
988368
Tue, Jul 8, 2025

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 611-622 |
Back to browse issues page


Ethics code: IR-.ARUMS.REC.1399.045
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahmadboukani S, Fathi D, Bashirgonbadi S, Raisi L, Derakhshan M, Molaei B. The Relationship Between Health Literacy, Perceived Stress, Anxiety Sensitivity, and Self-care for COVID-19: The Mediating Role of Health Locus of Control. Iranian Rehabilitation Journal 2023; 21 (4) :611-622
URL: http://irj.uswr.ac.ir/article-1-1783-en.html
URL: http://irj.uswr.ac.ir/article-1-1783-en.html
Soliman Ahmadboukani1 

 , Davod Fathi1 , Sepideh Bashirgonbadi1 , Leila Raisi2 , Meraj Derakhshan3 , Behnam Molaei *4
, Davod Fathi1 , Sepideh Bashirgonbadi1 , Leila Raisi2 , Meraj Derakhshan3 , Behnam Molaei *4
, Davod Fathi1 , Sepideh Bashirgonbadi1 , Leila Raisi2 , Meraj Derakhshan3 , Behnam Molaei *4
1- Department of Counseling, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
2- Department of Midwifery, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran.
3- Department of Counseling, Bushehr Farhangian University, Bushehr, Iran.
4- Department of Psychiatry, Faculty of Medicine, Ardabil University of Medical Science, Ardabil, Iran.
2- Department of Midwifery, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran.
3- Department of Counseling, Bushehr Farhangian University, Bushehr, Iran.
4- Department of Psychiatry, Faculty of Medicine, Ardabil University of Medical Science, Ardabil, Iran.
Keywords: Perceived stress, Anxiety sensitivity, Self-care, Health literacy, Health locus of control, COVID-19
Full-Text [PDF 683 kb]
(722 Downloads)
| Abstract (HTML) (2459 Views)
Full-Text: (518 Views)
Introduction
Despite significant developments in disease control, infectious diseases are still major concerns for epidemiologists and public health professionals [1]. Following the environmental conditions and the re-emergence of these diseases, most countries do not have the capacity required for quick identification and timely response [2]. COVID-19 is a pandemic induced by a novel beta coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]). It started in China in late December 2019 and affected people worldwide within almost 4 months. Accordingly, on March 11, 2020, World Health Organization (WHO) declared COVID-19 to be a pandemic to redirect public attention to its importance. Currently, many think tanks in the world consider the COVID-19 pandemic to be the greatest public health, economic, and national policy challenge for many countries [3]. It seems that the critical challenge created by this pandemic is the health of human lives worldwide, which has imposed many problems and costs on countries [4]. Researchers have concluded that in addition to physical and therapeutic interventions, affected people need psychological interventions to reduce the psychological harm of this disease [5].
One of the psychological solutions to control and reduce the complications and costs caused by COVID-19 is to promote self-care behaviors. Self-care behaviors by the sick person or positive and specific attitudes towards himself and his illness are formed in a conscious and controlled way. Self-care behaviors refer to a set of spontaneous activities performed by the patient to understand their conditions and factors affecting their health [6]. These activities include choosing the right food, physical activity, receiving medicines, and following a healthy lifestyle [7]. The extent to which patients engage in self-care behaviors varies in different societies, and even though improving self-care behaviors is one of the effective solutions to control the disease and its complications, only a small number of adults perform self-care methods efficiently [8]. According to previous studies, encouraging healthcare officials and family members to perform self-care behaviors and control eating habits is effective and plays an essential role in controlling the complications caused by diseases [9]. For example, Pandit et al. showed that engaging in self-care behavior is effective in the occurrence of complications and disease recovery [10]. MacPherson et al. also showed that self-care can greatly reduce pain in patients [11]. However, given the low doctor-patient ratio and the high prevalence of COVID-19, paying attention to self-care is very rational and necessary.
Nevertheless, different factors may affect people’s self-care ability. For example, Siegel and Lopez showed a negative relationship between anxiety and non-adherence to treatment [12]. Harvie and Steel also showed that self-care greatly reduces the anxiety of the disease and helps the treatment process [13]. Anxiety is a part of modern human life; it is present in all people on average and is considered an adaptive response to environmental stimuli [14, 15]. An anxiety construct that has received extensive attention in anxiety disorder studies is anxiety sensitivity. Anxiety sensitivity is one of the critical mediating variables between stress and disease. Anxiety sensitivity refers to a stable tendency and desire to consider the physical, psychological, and social consequences of anxiety to be annoying and dangerous [16]. Anxiety sensitivity leads to bias in retrieving and processing information related to anxiety-inducing stimuli, paving the way for a person to suffer from mental disorders, including anxiety and panic [17]. Furthermore, studies on the relationship between stress and self-care in patients have reported conflicting results. They have shown that although anxiety reduces a person’s ability to take care of himself, having a certain degree of stress makes the person take more care of themselves and thus be less at risk of developing the disease [18].
The concept of perceived stress is derived from Lazarus’ and Folkman’s theory about the role of evaluation in the stress process, whereby interpreting an event as a stressful event imposes pressure on a person. Perceived stress is a person’s overall perception and interpretation of susceptibility to stress [19, 20]. Different people perceive and interpret the same stressor in different ways, and different factors can affect the formation of perceived stress and a person’s interpretation of the stress severity [21]. However, some researchers believe that due to their inherent concern, stressed people often tend to engage in self-care behaviors due to the fear of the consequences of inadequate self-care and may even avoid high-risk behaviors or engage in daily self-care without having any specific illness [18].
It is also expected that people need to have more advanced levels of health literacy to have adequate self-care [22]. Health literacy instrument for Iranian adults (HELIA) refers to cognitive and social skills that affect the motivation and ability of people to acquire, understand, and use information to improve and maintain their health. HELIA has two individual and social aspects, the individual aspect involves personal information, capacities, and potentials, and the social aspect involves culture, ethnicity, family-social influences, and economic status that can affect people’s health behaviors [23]. Although it is not yet known exactly how much health literacy affects health outcomes, a huge bulk of evidence indicates that many unfavorable health-related outcomes are the result of insufficient health literacy [24]. As a case in point, the effect of self-care on diseases spread by viruses was investigated and showed that self-care and compliance with the instructions given to people by healthcare workers can greatly contribute to prevent the spread of viral and contagious diseases [25]. Studies have demonstrated that self-care is associated with health literacy, and health literacy leads to higher levels of self-care in patients [26].
However, researchers assume that patients with higher levels of self-reliance and independence are likely to have weaker cooperation with healthcare providers and thus less motivation to engage in self-care behaviors [27]. This issue can be addressed through the concept of health locus of control (HLOC) because the perception of individual effectiveness and personal responsibility for well-being, in principle, is a moderating variable to increase the effectiveness of coping and adopting healthy behavioral styles [28]. HLOC is the extent to which people believe that they, significant others, or chance affect their health or illness [29]. The construct of HLOC was developed based on the social learning theory proposed by Rotter. This theory suggests that based on the history of their reinforcements, people learn to develop their general and specific expectations, and through the learning process, come to believe that certain consequences are the outcome of their actions (internal) or the outcome of other factors independent of themselves (external). Those who believe that they control their health or life events have an internal locus of control (ILOC), and conversely, those who feel that others or chance are responsible for what happens to their health have an external locus of control (ELOC). A review of the literature shows that individuals with an ILOC often tend to perform health-promoting behaviors compared to people who believe that chance or social factors are responsible for their health [30] and are also less prone to learned helplessness [31]. Researchers have shown that HLOC is associated with health-promoting behaviors. Thus, to promote health behaviors, one should focus more on people’s perceptions of the impact of internal factors and their abilities, as well as the influence of important people on the control of external factors and chance [32, 33].
