
988368
Thu, Jul 30, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 655-662 |
Back to browse issues page



Ethics code: approval No: P.T.REC/012/003833
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
AL-Nemr A. Relationship Between Body Mass Index, Selective Voluntary Motor Control and Functional Independence in Children With Cerebral Palsy. Iranian Rehabilitation Journal 2024; 22 (4) :655-662
URL: http://irj.uswr.ac.ir/article-1-1835-en.html
URL: http://irj.uswr.ac.ir/article-1-1835-en.html



Department of Physical Therapy for Pediatrics, Faculty of Physical Therapy, Cairo University, Giza, Egypt.
Keywords: Body mass index, Cerebral palsy (CP), Diplegia, Functional independence, Selective voluntary motor control (SVMC)
Full-Text [PDF 475 kb]
(767 Downloads)
| Abstract (HTML) (3123 Views)
Full-Text: (515 Views)
Introduction
Cerebral palsy (CP) is a disorder characterized by abnormal posture, tone, and movement and is classified clinically according to the predominant motor syndrome [1]. The overall CP birth prevalence for high-income countries is 1.6 per 1000 live births, while low-income countries showed marked higher birth prevalence [2], in addition to a higher prevalence of 60 to 150 per 1000 live births among preterm infants [3]. The most prevalent type of CP is spastic diplegia which is commonly associated with prematurity [4]. Children with spastic CP suffer from multiple neurological abnormalities, including muscle weakness, spasticity, and abnormal movement pattern [1]. Abnormal movement pattern occurs in children with spastic CP due to coordination problems which are caused by extensor or flexor synergies that interfere with isolated joint movement [5].
Selective voluntary motor control (SVMC) is an integral part of normal human motion and can independently control joint movement. Reduced SVMC is defined as a disturbance of the capability of isolating the muscle activation in selected patterns due to voluntary movement or posture demands [6] which means that a child with impaired SVMC does not have the expected activation pattern that is present in healthy children, either due to lack or excessive muscle activity [7]. This is one of the neuromuscular disorders associated with spastic CP and commonly coexists with muscle weakness and spasticity. All of the previously-mentioned motor disorders are related to the damage of the corticospinal tract and other descending motor pathways, resulting in interruption of the descending excitability and inhibitory signals leading to dysfunction [8, 9].
Children with CP have less energy consumption, and limited participation in physical activities compatible with their age compared to their healthy peers. Thus, the risk of obesity in these children is higher than in healthy subjects [10]. The prevalence of obesity in children with CP who are ambulant has increased from 7.7% to 16.5% in the last decade which affect negatively the general health of these children [11]. Through the analysis of body mass index (BMI) and waist-hip ratio, Bansal et al. suggest that children with CP have a high rate of being overweight and are at risk of being obese, particularly central obesity [12]. Fat mass can be assessed by several tools, such as hydrostatic weighing and dual-energy x-ray absorptiometry which are valid tools for measuring obesity. However, these tools have limited usage and are more invasive than BMI. Therefore, BMI is widely recommended by many institutions as the World Health Organization (WHO) and the World Obesity Federation [13, 14].
The risk of becoming overweight or obese increases throughout the range of dysfunction in children who have mild to moderate motor disabilities [15]. Obesity is of particular concern to children with CP because of the long-term health risks associated with obesity and the potentially increased impairment of functional mobility associated with obesity [16]. mDixon magnetic resonance images showed a lower intramuscular fat ratio in normal children than children with spastic CP who can ambulate [17]. Also, bioelectrical impedance analysis was used to estimate fat-free mass in preschool children with CP, and altered body composition was detected in these children across functional capacities [16].
Former studies have shown the relationship between lower limb SVMC and gait in children with CP [18, 19], and between health-related quality of life and BMI [20]; however, no available studies are detected regarding the relationship between BMI, isolated motor control, and functional independence in children with spastic diplegic CP. Accordingly, this study detects the relationship between BMI, SVMC and functional independence in children with spastic diplegic CP.
Materials and Methods
Study design and setting
This is an observational correlational study conducted between January to August 2022 at the Outpatient Clinic of the Faculty of Physical Therapy, Cairo University.
Sample size
G*Power statistical software, version 3.1 was used for estimating the sample size before the study using effect size=0.3, β=0.2 and α=0.05, which were calculated from a pilot study and showed that the total sample size is 84 children. Hence, 90 children were enrolled, considering prospective dropouts.
