
988368
Thu, May 28, 2026

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 767-774 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hajian P, Guitinavard F, Bateni F S. Pulmonary Embolism and Deep Vein Thrombosis Presenting as Anxiety, Akathisia, and Aggression in a Bipolar Patient: A Case Report From Iran. Iranian Rehabilitation Journal 2023; 21 (4) :767-774
URL: http://irj.uswr.ac.ir/article-1-1799-en.html
URL: http://irj.uswr.ac.ir/article-1-1799-en.html



1- Psychosis Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Urology, Urology Research Center, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
2- Department of Urology, Urology Research Center, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Keywords: Venous thromboembolism, Pulmonary embolism (PE), Bipolar disorder, Restlessness, Mortality, Psychiatric ward
Full-Text [PDF 5032 kb]
(998 Downloads)
| Abstract (HTML) (3082 Views)
Full-Text: (637 Views)
Introduction
Mortality from cardiovascular causes, including pulmonary embolism (PE), is the second most common cause of mortality in psychiatric patients [1]. PE has a wide range of clinical presentations and classically manifests with sudden pleuritic chest pain and unexplained dyspnea [2]. Signs and symptoms that are specific to PE include tachycardia, dyspnea chest pain, and hemoptysis. Many of these clinical characteristics are included in clinical prediction rules, such as the Wells pre-test probability score for deep vein thrombosis (DVT) or PE or the Geneva score for PE [3]. It rarely manifests as acute psychosis [4] and other unspecific signs and symptoms.
Many common treatment modalities for psychiatric disorders increase the risk of coagulopathies, particularly antipsychotic medications [5] and conditions, such as catatonia are associated with an increased incidence of venous thromboembolism (VTE) [6]. PE is a relatively common and largely preventable cause of death for psychiatric patients [7]. Therefore, we present this case to emphasize the importance of thromboembolic complications in psychiatric patients, especially hospitalized patients.
Case Presentation
On 16 May 2021, a 56-year-old woman was hospitalized a week before admission due to aggression. In the interview, she said only two sentences: “ Doctor, help me please!”, “I am not good”. Her brother reported that she had been impulsive, and verbally aggressive ever since. She was insecure and was thinking some people were chasing her. She was also restless, disturbed, and uncomfortable and was walking most of the time.
Her symptoms first appeared 27 years ago with elevated mood, grandiosity delusion, and increased religious beliefs. Since then, she has been hospitalized more than 6 times “with a diagnosis of the bipolar spectrum”. She lived in a care center from 20 years ago until last year and lived with her brother for the last year. She had no history of suicide or suicidal thoughts.
In past medical history, she had hypertension and hypothyroidism which were controlled and under treatment. Before admission, she was given medication, including citalopram 20 mg per os (PO) daily, doxepin 10 mg PO daily, olanzapine 10 mg PO nightly, losartan 25 mg PO daily, and nightly, amlodipine 5 mg PO daily, A.S.A 80 mg PO daily, levothyroxine 0.1 mg PO daily.
The psychiatric evaluation of the patient revealed a middle-aged woman who appeared to be her biological age. She was restless and had akathisia; therefore, she paced the examination room during the interview. She repeated two sentences and was uncooperative during the first full interview and psychiatric evaluation.
Investigations
On admission, vital signs were blood pressure 128.85, heart rate 75, and respiratory rate 18, the rest of the systemic examination was normal. An electrocardiogram (ECG) showed a normal sinus rate and normal heart axis (Figure 1).