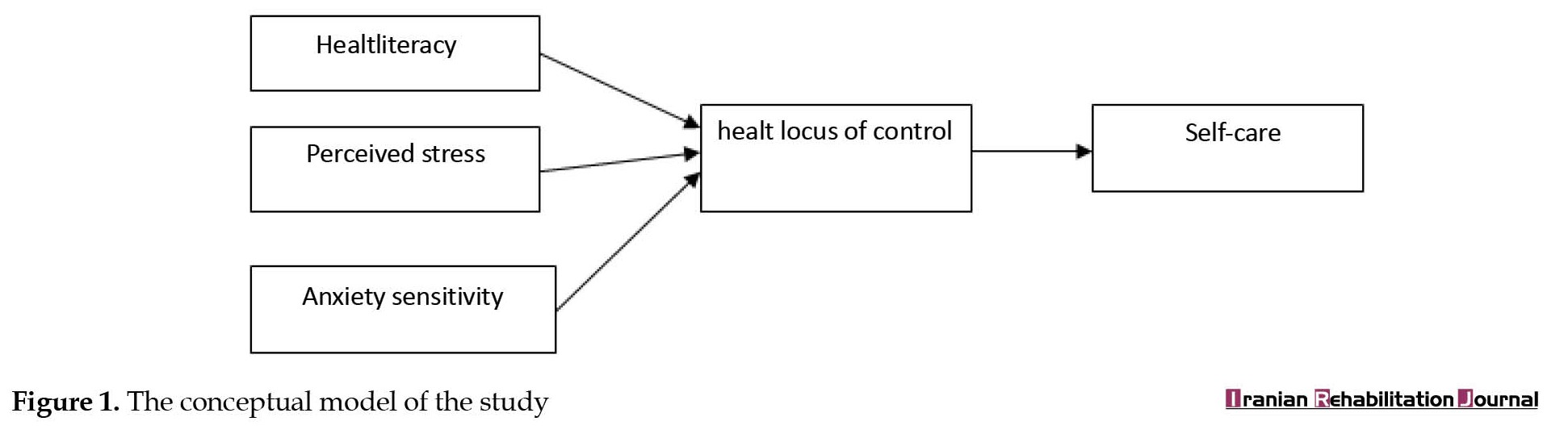
Accordingly, since the new coronavirus is spreading rapidly worldwide and many countries in the world have been affected by this virus, paying attention to the factors affecting self-care behaviors can be an effective step in managing this disease and reducing its complications. In the epidemiology of COVID-19, medical equipment and staff are not proportionate to the number of patients, and most of the treatment and prevention services are demoted to self-care behaviors. Thus, paying attention to self-care is essential as a crucial strategy to cope with COVID-19 and its risk factors to develop a model to identify and understand the mechanism of dealing with COVID-19. Therefore, the present study was conducted to specify whether HELIA, perceived stress scale (PSS), and anxiety sensitivity scale (ASS) are correlated with self-care for COVID-19, emphasizing the mediating role of HLOC components. Figure 1 shows the conceptual model of the study:
Materials and Methods
The present study was an applied study in terms of its objectives and was conducted using a correlational and path analysis method. The research population included households living in Ardabil City. The participants included 300 persons who were selected via the convenience sampling method. According to Kline, the number of participants in structural equation modeling studies should be equal to or >200 [33].
Before administering the instruments to the respondents, some instructions were provided to them about the objectives of the study and the importance of COVID-19. After obtaining informed consent from the respondents, the link of the questionnaires was provided to them and they were asked to complete them online.
Instruments
HELIA
Montazeri et al. [34] constructed a health literacy HELIA to measure health literacy among Iranian urban adults aged 18 to 65 years. The instrument has some features, such as a small number of items, ease of administration, coverage of all health literacy aspects (access to information, reading skills, understanding, appraisal, and decision-making), and generality. Thus, this tool has not been developed for a specific class, occupation, education, or age group and can be administered to different demographic groups [34]. Panahi et al [35] assessed the construct validity and reliability of the instrument by administering it to a sample of students. The confirmatory factor analysis showed that the instrument has an acceptable goodness of fit [35].
PSS
Cohen et al. designed the perceived stress scale PSS and it has 14 five-point Likert items. The scale has two subscales. Cohen et al. calculated its correlation coefficient with semiotic measures from 0.52 to 0.76 to assess the criterion validity of the scale [35]. In Iran, Mohammadi-Yeganeh et al. confirmed the reliability of the tool using internal consistency and reported its Cronbach’s α as 0.74 [36].
ASS
Taylor and Cox [37]. developed the ASS to assess the degree of fear of anxiety symptoms and consequences. This 36-item self-report scale assesses 6 specific features of anxiety sensitivity, including fears of publicly observable anxiety reactions (8 items), cardiovascular (6 items), respiratory (7 items), gastrointestinal (4 items) dissociative/neurological (6 items), and cognitive dyscontrol symptoms (5 items). The items are rated on a five-point Likert scale. Taylor and Cox have reported alpha coefficients from 0.83 to 0.94, confirming the internal consistency of the scale [37]. In Iran, the coefficients measured for the scale and its subscales varied from 0.82 to 0.93, confirming the internal consistency of the scale [38].
Self-care questionnaire
The self-care questionnaire contains 17 items rated on a five-point scale (1=never to 5=always). The items were developed through qualitative interviews and a review of the literature. The face and structure validity of the tool has been confirmed, and the assessment of its content validity showed that the content of the tool is fully consistent with the research objectives. The results of the factor analysis confirmed the validity of the tool. The tool’s reliability was evaluated by Cronbach’s α, with the corresponding values of 0.71 and 0.83 for personal care and social responsibility factors, respectively.
Multidimensional health locus of control (MHLC) scale
Wallston et al. [39]. developed a MHLC. It has three scales (A, B, C). Forms A and B measure HLOC. Each of these two equivalent forms includes three subscales each with 6 items, internal and external, significant others, and external, chance. In the past 25 years, forms A and B have been used in many studies. Form C was developed for use in disease conditions and can be used instead of form A or B when people with a disease are being studied. Like forms A and B, form C also contains 18 items, but the subscale of significant others has been replaced by two subscales of doctors and significant others, each with 3 items [39]. The construct validity of the instrument in Iran was confirmed through confirmatory factor analysis and its internal consistency was established with Cronbach’s α of 0.70 [32]. The α value for this scale was 0.83.
Statistical analysis
The Mean±SD was utilized in the present study to verify the descriptive characteristics of the variables. In addition, path analysis was used to evaluate the mediating roles of the variables. SPSS software, version 25 and AMOS software, version 24 were used to analyze the collected data.
Results
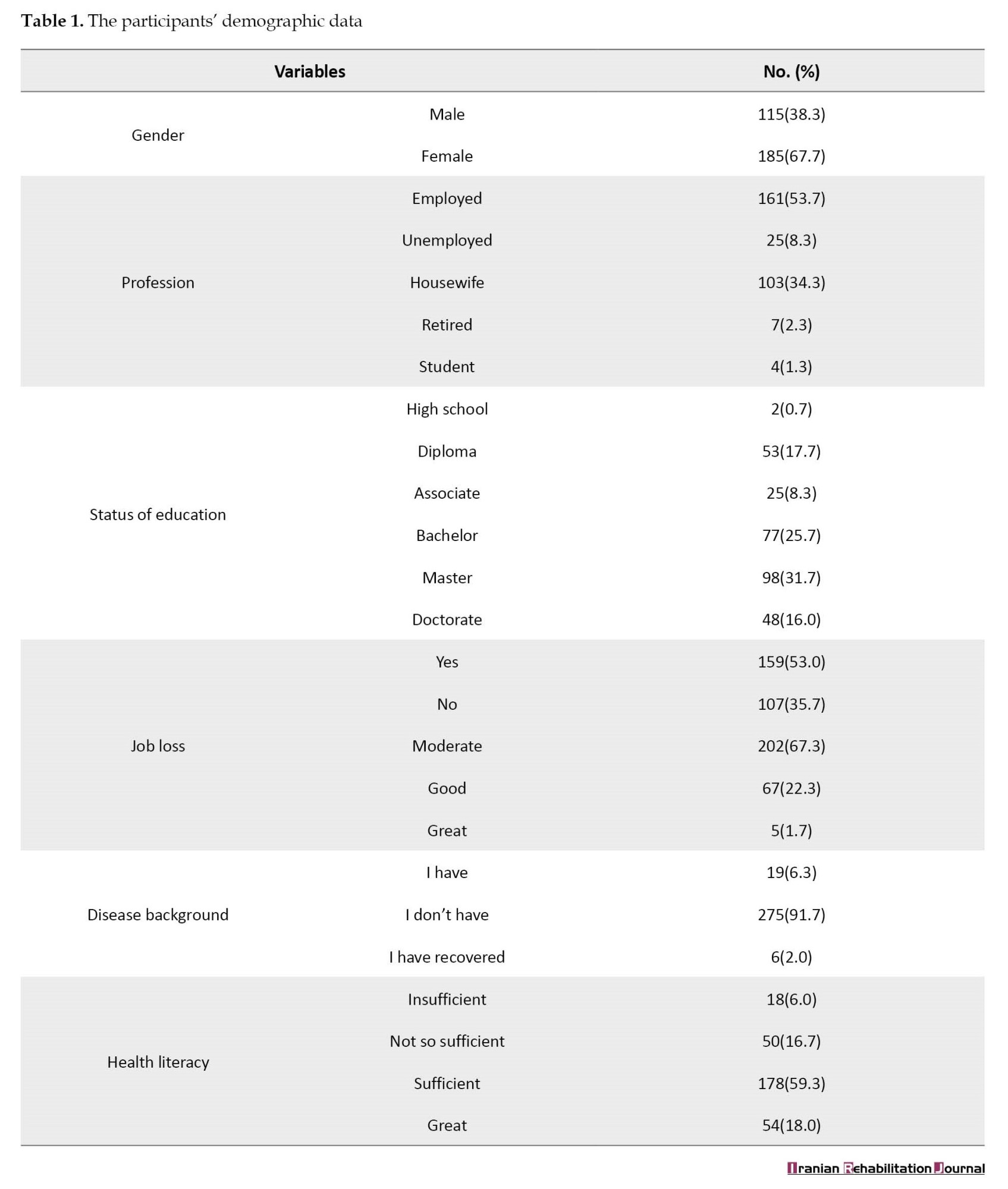
The results showed that 115 participants (38.3%) were men and 185 participants (61.7%) were women. Of these, 152 persons (50.7%) were married and 148 persons (49.3%) were single. In addition, 31% of participants had postgraduate education. The household income of 67.3% of the participants was at the average level. Furthermore, the participants’ average age was 33.37±9.09 years. The data also showed that the average score of health literacy among the participants was 73.76 out of 100. Thus, 73% of the participants had adequate health literacy and only 26% of them had a low level of health literacy (Table 1).