Participant recruitment and selection criteria
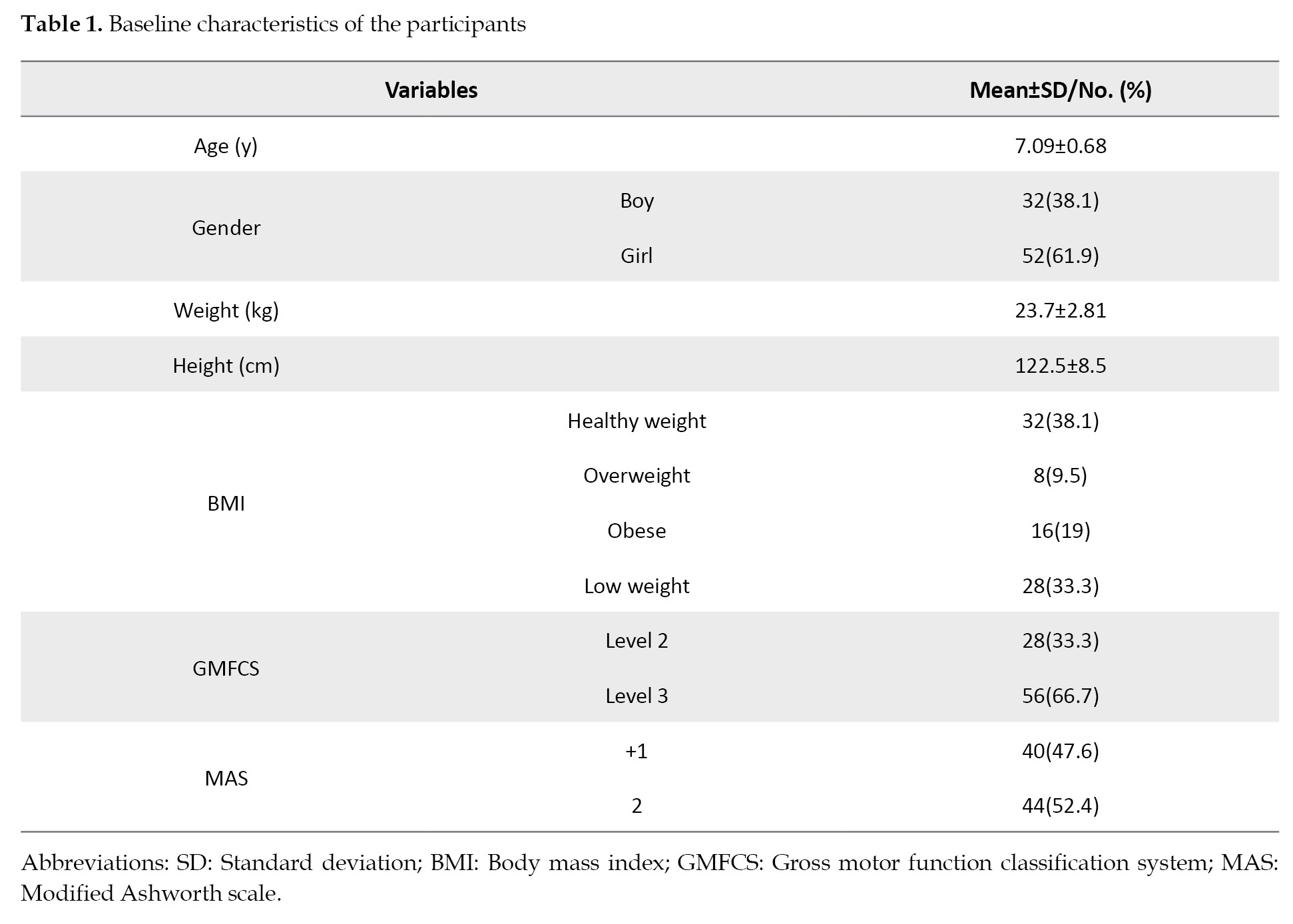
Initially, 90 children were enrolled and 6 children were excluded. Then, 2 children had lower limb surgical operations, and 4 subjects quit before the assessment termination. Accordingly, 84 children with spastic diplegic CP (32 male and 52 female) were involved in this study. The participants were selected from the Outpatient Clinic of the Faculty of Physical Therapy, Cairo University.
Children diagnosed as spastic diplegic CP, whose chronological age ranges from 6 up to 9 years, with spasticity levels +1 and 2 in the affected lower limbs as specified by the modified Ashworth scale (MAS), and levels II and III of the gross motor functional classification system expanded and revised (GMFCS E&R), who could follow the given instructions during the assessment were included in this study. The patients who had contractures of the lower limb joints were injected with botulinum toxin or any orthopedic surgery of the lower extremities in the last 6 months before the study, or who had epilepsy, were excluded from the study. Accordingly, Table 1 shows the characteristics of the participating children.
Testing procedures
Anthropometric measurements
A calibrated digital scale was used to measure children’s weight and Harpenden Stadiometer to measure their height. BMI was calculated as weight (kg)/height (m2). Growth charts for children and adolescents with ages ranging from 2–20 years were used to calculate the percentile scores of BMI, which consider the child’s age and sex. BMI was assigned, using these charts, to one of four categories: Underweight, healthy, overweight, or obese [21].
Selective control assessment of the lower extremity
The selective control assessment of the lower extremity (SCALE) is a reliable and valid scale used to evaluate SVMC of the toes, subtalar, ankle, knee, and hip joints in children with spastic CP [22]. The isolated movements are evaluated bilaterally. Scores of 2 (Normal), 1 (impaired), or 0 (unable) were given for each joint; 10 points for each limb, with 20 points as a total maximum score. Children were instructed to do specific isolated movements, reported in the SCALE, at each joint using a 3 s verbal count [22].
Pediatric functional independence measure (Wee-FIM)
The Wee-FIM is a reliable and valid scale used to evaluate the daily life activities of children with CP. Evaluation can be supplemented by observation of the child and interview with the caregiver, with 20 min administration time. This scale assesses the physical and cognitive ability of the child. It includes 6 domains of function which were evaluated in this study. Four of these are physical and two are cognitive. Items are scored with based on a 7-point ordinal scale, with 7 indicating complete independence and 1 showing total dependency. Caregiver assistance is needed for scores of 1 to 5. Higher scores indicate more independence with possible scores ranging from 18 to 126 [23].
The gross motor function classification system (GMFCS) expanded and revised
GMFCS E&R is a valid and reliable classification that differentiates children with CP following their gross motor abilities and limitations. It contains 5 levels [24]. The distinction between different levels, ranging from level I (the highest gross motor function) up to level V (the lowest level) is based on the need for assistive technology and functional abilities, rather than the quality of movement [25]. As nearly 98% of children with spastic diplegia are classified as level I, II, or III [26] and children with level I of GMFCS were more likely to have a healthy weight [27], only levels II and III were included in this study.
Modified Ashworth scale (MAS)
MAS is a widely accepted clinical tool that is used to measure spasticity. It is based on a 6-point ordinal scale with a grade score of 0, 1, +1, 2, 3 and 4, where a higher grade score indicates increased spasticity [28]. According to the MAS scoring system, the selected children were graded +1 and 2 which are the most available grades in the outpatient clinic during this study.
