
988368
Sat, Jul 11, 2026

Volume 22, Issue 1 (March 2024)
Iranian Rehabilitation Journal 2024, 22(1): 143-150 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rathee M, Divakar S, Jain P, Chahal S, Singh S. 3D Oriented Prosthetic Rehabilitation of Bilaterally Congenital Missing Ears: A Case Report. Iranian Rehabilitation Journal 2024; 22 (1) :143-150
URL: http://irj.uswr.ac.ir/article-1-1826-en.html
URL: http://irj.uswr.ac.ir/article-1-1826-en.html



1- Department of Prosthodontics, Post Graduate Institute of Dental Sciences, Rohtak, India.
Keywords: Adhesives, Anotia, Congenital missing ear, Microtia, Room temperature vulcanizing silicone
Full-Text [PDF 1358 kb]
(1260 Downloads)
| Abstract (HTML) (3274 Views)
Full-Text: (729 Views)
Introduction
Microtia/anotia is a congenital malformation of the ear characterized by the underdevelopment and malformation (microtia) or absence (anotia) of the external ear (auricle). Found as an isolated finding in 60–80% of infants with impairment of hearing as a related finding, it may also be seen as part of syndromic conditions, involving the mandible and face, such as ocular-auricula-vertebral spectrum (OAVS) and Goldenhar “syndrome”, Treacher-Collins syndrome and trisomy 18, or maybe of teratogenic origin, such as retinoic acid embryopathy [1, 2].
The treatment options for reconstruction of the missing auricular region can be done either surgically or prosthetically. Surgical reconstruction involves autografting cartilage harvested from the ribs or implanting synthetic or alloplastic materials, which are then covered with scalp tissues. However, surgical reconstruction can only be performed until the growth spurt is completed. In patients with completed growth, prosthetic rehabilitation using an artificial ear is the treatment of choice [3].
Various materials have been described in the literature for the fabrication of maxillofacial prostheses, including acrylic resins, vinyl polymers, polyurethane elastomers, chlorinated polyethylene, and silicone elastomers. Among these materials, room temperature vulcanizing (RTV) silicones are commonly used due to their ability to achieve a lifelike appearance and natural movement, thanks to their lack of chemical reactivity and rigidity [4]. Although many case reports and studies in the literature describe the techniques for rehabilitating missing ears, very few have demonstrated the precise orientation of an auricular prosthesis to the patient’s face. Hence, this case report demonstrated the three-dimensional (3D) orientated prosthetic rehabilitation of bilateral microtia ears fabricated using RTV silicone elastomers secured using a hairband and adhesives.
Case Presentation
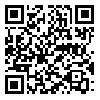
A 26 year-old male patient with complaints of microtia of bilateral ear for prosthetic rehabilitation was referred from the Department of Plastic Surgery. The patient was born with a complete absence of an external ear on the left side and a slight elevation of soft tissues on the right side. He also reported a history of compromised hearing on both sides of the ear. The patient had not undergone any treatment due to financial issues. He had no relevant past medical history and no syndromes or anomalies associated with microtia. On general examination, the patient was well-built, with a normal gait, conscious, oriented in time, place, and person. On extraoral examination, the patient had a bilaterally symmetrical face with normal muscle tone and development. On further examination, the patient had bilateral ear absence with slight soft tissue elevation on the right side and complete ear loss on the left side. The right external auditory canal was partially obliterated with complete obliteration on the contralateral side. The skin and the hairs over the auricular region were completely normal (Figures 1A, 1B and 1C). The patient was referred to the ear, nose, and throat (ENT) department for hearing loss, where they advised canaloplasty of the ear, but he was not willing to undergo the surgical procedure.
Treatment planning
The treatment options of ear prostheses using implants and glue were presented to the patient. Because the adhesive-retained prosthesis requires surgery and is very expensive, the patient refuses it. Hence, considering their socioeconomic status, an adhesive-retained auricular prosthesis fabricated using RTV silicone with additional retention using a hair band was planned for the patient.