To check the simple relationships between the research variables, the correlations between the variables were calculated. The results showed that the correlations between the variables were significant in most cases. Thus, it was possible to assess the model. Table 2 presents the correlation matrix for the research variables.
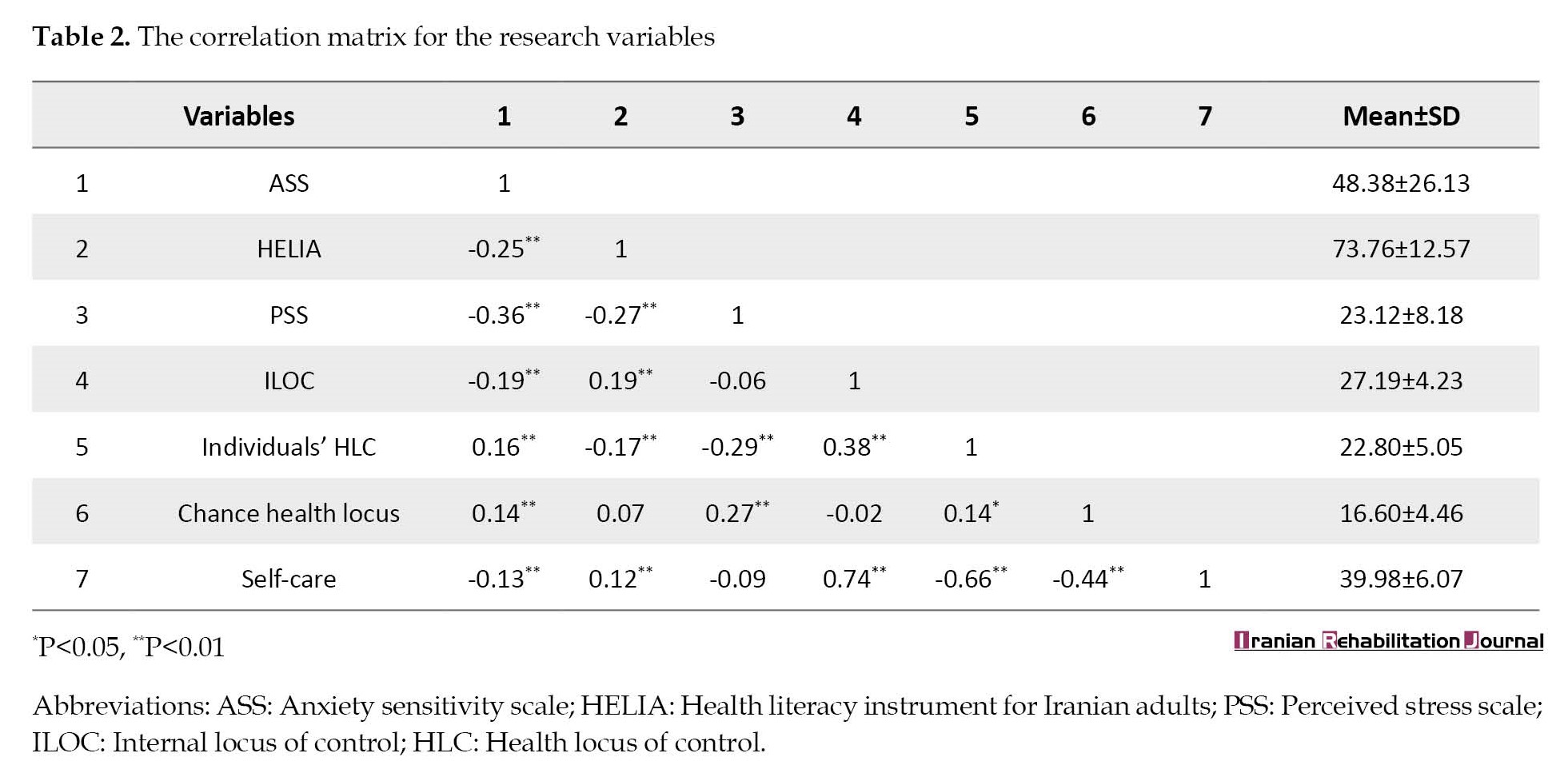
As presented in Table 2, ILOC and self-care have the highest correlation coefficient. To test the proposed model, after examining the assumptions of path modeling, i.e. the normality of the variables and the linearity of the relationship between the variables, the model was assessed. Table 2 presents the fit indices of the model.
Since the proposed model does not fit the data, the model should be modified by correlating the errors, adding paths, or removing non-significant paths for the optimal fit of the model. The data in Table 3 show that root means square error of approximation (RMSEA), comparative fit index (CFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), and normalized fit index (NFI) was equal to 0.050, 0.997, 0.990, 0.983, and 0.995, indicating the optimal fit of the conceptual model.
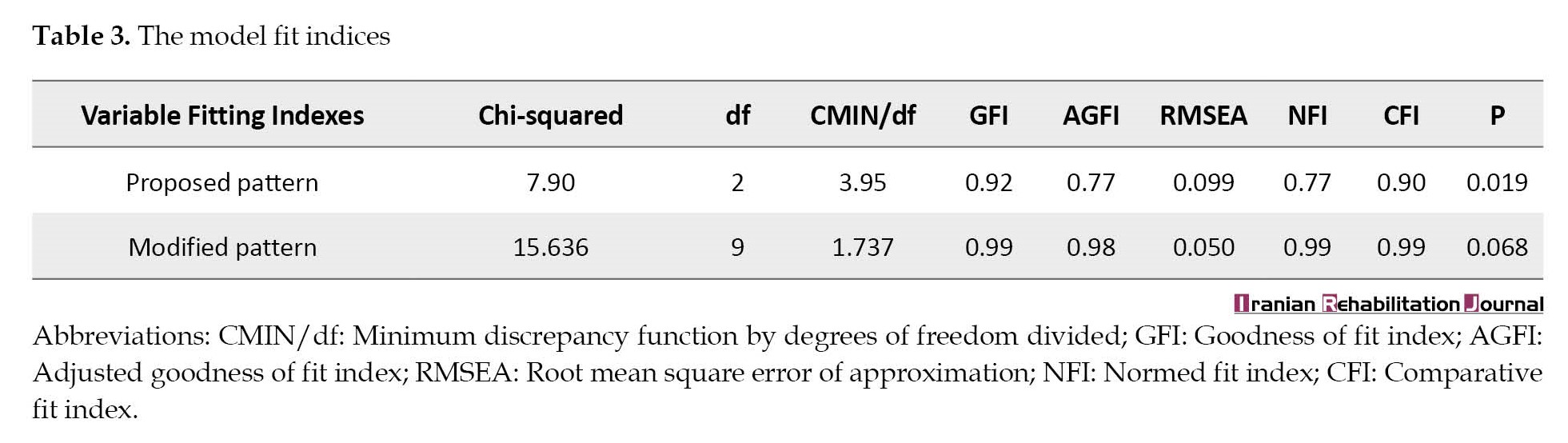
Table 3 also presents the standard coefficients of direct paths:
As illustrated in Table 4, the greatest coefficient of a direct effect on self-care is related to the ILOC and the lowest coefficient of the direct effect on the ILOC is related to anxiety sensitivity.
