
988368
Wed, Jul 29, 2026

Volume 22, Issue 2 (June 2024)
Iranian Rehabilitation Journal 2024, 22(2): 167-174 |
Back to browse issues page



Ethics code: IEC 169/2019
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Korada H, Gundmi Maiya A, Kumar Rao S, Hande M, Shetty S, Anumasa R. Influence of Photobiomodulation Therapy on Altered Plantar Pressure Distribution and Ankle Biomechanics in Individuals With Diabetic Foot Syndrome. Iranian Rehabilitation Journal 2024; 22 (2) :167-174
URL: http://irj.uswr.ac.ir/article-1-1868-en.html
URL: http://irj.uswr.ac.ir/article-1-1868-en.html
Hrishikesh Korada *1 

 , Arun Gundmi Maiya2 , Sharath Kumar Rao3 , Manjunath Hande4 , Sahana Shetty5 , Ranjith Anumasa6
, Arun Gundmi Maiya2 , Sharath Kumar Rao3 , Manjunath Hande4 , Sahana Shetty5 , Ranjith Anumasa6
, Arun Gundmi Maiya2 , Sharath Kumar Rao3 , Manjunath Hande4 , Sahana Shetty5 , Ranjith Anumasa6
1- Footryx Healthcare Private Limited, CfHE, Indian Institute of Technology Hyderabad, Hyderabad, India.
2- Department of Physiotherapy, Manipal College of Health Professions, Manipal Academy of Higher Education, Manipal, India.
3- Department of Orthopedics, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
4- Department of Medicine, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
5- Department of Endocrinology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
6- Department of Physiotherapy, Yashoda College of Physiotherapy, Hyderabad, India.
2- Department of Physiotherapy, Manipal College of Health Professions, Manipal Academy of Higher Education, Manipal, India.
3- Department of Orthopedics, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
4- Department of Medicine, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
5- Department of Endocrinology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
6- Department of Physiotherapy, Yashoda College of Physiotherapy, Hyderabad, India.
Keywords: Low-level laser therapy, Plantar pressure distribution, Foot biomechanics, Bio-stimulation, Peripheral neuropathy
Full-Text [PDF 1016 kb]
(1132 Downloads)
| Abstract (HTML) (3691 Views)
Full-Text: (890 Views)
Introduction
he triad of neurological, vascular, and biomechanical impairments associated with the development of type 2 diabetes mellitus is known as diabetic foot syndrome (DFS) [1, 2]. It is commonly associated with functional impairment of limbs and poor quality of life. Reduced sensations, pain, muscle weakness, spasms, loss of balance, and proprioception are the main symptoms often presented due to damage or injury to the vasa nervorum, axons, and atrophy of the axons [3]. The prevalence of DFS is approximately 24.6% to 49% in India [4, 5].
Altered sensory and motor nerve functions in diabetic peripheral neuropathy (DPN) can affect altered biomechanics in ankle kinematics, gait kinetics and plantar pressure distribution [6]. Plantar pressures are the pressure field that acts between the foot and the support surface during everyday locomotor activities. The literature indicates that elevated plantar pressures and aberrant lower limb biomechanics, which may contribute to the development of diabetic foot ulceration, have a strong association with DPN [7].
The use of non-invasive medical treatments has reported symptomatic relief of DPN. Among the conventional electrotherapy modalities, because photobiomodulation therapy (PBMT) can generate a biostimulation effect on the nervous system’s cells, it has been used to treat nerve injuries and other disorders connected to nerves [8]. Since PBMT stimulates nerve regeneration to enhance neural function and vascularity, it has been utilized to treat peripheral nerve damage and other diabetes problems at different wavelengths [9].
Even though PBMT is effective in reducing pain, improving nerve physiology and conduction, and regeneration, there is a dearth of literature on the influence of PBMT on plantar pressure parameters and ankle biomechanics in diabetic foot individuals in the Indian scenario. Accordingly, this study assesses how plantar pressure distribution and ankle biomechanics in DFS are affected by PBMT.
Materials and Methods
A total of 97 participants were screened and 20 DFS subjects were recruited based on the inclusion and exclusion criteria. A comprehensive diabetic foot evaluation was performed which included history, sensory, motor, biomechanics, neuropathy components were evaluated. DPN was assessed as per International Diabetes Federation (IDF) 2021 guidelines. The inclusion criteria were 1) Inability to feel or perceive monofilament 10 g at least one out of 6 sites at the plantar surface of feet; 2) Using a biothesiometer, unable to perceive the vibration perception test <20 V at plantar surface region; and 3) Absence of ankle reflexes using a reflex hammer. Exclusion criteria were neuropathies other than diabetes origin. Any orthopedic, vision-related issues, central nervous system, or other disability that may affect gait and posture. Resting limb pain, peripheral vascular disease, current pain, injury, severe ulceration, ulcer history, or toe amputation [9].