Treatment progress
Impression creation
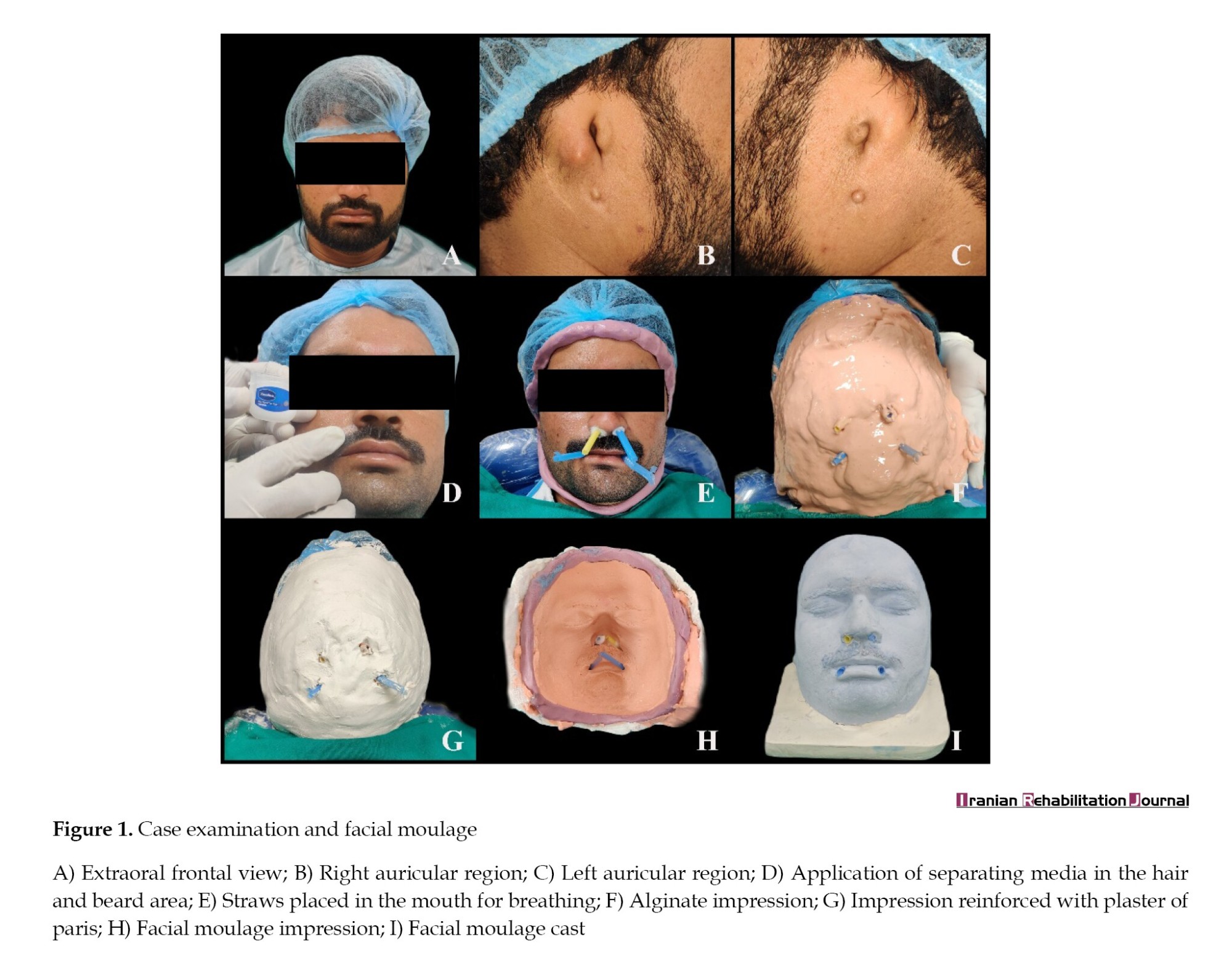
The patient had a bilateral missing ear; thus, we planned to make three impressions: A complete facial impression for facial moulage and a localized bilateral ear impression. For facial moulage, the patient was kept in an almost supine position on the dental chair. Petroleum jelly was applied to the hair, eyebrows, and beard areas to facilitate easy removal of the impression (Figure 1D). A gauze piece was inserted into the nostril and auditory canal, secured with dental floss, to prevent the flow of impression material into them. Two straws were placed at the corners of the mouth to allow for respiration, and the patient was instructed to gently close his mouth (Figure 1E). An elastomeric putty beading was done around the face to avoid unnecessary flow of impression material into the neck and shoulder region. The irreversible hydrocolloid (Algitex Alginate Impression Material-Dental Product of India) was chosen as the impression material and mixed with cold water to extend the setting time. The first layer of alginate was mixed to a thin liquid consistency for easy flow over the entire facial area. Then, a second layer was mixed to a thick consistency and placed over the first layer (Figure 1F). Before the complete setting of alginate, moist gauze pieces were added to the impression and reinforced with fast-setting plaster (Kaldent dental plaster; Kalabhai Karson Pvt Ltd.) to facilitate the removal of the impression without tearing and distortion (Figure 1G). A cast was made using type III gypsum product (Ultrastone dental stone; Kalabhai Karson Pvt Ltd.) (Figures 1H and 1I). For ear impression, a plastic round box was customized according to the auricular region of patient (Figures 2A and 2B). The ear area was prepared by using petroleum gel and placing a piece of cleaning gauze inside the ear canal. The alginate was mixed and poured inside the box (Figures 2C and 2D). After adjustment and restoration, the impression was poured using dental stone and the cast was retrieved (Figure 1E).
Donor impression
The patient’s elder brother was selected as the donor for ear prosthesis due to having a similar age, size, and color as the patient. Elastomeric impression materials were selected as the material of choice for their accurate and detailed reproduction capabilities. Similar to the facial moulage procedure, petroleum jelly was applied, and a gauze piece was inserted into the canal. First, the light body addition silicone (Avuegum Light body; Dental Avenue) (Figures 2F and 2G) was applied first, followed by the addition of silicone putty (Avuegum Putty; Dental Avenue) applied over it for reinforcement (Figures 2H and 2I). The impressions of each ear were then removed and disinfected (Figure 2J).