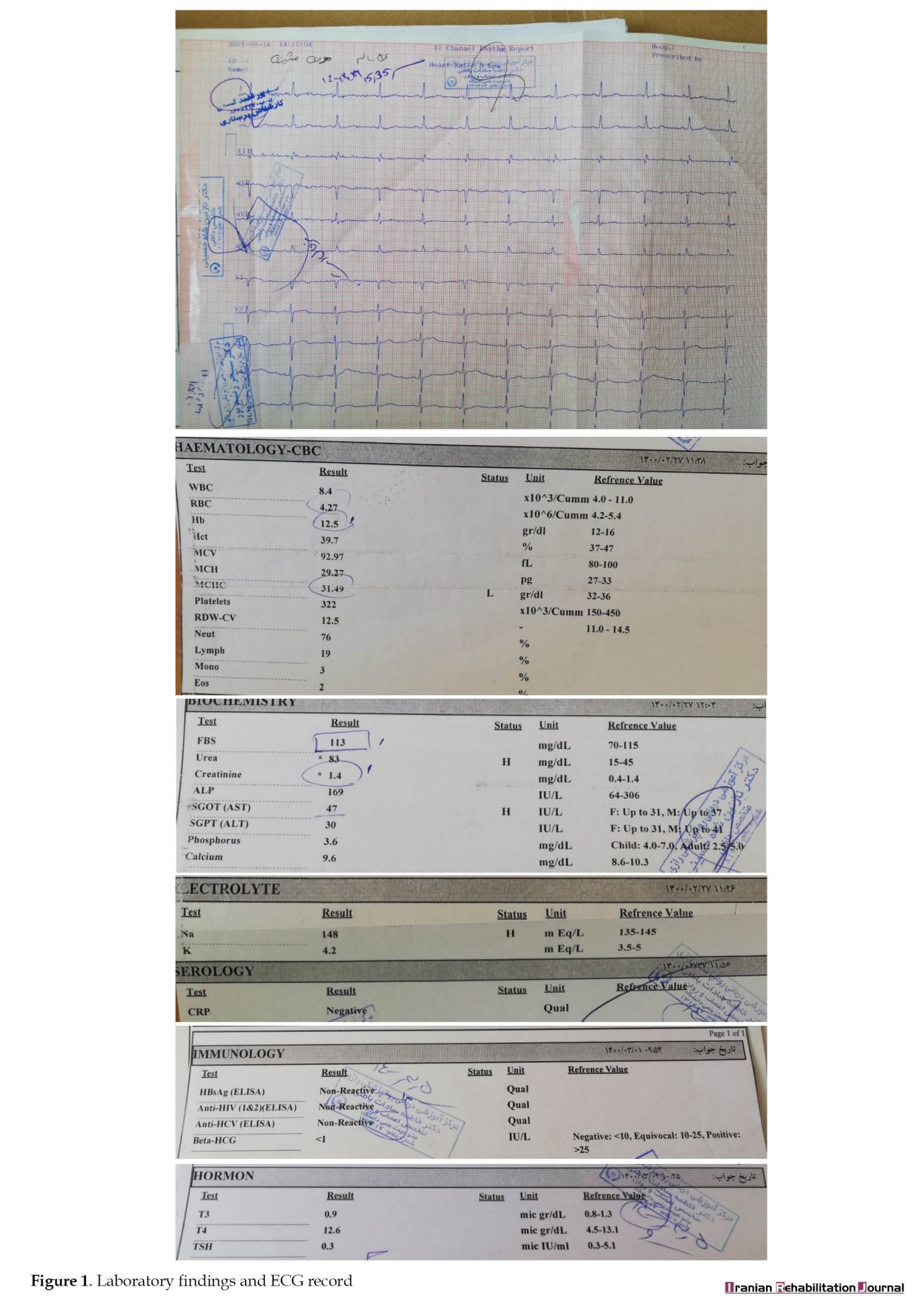
 Blood tests show mild anemia with hemoglobin 12.5 gr/dL, white cell count 8400, platelets 322000, C-reactive protein was negative, electrolytes were in the normal range, fasting blood glucose (FBS) 113 mg/dL, creatinine 1.4 mg/dL, urea 83 mg/dL, thyroid stimulating hormone (TSH) 0.3 micro IU/mL and polymerase chain reaction (PCR) for COVID-19 was negative (Figure 1).
Blood tests show mild anemia with hemoglobin 12.5 gr/dL, white cell count 8400, platelets 322000, C-reactive protein was negative, electrolytes were in the normal range, fasting blood glucose (FBS) 113 mg/dL, creatinine 1.4 mg/dL, urea 83 mg/dL, thyroid stimulating hormone (TSH) 0.3 micro IU/mL and polymerase chain reaction (PCR) for COVID-19 was negative (Figure 1).