Statistical analysis
The relationship between BMI, SVMC and the level of functional independence in children with diplegic CP was assessed using correlation analysis. The SPSS software, version 25 was used to perform the statistical analyses. Descriptive statistics were expressed in numerical (n) and percent (%) formats, and Mean±SD. The Spearman correlation coefficient was selected to examine the relationships due to the ordinal nature of the data. A correlation was considered significant at a P<0.05.
Results
In this study, 84 children with spastic diplegic CP were selected. Table 1 displays the general characteristics of the children participating in the study. The results showed a positive, strong and significant correlation between MAS and BMI (rs=+0.677, P<0.001), WEE FIM total score and SCALE (rs=+0.718, P<0.001), the physical dimension of WEE FIM and SCALE (rs=+0.843, P<0.001), and the cognitive dimension of WEE FIM and SCALE (rs=+0.904, P<0.001); however, there was a negative, strong and significant correlation between MAS and WEE FIM total score (rs=-0.669, P<0.001), MAS and the physical dimension of WEE FIM (rs=-0.712, P<0.001), MAS and the cognitive dimension of WEE FIM, (rs=-0.793, P<0.001), MAS and SCALE (rs=-0.830, P<0.001), the cognitive dimension of WEE FIM and GMFCS (rs=-0.660, P<0.001), SCALE and GMFCS (rs=-0.707, P<0.001) and WEE FIM total score and BMI (rs=-0.607, P<0.001) as presented in Table 2.
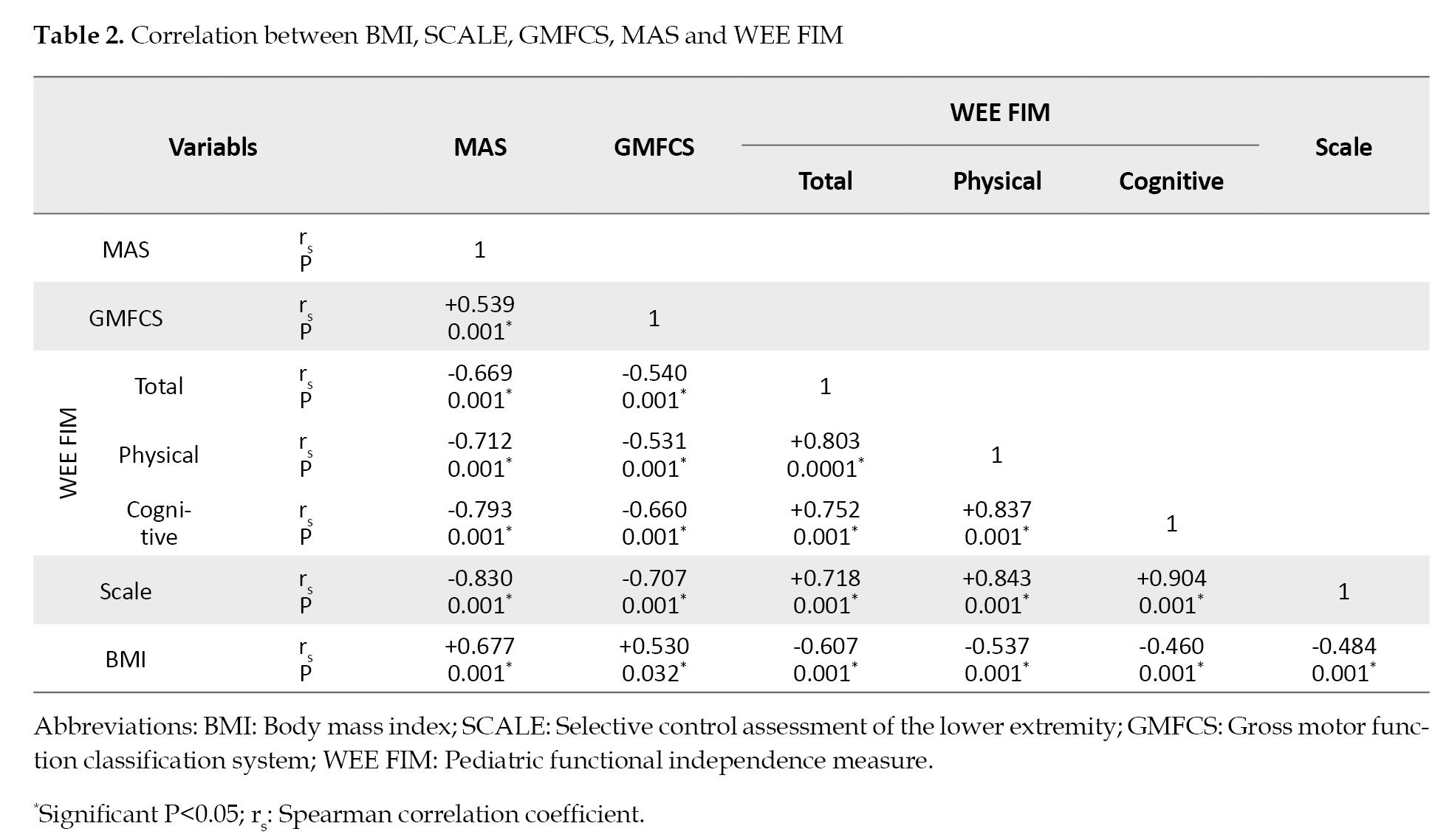
In addition, there was a positive, moderate, and significant correlation between MAS and GMFCS (rs=+0.539, P<0.001) and BMI and GMFCS (rs=+0.53, P<0.032); however, there was a negative, moderate, and significant correlation between GMFCS and WEE FIM total score(rs=-0.540, P<0.001), GMFCS and the physical dimension of WEE FIM (rs=-0.531, P<0.001), BMI and SCALE (rs=-0.484, P<0.001), BMI and the physical dimension of WEE FIM (rs=-0.537, P<0.001) and BMI and the cognitive dimension of WEE FIM (rs=-0.460, P<0.001), as presented in Table 2.