Wax pattern fabrication
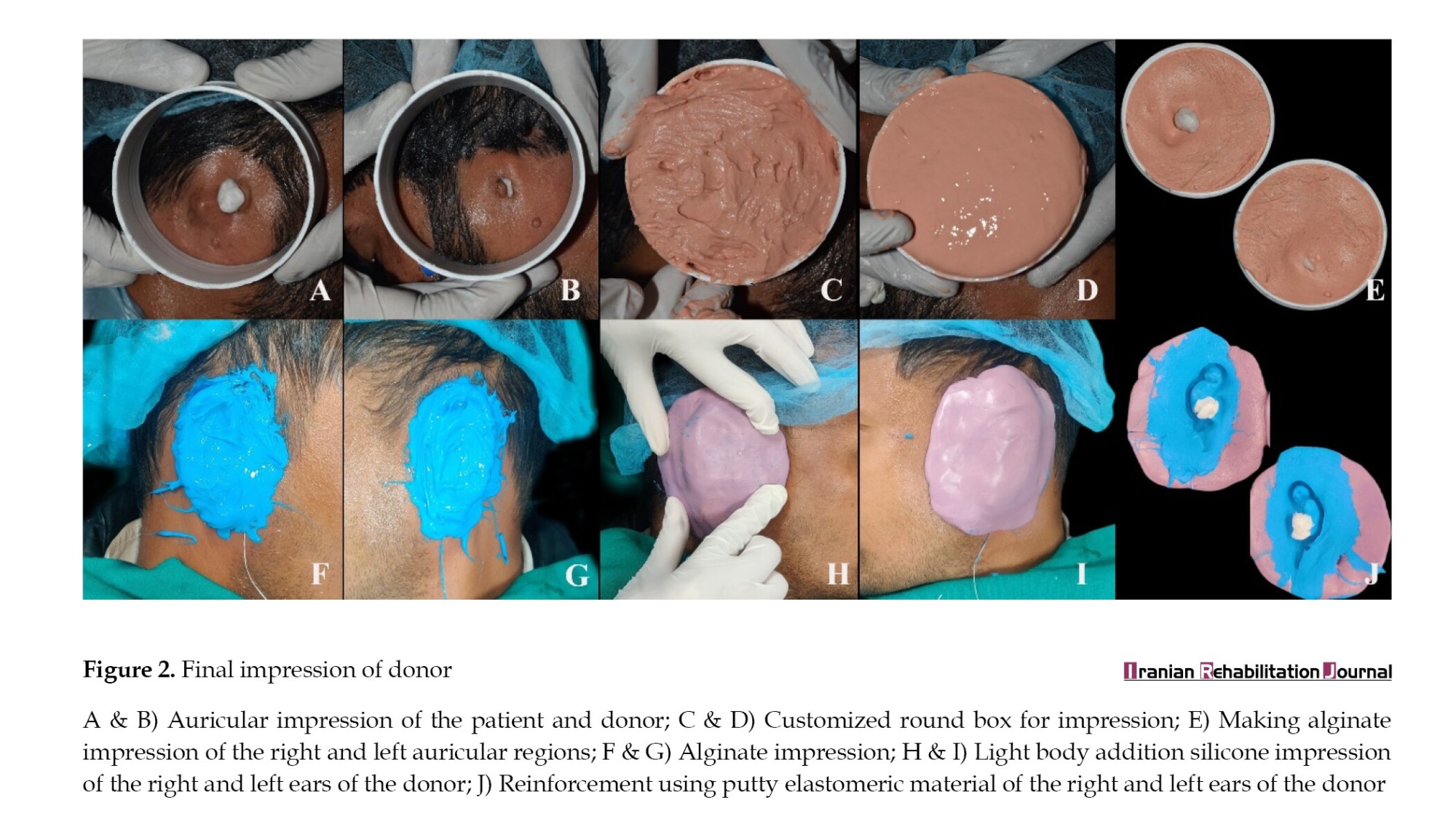
The donor impression was poured using modeling wax by melting it completely using the torch flame. After the wax hardened, the elastomeric impression was cut slowly using a Bard Parker blade, and the wax patterns of both ears were retrieved then, the wax patterns were placed over the cast of the patient and carved and modified according to his face (Figure 3A).
3D orientation of ears to face
Prior to 3D orientation, the position, length, width, and visibility of ears were first determined according to the patient facial form. The anthropometric measurements coupled with an established reference plane were used as the tool for determining the prosthetic site. Since the patient’s face had a mild oval to square shape, ear length was determined by using the distance between the bridge of the nose and the gnathion as a landmark and was measured using an vernier caliper (Figures 3B and 3C). To determine the width of the ear, the inter-alar distance was used as a reference point and measured (Figure 3D and 3E). The ears were positioned at the level of the subnasale as most facial forms are at the level of the subnasale (Figure 3F). The angulation of the ears was kept lesser than the angulation of the nose.
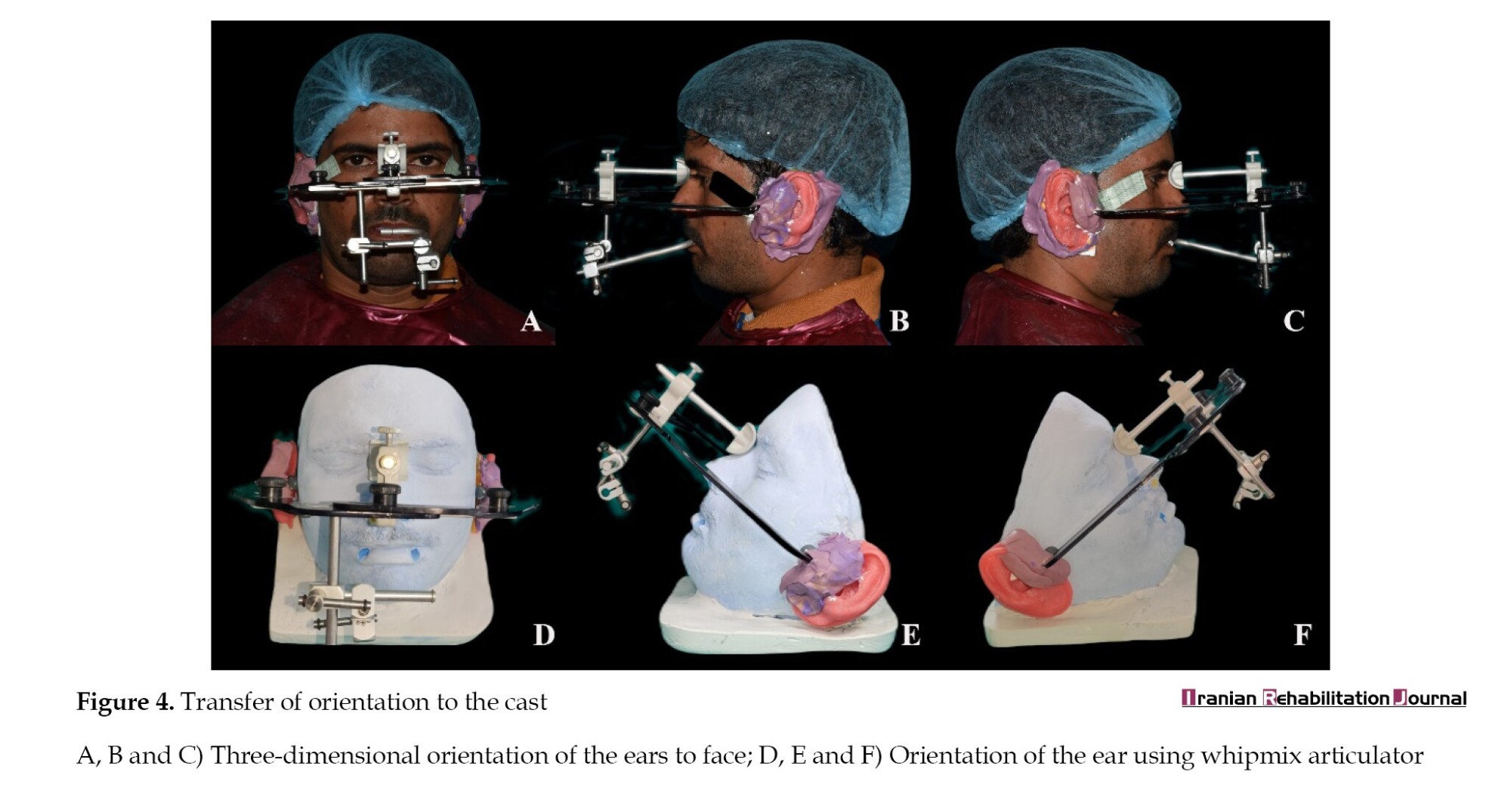
