
988368
Fri, Jul 31, 2026

Volume 22, Issue 2 (June 2024)
Iranian Rehabilitation Journal 2024, 22(2): 277-284 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zehra A, Ahmer Z, Qadri U, Ovais M. Depression, Anxiety and Stress in Formal and Informal Caregivers of Autistic Children in Karachi. Iranian Rehabilitation Journal 2024; 22 (2) :277-284
URL: http://irj.uswr.ac.ir/article-1-1892-en.html
URL: http://irj.uswr.ac.ir/article-1-1892-en.html



1- Sindh Institute of Physical Medicine and Rehabilitation, Civil Hospital Karachi, Dow University of Health Sciences, Karachi, Pakistan.
2- APPNA Institute of Public Health, Jinnah Sindh Medical University, Karachi, Pakistan.
3- Department of Medicine, Sindh Government Hospital, Liaquatabad, Pakistan.
2- APPNA Institute of Public Health, Jinnah Sindh Medical University, Karachi, Pakistan.
3- Department of Medicine, Sindh Government Hospital, Liaquatabad, Pakistan.
Keywords: Autism spectrum disorder, Informal caregiver, Formal caregiver, Depression, Anxiety, Stress
Full-Text [PDF 597 kb]
(1136 Downloads)
| Abstract (HTML) (3233 Views)
Full-Text: (829 Views)
Introduction
Autism spectrum disorder (ASD) is characterized by impaired social behavior, communication, and language, a lack of interests. and repetitive activities that are unique to the individual [1]. The average age for the symptoms of autism to appear is before the age of 3 years [2]. About 1 out of 100 children are suffering from ASD [3]. The worldwide prevalence of autism is 1-2 per 1000 children and according to the Centre for Disease Control, 9 out of 1000 children have been diagnosed with autism in the United States [4]. Autism is associated with a high incidence of stress, anxiety, and depression in its caregivers. A study conducted on a sample of 220 caregivers of ASD in Oman in 2016 reported 45.9% and 48.6% of anxiety and stress, respectively [5]. A study in Thailand in 2010 showed the prevalence of depression at 25.6% [6].
Children with ASD may have various symptoms, such as hyperactivity, self-injurious behavior, cognitive impairment, or the presence of repetitive movements [7, 8]. These lead to an array of factors, including social criticism, affected interpersonal relationships, uncontrolled behaviors, and reduced care which can then affect the quality of life [4, 5, 9]. It is also reported that psychological distress is higher among caregivers of ASD, especially mothers, who are informal caregivers. They are more prone to depression, stress, and anxiety as compared to mothers of children with mild intellectual disability and normal developmental children [4, 5, 10]. Families with special needs face everyday challenges, and experience more psychological burdens that include somatic complaints, heart pain, breathing difficulties, stress, financial burden, and reduced interpersonal relationships [5, 11].
Behavior problems of autistic children are the most common cause of high parental stress, anxiety, and depression; however, the relation between behavior problems and these three issues receives little attention in the population. Formal caregivers who include trained professionals who care for children with ASD are largely ignored when reporting caregiver burden. According to our knowledge, no studies have been focused on formal caregivers of ASD in Pakistan.
This study helps to identify the gravity of the issue in both formal and informal caregivers so that support and non-pharmacological intervention can be provided to the caregivers. This will eventually help the sufferers of autism. Therefore, this study evaluates depression, stress, and anxiety among formal and informal caregivers of ASD.
Materials and Methods
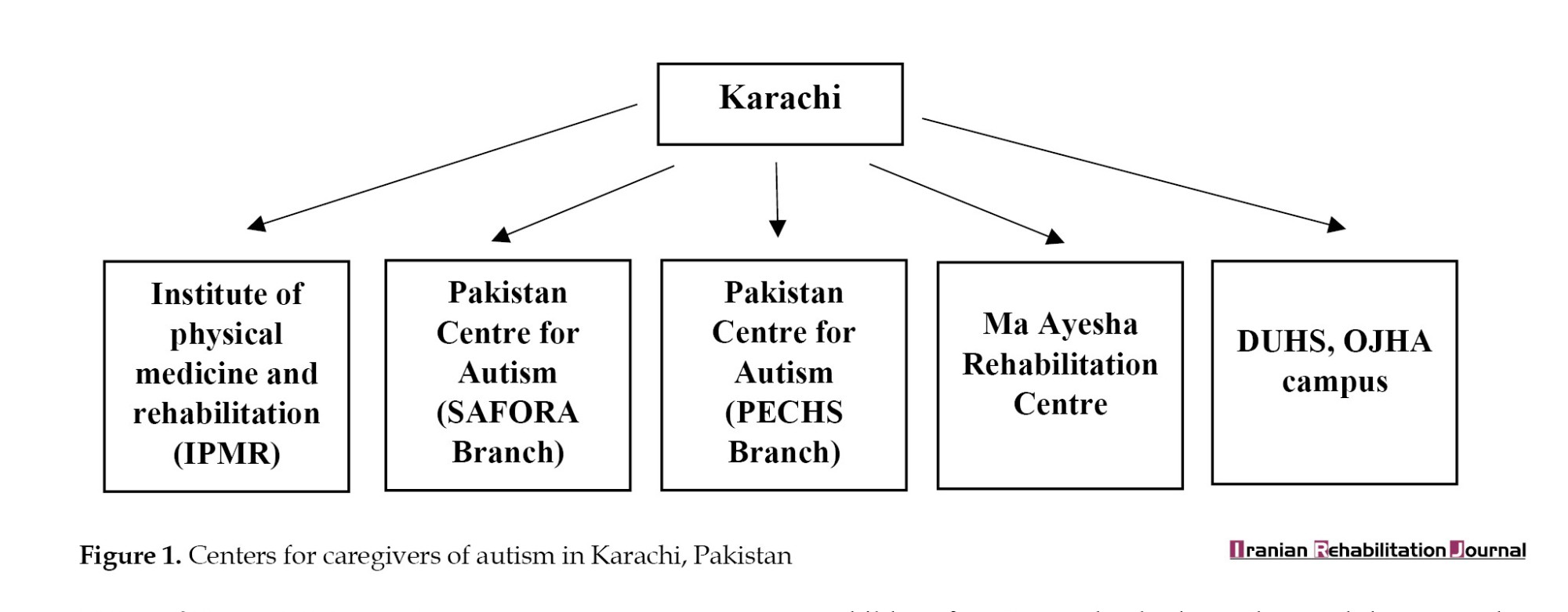
This was a cross-sectional study conducted among the formal and informal caregivers of autistic children in the following centers in Karachi (Figure 1).
