
988368
Tue, Jul 8, 2025

Volume 22, Issue 1 (March 2024)
Iranian Rehabilitation Journal 2024, 22(1): 107-116 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Taghipour M, Ramezani M, Oliaei F, Bahrami M. Comparison of Taping and Mobilization on Pain, Range of Motion and Shoulder Disability in Sub Acromial Impingement Syndrome in Dialysis Patients. Iranian Rehabilitation Journal 2024; 22 (1) :107-116
URL: http://irj.uswr.ac.ir/article-1-1849-en.html
URL: http://irj.uswr.ac.ir/article-1-1849-en.html



1- Mobility Impairment Research Center, Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran.
2- Department of Physiotherapy, School of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
3- Department of Internal Medicine, School of Medicine, Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran.
4- Department of Orthopedics, School of Medicine, Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran.
2- Department of Physiotherapy, School of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
3- Department of Internal Medicine, School of Medicine, Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran.
4- Department of Orthopedics, School of Medicine, Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran.
Keywords: Subacromial impingement syndrome, Hemodialysis, Deltoid kinesio taping, Supraspinatus kinesio taping, Shoulder mobilization
Full-Text [PDF 947 kb]
(842 Downloads)
| Abstract (HTML) (2240 Views)
Full-Text: (538 Views)
Introduction
Shoulder pain is one of the most common complaints among patients of different age groups when they seek treatment at various clinics. It is often attributed to issues related to the rotator cuff, such as defects, or subacromial impingement syndrome (SAIS) [1-3]. In this syndrome, the supraspinatus tendon, shoulder capsule, and subacromial bursa, as well as the long head of the biceps tendon are involved [4]. This syndrome mainly occurs unilaterally and between the ages of 20 and 65 [3, 5, 6]. SAIS can lead to various impairments, including reduced strength, coordination issues, disruption of the shoulder’s rotator cuff and girdle muscles, alterations in mechanical and anatomical structures, and scapular instability. Additionally, it results in limitations in shoulder mobility [7]. A common cause of this syndrome is supraspinatus tendonitis, with approximately 80% of hemodialysis patients experiencing supraspinatus tendinopathy, with key complaints about shoulder pain and musculoskeletal discomfort pain during dialysis [8, 9]. In dialysis patients, factors contributing to SAIS include calcium buildup in the bones due to hyperparathyroidism, elevated levels of B2 microglobulin (B2M) protein, and amyloidosis. Changes in iron, potassium, phosphate, aluminum, the amino acid L-carnitine, and thyroid levels can also contribute to muscle dysfunction. Additionally, not using the fistula hand can lead to the syndrome developing in the opposite hand due to overuse [10-14]. There are many physiotherapy treatments for patients with SAIS, including electrotherapy, manual therapy, and exercise therapy 6. Among the non-invasive methods, oscillatory mobilization affecting the circulatory system, including ischemia, fibrosis, and inflammatory chemicals can be mentioned, causing these substances to move away from the site, thus reducing pain and inflammation [15-17]. Mobilization of the upper and lower limb joints has positive effects on the lives of hemodialysis patients. Patients who undergo mobilization tend to experience improved sleep patterns, reduced pain, and an overall enhanced sense of well-being [18]. Also, mobilization of the joints of the upper and lower limbs has positive effects on blood circulation, blood pressure regulation, and the reduction of edema and muscle atrophy. This, in turn, contributes to a better quality of life and increased activity levels among dialysis patients [19]. Through stimulating kinematic sense and mechanoreceptors in the joint, this technique reduces pain while increasing the shoulder joint range of motion (ROM) [20].
Kinesio tape is another non-invasive intervention used to treat these patients [21]. It is a new method with beneficial effects, particularly when an immediate effect is needed. The immediate effects of Kinesio tape may be due to the creation of the right direction and improvement of the lymph fluid movement in the subacromial area [22, 23]. The characteristics of Kinesio tape elastic tissue are similar to those of human skin. Its application is considered a functional treatment that doesn’t hinder the patient’s daily activities and allows them to perform their usual tasks [21].
Kaya et al. argued that as an adjunctive and non-invasive treatment, Kinesio tape could be employed in the treatment of SAIS, particularly for patients unable to perform daily physiotherapy. Since the tape remains on the patient’s skin after the physiotherapy session, it does not impose any limitations on the patient’s daily activities, such as exercising, showering, swimming, etc. [23]. To the best of our knowledge, performing mobilization and Kinesio tape interventions at the time of the patient’s visit for dialysis, without the need to move the patient and without returning to the physiotherapy department, can be a suitable treatment (in terms of time and cost). Given the growing population of dialysis patients and the prevalence of SAIS among them, which significantly affects their health and quality of life, we conducted a study to compare pain intensity at rest and during active shoulder abduction, shoulder active abduction ROM, and shoulder functional disability in two groups: One receiving mobilization alone and the other receiving both mobilization and Kinesio taping in dialysis patients with SAIS.
Materials and Methods
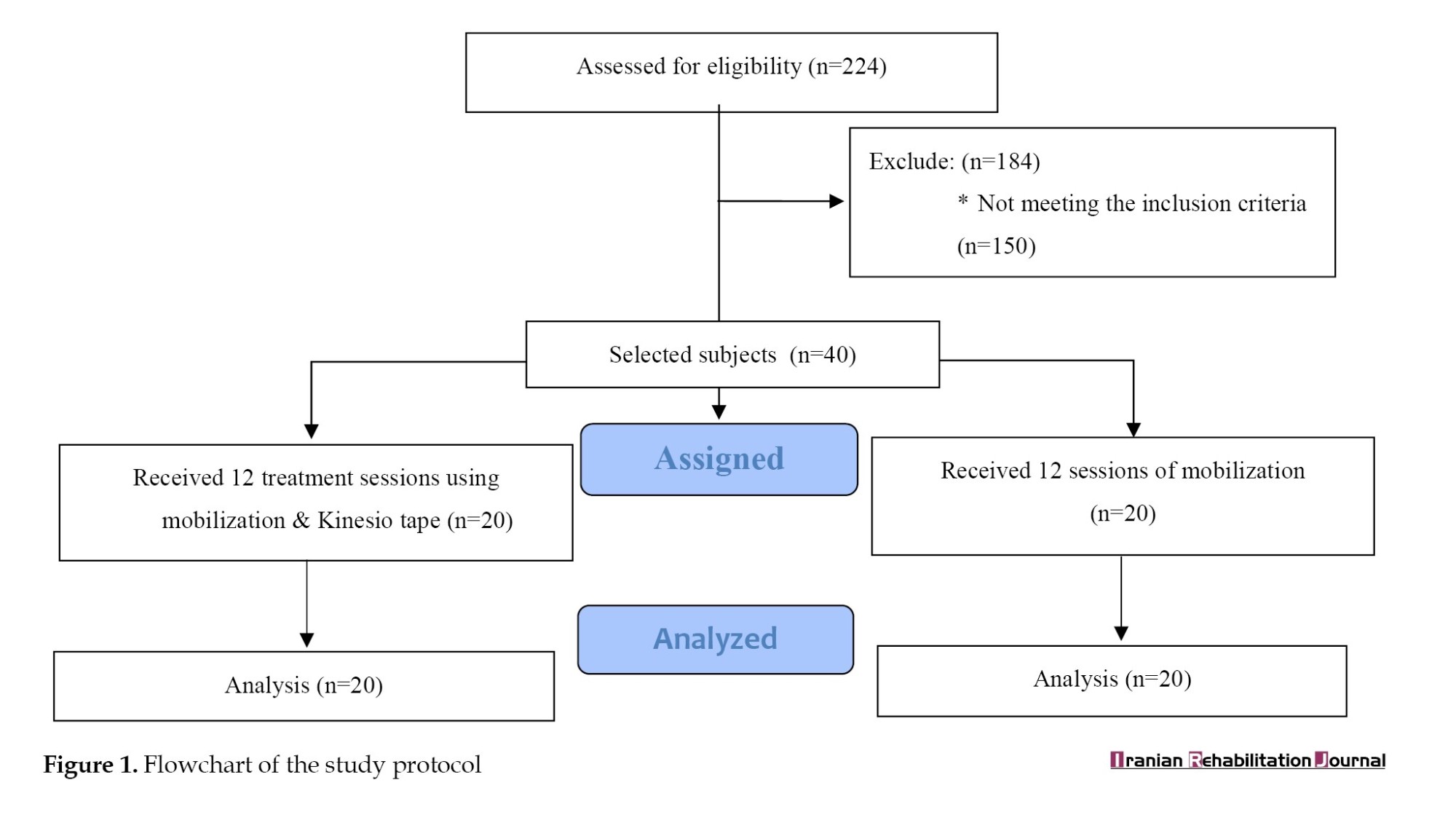
In this study, out of the 224 dialysis patients at Shahid Beheshti Hospital in Babol, 74 met our inclusion criteria. However, 34 of them were unwilling to participate. Ultimately, 40 dialysis patients with SAIS (22 women and 18 men) within the age range of 40-60 years agreed to take part in our study (Figure 1). The assessment and treatment using mobilization and Kinesio tape techniques were carried out for these patients in the dialysis ward of Shahid Beheshti Hospital of Babol by a physiotherapist.