Regarding the WEE FIM scale, there was a positive, strong, and significant correlation between the WEE FIM total score with its physical and cognitive dimensions (rs=+0.803, P<0.001; rs=+0.752, P=0.001), respectively and the physical and cognitive dimensions of WEE FIM scale (rs=+0.837, P<0.001), as presented in Table 2.
Discussion
Children with spastic diplegia have disabilities of the lower extremities resulting in dependency on their functional daily activities. Spasticity, muscle weakness, and activity limitations contribute to a lack of isolated motor control, limitations in their daily living activities, and also obesity in some children [8, 29]. This study assessed the relations between BMI, SVMC and functional independence in children with spastic diplegic CP. The findings showed a significant correlation between BMI, SVMC, functional independence, and spasticity in spastic diplegic CP children. This correlation was positive, strong, and significant between spasticity and BMI and between functional independence and SVMC; however, it was negative, strong and significant between spasticity and functional independence, between spasticity and SVMC, and between functional independence and BMI. The correlation was positive, moderate and significant between BMI and the level of gross motor function, and also between gross motor function level and spasticity, while it was negative, moderate, and significant between the level of gross motor function and functional independence and also between BMI and SVMC.
Many studies suggest different mechanisms by which children with CP are liable to becoming obese. One such mechanism is that children with CP often are premature babies which is associated with obesity [30]. In addition, children with CP face unique difficulties in the issues related to physical activity and functional ability. Hence, children with CP have a higher prevalence of overweight and obesity compared to their normal peers, especially the ones who can walk [20, 12]. In line with these studies, this study showed a significant negative correlation between functional independence and BMI.
The body composition of CP is affected by dietary components and also non-nutritional aspects such as impaired mobility, atypical movement patterns, motor impairment severity and type of CP that affect obesity. Karatekin et al. reported that normal children had a lower rate of obesity compared to ambulant children with CP. In addition, they found that gross motor function was significantly associated with BMI and weight [31].
Oftedal et al. [16] added that children with GMFCS levels II–V have a higher body fat percentage than those children with GMFCS level I, which is consistent with the positive significant correlation between GMFCS E&R and BMI in this study. Therefore, it is important to measure and follow BMI during the evaluation and rehabilitation of children with diplegic CP when the goal is to improve their functional independence and gross motor functions.
Laurent et al. showed in their cross-sectional study that a higher BMI was associated with a thinner prefrontal cortex and diminished executive functions in children [32]. In addition, Meo et al. observed significant impairments in cognitive functions in markedly obese students. [33]. This is in line with the results of this study which reported a negative significant correlation between BMI and the cognitive dimension of WEE FIM.
The response to physical activity in children with CP may vary according to the degree of motor impairment and the type of the disorder. Accordingly, in contrast to the results of this study which showed a positive significant correlation between GMFCS E&R and BMI, Arshad and Arora [34] showed a negative correlation. This can be illustrated by including all five levels of GMFCS E&R in their study, not only levels II and III.
Being active is more difficult for children with CP who have more severe motor affection than children who have mild impairment. They may have cognitive, perceptive, behavioral, or communication disorders in addition to disorders of muscle tone and strength, that negatively affect their functional ability in different ways [35]. This supports the results of the current study which found a negative significant correlation between gross motor function level with both functional ability and SVMC. Arruda et al. [35] added that in addition to the reduction in muscle strength and high muscle tone, other factors can likely explain more affected functional ability among children with greater motor impairment, such as skeletal muscle deformities and more frequent use of medications. This can illustrate the negative significant correlation between functional independence with both spasticity and gross motor function level in this study.
Reduced selective motor control and increased resistance to joint movement are important factors that influence gross motor function. Noble et al. [8] found a positive significant correlation between gross motor function and selectivity (r=0.901) and a negative significant correlation between gross motor function and MAS (r=-0.691), which comes in line with the results of this study.
Selective motor control disorders are affected by brain damage and are difficult to improve. Thus, SVMC is an important factor that affects motor function in children with CP. In this study, there was a negative strong correlation between SCALE scores and levels of gross motor function which are similar to findings of previous studies of SVMC in children with CP [36, 37].
Conclusion
This study shows a significant relationship between BMI, SVMC and functional independence in children with spastic diplegia. These results could have a remarkable future effect in educational, experimental, and clinical settings. This study provides evidence that BMI and SVMC impairments should be included while studying and clinically evaluating children with diplegic CP. Therapeutic intervention of SVMC should be carefully considered when planning a program to increase the functional independence of children with spastic diplegia. Also, regular height and weight measurement is an important factor in the rehabilitation programs that aim to increase functional abilities in these children.
Study limitations
The study included only children with spastic diplegic CP, which may limit the generalizability of the findings to other types of CP. The study included only children with GMFCS E&R levels II and III, which may exclude severely disabled children and limit the generalizability of the findings to other levels of GMFCS E&R. The study used MAS to assess spasticity, which has been questioned for its validity. More advanced measurements of spasticity, such as electromyography, may provide more accurate assessments of spasticity. Finally, the study did not account for the effects of medication use on the study outcomes, which may have confounded the results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Cairo University (Code: P.T.REC/012/003833) and followed the tenets of the Declaration of Helsinki. Children were only allowed to be included in this study after having a signed written consent form from their parents.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
References
Cerebral palsy (CP) is a disorder characterized by abnormal posture, tone, and movement and is classified clinically according to the predominant motor syndrome [1]. The overall CP birth prevalence for high-income countries is 1.6 per 1000 live births, while low-income countries showed marked higher birth prevalence [2], in addition to a higher prevalence of 60 to 150 per 1000 live births among preterm infants [3]. The most prevalent type of CP is spastic diplegia which is commonly associated with prematurity [4]. Children with spastic CP suffer from multiple neurological abnormalities, including muscle weakness, spasticity, and abnormal movement pattern [1]. Abnormal movement pattern occurs in children with spastic CP due to coordination problems which are caused by extensor or flexor synergies that interfere with isolated joint movement [5].
