
988368
Thu, Jul 30, 2026

Volume 22, Issue 1 (March 2024)
Iranian Rehabilitation Journal 2024, 22(1): 47-54 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Havaei N, Kashefimehr B, Huri̇ M, Bowyer P, Saei S. Validation of the Persian Version of Short Child Occupational Profile in Iranian Population. Iranian Rehabilitation Journal 2024; 22 (1) :47-54
URL: http://irj.uswr.ac.ir/article-1-1804-en.html
URL: http://irj.uswr.ac.ir/article-1-1804-en.html



1- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, Tabriz University of Medical Sciences, Tabriz, Iran.
2- Department of Occupational Therapy, Faculty of Health Sciences, Hacettepe University, Ankara, Turkey.
3- Department of Occupational Therapy, Texas Woman’s University, Denton, United States.
4- Department of Occupational Therapy, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Occupational Therapy, Faculty of Health Sciences, Hacettepe University, Ankara, Turkey.
3- Department of Occupational Therapy, Texas Woman’s University, Denton, United States.
4- Department of Occupational Therapy, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 519 kb]
(972 Downloads)
| Abstract (HTML) (3476 Views)
Full-Text: (895 Views)
Introduction
Occupational therapy is the use of purposeful activities to maximize independence, prevent disability, and maintain health for people suffering from functional, psychological, social, and developmental limitations, learning disabilities, poverty, and cultural differences, or the aging process due to injury or disease, which includes assessment, treatment, and counseling processes [1].
In the area of children, occupational therapists utilize standard tests to detect the need for occupational therapy interventions, select the best, most appropriate, and most effective intervention, and finally assess the child’s progress following the provided interventions. A standard occupational performance assessment tool assesses the child in specific occupational areas and provides an opportunity for the child’s condition to be used and interpreted by other occupational therapists and specialists by providing a criterion score. On the other hand, the use of specific therapeutic models and approaches is one of the things that defines occupational therapists’ professional identity and provides the necessary integration and coherence in interventions. In recent years much emphasis has been placed on the use of specific occupational therapy models and their related assessment tools [2].
Model of human occupation (MOHO) is one of the popular and evidence-based occupational therapy models used by many occupational therapists and several assessment tools have been developed based on it [3].
MOHO emphasizes explaining the voluntary processes, habits, and patterns that direct and build people’s participation in the occupations. Performances are underlined by motor skills, process skills, communication skills, and interactions. Besides, the mental experiences of involving in an occupation are determinative. MOHO is a well-researched strategy that enables you to engage more deeply with children, adolescents, and their families by identifying their motivations and putting them into action to promote higher health and well-being [4]. In the assessment of children and the selection of assessment tools, less attention is paid to evaluating performance [5], and more to examining physical structure. While, according to the international classification of functioning (ICF) and the occupational therapy practice framework (OTPF4), the level of participation and performance should be the goal of the intervention [6].
Short child occupational profile (SCOPE), designed by Bowyer [7], is a screening tool based on MOHO and examines occupational domains according to this model. It is occupation-based and evaluates the levels of volition, habits, skills, and limitations of a child in the environment. SCOPE does not directly assess performance capacities, but rather addresses the child’s skills. Skills are goal-directed actions used to perform the occupations. In contrast to performance capacity, which relates to inherent ability, skills refer to defined functional acts. SCOPE is used to measure several aspects of functional abilities in children and adolescents aged 3 to 21 years. Another characteristic of SCOPE is that it records individuals’ development via occupational therapy treatments and identifies areas that need occupational therapy intervention. SCOPE ratings are based on the growth process specific to each child. It helps anticipate obstacles in the course of progress and thereby enables therapists to detect children’s abilities and their potential challenges [8, 9].
According to the MOHO structures, SCOPE evaluates the domains of volition, habits, skills, and environment [7]. According to previous studies, based on the level of ability, the SCOPE questionnaire provides scores in six occupational and skill domains [10]. In each domain, scores of 4 and 1 indicate the highest and the lowest ability. The score of each domain is determined by summing the scores, and the total score of the questionnaire is the product of the summed scores of six domains. Therefore, a higher score will be indicative of better functioning.
SCOPE as a theoretical base tool to assess the child’s occupational participation and the facilitating level of the environment encourages and helps the therapist process reasoning with a holistic and client-centered view while helping develop self-belief and professional identity [11]. It is a theoretically-based questionnaire that supports interventions by professional principals and evaluates child abilities without comparing them with other children; it compares them only with an earlier situation of their abilities.
Because such a tool or a questionnaire in Persian is not available, it is necessary to prepare this questionnaire to facilitate using the occupational therapy principles and models by Iranian occupational therapists in various fields. Since SCOPE has not been translated into Persian in Iran, this study aims to prepare and validate a Persian version of this assessment tool.
Materials and Methods
Participants
A total of 182 clients, selected by convenience sampling, referred to the comprehensive rehabilitation centers and occupational therapy clinics in Tabriz City, Iran, during six months from July 2021 to January 2022 participated in this study. The inclusion criteria included an age range from 3-21 years and their willingness to participate in this study was obtained by filing a consent form. Trained occupational therapist practitioners reviewed the SCOPE, version 2.2, for all clients of the occupational therapy unit. The therapist has answered the questions of the questionnaire using her clinical observations as well as the explanations of the parents and clients (if able).
Diagnosis such as attention deficit and hyperactivity (ADHD) cerebral palsy (CP), and autism were considered prevalent diagnoses (>5 cases) and were included in the study.
Participants were classified into two groups of normal (n=103) and diagnosed with chronic disease (n=79). The normal group consists of the client’s family members (sisters, brothers, or cousins) who do not have a history of disability and who are examined by the same therapists in the same way as the clients. The disabled participants were diagnosed with ADHD, CP, and autism (prevalent clients). Other types of clients (diagnosis <5) were not included in the study. Demographic data of participants were obtained by a checklist designed by the researchers.
