Risk factors and burden of osteoarthritis. Annals of Physical and Rehabilitation Medicine. 2016; 59(3):134-8. [DOI:10.1016/j.rehab.2016.01.006] [PMID]
- Farrokhi S, Mazzone B, Yoder A, Grant K, Wyatt M. A narrative review of the prevalence and risk factors associated with development of knee osteoarthritis after traumatic unilateral lower limb amputation. Military Medicine. 2016; 181(S4):38-44. [DOI:10.7205/MILMED-D-15-00510] [PMID]
- Sen R, Hurley JA. Osteoarthritis. Treasure Island: StatPearls Publishing; 2022. [Link]
- Swagerty DL, Hellinger D. Radiographic assessment of osteoarthritis. American Family Physician. 2001; 64(2):279-87. [PMID]
- Pröbsting E, Kannenberg A, Blumentritt S. Back pain and osteoarthritis as secondary disabilities of lower limb amputation. Canadian Prosthetics & Orthotics Journal. 2018; 1(2):26-9. [DOI:10.33137/cpoj.v1i2.32034]
- Ngo W, Finnerty C, Finco MG,B Holley B, Menegaz RA. Additive effects of diabetes and lower-limb amputation on osteoarthritis with comparison to diabetic and healthy controls. The FASEB Journal. 2022; 36(S1):307490. [DOI:10.1096/fasebj.2022.36.S1.R3505]
- Burke MJ, Roman V, Wright V. Bone and joint changes in lower limb amputees. Annals of The Rheumatic Diseases. 1978; 37(3):252-4. [PMID]
- Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Caspian Journal of Internal Medicine. 2011; 2(2):205-12. [PMID] [PMCID]
- Khokhlova OI, Vasilchenko EM, Berman AM. The role of classical risk factors for knee osteoarthritis in unilateral transtibial amputation. Kazan Medical Journal. 2021; 102(6):891-901 [DOI:10.17816/KMJ2021-893]
- Russell Esposito E, Wilken JM. Biomechanical risk factors for knee osteoarthritis when using passive and powered ankle-foot prostheses. Clinical Biomechanics. 2014; 29(10):1186-92. [DOI:10.1016/j.clinbiomech.2014.09.005] [PMID]
- D'Lima DD, Fregly BJ, Patil S, Steklov N, Colwell CW Jr. Knee joint forces: Prediction, measurement, and significance. Proceedings of the Institution of Mechanical Engineers. 2012; 226(2):95-102. [DOI:10.1177/0954411911433372] [PMID] [PMCID]
- Aftab A, Siddiqi F, Babur MN, Memon AR. Risk factors in the development of knee osteoarthritis: A case-control study. Int. International Journal of Rehabilitation Research. 2015; 4(1):1-4. [Link]
- Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and therapeutic criteria committee of the american rheumatism association. Arthritis and Rheumatism. 1986; 29(8):1039-49. [DOI:10.1002/art.1780290816] [PMID]
- Struyf PA, van Heugten CM, Hitters MW, Smeets RJ. The prevalence of osteoarthritis of the intact hip and knee among traumatic leg amputees. Archives of Physical Medicine and Rehabilitation. 2009; 90(3):440-6. [DOI:10.1016/j.apmr.2008.08.220] [PMID]
- Welke B, Jakubowitz E, Seehaus F, Daniilidis K, Timpner M, Tremer N, et al. The prevalence of osteoarthritis: Higher risk after transfemoral amputation?-A database analysis with 1, 569 amputees and matched controls. Plos One. 2019; 14(1):e0210868. [DOI:10.1371/journal.pone.0210868] [PMID] [PMCID]
- Norvell DC, Czerniecki JM, Reiber GE, Maynard C, Pecoraro JA, Weiss NS. The prevalence of knee pain and symptomatic knee osteoarthritis among veteran traumatic amputees and nonamputees. Archives of Physical Medicine and Rehabilitation. 2005; 86(3):487-93. [DOI:10.1016/j.apmr.2004.04.034] [PMID]
- Alrowaili MG. Magnetic resonance evaluation of knee osteoarthritis among the Saudi Population. Pakistan Journal of Medical Sciences. 2019; 35(6):1575-81. [DOI:10.12669/pjms.35.6.874] [PMID]
- Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian Journal of Orthopaedics. 2016; 50(5):518-22. [DOI:10.4103/0019-5413.189608] [PMID] [PMCID]
- Laitner MH, Erickson LC, Ortman E. Understanding the impact of sex and gender in osteoarthritis: Assessing research gaps and unmet needs. Journal of Women's Health. 2021; 30(5):634-41. [DOI:10.1089/jwh.2020.8828] [PMID]
- Stiebel M, Miller LE, Block JE. Post-traumatic knee osteoarthritis in the young patient: Therapeutic dilemmas and emerging technologies. Open Access Journal of Sports Medicine. 2014; 5:73-9. [PMID]
- Jørgensen KT, Pedersen BV, Nielsen NM, Hansen AV, Jacobsen S, Frisch M. Socio-demographic factors, reproductive history and risk of osteoarthritis in a cohort of 4.6 million Danish women and men. Osteoarthritis and Cartilage. 2011; 19(10):1176-82. [DOI:10.1016/j.joca.2011.07.009] [PMID]
- Cutti AG, Verni G, Migliore GL, Amoresano A, Raggi M. Reference values for gait temporal and loading symmetry of lower-limb amputees can help in refocusing rehabilitation targets. Journal of Neuroengineering and Rehabilitation. 2018; 15(Suppl 1):61. [DOI:10.1186/s12984-018-0403-x] [PMID] [PMCID]
- Karimi MT, Salami F, Esrafilian A, Heitzmann DWW, Alimusaj M, Putz C, et al. Sound side joint contact forces in below knee amputee gait with an ESAR prosthetic foot. Gait & Posture. 2017; 58:246-51. [DOI:10.1016/j.gaitpost.2017.08.007] [PMID]
- Ding Z, Jarvis HL, Bennett AN, Baker R, Bull AMJ. Higher knee contact forces might underlie increased osteoarthritis rates in high functioning amputees: A pilot study. Journal of Orthopaedic Research. 2021; 39(4):850-60. [DOI:10.1002/jor.24751] [PMID]
- Hsu H, Siwiec RM. Knee osteoarthritis. 2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. [PMID]
- Dahaghin S, Tehrani-Banihashemi SA, Faezi ST, Jamshidi AR, Davatchi F. Squatting, sitting on the floor, or cycling: Are life-long daily activities risk factors for clinical knee osteoarthritis? Stage III results of a community-based study. Arthritis and Rheumatism. 2009; 61(10):1337-42. [DOI:10.1002/art.24737] [PMID]
- Melzer I, Yekutiel M, Sukenik S. Comparative study of osteoarthritis of the contralateral knee joint of male amputees who do and do not play volleyball. The Journal of Rheumatology. 2001; 28(1):169-72. [Link]
Article type: Original Research Articles |
Subject:
epidemiological studies
Received: 2022/09/21 | Accepted: 2023/09/5 | Published: 2023/12/1
Received: 2022/09/21 | Accepted: 2023/09/5 | Published: 2023/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