Selective voluntary motor control (SVMC) is an integral part of normal human motion and can independently control joint movement. Reduced SVMC is defined as a disturbance of the capability of isolating the muscle activation in selected patterns due to voluntary movement or posture demands [6] which means that a child with impaired SVMC does not have the expected activation pattern that is present in healthy children, either due to lack or excessive muscle activity [7]. This is one of the neuromuscular disorders associated with spastic CP and commonly coexists with muscle weakness and spasticity. All of the previously-mentioned motor disorders are related to the damage of the corticospinal tract and other descending motor pathways, resulting in interruption of the descending excitability and inhibitory signals leading to dysfunction [8, 9].
Children with CP have less energy consumption, and limited participation in physical activities compatible with their age compared to their healthy peers. Thus, the risk of obesity in these children is higher than in healthy subjects [10]. The prevalence of obesity in children with CP who are ambulant has increased from 7.7% to 16.5% in the last decade which affect negatively the general health of these children [11]. Through the analysis of body mass index (BMI) and waist-hip ratio, Bansal et al. suggest that children with CP have a high rate of being overweight and are at risk of being obese, particularly central obesity [12]. Fat mass can be assessed by several tools, such as hydrostatic weighing and dual-energy x-ray absorptiometry which are valid tools for measuring obesity. However, these tools have limited usage and are more invasive than BMI. Therefore, BMI is widely recommended by many institutions as the World Health Organization (WHO) and the World Obesity Federation [13, 14].
The risk of becoming overweight or obese increases throughout the range of dysfunction in children who have mild to moderate motor disabilities [15]. Obesity is of particular concern to children with CP because of the long-term health risks associated with obesity and the potentially increased impairment of functional mobility associated with obesity [16]. mDixon magnetic resonance images showed a lower intramuscular fat ratio in normal children than children with spastic CP who can ambulate [17]. Also, bioelectrical impedance analysis was used to estimate fat-free mass in preschool children with CP, and altered body composition was detected in these children across functional capacities [16].
Former studies have shown the relationship between lower limb SVMC and gait in children with CP [18, 19], and between health-related quality of life and BMI [20]; however, no available studies are detected regarding the relationship between BMI, isolated motor control, and functional independence in children with spastic diplegic CP. Accordingly, this study detects the relationship between BMI, SVMC and functional independence in children with spastic diplegic CP.
Materials and Methods
Study design and setting
This is an observational correlational study conducted between January to August 2022 at the Outpatient Clinic of the Faculty of Physical Therapy, Cairo University.
Sample size
G*Power statistical software, version 3.1 was used for estimating the sample size before the study using effect size=0.3, β=0.2 and α=0.05, which were calculated from a pilot study and showed that the total sample size is 84 children. Hence, 90 children were enrolled, considering prospective dropouts.
Participant recruitment and selection criteria
Initially, 90 children were enrolled and 6 children were excluded. Then, 2 children had lower limb surgical operations, and 4 subjects quit before the assessment termination. Accordingly, 84 children with spastic diplegic CP (32 male and 52 female) were involved in this study. The participants were selected from the Outpatient Clinic of the Faculty of Physical Therapy, Cairo University.
Children diagnosed as spastic diplegic CP, whose chronological age ranges from 6 up to 9 years, with spasticity levels +1 and 2 in the affected lower limbs as specified by the modified Ashworth scale (MAS), and levels II and III of the gross motor functional classification system expanded and revised (GMFCS E&R), who could follow the given instructions during the assessment were included in this study. The patients who had contractures of the lower limb joints were injected with botulinum toxin or any orthopedic surgery of the lower extremities in the last 6 months before the study, or who had epilepsy, were excluded from the study. Accordingly, Table 1 shows the characteristics of the participating children.
Testing procedures
Anthropometric measurements
A calibrated digital scale was used to measure children’s weight and Harpenden Stadiometer to measure their height. BMI was calculated as weight (kg)/height (m2). Growth charts for children and adolescents with ages ranging from 2–20 years were used to calculate the percentile scores of BMI, which consider the child’s age and sex. BMI was assigned, using these charts, to one of four categories: Underweight, healthy, overweight, or obese [21].
Selective control assessment of the lower extremity
The selective control assessment of the lower extremity (SCALE) is a reliable and valid scale used to evaluate SVMC of the toes, subtalar, ankle, knee, and hip joints in children with spastic CP [22]. The isolated movements are evaluated bilaterally. Scores of 2 (Normal), 1 (impaired), or 0 (unable) were given for each joint; 10 points for each limb, with 20 points as a total maximum score. Children were instructed to do specific isolated movements, reported in the SCALE, at each joint using a 3 s verbal count [22].
Pediatric functional independence measure (Wee-FIM)
The Wee-FIM is a reliable and valid scale used to evaluate the daily life activities of children with CP. Evaluation can be supplemented by observation of the child and interview with the caregiver, with 20 min administration time. This scale assesses the physical and cognitive ability of the child. It includes 6 domains of function which were evaluated in this study. Four of these are physical and two are cognitive. Items are scored with based on a 7-point ordinal scale, with 7 indicating complete independence and 1 showing total dependency. Caregiver assistance is needed for scores of 1 to 5. Higher scores indicate more independence with possible scores ranging from 18 to 126 [23].
The gross motor function classification system (GMFCS) expanded and revised
GMFCS E&R is a valid and reliable classification that differentiates children with CP following their gross motor abilities and limitations. It contains 5 levels [24]. The distinction between different levels, ranging from level I (the highest gross motor function) up to level V (the lowest level) is based on the need for assistive technology and functional abilities, rather than the quality of movement [25]. As nearly 98% of children with spastic diplegia are classified as level I, II, or III [26] and children with level I of GMFCS were more likely to have a healthy weight [27], only levels II and III were included in this study.
