
988368
Tue, Jul 28, 2026

Volume 23, Issue 2 (June 2025)
Iranian Rehabilitation Journal 2025, 23(2): 141-152 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sedaghati P, Ghafoori M, Parvaneh Sarand A. Functional Tests' Sensitivity and Specificity for Return to Sport After ACL Reconstruction: A Scoping Review. Iranian Rehabilitation Journal 2025; 23 (2) :141-152
URL: http://irj.uswr.ac.ir/article-1-1908-en.html
URL: http://irj.uswr.ac.ir/article-1-1908-en.html



1- Department of Physical Education and Sport Sciences, Faculty of Physical Education and Sports Sciences, University of Guilan, Rasht, Iran.
Full-Text [PDF 621 kb]
(1568 Downloads)
| Abstract (HTML) (4576 Views)
Full-Text: (557 Views)
Introduction
One of the most common knee injuries is anterior cruciate ligament (ACL) injury, which occurs among patients aged 16-39 years [1-3]. ACL injuries can have short- and long-term consequences that encompass several factors. These consequences may include muscle weakness, physical deficits, decreased engagement in sports activities, an elevated risk of re-injury to the knee, and the potential development of osteoarthritis in the affected knee. These outcomes can significantly impact an individual’s overall physical function and quality of life. It is essential to consider these factors when evaluating the effects of ACL injuries and determining appropriate interventions for rehabilitation and return to sports (RTS) [4-7]. Deciding when an athlete is ready to RTS can be difficult as a physician or clinician. Various elements must be considered, such as muscle strength, cardiovascular fitness, balance, and psychological readiness. By tracking progress in these areas, practitioners can make more informed decisions and increase the likelihood that the athlete will RTS at an optimal performance level [8]. Owing to the latest technological developments, medical, rehabilitation, and performance professionals can now easily gather data that can be utilized to enhance the care and development of athletes as they prepare for RTS. Nevertheless, understanding the significance and application of collected data remains challenging [8]. The success of RTS after ACL injuries often relies on a comprehensive biopsychosocial approach to rehabilitation. This approach considers the biological aspects of injury and recovery, as well as the psychological and social factors that can influence an individual’s ability to RTS successfully. By addressing all these dimensions, including physical rehabilitation, psychological support, and social factors, the chances of a successful RTS can be significantly enhanced [9], and several factors likely affect its success. As a result, RTS assessments have become a vital and indispensable clinical and functional tool for determining readiness to RTS [10]. The selected papers and their results can be clinically crucial in advancing the RTS procedure and assessing the risk of reinjury after ACL reconstruction (ACLR). The findings from these studies can provide valuable insights and inform clinical decision-making to enhance the RTS process and minimize the chances of reinjury following ACLR [11]. The RTS process consists of several phases that pave the way and open the door for clinicians, practitioners, and trainers to focus on functional tests that play a crucial role in helping athletes after ACLR. Both clinical and functional tests are available. The term “sensitivity” is commonly used in medical testing and refers to the ability of a test to accurately identify individuals with the disease or condition being tested. In other words, a test’s sensitivity measures its ability to correctly recognize individuals with errors [12]. An assessment with 100% sensitivity accurately identifies all individuals with the errors, whereas a test with 80% sensitivity can identify 80% of those with the error, leaving 20% of cases unnoticed [12]. To pinpoint a significant yet avoidable mistake, a high level of sensitivity is particularly crucial [12]. Conversely, the term “specificity” pertains to the test’s capability to accurately exclude individuals who do not possess the disease or condition under examination [12]. Hence, a test with 100% sensitivity precisely identifies all individuals without errors [12]. An 80% specificity test correctly classifies 80% of individuals without errors as test negatives (true negatives), yet it erroneously categorizes 20% of error-free individuals as test positives (false positives) [12]. Herbst et al. [13] and Hildebrandt et al. as an example, [14] conducted seven functional assessments, which included the two-leg stability test, one-leg stability test, two-leg counter-movement jump, one-leg counter-movement jump, plyometric jumps, speedy test, and quick feet test. The results indicated that all the tests demonstrated moderate to substantial levels of reliability [15]. Although these functional tests’ validity and test, re-test reliability have been investigated and verified, they have limitations when used as a standardized set of measurements. This is primarily due to their time-consuming and intricate testing procedures [14, 16, 17]. When assessing sports-related performance, it is crucial to consider factors beyond the reliability and validity of functional tests. Considerations, such as cost, user-friendliness, and portability, are also significant. The single-leg hop test, which has consistently been suggested, serves as a valuable tool for evaluating athletic outcomes after ACLR [18, 19]. Hence, this study aimed to explore functional tests and assess their sensitivity and specificity in RTS after ACLR.