The duration of the study was 6-8 months, but due to the COVID-19 pandemic and the sudden complete lockdown of the city in 2020, the data collection process was delayed. Due to precautionary measures, it took around 2 years to complete the data collection procedure.
The sample size was calculated using the open access online sample size calculator (Open Epi calculator), by using a previous study in Australia with the prevalence of depression at 21%, anxiety at 17.1% and stress at 13.3% among caregivers of autistic children. The estimated sample size calculated for the prevalence of depression was 255, for anxiety 218, and stress 178 subjects. Accordingly, the highest prevalence of depression was taken as the anticipated frequency at the confidence level of 95%, and bound on the error of 5%, the sample size was obtained at 255 [12]. There were 255 participants out of which 111 were formal caregivers working with autism in specified centers of Karachi City, Pakistan, and 144 were informal caregivers. There were mostly females (mothers) because most fathers were not available in the therapy center and they did not have the time to complete the questionnaire due to their tough job.
Since a sampling frame was not available, the convenience sampling method was used to recruit the participants. Study participants who were available at the time of data collection and willing to be part of the survey were invited to the study. Formal caregivers were operationalized as trained professionals who spent 30 min to 1 h of their time with the autistic child and were paid for their services [13]. In this context, formal caregivers included employees working in the institute with ASD children for >3 months, both genders and the ones who gave informed written consent. The informal caregivers were operationalized as parents with one or more autistic children who gave informed written consent. Caregivers who were tending to children with any physical disabilities or those who had any history of psychological disorder or a history of drug addiction, and who did not provide consent to participate were excluded from this study.
The data collection tool was the depression anxiety stress scale 42 (DASS-42) developed by Lovibond (1995) [14]. Before the use of scale, permission was taken from the author through email. The DASS-42 is a set of three self-report scales designed to measure the negative emotional states of depression, anxiety, and stress. The test-retest reliability of the three scales was considered adequate with a Cronbach α of 0.71 for depression, 0.79 for anxiety, and 0.81 for stress. The participants were asked to use 4-point severity/frequency scales to rate the extent to which they have experienced each state. Scores for depression, anxiety and stress were calculated by summing the scores for the relevant items.
Each of the three DASS-42 scales contains 14 items, which are divided into subscales of 2-5 items with similar content. The scale was comprised of normal, mild moderate, severe, and highly severe with scores ranging from 0 to 32. The higher the scores for each domain reflected greater levels of depression, anxiety, and stress. A semi-structured questionnaire was also used to gather information on socio-demographic characteristics, including age, gender, occupation, socioeconomic status, education, financial issues faced, family system, working hours and job satisfaction along with DASS-42.
The participants were invited directly from the selected institutes for quantitative assessment. Subjects who fulfilled the criteria of the study and provided their consent were approached. The data were entered with caution to avoid any missing values.
Statistical analysis
All the data was entered and analyzed using the SPSS software, version 22. Percentages were reported for all the categorical variables, including gender, occupation, and education. Since we hypothesized that DASS-42 is more common among informal caregivers as compared to formal caregivers we applied the Fisher exact test to determine the relationship between the frequency of depression anxiety and stress among both the groups. The statistical significance was set at 0.05.