Procedure
We conducted this methodological research in two stages. In the first stage, we translated and culturally adapted the questionnaire appropriately, and then validated the final version using the content validity and internal and external reliability of the questionnaire. Finally, we assessed the discriminant construct validity of the questionnaire in the normal and disabled groups. This study was ethically approved (details omitted for double-anonymized peer review).
According to studies on the translation and adaptation of questionnaires [12], we first obtained permission from the SCOPE developer and then translated the English version of this questionnaire separately using the forward translation method by four professors fluent in English practicing in the field of medical sciences to evaluate the linguistic validation. Then, the translations were compared by a committee consisting of four translators, and needed linguistic and cultural adaptations were made to the meanings, and a Persian version was prepared.
Backward translation
In the next stage, one of the professors fluent in English who was not aware of the content of the initial questionnaire, and an official translator performed a backward translation (from Persian to English). We submitted the last version to the developer of the questionnaire for approval, and the group of translators examined the raised comments.
Cultural and linguistic adaptations of SCOPE can enable the inclusion of a broader study population and enhance the generalizability of results. However, if a measure has not been adapted or translated appropriately, then the population may not understand what is being asked of them. Therefore, the data collected from the measure may not accurately reflect the underlying construct(s) of interest [13].
The required corrections were made in the Persian version considering these comments. Then, we evaluated the validity and reliability of the questionnaire using this version (pre-final) to prepare the final version.
In general, the validity of a questionnaire determines the extent to which the measurement tool measures the intended feature, and content validity indicates the extent to which a scale (questionnaire) measures all aspects of the target structure. The content validity of the present questionnaire was approved by the participation of 20 experts. Validity is measured by several methods, and the most commonly used one is content validity via calculating content validity ratio (CVR) and content validity index (CVI). Twenty specialists (eight occupational therapists, three physiotherapists, four psychologists, and five speech therapists) evaluated content validation. This evaluation included analyzing the necessity of items CVR, clarity, relevance, and simplicity of items CVI. The acceptance scores of items were ≥0.42 and ≥0.79 in the CVR and CVI methods, respectively [14]. The construct validity was evaluated by the discriminant validity method, in which comparisons were made among the questionnaires filled in by the normal and disabled participants. To perform the evaluation, the main researcher trained the related therapists using standard videotapes and scales provided by the SCOPE developer. Considering the high volume of items assessed by the questionnaire, CVI and CVR were reported as a range.
The reliability of the questionnaire was analyzed by internal consistency and test re-test reliability. For test re-test, the therapist performed the first assessment, and the second one two weeks later on the same participants (n=30).
Data analysis
The content validity was evaluated by CVR and CVI methods. Construct validity (discriminant validity) was assessed by comparing the normal and disabled groups using an independent t-test. The internal consistency of the questionnaire was calculated by the Cronbach's α coefficient and test re-test reliability by the intraclass correlation coefficient (ICC) method. Data were analyzed by SPSS software, version 25. P<0.05 indicated statistical significance.
Results
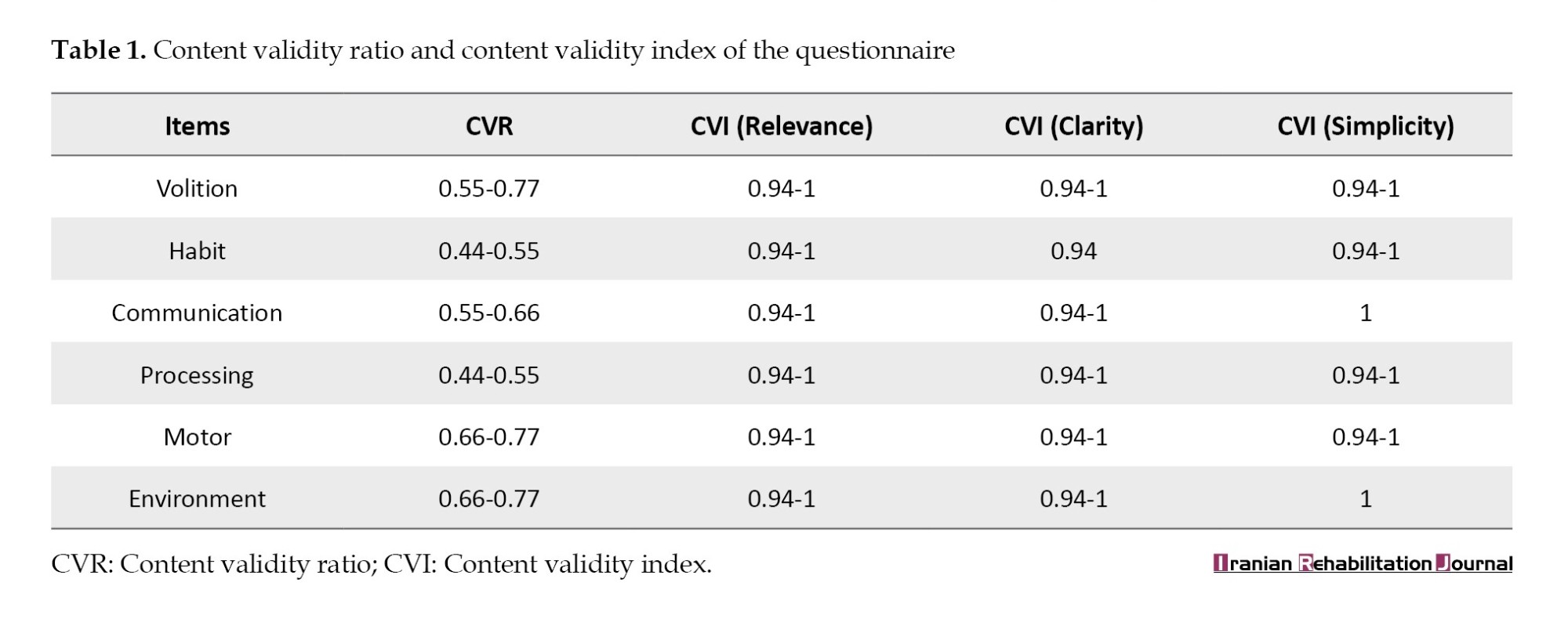
Regarding the number of specialists (n=20) participating in the expert panel, the acceptance scores of items were ≥0.42 and ≥0.79 in the CVR and CVI methods, respectively [14]. The results of the content validity of the questionnaire (CVR & CVI) are presented in Table 1.