After the initial positioning, the 3D orientation was carried out by using a whipmix articulator. Beyron’s point (a point on the line from the center of the tragus to the outer canthus of the eye 13 mm from the anterior to the posterior margin of the tragus) was used as a posterior reference point. The whip mix articulator was positioned using a bite fork and the two earpieces were placed at Breyon’s point (Figure 4A). Then, the elastomeric putty was placed between the earpiece of the articulator and the wax pattern to stabilize it with the articulator (Figures 4B and 4C). The articulator was removed along with the wax pattern and positioned in the cast for transfer of the 3D orientation (Figures 4D and 4E).
Wax try-in
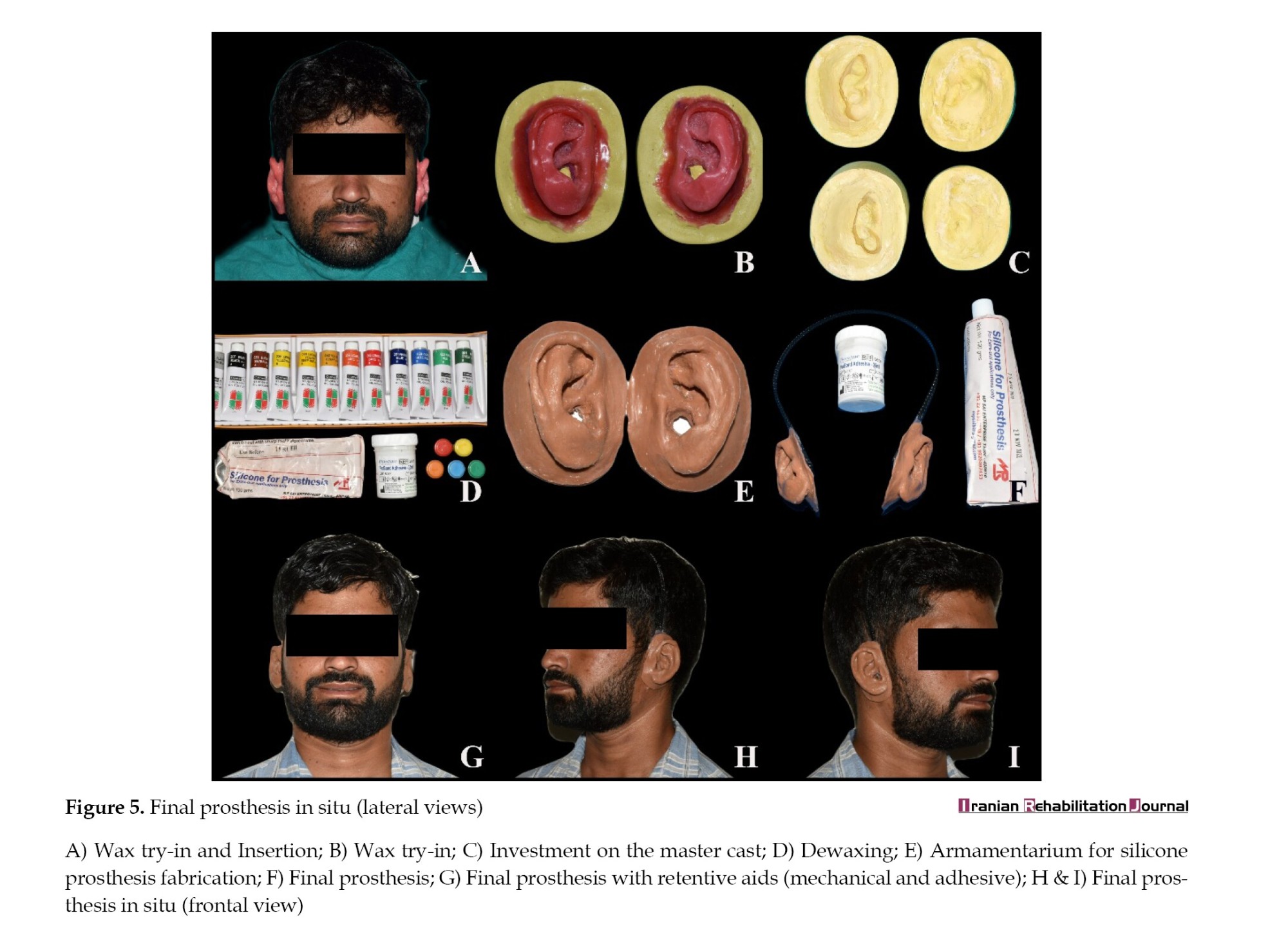
The wax patterns were carved according to the newly oriented position in the facial moulage placed in the same position on the patient’s auricular region and stabilized using a hair band and adhesive. After stabilizing, the wax pattern was evaluated for position, angulation, and visibility according to the patient’s face (Figure 5A). After evaluation, the external shade selection was done using silicone material. Following the approval of shade by the patient, the manufacturing of a silicone prosthesis was carried out.
