
988368
Sat, Aug 8, 2026

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 577-590 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khodaverdizadeh M, Mohammad Rahimi N, Esfahani M. A Systematic Review and Meta-analysis: The Effect of Scapular-focused Exercise Therapy on Shoulder Pain and Function and Scapular Positioning in People With Scapular Dyskinesia. Iranian Rehabilitation Journal 2023; 21 (4) :577-590
URL: http://irj.uswr.ac.ir/article-1-1793-en.html
URL: http://irj.uswr.ac.ir/article-1-1793-en.html



1- Department of Sports Sciences, Faculty of Literature and Humanities, Imam Reza International University, Mashhad, Iran.
Full-Text [PDF 837 kb]
(6158 Downloads)
| Abstract (HTML) (5023 Views)
Full-Text: (3498 Views)
Introduction
Shoulder pain is a common musculoskeletal issue that can result in functional impairment, impact work productivity, affect athletic performance, and be connected with an enormous economic burden [1], with a predicted incidence between 20% and 33% in public people. Shoulder pain is regarded as the third most typical musculoskeletal disorder [1].
Several studies have indicated that pain, physical function limitations, and activity restrictions are the most common symptoms experienced by individuals with shoulder pain [1, 2]. Moreover, it has been confirmed that persons who face shoulder pains typically exhibit an imbalance in scapulothoracic muscle activation [3, 4], which includes reduced activation of the serratus anterior (SA) and lower trapezius (LT), alongside incremented activation of the upper trapezius (UT) [1]. Tightness of soft tissues has also been associated with scapular dyskinesis (SD) [5].
In addition, it is crucial to maintain proper scapular position and motion to achieve optimal functioning of the shoulder joint. This is particularly important for facilitating repetitive movements of the shoulder [6]. The scapular as a multi-task component and a base for muscle attachments implements numerous functions contributing to the stability and mobility of the shoulder girdle.
The implementation of scapula external rotation (ER), posterior tilt, and upward rotation (UR) plays a crucial role in maintaining the appropriate length-tension relationship of the muscles related to the scapula [7, 8]. Additionally, these movements help to prevent the occurrence of subacromial space impingement when the shoulder is elevated [9, 10].
According to existing literature, there is a suggestion that the glenohumeral joint may experience decreased efficiency in its functioning when the stabilizing function of the scapula is compromised. This impairment in scapular stabilization can lead to a reduction in the overall role of the neuromuscular system, ultimately causing potential shoulder joint dysfunction [11]. Kibler et al. found that as a stable base for optimal muscle activation, the scapula has a crucial role in the upper limb function, an integrated cavity for joint kinematics, and a transition chain for improved development energies in the kinetic chain reaction [12]. SD is illustrated by an eminent medial edge and inferior angle of the scapula concerning the thoracic spine, both in static and dynamic positions. This condition is often accompanied by early scapular elevation or shrugging, and improper upward and downward rotation of the scapula in concurrent up or down movement upper limb [12, 13, 14]. Because of kinetic and muscular chains, SD [13, 15] can reduce the stability of the glenohumeral joint [15, 16, 17], resulting in an increased risk of shoulder pain in up to 43% of overhead activities [18]. Previous studies have provided evidence that a considerable percentage, spanning from 33% to 100%, of individuals who have been clinically diagnosed with different types of shoulder ailments, such as subacromial impingement syndrome (SIS), frequently demonstrate SD [19, 20].
The main group muscles optimizing scapula position and scapulohumeral rhythm are the serratus anterior, rhomboid, and trapezius, which decrease pain and enhance function [21, 22]. Regarding this particular issue, there has been a proposal that a heightened degree of movement in the UT, combined with a reduction in movement in the LT and SA, might be associated with modified scapular motion. These alterations include diminished UR, reduced posterior scapular tilting, and ER [5, 23].
Several studies have provided evidence regarding the significance of exercise therapy in restoring typical scapular motion [13, 21]. Therefore, the implementation of exercise therapy that specifically targets the scapula is considered a crucial intervention in physiotherapy for individuals diagnosed with SIS and SD [24]. Various systematic reviews have been conducted to assess the usefulness of physical exercise therapy in reducing pain and improving the function of individuals with SIS [11, 22, 25]. The findings from these reviews indicate a moderate to a strong level of evidence supporting the usefulness of physical exercise therapy in reducing discomfort and improving the function of this population during short-term follow-up [11, 22, 25]. However, there is significant doubt concerning the effectiveness of such strategies in recovering healthy scapular motions. In their systematic review, Bury et al. (2016) proposed that the implementation of scapular muscle corrective exercise can significantly alleviate shoulder pain. However, the review found that the impact of this exercise on scapular alignment and movement, based on the analysis of four included investigations, remained uncertain [26].
Moreover, the conducted studies failed to include individuals who were asymptomatic and diagnosed with scapular dyskinesia. Therefore, certain pertinent studies may be omitted. Hence, given the lack of clear evidence regarding the impact of suggested interventions for SD on its improvement, this systematic review and meta-analysis seeks to evaluate the efficacy of exercise therapy in mitigating shoulder pain and enhancing both shoulder function and scapular position among people afflicted with SD. Additionally, the investigation determines whether any improvements in disability and discomfort are attended by advancements in scapular alignment and movement.
Materials and Methods
The present systematic review pursued the procedures outlined in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) [27]. Before beginning the research, the techniques for the review were developed; however, we did not register the protocol.
Search strategy
Possible related research was determined by a systematic review librarian. Databases including PubMed, Medline (Ovid), Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Physiotherapy Evidence Database (PEDro), Google Scholar, and Scopus were applied for a detailed electronic search. Furthermore, the process of cross-referencing the included studies in the reference list was implemented, and consultation with subject matter experts was also undertaken to validate any supplementary sources, whether published or unpublished. To ensure a comprehensive search, additional efforts were made to find relevant studies beyond the usual sources. This involved searching grey literature resources like conference and government websites, without any limitations on the outcome. The search also included informal sources like conference abstracts and PhD theses to expand the scope of the search. The inquiries utilized a variety of both medical subject headings (MeSH) and free-text terms related to the keywords “SD,” “therapy,” “physical therapy,” “exercise therapy,” “subacromial impingement syndrome,” “scapular position,” “shoulder function,” “shoulder rehabilitation,” “shoulder exercise,” “shoulder impingement syndrome,” and “scapular stabilization exercises.” To optimize the search process, we utilized Boolean search terms (AND, OR, NOT) to combine various search terms. Specifically, we integrated the search terms related to exercise therapy participation with those related to shoulder dyskinesis and/or shoulder impingement syndrome. The search was executed in July 2021, encompassing databases from their inception to July 2021. Subsequently, behind the initial screening process, systematic reviews, meta-analyses, and all study references were thoroughly examined to ascertain the inclusion and exclusion criteria, thereby ensuring the comprehensive identification of all pertinent papers.
Selection criteria
To establish the parameters for study inclusion, we employed the PICOTS criteria, which encompassed the following elements: Participants, intervention, comparison, outcome, time, and study design. The titles and/or abstracts of studies that were recognized utilizing the search strategy, as well as those obtained from extra references, were allocated among three authors. The full-text papers of probability suitable studies were recovered and considered for eligibility by two writers, working unassisted. Any divergence of opinion between the two authors was effectively resolved through a process of deliberation involving the third author. In this meta-analysis, exercise therapies included various therapies like scapular strengthening exercise, scapular stabilization exercise, and shoulder girdle muscle stretching were included. Articles entered in the present review compared adults in the experimental and control groups (CG).
Inclusion/exclusion criteria
To ascertain and choose the articles that met the requirements, the following criteria were taken into consideration. This study exclusively includes randomized controlled trials (RCTs) or control trials that have been published in the English language. The study included adults who were 18 years of age or older. The articles selected for analysis employed scapular-focused exercises in a pre-post design, with a control group. The present study has excluded review articles, literature reviews, conference abstracts, and study protocols. Additionally, research involving participants who were involved in an exercise therapy regimen within the past six months has also been excluded. The identified studies have been subjected to independent evaluation by two reviewers, with discrepancies being resolved by the third reviewer.
Outcome measures
The result measurements of the current meta-analysis were pain shoulder, scapula positioning or orientation, and shoulder function.
Data extraction
The data extraction process was accomplished by two researchers (MKH and ME), who unassisted and archived the information in a database. In cases where disagreements arose, a third researcher (NMR), was responsible for resolving them. The extracted information encompassed various elements like the author’s name, year of publication, and country of origin. Additionally, it included details regarding the number of cases and controls, the average age of participants, their gender distribution, characteristics of the exercise protocol, and the Mean±SD values of the variable measures both before and after the protocol, or the differences observed between these two-time points.