Following a detailed baseline comprehensive diabetic foot evaluation, all subjects were irradiated with two separate low-level Laser therapy equipment. The scanning mode laser wavelength of 632.8 nm with a dosage of 3.1 J/cm2 (Tech Laser SS-1000, Technomed, India, 2018), and the probe laser, a wavelength of 660 nm and 850 nm with a dosage of 3.4 J/cm2 and power density of 50-150 mW/cm2 (Thor Laser LX2.3, Thor Photomedicine LTD, UK). The scanning mode with a duration of 9-min covering the entire plantar and dorsum region of the foot and the Thor laser probe was used with the contact method over the popliteal fossa for 5 min for a total of 10 sessions (Figure 1). All subjects were reassessed with detailed diabetic foot evaluation at the end of the 10 sessions. Plantar pressure parameters were measured on the WinTrack pressure plate (Medicapteurs France SAS, Balma, France). Average plantar pressure (APP), maximum plantar pressure (MPP), the forefoot-hind foot ratio (FHR) and total contact area (TCA) measurements were taken, and the data were analyzed with WinTrack software, version 12 (Medicapteurs France SAS, Balma, France). For gait analysis, the 3D SIMI motion analysis system, version 2018 measured ankle biomechanics parameters, like angular velocity and acceleration. Initially, three trials were conducted for participants to walk at an average pace on the pressure plate platform. The data were analyzed using the SPSS software, version 21. To investigate the group’s pre-test and post-test changes, descriptive statistics and paired t-tests were used with the significance level set at P<0.05.

Results
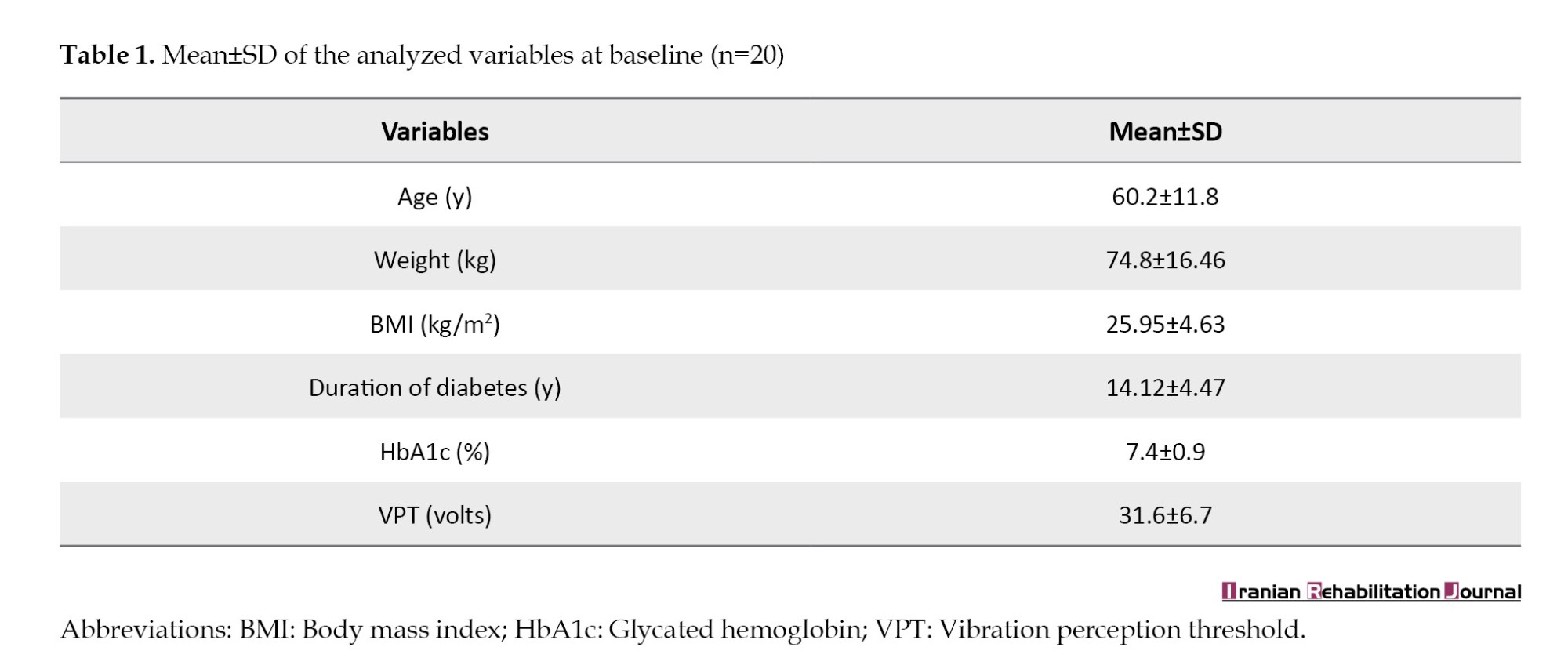
A total of 20 subjects participated in this study. The demographic characteristics of the subjects are provided in Table 1. The mean age was 60.2±11.8 years in addition to the history of type 2 diabetes mellitus with a mean duration of 14.12±4.47 years and a mean body mass index of 25.9±4.6 kg/m2.