Fabrication of prosthesis
The wax pattern was invested in the type III gypsum product (labstone, Kalabhai Dental Pvt Ltd.) and soaked in hot water for dewaxing (Figure 5B). After dewaxing, the separating medium (cold mould seal) was applied (Figure 5C). The extraoral silicone (RTV Silicone, Silastic-MDX 44210 MP Sai Enterprises, Mumbai, India) and pigments were blended in-house to match the patient shade, which was verified during wax try-in (Figure 5D). Then, the silicone material was applied to the mould with light pressure and the mould was positioned and secured with elastics. After room temperature polymerization for 24 hours, the prosthesis was removed and trimmed using silicone finishing and polishing burs (Figure 5E).
Insertion of prosthesis
A trough was made at the tissue surface of the prosthesis, on which the hair band was positioned and the trough was filled with extraoral silicone material (Figure 5F). After the material was set, the prosthesis was positioned and attached using adhesive (medical grade Technovent Probond Adhesive) (Figures 5G, 5H and5I). The patient was guided regarding the use, placement, and removal of the prosthesis. The patient was instructed to remove the prosthesis before going to bed to avoid overheating. He was instructed to clean the prosthesis with a solution, like shampoo and antibacterial soap, and then rinse it thoroughly and dry it with a tissue. The patient was recalled for the follow-up after a day, a week, and a month.
Discussion
About 1 in 8,000 to 10,000 babies experience microtia/anotia. Although the exact origin of microtia in children is yet unknown, some studies have described genetic deformities in one or more genes, being born at high altitudes, and gestational diabetes. Underweight newborns, male sex, women’s gravidity and parity, and using Accutane (isotretinoin) during pregnancy are also the risk factors reported in the literature. There are four grades of microtia: Grade 1: The external ear is smaller than usual but looks normal; grade 2: The external ear is only partly formed and 50% to 66% smaller than normal; grade 3: The external ear is a tiny piece of cartilage shaped like a peanut; grade 4: Anotia: The external ear is missing [2, 5].
According to the above classification, our patient is placed in grade 4 on the left side and grade 3 on the right side, which makes surgical reconstruction and rehabilitation of the prosthesis very difficult. Hence, we used adhesive and mechanical (hair band) retentive aids. There are various mechanical retentive aids available in literature, like magnets, spectacles, and orthodontics wires [6, 7]. Magnets and orthodontics are not used because no outer ear is available on both sides. The patient was not interested in wearing spectacles; hence, after consulting with the patient, a hair band was used, and the patient was asked to grow long hairs to make the hair band invisible.
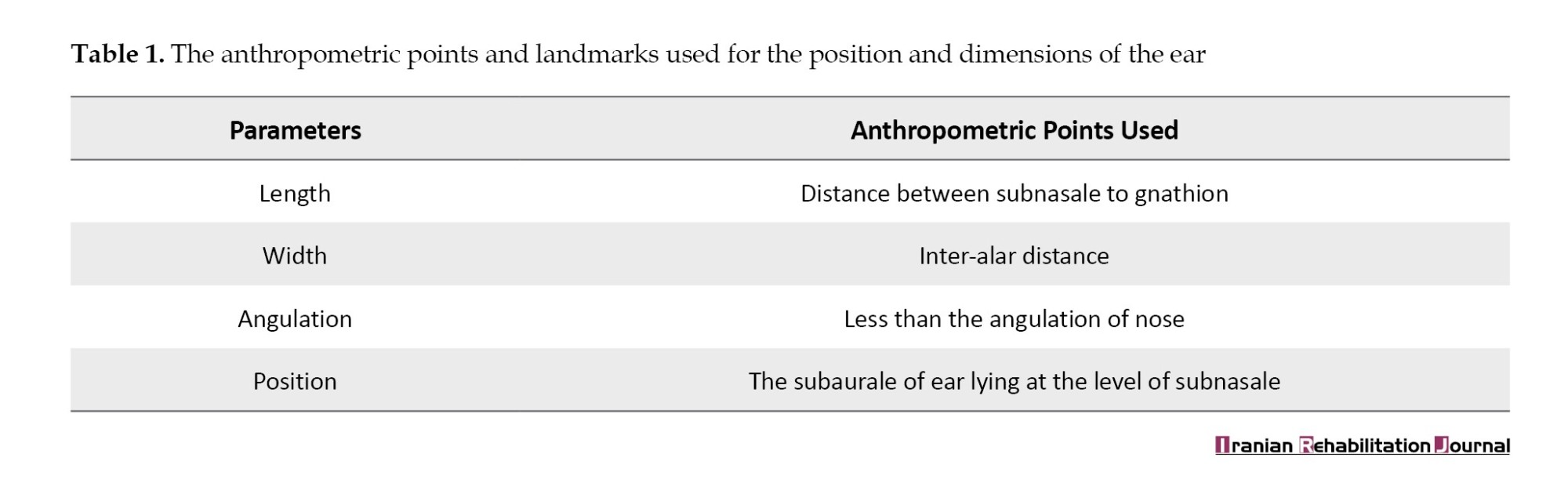
Mohamed et al. (2014) [8] assessed the ear position, angulations, visibility, and dimensions using various anthropometric points of the face and reference plane indicators according to the different facial forms (ovoid, square, tapering, and square-tapering). This helped us to find accurately the position of the prosthetic site. Upon extraoral examination, our patient has a bilaterally symmetrical ovoid to the square form of the face. Hence, we used highly significant anthropometric points and landmarks of ovoid and square facial forms described in the study and as discussed in Table 1.