Data synthesis
For each of the articles that were incorporated, the effect size of any result was concisely summarized through the computation of the mean difference (MD) between the exercise protocol and control condition, spanning from pre-protocol to post-protocol. The results were analyzed using the weighted MD with a 95% CI, assuming similarity in the evaluation method or reporting. Nevertheless, to account for variations in evaluation or documenting methods, a standardized mean difference (SMD) was utilized for the analysis of outcomes. The analysis for this study was conducted utilizing Review Manager software, version 5.3, developed by The Nordic Cochrane Centre in Copenhagen, Denmark. The data were obtained by calculating the changes in the mean and SD values. The difference between the mean at pre-protocol and the mean at post-protocol was computed, and the SD of this difference was computed for the investigation group participants. This was done in cases where the change in Mean±SD was not explicitly provided, and instead, group p or a 95% CI were documented. In studies where the standard error of the mean (SEM) data was provided rather than SD, the SEM was altered to SD [28]. In instances where data were not provided in written form or tabulated, and the authors were inaccessible, data depicted in figures were extracted or acquired, when possible, using the GetData Graph Digitizer software. Subsequently, the inverse of the variance was utilized to assign weights to each effect size. The utilization of random-effects models, which account for heterogeneity within the model, was employed to aggregate the primary and secondary outcomes across all study groups.
The researchers utilized a random-effects model to obtain pooled estimates of the impact of exercise therapy on variable measures. The researchers evaluated the heterogeneity among the studies using the I2 statistic, where values >50% indicate significant heterogeneity [28]. The I2 metric spans a scale of 0 to 100%, with a point of 0% demonstrating the scarcity of experimental heterogeneity. Scores of 25%, 50%, and 75% correspond to low, moderate, and high levels of heterogeneity, respectively [28]. The meta-analysis was conducted utilizing Forest plots and a significance level of 5% was employed to determine the statistical remarkable of the outcomes. The assessment of publication bias risk was conducted through the utilization of Funnel plots [29].
Study quality
The quality of the investigations contained in the analysis was evaluated separately utilizing a validated tool called tool for the assessment of study quality and reporting in exercise (TESTEX). This tool utilizes a fifteen-point scale to evaluate both the quality (with a maximum of five scores) and documentation (with a maximum of ten scores) of exercise therapy programs [30]. This evaluation was conducted by two authors separately. In instances of disagreement, consultation with the third author was sought. The allocation of included studies was conducted randomly among the authors. Furthermore, the studies were cross-checked to ensure the accuracy of data extraction and to evaluate the quality of per investigation. Lastly, the review process involved two authors who independently evaluated the studies. A sub-analysis was conducted to evaluate the quality of the investigation, which was categorized regarding a TESTEX score of 10 or higher and a within-study risk evaluation ranging from low to medium.
Results
Study and participants’ characteristics
A total of 985 records were specified during the initial search. After excluding duplicate articles (n=222), the staying articles were evaluated concerning their title and abstract, resulting in the removal of 743 studies. This process yielded a final selection of 20 full-text studies. Nine additional articles were excluded due to the following rationales: a) Non-RCTs [31–37], b) Case report [38], and d) Study with active CG [39]. Eleven studies [14-24, 40-50] met our inclusion criteria and were used in the meta-analysis (PRISMA flow diagram; Figure 1).
 Studies were performed in Turkey (3), Iran (2), German (1), Brazil (1), India (1), Belgium (1), Norway (1), and USA (1). The mean age and gender distribution for each of the 11 studies included in the analysis are presented in Table 1.
Studies were performed in Turkey (3), Iran (2), German (1), Brazil (1), India (1), Belgium (1), Norway (1), and USA (1). The mean age and gender distribution for each of the 11 studies included in the analysis are presented in Table 1.


The total number of participants in all studies was 594, with an equal number of participants (50%) in the experimental and CG (298 participants in each group). The sample size for each study ranged from 22 to 104 participants.
Intervention details
The interventions utilized by the 11 studies included in the analysis exhibited a degree of variability and encompassed scapular mobilization, muscle retraining, and stretching, as can be observed in Table 1. Among the studies, three of them specifically examined the efficacy of scapular-focused exercise training when added to conventional therapy, which employed an additive design [40, 41, 49], while six articles straightforward compared scapular-based exercise training with non-scapular-based [42–46, 50]. Two studies investigated the effect of scapular stabilization or resistance exercises [47, 48]. All included studies recruited both males and females, but one study [46] did not mention the number of each gender in each group.
Ten included studies assessed pain with activity, with a study unclearly documenting whether pain was evaluated during exercise [49]. Shoulder function including disabilities of the arm, shoulder, and hand (Quick DASH scale), shoulder pain and disability index (SPADI), and strengths and disabilities questionnaire (SDQ) was evaluated in nine investigations [40, 42–45, 47–50]. Moreover, in four studies [41, 47–49] lateral scapular slide test (LSST) was used to determine scapular dyskinesia.
Meta-analysis results
Change in shoulder pain
Eleven investigations comprising 594 individuals (298 in the experimental group and 296 in the CG, respectively) documented the outcome measure of shoulder pain. Pooled findings showed that exercise therapy produced a significant decrease in shoulder pain (SMD=-0.83; 95% CI,-1.44%, -0.22%; P=0.008) in comparison to the CG (Figure 2).

Change in shoulder function
Nine investigations, comprising a total of 482 individuals, have reported on the outcome measure of shoulder function. Upon pooling the results from the random-effects model, it was found that exercise therapy has a remarkable proper influence on shoulder function (SMD=-0.62; 95% CI, -1.08%, -0.16%; P=0.008; Figure 3).

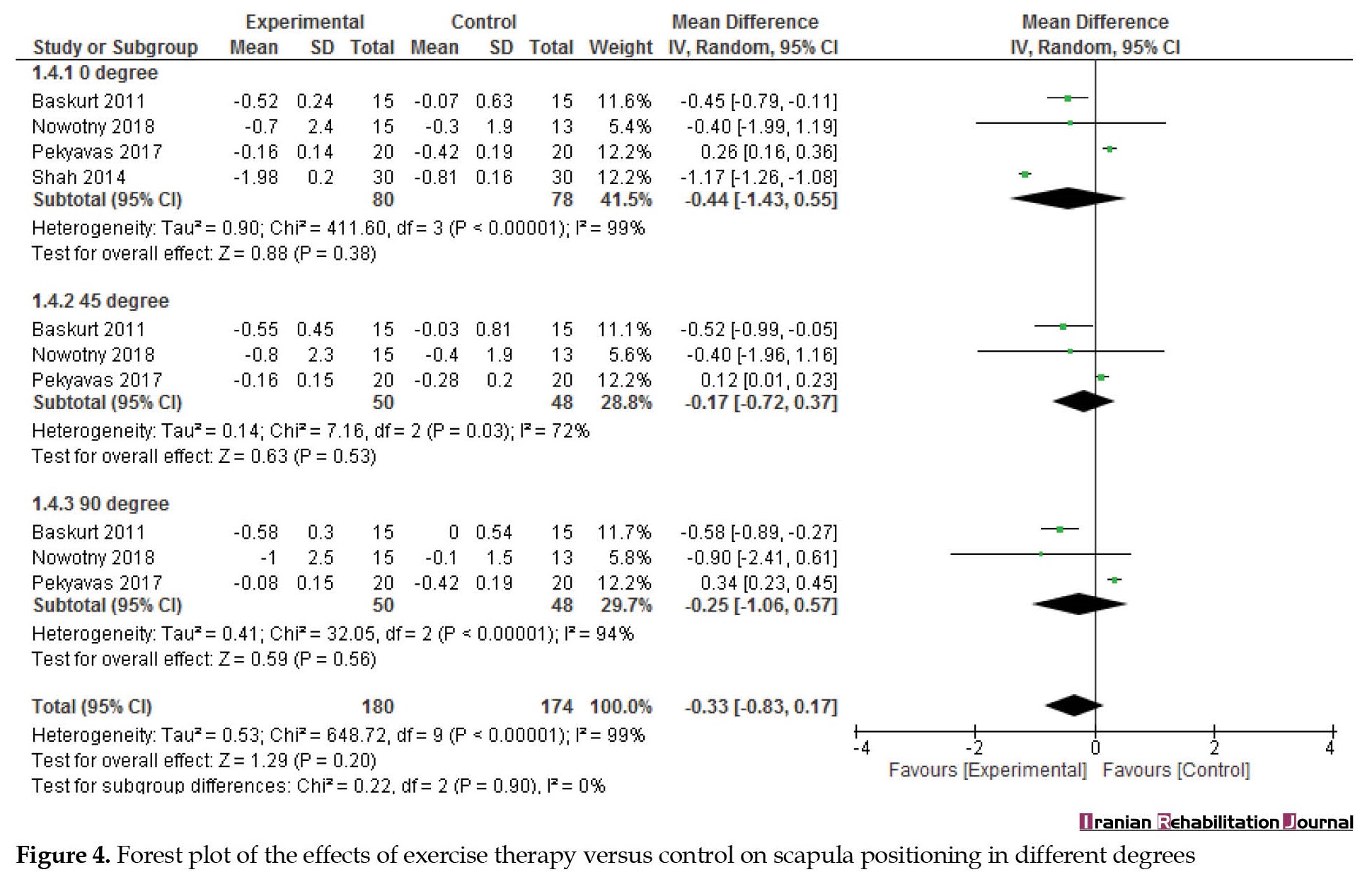
Scapula positioning
Four studies reported scapula positioning in 0°, three studies reported scapula in 45° and 90° as an outcome measure. Upon pooling the results from the random-effects model, it was found that exercise therapy had no significant effect on scapula positioning at any angle (0°: MD=-0.44; 95% CI, -1.43%, 0.55%; P=0.38; 45°: MD=-0.17; 95% CI, -0.72%, 0.37%; P=0.53; 90°: MD=-0.25; 95% CI, -1.06%, 0.57%; P=0.56; Figure 4).