Inclusion criteria included positiveness of at least one of the shoulder’s tests (Hawkins, Neer, and painful arch), dialysis for more than six months, pain of shoulder joint for more than two months, and shoulder pain in anterior and anterior-lateral area [5, 15, 24-26]. Exclusion criteria included neck pain consequent of radiculopathy, trauma, and shoulder fracture in the last six months, shoulder and breast surgery, cervical rib, pregnancy, cancer, sensitive skin to Kinesio tape, history of physiotherapy or corticosteroid injection in the last three months, rheumatoid arthritis (RA) disease, and the use of nonsteroidal anti-inflammatory drugs [27-32]. After receiving an explanation of the research methodology, the subjects provided written consent. Demographic information about the subjects, including their sex, age, body mass index (BMI), duration of dialysis initiation, number of dialysis sessions per week, and onset duration of pain, was collected through patient files, questionnaires, and interviews.
Using Stata software, version 24 the sample size of this study was specified, following the approach outlined in Kaya et al.’s study [33]. Moreover, based on the study by Joyce et al. [34], the minimal clinically important difference (MCID) was set at 1.37 for the visual analog scale (VAS) and 2 for the standard deviation (SD). Assuming a significance level (α) of 0.05 and a power of 80%, a sample size of 20 individuals was calculated for each group. The patients were randomly divided into two groups: Mobilization alone (20 patients) and mobilization with Kinesio taping (20 patients). Randomization was achieved using a block size of 4 and a block number of ten.
Outcome measures
Primary outcome measures included
A) The intensity of shoulder pain at rest was measured by a numerical pain rating scale [35]. B) Pain intensity during active shoulder abduction movement, for measuring which the numerical pain scale was employed [35].
Secondary outcome measures included
A) Active abduction ROM of the shoulder was assessed using a goniometer [36, 37]. To measure the degree of active shoulder abduction, the patient was supine and the shoulder was placed in external rotation. The support of the goniometer axis was placed on the anterior edge of the acromion, the fixed arm was placed parallel to the longitudinal axis of the sternum, and the movable arm was placed parallel to the longitudinal axis of the humors [38]. B) The degree of shoulder functional disability was assessed by the disabilities of the arm, shoulder, and hand (DASH) questionnaire [39].
The DASH questionnaire contains 30 questions about the symptoms and function of the upper limb involved in orthopedic and neurological disorders [40]. Each question has five parts providing a range of scores from 1–5. A higher score indicates greater symptoms so that if there is no symptom, it is considered as one, and if there is the most disability and symptoms, it is considered five [40]. In the DASH scale, a higher score indicates a greater level of disability and severity, whereas, lower scores indicate a lower level of disability. The score on this test ranges from 0 (no disability) to 100 (most severe disability) [40]. The obtained score is minus 30 and divided by the maximum score minus the minimum score [40].
Intervention
First group
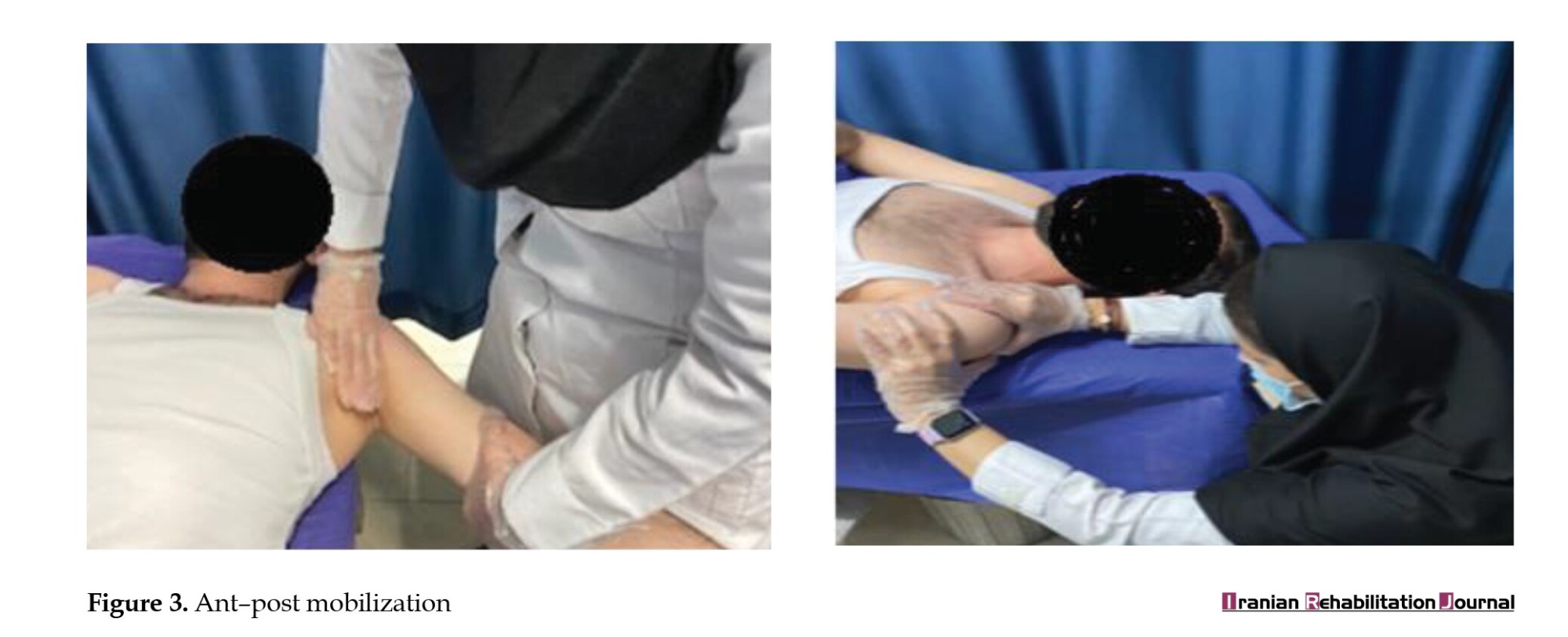
This group, referred to as the mobilization-alone group, consisted of dialysis patients with SAIS who received mobilization grades I and II. This mobilization involved caudal, anterior, and posterior movements of the glenohumeral joint [41]. Passive oscillatory movements were performed at the rate of 2-3 glides per second for 30 seconds and each glide was given for five sets, which was totally applied for about 4 to 5 minutes. Finally, 12-15 minutes of mobilization was performed in each session. This method was used three times a week for four weeks (12 sessions) 17 (Figures 2 and 3).