Based on available information, a diagnosis of “unspecified and related bipolar disorder” with akathisia (possibly doxepin and selective serotonin reuptake inhibitor [SSRI] induced) was considered. On the Barnes Akathisia rating scale, her total score was 11. Initially, doxepin, citalopram, and olanzapine were tapered. Also, sodium valproate tablet 200 mg/qid and propranolol tablet 20 mg/bid were added to her drugs, according to the considered diagnosis.
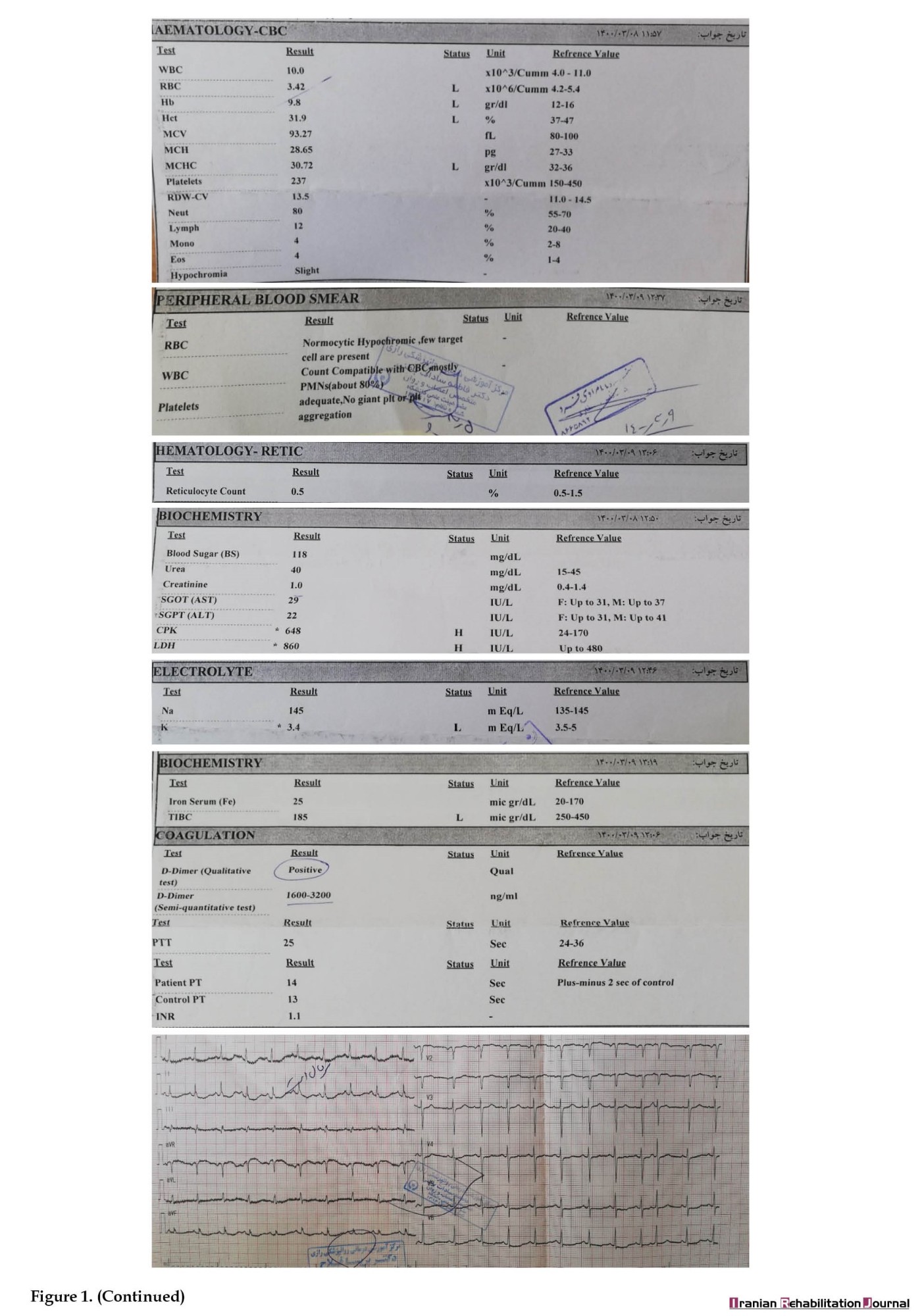
After two weeks, not only no progress in relieving symptoms was observed, but also the symptoms of restlessness, akathisia, and anxiety became severe. During the daily evaluation and monitoring of vital signs, tachycardia was detected. After consultation with an internal medicine specialist, ECG, complete blood count, peripheral blood smear, retic count, blood sugar, urea, creatinine, serum glutamic-oxaloacetic transaminase (SGOT), serum glutamate-pyruvate transaminase (SGPT), creatine phosphokinase, lactate dehydrogenase, D-dimer, urine analysis and urine culture were requested.