Pre-test and post-test study means values of the plantar pressure parameters in the intervention group
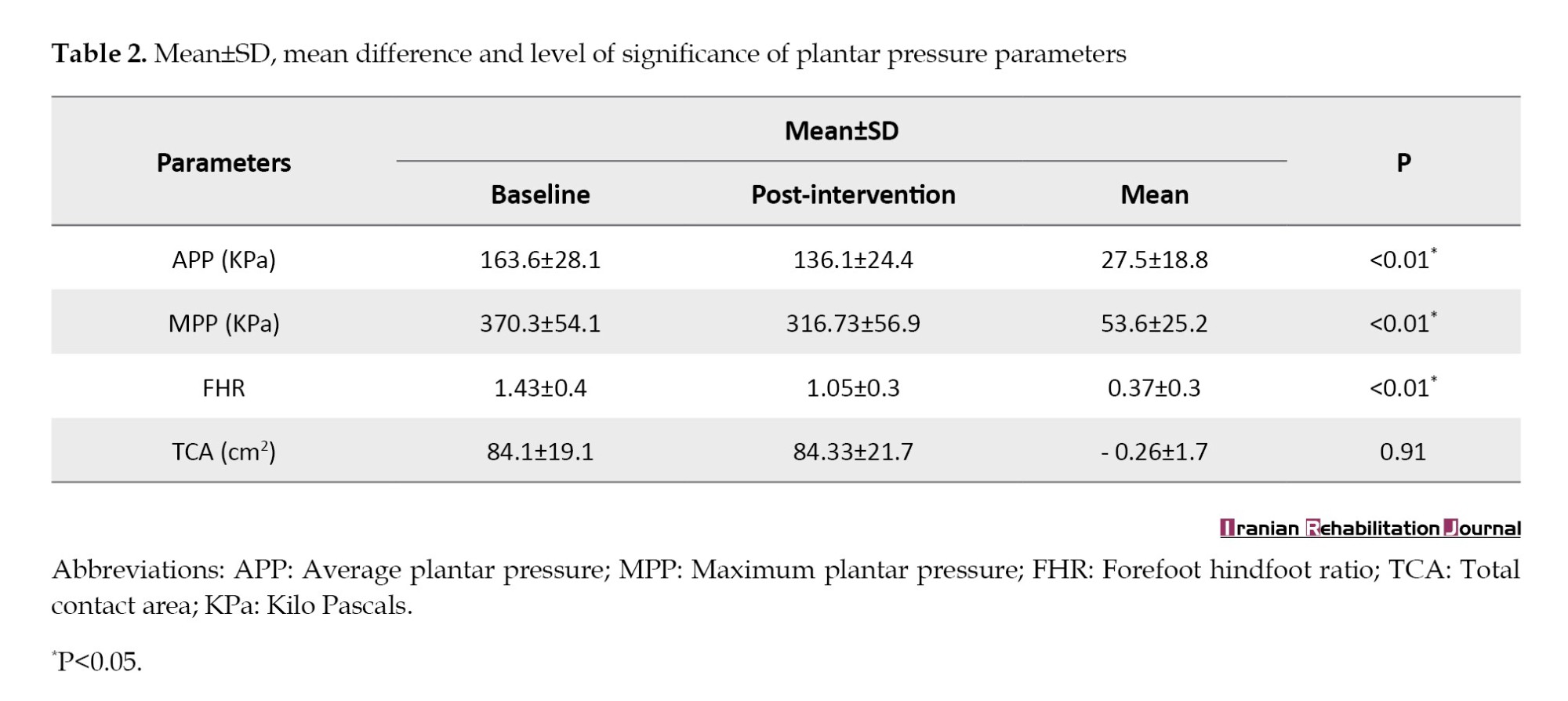
According to Table 2, the Mean±SD for APP at baseline were 163.6±28.1 and at the tenth session was 136.1±24.4 with a mean change of 27.5±18.8 (t=3.39, P<0.01). Meanwhile, MPP at baseline was 370.3±54.1 and at the tenth session was 316.73±56.9, with a mean change of a mean change of 53.6±25.2 (t=8.22, P<0.01). FHR at the baseline was 1.43±0.4 and at the tenth session was 1.05±0.3, with a mean change of 0.37±0.3, (t=4.35, P<0.01). And, the TCA at baseline was 84.1±19.1 and at the end of the tenth session was 84.33±21.7, with a mean change of 0.26±1.7 (t=0.08, P=0.91).
Pre-test and post-test study means values of the ankle biomechanics in the intervention group
According to Table 3, the Mean±SD for the parameters of ankle biomechanics, peak angular velocity at heel strike phase baseline was 43.2±8.9 and at the tenth session was 65.2±5.3, with a mean change of 22.1±11.2 (t=-3.5, P<0.01). At the midstance phase, the value was 33.9±7.7 and at the tenth session, it was 33.7±7.8 with a mean change of 0.16±8.1 (t=-2.1, P=0.98). In addition, at the toe-off phase, the value was 219.8±25.9 and at the tenth session was 254.3±32.8, with the mean change of 34.4±26.7 (t=-6.7, P<0.01).