Results
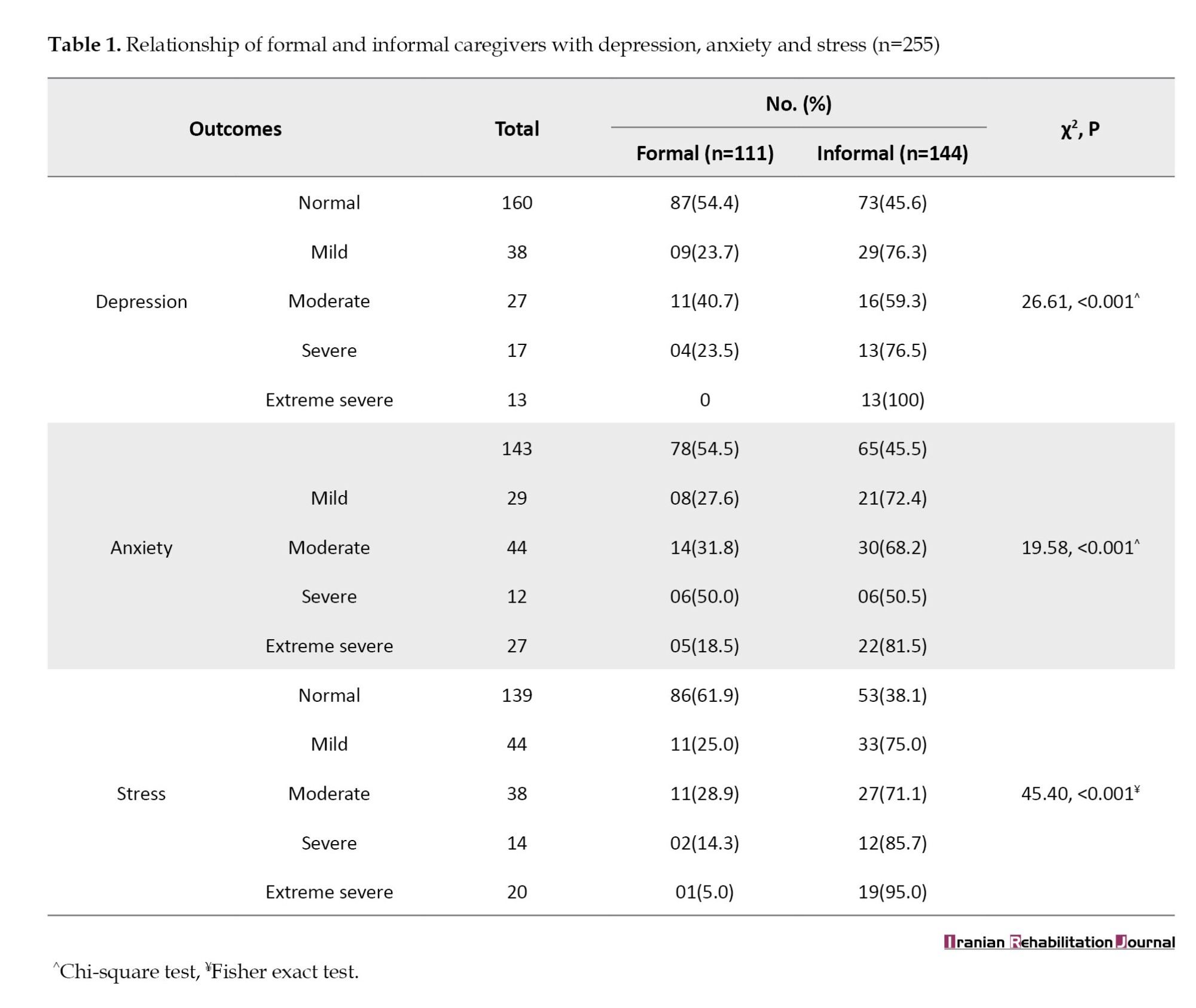
The relationship of formal and informal caregivers with depression, anxiety, and stress is shown in Table 1. Accordingly, 76.3% of informal caregivers were suffering from mild depression, 59.3% were moderately depressed, and 76.5 % were severely depressed (P<0.01, χ2=26.61). Similarly, 72.4% had mild anxiety, 68.2% were moderately anxious and 50.5% were severely anxious (P<0.01, χ2 =19.58). Also, 75.0% had mild stress, 71.1% had moderate stress, 85.7% had severe stress, and 95.0% had extremely severe stress (P<0.01, χ2=45.4).
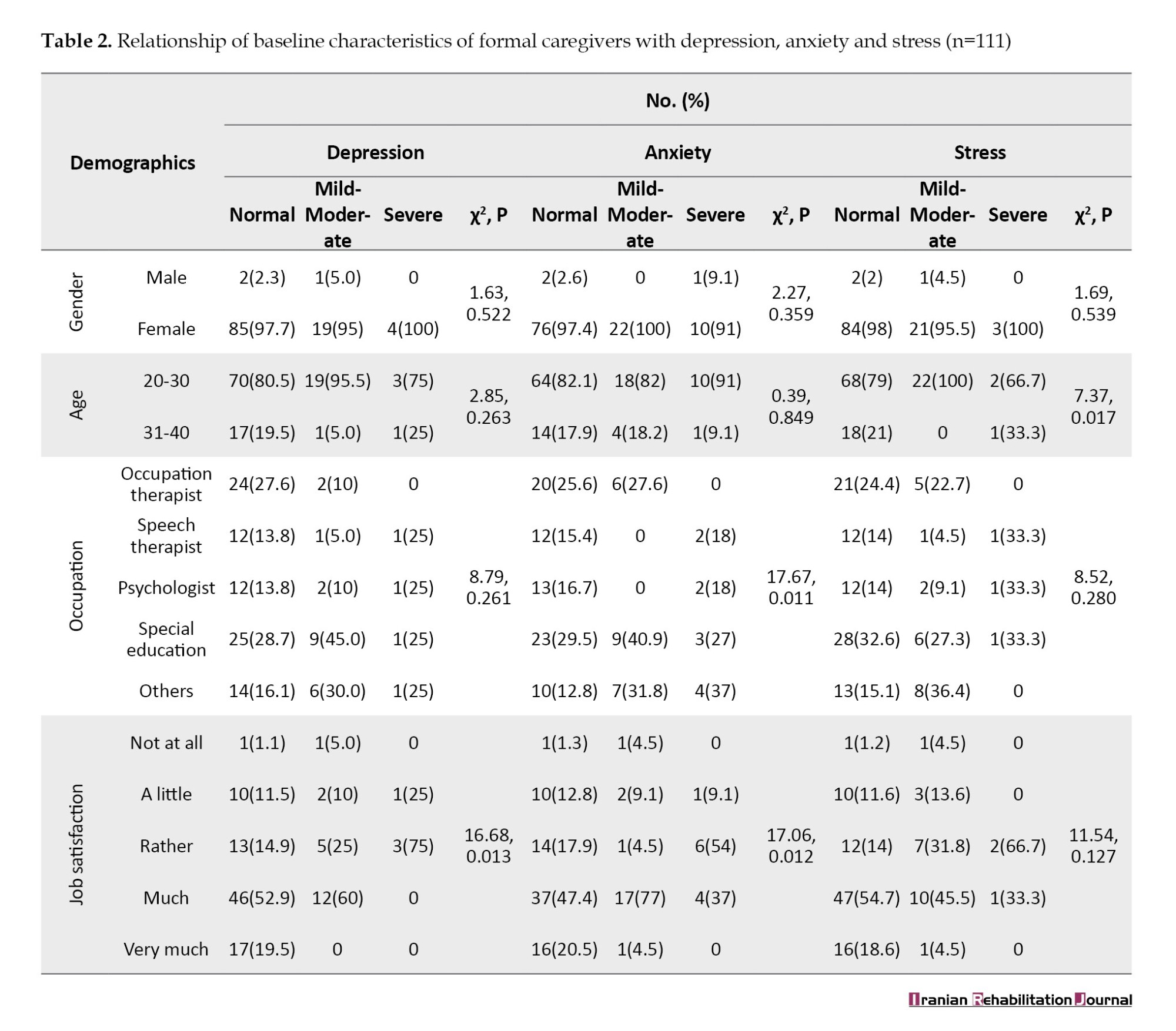
Formal caregivers who were aged between 20-30 years showed more stress (P=0.017, χ2=7.37). In terms of occupation, the special educators showed a significant anxiety score (P=0.011, χ2=17.67) (Table 2). Meanwhile, satisfaction with the job was the main factor that was also associated with depression and anxiety in formal caregivers. Some of the participants were significantly depressed (P=0.013, χ2=16.68) and had significant anxiety scores (P=0.012, χ2=17.06).
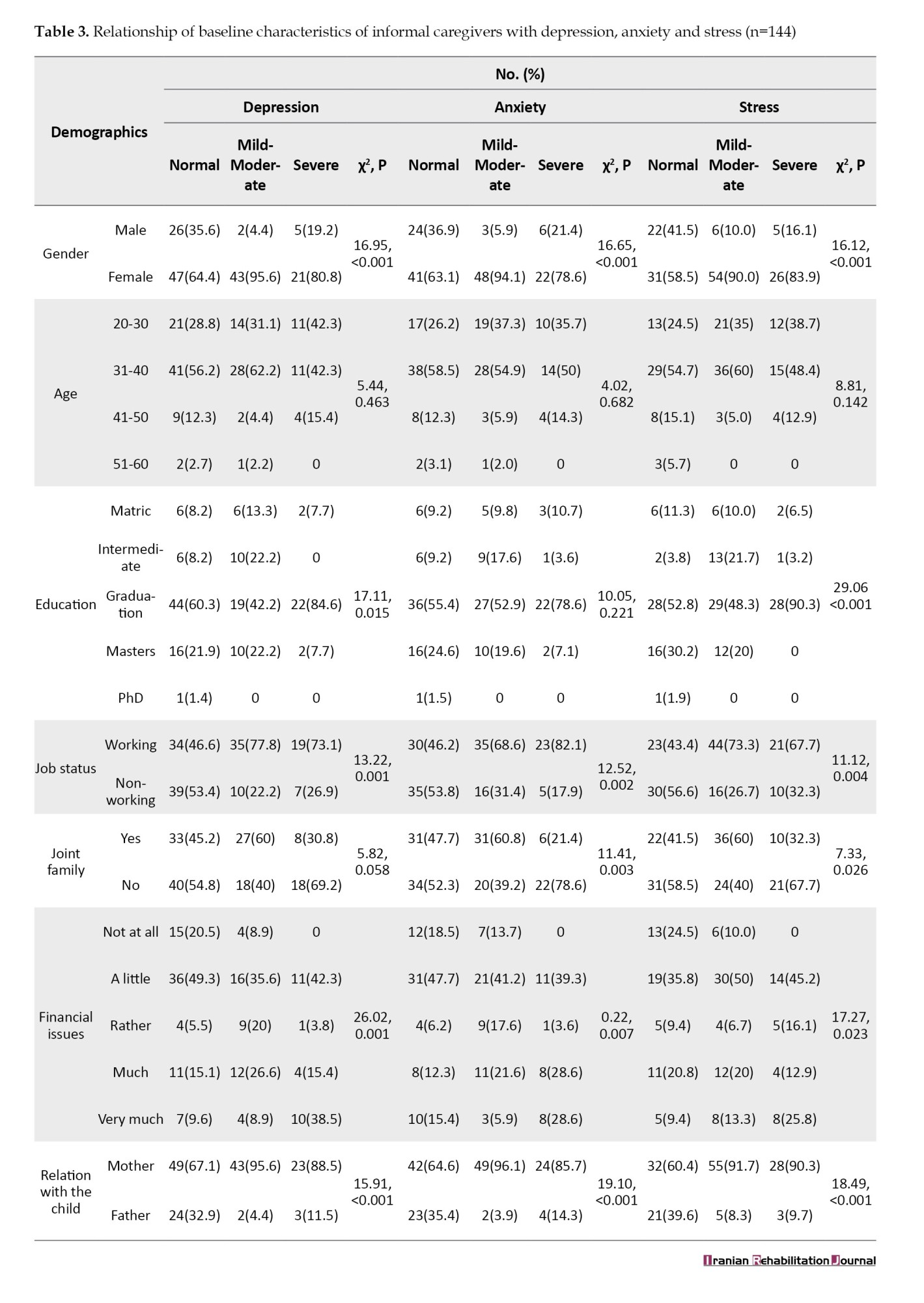
Most of the informal caregivers were literate with graduates having more depression scores (P=0.015, χ2=17.11) and stress scores (P<0.001, χ2=29.06) (Table 3). Significant depression, anxiety, and stress were observed in females (P<0.001, χ2=16.95, 16.65, 16.12, respectively). Participants who were not working were severely depressed (P<0.001, χ2=13.22), were severely anxious (P=0.002, χ2=12.52), and were in extremely severe stress (P=0.004, χ2=11.12). Parents of autistic children living separately were severely anxious (P=0.003, χ2=11.41) and had significant stress (P=0.026, χ2=7.33). Due to financial burden, parents were mild to moderately depressed (P=0.001, χ2=26.02), mild to moderately anxious (P=0.007, χ2=20.22), and mild to moderately stressed (P=0.023, χ2=17.27).
Discussion
Parents of children with ASD often have more stress, anxiety, and depression [15]. This study compared depression, anxiety and stress among the formal and informal caregivers of children with ASD and results show that informal caregivers are more prone to depression, anxiety, and stress as compared to the formal caregivers.