According to demographic data, 182 clients who completed the consent form were available to examine the discriminant construct validity of this questionnaire in a cross-sectional descriptive manner. The demographic information of participants is presented in Table 2.
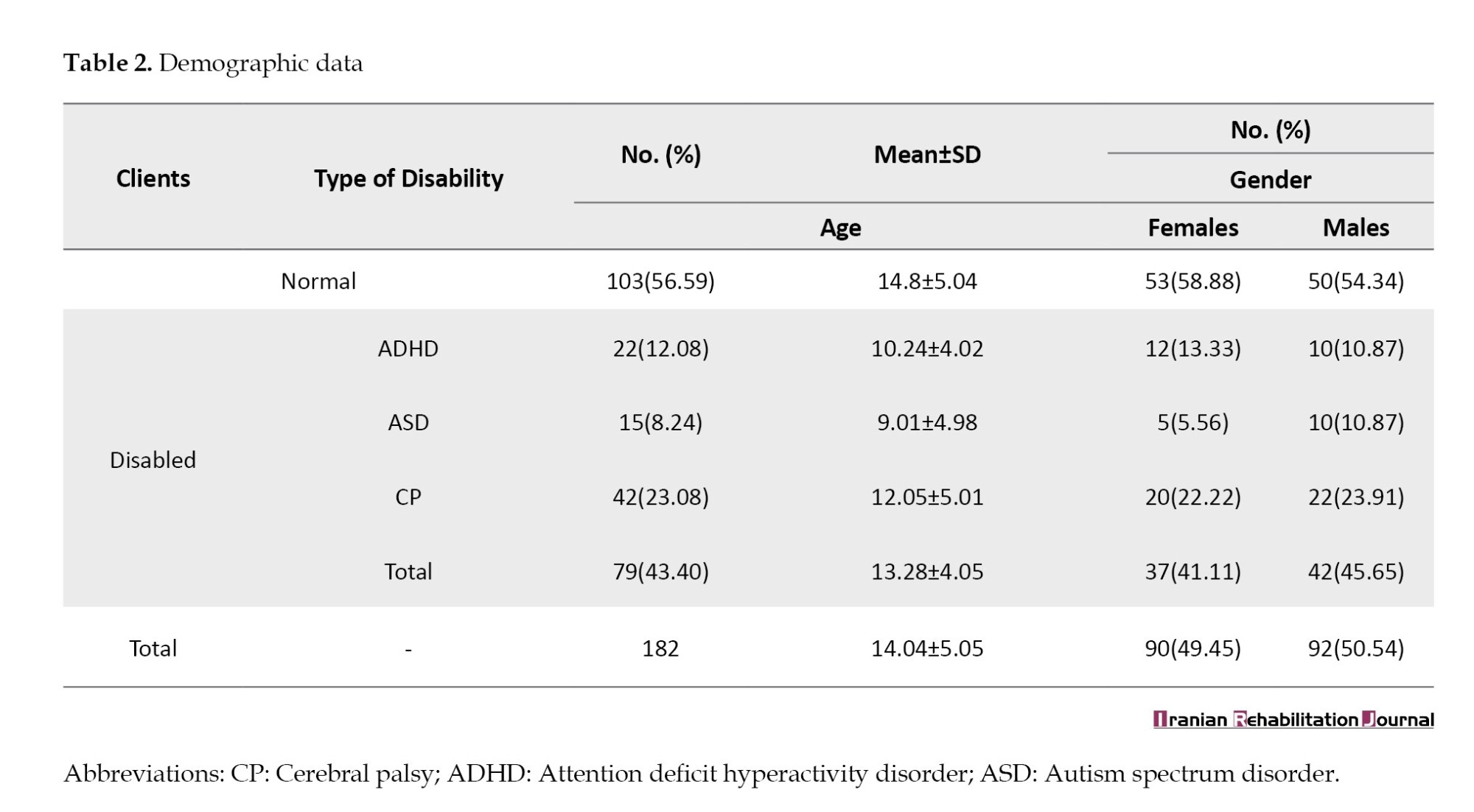
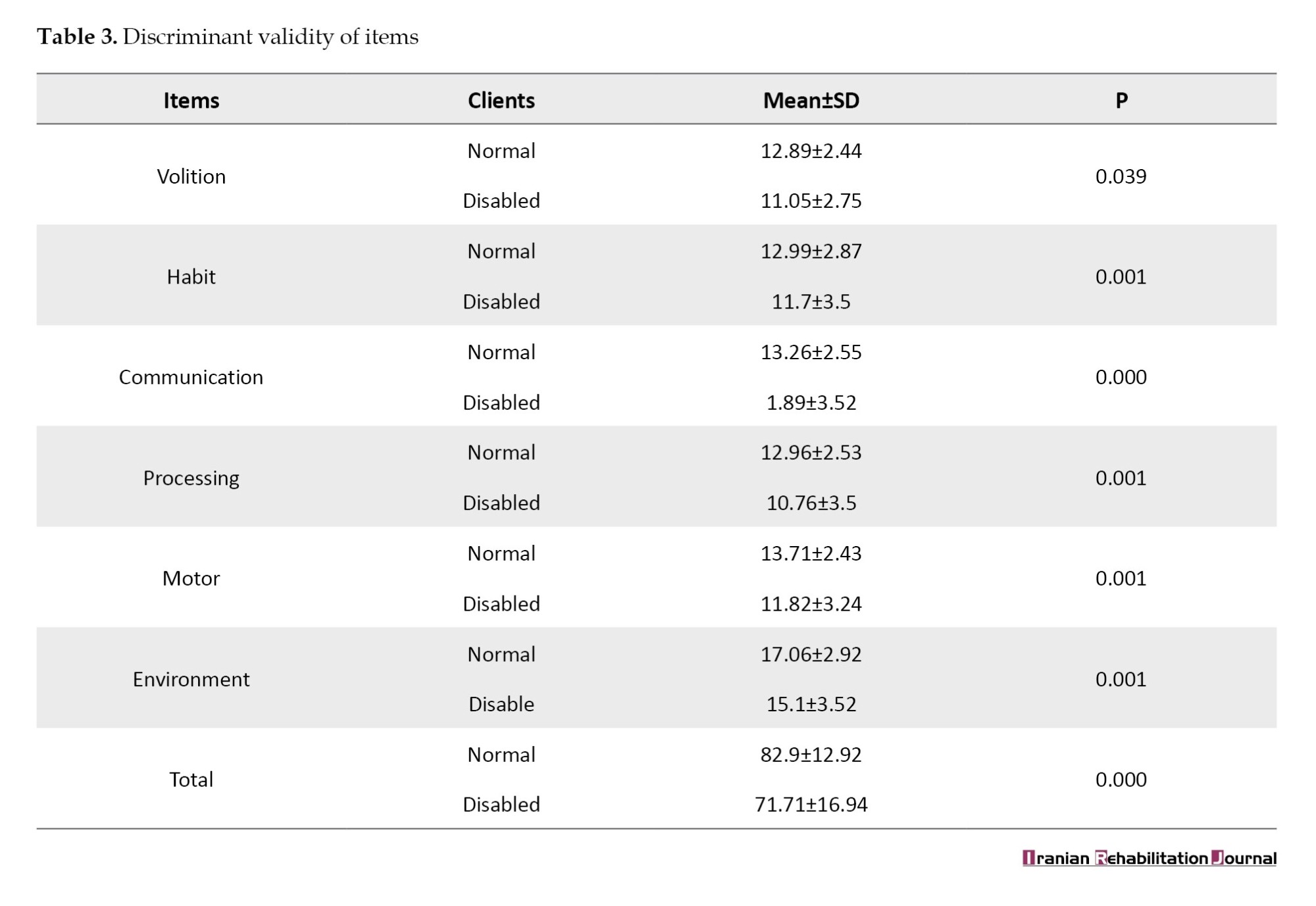
Table 3 shows the results of construct validity (discriminant validity) between the normal and disabled groups. The lower scores belong to the disabled group, including ADHD, CP, and autism. These