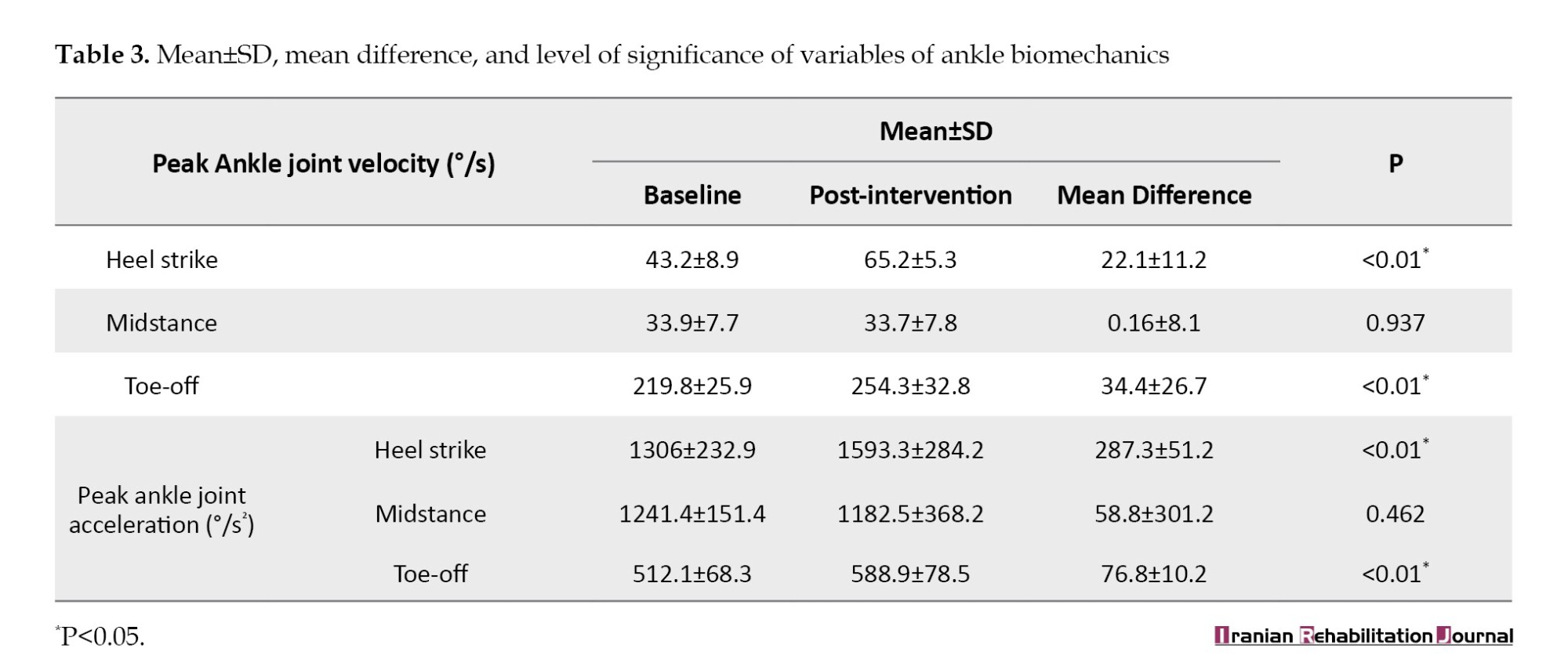
In peak angular acceleration at the heel strike phase, the baseline was 1306±232.9 and at the tenth session was 1593.3±284.2 with a mean change of 76.8±10.2 (t=-6.7, P<0.01). In addition, at the midstance phase, the value was 1241.4±151.4 and at the tenth session, it was 1182.5±368.2, with a mean change of 58.8±301.2 (t=-2.05, P=0.46). The toe-off phase was 512.1±68.3 and at the tenth session was 588.9±78.5 with a mean change of 76.8±10.2 (t=-4.7, P<0.01).
Discussion
Plantar pressure distribution and ankle biomechanics are drastically altered in individuals with DFS due to sensory and motor nerve deficits. These modifications may be critical risk factors for developing a diabetic foot ulcer in the future [10]. The loss of protective sensation, abnormal muscle activity, and plantar tissue stiffness due to diabetic neuropathy can be a potential variable associated with DFS that can impact reduced ankle biomechanics compared with healthy individuals [11].
The purpose of this research was to determine the effect of PBMT among individuals with DFS. Dynamic pressure foot scanning was used to determine APP, MPP, FHR and TCA. Foot plantar pressure scanning is dependable, precise, and simple to replicate [12]. Ankle biomechanics parameters were measured using 3D motion gait analysis, and various variables, like peak ankle angular velocity and peak angular acceleration at heel strike, midstance, and toe-off of stance phase were evaluated [13].
Accordingly, at the post-intervention comparison, plantar pressure parameters and ankle biomechanics were significantly improved compared to baseline after the PBMT. This may be due to increased electrophysiological changes in peripheral nerves, especially the peroneal nerve. No difference was seen in the TCA and midstance kinematics. Regarding the influence of PBMT on plantar pressure parameters, the study found that APP decreased by about 16.5%, MPP decreased by about 14.3% and FHR reduced by about 25.8% compared to the baseline.
An evaluation of plantar pressures in offloading or pressure redistribution treatment is helpful because it provides a perspective on the pressure reduction level required to heal and prevent foot ulcers [14]. Increased FHR is a high predictor of ulcers in DFS. In the average population, FHR is less than one; that is, the hind foot takes higher loading than the forefoot during gait [15]. In DFS, due to loss of protective sensation and muscle function alteration, there is an increase in forwarding translation of loading, thus increasing FHR by more than one [16]. As per the literature, both forefoot and rearfoot MPP is increased, the FHR ratio was significantly higher in severe neuropathy, and an FHR ratio greater than one can predict ulcer development in the foot region [17].
Another study observed significant variations in joint angle, joint velocity, and acceleration during the heel strike, midstance, and toe-off phases of gait walking in people with DPN compared to people without DPN [7]. Recent advances in motion analysis technology, such as improved multi-segment foot models, 2D/3D movement analysis, or motion detection system studies that support connections between peripheral neuropathy and a decline in gait excursions of the ankle complex and sub-segments of the foot are emerging [18, 19]. Also, ankle angular velocity at heel strike and toe-off was increased by about 51.1% and 15.7%, and ankle angular acceleration at heel strike and toe-off was increased by about 21.9% and 14.9%, respectively.