Almost 50% of the formal caregivers, including occupational therapists, speech therapists, psychologists, and special educators had normal depression, anxiety and stress levels. Formal caregivers are satisfied with their jobs and the profession with active involvement with the environment and have financial stability. Therapists usually took 30-40 min sessions and were not involved emotionally. Additionally, this limited time spent with the ASD child could account for this finding as compared to parents who spend all the time with their children. Furthermore, therapists probably had more training, resources, and experience with children with ASD and behavior problems than parents [16].
A previous study conducted in Australia shows a higher prevalence of anxiety among informal caregivers, 17.1% as compared to the normal adult population which was reported as 9.1%; similarly, 60% of the parents of children with autism experience depression compared to 15% of the general Australian population [11]. Another study conducted in Australia in 2017 reported that 10% of caregivers of ASD were depressed and 13.3% were anxious and stressed [9].
In this study, mothers of autistic children experienced more depression, anxiety and stress as compared to fathers. These results are comparable with a study conducted by Hodapp et al. [19] and Dabrowska et al. [20]. It may be because mothers spend more time with their children as compared to fathers as in our part of the world, fathers are the main breadwinners of families and this usually requires late working hours [17]. In addition, participants in our study were predominantly females.
In addition, the level of education of parents of autistic children was not significantly associated with anxiety but parents with higher education status reported moderate to severe depression and stress. In contrast, previous studies showed that the educational level was not significantly associated with stress but found that depression and anxiety were higher among more educated caregivers [4]. This may be because higher education status leads to more awareness about the condition and eventually results in worries about the child’s future.