After the positioning, the whipmix articulator was used to orient the position and transfer it to the facial moulage. This helped us to attach the mechanical retentive aid (hair band) without changing its exact position. The limitation of the case is that we used a hair band as additional retention for the male patient as he insisted on a hair band, which he used periodically. This technique can be considered for female patients and cannot used widely for male patients. Hence, new retentive aids should be considered in future studies in male patients.
Conclusion
Leading a life with physical deformity is a stressful and depressing experience for the patient as it directly affects their mental, social, and psychological well-being. Methods to replace lost body parts have been documented even from ancient times. Although the surgical reconstruction of the ear is a permanent treatment, it has its own limitations and drawbacks. The prosthetic replacement of anatomical parts is an art and science. Prosthesis form, coloration, and texture must be as indiscernible as possible from the surrounding natural tissue. Besides, the orientation of both the ears to the facial form is also an important factor to be considered. Hence, this case report shows the conservative and cost-effective prosthetic rehabilitation of bilateral artificial auricular prosthesis retained by hair band and adhesive and the technique for orienting both ears in their natural position.
Ethical Considerations
Compliance with ethical guidelines
A written informed consent was signed by the patient for the treatment procedure and publication of his photographs.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: All authors; Methodology and writing the original draft: Santhanam Divakar, Sandeep Singh and Sujata Chahal; Review, editing and supervision: Manu Rathee and Prachi Jain.
Conflict of interest
The authors declared no conflict of interest.
References
Microtia/anotia is a congenital malformation of the ear characterized by the underdevelopment and malformation (microtia) or absence (anotia) of the external ear (auricle). Found as an isolated finding in 60–80% of infants with impairment of hearing as a related finding, it may also be seen as part of syndromic conditions, involving the mandible and face, such as ocular-auricula-vertebral spectrum (OAVS) and Goldenhar “syndrome”, Treacher-Collins syndrome and trisomy 18, or maybe of teratogenic origin, such as retinoic acid embryopathy [1, 2].
The treatment options for reconstruction of the missing auricular region can be done either surgically or prosthetically. Surgical reconstruction involves autografting cartilage harvested from the ribs or implanting synthetic or alloplastic materials, which are then covered with scalp tissues. However, surgical reconstruction can only be performed until the growth spurt is completed. In patients with completed growth, prosthetic rehabilitation using an artificial ear is the treatment of choice [3].
Various materials have been described in the literature for the fabrication of maxillofacial prostheses, including acrylic resins, vinyl polymers, polyurethane elastomers, chlorinated polyethylene, and silicone elastomers. Among these materials, room temperature vulcanizing (RTV) silicones are commonly used due to their ability to achieve a lifelike appearance and natural movement, thanks to their lack of chemical reactivity and rigidity [4]. Although many case reports and studies in the literature describe the techniques for rehabilitating missing ears, very few have demonstrated the precise orientation of an auricular prosthesis to the patient’s face. Hence, this case report demonstrated the three-dimensional (3D) orientated prosthetic rehabilitation of bilateral microtia ears fabricated using RTV silicone elastomers secured using a hairband and adhesives.
Case Presentation
A 26 year-old male patient with complaints of microtia of bilateral ear for prosthetic rehabilitation was referred from the Department of Plastic Surgery. The patient was born with a complete absence of an external ear on the left side and a slight elevation of soft tissues on the right side. He also reported a history of compromised hearing on both sides of the ear. The patient had not undergone any treatment due to financial issues. He had no relevant past medical history and no syndromes or anomalies associated with microtia. On general examination, the patient was well-built, with a normal gait, conscious, oriented in time, place, and person. On extraoral examination, the patient had a bilaterally symmetrical face with normal muscle tone and development. On further examination, the patient had bilateral ear absence with slight soft tissue elevation on the right side and complete ear loss on the left side. The right external auditory canal was partially obliterated with complete obliteration on the contralateral side. The skin and the hairs over the auricular region were completely normal (Figures 1A, 1B and 1C). The patient was referred to the ear, nose, and throat (ENT) department for hearing loss, where they advised canaloplasty of the ear, but he was not willing to undergo the surgical procedure.
Treatment planning
The treatment options of ear prostheses using implants and glue were presented to the patient. Because the adhesive-retained prosthesis requires surgery and is very expensive, the patient refuses it. Hence, considering their socioeconomic status, an adhesive-retained auricular prosthesis fabricated using RTV silicone with additional retention using a hair band was planned for the patient.