Study quality
The researchers assessed the quality of the studies that entered the analysis and determined it to be moderate. The median TESTEX score was 9, with a range of 7 to 10 out of a possible maximum point of 15. Table 2 presents the distribution of scores obtained in the aforementioned studies.
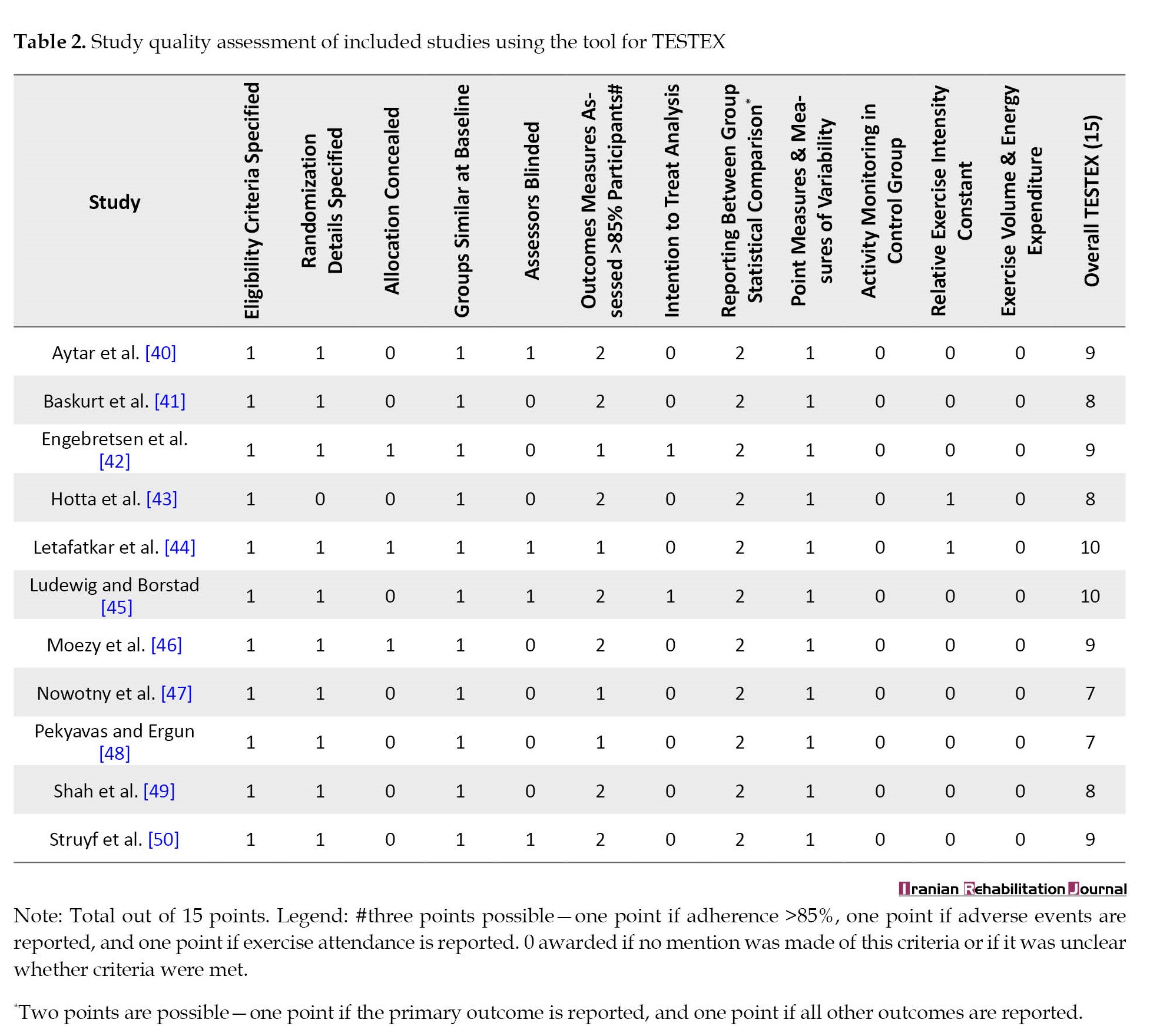
Specifically, two studies obtained a point of 10, four studies obtained a point of 9, three studies obtained a point of 8, and two studies obtained a point of 7. Of the TESTEX criteria, the following was accomplished especially poorly: Training volume and energy cost and workout monitoring in the CG 0/11; relative exercise intensity constant and preference to treat studies only 2/11 studies; allocation concealment only 3/11 studies; assessors blinded 4/11 studies. The other criteria were met in at least 50% of investigations.
Heterogeneity and publication bias
Our analyses in shoulder pain and scapula positioning at 0° revealed moderate heterogeneity (I2=74%, P<0.0001, and I2=72%, P<0.00001, respectively). However, the heterogeneity in shoulder function and scapula positioning at 90° and 45° revealed high heterogeneity (I2=82%, P<0.0001, I2=94%, P<0.00001, and I2=99%, P<0.0001, respectively). Egger plots revealed little to moderate evidence of publication bias (Figure 5a and b).

Discussion
The current systematic review and meta-analysis synthesized the existing literature regarding the impact of exercise therapy on shoulder pain, function, and scapular positioning among people diagnosed with SD. The findings indicated that, in comparison to the CG, the exercise therapy protocol proved to be a successful intervention in significantly reducing pain and enhancing shoulder function. Nevertheless, exercise therapy had no significant effect on scapula positioning at any angle. Accordingly, the hypothesis of this investigation was supported just by pain and shoulder function.
The findings of this review indicated that therapeutic exercises did not yield a statistically significant impact on scapula positioning. However, it is worth noting that these exercises demonstrated a potential positive influence on both shoulder pain and function. It is conceivable that the enhancement of joint proprioception may contribute, at least in part, to the observed improvement in therapeutic exercise outcomes. The management of SD necessitates addressing the overall biomechanics of the body, rather than solely focusing on a specific region such as the shoulder, neck, trunk, or pelvis. Given that the human body functions as a kinetic chain, it is worth considering the incorporation of scapular-focused exercise therapy and the examination of scapular biomechanics in conjunction with neighboring segments [51].
Shoulder pathology management should include evaluation and administration of the scapula position and motion. Frequently, scapular position and motion findings promote determining management options, rehabilitation protocols and return to activity [52]. SD is a condition that is generally linked to shoulder pathology and regarded as a risk factor for more injury; however, it is additionally present in asymptomatic people [20]. Evidence recommends that scapular motion disorders such as reduced scapular UR, limited scapular posterior tipping, and ER can cause rotator cuff–related shoulder pain [9, 53, 54]. It has been suggested that the weakness of scapular muscles can be an influential factor in unusual scapular kinematics [55 56]. Notably, enhanced facilitation of the UT with inhibition of the LT and SA has been linked to changed scapular position and motion [5]. Nevertheless, it is not clear if these differences are compensatory strategies or causative factors [20, 57].