results show significant differences between the normal and disabled groups in all questionnaire items. This means this questioner could distinguish between normal and disabled groups.
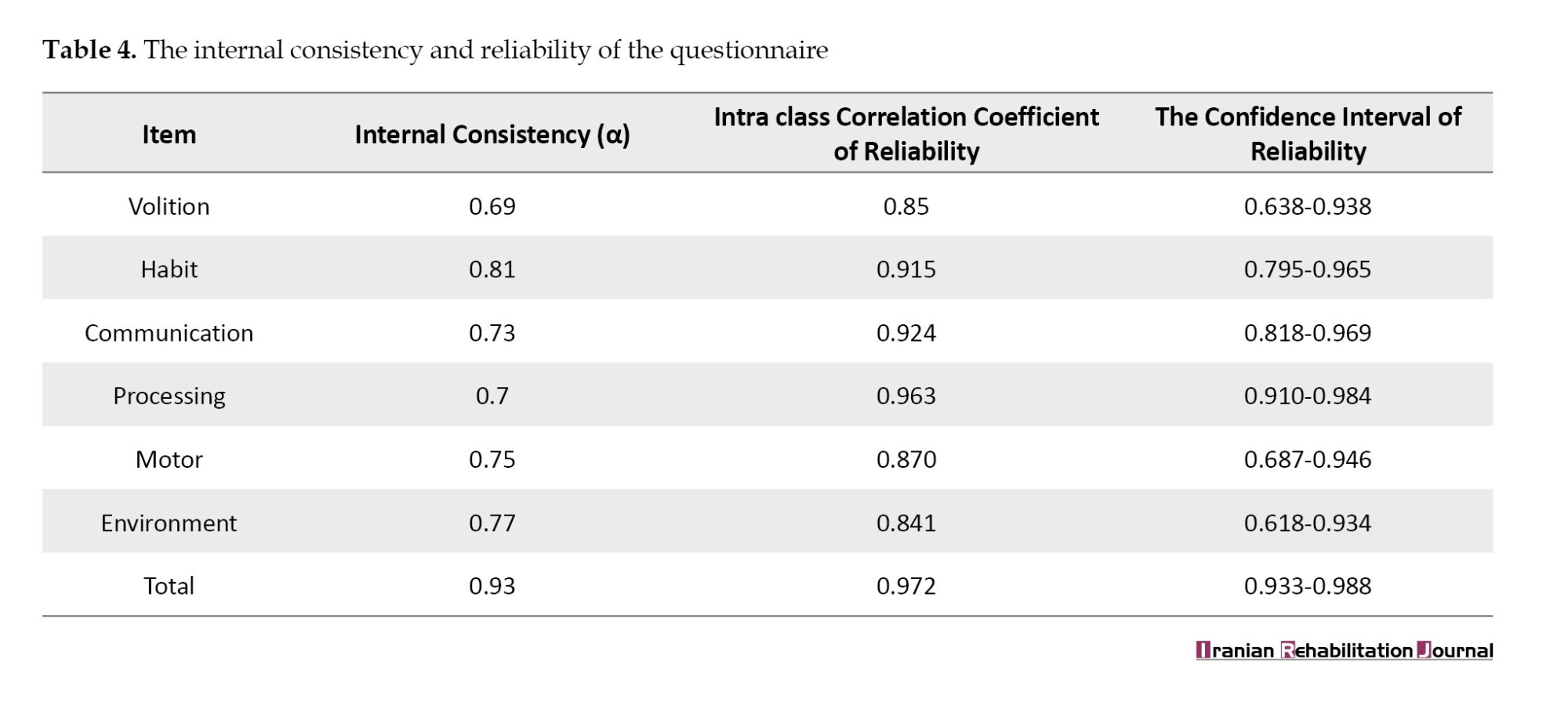
A total of 30 subjects participated to evaluate the test re-test reliability of the questionnaire. The results indicate the stability of the answers in all items of the questionnaire. The internal consistency of the questionnaire was confirmed by the results of the Cronbach's α in the evaluated subjects (Table 4).