Second group
In addition to mobilization, Kinesio tape was applied to the deltoid and supraspinatus muscles in this group. Mobilization and the new Kinesio tape intervention were alternated every 12 sessions (every other day). The Kinesio tape used in this study was the BioBalance brand, manufactured in Korea.
Kinesio tape application method
Supraspinatus muscle Kinesio tape
The beginning of the Kinesio tape is placed from the humorous tubercle without tension, then the shoulder is placed in horizontal adduction and the hand is in pronation, and the Kinesio tape is placed on the top and bottom of the scapula spine with 10-15% tension and the two ends of the Y of the Kinesio tape without tension on the transverse process of T2 and T4 was attached at the end [21].
To apply the Kinesio tape of the deltoid muscle
The Kinesio tape was first placed on the deltoid tubercle without tension and followed the two ends of the Y-strip Kinesio tape of the anterior and posterior deltoid muscles. The anterior deltoid muscle of the shoulder should be in the extension position and the posterior deltoid muscle of the shoulder should be in the flexion position. The Kinesio tape was applied with 10-15% tension on the muscle belly, and then, the end of the Kinesio tape was attached without tension on the front and back of the big tubercle [21] (Figure 4).

Evaluation of primary and secondary outcomes was done in three phases: Before treatment, after treatment (after 12 sessions), and in the follow-up phase (ten days after treatment. SPSS software, version 18 was used for data analysis. Before analyzing the main variables, we used the Kolmogorov-Smirnov test to assess the normal distribution of the variables, but the normality of the data distribution was not confirmed [42]. Therefore, the nonparametric Friedman test was used for intragroup comparisons [42]. The Wilcoxon’s test was applied to compare different time points in the same group [44]. The Mann-Whitney test was applied to compare the mean values between the two groups at different time points [42].
Results
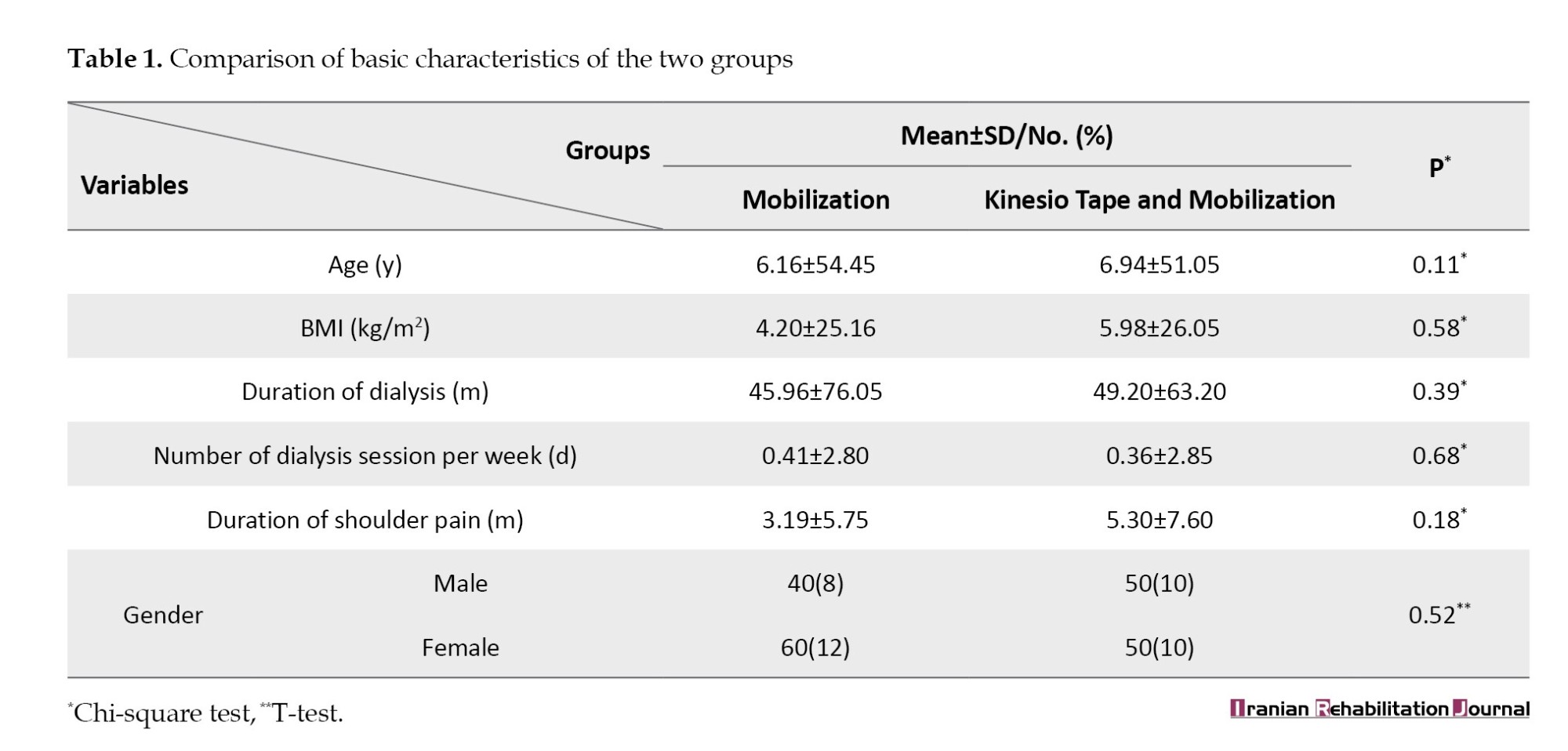
Forty dialysis patients with SAIS were divided into two groups: Mobilization alone and mobilization with Kinesio taping, participating in our study. No significant differences were observed between the two groups in terms of demographic variables, duration of dialysis, dialysis sessions per week, and the duration of pain onset. Thus, the matching of the groups was confirmed (Table 1).
Using the Friedman test in both groups, the results revealed a decrease in pain intensity at rest and during active shoulder abduction, an increase in the ROM of shoulder active abduction, and a decrease in shoulder functional disability (P<0.001). The effect size of the treatment was strong in both groups using Kendall value [42] (Table 2).