Modified Ashworth scale (MAS)
MAS is a widely accepted clinical tool that is used to measure spasticity. It is based on a 6-point ordinal scale with a grade score of 0, 1, +1, 2, 3 and 4, where a higher grade score indicates increased spasticity [28]. According to the MAS scoring system, the selected children were graded +1 and 2 which are the most available grades in the outpatient clinic during this study.
Statistical analysis
The relationship between BMI, SVMC and the level of functional independence in children with diplegic CP was assessed using correlation analysis. The SPSS software, version 25 was used to perform the statistical analyses. Descriptive statistics were expressed in numerical (n) and percent (%) formats, and Mean±SD. The Spearman correlation coefficient was selected to examine the relationships due to the ordinal nature of the data. A correlation was considered significant at a P<0.05.
Results
In this study, 84 children with spastic diplegic CP were selected. Table 1 displays the general characteristics of the children participating in the study. The results showed a positive, strong and significant correlation between MAS and BMI (rs=+0.677, P<0.001), WEE FIM total score and SCALE (rs=+0.718, P<0.001), the physical dimension of WEE FIM and SCALE (rs=+0.843, P<0.001), and the cognitive dimension of WEE FIM and SCALE (rs=+0.904, P<0.001); however, there was a negative, strong and significant correlation between MAS and WEE FIM total score (rs=-0.669, P<0.001), MAS and the physical dimension of WEE FIM (rs=-0.712, P<0.001), MAS and the cognitive dimension of WEE FIM, (rs=-0.793, P<0.001), MAS and SCALE (rs=-0.830, P<0.001), the cognitive dimension of WEE FIM and GMFCS (rs=-0.660, P<0.001), SCALE and GMFCS (rs=-0.707, P<0.001) and WEE FIM total score and BMI (rs=-0.607, P<0.001) as presented in Table 2.
In addition, there was a positive, moderate, and significant correlation between MAS and GMFCS (rs=+0.539, P<0.001) and BMI and GMFCS (rs=+0.53, P<0.032); however, there was a negative, moderate, and significant correlation between GMFCS and WEE FIM total score(rs=-0.540, P<0.001), GMFCS and the physical dimension of WEE FIM (rs=-0.531, P<0.001), BMI and SCALE (rs=-0.484, P<0.001), BMI and the physical dimension of WEE FIM (rs=-0.537, P<0.001) and BMI and the cognitive dimension of WEE FIM (rs=-0.460, P<0.001), as presented in Table 2.
Regarding the WEE FIM scale, there was a positive, strong, and significant correlation between the WEE FIM total score with its physical and cognitive dimensions (rs=+0.803, P<0.001; rs=+0.752, P=0.001), respectively and the physical and cognitive dimensions of WEE FIM scale (rs=+0.837, P<0.001), as presented in Table 2.
Discussion
Children with spastic diplegia have disabilities of the lower extremities resulting in dependency on their functional daily activities. Spasticity, muscle weakness, and activity limitations contribute to a lack of isolated motor control, limitations in their daily living activities, and also obesity in some children [8, 29]. This study assessed the relations between BMI, SVMC and functional independence in children with spastic diplegic CP. The findings showed a significant correlation between BMI, SVMC, functional independence, and spasticity in spastic diplegic CP children. This correlation was positive, strong, and significant between spasticity and BMI and between functional independence and SVMC; however, it was negative, strong and significant between spasticity and functional independence, between spasticity and SVMC, and between functional independence and BMI. The correlation was positive, moderate and significant between BMI and the level of gross motor function, and also between gross motor function level and spasticity, while it was negative, moderate, and significant between the level of gross motor function and functional independence and also between BMI and SVMC.
Many studies suggest different mechanisms by which children with CP are liable to becoming obese. One such mechanism is that children with CP often are premature babies which is associated with obesity [30]. In addition, children with CP face unique difficulties in the issues related to physical activity and functional ability. Hence, children with CP have a higher prevalence of overweight and obesity compared to their normal peers, especially the ones who can walk [20, 12]. In line with these studies, this study showed a significant negative correlation between functional independence and BMI.
The body composition of CP is affected by dietary components and also non-nutritional aspects such as impaired mobility, atypical movement patterns, motor impairment severity and type of CP that affect obesity. Karatekin et al. reported that normal children had a lower rate of obesity compared to ambulant children with CP. In addition, they found that gross motor function was significantly associated with BMI and weight [31].
Oftedal et al. [16] added that children with GMFCS levels II–V have a higher body fat percentage than those children with GMFCS level I, which is consistent with the positive significant correlation between GMFCS E&R and BMI in this study. Therefore, it is important to measure and follow BMI during the evaluation and rehabilitation of children with diplegic CP when the goal is to improve their functional independence and gross motor functions.
Laurent et al. showed in their cross-sectional study that a higher BMI was associated with a thinner prefrontal cortex and diminished executive functions in children [32]. In addition, Meo et al. observed significant impairments in cognitive functions in markedly obese students. [33]. This is in line with the results of this study which reported a negative significant correlation between BMI and the cognitive dimension of WEE FIM.
The response to physical activity in children with CP may vary according to the degree of motor impairment and the type of the disorder. Accordingly, in contrast to the results of this study which showed a positive significant correlation between GMFCS E&R and BMI, Arshad and Arora [34] showed a negative correlation. This can be illustrated by including all five levels of GMFCS E&R in their study, not only levels II and III.
Being active is more difficult for children with CP who have more severe motor affection than children who have mild impairment. They may have cognitive, perceptive, behavioral, or communication disorders in addition to disorders of muscle tone and strength, that negatively affect their functional ability in different ways [35]. This supports the results of the current study which found a negative significant correlation between gross motor function level with both functional ability and SVMC. Arruda et al. [35] added that in addition to the reduction in muscle strength and high muscle tone, other factors can likely explain more affected functional ability among children with greater motor impairment, such as skeletal muscle deformities and more frequent use of medications. This can illustrate the negative significant correlation between functional independence with both spasticity and gross motor function level in this study.