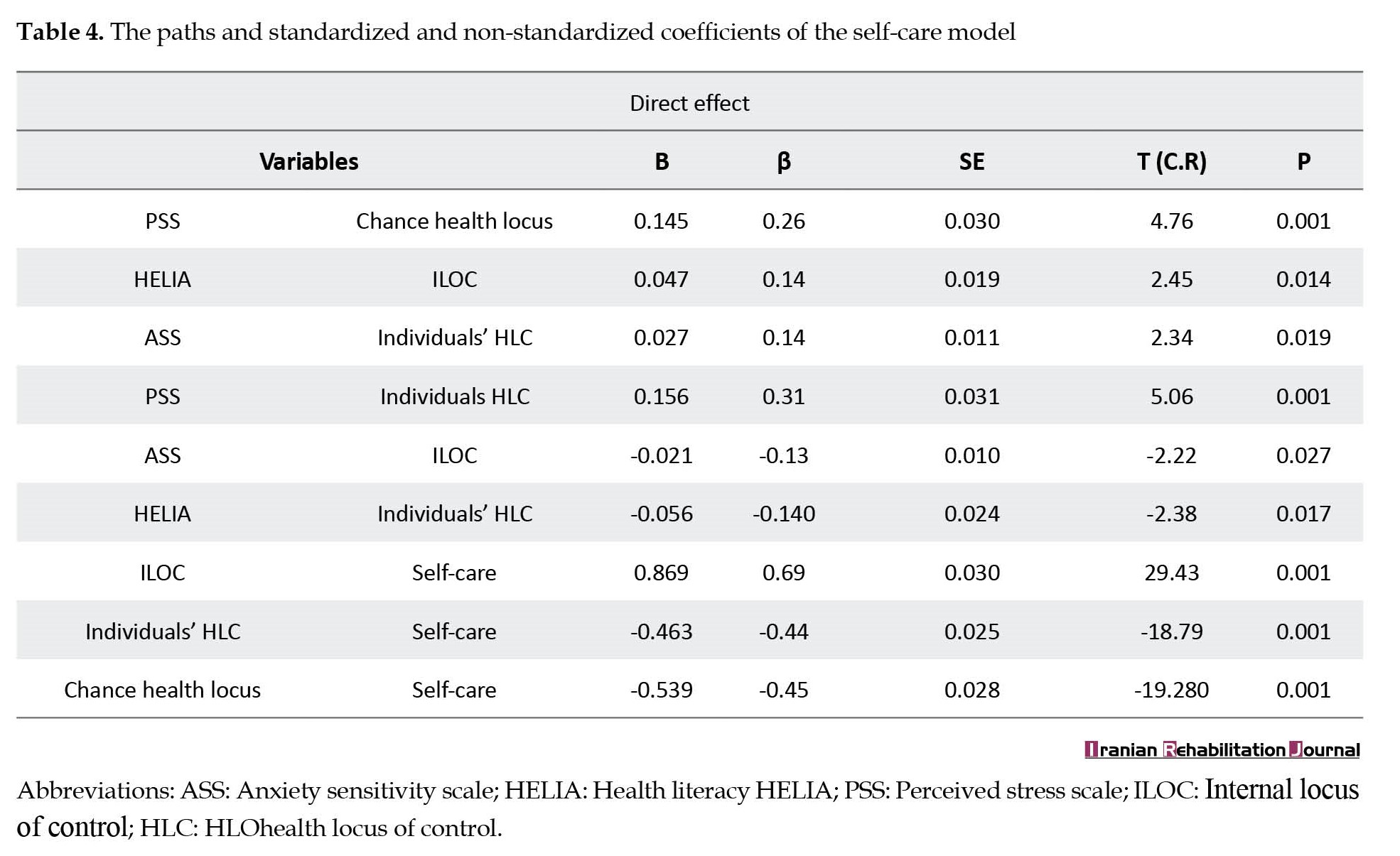
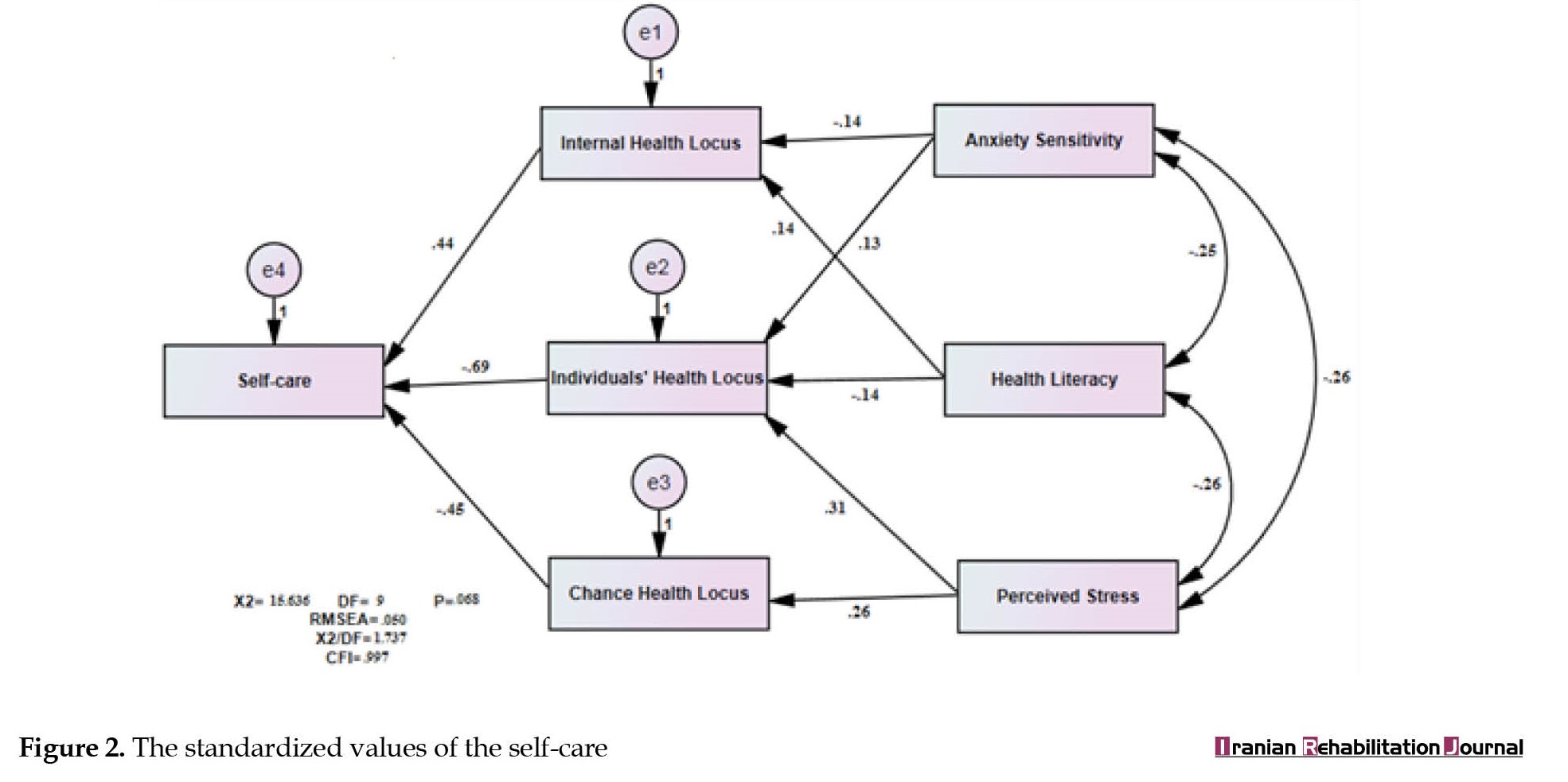
Figure 2 shows the final model and its standardized coefficients:
 The mediation paths were investigated using the bootstrap method, as shown in Table 5.
The mediation paths were investigated using the bootstrap method, as shown in Table 5.
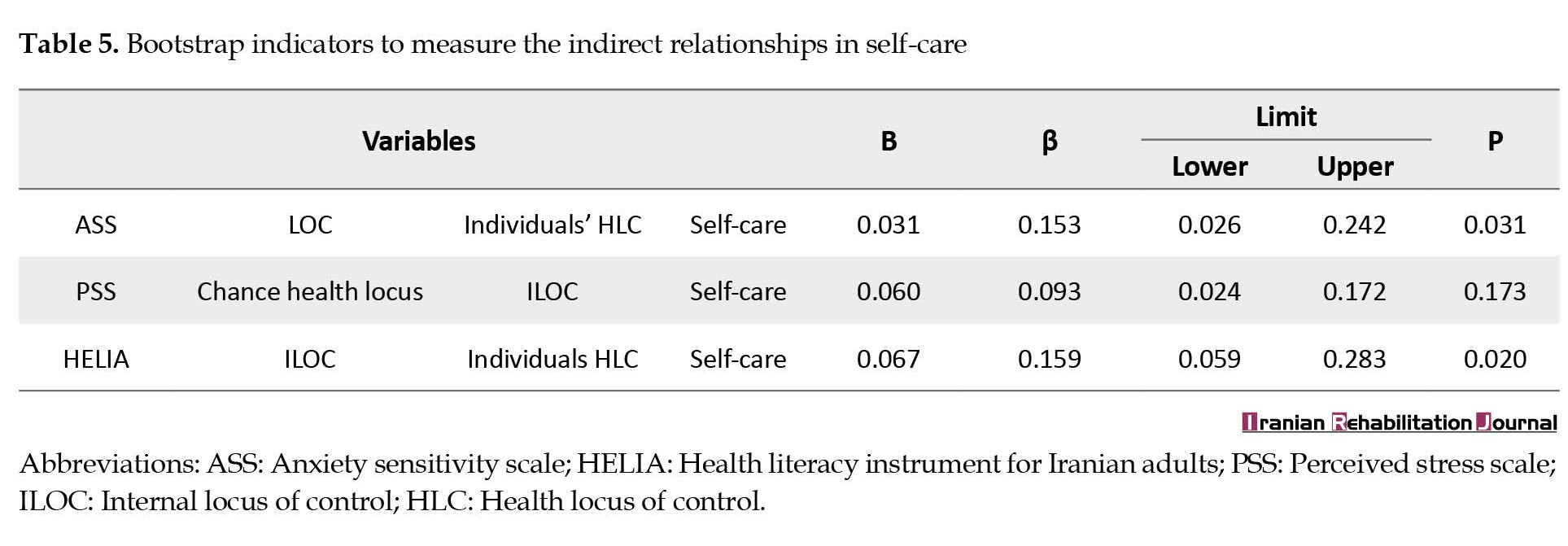
As shown in the Table 5, the upper and lower boundaries of the ILOC and the individual HLOC in the relationship between anxiety sensitivity and self-care do not include zero. Thus, these variables are mediators between anxiety sensitivity and self-care. Besides, the upper and lower boundaries of the ILOC and the individual HLOC in the relationship between health literacy and self-care do not include zero, indicating that the ILOC and the individual HLOC act as the mediating variables in the relationship between the two variables. In addition, the lower and upper boundaries of the health locus of chance and the ILOC in the relationship between perceived stress and self-care include zero, indicating that the health locus of chance and the ILOC do not play a mediating role in the relationship between perceived stress and self-care.