Materials and Methods
This scoping review was based on the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.
Search strategy
A thorough analysis of functional tests, encompassing their sensitivity and specificity for RTS after ACLR by searching the Web of Science, PEDRO, Google Scholar, PubMed, ScienceDirect, SCOPUS, CINAHL databases with the keywords using three groups of search terms: (group 1) “ACL RTS” OR “return to play” OR “return to competition” OR “return to activities” OR “return to participation;” AND (group 2) “lower extremity” OR “lower body” OR “lower limb” OR “ACL complex;” AND (group 3) “ACL functional tests” OR “ACL functional battery tests” OR “ACL functional assessment” OR “ACL functional evaluation.” These combinations (involving three groups) were investigated in the titles, abstracts, and keywords of studies published in indexed journals from 2000 to January 2023. Manual searches were conducted to identify articles that might not have appeared in online searches, and a thorough review of article sources was performed.
Eligibility criteria
The inclusion criteria included athletes or people who underwent rehabilitation programs, suffered ACL injuries, used functional tests to RTS; English-language articles, full-text studies were published, and also studies which were randomized control trial (RCT), cross-sectional, and cohort designs; other knee injuries, such as fractures of the proximal arm and articles that were published briefly in congresses and seminars. The exclusion criteria included non-English articles and tests that were not used for RTS.
Study selection
English was used for this search. The researchers screened all the texts. Finally, 127 articles were received from databases using relevant keywords. At first, the titles of the articles were examined, and 12 duplicate articles were removed. In the next step, the abstracts of 115 articles were examined, and, 78 articles were excluded from the survey because they did not meet the inclusion criteria. Next, 37 articles were thoroughly examined in their entirety. Subsequently, 23 of these articles were eliminated from consideration because they did not meet the inclusion criteria. For example, articles in Chinese (9 articles) and Hindi (5 articles) that did not use performance tests for returning to sports after ACLR were deleted. Finally, 14 articles were included in the present review and their results were fully reported. The final compilation of the acquired articles was reviewed by another prominent researcher to ensure that they aligned with the study objectives. The process of obtaining study 2 is illustrated in Figure 1. The structure adheres to the population, intervention, comparison, outcomes, and study (PICOS) framework (Table 1), which is connected to the survey question below.