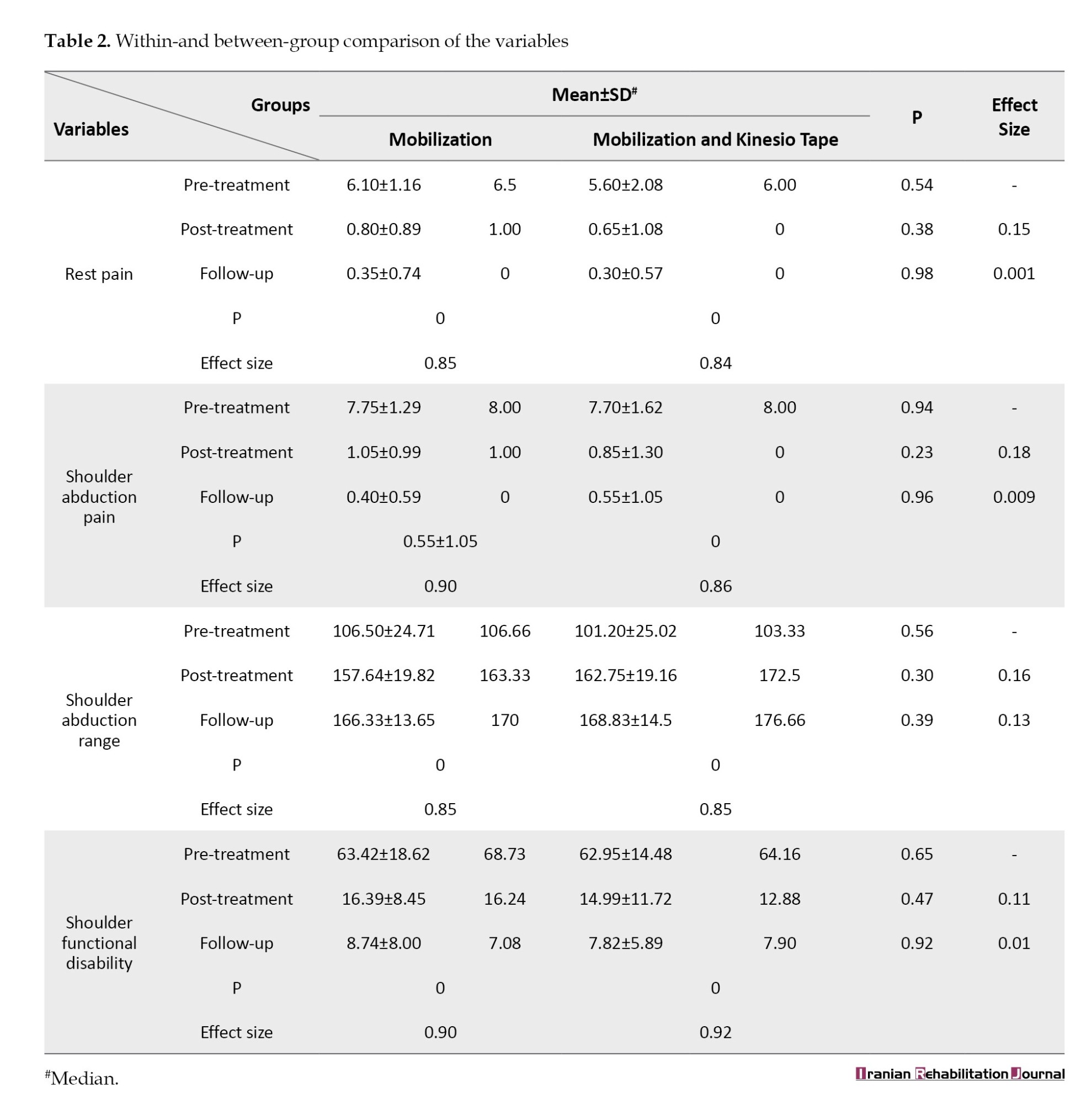
Using the Wilcoxon test for pairwise comparison of pre-treatment with post-treatment times, pre-treatment with follow-up exhibited a significant difference in all parameters in both groups (P≤0.05). Nevertheless, the comparison results between post-treatment and follow-up revealed a significant difference between all parameters except shoulder pain at rest time in both groups and pain during active shoulder abduction in the mobilization and Kinesio taping group (P≥0.05) (Table 2). The Mann-Whitney test showed no significant difference between the two groups after treatment and in the follow-up (P≥0.05). The rank-biserial correlation (r) value showed that the effect size between the two groups in all parameters after treatment was stronger than in the follow-up (Table 2).
Discussion
This study aimed to compare the effects of mobilization with Kinesio taping and mobilization alone on pain intensity, ROM, and shoulder functional disability in dialysis patients with SAIS. The results showed after 12 intervention sessions, both mobilization alone and mobilization with Kinesio taping reduced pain intensity at rest and during active shoulder abduction, increased the ROM of shoulder active abduction, and decreased shoulder functional disability in dialysis patients with SAIS and this effect lasted for up to ten days after the end of treatment.
Mobilization may control pain by activating mechanoreceptors and inhibiting nociceptors, thereby modulating the pain gate and reducing the individual’s perception of pain [43]. Also, manual therapy declines swelling and pain in SAIS by improving synovial fluid movement and abnormal collagen traction. In the present study, mobilization grades I and II in the glenohumeral joint were used, which may have enhanced the subacromial area by reducing pain and inflammation while improving blood flow. Following mobilization, there was an increase in active shoulder abduction ROM and a decrease in the degree of shoulder functional disability [44].
In the current study, adding Kinesio tape to mobilization was not able to improve the mobilization’s therapeutic effect. It is possible that in dialysis patients with SAIS, who experience an imbalance between the rotator cuff and deltoid muscles, along with the upward force exerted on the glenohumeral joint by the deltoid muscle, the subacromial area becomes reduced. In this study, the Kinesio tape was used to inhibit the rotator cuff muscles with tendonitis and suppress the deltoid muscle. Park et al. reported Kinesio tape’s effects on reducing pain, inflammation, and correct movement improvement [7]. Nevertheless, in the present study, Kinesio tape was employed on most patients with SAIS and fistula hand. Dialysis patients are usually advised not to use their fistula hand, and due to their sedentary lifestyle and musculoskeletal problems, they may not be able to accurately report the effect of Kinesio tape on their upper limb function.
Furthermore, it is possible that due to the compromised muscle function in dialysis patients resulting from the pathophysiology of hemodialysis, the inhibition of the deltoid and supraspinatus muscles by Kinesio tape is not as effective in reducing pain, increasing ROM, and decreasing the degree of shoulder functional disability as it might be in non-dialysis patients.
Previous studies have assessed the effects of Kinesio tape and mobilization on non-dialysis patients with SAIS. As far as we know, this is the first study to investigate the effects of Kinesio tape on SAIS in dialysis patients.
Our results were in line with those of Senbursa et al. and Maricar et al. and Kachingwe et al. These studies reported that mobilization associated with exercise was effective in reducing pain intensity and shoulder functional disability as well as increasing shoulder ROM in non-dialysis patients with SAIS. Although the present study only performed mobilization as a treatment, its effects were similar to the results of other studies [45-47]. In this regard, Park et al. examined the effects of mobilization with Kinesio taping on SAIS in five non-dialysis patients and showed reduced pain intensity and increased ROM, as well as decreased rotator cuff muscle tone and stiffness. In this study, by reducing the fascia layers, Kinesio tape reduced muscle tone, thus reducing pain and increasing ROM [7]. Furthermore, Thelen et al. reported that after the application of Kinesio tape in non-dialysis SAIS, the pain intensity during movement immediately declined in the Kinesio tape-treated group compared to the placebo group, while a Kinesio tape effect alone was not observed in our study. This discrepancy may be attributed to the fact that Thelen’s study had a sample of younger non-dialysis patients compared to our study, and they lacked a control group [22].
Our study results were different from those of Shakeri et al. who reported a greater of Kinesio tape compared to Kinesio tape placebo using the DASH questionnaire in non-dialysis patients with SAIS. Perhaps the higher effectiveness of Kinesio tape in their study was due to the three-day interval between Kinesio tape sessions. However, in the present study, a one-day interval between Kinesio tape sessions may have stimulated changes in the subacromial area structure. Additionally, differences in the type of Kinesio tape, the expertise in applying and securing the Kinesio tape, and the Kinesio tape application method (50% tension for deltoid muscle and lower trapezius in the above study, compared to 10-15% tension for deltoid muscle and supraspinatus in our study) could account for variations in results [48].