In subjects displaying scapular dyskinesia, a lack of flexibility or strength in a particular agonistic muscle, which is then compensated by the antagonist’s muscle [58], may result in the onset of shoulder pain [18, 52, 54] due to a decrease in subacromial space, dysfunction of the shoulder griddle, and eventually structural damage [58], as well as an increase in mechanical stress on the soft tissue of glenohumeral [59].
This study comprised 11 trials with different therapeutic exercises including scapular flexibility, strengthening, and stability exercises given to intervention groups [41, 46, 49], scapular control and dynamic scapular stability [42, 50], neuromuscular training and per scapular strengthening [43], stretching and strengthening exercises [33, 40, 44, 45], stabilization exercise [47, 60], home exercise program, and resistive training with proper resistance of Thera band [48].
The lack of scapular stability appears to be a crucial factor in the enhancement of shoulder pain and disability. The efficacy of therapeutic exercise in retraining motor skills and activating stabilization muscles has been observed to have a positive impact on scapular kinematics. Therefore, it is recommended that this approach be included as part of a multidisciplinary treatment plan. The scapular-focused interventions that can include various exercises are often suggested for shoulder pain and disability in subjects with scapular dyskinesia. However, several studies of moderate to high quality have managed to yield strong evidence about the efficacy and safety of these interventions.
Struyf et al. (2013) concluded that a large clinically meaningful treatment effect favoring scapular motor control training was observed in dysfunction. A notable reduction in pain of moderate to large clinical significance was observed during the administration of the Hawkins test, Neer test, and empty can test. Furthermore, the experimental group illustrated an average decrease in self-perceived pain while at rest, as measured by the visual analog scale (VAS), whereas the CG did not exhibit any changes. The observed outcomes remained consistent during the three-month follow-up period [50]. Further, scapula-focused motor control and muscular strengthening exercises can affect subjects’ resting position, scapular movement patterns, and improved function of the affected shoulder in subjects with SIS [43].
Engebretsen et al. (2011) observed a substantial alteration between the supervised scapular control and dynamic scapular stability and radial extracorporeal shock-wave therapy groups after 18 weeks. However, the findings indicated that there was no reported therapeutic advantage of scapular stability compared to radial extracorporeal shock-wave therapy in this particular group of individuals during the 1-year follow-up period. A smaller number of patients in the scapular stability group underwent supplementary interventions [42]. Furthermore, there is empirical substantiation that corroborates the efficacy of scapular stabilization exercises as a form of exercise therapy for reducing pain and facilitating rehabilitation in people with SIS [46] demonstrated through statistical and clinical evidence that combining stretching and strengthening exercises is more effective than solely performing these exercises for enhancing the strength of the scapular muscles, preventing shoulder dysfunction, and enhancing the sense of joint position [41].
Besides, the study of Shah et al. (2014) [49] supported the hypothesis that there will be significant relief with the use of scapular stability exercises in patients with SIS. Hence, it was concluded that there is a significant difference between conventional exercise alone and conventional exercise therapy and scapular stability exercises in relieving pain and improving physical function in SIS, as seen with the VAS shoulder pain, disability index, and lateral scapular stability test. After four weeks of treatment, a significant improvement in pain and functional status was detected in patients performing conventional exercise therapy and scapular stability exercises rather than performing conventional exercise therapy alone [49].
Strengths and limitations /future research
Our findings will be more convincing thanks to a thorough search of English databases, reliable quality assessment, and a useful analysis methodology used in this systematic review and meta-analysis. It is important to acknowledge certain limitations. One potential limitation of this study is the restriction to articles published exclusively in English. This approach may overlook relevant research published in other languages, potentially leading to an incomplete representation of the topic under investigation. One additional limitation is the potential for significant heterogeneity to arise, which can have a detrimental impact on participants’ conclusions and baseline characteristics. The examination of publication bias was not carried out as a result of the restricted quantity of studies encompassed, particularly concerning scapula positioning. Given the restricted accessibility of outcome data for certain research endeavors and the comparably diminutive quantity of research endeavors that were encompassed, it is sensible to exercise prudence when comprehending the conclusions of this particular investigation.
Conclusion
To sum up, in the final analysis, our systematic review and meta-analysis revealed that exercise therapy protocols have a positive impact on pain reduction and functional improvement among individuals with scapular dyskinesia. However, no significant alterations in scapula positioning were observed as a result of these interventions. Additional long-term and rigorous trials are necessary to evaluate and validate the results presented in this study.
Ethical Considerations
Compliance with ethical guidelines
This systematic review and meta-analysis study is regarded exclusively on published literature.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology and investigation: All authors; Methodology: Nasser Mohammad Rahimi; Writing original draft: Mahdi Esfahani and Mohammad Khodaverdizadeh; Review and editing: Nasser Mohammad Rahimi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Department of Sports Sciences, Imam Reza International University.
References
Shoulder pain is a common musculoskeletal issue that can result in functional impairment, impact work productivity, affect athletic performance, and be connected with an enormous economic burden [1], with a predicted incidence between 20% and 33% in public people. Shoulder pain is regarded as the third most typical musculoskeletal disorder [1].
Several studies have indicated that pain, physical function limitations, and activity restrictions are the most common symptoms experienced by individuals with shoulder pain [1, 2]. Moreover, it has been confirmed that persons who face shoulder pains typically exhibit an imbalance in scapulothoracic muscle activation [3, 4], which includes reduced activation of the serratus anterior (SA) and lower trapezius (LT), alongside incremented activation of the upper trapezius (UT) [1]. Tightness of soft tissues has also been associated with scapular dyskinesis (SD) [5].
In addition, it is crucial to maintain proper scapular position and motion to achieve optimal functioning of the shoulder joint. This is particularly important for facilitating repetitive movements of the shoulder [6]. The scapular as a multi-task component and a base for muscle attachments implements numerous functions contributing to the stability and mobility of the shoulder girdle.
The implementation of scapula external rotation (ER), posterior tilt, and upward rotation (UR) plays a crucial role in maintaining the appropriate length-tension relationship of the muscles related to the scapula [7, 8]. Additionally, these movements help to prevent the occurrence of subacromial space impingement when the shoulder is elevated [9, 10].
According to existing literature, there is a suggestion that the glenohumeral joint may experience decreased efficiency in its functioning when the stabilizing function of the scapula is compromised. This impairment in scapular stabilization can lead to a reduction in the overall role of the neuromuscular system, ultimately causing potential shoulder joint dysfunction [11]. Kibler et al. found that as a stable base for optimal muscle activation, the scapula has a crucial role in the upper limb function, an integrated cavity for joint kinematics, and a transition chain for improved development energies in the kinetic chain reaction [12]. SD is illustrated by an eminent medial edge and inferior angle of the scapula concerning the thoracic spine, both in static and dynamic positions. This condition is often accompanied by early scapular elevation or shrugging, and improper upward and downward rotation of the scapula in concurrent up or down movement upper limb [12, 13, 14]. Because of kinetic and muscular chains, SD [13, 15] can reduce the stability of the glenohumeral joint [15, 16, 17], resulting in an increased risk of shoulder pain in up to 43% of overhead activities [18]. Previous studies have provided evidence that a considerable percentage, spanning from 33% to 100%, of individuals who have been clinically diagnosed with different types of shoulder ailments, such as subacromial impingement syndrome (SIS), frequently demonstrate SD [19, 20].
The main group muscles optimizing scapula position and scapulohumeral rhythm are the serratus anterior, rhomboid, and trapezius, which decrease pain and enhance function [21, 22]. Regarding this particular issue, there has been a proposal that a heightened degree of movement in the UT, combined with a reduction in movement in the LT and SA, might be associated with modified scapular motion. These alterations include diminished UR, reduced posterior scapular tilting, and ER [5, 23].
Several studies have provided evidence regarding the significance of exercise therapy in restoring typical scapular motion [13, 21]. Therefore, the implementation of exercise therapy that specifically targets the scapula is considered a crucial intervention in physiotherapy for individuals diagnosed with SIS and SD [24]. Various systematic reviews have been conducted to assess the usefulness of physical exercise therapy in reducing pain and improving the function of individuals with SIS [11, 22, 25]. The findings from these reviews indicate a moderate to a strong level of evidence supporting the usefulness of physical exercise therapy in reducing discomfort and improving the function of this population during short-term follow-up [11, 22, 25]. However, there is significant doubt concerning the effectiveness of such strategies in recovering healthy scapular motions. In their systematic review, Bury et al. (2016) proposed that the implementation of scapular muscle corrective exercise can significantly alleviate shoulder pain. However, the review found that the impact of this exercise on scapular alignment and movement, based on the analysis of four included investigations, remained uncertain [26].