Increased motor and sensory nerve conduction velocity and voluntary muscle activity recruitment were found after applying PBMT transcutaneously. Increased sensation of the plantar region may increase the sense of awareness of the foot, thus reducing plantar pressure distribution. The possible mechanism explained is: a) Increased nerve metabolism, b) Prevents motor cell degeneration, c) Stimulates Schwann cell proliferation, d) Facilitates and increases myelination, and e) Regeneration of axons [20].
Other possible cellular mechanisms for tissue regeneration by PBMT involve the following items: 1) Elevated calcium in the cell cytoplasm; 2) Accelerated division of cells and development; 3) Interactions with cytochromes resulting in cell stimulation; 4) Protein and cytokine formation and activation; 5) Adenosine triphosphate production; and 6) Vasodilation and skin microcirculation in the blood [21, 22]. An improvement in plantar pressure parameters following PBMT can be comprehended as improving the peripheral neural function of both the sensory and motor nerves in the lower limb resulting in a significant reduction in pain level [23]. All of these implications can be clinically and operationally indicated during walking to reset plantar pressure parameters and improve ankle kinematics [24].
DFS is usually a typical scenario that starts as injury or damage to peripheral nerves. The research findings highlight that PBMT’s bio-stimulation effect improves the nervous system [25]. This study used the total dosage of 3.1 J/cm2 and 3.4 J/cm2. It has been documented that the sensory nerve and motor nerve velocity and latency in subjects with carpal tunnel syndrome with an intensity of 2.7 to 3.6 J/cm2 have increased significantly [26].
Conclusion
PBMT can effectively reduce foot plantar pressures and improve ankle biomechanics in individuals with diabetic foot syndrome. This therapy should be implemented in routine foot care management as preventive therapy that can reduce the risk of development of foot ulcers in type 2 diabetes mellitus patients.
Study limitations
This study had limitations due to a small number of participants and a short treatment period, with no control or placebo to compare the results for better interpretation. Further studies with a significant number of participants using distinctive laser wavelengths and the same application method are required.
Ethical Considerations
Compliance with ethical guidelines
This research approved by Kasturba Medical College and Hospitals Institutional of Manipal Academy of Higher Education (MAHE) Ethics Committee (Code: IEC-169/2019). Each participant provided informed written consent.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Centre for Diabetic Foot Care and Research (CDFCR), Department of Physiotherapy, Manipal College of Health Professions (MCHP), Manipal Academy of Higher Education (MAHE), Manipal, India.
References
he triad of neurological, vascular, and biomechanical impairments associated with the development of type 2 diabetes mellitus is known as diabetic foot syndrome (DFS) [1, 2]. It is commonly associated with functional impairment of limbs and poor quality of life. Reduced sensations, pain, muscle weakness, spasms, loss of balance, and proprioception are the main symptoms often presented due to damage or injury to the vasa nervorum, axons, and atrophy of the axons [3]. The prevalence of DFS is approximately 24.6% to 49% in India [4, 5].
Altered sensory and motor nerve functions in diabetic peripheral neuropathy (DPN) can affect altered biomechanics in ankle kinematics, gait kinetics and plantar pressure distribution [6]. Plantar pressures are the pressure field that acts between the foot and the support surface during everyday locomotor activities. The literature indicates that elevated plantar pressures and aberrant lower limb biomechanics, which may contribute to the development of diabetic foot ulceration, have a strong association with DPN [7].
The use of non-invasive medical treatments has reported symptomatic relief of DPN. Among the conventional electrotherapy modalities, because photobiomodulation therapy (PBMT) can generate a biostimulation effect on the nervous system’s cells, it has been used to treat nerve injuries and other disorders connected to nerves [8]. Since PBMT stimulates nerve regeneration to enhance neural function and vascularity, it has been utilized to treat peripheral nerve damage and other diabetes problems at different wavelengths [9].
Even though PBMT is effective in reducing pain, improving nerve physiology and conduction, and regeneration, there is a dearth of literature on the influence of PBMT on plantar pressure parameters and ankle biomechanics in diabetic foot individuals in the Indian scenario. Accordingly, this study assesses how plantar pressure distribution and ankle biomechanics in DFS are affected by PBMT.
Materials and Methods
A total of 97 participants were screened and 20 DFS subjects were recruited based on the inclusion and exclusion criteria. A comprehensive diabetic foot evaluation was performed which included history, sensory, motor, biomechanics, neuropathy components were evaluated. DPN was assessed as per International Diabetes Federation (IDF) 2021 guidelines. The inclusion criteria were 1) Inability to feel or perceive monofilament 10 g at least one out of 6 sites at the plantar surface of feet; 2) Using a biothesiometer, unable to perceive the vibration perception test <20 V at plantar surface region; and 3) Absence of ankle reflexes using a reflex hammer. Exclusion criteria were neuropathies other than diabetes origin. Any orthopedic, vision-related issues, central nervous system, or other disability that may affect gait and posture. Resting limb pain, peripheral vascular disease, current pain, injury, severe ulceration, ulcer history, or toe amputation [9].