A contributing factor for depression, anxiety, and stress in our study was financial stability. The informal caregivers reported 35.6%, 41.2% and 50% of mild to moderate depression, anxiety, and stress, respectively, who were facing a little financial issue [18]. These financial challenges could be because of expensive treatment and therapies for ASD children.
Conclusion
Depression, anxiety and stress are more common in parents of autistic children (informal caregivers) as compared to formal caregivers. Formal caregivers coped better with depression, stress, and anxiety as compared to informal caregivers. Further studies are warranted with gold-standard interviews and qualitative approaches which should focus on the correlation of these indices. Intervention-based approaches and strategies should be included. To gain more insight, various measures, such as counseling, building community, and family and social support to the affected child’s parents must be incorporated.
Study limitations
To the best of our knowledge, this was the kind of the first study conducted in Pakistan on the mental states of especially formal caregivers. However, our study is subjected to certain limitations. The male-to-female ratio of participants was unbalanced. This study used the DASS-42 scale, which comprises on symptoms checklist only so it is inferior to the gold standard interviews or qualitative approach. In addition, the chances of reporting bias cannot be ignored. The results from the present study are limited in their generalizability due to the relatively small study sample.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Institutional Review Board (IRB) of Jinnah Sindh Medical University (Code: JSMU/IRB/2019/-171). All procedures performed in studies involving human participants were following the ethical standards of the institutional and/or National Research Committee and with the Helsinki Declaration.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design, conceptualization, data collection and data analysis: Aliza Zehra; Formal analysis: Uzma Qadri Writing the original draft: Muhammad Ovais; Supervision, review and editing: Zaeema Ahmer.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge Iqbal Afridi for validating the questionnaire and providing guidance at the start of the project.