Discussion
The present study was conducted to discover whether health literacy, perceived stress, and anxiety sensitivity are correlated with self-care for COVID-19, focusing on the mediating role of HLOC in families of Ardabil City. The results showed that anxiety sensitivity has a negative relationship with ILOC and a positive and significant relationship with ELOC. Similarly, Cvengros et al. found that people with a high ILOC have less anxiety, while people with an ELOC experience more anxiety and are more likely to develop mental illness and psychological distress [40]. Anxiety is associated with the fundamental belief about the locus of control. Thus, the anxious person feels that they have no control over life situations, including health. Besides, ELOC is associated with the belief that situations are beyond the individual’s control, while low anxiety sensitivity is related to the belief in the ability to control situations. Accordingly, it can be argued that anxiety sensitivity adversely affects the center of internal health control and belief in one’s role in disease control and has a positive and direct effect on the ELOC.
The data analysis also revealed that health literacy has a positive correlation with ILOC and has a negative and significant relationship with ELOC. Zeidner [41] showed that individuals who have scored higher on ILOC have a greater tendency to engage in preventive and health-promoting behaviors, and are more likely to engage in preventive behaviors, such as following healthy eating habits and performing medical examinations, compared to people with an ELOC. Higher levels of literacy and awareness are correlated with individual sensitivity to preventing harm and finding individual solutions. People with a high level of health literacy are aware of the mechanism of diseases and health-promoting strategies. Relying on individual control, they take preventive measures to promote health and encourage others to accept personal responsibility for maintaining health. However, low literacy and unawareness of personal control strategies are associated with less self-efficacy and sensitivity toward self-care behaviors. Accordingly, it can be argued that the ILOC is associated with improving health literacy, and health literacy has an inverse relationship with attention to external control.
The study’s results showed that perceived stress has a positive and direct impact on ELOC and the chance locus of control, implying that since perceived stress is a person’s overall perception and interpretation of being susceptible to stress [19], people who experience higher levels of stress imagine themselves exposed to events that only the help of others can protect them from harm. Moreover, perceived stress refers to a psychological state in which an individual perceives their physical and psychological well-being as threatened. This perceived threat is induced by COVID-19, and the high level of stress has a positive and significant relationship with attributing the disease to chance and others. Indeed, developing stress depends on individual impressions and perceptions of events and situations. A situation may be perceived as safe for one individual and as a threat to another individual [42]. Thus, people who are stressed cannot regain their responsibility and control [43] and attribute the locus of control over their health related to illness to others and chance.
The current study indicated that ILOC has a positive and direct relationship with self-care for COVID-19, and ELOC and chance have a negative and direct relationship with self-care for COVID-19. Although no study has addressed the relationship between these variables in the case of COVID-19, previous studies have supported the relationship between ILOC and self-care [28, 31, 32]. This is to argue that HLOC refers to people’s perceptions of how to control the environment. The locus of control is a system of beliefs that evaluates their successes and failures according to their abilities and weaknesses [30]. Those with ELOC believe that the outcomes of their lives are controlled by external forces, such as doctors, luck, and fate. In contrast, people with an ILOC believe that certain outcomes in life are the result of their behaviors and actions, and their health is directly affected by their actions and behaviors [30]. Consequently, people with ILOC take more care of themselves.
The data in this study indicated that HLOC plays a mediating role in the relationships between the research variables. Accordingly, health literacy and anxiety sensitivity are related to self-care for COVID-19 through the mediating role of the ILOC and individual locus of control. Since anxiety sensitivity means expecting an outcome and reflects personal differences in the tendency to experience fear [16], when a person believes that their behaviors and beliefs can affect COVID-19, they are more likely to engage in self-care behaviors. Hence, ILOC causes anxiety sensitivity to be directed in the right direction leading to self-care behaviors. On the other hand, ELOC means that the people around the person, the health-treatment system, and even the government are responsible for maintaining health. This belief has a significant impact on the relationship between anxiety sensitivity and self-care because believing in the importance and priority of the role of others in controlling COVID-19 diminishes the sense of internal responsibility for caring for COVID-19. Anxiety sensitivity about the locus of control and the locus of control as an intermediary belief is related to self-care. Therefore, it seems logical that HLOC plays a mediating role in the relationship between anxiety sensitivity and caring for COVID-19.
Health literacy refers to cognitive and social skills that motivate and enable people to acquire, understand, and use information to improve and maintain their health in both individual and social domains [25]. Thus, it can be argued that ILOC, or a person’s belief that they or others are effective in promoting health and that this matter is not dependent on chance and fortune, can improve their cognitive skills in health promotion and self-care behaviors. The stronger the people’s ILOC and their self-belief about their influence on their health, the more they are likely to engage in self-care behaviors. Moreover, the tendency towards ELOC decreases self-care behaviors because individuals with an ILOC have more control over their health, hygiene, and quality and tend to perform behaviors that help them diagnose and control diseases. These people also experience fewer psychological problems, including anxiety [40].
The results of this study showed that HLOC does not play a mediating role in the relationship between perceived stress and self-care. Previous studies have reported inconsistent results in this regard. Some researchers believe that stress causes people to act more actively to protect their health and perform self-care behaviors, regardless of factors such as internal or ELOC, and they are even more aware of avoiding risky behaviors [17]. Sometimes stress causes a decline in a person’s efficiency and reduces their self-care ability since different people perceive the same stressful factor in different ways [18]. Thus, it cannot be expected that HLOC can mediate between perceived stress and caring for COVID-19.
Conclusion
The present study showed that health literacy, anxiety sensitivity, and perceived stress are related to self-care for COVID-19, mediated by (internal and individual) HLOC. These results are significant because infectious diseases, such as COVID-19 require special attention due to their spread, and every person with self-care skills can prevent the risk of developing these diseases and in the case of infection, such skills will help them regain their health. Identifying the factors affecting self-care in COVID-19 can contribute to developing interventions to improve self-care and thus prevent the spread of the disease. In addition, the results of this study can have some implications for other infectious diseases as well. However, this research project was conducted with some limitations. Since this study was conducted on households in Ardabil City, caution should be taken in generalizing its results to other populations and groups. Furthermore, the data in this study were collected through self-report instruments. Thus, the participants may have difficulty expressing their emotions and thoughts. Accordingly, other data collection instruments, such as qualitative designs or interviews should be used in similar studies to obtain more reliable results. Nevertheless, following the results of the present study, interventional training programs can be implemented to improve the ILOC in people during the outbreak of COVID-19 to reduce anxiety and increase self-care in people. Moreover, this study can be replicated on other chronic diseases, including diabetes and multiple sclerosis (MS), to clarify the role of HLOC.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Ardabil University of Medical Sciences (Code: IR.ARUMS.REC.1399.045).
Funding
This article is a part of the research project (Code: IR.ARUMS.REC.1399.045) and financially supported by the Ardabil University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
In the end, all the researchers of this study wish to thank the Esteemed Vice Chancellor of Ardabil University of Medical Sciences and all other staff for their cooperation in approving and financially supporting this study, as well as all the families participating in this study.
Reference
Despite significant developments in disease control, infectious diseases are still major concerns for epidemiologists and public health professionals [1]. Following the environmental conditions and the re-emergence of these diseases, most countries do not have the capacity required for quick identification and timely response [2]. COVID-19 is a pandemic induced by a novel beta coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]). It started in China in late December 2019 and affected people worldwide within almost 4 months. Accordingly, on March 11, 2020, World Health Organization (WHO) declared COVID-19 to be a pandemic to redirect public attention to its importance. Currently, many think tanks in the world consider the COVID-19 pandemic to be the greatest public health, economic, and national policy challenge for many countries [3]. It seems that the critical challenge created by this pandemic is the health of human lives worldwide, which has imposed many problems and costs on countries [4]. Researchers have concluded that in addition to physical and therapeutic interventions, affected people need psychological interventions to reduce the psychological harm of this disease [5].
One of the psychological solutions to control and reduce the complications and costs caused by COVID-19 is to promote self-care behaviors. Self-care behaviors by the sick person or positive and specific attitudes towards himself and his illness are formed in a conscious and controlled way. Self-care behaviors refer to a set of spontaneous activities performed by the patient to understand their conditions and factors affecting their health [6]. These activities include choosing the right food, physical activity, receiving medicines, and following a healthy lifestyle [7]. The extent to which patients engage in self-care behaviors varies in different societies, and even though improving self-care behaviors is one of the effective solutions to control the disease and its complications, only a small number of adults perform self-care methods efficiently [8]. According to previous studies, encouraging healthcare officials and family members to perform self-care behaviors and control eating habits is effective and plays an essential role in controlling the complications caused by diseases [9]. For example, Pandit et al. showed that engaging in self-care behavior is effective in the occurrence of complications and disease recovery [10]. MacPherson et al. also showed that self-care can greatly reduce pain in patients [11]. However, given the low doctor-patient ratio and the high prevalence of COVID-19, paying attention to self-care is very rational and necessary.