Discussion
Child therapeutic interventions have specific characteristics related to the importance of interactions and children’s participation in daily activities; On the other hand, occupational therapists emphasize these factors [1]. Various occupational therapy services focus on occupational performance; these services are provided individually, in groups, or social systems. In line with the main goal of occupational therapists to increase occupational performance levels in different areas and the health of clients, proper evaluation of occupational performance is necessary.
An effective and targeted intervention will not be possible without analyzing occupational domains. Moreover, clinicians and treatment systems need specialized standard tools to evaluate the results of interventions and recovery rates. This questionnaire will be an efficient tool to achieve these goals. Since the Persian translation of this questionnaire was valid and reliable, this measurement tool can be useful for clinicians and rehabilitation systems.
SCOPE questionnaire was translated by a common scientific method [15]. This method was also used to translate this questionnaire into the Portuguese language [16]. It was statistically validated after the approval by the team of translators and the publisher of the questionnaire. Since the employed team of translators was related to the concepts of the questionnaire with high insights into the subject matter, along with the appropriate consultation with the questionnaire developer, this translation acquired the appropriate quality in terms of maintaining the meaning and understanding of the concepts, with no problems at the validation stages.
Based on recorded demographic information (Table 2), as well as the characteristics and age range defined for the questionnaire [17], the demographic characteristics of the studied samples were of appropriate age balance and gender distribution in the normal and disabled groups. The discriminant validity of the questionnaire was acceptable, as evidenced by the results of this study, which were obtained from scores of normal samples with no function-affecting disease, as well as those obtained from samples with function-affecting diseases and diagnoses (ADHD, CP, and autism) in the statistical population. Similar results were obtained in a sample translated into Turkish [18]. A previous study of SCOPE supported the psychometric soundness of the instrument overall [6].
The results of the study by Bowyer et al. indicate that practitioners’ decisions to use SCOPE in practice mainly regard the assessment’s top-down and occupation focus and its ability to facilitate family-centered care [19].
Therefore, based on the goals of researchers and presented needs which are reported by Shafaroodi et al. (2017) [11], translating and reviewing the psychometric properties of SCOPE can draw the attention of the Iranian community of occupational therapists to top-down and client-center concepts of occupational therapy and clinically facilitate them.
Considering the importance of stability and reliability of the questionnaire in our study, the internal consistency of results obtained in the statistical sample and the Cronbach's α findings indicate high consistency in questions related to each domain. Moreover, the test re-test evaluation in 30 separate samples indicates the good reliability of the questionnaire in different domains (0.7-0.9), which is in agreement with the study that translated the questionnaire into Turkish [18].
However, the unequal numbers of normal and disabled samples can influence the obtained results which can be considered in supplementary studies. Studying with a larger and more homogeneous statistical population, a more complete statistical analysis and the calculation of criterion validity can be recommended in future studies. It will be possible to analyze the factors connected to the effect of application and the scope of use of this questionnaire by interviewing occupational therapists and assessing the prevalence of employing the questionnaire in future research.
Conclusion
The Persian version of the SCOPE questionnaire can be used as a valid and reliable tool by child therapists, in particular, occupational therapists. Persian version of this questionnaire has the potential to turn into a practical guide to evaluate the occupational performance levels of people aged 3-21 years. It can facilitate the therapists’ emphasis on functional skills in treatment without interpersonal comparisons and only by comparing the before and after conditions of clients. Having a suitable and easy-to-use clinical tool is a good opportunity to motivate therapists to apply the relevant theoretical concepts. Due to a lack of practical questionnaires in the domains of occupational performance, therapists may have relied on non-occupational questionnaires, resulting in the rise in popularity of bottom-up treatments. Examining this idea in supplementary studies can be enlightening. On the other hand, the existence of standard and valid tools for documentation and follow-up of clients, as well as strong interaction with other disciplines is of great advantage provided by this questionnaire for occupational therapists in governmental and private health systems.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Tabriz University of Medical Sciences (Code: IR.TBZMED.REC.1398.136).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Naser Havaei and Babak Kashefimehr; Investigation: Meral Huri and Patricia Bowyer; Resources: Naser Havaei; Methodology and writing the original draft: Shafagh Saei; Review and editing: Babak Kashefimehr and Patricia Bowyer; Supervision: Babak Kashefimehr and Meral Huri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the translation support group which was willing to participate in this study.
References
Occupational therapy is the use of purposeful activities to maximize independence, prevent disability, and maintain health for people suffering from functional, psychological, social, and developmental limitations, learning disabilities, poverty, and cultural differences, or the aging process due to injury or disease, which includes assessment, treatment, and counseling processes [1].