Following a detailed baseline comprehensive diabetic foot evaluation, all subjects were irradiated with two separate low-level Laser therapy equipment. The scanning mode laser wavelength of 632.8 nm with a dosage of 3.1 J/cm2 (Tech Laser SS-1000, Technomed, India, 2018), and the probe laser, a wavelength of 660 nm and 850 nm with a dosage of 3.4 J/cm2 and power density of 50-150 mW/cm2 (Thor Laser LX2.3, Thor Photomedicine LTD, UK). The scanning mode with a duration of 9-min covering the entire plantar and dorsum region of the foot and the Thor laser probe was used with the contact method over the popliteal fossa for 5 min for a total of 10 sessions (Figure 1). All subjects were reassessed with detailed diabetic foot evaluation at the end of the 10 sessions. Plantar pressure parameters were measured on the WinTrack pressure plate (Medicapteurs France SAS, Balma, France). Average plantar pressure (APP), maximum plantar pressure (MPP), the forefoot-hind foot ratio (FHR) and total contact area (TCA) measurements were taken, and the data were analyzed with WinTrack software, version 12 (Medicapteurs France SAS, Balma, France). For gait analysis, the 3D SIMI motion analysis system, version 2018 measured ankle biomechanics parameters, like angular velocity and acceleration. Initially, three trials were conducted for participants to walk at an average pace on the pressure plate platform. The data were analyzed using the SPSS software, version 21. To investigate the group’s pre-test and post-test changes, descriptive statistics and paired t-tests were used with the significance level set at P<0.05.
Results
A total of 20 subjects participated in this study. The demographic characteristics of the subjects are provided in Table 1. The mean age was 60.2±11.8 years in addition to the history of type 2 diabetes mellitus with a mean duration of 14.12±4.47 years and a mean body mass index of 25.9±4.6 kg/m2.
Pre-test and post-test study means values of the plantar pressure parameters in the intervention group
According to Table 2, the Mean±SD for APP at baseline were 163.6±28.1 and at the tenth session was 136.1±24.4 with a mean change of 27.5±18.8 (t=3.39, P<0.01). Meanwhile, MPP at baseline was 370.3±54.1 and at the tenth session was 316.73±56.9, with a mean change of a mean change of 53.6±25.2 (t=8.22, P<0.01). FHR at the baseline was 1.43±0.4 and at the tenth session was 1.05±0.3, with a mean change of 0.37±0.3, (t=4.35, P<0.01). And, the TCA at baseline was 84.1±19.1 and at the end of the tenth session was 84.33±21.7, with a mean change of 0.26±1.7 (t=0.08, P=0.91).
Pre-test and post-test study means values of the ankle biomechanics in the intervention group
According to Table 3, the Mean±SD for the parameters of ankle biomechanics, peak angular velocity at heel strike phase baseline was 43.2±8.9 and at the tenth session was 65.2±5.3, with a mean change of 22.1±11.2 (t=-3.5, P<0.01). At the midstance phase, the value was 33.9±7.7 and at the tenth session, it was 33.7±7.8 with a mean change of 0.16±8.1 (t=-2.1, P=0.98). In addition, at the toe-off phase, the value was 219.8±25.9 and at the tenth session was 254.3±32.8, with the mean change of 34.4±26.7 (t=-6.7, P<0.01).
In peak angular acceleration at the heel strike phase, the baseline was 1306±232.9 and at the tenth session was 1593.3±284.2 with a mean change of 76.8±10.2 (t=-6.7, P<0.01). In addition, at the midstance phase, the value was 1241.4±151.4 and at the tenth session, it was 1182.5±368.2, with a mean change of 58.8±301.2 (t=-2.05, P=0.46). The toe-off phase was 512.1±68.3 and at the tenth session was 588.9±78.5 with a mean change of 76.8±10.2 (t=-4.7, P<0.01).
Discussion
Plantar pressure distribution and ankle biomechanics are drastically altered in individuals with DFS due to sensory and motor nerve deficits. These modifications may be critical risk factors for developing a diabetic foot ulcer in the future [10]. The loss of protective sensation, abnormal muscle activity, and plantar tissue stiffness due to diabetic neuropathy can be a potential variable associated with DFS that can impact reduced ankle biomechanics compared with healthy individuals [11].
The purpose of this research was to determine the effect of PBMT among individuals with DFS. Dynamic pressure foot scanning was used to determine APP, MPP, FHR and TCA. Foot plantar pressure scanning is dependable, precise, and simple to replicate [12]. Ankle biomechanics parameters were measured using 3D motion gait analysis, and various variables, like peak ankle angular velocity and peak angular acceleration at heel strike, midstance, and toe-off of stance phase were evaluated [13].
Accordingly, at the post-intervention comparison, plantar pressure parameters and ankle biomechanics were significantly improved compared to baseline after the PBMT. This may be due to increased electrophysiological changes in peripheral nerves, especially the peroneal nerve. No difference was seen in the TCA and midstance kinematics. Regarding the influence of PBMT on plantar pressure parameters, the study found that APP decreased by about 16.5%, MPP decreased by about 14.3% and FHR reduced by about 25.8% compared to the baseline.
An evaluation of plantar pressures in offloading or pressure redistribution treatment is helpful because it provides a perspective on the pressure reduction level required to heal and prevent foot ulcers [14]. Increased FHR is a high predictor of ulcers in DFS. In the average population, FHR is less than one; that is, the hind foot takes higher loading than the forefoot during gait [15]. In DFS, due to loss of protective sensation and muscle function alteration, there is an increase in forwarding translation of loading, thus increasing FHR by more than one [16]. As per the literature, both forefoot and rearfoot MPP is increased, the FHR ratio was significantly higher in severe neuropathy, and an FHR ratio greater than one can predict ulcer development in the foot region [17].