According to tachycardia detected in ECG (Figure 1), high level of D-dimer, and low saturation, we considered thromboembolism, and the patient was sent to a general hospital. After diagnostic evaluation in that center, including computed tomography (CT) angiography and color Doppler ultrasound, the diagnosis of thromboembolism was confirmed for the patient (Figure 2).
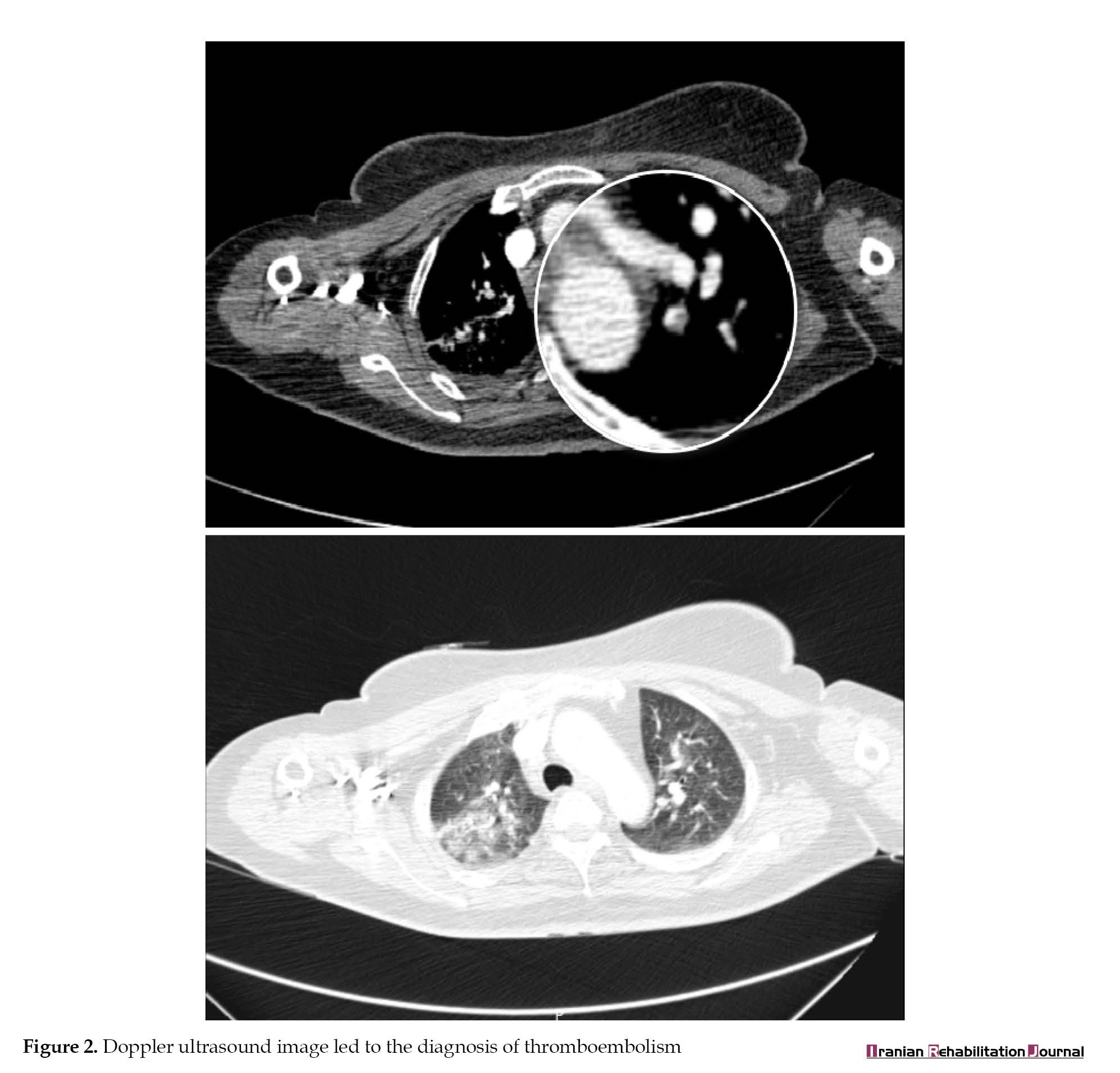 She received anticoagulants for a week in that center and then was returned to Razi Psychiatric Hospital to continue the treatment.