In the area of children, occupational therapists utilize standard tests to detect the need for occupational therapy interventions, select the best, most appropriate, and most effective intervention, and finally assess the child’s progress following the provided interventions. A standard occupational performance assessment tool assesses the child in specific occupational areas and provides an opportunity for the child’s condition to be used and interpreted by other occupational therapists and specialists by providing a criterion score. On the other hand, the use of specific therapeutic models and approaches is one of the things that defines occupational therapists’ professional identity and provides the necessary integration and coherence in interventions. In recent years much emphasis has been placed on the use of specific occupational therapy models and their related assessment tools [2].
Model of human occupation (MOHO) is one of the popular and evidence-based occupational therapy models used by many occupational therapists and several assessment tools have been developed based on it [3].
MOHO emphasizes explaining the voluntary processes, habits, and patterns that direct and build people’s participation in the occupations. Performances are underlined by motor skills, process skills, communication skills, and interactions. Besides, the mental experiences of involving in an occupation are determinative. MOHO is a well-researched strategy that enables you to engage more deeply with children, adolescents, and their families by identifying their motivations and putting them into action to promote higher health and well-being [4]. In the assessment of children and the selection of assessment tools, less attention is paid to evaluating performance [5], and more to examining physical structure. While, according to the international classification of functioning (ICF) and the occupational therapy practice framework (OTPF4), the level of participation and performance should be the goal of the intervention [6].
Short child occupational profile (SCOPE), designed by Bowyer [7], is a screening tool based on MOHO and examines occupational domains according to this model. It is occupation-based and evaluates the levels of volition, habits, skills, and limitations of a child in the environment. SCOPE does not directly assess performance capacities, but rather addresses the child’s skills. Skills are goal-directed actions used to perform the occupations. In contrast to performance capacity, which relates to inherent ability, skills refer to defined functional acts. SCOPE is used to measure several aspects of functional abilities in children and adolescents aged 3 to 21 years. Another characteristic of SCOPE is that it records individuals’ development via occupational therapy treatments and identifies areas that need occupational therapy intervention. SCOPE ratings are based on the growth process specific to each child. It helps anticipate obstacles in the course of progress and thereby enables therapists to detect children’s abilities and their potential challenges [8, 9].
According to the MOHO structures, SCOPE evaluates the domains of volition, habits, skills, and environment [7]. According to previous studies, based on the level of ability, the SCOPE questionnaire provides scores in six occupational and skill domains [10]. In each domain, scores of 4 and 1 indicate the highest and the lowest ability. The score of each domain is determined by summing the scores, and the total score of the questionnaire is the product of the summed scores of six domains. Therefore, a higher score will be indicative of better functioning.
SCOPE as a theoretical base tool to assess the child’s occupational participation and the facilitating level of the environment encourages and helps the therapist process reasoning with a holistic and client-centered view while helping develop self-belief and professional identity [11]. It is a theoretically-based questionnaire that supports interventions by professional principals and evaluates child abilities without comparing them with other children; it compares them only with an earlier situation of their abilities.
Because such a tool or a questionnaire in Persian is not available, it is necessary to prepare this questionnaire to facilitate using the occupational therapy principles and models by Iranian occupational therapists in various fields. Since SCOPE has not been translated into Persian in Iran, this study aims to prepare and validate a Persian version of this assessment tool.
Materials and Methods
Participants
A total of 182 clients, selected by convenience sampling, referred to the comprehensive rehabilitation centers and occupational therapy clinics in Tabriz City, Iran, during six months from July 2021 to January 2022 participated in this study. The inclusion criteria included an age range from 3-21 years and their willingness to participate in this study was obtained by filing a consent form. Trained occupational therapist practitioners reviewed the SCOPE, version 2.2, for all clients of the occupational therapy unit. The therapist has answered the questions of the questionnaire using her clinical observations as well as the explanations of the parents and clients (if able).
Diagnosis such as attention deficit and hyperactivity (ADHD) cerebral palsy (CP), and autism were considered prevalent diagnoses (>5 cases) and were included in the study.
Participants were classified into two groups of normal (n=103) and diagnosed with chronic disease (n=79). The normal group consists of the client’s family members (sisters, brothers, or cousins) who do not have a history of disability and who are examined by the same therapists in the same way as the clients. The disabled participants were diagnosed with ADHD, CP, and autism (prevalent clients). Other types of clients (diagnosis <5) were not included in the study. Demographic data of participants were obtained by a checklist designed by the researchers.
Procedure
We conducted this methodological research in two stages. In the first stage, we translated and culturally adapted the questionnaire appropriately, and then validated the final version using the content validity and internal and external reliability of the questionnaire. Finally, we assessed the discriminant construct validity of the questionnaire in the normal and disabled groups. This study was ethically approved (details omitted for double-anonymized peer review).
According to studies on the translation and adaptation of questionnaires [12], we first obtained permission from the SCOPE developer and then translated the English version of this questionnaire separately using the forward translation method by four professors fluent in English practicing in the field of medical sciences to evaluate the linguistic validation. Then, the translations were compared by a committee consisting of four translators, and needed linguistic and cultural adaptations were made to the meanings, and a Persian version was prepared.
Backward translation
In the next stage, one of the professors fluent in English who was not aware of the content of the initial questionnaire, and an official translator performed a backward translation (from Persian to English). We submitted the last version to the developer of the questionnaire for approval, and the group of translators examined the raised comments.
Cultural and linguistic adaptations of SCOPE can enable the inclusion of a broader study population and enhance the generalizability of results. However, if a measure has not been adapted or translated appropriately, then the population may not understand what is being asked of them. Therefore, the data collected from the measure may not accurately reflect the underlying construct(s) of interest [13].