Treatment progress
Impression creation
The patient had a bilateral missing ear; thus, we planned to make three impressions: A complete facial impression for facial moulage and a localized bilateral ear impression. For facial moulage, the patient was kept in an almost supine position on the dental chair. Petroleum jelly was applied to the hair, eyebrows, and beard areas to facilitate easy removal of the impression (Figure 1D). A gauze piece was inserted into the nostril and auditory canal, secured with dental floss, to prevent the flow of impression material into them. Two straws were placed at the corners of the mouth to allow for respiration, and the patient was instructed to gently close his mouth (Figure 1E). An elastomeric putty beading was done around the face to avoid unnecessary flow of impression material into the neck and shoulder region. The irreversible hydrocolloid (Algitex Alginate Impression Material-Dental Product of India) was chosen as the impression material and mixed with cold water to extend the setting time. The first layer of alginate was mixed to a thin liquid consistency for easy flow over the entire facial area. Then, a second layer was mixed to a thick consistency and placed over the first layer (Figure 1F). Before the complete setting of alginate, moist gauze pieces were added to the impression and reinforced with fast-setting plaster (Kaldent dental plaster; Kalabhai Karson Pvt Ltd.) to facilitate the removal of the impression without tearing and distortion (Figure 1G). A cast was made using type III gypsum product (Ultrastone dental stone; Kalabhai Karson Pvt Ltd.) (Figures 1H and 1I). For ear impression, a plastic round box was customized according to the auricular region of patient (Figures 2A and 2B). The ear area was prepared by using petroleum gel and placing a piece of cleaning gauze inside the ear canal. The alginate was mixed and poured inside the box (Figures 2C and 2D). After adjustment and restoration, the impression was poured using dental stone and the cast was retrieved (Figure 1E).
Donor impression
The patient’s elder brother was selected as the donor for ear prosthesis due to having a similar age, size, and color as the patient. Elastomeric impression materials were selected as the material of choice for their accurate and detailed reproduction capabilities. Similar to the facial moulage procedure, petroleum jelly was applied, and a gauze piece was inserted into the canal. First, the light body addition silicone (Avuegum Light body; Dental Avenue) (Figures 2F and 2G) was applied first, followed by the addition of silicone putty (Avuegum Putty; Dental Avenue) applied over it for reinforcement (Figures 2H and 2I). The impressions of each ear were then removed and disinfected (Figure 2J).
Wax pattern fabrication
The donor impression was poured using modeling wax by melting it completely using the torch flame. After the wax hardened, the elastomeric impression was cut slowly using a Bard Parker blade, and the wax patterns of both ears were retrieved then, the wax patterns were placed over the cast of the patient and carved and modified according to his face (Figure 3A).
3D orientation of ears to face
Prior to 3D orientation, the position, length, width, and visibility of ears were first determined according to the patient facial form. The anthropometric measurements coupled with an established reference plane were used as the tool for determining the prosthetic site. Since the patient’s face had a mild oval to square shape, ear length was determined by using the distance between the bridge of the nose and the gnathion as a landmark and was measured using an vernier caliper (Figures 3B and 3C). To determine the width of the ear, the inter-alar distance was used as a reference point and measured (Figure 3D and 3E). The ears were positioned at the level of the subnasale as most facial forms are at the level of the subnasale (Figure 3F). The angulation of the ears was kept lesser than the angulation of the nose.
After the initial positioning, the 3D orientation was carried out by using a whipmix articulator. Beyron’s point (a point on the line from the center of the tragus to the outer canthus of the eye 13 mm from the anterior to the posterior margin of the tragus) was used as a posterior reference point. The whip mix articulator was positioned using a bite fork and the two earpieces were placed at Breyon’s point (Figure 4A). Then, the elastomeric putty was placed between the earpiece of the articulator and the wax pattern to stabilize it with the articulator (Figures 4B and 4C). The articulator was removed along with the wax pattern and positioned in the cast for transfer of the 3D orientation (Figures 4D and 4E).
Wax try-in
The wax patterns were carved according to the newly oriented position in the facial moulage placed in the same position on the patient’s auricular region and stabilized using a hair band and adhesive. After stabilizing, the wax pattern was evaluated for position, angulation, and visibility according to the patient’s face (Figure 5A). After evaluation, the external shade selection was done using silicone material. Following the approval of shade by the patient, the manufacturing of a silicone prosthesis was carried out.
Fabrication of prosthesis
The wax pattern was invested in the type III gypsum product (labstone, Kalabhai Dental Pvt Ltd.) and soaked in hot water for dewaxing (Figure 5B). After dewaxing, the separating medium (cold mould seal) was applied (Figure 5C). The extraoral silicone (RTV Silicone, Silastic-MDX 44210 MP Sai Enterprises, Mumbai, India) and pigments were blended in-house to match the patient shade, which was verified during wax try-in (Figure 5D). Then, the silicone material was applied to the mould with light pressure and the mould was positioned and secured with elastics. After room temperature polymerization for 24 hours, the prosthesis was removed and trimmed using silicone finishing and polishing burs (Figure 5E).
Insertion of prosthesis
A trough was made at the tissue surface of the prosthesis, on which the hair band was positioned and the trough was filled with extraoral silicone material (Figure 5F). After the material was set, the prosthesis was positioned and attached using adhesive (medical grade Technovent Probond Adhesive) (Figures 5G, 5H and5I). The patient was guided regarding the use, placement, and removal of the prosthesis. The patient was instructed to remove the prosthesis before going to bed to avoid overheating. He was instructed to clean the prosthesis with a solution, like shampoo and antibacterial soap, and then rinse it thoroughly and dry it with a tissue. The patient was recalled for the follow-up after a day, a week, and a month.