Among the research that has so far investigated the effects of mobilization and Kinesio taping as well as mobilization alone on patients with SAIS, our study is the first one to examine the effects of these two treatment methods on dialysis patients with SAIS, and the sample size in the above study has been with 80% power.
Among the limitations of our study, we can mention the lack of patient examination by means of MRI, CT SCAN, x-ray, and ultrasound because of the difficult mobility of patients besides the small number of samples for normalization and short-term treatment follow-up (10 days).
It is suggested to apply mobilization in a different time period than the above-mentioned study (4-5 minutes), examine patients based on the type of tissue involved and the severity of pain, and apply mobilization in other directions of the shoulder and other Kinesio tape techniques of SAIS using larger sample sizes and longer follow-up with the help of exercise therapy and physiotherapy modalities to treat these patients. Using MRI, ultrasound, etc. as objective evaluation indicators is also recommended.
Conclusion
Both mobilization alone and mobilization combined with Kinesio taping were effective in declining the pain intensity at rest during active shoulder abduction, increasing the ROM of shoulder active abduction, and decreasing the degree of shoulder functional disability. Due to the absence of a significant difference between the two methods in our study, it can be concluded that adding Kinesio tape to mobilization compared to mobilization alone had no additional impacts on pain at rest and during active shoulder abduction, increasing active shoulder abduction ROM, and reducing shoulder functional disability in dialysis subjects with SAIS.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Babol University of Medical Sciences (Code: IRMUBABOL.REC.1399297). It was also registered at the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20091274002851N5).
Funding
This study was financially supported by the Babol University of Medical Sciences (Code: 9910528).
Authors' contributions
Conceptualization and supervision: Mohammad Taghipour; Methodology: Mohammad Taghipour and Mona Ramezani; Data collection: Mona Ramezani; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patients for participation in this research and also the staff of Shahid Beheshti Hospital and the Babol University of Medical Sciences.
References
Shoulder pain is one of the most common complaints among patients of different age groups when they seek treatment at various clinics. It is often attributed to issues related to the rotator cuff, such as defects, or subacromial impingement syndrome (SAIS) [1-3]. In this syndrome, the supraspinatus tendon, shoulder capsule, and subacromial bursa, as well as the long head of the biceps tendon are involved [4]. This syndrome mainly occurs unilaterally and between the ages of 20 and 65 [3, 5, 6]. SAIS can lead to various impairments, including reduced strength, coordination issues, disruption of the shoulder’s rotator cuff and girdle muscles, alterations in mechanical and anatomical structures, and scapular instability. Additionally, it results in limitations in shoulder mobility [7]. A common cause of this syndrome is supraspinatus tendonitis, with approximately 80% of hemodialysis patients experiencing supraspinatus tendinopathy, with key complaints about shoulder pain and musculoskeletal discomfort pain during dialysis [8, 9]. In dialysis patients, factors contributing to SAIS include calcium buildup in the bones due to hyperparathyroidism, elevated levels of B2 microglobulin (B2M) protein, and amyloidosis. Changes in iron, potassium, phosphate, aluminum, the amino acid L-carnitine, and thyroid levels can also contribute to muscle dysfunction. Additionally, not using the fistula hand can lead to the syndrome developing in the opposite hand due to overuse [10-14]. There are many physiotherapy treatments for patients with SAIS, including electrotherapy, manual therapy, and exercise therapy 6. Among the non-invasive methods, oscillatory mobilization affecting the circulatory system, including ischemia, fibrosis, and inflammatory chemicals can be mentioned, causing these substances to move away from the site, thus reducing pain and inflammation [15-17]. Mobilization of the upper and lower limb joints has positive effects on the lives of hemodialysis patients. Patients who undergo mobilization tend to experience improved sleep patterns, reduced pain, and an overall enhanced sense of well-being [18]. Also, mobilization of the joints of the upper and lower limbs has positive effects on blood circulation, blood pressure regulation, and the reduction of edema and muscle atrophy. This, in turn, contributes to a better quality of life and increased activity levels among dialysis patients [19]. Through stimulating kinematic sense and mechanoreceptors in the joint, this technique reduces pain while increasing the shoulder joint range of motion (ROM) [20].
Kinesio tape is another non-invasive intervention used to treat these patients [21]. It is a new method with beneficial effects, particularly when an immediate effect is needed. The immediate effects of Kinesio tape may be due to the creation of the right direction and improvement of the lymph fluid movement in the subacromial area [22, 23]. The characteristics of Kinesio tape elastic tissue are similar to those of human skin. Its application is considered a functional treatment that doesn’t hinder the patient’s daily activities and allows them to perform their usual tasks [21].
Kaya et al. argued that as an adjunctive and non-invasive treatment, Kinesio tape could be employed in the treatment of SAIS, particularly for patients unable to perform daily physiotherapy. Since the tape remains on the patient’s skin after the physiotherapy session, it does not impose any limitations on the patient’s daily activities, such as exercising, showering, swimming, etc. [23]. To the best of our knowledge, performing mobilization and Kinesio tape interventions at the time of the patient’s visit for dialysis, without the need to move the patient and without returning to the physiotherapy department, can be a suitable treatment (in terms of time and cost). Given the growing population of dialysis patients and the prevalence of SAIS among them, which significantly affects their health and quality of life, we conducted a study to compare pain intensity at rest and during active shoulder abduction, shoulder active abduction ROM, and shoulder functional disability in two groups: One receiving mobilization alone and the other receiving both mobilization and Kinesio taping in dialysis patients with SAIS.
Materials and Methods
In this study, out of the 224 dialysis patients at Shahid Beheshti Hospital in Babol, 74 met our inclusion criteria. However, 34 of them were unwilling to participate. Ultimately, 40 dialysis patients with SAIS (22 women and 18 men) within the age range of 40-60 years agreed to take part in our study (Figure 1). The assessment and treatment using mobilization and Kinesio tape techniques were carried out for these patients in the dialysis ward of Shahid Beheshti Hospital of Babol by a physiotherapist.
Inclusion criteria included positiveness of at least one of the shoulder’s tests (Hawkins, Neer, and painful arch), dialysis for more than six months, pain of shoulder joint for more than two months, and shoulder pain in anterior and anterior-lateral area [5, 15, 24-26]. Exclusion criteria included neck pain consequent of radiculopathy, trauma, and shoulder fracture in the last six months, shoulder and breast surgery, cervical rib, pregnancy, cancer, sensitive skin to Kinesio tape, history of physiotherapy or corticosteroid injection in the last three months, rheumatoid arthritis (RA) disease, and the use of nonsteroidal anti-inflammatory drugs [27-32]. After receiving an explanation of the research methodology, the subjects provided written consent. Demographic information about the subjects, including their sex, age, body mass index (BMI), duration of dialysis initiation, number of dialysis sessions per week, and onset duration of pain, was collected through patient files, questionnaires, and interviews.
Using Stata software, version 24 the sample size of this study was specified, following the approach outlined in Kaya et al.’s study [33]. Moreover, based on the study by Joyce et al. [34], the minimal clinically important difference (MCID) was set at 1.37 for the visual analog scale (VAS) and 2 for the standard deviation (SD). Assuming a significance level (α) of 0.05 and a power of 80%, a sample size of 20 individuals was calculated for each group. The patients were randomly divided into two groups: Mobilization alone (20 patients) and mobilization with Kinesio taping (20 patients). Randomization was achieved using a block size of 4 and a block number of ten.
Outcome measures
Primary outcome measures included
A) The intensity of shoulder pain at rest was measured by a numerical pain rating scale [35]. B) Pain intensity during active shoulder abduction movement, for measuring which the numerical pain scale was employed [35].