The required corrections were made in the Persian version considering these comments. Then, we evaluated the validity and reliability of the questionnaire using this version (pre-final) to prepare the final version.
In general, the validity of a questionnaire determines the extent to which the measurement tool measures the intended feature, and content validity indicates the extent to which a scale (questionnaire) measures all aspects of the target structure. The content validity of the present questionnaire was approved by the participation of 20 experts. Validity is measured by several methods, and the most commonly used one is content validity via calculating content validity ratio (CVR) and content validity index (CVI). Twenty specialists (eight occupational therapists, three physiotherapists, four psychologists, and five speech therapists) evaluated content validation. This evaluation included analyzing the necessity of items CVR, clarity, relevance, and simplicity of items CVI. The acceptance scores of items were ≥0.42 and ≥0.79 in the CVR and CVI methods, respectively [14]. The construct validity was evaluated by the discriminant validity method, in which comparisons were made among the questionnaires filled in by the normal and disabled participants. To perform the evaluation, the main researcher trained the related therapists using standard videotapes and scales provided by the SCOPE developer. Considering the high volume of items assessed by the questionnaire, CVI and CVR were reported as a range.
The reliability of the questionnaire was analyzed by internal consistency and test re-test reliability. For test re-test, the therapist performed the first assessment, and the second one two weeks later on the same participants (n=30).
Data analysis
The content validity was evaluated by CVR and CVI methods. Construct validity (discriminant validity) was assessed by comparing the normal and disabled groups using an independent t-test. The internal consistency of the questionnaire was calculated by the Cronbach's α coefficient and test re-test reliability by the intraclass correlation coefficient (ICC) method. Data were analyzed by SPSS software, version 25. P<0.05 indicated statistical significance.
Results
Regarding the number of specialists (n=20) participating in the expert panel, the acceptance scores of items were ≥0.42 and ≥0.79 in the CVR and CVI methods, respectively [14]. The results of the content validity of the questionnaire (CVR & CVI) are presented in Table 1.
According to demographic data, 182 clients who completed the consent form were available to examine the discriminant construct validity of this questionnaire in a cross-sectional descriptive manner. The demographic information of participants is presented in Table 2.
Table 3 shows the results of construct validity (discriminant validity) between the normal and disabled groups. The lower scores belong to the disabled group, including ADHD, CP, and autism. These results show significant differences between the normal and disabled groups in all questionnaire items. This means this questioner could distinguish between normal and disabled groups.
A total of 30 subjects participated to evaluate the test re-test reliability of the questionnaire. The results indicate the stability of the answers in all items of the questionnaire. The internal consistency of the questionnaire was confirmed by the results of the Cronbach's α in the evaluated subjects (Table 4).
Discussion
Child therapeutic interventions have specific characteristics related to the importance of interactions and children’s participation in daily activities; On the other hand, occupational therapists emphasize these factors [1]. Various occupational therapy services focus on occupational performance; these services are provided individually, in groups, or social systems. In line with the main goal of occupational therapists to increase occupational performance levels in different areas and the health of clients, proper evaluation of occupational performance is necessary.
An effective and targeted intervention will not be possible without analyzing occupational domains. Moreover, clinicians and treatment systems need specialized standard tools to evaluate the results of interventions and recovery rates. This questionnaire will be an efficient tool to achieve these goals. Since the Persian translation of this questionnaire was valid and reliable, this measurement tool can be useful for clinicians and rehabilitation systems.
SCOPE questionnaire was translated by a common scientific method [15]. This method was also used to translate this questionnaire into the Portuguese language [16]. It was statistically validated after the approval by the team of translators and the publisher of the questionnaire. Since the employed team of translators was related to the concepts of the questionnaire with high insights into the subject matter, along with the appropriate consultation with the questionnaire developer, this translation acquired the appropriate quality in terms of maintaining the meaning and understanding of the concepts, with no problems at the validation stages.
Based on recorded demographic information (Table 2), as well as the characteristics and age range defined for the questionnaire [17], the demographic characteristics of the studied samples were of appropriate age balance and gender distribution in the normal and disabled groups. The discriminant validity of the questionnaire was acceptable, as evidenced by the results of this study, which were obtained from scores of normal samples with no function-affecting disease, as well as those obtained from samples with function-affecting diseases and diagnoses (ADHD, CP, and autism) in the statistical population. Similar results were obtained in a sample translated into Turkish [18]. A previous study of SCOPE supported the psychometric soundness of the instrument overall [6].
The results of the study by Bowyer et al. indicate that practitioners’ decisions to use SCOPE in practice mainly regard the assessment’s top-down and occupation focus and its ability to facilitate family-centered care [19].
Therefore, based on the goals of researchers and presented needs which are reported by Shafaroodi et al. (2017) [11], translating and reviewing the psychometric properties of SCOPE can draw the attention of the Iranian community of occupational therapists to top-down and client-center concepts of occupational therapy and clinically facilitate them.
Considering the importance of stability and reliability of the questionnaire in our study, the internal consistency of results obtained in the statistical sample and the Cronbach's α findings indicate high consistency in questions related to each domain. Moreover, the test re-test evaluation in 30 separate samples indicates the good reliability of the questionnaire in different domains (0.7-0.9), which is in agreement with the study that translated the questionnaire into Turkish [18].
However, the unequal numbers of normal and disabled samples can influence the obtained results which can be considered in supplementary studies. Studying with a larger and more homogeneous statistical population, a more complete statistical analysis and the calculation of criterion validity can be recommended in future studies. It will be possible to analyze the factors connected to the effect of application and the scope of use of this questionnaire by interviewing occupational therapists and assessing the prevalence of employing the questionnaire in future research.