Reduced selective motor control and increased resistance to joint movement are important factors that influence gross motor function. Noble et al. [8] found a positive significant correlation between gross motor function and selectivity (r=0.901) and a negative significant correlation between gross motor function and MAS (r=-0.691), which comes in line with the results of this study.
Selective motor control disorders are affected by brain damage and are difficult to improve. Thus, SVMC is an important factor that affects motor function in children with CP. In this study, there was a negative strong correlation between SCALE scores and levels of gross motor function which are similar to findings of previous studies of SVMC in children with CP [36, 37].
Conclusion
This study shows a significant relationship between BMI, SVMC and functional independence in children with spastic diplegia. These results could have a remarkable future effect in educational, experimental, and clinical settings. This study provides evidence that BMI and SVMC impairments should be included while studying and clinically evaluating children with diplegic CP. Therapeutic intervention of SVMC should be carefully considered when planning a program to increase the functional independence of children with spastic diplegia. Also, regular height and weight measurement is an important factor in the rehabilitation programs that aim to increase functional abilities in these children.
Study limitations
The study included only children with spastic diplegic CP, which may limit the generalizability of the findings to other types of CP. The study included only children with GMFCS E&R levels II and III, which may exclude severely disabled children and limit the generalizability of the findings to other levels of GMFCS E&R. The study used MAS to assess spasticity, which has been questioned for its validity. More advanced measurements of spasticity, such as electromyography, may provide more accurate assessments of spasticity. Finally, the study did not account for the effects of medication use on the study outcomes, which may have confounded the results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Cairo University (Code: P.T.REC/012/003833) and followed the tenets of the Declaration of Helsinki. Children were only allowed to be included in this study after having a signed written consent form from their parents.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
References
- Patel DR, Neelakantan M, Pandher K, Merrick J. Cerebral palsy in children: A clinical overview. Translational Pediatrics. 2020; 9(Suppl 1):S125-35. [DOI:10.21037/tp.2020.01.01] [PMID]
- McIntyre S, Goldsmith S, Webb A, Ehlinger V, Hollung SJ, McConnell K, et al. Global prevalence of cerebral palsy: A systematic analysis. Developmental Medicine and Child Neurology. 2022; 64(12):1494-506. [DOI:10.1111/dmcn.15346] [PMID]
- Oskoui M, Coutinho F, Dykeman J, Jetté N, Pringsheim T. An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Developmental Medicine & Child Neurology. 2013; 55(6):509-19. [DOI:10.1111/dmcn.12080]
- Bourgleh S, Nemeş RN, Hetaimish B, Burileanu AH, Fallatah S, Chiuţu LC. Cerebral Palsy. Considerations upon 249 consecutive patients and review of literature. Current Health Sciences Journal. 2019; 45(4):405-11. [PMID]
- Zhou JY, Lowe E, Cahill-Rowley K, Mahtani GB, Young JL, Rose J. Influence of impaired selective motor control on gait in children with cerebral palsy. Journal of Children's Orthopaedics. 2019; 13(1):73-81. [DOI:10.1302/1863-2548.13.180013] [PMID]
- Sanger TD, Chen D, Delgado MR, Gaebler-Spira D, Hallett M, Mink JW et al. Definition and classification of negative motor signs in childhood. Pediatrics. 2006; 118(5):2159-67. [DOI:10.1542/peds.2005-3016] [PMID]
- Fahr A, Keller JW, van Hedel HJA. A systematic review of training methods that may improve selective voluntary motor control in children with spastic cerebral palsy. Frontiers in Neurology. 2020; 11:572038. [DOI:10.3389/fneur.2020.572038] [PMID]
- Noble JJ, Gough M, Shortland AP. Selective motor control and gross motor function in bilateral spastic cerebral palsy. Developmental Medicine and Child Neurology. 2019; 61(1):57-61. [DOI:10.1111/dmcn.14024] [PMID]
- Cahill-Rowley K, Rose J. Etiology of impaired selective motor control: Emerging evidence and its implications for research and treatment in cerebral palsy. Developmental Medicine & Child Neurology. 2014; 56(6):522-8. [DOI:10.1111/dmcn.12355] [PMID]
- Kiernan D, Nikolopoulou C, Brady K. Prevalence of overweight and obesity in Irish ambulant children with cerebral palsy. Irish Journal of Medical Science. 2021; 190(1):225-31. [DOI:10.1007/s11845-020-02294-4] [PMID]
- Rogozinski BM, Davids JR, Davis RB, Christopher LM, Anderson JP, Jameson GG, et al. Prevalence of obesity in ambulatory children with cerebral palsy. Journal of Bone and Joint Surgery. 2007; 89(11):2421-6. [DOI:10.2106/JBJS.F.01080] [PMID]
- Bansal A, Diwan S, Diwan J, Vyas N. Prevalance of obesity in children with cerebral palsy. Journal of Clinical and Diagnostic Research. 2014; 8(8):BC08-11. [PMID]
- Duran I, Schulze J, Martakis K, Stark C, Schoenau E. Diagnostic performance of body mass index to identify excess body fat in children with cerebral palsy. Developmental Medicine and Child Neurology. 2018; 60(7):680-6. [DOI:10.1111/dmcn.13714] [PMID]
- WHO. Body mass index (BMI). Geneva: WHO; 2023. [Link]