She received anticoagulants for a week in that center and then was returned to Razi Psychiatric Hospital to continue the treatment.
Discussion
PE is a relatively common and largely preventable cause of death for psychiatric patients [7]. Evidence shows a significantly increased risk of venous thromboembolism and PE in antipsychotic users compared to non-users [8]. A chart review study in Japan between May 1, 2009, and April 30, 2017, showed that catatonia was associated with an increased incidence of VTE [6-8]. According to the study conducted by Barbosa et al., among the causes of death in “unit of a Portuguese general hospital among the acute psychiatric inpatients,” the main causes were circulatory system disorders (66.66%), mainly PE (28.57%) and stroke (14.29%) [7]. Also, according to the study conducted by Shinde et al. in India, the leading cause of death among inpatients of a psychiatric hospital was cardiovascular disorders (43.6%), and only (6.9%) of subjects died due to suicide [9]. Studies showed that the main clinical symptom of vein thromboembolism in patients was chest tightness (36.16%) [10], which is a common chief complaint in psychiatric patients.
Therefore, one of the vital causes of death in psychiatric wards is VTE. Psychiatric drugs and conditions, including catatonia, increase the risk of VTE, on the other hand, VTE in psychiatric patients, can show unspecific signs and symptoms. All these reasons make the diagnosis of VTE difficult in psychiatric patients and can increase the risk of misdiagnosis. Therefore, psychiatrists must pay attention to this diagnosis, and always perform essential assessments and evaluations for patients with clinical suspicion.
Conclusion
We publish this case to raise awareness of thromboembolic complications in psychiatric patients, especially hospitalized patients. The main concern in psychiatric wards has always been the risk of suicide of the patients, although suicide is one of the causes of death in the psychiatric ward, cardiovascular events led by embolism are the leading cause of death in psychiatric hospitals. Therefore, psychiatrists should always consider cardiovascular diseases, including VTE, in suspicious patients in the psychiatric ward to reduce the mortality rate in psychiatric wards.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Fatemeh Sadat Bateni; Investigation and writing:Pouya Hajian; Data collection: Fatemeh Guitinavard.
Conflict of interest
The authors declared no conflict of interest.
References
Mortality from cardiovascular causes, including pulmonary embolism (PE), is the second most common cause of mortality in psychiatric patients [1]. PE has a wide range of clinical presentations and classically manifests with sudden pleuritic chest pain and unexplained dyspnea [2]. Signs and symptoms that are specific to PE include tachycardia, dyspnea chest pain, and hemoptysis. Many of these clinical characteristics are included in clinical prediction rules, such as the Wells pre-test probability score for deep vein thrombosis (DVT) or PE or the Geneva score for PE [3]. It rarely manifests as acute psychosis [4] and other unspecific signs and symptoms.
Many common treatment modalities for psychiatric disorders increase the risk of coagulopathies, particularly antipsychotic medications [5] and conditions, such as catatonia are associated with an increased incidence of venous thromboembolism (VTE) [6]. PE is a relatively common and largely preventable cause of death for psychiatric patients [7]. Therefore, we present this case to emphasize the importance of thromboembolic complications in psychiatric patients, especially hospitalized patients.