Secondary outcome measures included
A) Active abduction ROM of the shoulder was assessed using a goniometer [36, 37]. To measure the degree of active shoulder abduction, the patient was supine and the shoulder was placed in external rotation. The support of the goniometer axis was placed on the anterior edge of the acromion, the fixed arm was placed parallel to the longitudinal axis of the sternum, and the movable arm was placed parallel to the longitudinal axis of the humors [38]. B) The degree of shoulder functional disability was assessed by the disabilities of the arm, shoulder, and hand (DASH) questionnaire [39].
The DASH questionnaire contains 30 questions about the symptoms and function of the upper limb involved in orthopedic and neurological disorders [40]. Each question has five parts providing a range of scores from 1–5. A higher score indicates greater symptoms so that if there is no symptom, it is considered as one, and if there is the most disability and symptoms, it is considered five [40]. In the DASH scale, a higher score indicates a greater level of disability and severity, whereas, lower scores indicate a lower level of disability. The score on this test ranges from 0 (no disability) to 100 (most severe disability) [40]. The obtained score is minus 30 and divided by the maximum score minus the minimum score [40].
Intervention
First group
This group, referred to as the mobilization-alone group, consisted of dialysis patients with SAIS who received mobilization grades I and II. This mobilization involved caudal, anterior, and posterior movements of the glenohumeral joint [41]. Passive oscillatory movements were performed at the rate of 2-3 glides per second for 30 seconds and each glide was given for five sets, which was totally applied for about 4 to 5 minutes. Finally, 12-15 minutes of mobilization was performed in each session. This method was used three times a week for four weeks (12 sessions) 17 (Figures 2 and 3).
Second group
In addition to mobilization, Kinesio tape was applied to the deltoid and supraspinatus muscles in this group. Mobilization and the new Kinesio tape intervention were alternated every 12 sessions (every other day). The Kinesio tape used in this study was the BioBalance brand, manufactured in Korea.
Kinesio tape application method
Supraspinatus muscle Kinesio tape
The beginning of the Kinesio tape is placed from the humorous tubercle without tension, then the shoulder is placed in horizontal adduction and the hand is in pronation, and the Kinesio tape is placed on the top and bottom of the scapula spine with 10-15% tension and the two ends of the Y of the Kinesio tape without tension on the transverse process of T2 and T4 was attached at the end [21].
To apply the Kinesio tape of the deltoid muscle
The Kinesio tape was first placed on the deltoid tubercle without tension and followed the two ends of the Y-strip Kinesio tape of the anterior and posterior deltoid muscles. The anterior deltoid muscle of the shoulder should be in the extension position and the posterior deltoid muscle of the shoulder should be in the flexion position. The Kinesio tape was applied with 10-15% tension on the muscle belly, and then, the end of the Kinesio tape was attached without tension on the front and back of the big tubercle [21] (Figure 4).
Evaluation of primary and secondary outcomes was done in three phases: Before treatment, after treatment (after 12 sessions), and in the follow-up phase (ten days after treatment. SPSS software, version 18 was used for data analysis. Before analyzing the main variables, we used the Kolmogorov-Smirnov test to assess the normal distribution of the variables, but the normality of the data distribution was not confirmed [42]. Therefore, the nonparametric Friedman test was used for intragroup comparisons [42]. The Wilcoxon’s test was applied to compare different time points in the same group [44]. The Mann-Whitney test was applied to compare the mean values between the two groups at different time points [42].
Results
Forty dialysis patients with SAIS were divided into two groups: Mobilization alone and mobilization with Kinesio taping, participating in our study. No significant differences were observed between the two groups in terms of demographic variables, duration of dialysis, dialysis sessions per week, and the duration of pain onset. Thus, the matching of the groups was confirmed (Table 1).
Using the Friedman test in both groups, the results revealed a decrease in pain intensity at rest and during active shoulder abduction, an increase in the ROM of shoulder active abduction, and a decrease in shoulder functional disability (P<0.001). The effect size of the treatment was strong in both groups using Kendall value [42] (Table 2).
Using the Wilcoxon test for pairwise comparison of pre-treatment with post-treatment times, pre-treatment with follow-up exhibited a significant difference in all parameters in both groups (P≤0.05). Nevertheless, the comparison results between post-treatment and follow-up revealed a significant difference between all parameters except shoulder pain at rest time in both groups and pain during active shoulder abduction in the mobilization and Kinesio taping group (P≥0.05) (Table 2). The Mann-Whitney test showed no significant difference between the two groups after treatment and in the follow-up (P≥0.05). The rank-biserial correlation (r) value showed that the effect size between the two groups in all parameters after treatment was stronger than in the follow-up (Table 2).
Discussion
This study aimed to compare the effects of mobilization with Kinesio taping and mobilization alone on pain intensity, ROM, and shoulder functional disability in dialysis patients with SAIS. The results showed after 12 intervention sessions, both mobilization alone and mobilization with Kinesio taping reduced pain intensity at rest and during active shoulder abduction, increased the ROM of shoulder active abduction, and decreased shoulder functional disability in dialysis patients with SAIS and this effect lasted for up to ten days after the end of treatment.
Mobilization may control pain by activating mechanoreceptors and inhibiting nociceptors, thereby modulating the pain gate and reducing the individual’s perception of pain [43]. Also, manual therapy declines swelling and pain in SAIS by improving synovial fluid movement and abnormal collagen traction. In the present study, mobilization grades I and II in the glenohumeral joint were used, which may have enhanced the subacromial area by reducing pain and inflammation while improving blood flow. Following mobilization, there was an increase in active shoulder abduction ROM and a decrease in the degree of shoulder functional disability [44].
In the current study, adding Kinesio tape to mobilization was not able to improve the mobilization’s therapeutic effect. It is possible that in dialysis patients with SAIS, who experience an imbalance between the rotator cuff and deltoid muscles, along with the upward force exerted on the glenohumeral joint by the deltoid muscle, the subacromial area becomes reduced. In this study, the Kinesio tape was used to inhibit the rotator cuff muscles with tendonitis and suppress the deltoid muscle. Park et al. reported Kinesio tape’s effects on reducing pain, inflammation, and correct movement improvement [7]. Nevertheless, in the present study, Kinesio tape was employed on most patients with SAIS and fistula hand. Dialysis patients are usually advised not to use their fistula hand, and due to their sedentary lifestyle and musculoskeletal problems, they may not be able to accurately report the effect of Kinesio tape on their upper limb function.
Furthermore, it is possible that due to the compromised muscle function in dialysis patients resulting from the pathophysiology of hemodialysis, the inhibition of the deltoid and supraspinatus muscles by Kinesio tape is not as effective in reducing pain, increasing ROM, and decreasing the degree of shoulder functional disability as it might be in non-dialysis patients.
Previous studies have assessed the effects of Kinesio tape and mobilization on non-dialysis patients with SAIS. As far as we know, this is the first study to investigate the effects of Kinesio tape on SAIS in dialysis patients.
Our results were in line with those of Senbursa et al. and Maricar et al. and Kachingwe et al. These studies reported that mobilization associated with exercise was effective in reducing pain intensity and shoulder functional disability as well as increasing shoulder ROM in non-dialysis patients with SAIS. Although the present study only performed mobilization as a treatment, its effects were similar to the results of other studies [45-47]. In this regard, Park et al. examined the effects of mobilization with Kinesio taping on SAIS in five non-dialysis patients and showed reduced pain intensity and increased ROM, as well as decreased rotator cuff muscle tone and stiffness. In this study, by reducing the fascia layers, Kinesio tape reduced muscle tone, thus reducing pain and increasing ROM [7]. Furthermore, Thelen et al. reported that after the application of Kinesio tape in non-dialysis SAIS, the pain intensity during movement immediately declined in the Kinesio tape-treated group compared to the placebo group, while a Kinesio tape effect alone was not observed in our study. This discrepancy may be attributed to the fact that Thelen’s study had a sample of younger non-dialysis patients compared to our study, and they lacked a control group [22].