Another study observed significant variations in joint angle, joint velocity, and acceleration during the heel strike, midstance, and toe-off phases of gait walking in people with DPN compared to people without DPN [7]. Recent advances in motion analysis technology, such as improved multi-segment foot models, 2D/3D movement analysis, or motion detection system studies that support connections between peripheral neuropathy and a decline in gait excursions of the ankle complex and sub-segments of the foot are emerging [18, 19]. Also, ankle angular velocity at heel strike and toe-off was increased by about 51.1% and 15.7%, and ankle angular acceleration at heel strike and toe-off was increased by about 21.9% and 14.9%, respectively.
Increased motor and sensory nerve conduction velocity and voluntary muscle activity recruitment were found after applying PBMT transcutaneously. Increased sensation of the plantar region may increase the sense of awareness of the foot, thus reducing plantar pressure distribution. The possible mechanism explained is: a) Increased nerve metabolism, b) Prevents motor cell degeneration, c) Stimulates Schwann cell proliferation, d) Facilitates and increases myelination, and e) Regeneration of axons [20].
Other possible cellular mechanisms for tissue regeneration by PBMT involve the following items: 1) Elevated calcium in the cell cytoplasm; 2) Accelerated division of cells and development; 3) Interactions with cytochromes resulting in cell stimulation; 4) Protein and cytokine formation and activation; 5) Adenosine triphosphate production; and 6) Vasodilation and skin microcirculation in the blood [21, 22]. An improvement in plantar pressure parameters following PBMT can be comprehended as improving the peripheral neural function of both the sensory and motor nerves in the lower limb resulting in a significant reduction in pain level [23]. All of these implications can be clinically and operationally indicated during walking to reset plantar pressure parameters and improve ankle kinematics [24].
DFS is usually a typical scenario that starts as injury or damage to peripheral nerves. The research findings highlight that PBMT’s bio-stimulation effect improves the nervous system [25]. This study used the total dosage of 3.1 J/cm2 and 3.4 J/cm2. It has been documented that the sensory nerve and motor nerve velocity and latency in subjects with carpal tunnel syndrome with an intensity of 2.7 to 3.6 J/cm2 have increased significantly [26].
Conclusion
PBMT can effectively reduce foot plantar pressures and improve ankle biomechanics in individuals with diabetic foot syndrome. This therapy should be implemented in routine foot care management as preventive therapy that can reduce the risk of development of foot ulcers in type 2 diabetes mellitus patients.
Study limitations
This study had limitations due to a small number of participants and a short treatment period, with no control or placebo to compare the results for better interpretation. Further studies with a significant number of participants using distinctive laser wavelengths and the same application method are required.
Ethical Considerations
Compliance with ethical guidelines
This research approved by Kasturba Medical College and Hospitals Institutional of Manipal Academy of Higher Education (MAHE) Ethics Committee (Code: IEC-169/2019). Each participant provided informed written consent.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Centre for Diabetic Foot Care and Research (CDFCR), Department of Physiotherapy, Manipal College of Health Professions (MCHP), Manipal Academy of Higher Education (MAHE), Manipal, India.
References
- Korada H, Maiya A, Rao SK, Hande M. Effectiveness of customized insoles on maximum plantar pressure in diabetic foot syndrome: A systematic review. Diabetes & metabolic syndrome. 2020; 14(5):1093-9. [DOI:10.1016/j.dsx.2020.06.041] [PMID]
- Volmer-Thole M, Lobmann R. Neuropathy and diabetic foot syndrome. International Journal of Molecular Sciences. 2016; 17(6):917. [DOI:10.3390/ijms17060917] [PMID] [PMCID]
- Yamany AA, Bitesha K. Effect of 850 nm He-Ne laser therapy on nerve conduction and foot planter pressures distribution of painful diabetic neuropathy: A randomized controlled trial. Journal of Novel Physiotherapies. 2016; 6(4):1000300. [DOI:10.4172/2165-7025.1000300]
- Vibha SP, Kulkarni MM, Kirthinath Ballala AB, Kamath A, Maiya GA. Community based study to assess the prevalence of diabetic foot syndrome and associated risk factors among people with diabetes mellitus. BMc Endocrine Disorders. 2018; 18(1):43. [DOI:10.1186/s12902-018-0270-2] [PMID] [PMCID]
- Maiya AG, Gundmi S, Matpady P, Jadhav R, Lingadakai R, Hande M, et al. Prevalence of foot complications in people with type 2 diabetes mellitus: A community-based survey in rural Udupi. The international Journal of Lower Extremity Wounds. 2018; 17(3):169-75. [DOI:10.1177/1534734618791853] [PMID]
- Kumar S, Maiya A, Hande M, Rajagopal KV, Vidyasagar S, Rao K, Hazari A. Plantar pressure distribution in type 2 diabetes mellitus without peripheral neuropathy. The Diabetic Foot Journal Middle East. 2015; 1(2):19-21. [Link]