Moreover, the conducted studies failed to include individuals who were asymptomatic and diagnosed with scapular dyskinesia. Therefore, certain pertinent studies may be omitted. Hence, given the lack of clear evidence regarding the impact of suggested interventions for SD on its improvement, this systematic review and meta-analysis seeks to evaluate the efficacy of exercise therapy in mitigating shoulder pain and enhancing both shoulder function and scapular position among people afflicted with SD. Additionally, the investigation determines whether any improvements in disability and discomfort are attended by advancements in scapular alignment and movement.
Materials and Methods
The present systematic review pursued the procedures outlined in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) [27]. Before beginning the research, the techniques for the review were developed; however, we did not register the protocol.
Search strategy
Possible related research was determined by a systematic review librarian. Databases including PubMed, Medline (Ovid), Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Physiotherapy Evidence Database (PEDro), Google Scholar, and Scopus were applied for a detailed electronic search. Furthermore, the process of cross-referencing the included studies in the reference list was implemented, and consultation with subject matter experts was also undertaken to validate any supplementary sources, whether published or unpublished. To ensure a comprehensive search, additional efforts were made to find relevant studies beyond the usual sources. This involved searching grey literature resources like conference and government websites, without any limitations on the outcome. The search also included informal sources like conference abstracts and PhD theses to expand the scope of the search. The inquiries utilized a variety of both medical subject headings (MeSH) and free-text terms related to the keywords “SD,” “therapy,” “physical therapy,” “exercise therapy,” “subacromial impingement syndrome,” “scapular position,” “shoulder function,” “shoulder rehabilitation,” “shoulder exercise,” “shoulder impingement syndrome,” and “scapular stabilization exercises.” To optimize the search process, we utilized Boolean search terms (AND, OR, NOT) to combine various search terms. Specifically, we integrated the search terms related to exercise therapy participation with those related to shoulder dyskinesis and/or shoulder impingement syndrome. The search was executed in July 2021, encompassing databases from their inception to July 2021. Subsequently, behind the initial screening process, systematic reviews, meta-analyses, and all study references were thoroughly examined to ascertain the inclusion and exclusion criteria, thereby ensuring the comprehensive identification of all pertinent papers.
Selection criteria
To establish the parameters for study inclusion, we employed the PICOTS criteria, which encompassed the following elements: Participants, intervention, comparison, outcome, time, and study design. The titles and/or abstracts of studies that were recognized utilizing the search strategy, as well as those obtained from extra references, were allocated among three authors. The full-text papers of probability suitable studies were recovered and considered for eligibility by two writers, working unassisted. Any divergence of opinion between the two authors was effectively resolved through a process of deliberation involving the third author. In this meta-analysis, exercise therapies included various therapies like scapular strengthening exercise, scapular stabilization exercise, and shoulder girdle muscle stretching were included. Articles entered in the present review compared adults in the experimental and control groups (CG).
Inclusion/exclusion criteria
To ascertain and choose the articles that met the requirements, the following criteria were taken into consideration. This study exclusively includes randomized controlled trials (RCTs) or control trials that have been published in the English language. The study included adults who were 18 years of age or older. The articles selected for analysis employed scapular-focused exercises in a pre-post design, with a control group. The present study has excluded review articles, literature reviews, conference abstracts, and study protocols. Additionally, research involving participants who were involved in an exercise therapy regimen within the past six months has also been excluded. The identified studies have been subjected to independent evaluation by two reviewers, with discrepancies being resolved by the third reviewer.
Outcome measures
The result measurements of the current meta-analysis were pain shoulder, scapula positioning or orientation, and shoulder function.
Data extraction
The data extraction process was accomplished by two researchers (MKH and ME), who unassisted and archived the information in a database. In cases where disagreements arose, a third researcher (NMR), was responsible for resolving them. The extracted information encompassed various elements like the author’s name, year of publication, and country of origin. Additionally, it included details regarding the number of cases and controls, the average age of participants, their gender distribution, characteristics of the exercise protocol, and the Mean±SD values of the variable measures both before and after the protocol, or the differences observed between these two-time points.
Data synthesis
For each of the articles that were incorporated, the effect size of any result was concisely summarized through the computation of the mean difference (MD) between the exercise protocol and control condition, spanning from pre-protocol to post-protocol. The results were analyzed using the weighted MD with a 95% CI, assuming similarity in the evaluation method or reporting. Nevertheless, to account for variations in evaluation or documenting methods, a standardized mean difference (SMD) was utilized for the analysis of outcomes. The analysis for this study was conducted utilizing Review Manager software, version 5.3, developed by The Nordic Cochrane Centre in Copenhagen, Denmark. The data were obtained by calculating the changes in the mean and SD values. The difference between the mean at pre-protocol and the mean at post-protocol was computed, and the SD of this difference was computed for the investigation group participants. This was done in cases where the change in Mean±SD was not explicitly provided, and instead, group p or a 95% CI were documented. In studies where the standard error of the mean (SEM) data was provided rather than SD, the SEM was altered to SD [28]. In instances where data were not provided in written form or tabulated, and the authors were inaccessible, data depicted in figures were extracted or acquired, when possible, using the GetData Graph Digitizer software. Subsequently, the inverse of the variance was utilized to assign weights to each effect size. The utilization of random-effects models, which account for heterogeneity within the model, was employed to aggregate the primary and secondary outcomes across all study groups.
The researchers utilized a random-effects model to obtain pooled estimates of the impact of exercise therapy on variable measures. The researchers evaluated the heterogeneity among the studies using the I2 statistic, where values >50% indicate significant heterogeneity [28]. The I2 metric spans a scale of 0 to 100%, with a point of 0% demonstrating the scarcity of experimental heterogeneity. Scores of 25%, 50%, and 75% correspond to low, moderate, and high levels of heterogeneity, respectively [28]. The meta-analysis was conducted utilizing Forest plots and a significance level of 5% was employed to determine the statistical remarkable of the outcomes. The assessment of publication bias risk was conducted through the utilization of Funnel plots [29].
Study quality
The quality of the investigations contained in the analysis was evaluated separately utilizing a validated tool called tool for the assessment of study quality and reporting in exercise (TESTEX). This tool utilizes a fifteen-point scale to evaluate both the quality (with a maximum of five scores) and documentation (with a maximum of ten scores) of exercise therapy programs [30]. This evaluation was conducted by two authors separately. In instances of disagreement, consultation with the third author was sought. The allocation of included studies was conducted randomly among the authors. Furthermore, the studies were cross-checked to ensure the accuracy of data extraction and to evaluate the quality of per investigation. Lastly, the review process involved two authors who independently evaluated the studies. A sub-analysis was conducted to evaluate the quality of the investigation, which was categorized regarding a TESTEX score of 10 or higher and a within-study risk evaluation ranging from low to medium.
Results
Study and participants’ characteristics
A total of 985 records were specified during the initial search. After excluding duplicate articles (n=222), the staying articles were evaluated concerning their title and abstract, resulting in the removal of 743 studies. This process yielded a final selection of 20 full-text studies. Nine additional articles were excluded due to the following rationales: a) Non-RCTs [31–37], b) Case report [38], and d) Study with active CG [39]. Eleven studies [14-24, 40-50] met our inclusion criteria and were used in the meta-analysis (PRISMA flow diagram; Figure 1).
The total number of participants in all studies was 594, with an equal number of participants (50%) in the experimental and CG (298 participants in each group). The sample size for each study ranged from 22 to 104 participants.
Intervention details
The interventions utilized by the 11 studies included in the analysis exhibited a degree of variability and encompassed scapular mobilization, muscle retraining, and stretching, as can be observed in Table 1. Among the studies, three of them specifically examined the efficacy of scapular-focused exercise training when added to conventional therapy, which employed an additive design [40, 41, 49], while six articles straightforward compared scapular-based exercise training with non-scapular-based [42–46, 50]. Two studies investigated the effect of scapular stabilization or resistance exercises [47, 48]. All included studies recruited both males and females, but one study [46] did not mention the number of each gender in each group.
Ten included studies assessed pain with activity, with a study unclearly documenting whether pain was evaluated during exercise [49]. Shoulder function including disabilities of the arm, shoulder, and hand (Quick DASH scale), shoulder pain and disability index (SPADI), and strengths and disabilities questionnaire (SDQ) was evaluated in nine investigations [40, 42–45, 47–50]. Moreover, in four studies [41, 47–49] lateral scapular slide test (LSST) was used to determine scapular dyskinesia.