References
Autism spectrum disorder (ASD) is characterized by impaired social behavior, communication, and language, a lack of interests. and repetitive activities that are unique to the individual [1]. The average age for the symptoms of autism to appear is before the age of 3 years [2]. About 1 out of 100 children are suffering from ASD [3]. The worldwide prevalence of autism is 1-2 per 1000 children and according to the Centre for Disease Control, 9 out of 1000 children have been diagnosed with autism in the United States [4]. Autism is associated with a high incidence of stress, anxiety, and depression in its caregivers. A study conducted on a sample of 220 caregivers of ASD in Oman in 2016 reported 45.9% and 48.6% of anxiety and stress, respectively [5]. A study in Thailand in 2010 showed the prevalence of depression at 25.6% [6].
Children with ASD may have various symptoms, such as hyperactivity, self-injurious behavior, cognitive impairment, or the presence of repetitive movements [7, 8]. These lead to an array of factors, including social criticism, affected interpersonal relationships, uncontrolled behaviors, and reduced care which can then affect the quality of life [4, 5, 9]. It is also reported that psychological distress is higher among caregivers of ASD, especially mothers, who are informal caregivers. They are more prone to depression, stress, and anxiety as compared to mothers of children with mild intellectual disability and normal developmental children [4, 5, 10]. Families with special needs face everyday challenges, and experience more psychological burdens that include somatic complaints, heart pain, breathing difficulties, stress, financial burden, and reduced interpersonal relationships [5, 11].
Behavior problems of autistic children are the most common cause of high parental stress, anxiety, and depression; however, the relation between behavior problems and these three issues receives little attention in the population. Formal caregivers who include trained professionals who care for children with ASD are largely ignored when reporting caregiver burden. According to our knowledge, no studies have been focused on formal caregivers of ASD in Pakistan.
This study helps to identify the gravity of the issue in both formal and informal caregivers so that support and non-pharmacological intervention can be provided to the caregivers. This will eventually help the sufferers of autism. Therefore, this study evaluates depression, stress, and anxiety among formal and informal caregivers of ASD.
Materials and Methods
This was a cross-sectional study conducted among the formal and informal caregivers of autistic children in the following centers in Karachi (Figure 1).
The duration of the study was 6-8 months, but due to the COVID-19 pandemic and the sudden complete lockdown of the city in 2020, the data collection process was delayed. Due to precautionary measures, it took around 2 years to complete the data collection procedure.
The sample size was calculated using the open access online sample size calculator (Open Epi calculator), by using a previous study in Australia with the prevalence of depression at 21%, anxiety at 17.1% and stress at 13.3% among caregivers of autistic children. The estimated sample size calculated for the prevalence of depression was 255, for anxiety 218, and stress 178 subjects. Accordingly, the highest prevalence of depression was taken as the anticipated frequency at the confidence level of 95%, and bound on the error of 5%, the sample size was obtained at 255 [12]. There were 255 participants out of which 111 were formal caregivers working with autism in specified centers of Karachi City, Pakistan, and 144 were informal caregivers. There were mostly females (mothers) because most fathers were not available in the therapy center and they did not have the time to complete the questionnaire due to their tough job.
Since a sampling frame was not available, the convenience sampling method was used to recruit the participants. Study participants who were available at the time of data collection and willing to be part of the survey were invited to the study. Formal caregivers were operationalized as trained professionals who spent 30 min to 1 h of their time with the autistic child and were paid for their services [13]. In this context, formal caregivers included employees working in the institute with ASD children for >3 months, both genders and the ones who gave informed written consent. The informal caregivers were operationalized as parents with one or more autistic children who gave informed written consent. Caregivers who were tending to children with any physical disabilities or those who had any history of psychological disorder or a history of drug addiction, and who did not provide consent to participate were excluded from this study.
The data collection tool was the depression anxiety stress scale 42 (DASS-42) developed by Lovibond (1995) [14]. Before the use of scale, permission was taken from the author through email. The DASS-42 is a set of three self-report scales designed to measure the negative emotional states of depression, anxiety, and stress. The test-retest reliability of the three scales was considered adequate with a Cronbach α of 0.71 for depression, 0.79 for anxiety, and 0.81 for stress. The participants were asked to use 4-point severity/frequency scales to rate the extent to which they have experienced each state. Scores for depression, anxiety and stress were calculated by summing the scores for the relevant items.
Each of the three DASS-42 scales contains 14 items, which are divided into subscales of 2-5 items with similar content. The scale was comprised of normal, mild moderate, severe, and highly severe with scores ranging from 0 to 32. The higher the scores for each domain reflected greater levels of depression, anxiety, and stress. A semi-structured questionnaire was also used to gather information on socio-demographic characteristics, including age, gender, occupation, socioeconomic status, education, financial issues faced, family system, working hours and job satisfaction along with DASS-42.
The participants were invited directly from the selected institutes for quantitative assessment. Subjects who fulfilled the criteria of the study and provided their consent were approached. The data were entered with caution to avoid any missing values.
Statistical analysis
All the data was entered and analyzed using the SPSS software, version 22. Percentages were reported for all the categorical variables, including gender, occupation, and education. Since we hypothesized that DASS-42 is more common among informal caregivers as compared to formal caregivers we applied the Fisher exact test to determine the relationship between the frequency of depression anxiety and stress among both the groups. The statistical significance was set at 0.05.