Our study results were different from those of Shakeri et al. who reported a greater of Kinesio tape compared to Kinesio tape placebo using the DASH questionnaire in non-dialysis patients with SAIS. Perhaps the higher effectiveness of Kinesio tape in their study was due to the three-day interval between Kinesio tape sessions. However, in the present study, a one-day interval between Kinesio tape sessions may have stimulated changes in the subacromial area structure. Additionally, differences in the type of Kinesio tape, the expertise in applying and securing the Kinesio tape, and the Kinesio tape application method (50% tension for deltoid muscle and lower trapezius in the above study, compared to 10-15% tension for deltoid muscle and supraspinatus in our study) could account for variations in results [48].
Among the research that has so far investigated the effects of mobilization and Kinesio taping as well as mobilization alone on patients with SAIS, our study is the first one to examine the effects of these two treatment methods on dialysis patients with SAIS, and the sample size in the above study has been with 80% power.
Among the limitations of our study, we can mention the lack of patient examination by means of MRI, CT SCAN, x-ray, and ultrasound because of the difficult mobility of patients besides the small number of samples for normalization and short-term treatment follow-up (10 days).
It is suggested to apply mobilization in a different time period than the above-mentioned study (4-5 minutes), examine patients based on the type of tissue involved and the severity of pain, and apply mobilization in other directions of the shoulder and other Kinesio tape techniques of SAIS using larger sample sizes and longer follow-up with the help of exercise therapy and physiotherapy modalities to treat these patients. Using MRI, ultrasound, etc. as objective evaluation indicators is also recommended.
Conclusion
Both mobilization alone and mobilization combined with Kinesio taping were effective in declining the pain intensity at rest during active shoulder abduction, increasing the ROM of shoulder active abduction, and decreasing the degree of shoulder functional disability. Due to the absence of a significant difference between the two methods in our study, it can be concluded that adding Kinesio tape to mobilization compared to mobilization alone had no additional impacts on pain at rest and during active shoulder abduction, increasing active shoulder abduction ROM, and reducing shoulder functional disability in dialysis subjects with SAIS.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Babol University of Medical Sciences (Code: IRMUBABOL.REC.1399297). It was also registered at the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20091274002851N5).
Funding
This study was financially supported by the Babol University of Medical Sciences (Code: 9910528).
Authors' contributions
Conceptualization and supervision: Mohammad Taghipour; Methodology: Mohammad Taghipour and Mona Ramezani; Data collection: Mona Ramezani; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patients for participation in this research and also the staff of Shahid Beheshti Hospital and the Babol University of Medical Sciences.
References
- Kooijman M, Swinkels I, Dijk Cv, Bakker Dd, Veenhof C:Patients with shoulder syndromes in general and physiotherapy practice: An observational study. BMC Musculoskeletal Disorders. 2013; 14(1):1-7. [DOI:10.1186/1471-2474-14-128] [PMID] [PMCID]
- Ostör AJ, Richards CA, Prevost AT, Speed CA, Hazleman BL. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology. 2005; 44(6):800-5. [DOI:10.1093/rheumatology/keh598] [PMID]
- Van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: Incidence, patient characteristics, and management. Annals of the Rheumatic Diseases. 1995; 54(12):959-64. [DOI:10.1136/ard.54.12.959] [PMID] [PMCID]
- Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clinical Biomechanics. 2003; 18(5):369-79. [DOI:10.1016/S0268-0033(03)00047-0] [PMID]
- Neer CS. Impingement lesions. Clinical Orthopaedics and Related Research. 1983; 173:70-7. [DOI:10.1097/00003086-198303000-00010]
- Hedtmann A. [Weichteilerkrankungen der schulter-subakromialsyndrome (German)]. Orthopädie und Unfallchirurgie up2date. 2009; 4(02):85-106. [DOI:10.1055/s-0029-1214456]
- Park SE, Kim YR, San Wang J. Immediate effects of maitland joint mobilization with kinematic taping on shoulder pain, ROM, and muscle tone in subacromial impingement syndrome. Journal of International Academy of Physical Therapy Research. 2017; 8(3):1206-10. [DOI:10.20540/JIAPTR.2017.8.3.1206]
- Soyupek F, Demir M, Süslü FE, Baykal B, Sezer MT, Yesildag A. The upper extremity musculoskeletal complications in dialysis patients: Comparison between hemodialysis and peritoneal dialysis. Journal of Back and Musculoskeletal Rehabilitation. 2013; 26(3):267-371. [DOI:10.3233/BMR-130375] [PMID]
- Bardin T. Musculoskeletal manifestations of chronic renal failure. Current Opinion in Rheumatology. 2003; 15(1):48-54. [DOI:10.1097/00002281-200301000-00009] [PMID]
- Goodman TR, McNally E. Shoulder pain in a patient on haemodialysis. Annals of the Rheumatic Diseases. 1994; 53(8):497-500. [DOI:10.1136/ard.53.8.497] [PMID] [PMCID]
- Bardin T, Zingraff J, Shirahama T, Noel LH, Droz D, Voisin MC, et al. Hemodialysis-associated amyloidosis and beta-2 microglobulin. Clinical and immunohistochemical study. The American Journal of Medicine. 1987; 83(3):419-24. [DOI:10.1016/0002-9343(87)90750-9] [PMID]
- Kessler M, Netter P, Azoulay E, Mayeux D, Pere P, Gaucher A. Dialysis-associated arthropathy: A multicentre survey of 171 patients receiving haemodialysis for over 10 years. The co-operative group on dialysis-associated arthropathy. British Journal of Rheumatology. 1992; 31(3):157-62. [DOI:10.1093/rheumatology/31.3.157] [PMID]
- Sargent MA, Fleming SJ, Chattopadhyay C, Ackrill P, Sambrook P. Bone cysts and haemodialysis-related amyloidosis. Clinical Radiology. 1989; 40(3):277-81. [DOI:10.1016/S0009-9260(89)80201-6] [PMID]
- Pianta TF. The role of physical therapy in improving physical functioning of renal patients. Advances in Renal Replacement Therapy. 1999; 6(2):149-58. [DOI:10.1016/S1073-4449(99)70033-6] [PMID]
- Kumar A, Kumar S, Aggarwal A, Kumar R, Das PG. Effectiveness of maitland techniques in idiopathic shoulder adhesive capsulitis. International Scholarly Research Network. 2012; 2012:1-8. [DOI:10.5402/2012/710235]
- Biswas AK, Sur BN, Gupta CR. Treatment of periarthritis shoulder. Journal of the Indian Medical Association. 1979; 72(12):276-7. [PMID]
- Maitland GD. Maitlands prtipheral manipulation. Oxford: Elsevier Butterworth-Heinemann; 2008. [Link]
- Asouzu NC, Ibeneme SC, Arodiwe EB, Abdu A, Osegbe ID, et al. Responses of urea, creatinine and uric acid to soft tissue and passive mobilization in patients with renal diseases undergoing haemodialysis. Journal of Nephrology & Therapeutics. 2019; 9(326):2. [DOI:10.37421/jnt.2019.9.326]