Meta-analysis results
Change in shoulder pain
Eleven investigations comprising 594 individuals (298 in the experimental group and 296 in the CG, respectively) documented the outcome measure of shoulder pain. Pooled findings showed that exercise therapy produced a significant decrease in shoulder pain (SMD=-0.83; 95% CI,-1.44%, -0.22%; P=0.008) in comparison to the CG (Figure 2).
Change in shoulder function
Nine investigations, comprising a total of 482 individuals, have reported on the outcome measure of shoulder function. Upon pooling the results from the random-effects model, it was found that exercise therapy has a remarkable proper influence on shoulder function (SMD=-0.62; 95% CI, -1.08%, -0.16%; P=0.008; Figure 3).
Scapula positioning
Four studies reported scapula positioning in 0°, three studies reported scapula in 45° and 90° as an outcome measure. Upon pooling the results from the random-effects model, it was found that exercise therapy had no significant effect on scapula positioning at any angle (0°: MD=-0.44; 95% CI, -1.43%, 0.55%; P=0.38; 45°: MD=-0.17; 95% CI, -0.72%, 0.37%; P=0.53; 90°: MD=-0.25; 95% CI, -1.06%, 0.57%; P=0.56; Figure 4).
Study quality
The researchers assessed the quality of the studies that entered the analysis and determined it to be moderate. The median TESTEX score was 9, with a range of 7 to 10 out of a possible maximum point of 15. Table 2 presents the distribution of scores obtained in the aforementioned studies.
Specifically, two studies obtained a point of 10, four studies obtained a point of 9, three studies obtained a point of 8, and two studies obtained a point of 7. Of the TESTEX criteria, the following was accomplished especially poorly: Training volume and energy cost and workout monitoring in the CG 0/11; relative exercise intensity constant and preference to treat studies only 2/11 studies; allocation concealment only 3/11 studies; assessors blinded 4/11 studies. The other criteria were met in at least 50% of investigations.
Heterogeneity and publication bias
Our analyses in shoulder pain and scapula positioning at 0° revealed moderate heterogeneity (I2=74%, P<0.0001, and I2=72%, P<0.00001, respectively). However, the heterogeneity in shoulder function and scapula positioning at 90° and 45° revealed high heterogeneity (I2=82%, P<0.0001, I2=94%, P<0.00001, and I2=99%, P<0.0001, respectively). Egger plots revealed little to moderate evidence of publication bias (Figure 5a and b).
Discussion
The current systematic review and meta-analysis synthesized the existing literature regarding the impact of exercise therapy on shoulder pain, function, and scapular positioning among people diagnosed with SD. The findings indicated that, in comparison to the CG, the exercise therapy protocol proved to be a successful intervention in significantly reducing pain and enhancing shoulder function. Nevertheless, exercise therapy had no significant effect on scapula positioning at any angle. Accordingly, the hypothesis of this investigation was supported just by pain and shoulder function.
The findings of this review indicated that therapeutic exercises did not yield a statistically significant impact on scapula positioning. However, it is worth noting that these exercises demonstrated a potential positive influence on both shoulder pain and function. It is conceivable that the enhancement of joint proprioception may contribute, at least in part, to the observed improvement in therapeutic exercise outcomes. The management of SD necessitates addressing the overall biomechanics of the body, rather than solely focusing on a specific region such as the shoulder, neck, trunk, or pelvis. Given that the human body functions as a kinetic chain, it is worth considering the incorporation of scapular-focused exercise therapy and the examination of scapular biomechanics in conjunction with neighboring segments [51].
Shoulder pathology management should include evaluation and administration of the scapula position and motion. Frequently, scapular position and motion findings promote determining management options, rehabilitation protocols and return to activity [52]. SD is a condition that is generally linked to shoulder pathology and regarded as a risk factor for more injury; however, it is additionally present in asymptomatic people [20]. Evidence recommends that scapular motion disorders such as reduced scapular UR, limited scapular posterior tipping, and ER can cause rotator cuff–related shoulder pain [9, 53, 54]. It has been suggested that the weakness of scapular muscles can be an influential factor in unusual scapular kinematics [55 56]. Notably, enhanced facilitation of the UT with inhibition of the LT and SA has been linked to changed scapular position and motion [5]. Nevertheless, it is not clear if these differences are compensatory strategies or causative factors [20, 57].
In subjects displaying scapular dyskinesia, a lack of flexibility or strength in a particular agonistic muscle, which is then compensated by the antagonist’s muscle [58], may result in the onset of shoulder pain [18, 52, 54] due to a decrease in subacromial space, dysfunction of the shoulder griddle, and eventually structural damage [58], as well as an increase in mechanical stress on the soft tissue of glenohumeral [59].
This study comprised 11 trials with different therapeutic exercises including scapular flexibility, strengthening, and stability exercises given to intervention groups [41, 46, 49], scapular control and dynamic scapular stability [42, 50], neuromuscular training and per scapular strengthening [43], stretching and strengthening exercises [33, 40, 44, 45], stabilization exercise [47, 60], home exercise program, and resistive training with proper resistance of Thera band [48].
The lack of scapular stability appears to be a crucial factor in the enhancement of shoulder pain and disability. The efficacy of therapeutic exercise in retraining motor skills and activating stabilization muscles has been observed to have a positive impact on scapular kinematics. Therefore, it is recommended that this approach be included as part of a multidisciplinary treatment plan. The scapular-focused interventions that can include various exercises are often suggested for shoulder pain and disability in subjects with scapular dyskinesia. However, several studies of moderate to high quality have managed to yield strong evidence about the efficacy and safety of these interventions.
Struyf et al. (2013) concluded that a large clinically meaningful treatment effect favoring scapular motor control training was observed in dysfunction. A notable reduction in pain of moderate to large clinical significance was observed during the administration of the Hawkins test, Neer test, and empty can test. Furthermore, the experimental group illustrated an average decrease in self-perceived pain while at rest, as measured by the visual analog scale (VAS), whereas the CG did not exhibit any changes. The observed outcomes remained consistent during the three-month follow-up period [50]. Further, scapula-focused motor control and muscular strengthening exercises can affect subjects’ resting position, scapular movement patterns, and improved function of the affected shoulder in subjects with SIS [43].
Engebretsen et al. (2011) observed a substantial alteration between the supervised scapular control and dynamic scapular stability and radial extracorporeal shock-wave therapy groups after 18 weeks. However, the findings indicated that there was no reported therapeutic advantage of scapular stability compared to radial extracorporeal shock-wave therapy in this particular group of individuals during the 1-year follow-up period. A smaller number of patients in the scapular stability group underwent supplementary interventions [42]. Furthermore, there is empirical substantiation that corroborates the efficacy of scapular stabilization exercises as a form of exercise therapy for reducing pain and facilitating rehabilitation in people with SIS [46] demonstrated through statistical and clinical evidence that combining stretching and strengthening exercises is more effective than solely performing these exercises for enhancing the strength of the scapular muscles, preventing shoulder dysfunction, and enhancing the sense of joint position [41].
Besides, the study of Shah et al. (2014) [49] supported the hypothesis that there will be significant relief with the use of scapular stability exercises in patients with SIS. Hence, it was concluded that there is a significant difference between conventional exercise alone and conventional exercise therapy and scapular stability exercises in relieving pain and improving physical function in SIS, as seen with the VAS shoulder pain, disability index, and lateral scapular stability test. After four weeks of treatment, a significant improvement in pain and functional status was detected in patients performing conventional exercise therapy and scapular stability exercises rather than performing conventional exercise therapy alone [49].
Strengths and limitations /future research
Our findings will be more convincing thanks to a thorough search of English databases, reliable quality assessment, and a useful analysis methodology used in this systematic review and meta-analysis. It is important to acknowledge certain limitations. One potential limitation of this study is the restriction to articles published exclusively in English. This approach may overlook relevant research published in other languages, potentially leading to an incomplete representation of the topic under investigation. One additional limitation is the potential for significant heterogeneity to arise, which can have a detrimental impact on participants’ conclusions and baseline characteristics. The examination of publication bias was not carried out as a result of the restricted quantity of studies encompassed, particularly concerning scapula positioning. Given the restricted accessibility of outcome data for certain research endeavors and the comparably diminutive quantity of research endeavors that were encompassed, it is sensible to exercise prudence when comprehending the conclusions of this particular investigation.
Conclusion
To sum up, in the final analysis, our systematic review and meta-analysis revealed that exercise therapy protocols have a positive impact on pain reduction and functional improvement among individuals with scapular dyskinesia. However, no significant alterations in scapula positioning were observed as a result of these interventions. Additional long-term and rigorous trials are necessary to evaluate and validate the results presented in this study.