Results
The relationship of formal and informal caregivers with depression, anxiety, and stress is shown in Table 1. Accordingly, 76.3% of informal caregivers were suffering from mild depression, 59.3% were moderately depressed, and 76.5 % were severely depressed (P<0.01, χ2=26.61). Similarly, 72.4% had mild anxiety, 68.2% were moderately anxious and 50.5% were severely anxious (P<0.01, χ2 =19.58). Also, 75.0% had mild stress, 71.1% had moderate stress, 85.7% had severe stress, and 95.0% had extremely severe stress (P<0.01, χ2=45.4).
Formal caregivers who were aged between 20-30 years showed more stress (P=0.017, χ2=7.37). In terms of occupation, the special educators showed a significant anxiety score (P=0.011, χ2=17.67) (Table 2). Meanwhile, satisfaction with the job was the main factor that was also associated with depression and anxiety in formal caregivers. Some of the participants were significantly depressed (P=0.013, χ2=16.68) and had significant anxiety scores (P=0.012, χ2=17.06).
Most of the informal caregivers were literate with graduates having more depression scores (P=0.015, χ2=17.11) and stress scores (P<0.001, χ2=29.06) (Table 3). Significant depression, anxiety, and stress were observed in females (P<0.001, χ2=16.95, 16.65, 16.12, respectively). Participants who were not working were severely depressed (P<0.001, χ2=13.22), were severely anxious (P=0.002, χ2=12.52), and were in extremely severe stress (P=0.004, χ2=11.12). Parents of autistic children living separately were severely anxious (P=0.003, χ2=11.41) and had significant stress (P=0.026, χ2=7.33). Due to financial burden, parents were mild to moderately depressed (P=0.001, χ2=26.02), mild to moderately anxious (P=0.007, χ2=20.22), and mild to moderately stressed (P=0.023, χ2=17.27).
Discussion
Parents of children with ASD often have more stress, anxiety, and depression [15]. This study compared depression, anxiety and stress among the formal and informal caregivers of children with ASD and results show that informal caregivers are more prone to depression, anxiety, and stress as compared to the formal caregivers.
Almost 50% of the formal caregivers, including occupational therapists, speech therapists, psychologists, and special educators had normal depression, anxiety and stress levels. Formal caregivers are satisfied with their jobs and the profession with active involvement with the environment and have financial stability. Therapists usually took 30-40 min sessions and were not involved emotionally. Additionally, this limited time spent with the ASD child could account for this finding as compared to parents who spend all the time with their children. Furthermore, therapists probably had more training, resources, and experience with children with ASD and behavior problems than parents [16].
A previous study conducted in Australia shows a higher prevalence of anxiety among informal caregivers, 17.1% as compared to the normal adult population which was reported as 9.1%; similarly, 60% of the parents of children with autism experience depression compared to 15% of the general Australian population [11]. Another study conducted in Australia in 2017 reported that 10% of caregivers of ASD were depressed and 13.3% were anxious and stressed [9].
In this study, mothers of autistic children experienced more depression, anxiety and stress as compared to fathers. These results are comparable with a study conducted by Hodapp et al. [19] and Dabrowska et al. [20]. It may be because mothers spend more time with their children as compared to fathers as in our part of the world, fathers are the main breadwinners of families and this usually requires late working hours [17]. In addition, participants in our study were predominantly females.
In addition, the level of education of parents of autistic children was not significantly associated with anxiety but parents with higher education status reported moderate to severe depression and stress. In contrast, previous studies showed that the educational level was not significantly associated with stress but found that depression and anxiety were higher among more educated caregivers [4]. This may be because higher education status leads to more awareness about the condition and eventually results in worries about the child’s future.
A contributing factor for depression, anxiety, and stress in our study was financial stability. The informal caregivers reported 35.6%, 41.2% and 50% of mild to moderate depression, anxiety, and stress, respectively, who were facing a little financial issue [18]. These financial challenges could be because of expensive treatment and therapies for ASD children.
Conclusion
Depression, anxiety and stress are more common in parents of autistic children (informal caregivers) as compared to formal caregivers. Formal caregivers coped better with depression, stress, and anxiety as compared to informal caregivers. Further studies are warranted with gold-standard interviews and qualitative approaches which should focus on the correlation of these indices. Intervention-based approaches and strategies should be included. To gain more insight, various measures, such as counseling, building community, and family and social support to the affected child’s parents must be incorporated.
Study limitations
To the best of our knowledge, this was the kind of the first study conducted in Pakistan on the mental states of especially formal caregivers. However, our study is subjected to certain limitations. The male-to-female ratio of participants was unbalanced. This study used the DASS-42 scale, which comprises on symptoms checklist only so it is inferior to the gold standard interviews or qualitative approach. In addition, the chances of reporting bias cannot be ignored. The results from the present study are limited in their generalizability due to the relatively small study sample.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Institutional Review Board (IRB) of Jinnah Sindh Medical University (Code: JSMU/IRB/2019/-171). All procedures performed in studies involving human participants were following the ethical standards of the institutional and/or National Research Committee and with the Helsinki Declaration.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design, conceptualization, data collection and data analysis: Aliza Zehra; Formal analysis: Uzma Qadri Writing the original draft: Muhammad Ovais; Supervision, review and editing: Zaeema Ahmer.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge Iqbal Afridi for validating the questionnaire and providing guidance at the start of the project.