Case Presentation
On 16 May 2021, a 56-year-old woman was hospitalized a week before admission due to aggression. In the interview, she said only two sentences: “ Doctor, help me please!”, “I am not good”. Her brother reported that she had been impulsive, and verbally aggressive ever since. She was insecure and was thinking some people were chasing her. She was also restless, disturbed, and uncomfortable and was walking most of the time.
Her symptoms first appeared 27 years ago with elevated mood, grandiosity delusion, and increased religious beliefs. Since then, she has been hospitalized more than 6 times “with a diagnosis of the bipolar spectrum”. She lived in a care center from 20 years ago until last year and lived with her brother for the last year. She had no history of suicide or suicidal thoughts.
In past medical history, she had hypertension and hypothyroidism which were controlled and under treatment. Before admission, she was given medication, including citalopram 20 mg per os (PO) daily, doxepin 10 mg PO daily, olanzapine 10 mg PO nightly, losartan 25 mg PO daily, and nightly, amlodipine 5 mg PO daily, A.S.A 80 mg PO daily, levothyroxine 0.1 mg PO daily.
The psychiatric evaluation of the patient revealed a middle-aged woman who appeared to be her biological age. She was restless and had akathisia; therefore, she paced the examination room during the interview. She repeated two sentences and was uncooperative during the first full interview and psychiatric evaluation.
Investigations
On admission, vital signs were blood pressure 128.85, heart rate 75, and respiratory rate 18, the rest of the systemic examination was normal. An electrocardiogram (ECG) showed a normal sinus rate and normal heart axis (Figure 1).
Based on available information, a diagnosis of “unspecified and related bipolar disorder” with akathisia (possibly doxepin and selective serotonin reuptake inhibitor [SSRI] induced) was considered. On the Barnes Akathisia rating scale, her total score was 11. Initially, doxepin, citalopram, and olanzapine were tapered. Also, sodium valproate tablet 200 mg/qid and propranolol tablet 20 mg/bid were added to her drugs, according to the considered diagnosis.
After two weeks, not only no progress in relieving symptoms was observed, but also the symptoms of restlessness, akathisia, and anxiety became severe. During the daily evaluation and monitoring of vital signs, tachycardia was detected. After consultation with an internal medicine specialist, ECG, complete blood count, peripheral blood smear, retic count, blood sugar, urea, creatinine, serum glutamic-oxaloacetic transaminase (SGOT), serum glutamate-pyruvate transaminase (SGPT), creatine phosphokinase, lactate dehydrogenase, D-dimer, urine analysis and urine culture were requested.
According to tachycardia detected in ECG (Figure 1), high level of D-dimer, and low saturation, we considered thromboembolism, and the patient was sent to a general hospital. After diagnostic evaluation in that center, including computed tomography (CT) angiography and color Doppler ultrasound, the diagnosis of thromboembolism was confirmed for the patient (Figure 2).
Discussion
PE is a relatively common and largely preventable cause of death for psychiatric patients [7]. Evidence shows a significantly increased risk of venous thromboembolism and PE in antipsychotic users compared to non-users [8]. A chart review study in Japan between May 1, 2009, and April 30, 2017, showed that catatonia was associated with an increased incidence of VTE [6-8]. According to the study conducted by Barbosa et al., among the causes of death in “unit of a Portuguese general hospital among the acute psychiatric inpatients,” the main causes were circulatory system disorders (66.66%), mainly PE (28.57%) and stroke (14.29%) [7]. Also, according to the study conducted by Shinde et al. in India, the leading cause of death among inpatients of a psychiatric hospital was cardiovascular disorders (43.6%), and only (6.9%) of subjects died due to suicide [9]. Studies showed that the main clinical symptom of vein thromboembolism in patients was chest tightness (36.16%) [10], which is a common chief complaint in psychiatric patients.