- Hurvitz EA, Green LB, Hornyak JE, Khurana SR, Koch LG. Body mass index measures in children with cerebral palsy related to gross motor function classification: A clinic-based study. American Journal of Physical Medicine & Rehabilitation. 2008; 87(5):395-403. [DOI:10.1097/PHM.0b013e3181617736] [PMID]
- Oftedal S, Davies PS, Boyd RN, Stevenson RD, Ware RS, Keawutan P, et al. Body composition, diet, and physical activity: A longitudinal cohort study in preschoolers with cerebral palsy. The American Journal of Clinical Nutrition. 2017; 105(2):369-78. [DOI:10.3945/ajcn.116.137810] [PMID]
- D'Souza A, Bolsterlee B, Lancaster A, Herbert RD. Intramuscular fat in children with unilateral cerebral palsy. Clinical Biomechanics. 2020; 80:105183. [DOI:10.1016/j.clinbiomech.2020.105183] [PMID]
- Papageorgiou E, Simon-Martinez C, Molenaers G, Ortibus E, Van Campenhout A, Desloovere K. Are spasticity, weakness, selectivity, and passive range of motion related to gait deviations in children with spastic cerebral palsy? A statistical parametric mapping study. Plos One. 2019; 14(10):e0223363.[DOI:10.1371/journal.pone.0223363] [PMID]
- Chruscikowski E, Fry NRD, Noble JJ, Gough M, Shortland AP. Selective motor control correlates with gait abnormality in children with cerebral palsy. Gait & Posture. 2017; 52:107-9. [DOI:10.1016/j.gaitpost.2016.11.031] [PMID]
- Şimşek TT, Tuç G. Examination of the relation between body mass index, functional level and health-related quality of life in children with cerebral palsy. Türk Pediatri Arşivi. 2014; 49(2):130-7. [DOI:10.5152/tpa.2014.1238] [PMID]
- Kuczmarski RJ. CDC growth charts: united states. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2000. [Link]
- Sukal-Moulton T, Fowler E. Selective voluntary motor control in children and youth with spastic cerebral palsy. In: Miller F, Bachrach S, Lennon N, O'Neil ME, editors. Cerebral Palsy. Cham: Springer; 2020. [DOI:10.1007/978-3-319-74558-9_162]
- Kim GW, Kim H, Jeon JY, Jang JS. Validity and reliability of functional independence measure for children (WeeFIM) for children with cerebral palsy. Inquiry (United States). 2022; 59:469580211072454. [DOI:10.1177/00469580211072454] [PMID]
- Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH. Content validity of the expanded and revised gross motor function classification system. Developmental Medicine and Child Neurology. 2008; 50(10):744-50. [DOI:10.1111/j.1469-8749.2008.03089.x] [PMID]
- Cerebral Palsy Guidance. Cerebral Palsy Gross Motor Classification System [Internet]. 2024 [Updated 15 January 2024]. Available from: [Link]
- Karen Pape. Cerebral Palsy - Diplegia - GMFCS I to III - KAREN PAPE, MD [Internet]. 2021 [Updated 13 April 2023]. Available from: [Link]
- Pascoe J, Thomason P, Graham HK, Reddihough D, Sabin MA. Body mass index in ambulatory children with cerebral palsy: A cohort study. Journal of Paediatrics and Child Health. 2016; 52(4):417-21. [DOI:10.1111/jpc.13097] [PMID]
- Harb A, Kishner S. Modified Ashworth Scale. StatPearls [Internet]. 2022 [Updated 12 April 2023]. Available from: [Link]
- Kusumoto Y, Takaki K, Matsuda T, Nitta O. Relation of selective voluntary motor control of the lower extremity and extensor strength of the knee joint in children with spastic diplegia. Journal of Physical Therapy Science. 2016; 28(6):1868-71. [DOI:10.1589/jpts.28.1868] [PMID]
- Gurka MJ, Kuperminc MN, Busby MG, Bennis JA, Grossberg RI, Houlihan CM, et al. Assessment and correction of skinfold thickness equations in estimating body fat in children with cerebral palsy. Developmental Medicine and Child Neurology. 2010; 52(2):e35-41. [DOI:10.1111/j.1469-8749.2009.03474.x] [PMID]
- Karatekin BD, Kacar G, Icagasioglu A. Obesity in ambulatory children with cerebral palsy in Turkey: A cross-sectional study. Journal of Pediatric Rehabilitation Medicine. 2023; 16(1):195-202. [DOI:10.3233/PRM-210093] [PMID]
- Laurent JS, Watts R, Adise S, Allgaier N, Chaarani B, Garavan H, et al. Associations Among Body Mass Index, cortical thickness, and executive function in children. JAMA Pediatrics. 2020; 174(2):170-7. [DOI:10.1001/jamapediatrics.2019.4708] [PMID]
- Meo SA, Altuwaym AA, Alfallaj RM, Alduraibi KA, Alhamoudi AM, Alghamdi SM, et al. Effect of obesity on cognitive function among school adolescents: A cross-sectional study. Obesity Facts. 2019; 12(2):150-6. [DOI:10.1159/000499386] [PMID]
- Arshad S, Arora S. Co-Relation between Body Mass Index and gross motor function classification in children with cerebral palsy. Journal of Medical and Dental Science Research. 2021; 8(8):55-8. [Link]
- Arruda RCBF, Tassitano RM, da Silva Brito AL, de Sousa Martins OS, Cabral PC, de Castro Antunes MM. Physical activity, sedentary time and nutritional status in Brazilian children with cerebral palsy. Jornal de Pediatria. 2022; 98(3):303-9. [DOI:10.1016/j.jped.2021.07.005] [PMID]
- Inoue T, Yokoi Y. Characteristics of selective motor control of the lower extremity in adults with bilateral spastic cerebral palsy. Journal of Physical Therapy Science. 2020; 32(5):348-51. [DOI:10.1589/jpts.32.348] [PMID]
- Balzer J, Marsico P, Mitteregger E, van der Linden ML, Mercer TH, van Hedel HJ. Construct validity and reliability of the Selective Control Assessment of the Lower Extremity in children with cerebral palsy. Developmental Medicine and Child Neurology. 2016; 58(2):167-72. [DOI:10.1111/dmcn.12805] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2022/11/29 | Accepted: 2023/10/11 | Published: 2024/03/16
Received: 2022/11/29 | Accepted: 2023/10/11 | Published: 2024/03/16
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