- Smith MC, Stallings MA, Mariner S, Burrall M. Benefits of massage therapy for hospitalized patients: A descriptive and qualitative evaluation. Alternative Therapies in Health and Medicine. 1999; 5(4):64. [Link]
- Panjabi MM, White AA. Biomechanics in the musculoskeletal system. London: Churchill Livingstone; 2008. [Link]
- Kase K, Wallis J, Kase T. Clinical therapeutic applications of the kinesio taping methods. Bethesda: Kinesio Taping Assoc; 2003. [Link]
- Thelen MD, Dauber JA, Stoneman PD. The clinical efficacy of kinesio tape for shoulder pain: A randomized, double-blinded, clinical trial. The Journal of orthopaedic and Sports Physical Therapy. 2008; 38(7):389-95. [DOI:10.2519/jospt.2008.2791] [PMID]
- Kaya E, Zinnuroglu M, Tugcu I. Kinesio taping compared to physical therapy modalities for the treatment of shoulder impingement syndrome. Clinical Rheumatology. 2011; 30(2):201-7. [DOI:10.1007/s10067-010-1475-6] [PMID]
- Capitanini A, Galligani C, Lange S, Cupisti A. Upper limb disability in hemodialysis patients: Evaluation of contributing factors aside from amyloidosis. Therapeutic Apheresis and Dialysis. 2012; 16(3):242-7. [DOI:10.1111/j.1744-9987.2011.01056.x] [PMID]
- Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. The American Journal of Sports Medicine. 1980; 8(3):151-8. [DOI:10.1177/036354658000800302] [PMID]
- Kessel L, Watson M. The painful arc syndrome. Clinical classification as a guide to management. The Journal of Bone and Joint Surgery. British Volume. 1977; 59(2):166-72. [DOI:10.1302/0301-620X.59B2.873977] [PMID]
- Turk AC, Fıdan N, Ozcan O, Ozdemır F, Tomak L, Ozkurt S, et al. Painful and painless shoulder magnetic resonance imaging comparisons in hemodialysis patients and correlation with clinical findings. Journal of Back and Musculoskeletal Rehabilitation. 2016; 30(1):63-9. [DOI:10.3233/BMR-160715] [PMID]
- Guru K, Anilkumar VA, Pandian J. Effect of gleno-humeral mobilisation and mobilisation of asymptomatic cervical spine in patients with shoulder impingement syndrome: A pilot trial. Saudi Journal for Health Sciences. 2015; 4(1):42-50. [DOI:10.4103/2278-0521.151408]
- Kocyigit F, Acar M, Turkmen MB, Kose T, Guldane N, Kuyucu E. Kinesio taping or just taping in shoulder subacromial impingement syndrome? A randomized, double-blind, placebo-controlled trial. Physiotherapy Theory and Practice. 2016; 32(7):501-8. [DOI:10.1080/09593985.2016.1219434] [PMID]
- Göksu H, Tuncay F, Borman P. The comparative efficacy of kinesio taping and local injection therapy in patients with subacromial impingement syndrome. Acta Orthopaedica et Traumatologica Turcica. 2016; 50(5):483-8. [DOI:10.1016/j.aott.2016.08.015] [PMID]
- Kul A, Ugur M. Comparison of the efficacy of conventional physical therapy modalities and kinesio taping treatments in shoulder impingement syndrome. The Eurasian Journal of Medicine. 2019; 51(2):139-44. [DOI:10.5152/eurasianjmed.2018.17421] [PMID] [PMCID]
- Abdelomnem SM, Egila SE, Fawzy RM, Mohamed MA, Abdelkader NA. Assessment of tendon involvement in chronic hemodialysis patients: An ultrasonographic study. Egyptian Rheumatology and Rehabilitation. 2019; 46(3):154-61. [DOI:10.4103/err.err_60_18]
- Kaya DO, Baltaci G, Toprak U, Atay AO. The clinical and sonographic effects of kinesiotaping and exercise in comparison with manual therapy and exercise for patients with subacromial impingement syndrome: A preliminary trial. Journal of Manipulative and Physiological Therapeutics. 2014; 37(6):422-32. [DOI:10.1016/j.jmpt.2014.03.004] [PMID]
- Joyce CR, Zutshi DW, Hrubes V, Mason RM. Comparison of fixed interval and visual analogue scales for rating chronic pain. European Journal of Clinical Pharmacology. 1975; 8(6):415-20. [DOI:10.1007/BF00562315] [PMID]
- Freyd M. The graphic rating scale. Journal of educational psychology. 1923; 14(2):83. [DOI:10.1037/h0074329]
- Couper MP, Tourangeau R, Conrad FG, Singer E. Evaluating the effectiveness of visual analog scales: A web experiment. Social Science Computer Review. 2006; 24(2):227-45. [DOI:10.1177/0894439305281503]
- Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain. The Cochrane Database of Systematic Reviews. 2003; 2003(2):CD004258 [DOI:10.1002/14651858.CD004258] [PMID] [PMCID]
- Fruth P. Fundamentals of the physical therapy examination. Burlington: Jones & Bartlett Learning; 2018. [Link]
- Mohseni Bandpei MA, Keshavarz R, Minoonejad H, Ebrahimi Varkiani M, Samadi H, Latifi S. [Shoulder pain and functional disability in Iranian premier league volleyball players (Persian)]. Journal of Mazandaran University of Medical Sciences. 2012; 22(90):95-103. [Link]
- Mahmoudi Hashemi F, Mousavi SJ, Attarbashi Moghaddam B, Talebian S, Mousavi S. [Cross cultural adaptation, Validity and Reliability study of the Persian version of the American shoulder and elbow surgeons (ASES) questionnaire for evaluation of shoulder function in injured athletes(Persian)]. Journal of Modern Rehabilitation. 2013; 7(1):34-9. [Link]
- Maitland GD. Treatment of the glenohumeral joint by passive movement. Physiotherapy. 1983; 69(1):3-7. [Link]
- Cohen J. Statistical power analysis for the behavior sciences. Milton Park: Taylor & Francis; 2013. [Link]
- Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. The Journal of Orthopaedic and Sports Physical Therapy. 2000; 30(3):126-37. [DOI:10.2519/jospt.2000.30.3.126] [PMID]
- Conroy DE, Hayes KW. The effect of joint mobilization as a component of comprehensive treatment for primary shoulder impingement syndrome. The Journal of Orthopaedic and Sports Physical Therapy. 1998; 28(1):3-14. [DOI:10.2519/jospt.1998.28.1.3] [PMID]
- Senbursa G, Baltaci G, Atay A. Comparison of conservative treatment with and without manual physical therapy for patients with shoulder impingement syndrome: A prospective, randomized clinical trial. Knee surgery, Sports Traumatology, Arthroscopy. 2007; 15(7):915-21. [DOI:10.1007/s00167-007-0288-x] [PMID]
- Maricar N, Shacklady C, McLoughlin L. Effect of maitland mobilization and exercises for the treatment of shoulder adhesive capsulitis: A single-case design. Physiotherapy Theory and Practice. 2009; 25(3):203-17. [DOI:10.1080/09593980902776654] [PMID]
- Kachingwe AF, Phillips B, Sletten E, Plunkett SW. Comparison of manual therapy techniques with therapeutic exercise in the treatment of shoulder impingement: A randomized controlled pilot clinical trial. The Journal of Manual & Manipulative Therapy. 2008; 16(4):238-47. [DOI:10.1179/106698108790818314] [PMID] [PMCID]
- Shakeri H, Keshavarz R, Arab AM, Ebrahimi I. Clinical effectiveness of kinesiological taping on pain and pain-free shoulder range of motion in patients with shoulder impingement syndrome: A randomized, double blinded, placebo-controlled trial. International Journal of Sports Physical Therapy. 2013; 8(6):800-10. [PMID] [PMCID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2022/12/23 | Accepted: 2023/09/2 | Published: 2024/03/1
Received: 2022/12/23 | Accepted: 2023/09/2 | Published: 2024/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