Therefore, one of the vital causes of death in psychiatric wards is VTE. Psychiatric drugs and conditions, including catatonia, increase the risk of VTE, on the other hand, VTE in psychiatric patients, can show unspecific signs and symptoms. All these reasons make the diagnosis of VTE difficult in psychiatric patients and can increase the risk of misdiagnosis. Therefore, psychiatrists must pay attention to this diagnosis, and always perform essential assessments and evaluations for patients with clinical suspicion.
Conclusion
We publish this case to raise awareness of thromboembolic complications in psychiatric patients, especially hospitalized patients. The main concern in psychiatric wards has always been the risk of suicide of the patients, although suicide is one of the causes of death in the psychiatric ward, cardiovascular events led by embolism are the leading cause of death in psychiatric hospitals. Therefore, psychiatrists should always consider cardiovascular diseases, including VTE, in suspicious patients in the psychiatric ward to reduce the mortality rate in psychiatric wards.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Fatemeh Sadat Bateni; Investigation and writing:Pouya Hajian; Data collection: Fatemeh Guitinavard.
Conflict of interest
The authors declared no conflict of interest.
References
- Hansen V, Jacobsen BK, Arnesen E. Cause-specific mortality in psychiatric patients after deinstitutionalisation. The British Journal of psychiatry. 2001; 179:438-43. [DOI:10.1192/bjp.179.5.438] [PMID]
- Alhassan S, Pelinescu A, Gandhi V, Naddour M, Singh AC, Bihler E. Clinical presentation and risk factors of venous thromboembolic disease. Critical Care Nursing Quarterly. 2017; 40(3):201-9. [DOI:10.1097/CNQ.0000000000000159] [PMID]
- Bauersachs RM. Clinical presentation of deep vein thrombosis and pulmonary embolism. Best practice & research. 2012; 25(3):243-51. [DOI:10.1016/j.beha.2012.07.004] [PMID]
- Co MLF, Agdamag AC, Esteban MJ, Mateo R. Massive pulmonary embolism presenting initially as acute psychosis. BMJ Case Reports. 2019; 12(4):e222018. [DOI:10.1136/bcr-2017-222018] [PMID] [PMCID]
- Zhang R, Dong L, Shao F, Tan X, Ying K. Antipsychotics and venous thromboembolism risk: A meta-analysis. Pharmacopsychiatry. 2011; 44(5):183-8. [DOI:10.1055/s-0031-1280814] [PMID]
- Ishida T, Sakurai H, Watanabe K, Iwashita S, Mimura M, Uchida H. Incidence of deep vein thrombosis in catatonic patients: A chart review. Psychiatry Research. 2016; 241:61-5. [DOI:10.1016/j.psychres.2016.04.105] [PMID]
- Barbosa S, Sequeira M, Castro S, Manso R, Klut Câmara C, Trancas B, et al. Causes of death in an acute psychiatric inpatient unit of a portuguese general hospital. Acta Medica Portuguesa. 2016; 29(7-8):468-75. [DOI:10.20344/amp.6905] [PMID]
- Liu Y, Xu J, Fang K, Xu Y, Gao J, Zhou C, et al. Current antipsychotic agent use and risk of venous thromboembolism and pulmonary embolism: A systematic review and meta-analysis of observational studies. Therapeutic Advances in Psychopharmacology. 2021; 11:2045125320982720. [DOI:10.1177/2045125320982720] [PMID]
- Gong B, Xu Q, Pang Y, Hu J. [Clinical features of patients with venous thromboembolism: 177 case analysis in 10 years (Chinese)]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019; 31(4):453-7. [DOI:10.3760/cma.j.issn.2095-4352.2019.04.016] [PMID]
- Shinde SS, Nagarajaiah, Narayanaswamy JC, Viswanath B, Kumar NC, Gangadhar BN, et al. Mortality among inpatients of a psychiatric hospital: Indian perspective. Indian Journal of Psychological Medicine. 2014; 36(2):142-6. [DOI:10.4103/0253-7176.130974] [PMID]
Article type: Case Reports |
Subject:
Psychiatry
Received: 2022/10/23 | Accepted: 2023/05/6 | Published: 2023/12/1
Received: 2022/10/23 | Accepted: 2023/05/6 | Published: 2023/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