Nevertheless, different factors may affect people’s self-care ability. For example, Siegel and Lopez showed a negative relationship between anxiety and non-adherence to treatment [12]. Harvie and Steel also showed that self-care greatly reduces the anxiety of the disease and helps the treatment process [13]. Anxiety is a part of modern human life; it is present in all people on average and is considered an adaptive response to environmental stimuli [14, 15]. An anxiety construct that has received extensive attention in anxiety disorder studies is anxiety sensitivity. Anxiety sensitivity is one of the critical mediating variables between stress and disease. Anxiety sensitivity refers to a stable tendency and desire to consider the physical, psychological, and social consequences of anxiety to be annoying and dangerous [16]. Anxiety sensitivity leads to bias in retrieving and processing information related to anxiety-inducing stimuli, paving the way for a person to suffer from mental disorders, including anxiety and panic [17]. Furthermore, studies on the relationship between stress and self-care in patients have reported conflicting results. They have shown that although anxiety reduces a person’s ability to take care of himself, having a certain degree of stress makes the person take more care of themselves and thus be less at risk of developing the disease [18].
The concept of perceived stress is derived from Lazarus’ and Folkman’s theory about the role of evaluation in the stress process, whereby interpreting an event as a stressful event imposes pressure on a person. Perceived stress is a person’s overall perception and interpretation of susceptibility to stress [19, 20]. Different people perceive and interpret the same stressor in different ways, and different factors can affect the formation of perceived stress and a person’s interpretation of the stress severity [21]. However, some researchers believe that due to their inherent concern, stressed people often tend to engage in self-care behaviors due to the fear of the consequences of inadequate self-care and may even avoid high-risk behaviors or engage in daily self-care without having any specific illness [18].
It is also expected that people need to have more advanced levels of health literacy to have adequate self-care [22]. Health literacy instrument for Iranian adults (HELIA) refers to cognitive and social skills that affect the motivation and ability of people to acquire, understand, and use information to improve and maintain their health. HELIA has two individual and social aspects, the individual aspect involves personal information, capacities, and potentials, and the social aspect involves culture, ethnicity, family-social influences, and economic status that can affect people’s health behaviors [23]. Although it is not yet known exactly how much health literacy affects health outcomes, a huge bulk of evidence indicates that many unfavorable health-related outcomes are the result of insufficient health literacy [24]. As a case in point, the effect of self-care on diseases spread by viruses was investigated and showed that self-care and compliance with the instructions given to people by healthcare workers can greatly contribute to prevent the spread of viral and contagious diseases [25]. Studies have demonstrated that self-care is associated with health literacy, and health literacy leads to higher levels of self-care in patients [26].
However, researchers assume that patients with higher levels of self-reliance and independence are likely to have weaker cooperation with healthcare providers and thus less motivation to engage in self-care behaviors [27]. This issue can be addressed through the concept of health locus of control (HLOC) because the perception of individual effectiveness and personal responsibility for well-being, in principle, is a moderating variable to increase the effectiveness of coping and adopting healthy behavioral styles [28]. HLOC is the extent to which people believe that they, significant others, or chance affect their health or illness [29]. The construct of HLOC was developed based on the social learning theory proposed by Rotter. This theory suggests that based on the history of their reinforcements, people learn to develop their general and specific expectations, and through the learning process, come to believe that certain consequences are the outcome of their actions (internal) or the outcome of other factors independent of themselves (external). Those who believe that they control their health or life events have an internal locus of control (ILOC), and conversely, those who feel that others or chance are responsible for what happens to their health have an external locus of control (ELOC). A review of the literature shows that individuals with an ILOC often tend to perform health-promoting behaviors compared to people who believe that chance or social factors are responsible for their health [30] and are also less prone to learned helplessness [31]. Researchers have shown that HLOC is associated with health-promoting behaviors. Thus, to promote health behaviors, one should focus more on people’s perceptions of the impact of internal factors and their abilities, as well as the influence of important people on the control of external factors and chance [32, 33].
Accordingly, since the new coronavirus is spreading rapidly worldwide and many countries in the world have been affected by this virus, paying attention to the factors affecting self-care behaviors can be an effective step in managing this disease and reducing its complications. In the epidemiology of COVID-19, medical equipment and staff are not proportionate to the number of patients, and most of the treatment and prevention services are demoted to self-care behaviors. Thus, paying attention to self-care is essential as a crucial strategy to cope with COVID-19 and its risk factors to develop a model to identify and understand the mechanism of dealing with COVID-19. Therefore, the present study was conducted to specify whether HELIA, perceived stress scale (PSS), and anxiety sensitivity scale (ASS) are correlated with self-care for COVID-19, emphasizing the mediating role of HLOC components. Figure 1 shows the conceptual model of the study:
Materials and Methods
The present study was an applied study in terms of its objectives and was conducted using a correlational and path analysis method. The research population included households living in Ardabil City. The participants included 300 persons who were selected via the convenience sampling method. According to Kline, the number of participants in structural equation modeling studies should be equal to or >200 [33].
Before administering the instruments to the respondents, some instructions were provided to them about the objectives of the study and the importance of COVID-19. After obtaining informed consent from the respondents, the link of the questionnaires was provided to them and they were asked to complete them online.
Instruments
HELIA
Montazeri et al. [34] constructed a health literacy HELIA to measure health literacy among Iranian urban adults aged 18 to 65 years. The instrument has some features, such as a small number of items, ease of administration, coverage of all health literacy aspects (access to information, reading skills, understanding, appraisal, and decision-making), and generality. Thus, this tool has not been developed for a specific class, occupation, education, or age group and can be administered to different demographic groups [34]. Panahi et al [35] assessed the construct validity and reliability of the instrument by administering it to a sample of students. The confirmatory factor analysis showed that the instrument has an acceptable goodness of fit [35].
PSS
Cohen et al. designed the perceived stress scale PSS and it has 14 five-point Likert items. The scale has two subscales. Cohen et al. calculated its correlation coefficient with semiotic measures from 0.52 to 0.76 to assess the criterion validity of the scale [35]. In Iran, Mohammadi-Yeganeh et al. confirmed the reliability of the tool using internal consistency and reported its Cronbach’s α as 0.74 [36].
ASS
Taylor and Cox [37]. developed the ASS to assess the degree of fear of anxiety symptoms and consequences. This 36-item self-report scale assesses 6 specific features of anxiety sensitivity, including fears of publicly observable anxiety reactions (8 items), cardiovascular (6 items), respiratory (7 items), gastrointestinal (4 items) dissociative/neurological (6 items), and cognitive dyscontrol symptoms (5 items). The items are rated on a five-point Likert scale. Taylor and Cox have reported alpha coefficients from 0.83 to 0.94, confirming the internal consistency of the scale [37]. In Iran, the coefficients measured for the scale and its subscales varied from 0.82 to 0.93, confirming the internal consistency of the scale [38].
Self-care questionnaire
The self-care questionnaire contains 17 items rated on a five-point scale (1=never to 5=always). The items were developed through qualitative interviews and a review of the literature. The face and structure validity of the tool has been confirmed, and the assessment of its content validity showed that the content of the tool is fully consistent with the research objectives. The results of the factor analysis confirmed the validity of the tool. The tool’s reliability was evaluated by Cronbach’s α, with the corresponding values of 0.71 and 0.83 for personal care and social responsibility factors, respectively.
Multidimensional health locus of control (MHLC) scale
Wallston et al. [39]. developed a MHLC. It has three scales (A, B, C). Forms A and B measure HLOC. Each of these two equivalent forms includes three subscales each with 6 items, internal and external, significant others, and external, chance. In the past 25 years, forms A and B have been used in many studies. Form C was developed for use in disease conditions and can be used instead of form A or B when people with a disease are being studied. Like forms A and B, form C also contains 18 items, but the subscale of significant others has been replaced by two subscales of doctors and significant others, each with 3 items [39]. The construct validity of the instrument in Iran was confirmed through confirmatory factor analysis and its internal consistency was established with Cronbach’s α of 0.70 [32]. The α value for this scale was 0.83.
Statistical analysis
The Mean±SD was utilized in the present study to verify the descriptive characteristics of the variables. In addition, path analysis was used to evaluate the mediating roles of the variables. SPSS software, version 25 and AMOS software, version 24 were used to analyze the collected data.
Results
The results showed that 115 participants (38.3%) were men and 185 participants (61.7%) were women. Of these, 152 persons (50.7%) were married and 148 persons (49.3%) were single. In addition, 31% of participants had postgraduate education. The household income of 67.3% of the participants was at the average level. Furthermore, the participants’ average age was 33.37±9.09 years. The data also showed that the average score of health literacy among the participants was 73.76 out of 100. Thus, 73% of the participants had adequate health literacy and only 26% of them had a low level of health literacy (Table 1).
To check the simple relationships between the research variables, the correlations between the variables were calculated. The results showed that the correlations between the variables were significant in most cases. Thus, it was possible to assess the model. Table 2 presents the correlation matrix for the research variables.
As presented in Table 2, ILOC and self-care have the highest correlation coefficient. To test the proposed model, after examining the assumptions of path modeling, i.e. the normality of the variables and the linearity of the relationship between the variables, the model was assessed. Table 2 presents the fit indices of the model.
Since the proposed model does not fit the data, the model should be modified by correlating the errors, adding paths, or removing non-significant paths for the optimal fit of the model. The data in Table 3 show that root means square error of approximation (RMSEA), comparative fit index (CFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), and normalized fit index (NFI) was equal to 0.050, 0.997, 0.990, 0.983, and 0.995, indicating the optimal fit of the conceptual model.
Table 3 also presents the standard coefficients of direct paths:
As illustrated in Table 4, the greatest coefficient of a direct effect on self-care is related to the ILOC and the lowest coefficient of the direct effect on the ILOC is related to anxiety sensitivity.