References
- Suthar N, Jain S, Nebhinani N, Singhai K. Autism spectrum disorder and its differential diagnosis: A nosological update. Journal of Indian Association for Child and Adolescent Mental Health. 2020; 16(1):86-101. [DOI:10.1177/0973134220200107]
- Sturner R, Howard B, Bergmann P, Attar S, Stewart-Artz L, Bet K, et al. Autism screening at 18 months of age: A comparison of the Q-CHAT-10 and M-CHAT screeners. Molecular Autism. 2022; 13(1):2. [DOI:10.1186/s13229-021-00480-4] [PMID]
- Zeidan J, Fombonne E, Scorah J, Ibrahim A, Durkin MS, Saxena S, et al. Global prevalence of autism: A systematic review update. Autism Research: Official Journal of the International Society for Autism Research. 2022; 15(5):778-90. [DOI:10.1002/aur.2696] [PMID]
- Almansour MA, Alateeq MA, Alzahrani MK, Algeffari MA, Alhomaidan HT. Depression and anxiety among parents and caregivers of autistic spectral disorder children. Neurosciences (Riyadh, Saudi Arabia). 2013; 18(1):58-63. [PMID]
- Rezendes DL, Scarpa A. Associations between Parental Anxiety/Depression and Child Behavior Problems Related to Autism Spectrum Disorders: The roles of parenting stress and parenting self-efficacy. Autism Research and Treatment. 2011; 2011:395190. [DOI:10.1155/2011/395190] [PMID]
- Charnsil C, Bathia N. Prevalence of depressive disorders among caregivers of children with autism in Thailand. ASEAN Journal of Psychiatry. 2010; 11(1):87-95. [Link]
- Sivberg B. Family system and coping behaviors: a comparison between parents of children with autistic spectrum disorders and parents with non-autistic children. Autism. 2002; 6(4):397-409. [DOI:10.1177/1362361302006004006] [PMID]
- Al-Farsi OA, Al-Farsi YM, Al-Sharbati MM, Al-Adawi S. Stress, anxiety, and depression among parents of children with autism spectrum disorder in Oman: A case-control study. Neuropsychiatric Disease and Treatment. 2016; 12:1943-51. [DOI:10.2147/NDT.S107103] [PMID]
- Falk NH, Norris K, Quinn MG. The factors predicting stress, anxiety and depression in the parents of children with autism. Journal of Autism and Developmental Disorders. 2014; 44(12):3185-203. [DOI:10.1007/s10803-014-2189-4] [PMID]
- Samadi SA, McConkey R. The impact on Iranian mothers and fathers who have children with an autism spectrum disorder. Journal of Intellectual Disability Research. 2014; 58(3):243-54. [DOI:10.1111/jir.12005] [PMID]
- Altiere M, Von Kluge S. Family functioning and coping behaviors in parents of children with autism. Journal of Child and Family Studies. 2008; 18:83-92. [DOI:10.1007/s10826-008-9209-y]
- Bitsika V, Sharpley CF. Stress, anxiety and depression among parents of children with autism spectrum disorder. Journal of Psychologists and Counsellors in Schools. 2004; 14(2):151-61. [DOI:10.1017/S1037291100002466]
- Ten Hoopen LW, de Nijs PF, Duvekot J, Greaves-Lord K, Hillegers MH, Brouwer WB, Hakkaart-van Roijen L. Caring for children with an autism spectrum disorder: Factors associating with health-and care-related quality of life of the caregivers. Journal of Autism and Developmental Disorders. 2022: 1:1-4. [DOI: 10.1007/s10803-019-04249-w]
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy. 1995; 33(3):335-43. [DOI:10.1016/0005-7967(94)00075-U] [PMID]
- Firth I, Dryer R. The predictors of distress in parents of children with autism spectrum disorder. Journal of Intellectual & Developmental Disability. 2013; 38(2):163-71. [DOI:10.3109/13668250.2013.773964] [PMID]
- Lecavalier L. Behavioral and emotional problems in young people with pervasive developmental disorders: Relative prevalence, effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders. 2006; 36(8):1101-14. [DOI:10.1007/s10803-006-0147-5] [PMID]
- Merkaj V, Kika M, Simaku A. Symptoms of stress, depression and anxiety between parents of autistic children and parents of tipically developing children. Academic Journal of Interdisciplinary Studies. 2013: 2(2):345. [DOI: 10.36941/ajis]
- Benderix Y, Sivberg B. Siblings’ experiences of having a brother or sister with autism and mental retardation: A case study of 14 siblings from five families. Journal of Pediatric Nursing. 2007; 22(5):410-8. [DOI:10.1016/j.pedn.2007.08.013] [PMID]
- Hodapp RM, Ricci LA, Ly TM, Fidler DJ. The effects of the child with Down syndrome on maternal stress. British Journal of Developmental Psychology. 2003; 21(1):137-51. [DOI: 10.1348/026151003321164672]
- Dabrowska A, Pisula E. Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. Journal of Intellectual Disability Research. 2010; 54(3):266-80. [DOI: 10.1111/j.1365-2788.2010.01258.x]
Article type: Original Research Articles |
Subject:
Psychology
Received: 2023/02/8 | Accepted: 2023/07/25 | Published: 2024/06/1
Received: 2023/02/8 | Accepted: 2023/07/25 | Published: 2024/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