.PNG)
.PNG)
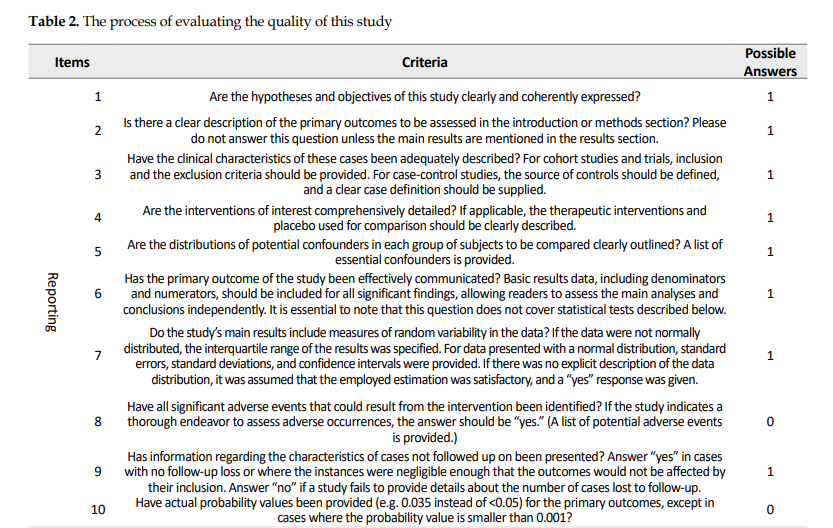
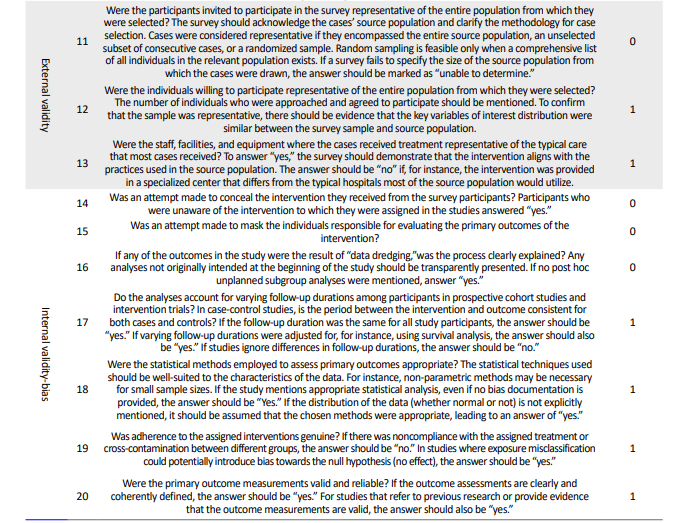
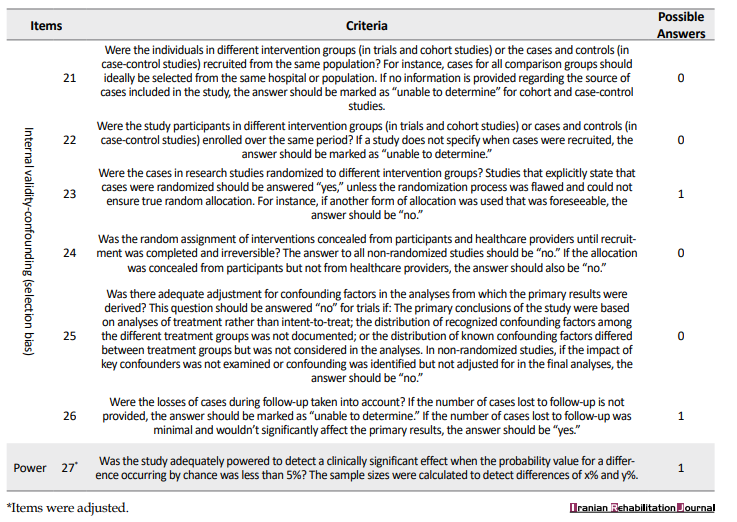
By searching databases, such as Web of Science, PEDRO, Google Scholar, PubMed, ScienceDirect, SCOPUS, and CINAHL, 127 papers were acquired. After removing duplicate titles, 115 abstracts were chosen for assessment. After reviewing these abstracts, 78 papers were excluded. Subsequently, 37 full-text papers were selected for further evaluation. After scrutinizing these full-text papers, 23 articles were disqualified, and 14 articles that met the criteria were included in the study. Table 2 shows the process of evaluating the quality of this study, and Figure 1 shows the process of evaluating and selecting research articles.
Results
The study included ACL functional tests, and the results were compared with those of existing studies. Approximately, 31 tests, including balance and postural control, agility, power, screening, and movement pattern tests, were included, each explained separately. Tables 3, 4, 5 and 6 present the RTS functional tests and their specificities and sensitivities.
.PNG)
Discussion
This review article was conducted to report the common functional tests and their sensitivity and specificity for RTS after ACLR. A significant finding of this review was that 60% of the articles showed that hop group tests are the most common functional tests after ACLR. Four tables were included: Balance and postural control, agility, power, screening, and movement pattern tests. The related explanation for each is discussed separately below.
Table 3 presents 20 tests of balance and postural control. Fifteen of 20 crucial tests were related to the hop group tests. The highest sensitivity was for the single-leg agility hop test and hopping obstacle course test (100% each) and the lowest sensitivity was for the balance error scoring system (BESS) test (34%). Also, the forward hop test and the hopping obstacle course test had the highest specificity (97% each), and the multiple single-leg hop stabilization test had the lowest specificity (63%). Finally, the sensitivity and specificity of the dynamic leap and balance (DLBT) test were unknown.