Figure 2 shows the final model and its standardized coefficients:
As shown in the Table 5, the upper and lower boundaries of the ILOC and the individual HLOC in the relationship between anxiety sensitivity and self-care do not include zero. Thus, these variables are mediators between anxiety sensitivity and self-care. Besides, the upper and lower boundaries of the ILOC and the individual HLOC in the relationship between health literacy and self-care do not include zero, indicating that the ILOC and the individual HLOC act as the mediating variables in the relationship between the two variables. In addition, the lower and upper boundaries of the health locus of chance and the ILOC in the relationship between perceived stress and self-care include zero, indicating that the health locus of chance and the ILOC do not play a mediating role in the relationship between perceived stress and self-care.
Discussion
The present study was conducted to discover whether health literacy, perceived stress, and anxiety sensitivity are correlated with self-care for COVID-19, focusing on the mediating role of HLOC in families of Ardabil City. The results showed that anxiety sensitivity has a negative relationship with ILOC and a positive and significant relationship with ELOC. Similarly, Cvengros et al. found that people with a high ILOC have less anxiety, while people with an ELOC experience more anxiety and are more likely to develop mental illness and psychological distress [40]. Anxiety is associated with the fundamental belief about the locus of control. Thus, the anxious person feels that they have no control over life situations, including health. Besides, ELOC is associated with the belief that situations are beyond the individual’s control, while low anxiety sensitivity is related to the belief in the ability to control situations. Accordingly, it can be argued that anxiety sensitivity adversely affects the center of internal health control and belief in one’s role in disease control and has a positive and direct effect on the ELOC.
The data analysis also revealed that health literacy has a positive correlation with ILOC and has a negative and significant relationship with ELOC. Zeidner [41] showed that individuals who have scored higher on ILOC have a greater tendency to engage in preventive and health-promoting behaviors, and are more likely to engage in preventive behaviors, such as following healthy eating habits and performing medical examinations, compared to people with an ELOC. Higher levels of literacy and awareness are correlated with individual sensitivity to preventing harm and finding individual solutions. People with a high level of health literacy are aware of the mechanism of diseases and health-promoting strategies. Relying on individual control, they take preventive measures to promote health and encourage others to accept personal responsibility for maintaining health. However, low literacy and unawareness of personal control strategies are associated with less self-efficacy and sensitivity toward self-care behaviors. Accordingly, it can be argued that the ILOC is associated with improving health literacy, and health literacy has an inverse relationship with attention to external control.
The study’s results showed that perceived stress has a positive and direct impact on ELOC and the chance locus of control, implying that since perceived stress is a person’s overall perception and interpretation of being susceptible to stress [19], people who experience higher levels of stress imagine themselves exposed to events that only the help of others can protect them from harm. Moreover, perceived stress refers to a psychological state in which an individual perceives their physical and psychological well-being as threatened. This perceived threat is induced by COVID-19, and the high level of stress has a positive and significant relationship with attributing the disease to chance and others. Indeed, developing stress depends on individual impressions and perceptions of events and situations. A situation may be perceived as safe for one individual and as a threat to another individual [42]. Thus, people who are stressed cannot regain their responsibility and control [43] and attribute the locus of control over their health related to illness to others and chance.
The current study indicated that ILOC has a positive and direct relationship with self-care for COVID-19, and ELOC and chance have a negative and direct relationship with self-care for COVID-19. Although no study has addressed the relationship between these variables in the case of COVID-19, previous studies have supported the relationship between ILOC and self-care [28, 31, 32]. This is to argue that HLOC refers to people’s perceptions of how to control the environment. The locus of control is a system of beliefs that evaluates their successes and failures according to their abilities and weaknesses [30]. Those with ELOC believe that the outcomes of their lives are controlled by external forces, such as doctors, luck, and fate. In contrast, people with an ILOC believe that certain outcomes in life are the result of their behaviors and actions, and their health is directly affected by their actions and behaviors [30]. Consequently, people with ILOC take more care of themselves.
The data in this study indicated that HLOC plays a mediating role in the relationships between the research variables. Accordingly, health literacy and anxiety sensitivity are related to self-care for COVID-19 through the mediating role of the ILOC and individual locus of control. Since anxiety sensitivity means expecting an outcome and reflects personal differences in the tendency to experience fear [16], when a person believes that their behaviors and beliefs can affect COVID-19, they are more likely to engage in self-care behaviors. Hence, ILOC causes anxiety sensitivity to be directed in the right direction leading to self-care behaviors. On the other hand, ELOC means that the people around the person, the health-treatment system, and even the government are responsible for maintaining health. This belief has a significant impact on the relationship between anxiety sensitivity and self-care because believing in the importance and priority of the role of others in controlling COVID-19 diminishes the sense of internal responsibility for caring for COVID-19. Anxiety sensitivity about the locus of control and the locus of control as an intermediary belief is related to self-care. Therefore, it seems logical that HLOC plays a mediating role in the relationship between anxiety sensitivity and caring for COVID-19.
Health literacy refers to cognitive and social skills that motivate and enable people to acquire, understand, and use information to improve and maintain their health in both individual and social domains [25]. Thus, it can be argued that ILOC, or a person’s belief that they or others are effective in promoting health and that this matter is not dependent on chance and fortune, can improve their cognitive skills in health promotion and self-care behaviors. The stronger the people’s ILOC and their self-belief about their influence on their health, the more they are likely to engage in self-care behaviors. Moreover, the tendency towards ELOC decreases self-care behaviors because individuals with an ILOC have more control over their health, hygiene, and quality and tend to perform behaviors that help them diagnose and control diseases. These people also experience fewer psychological problems, including anxiety [40].
The results of this study showed that HLOC does not play a mediating role in the relationship between perceived stress and self-care. Previous studies have reported inconsistent results in this regard. Some researchers believe that stress causes people to act more actively to protect their health and perform self-care behaviors, regardless of factors such as internal or ELOC, and they are even more aware of avoiding risky behaviors [17]. Sometimes stress causes a decline in a person’s efficiency and reduces their self-care ability since different people perceive the same stressful factor in different ways [18]. Thus, it cannot be expected that HLOC can mediate between perceived stress and caring for COVID-19.
Conclusion
The present study showed that health literacy, anxiety sensitivity, and perceived stress are related to self-care for COVID-19, mediated by (internal and individual) HLOC. These results are significant because infectious diseases, such as COVID-19 require special attention due to their spread, and every person with self-care skills can prevent the risk of developing these diseases and in the case of infection, such skills will help them regain their health. Identifying the factors affecting self-care in COVID-19 can contribute to developing interventions to improve self-care and thus prevent the spread of the disease. In addition, the results of this study can have some implications for other infectious diseases as well. However, this research project was conducted with some limitations. Since this study was conducted on households in Ardabil City, caution should be taken in generalizing its results to other populations and groups. Furthermore, the data in this study were collected through self-report instruments. Thus, the participants may have difficulty expressing their emotions and thoughts. Accordingly, other data collection instruments, such as qualitative designs or interviews should be used in similar studies to obtain more reliable results. Nevertheless, following the results of the present study, interventional training programs can be implemented to improve the ILOC in people during the outbreak of COVID-19 to reduce anxiety and increase self-care in people. Moreover, this study can be replicated on other chronic diseases, including diabetes and multiple sclerosis (MS), to clarify the role of HLOC.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Ardabil University of Medical Sciences (Code: IR.ARUMS.REC.1399.045).
Funding
This article is a part of the research project (Code: IR.ARUMS.REC.1399.045) and financially supported by the Ardabil University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
In the end, all the researchers of this study wish to thank the Esteemed Vice Chancellor of Ardabil University of Medical Sciences and all other staff for their cooperation in approving and financially supporting this study, as well as all the families participating in this study.