- Hazari A, Maiya AG, Shivashankara KN. Foot kinetic and kinematic profile in type 2 diabetes mellitus with peripheral neuropathy a hospital-based study from south India. Journal of the American Podiatric Medical Association. 2019; 109(1):36-49. [DOI:10.7547/17-059] [PMID]
- Anju M, Ummer VS, Maiya AG, Hande M. Low level laser therapy for the patients with painful diabetic peripheral neuropathy-A systematic review. Diabetes & Metabolic Syndrome. 2019g; 13(4):2667-70. [DOI:10.1016/j.dsx.2019.07.035] [PMID]
- Mohamed RA, Abdallah GA, Abdeen HA, Nassif AA. Influence of low level laser therapy versus pulsed electromagnetic field on diabetic peripheral neuropathy. Physical Therapy and Rehabilitation. 2017; 4(1):17. [DOI:10.7243/2055-2386-4-17]
- Fernando ME, Crowther RG, Lazzarini PA, Sangla KS, Wearing S, Buttner P, et al. Plantar pressures are higher in cases with diabetic foot ulcers compared to controls despite a longer stance phase duration. BMC Endocrine Disorders. 2016; 16(1):51. [DOI:10.1186/s12902-016-0131-9] [PMID] [PMCID]
- Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Research and Clinical Practice. 2022; 183:109119. [DOI:10.1016/j.diabres.2021.109119] [PMID] [PMCID]
- Chatwin KE, Abbott CA, Boulton AJM, Bowling FL, Reeves ND. The role of foot pressure measurement in the prediction and prevention of diabetic foot ulceration-A comprehensive review. Diabetes/Metabolism Research and Reviews. 2020; 36(4):e3258. [DOI:10.1002/dmrr.3258] [PMID] [PMCID]
- Hazari A, Maiya AG, Shivashankara KN, Monteiro MSA, Kumar CGS, Rao K, et al. 3D Biomechanical analysis of foot in diabetes with and without peripheral neuropathy-a pilot study. Research Journal of Pharmaceutical Biological and Chemical Sciences. 2016; 7(3):558-64. [Link]
- Asad A, Hameed MA, Khan UA, Butt MU, Ahmed N, Nadeem A. Comparison of nerve conduction studies with diabetic neuropathy symptom score and diabetic neuropathy examination score in type-2 diabetics for detection of sensorimotor polyneuropathy. The Journal of the Pakistan Medical Association. 2009; 59(9):594-8. [PMID]
- Veves A, Murray HJ, Young MJ, Boulton AJ. The risk of foot ulceration in diabetic patients with high foot pressure: A prospective study. Diabetologia. 1992; 35(7):660-3. [DOI:10.1007/BF00400259] [PMID]
- Amemiya A, Noguchi H, Oe M, Takehara K, Yamada A, Ohashi Y, et al. Relationship between elevated plantar pressure of toes and forefoot and gait features in diabetic patients. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. 2013; 2013:4633-6. [DOI:10.1109/EMBC.2013.6610580] [PMID]
- Caselli A, Pham H, Giurini JM, Armstrong DG, Veves A. The forefoot-to-rearfoot plantar pressure ratio is increased in severe diabetic neuropathy and can predict foot ulceration. Diabetes Care. 2002; 25(6):1066-71. [DOI:10.2337/diacare.25.6.1066] [PMID]
- Raspovic A. Gait characteristics of people with diabetes-related peripheral neuropathy, with and without a history of ulceration. Gait & Posture. 2013; 38(4):723-8. [DOI:10.1016/j.gaitpost.2013.03.009] [PMID]
- Sawacha Z, Gabriella G, Cristoferi G, Guiotto A, Avogaro A, Cobelli C. Diabetic gait and posture abnormalities: A biomechanical investigation through three dimensional gait analysis. Clinical Biomechanics. 2009; 24(9):722-8. [DOI:10.1016/j.clinbiomech.2009.07.007] [PMID]
- Barbosa RI, Marcolino AM, de Jesus Guirro RR, Mazzer N, Barbieri CH, de Cássia Registro Fonseca M. Comparative effects of wavelengths of low-power laser in regeneration of sciatic nerve in rats following crushing lesion. Lasers in Medical Science. 2010; 25(3):423-30. [DOI:10.1007/s10103-009-0750-8] [PMID]
- Klebanov GI, Kreinina MV, Poltanov EA, Khristoforova TV, Vladimirov YA. Mechanism of therapeutic effect of low-intensity infrared laser radiation. Bulletin of Experimental Biology and Medicine. 2001; 131(3):239-41. [DOI:10.1023/A:1017643230376] [PMID]
- Carmeliet P. Blood vessels and nerves: Common signals, pathways and diseases. Nature Reviews. Genetics. 2003; 4(9):710-20. [DOI:10.1038/nrg1158] [PMID]
- Bagis S, Comelekoglu U, Sahin G, Buyukakilli B, Erdogan C, Kanik A. Acute electrophysiologic effect of pulsed gallium-arsenide low energy laser irradiation on configuration of compound nerve action potential and nerve excitability. Lasers in Surgery and Medicine. 2002; 30(5):376-80. [DOI:10.1002/lsm.10057] [PMID]
- Yadav Korada H, Maiya GA, Kumar Rao S, Hande M. Photobiomodulation with customized insoles on maximum plantar pressure in diabetic foot syndrome by the biomechanical model: A case report. Iranian Rehabilitation Journal. 2021; 19(1):111-6. [DOI:10.32598/irj.19.1.1165.1]
- Yamany AA, Sayed HM. Effect of low level laser therapy on neurovascular function of diabetic peripheral neuropathy. Journal of Advanced Research. 2012; 3(1):21-8. [DOI:10.1016/j.jare.2011.02.009]
- Lazovic M, Ilic-Stojanovic O, Kocic M, Zivkovic V, Hrkovic M, Radosavljevic N. Placebo-controlled investigation of low-level laser therapy to treat carpal tunnel syndrome. Photomedicine and Laser Surgery. 2014; 32(6):336-44. [DOI:10.1089/pho.2013.3563] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2023/01/19 | Accepted: 2023/11/25 | Published: 2024/06/1
Received: 2023/01/19 | Accepted: 2023/11/25 | Published: 2024/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