Conclusion
The Persian version of the SCOPE questionnaire can be used as a valid and reliable tool by child therapists, in particular, occupational therapists. Persian version of this questionnaire has the potential to turn into a practical guide to evaluate the occupational performance levels of people aged 3-21 years. It can facilitate the therapists’ emphasis on functional skills in treatment without interpersonal comparisons and only by comparing the before and after conditions of clients. Having a suitable and easy-to-use clinical tool is a good opportunity to motivate therapists to apply the relevant theoretical concepts. Due to a lack of practical questionnaires in the domains of occupational performance, therapists may have relied on non-occupational questionnaires, resulting in the rise in popularity of bottom-up treatments. Examining this idea in supplementary studies can be enlightening. On the other hand, the existence of standard and valid tools for documentation and follow-up of clients, as well as strong interaction with other disciplines is of great advantage provided by this questionnaire for occupational therapists in governmental and private health systems.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Tabriz University of Medical Sciences (Code: IR.TBZMED.REC.1398.136).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Naser Havaei and Babak Kashefimehr; Investigation: Meral Huri and Patricia Bowyer; Resources: Naser Havaei; Methodology and writing the original draft: Shafagh Saei; Review and editing: Babak Kashefimehr and Patricia Bowyer; Supervision: Babak Kashefimehr and Meral Huri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the translation support group which was willing to participate in this study.
References
- American Occupational Therapy Association. Occupational therapy practice framework: Domain et process. The American Journal of Occupational Therapy. 2020; 74(2):1-87. [Link]
- Owen A, Adams F, Franszen D. Factors influencing model use in occupational therapy. South African Journal of Occupational Therapy. 2014; 44(1):41-7. [Link]
- Kielhofner G. Therapeutic reasoning: Planning, implementing and evaluating the outcomes of therapy. In: Kielhofner G, editor. A model of human occupation: Theory and application. Philadelphia: Lippincott Williams & Wilkins; 2008. [Link]
- Dunbar SB. Occupational therapy models for intervention with children and families. London: Eurospan Group; 2007. [Link]
- Rodger S. A survey of assessments used by pediatric occupational therapists. Australian Occupational Therapy Journal. 1994; 41(3):137-42. [DOI:10.1111/j.1440-1630.1994.tb01300.x]
- Kramer J, Bowyer P, O'Brien J, Kielhofner G, Maziero-Barbosa V. How interdisciplinary pediatric practitioners choose assessments. Canadian Journal of Occupational Therapy. 2009; 76(1):56-64. [DOI:10.1177/000841740907600114] [PMID]
- Bowyer PL, Kramer J, Ploszaj A, Ross M, Schwartz O, Kielhofner G, et al. A user’s manual for the short child occupational profile (SCOPE). Chicago: University of Illinois Chicago; 2005. [Link]
- Kramer J, Bowyer P, Kielhofner G, O'Brien J, Maziero-Barbosa V. Examining rater behaviour on a revised version of the short child occupational profile (SCOPE). OTJR: Occupation, Participation and Health. 2009; 29(2):88-96. [DOI: 10.3928/15394492-20090301-03]
- OBrien J, Hoffman J, Moreau E. Measuring OT intervention outcomes using the short child occupational profile (SCOPE). The American Journal of Occupational Therapy. 2019; 73(4_Supplement_1):7311515347p1. [DOI:10.5014/ajot.2019.73S1-PO4031]
- Bowyer PL, Kramer J, Kielhofner G, Maziero-Barbosa V, Girolami G. Measurement properties of the short child occupational profile (SCOPE). Physical & Occupational Therapy in Pediatrics. 2007; 27(4):67-85. [DOI:10.1080/J006v27n04_05]
- Shafaroodi N, Kamali M, Parvizi S, Hassani Mehraban A. Occupational therapists' clinical reasoning: A qualitative study. Iranian Rehabilitation Journal. 2017; 15(3):277-86. [DOI:10.29252/nrip.irj.15.3.277]
- Machado RS, Fernandes ADBF, Oliveira ALCB, Soares LS, Gouveia MTO, Silva GRF. [Cross-cultural adaptation methods of instruments in the nursing area (English, Portuguese)]. Revista Gaucha De Enfermagem. 2018; 39:e2017-0164 [DOI:10.1590/1983-1447.2018.2017-0164]
- Gjersing L, Caplehorn JR, Clausen T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Medical Research Methodology. 2010; 10:13. [DOI:10.1186/1471-2288-10-13] [PMCID] [PMID]
- Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000; 25(24):3186-91. [DOI:10.1097/00007632-200012150-00014] [PMID]
- Mazak MSR. [Adaptação transcultural do instrumento “the short child occupational profile”(SCOPE) para a língua Portuguesa do Brasileiro (Portuguese)]. Revista Brasileira de Educação Especial. 2022; 28:527-42. [DOI:10.1590/1980-54702022v28e0007]
- Bowyer P, Kramer J, Ploszaj A, Ross M, Schwartz O, Kielhofner G, et al. A user’s manual for the short child occupational profile (SCOPE). Chicago: University of Illinois; 2005. [Link]
- Huri M, Kashefi Mehr B, Kayihan H, Akel S, Öksüz C, Bumin G, et al. Adaptation, reliability, and validity testing of a Turkish version of the short child occupational profile SCOPE. Paper presented at: International Conference on Cerebral Palsy and Other Childhood-onset Disabilities. 1 June 2016; Stockholm, Sweden. [Link]
- Bowyer P, Lee J, Kramer J, Taylor RR, Kielhofner G. Determining the clinical utility of the short child occupational profile (SCOPE). British Journal of Occupational Therapy. 2012; 75(1):19-28. [DOI:10.4276/030802212X13261082051373]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2022/10/29 | Accepted: 2023/05/6 | Published: 2024/03/1
Received: 2022/10/29 | Accepted: 2023/05/6 | Published: 2024/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