Reference
- Fenwick A. The global burden of neglected tropical diseases. Public Health. 2012; 126(3):233-6. [DOI:10.1016/j.puhe.2011.11.015] [PMID]
- Edrisiane, GH. Malaria in Iran: Past and present situation. Iranian Journal of Parasitology. 2006; 1(1):1-14. [Link]
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. International Journal of Antimicrobial Agents. 2020; 55(3):105924. [DOI:10.1016/j.ijantimicag.2020.105924] [PMID] [PMCID]
- Farnoosh G, Alishiri G, Hosseini Zijoud SR, Dorostkar R, Jalali Farahani A. [Understanding the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease (COVID-19) based on available evidence - a narrative review (Persian)]. Journal of Military Medicine. 2022; 22(1):1-11. [DOI:10.30491/JMM.22.1.1]
- Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020; 395(10223):470-3. [DOI:10.1016/S0140-6736(20)30185-9] [PMID] [PMCID]
- Woodman J, Ballard K, Hewitt C, MacPherson H. Self-efficacy and self-care-related outcomes following Alexander Technique lessons for people with chronic neck pain in the ATLAS randomised, controlled trial. European Journal of Integrative Medicine. 2018; 17:64-71. [DOI:10.1016/j.eujim.2017.11.006] [PMID] [PMCID]
- Nikjoo RG, Janati A, Mohseni M. [Self-care ability of diabetic patients referring to Tabriz University of Medical Sciences clinics (Persian)]. Depiction of Health. 2019; 10(1):13-22. [Link]
- Austin S, Guay F, Senécal C, Fernet C, Nouwen A. Longitudinal testing of a dietary self-care motivational model in adolescents with diabetes. Journal of Psychosomatic Research. 2013; 75(2):153-9. [DOI:10.1016/j.jpsychores.2013.04.013][PMID]
- Johnson PJ, Ghildayal N, Rockwood T, Everson-Rose SA. Differences in diabetes self-care activities by race/ethnicity and insulin use. The Diabetes Educator. 2014; 40(6):767-77. [DOI:10.1177/0145721714552501] [PMID] [PMCID]
- Pandit AU, Bailey SC, Curtis LM, Seligman HK, Davis TC, Parker RM, et al. Disease-related distress, self-care and clinical outcomes among low-income patients with diabetes. Journal of Epidemiology and Community Health. 2014; 68(6):557-64. [DOI:10.1136/jech-2013-203063] [PMID]
- MacPherson H, Elliot B, Hopton A, Lansdown H, Birch S, Hewitt C. Lifestyle advice and self-care integral to acupuncture treatment for patients with chronic neck pain: Secondary analysis of outcomes within a randomized controlled trial. Journal of Alternative and Complementary Medicine. 2017; 23(3):180-7. [DOI:10.1089/acm.2016.0303] [PMID]
- Siegel D, Lopez J, Meier J. Antihypertensive medication adherence in the Department of Veterans Affairs. The American Journal of Medicine. 2007; 120(1):26-32. [DOI:10.1016/j.amjmed.2006.06.028] [PMID]
- Harvie A, Steel A, Wardle J. Traditional Chinese medicine self-care and lifestyle medicine outside of Asia: A systematic literature review. Journal of Alternative and Complementary Medicine. 2019; 25(8):789-808. [DOI:10.1089/acm.2018.0520] [PMID]
- Latas M, Pantić M, Obradović D. [Analysis of test anxiety in medical students (Serbian)]. Medicinski Pregled. 2010; 63(11-12):863-6.[DOI:10.2298/MPNS1012863L] [PMID]
- Saleh Manijeh H, Rostami M, Ahmadboukani S. Development of the Coronavirus Anxiety Model in the Elderly: Based on hope and health-related quality of life with the mediating role of perceived social support. Gerontology & Geriatric Medicine. 2021; 7:23337214211048324.[DOI:10.1177/23337214211048] [PMID] [PMCID]
- Deacon B, Abramowitz J. Anxiety sensitivity and its dimensions across the anxiety disorders. Journal of Anxiety Disorders. 2006; 20(7):837-57. [DOI:10.1016/j.janxdis.2006.01.003] [PMID]
- Zvolensky MJ, Arrindell WA, Taylor S, Bouvard M, Cox BJ, Stewart SH, et al. Anxiety sensitivity in six countries. Behav Res Ther. 2003; 41(7):841-59. [DOI:10.1016/S0005-7967(02)00187-0] [PMID]
- McCabe RE. Implicit and explicit memory for threat words in high-and low-anxiety-sensitive participants. Cognitive Therapy and Research. 1999; 23(1):21-38. [DOI:10.1023/A:1018706607051]
- Wauthia E, Lefebvre L, Huet K, Blekic W, El Bouragui K, Rossignol M. Examining the hierarchical influences of the big-five dimensions and anxiety sensitivity on anxiety symptoms in children. Frontiers in Psychology. 2019; 10:1185. [DOI:10.3389/fpsyg.2019.01185] [PMID] [PMCID]
- Ahmedbookani S, Khodabakhsh MR, Etemadi A, Kiani F. [The effects of Religious orientation and Parenting styles on students’ Mental Health (Persian)]. Community Health Journal. 2013; 7(2):20-9. [Link]
- Aghakhani N, sanaie K, Baghaei R, Khademvatan K. [The impact of educational- supportive self-care package on anxiety, depression and stress in myocardial infarction patients hospitalized in Shahid Gholipour Hospital, Boukan, Iran, 2016 (Persian)]. Nursing and Midwifery Journal. 2017; 15(4):281-91. [Link]
- Mehrizi Z, Nasiri A, Sahranavard S, Sebzari AR. [The effect of mindfulness-based intervention on perceived stress in family caregivers of patients with cancer (Persian)]. Iranian Journal of Psychiatric Nursing. 2020; 7(6):1-10. [Link]
- Hauser RM, Springer KW, Pudrovska T. Temporal structures of psychological well-being: continuityor change [PhD thesis]. Orlando: University of Wisconsin-Madison Orlando; 2005. [Link]
- Javadzade SH, Sharifirad G, Reisi M, Tavassoli E, Rajati F. [Health literacy among adults in Isfahan, Iran (Persian)]. Journal of Health System Research. 2013; 9(5):540-9. [Link]
- Berkman ND, Davis TC, McCormack L. Health literacy: What is it? Journal of Health Communication. 2010; 15(Suppl 2):9-19. [DOI:10.1080/10810730.2010.499985] [PMID]
- Gaglio B, Glasgow RE, Bull SS. Do patient preferences for health information vary by health literacy or numeracy? A qualitative assessment. Journal of Health Communication. 2012; 17(Suppl 3):109-21. [DOI:10.1080/10810730.2012.712616] [PMID]
- Zahedi S, Darvishpoor Kakhaki A, Hosseini M, Razzaghi Z. [The correlation between self-care and health literacy in patients undergoing hemodialysis (Persian)]. Iranian Journal of Diabetes and Metabolism. 2018; 17(4):180-8. [Link]
- Ciechanowski PS, Hirsch IB, Katon WJ. Interpersonal predictors of HbA(1c) in patients with type 1 diabetes. Diabetes Care. 2002; 25(4):731-6. [DOI:10.2337/diacare.25.4.731] [PMID]
- Shehu J, Mokgwathi MM. Health locus of control and internal resilience factors among adolescents in Botswana: A case-control study with implications for physical education. South African Journal for Research in Sport, Physical Education and Recreation. 2008; 30(2):95-105. [DOI:10.4314/sajrs.v30i2.25992]
- Blaxter M. Health and lifestyles. Milton Park: Taylor & Francis; 2003. [Link]
- Peterson C, Seligman ME. Causal explanations as a risk factor for depression: theory and evidence. Psychological Review. 1984; 91(3):347-74. [DOI:10.1037/0033-295X.91.3.347] [PMID]
- Aghamolaei T, Tavafian SS, Ghanbarnejad A. [Health locus of control and its relation with health-promoting behaviors among people over 15 in Bandar Abbas, Iran (Persian)]. Journal of Health Administration. 2014; 17(55):7-16. [Link]
- Kline RB. Response to Leslie Hayduk’s review of Principles and Practice of Structural Equation Modeling,14th edition; 2018; 3-4:188-95. [DOI 10.25336/csp29418]
- Montazeri A, Tavousi M, Rakhshani F, Azin SA, Jahangiri K, Ebadi M, et al. [Health Literacy for Iranian Adults (HELIA): Development and psychometric properties (Persian)]. Payesh. 2014; 13(5):589-99. [Link]
- Panahi R, Ramezankhani A, Tavousi M, Osmani F, Ghazanfari E, Niknami S. [Evaluation of health literacy and its influencing factors on dormitory students of Shahid Beheshti University of Medical Sciences in Tehran (Persian)]. Journal of Education and Community Health. 2016; 3(3):30-6. [DOI:10.21859/jech-03035]
- Mohammadi-Yeganeh L, Bastani F, Feizi Z, Agilar-Vafaie M, Haghani HA. [Effect of stress management education on mood and perceived stress among oral contraceptive pill users (Persian)]. Iran Journal of Nursing. 2008; 21(53):63-73. [Link]
- Taylor S, Cox BJ. An expanded anxiety sensitivity index: evidence for a hierarchic structure in a clinical sample. Journal of anxiety disorders. 1998 Sep 1;12(5):463-83. https://doi.org/10.1016/S0887-6185(98)00028-0
- Moradi MF. [Evaluation of psychometric properties of anxiety sensitivity index and its relationship with mental health in Shiraz University Students (Persian)] [Msc thesis]. Shiraz: Shiraz university; 1996.
- Wallston KA, Wallston BS, DeVellis R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Education Monographs. 1978; 6(2):160-70. [DOI:10.1177/109019817800600107] [PMID]
- Cvengros JA, Christensen AJ, Lawton WJ. Health locus of control and depression in chronic kidney disease: A dynamic perspective. Journal of Health Psychology. 2005; 10(5):677-86. [DOI:10.1177/1359105305055320] [PMID]
- Ng SM, Ke GN, Raymond W. The mediating role of work locus of control on the relationship among emotional intelligence, organisational citizenship behaviours, and mental health among nurses. Australian Journal of Psychology. 2014; 66(4):207-15. [Link]
- Clark KD. The relationship of perceived stress and self-efficacy among correctional employees in close-security and medium-security-level institutions [PhD dissertation]. Washington: Walden University; 2010. [Link]
- Soffer-Dudek N, Shahar G. Daily stress interacts with trait dissociation to predict sleep-related experiences in young adults. Journal of Abnormal Psychology. 2011; 120(3):719-29. [DOI:10.1037/a0022941] [PMID]
Article type: Original Research Articles |
Subject:
epidemiological studies
Received: 2022/10/5 | Accepted: 2023/09/9 | Published: 2023/12/1
Received: 2022/10/5 | Accepted: 2023/09/9 | Published: 2023/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