Ethical Considerations
Compliance with ethical guidelines
This systematic review and meta-analysis study is regarded exclusively on published literature.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology and investigation: All authors; Methodology: Nasser Mohammad Rahimi; Writing original draft: Mahdi Esfahani and Mohammad Khodaverdizadeh; Review and editing: Nasser Mohammad Rahimi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Department of Sports Sciences, Imam Reza International University.
References
- Kamonseki DH, Calixtre LB, Barreto RPG, Camargo PR. Effects of electromyographic biofeedback interventions for shoulder pain and function: Systematic review and meta-analysis. Clinical Rehabilitation. 2021; 35(7):952-963.[DOI:10.1177/0269215521990950] [PMID]
- Page MJ, O'Connor DA, Malek M, Haas R, Beaton D, Huang H, et al. Patients' experience of shoulder disorders: A systematic review of qualitative studies for the OMERACT Shoulder Core Domain Set. Rheumatology. 2019:kez046. [DOI:10.1093/rheumatology/kez046] [PMID]
- Camargo PR, Neumann DA. Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 2: trapezius. Brazilian Journal of Physical Therapy. 2019; 23(6):467-75. [DOI:10.1016/j.bjpt.2019.01.011] [PMID]
- Michener LA, Sharma S, Cools AM, Timmons MK. Relative scapular muscle activity ratios are altered in subacromial pain syndrome. Journal of Shoulder and Elbow Surgery. 2016; 25(11):1861-7. [DOI:10.1016/j.jse.2016.04.010] [PMID]
- Huang TS, Ou HL, Huang CY, Lin JJ. Specific kinematics and associated muscle activation in individuals with scapular dyskinesis. Journal of Shoulder and Elbow Surgery. 2015; 24(8):1227-34. [DOI:10.1016/j.jse.2014.12.022] [PMID]
- De Mey K, Danneels L, Cagnie B, Cools AM. Scapular muscle rehabilitation exercises in overhead athletes with impingement symptoms: Effect of a 6-week training program on muscle recruitment and functional outcome. The American Journal of Sports Medicine. 2012; 40(8):1906-15. [DOI:10.1177/0363546512453297] [PMID]
- Mottram SL. Dynamic stability of the scapula. Manual Therapy. 1997; 2(3):123-31. [DOI:10.1054/math.1997.0292] [PMID]
- Hwang M, Lee S, Lim C. Effects of the proprioceptive neuromuscular facilitation technique on scapula function in office workers with scapula dyskinesis. Medicina. 2021; 57(4):332. [DOI:10.3390/medicina57040332] [PMID]
- Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Physical Therapy. 2000; 80(3):276-91. [DOI:10.1093/ptj/80.3.276]
- Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF. Motion of the shoulder complex during multiplanar humeral elevation. The Journal of Bone and Joint Surgery. 2009; 91(2):378-89. [DOI:10.2106/JBJS.G.01483] [PMID]
- Ha SM, Kwon OY, Yi CH, Cynn HS, Weon JH, Kim TH. Effects of scapular upward rotation exercises on alignment of scapula and clavicle and strength of scapular upward rotators in subjects with scapular downward rotation syndrome. Journal of Electromyography and Kinesiology. 2016; 26:130-6. [DOI:10.1016/j.jelekin.2015.12.007] [PMID]
- Kibler WB, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the 'Scapular Summit'. British Journal of Sports Medicine. 2013; 47(14):877-85. [DOI:10.1136/bjsports-2013-092425] [PMID]
- Kibler WB, Sciascia A. Current concepts: Scapular dyskinesis. British Journal of Sports Medicine. 2010; 44(5):300-5. [DOI:10.1136/bjsm.2009.058834] [PMID]
- Hibberd EE, Oyama S, Spang JT, Prentice W, Myers JB. Effect of a 6-week strengthening program on shoulder and scapular-stabilizer strength and scapular kinematics in division I collegiate swimmers. Journal of Sport Rehabilitation. 2012; 21(3):253-65. [DOI:10.1123/jsr.21.3.253] [PMID]
- Page P. Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. International Journal of Sports Physical Therapy. 2011; 6(1):51-8. [PMID] [PMCID]
- Page P. Cervicogenic headaches: an evidence-led approach to clinical management. International Journal of Sports Physical Therapy. 2011; 6(3):254-66.[PMID] [PMCID]
- Kang JH, Park RY, Lee SJ, Kim JY, Yoon SR, Jung KI. The effect of the forward head posture on postural balance in long time computer based worker. Annals of Rehabilitation Medicine. 2012; 36(1):98-104. [DOI:10.5535/arm.2012.36.1.98] [PMID]
- Hickey D, Solvig V, Cavalheri V, Harrold M, Mckenna L. Scapular dyskinesis increases the risk of future shoulder pain by 43% in asymptomatic athletes: A systematic review and meta-analysis. British Journal of Sports Medicine. 2018; 52(2):102-10. [DOI:10.1136/bjsports-2017-097559] [PMID]
- Pluim BM. Scapular dyskinesis: Practical applications. British Journal of Sports Medicine. 2013; 47(14):875-6. [DOI:10.1136/bjsports-2013-092722] [PMID]
- Burn MB, McCulloch PC, Lintner DM, Liberman SR, Harris JD. Prevalence of scapular dyskinesis in overhead and nonoverhead athletes: A systematic review. Orthopaedic Journal of Sports Medicine. 2016; 4(2):2325967115627608. [DOI:10.1177/2325967115627608] [PMID]
- Cools AM, Struyf F, De Mey K, Maenhout A, Castelein B, Cagnie B. Rehabilitation of scapular dyskinesis: From the office worker to the elite overhead athlete. British Journal of Sports Medicine. 2014; 48(8):692-7. [DOI:10.1136/bjsports-2013-092148] [PMID]
- Gebremariam L, Hay EM, van der Sande R, Rinkel WD, Koes BW, Huisstede BM. Subacromial impingement syndrome--effectiveness of physiotherapy and manual therapy. British Journal of Sports Medicine. 2014; 48(16):1202-8. [DOI:10.1136/bjsports-2012-091802] [PMID]
- Lopes AD, Timmons MK, Grover M, Ciconelli RM, Michener LA. Visual scapular dyskinesis: kinematics and muscle activity alterations in patients with subacromial impingement syndrome. Archives of Physical Medicine and Rehabilitation. 2015; 96(2):298-306. [DOI:10.1016/j.apmr.2014.09.029] [PMID]
- Reijneveld EA, Noten S, Michener LA, Cools A, Struyf F. Clinical outcomes of a scapular-focused treatment in patients with subacromial pain syndrome: A systematic review. British Journal of Sports Medicine. 2017; 51(5):436-41. [DOI:10.1136/bjsports-2015-095460] [PMID]
- Haik MN, Alburquerque-Sendín F, Moreira RF, Pires ED, Camargo PR. Effectiveness of physical therapy treatment of clearly defined subacromial pain: A systematic review of randomised controlled trials. British Journal of Sports Medicine. 2016; 50(18):1124-34. [DOI:10.1136/bjsports-2015-095771] [PMID]
- Bury J, West M, Chamorro-Moriana G, Littlewood C. Effectiveness of scapula-focused approaches in patients with rotator cuff related shoulder pain: A systematic review and meta-analysis. Manual Therapy. 2016; 25:35-42. [DOI:10.1016/j.math.2016.05.337] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. Journal of Clinical Epidemiology. 2021; 134:103-12. [DOI:10.1016/j.jclinepi.2021.03.001] [PMID]
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327(7414):557-60. [DOI:10.1136/bmj.327.7414.557] [PMID]
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315(7109):629-34. [DOI:10.1136/bmj.315.7109.629] [PMID]
- Smart NA, Waldron M, Ismail H, Giallauria F, Vigorito C, Cornelissen V, et al. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. International Journal of Evidence-Based Healthcare. 2015; 13(1):9-18. [DOI:10.1097/XEB.0000000000000020] [PMID]
- Alshami AM, AlSadiq AI. The effects of scapulothoracic mobilization in patients with neck pain and scapular dyskinesis: A single-blind, randomized, clinical trial. 2020; [Unpublished]. [DOI:10.21203/rs.3.rs-41441/v1]
- Uga D, Nakazawa R, Sakamoto M. Strength and muscle activity of shoulder external rotation of subjects with and without scapular dyskinesis. Journal of Physical Therapy Science. 2016; 28(4):1100-5. [DOI:10.1589/jpts.28.1100] [PMID]