Discussion
About 1 in 8,000 to 10,000 babies experience microtia/anotia. Although the exact origin of microtia in children is yet unknown, some studies have described genetic deformities in one or more genes, being born at high altitudes, and gestational diabetes. Underweight newborns, male sex, women’s gravidity and parity, and using Accutane (isotretinoin) during pregnancy are also the risk factors reported in the literature. There are four grades of microtia: Grade 1: The external ear is smaller than usual but looks normal; grade 2: The external ear is only partly formed and 50% to 66% smaller than normal; grade 3: The external ear is a tiny piece of cartilage shaped like a peanut; grade 4: Anotia: The external ear is missing [2, 5].
According to the above classification, our patient is placed in grade 4 on the left side and grade 3 on the right side, which makes surgical reconstruction and rehabilitation of the prosthesis very difficult. Hence, we used adhesive and mechanical (hair band) retentive aids. There are various mechanical retentive aids available in literature, like magnets, spectacles, and orthodontics wires [6, 7]. Magnets and orthodontics are not used because no outer ear is available on both sides. The patient was not interested in wearing spectacles; hence, after consulting with the patient, a hair band was used, and the patient was asked to grow long hairs to make the hair band invisible.
Mohamed et al. (2014) [8] assessed the ear position, angulations, visibility, and dimensions using various anthropometric points of the face and reference plane indicators according to the different facial forms (ovoid, square, tapering, and square-tapering). This helped us to find accurately the position of the prosthetic site. Upon extraoral examination, our patient has a bilaterally symmetrical ovoid to the square form of the face. Hence, we used highly significant anthropometric points and landmarks of ovoid and square facial forms described in the study and as discussed in Table 1.
After the positioning, the whipmix articulator was used to orient the position and transfer it to the facial moulage. This helped us to attach the mechanical retentive aid (hair band) without changing its exact position. The limitation of the case is that we used a hair band as additional retention for the male patient as he insisted on a hair band, which he used periodically. This technique can be considered for female patients and cannot used widely for male patients. Hence, new retentive aids should be considered in future studies in male patients.
Conclusion
Leading a life with physical deformity is a stressful and depressing experience for the patient as it directly affects their mental, social, and psychological well-being. Methods to replace lost body parts have been documented even from ancient times. Although the surgical reconstruction of the ear is a permanent treatment, it has its own limitations and drawbacks. The prosthetic replacement of anatomical parts is an art and science. Prosthesis form, coloration, and texture must be as indiscernible as possible from the surrounding natural tissue. Besides, the orientation of both the ears to the facial form is also an important factor to be considered. Hence, this case report shows the conservative and cost-effective prosthetic rehabilitation of bilateral artificial auricular prosthesis retained by hair band and adhesive and the technique for orienting both ears in their natural position.
Ethical Considerations
Compliance with ethical guidelines
A written informed consent was signed by the patient for the treatment procedure and publication of his photographs.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: All authors; Methodology and writing the original draft: Santhanam Divakar, Sandeep Singh and Sujata Chahal; Review, editing and supervision: Manu Rathee and Prachi Jain.
Conflict of interest
The authors declared no conflict of interest.
References
- Srivastava A, Hazra R, Kumar D. Bridging form and function: A bilateral auricular prosthesis. Journal of Indian Prosthodontic Society. 2022; 22(3):300-4. [DOI:10.4103/jips.jips_546_21] [PMID] [PMCID]
- Luquetti DV, Heike CL, Hing AV, Cunningham ML, Cox TC. Microtia: Epidemiology and genetics. American Journal of Medical Genetics. Part A. 2012; 158A(1):124-39. [DOI:10.1002/ajmg.a.34352] [PMID] [PMCID]
- Humphries S, Joshi A, Webb WR, Kanegaonkar R. Auricular reconstruction: Where are we now? A critical literature review. European Archives of Oto-Rhino-Laryngology. 2022; 279(2):541-56. [DOI:10.1007/s00405-021-06903-5] [PMID]
- Singh A, Ghosh S, Kar S, Ahmed I. Silicone prosthesis for a patient with unilateral ear defect: A clinical case report. European Journal of General Dentistry. 2013; 2(03):315-9. [DOI:10.4103/2278-9626.115997]
- Baluch N, Nagata S, Park C, Wilkes GH, Reinisch J, Kasrai L, et al. Auricular reconstruction for microtia: A review of available methods. Plastic Surgery. 2014; 22(1):39-43. [DOI:10.1177/229255031402200102] [PMID] [PMCID]
- Swaminathan AA, Prasad A. Fabrication of a silicone auricular prosthesis–A case report. Journal of Health and Allied Sciences NU. 2016; 6(01):091-7. [DOI:10.1055/s-0040-1708627]
- Rathee M, Tamrakar AK, Kundu R, Yunus N. Three-dimensional precise orientation of bilateral auricular trial prosthesis using a facebow for a young adult with Crouzon syndrome. BMJ Case Reports. 2014; 2014:bcr2013203248. [DOI:10.1136/bcr-2013-203248] [PMID] [PMCID]
- Mohamed K, Christian J, Jeyapalan K, Natarajan S, Banu F, Veeravalli PT. Identifying position, visibility, dimensions, and angulation of the ear. Journal of Rehabilitation Research and Development. 2014; 51(4):599-608. [DOI:10.1682/JRRD.2013.06.0132] [PMID]
Article type: Case Reports |
Subject:
Rehabilitation Management
Received: 2022/11/18 | Accepted: 2023/05/29 | Published: 2024/03/1
Received: 2022/11/18 | Accepted: 2023/05/29 | Published: 2024/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