- Camargo PR, Alburquerque-Sendín F, Avila MA, Haik MN, Vieira A, Salvini TF. Effects of stretching and strengthening exercises, with and without manual therapy, on scapular kinematics, function, and pain in individuals with shoulder impingement: A randomized controlled trial. The Journal of Orthopaedic and Sports Physical Therapy. 2015; 45(12):984-97. [DOI:10.2519/jospt.2015.5939] [PMID]
- Pekgöz F, Taşkıran H, Kaya Mutlu E, Atalay A, Çeliker R. Comparison of mobilization with supervised exercise for patients with subacromial impingement syndrome. Turkish Journal of Physical Medicine and Rehabilitation. 2020; 66(2):184-92. [DOI:10.5606/tftrd.2020.3649] [PMID]
- Miller P, Osmotherly P. Does scapula taping facilitate recovery for shoulder impingement symptoms? A pilot randomized controlled trial. The Journal of Manual & Manipulative Therapy. 2009; 17(1):E6-13.[DOI:10.1179/jmt.2009.17.1.6E] [PMID]
- Vergili O, Oktas B, Canbeyli ID. Comparison of kinesiotaping, exercise and subacromial injection treatments on functionality and life quality in shoulder impingement syndrome: A randomized controlled study. Indian Journal of Orthopaedics. 2021; 55(1):195-202. [DOI:10.1007/s43465-020-00167-7] [PMID]
- Sharma S, Ghrouz AK, Hussain ME, Sharma S, Aldabbas M, Ansari S. Progressive resistance exercises plus manual therapy is effective in improving isometric strength in overhead athletes with shoulder impingement syndrome: A randomized controlled trial. BioMed Research International. 2021; 2021:9945775. [DOI:10.1155/2021/9945775] [PMID]
- Kim JT, Kim SY, Oh DW. An 8-week scapular stabilization exercise program in an elite archer with scapular dyskinesis presenting joint noise: A case report with one-year follow-up. Physiotherapy Theory and Practice. 2019; 35(2):183-9. [DOI:10.1080/09593985.2018.1442538] [PMID]
- Granviken F, Vasseljen O. Home exercises and supervised exercises are similarly effective for people with subacromial impingement: A randomised trial. Journal of Physiotherapy. 2015; 61(3):135-41. [DOI:10.1016/j.jphys.2015.05.014] [PMID]
- Aytar A, Baltaci G, Uhl TL, Tuzun H, Oztop P, Karatas M. The effects of scapular mobilization in patients with subacromial impingement syndrome: A randomized, double-blind, placebo-controlled clinical trial. Journal of Sport Rehabilitation. 2015; 24(2):116-29. [DOI:10.1123/jsr.2013-0120] [PMID]
- Başkurt Z, Başkurt F, Gelecek N, Özkan MH. The effectiveness of scapular stabilization exercise in the patients with subacromial impingement syndrome. Journal of Back and Musculoskeletal Rehabilitation. 2011; 24(3):173-9. [DOI:10.3233/BMR-2011-0291] [PMID]
- Engebretsen K, Grotle M, Bautz-Holter E, Ekeberg OM, Juel NG, Brox JI. Supervised exercises compared with radial extracorporeal shock-wave therapy for subacromial shoulder pain: 1-Year results of a single-blind randomized controlled trial. Physical Therapy. 2011; 91(1):37-47. [DOI:10.2522/ptj.20090338] [PMID]
- Hotta GH, Santos AL, McQuade KJ, de Oliveira AS. Scapular-focused exercise treatment protocol for shoulder impingement symptoms: Three-dimensional scapular kinematics analysis. Clinical Biomechanics. 2018; 51:76-81. [DOI:10.1016/j.clinbiomech.2017.12.005] [PMID]
- Letafatkar A, Rabiei P, Kazempour S, Alaei-Parapari S. Comparing the effects of no intervention with therapeutic exercise, and exercise with additional Kinesio tape in patients with shoulder impingement syndrome. A three-arm randomized controlled trial. Clinical Rehabilitation. 2021; 35(4):558-67.[DOI:10.1177/0269215520971764] [PMID]
- Ludewig PM, Borstad JD. Effects of a home exercise programme on shoulder pain and functional status in construction workers. Occupational and Environmental Medicine. 2003; 60(11):841-9.[DOI:10.1136/oem.60.11.841] [PMID]
- Moezy A, Sepehrifar S, Solaymani Dodaran M. The effects of scapular stabilization based exercise therapy on pain, posture, flexibility and shoulder mobility in patients with shoulder impingement syndrome: A controlled randomized clinical trial. Medical Journal of the Islamic Republic of Iran. 2014; 28:87. [PMID] [PMCID]
- Nowotny J, Kasten P, Kopkow C, Biewener A, Mauch F. Evaluation of a new exercise program in the treatment of scapular dyskinesis. International Journal of Sports Medicine. 2018; 39(10):782-90. [DOI:10.1055/a-0608-4584] [PMID]
- Pekyavas NO, Ergun N. Comparison of virtual reality exergaming and home exercise programs in patients with subacromial impingement syndrome and scapular dyskinesis: Short term effect. Acta Orthopaedica et Traumatologica Turcica. 2017; 51(3):238-42. [DOI:10.1016/j.aott.2017.03.008] [PMID]
- Shah M, Sutaria J, Khant A. Effectiveness of scapular stability exercises in the patient with the shoulder impingement syndrome. Indian Journal of Physical Therapy. 2014; 2(1):79-84. [Link]
- Struyf F, Nijs J, Mollekens S, Jeurissen I, Truijen S, Mottram S, et al. Scapular-focused treatment in patients with shoulder impingement syndrome: A randomized clinical trial. Clinical Rheumatology. 2013; 32(1):73-85. [DOI:10.1007/s10067-012-2093-2] [PMID]
- Özdemir F, Toy Ş, Kızılay F, Avcı ZT, Altay Z, Çolak C. Effects of scapular stabilization exercises in patients of chronic neck pain with scapular dyskinesis: A quasi-experimental study. Turkish Journal of Physical Medicine and Rehabilitation. 2021; 67(1):77. [DOI:10.5606/tftrd.2021.6775] [PMID]
- Kibler WB, Sciascia A, Wilkes T. Scapular dyskinesis and its relation to shoulder injury. The Journal of the American Academy of Orthopaedic Surgeons. 2012; 20(6):364-72. [DOI:10.5435/JAAOS-20-06-364] [PMID]
- McClure PW, Michener LA, Karduna AR. Shoulder function and 3-dimensional scapular kinematics in people with and without shoulder impingement syndrome. Physical Therapy. 2006; 86(8):1075-90. [DOI:10.1093/ptj/86.8.1075] [PMID]
- Timmons MK, Thigpen CA, Seitz AL, Karduna AR, Arnold BL, Michener LA. Scapular kinematics and subacromial-impingement syndrome: A meta-analysis. Journal of Sport Rehabilitation. 2012; 21(4):354-70. [DOI:10.1123/jsr.21.4.354] [PMID]
- Cools AM, Witvrouw EE, Declercq GA, Vanderstraeten GG, Cambier DC. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement symptoms. British Journal of Sports Medicine. 2004; 38(1):64-8. [DOI:10.1136/bjsm.2003.004952] [PMID]
- Leong HT, Tsui SS, Ng GY, Fu SN. Reduction of the subacromial space in athletes with and without rotator cuff tendinopathy and its association with the strength of scapular muscles. Journal of Science and Medicine in Sport. 2016; 19(12):970-4. [DOI:10.1016/j.jsams.2016.03.011] [PMID]
- Myers JB, Oyama S, Hibberd EE. Scapular dysfunction in high school baseball players sustaining throwing-related upper extremity injury: A prospective study. Journal of Shoulder and Elbow Surgery. 2013; 22(9):1154-9. [DOI:10.1016/j.jse.2012.12.029] [PMID]
- Page P, Frank C, Lardner R. Assessment and treatment of muscle imbalance: The Janda approach. Champaign: Human kinetics; 2010. [DOI:10.5040/9781718211445]
- Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clinical Biomechanics. 2003; 18(5):369-79. [DOI:10.1016/S0268-0033(03)00047-0] [PMID]
- Turgut E, Duzgun I, Baltaci G. Effects of scapular stabilization exercise training on scapular kinematics, disability, and pain in subacromial impingement: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation. 2017; 98(10):1915-23. [DOI:10.1016/j.apmr.2017.05.023] [PMID]
Article type: Reviews |
Subject:
Sport rehabilitation
Received: 2022/10/20 | Accepted: 2023/09/23 | Published: 2023/12/1
Received: 2022/10/20 | Accepted: 2023/09/23 | Published: 2023/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