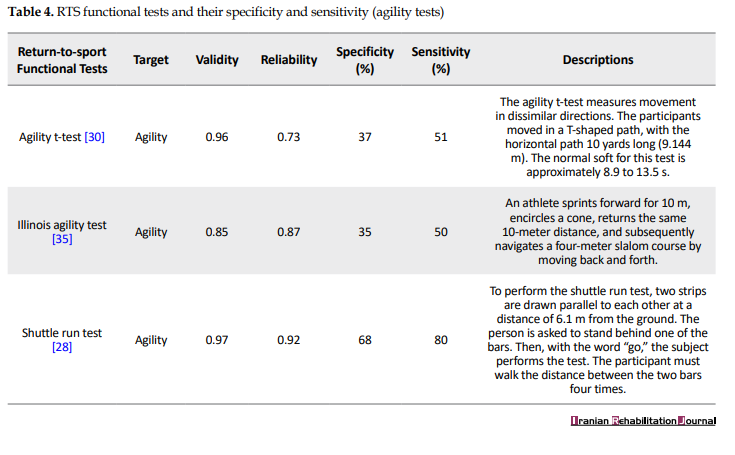
Table 4 presents the three agility tests. The shuttle run test had the highest sensitivity (80%), and the Illinois test had the lowest sensitivity (34%). Also, the shuttle run test had the highest specificity (68%), and the Illinois test had the lowest specificity (35%).
Table 5 presents three tests of power. The vertical jump test and the single-leg vertical jump test had the highest sensitivity (95% each), and the Carioca test had the lowest sensitivity (75%). Also, the Carioca test had the highest specificity (80%), while the vertical jump and single-leg vertical jump tests had the lowest specificity (46% each).
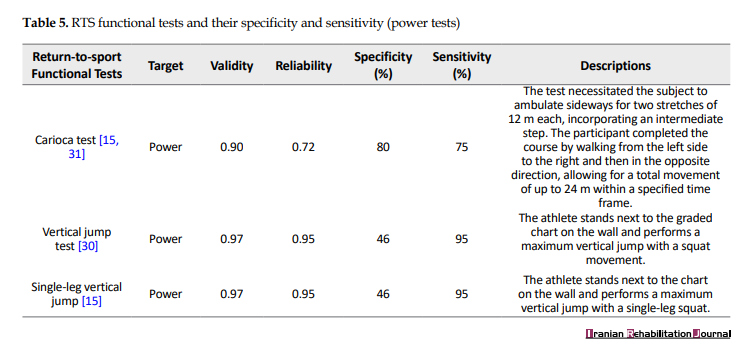
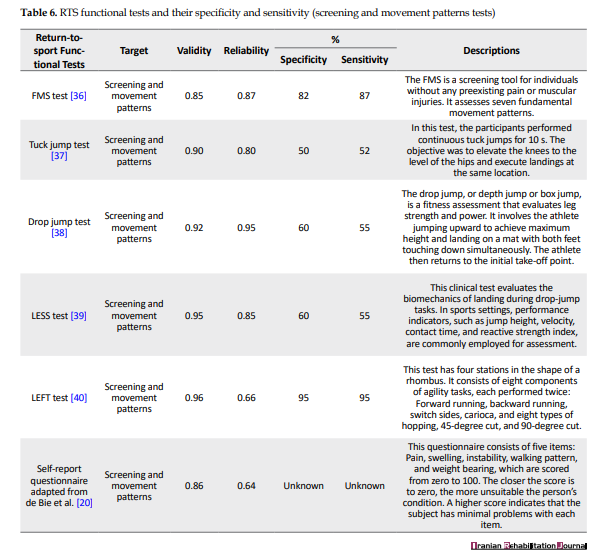
Table 6 presents six screening and movement pattern tests; one was a self-report questionnaire. The highest sensitivity was for the lower extremity functional test (LEFT) protocol (95%), and the lowest sensitivity was for the tuck jump test (52%). Also, the highest specificity was for the LEFT (95%), and the lowest specificity was for the tuck jump test (50%). Finally, the sensitivity and specificity of the self-report questionnaire adapted from de Bie et al. were unknown [20].
According to the above findings of each Table, it can be mentioned that the hop tests (Table 3), the shuttle run test (Table 4), the vertical jump tests and the Carioca test (Table 5), and the LEFT test may be more appropriate functional tests for RTS after ACLR in terms of sensitivity and specificity which were the main focus of this scoping review. Additionally, 10 of the 14 articles in this review assessed football players using hop tests, highlighting the importance of dynamic and static stability in football. However, others have focused on other components that are also crucial in sports. Considering the body as a whole and focusing on training principles, such as performing a task unilaterally in an open or closed kinetic chain with perturbation, along with dual tasks and focusing on movement pattern tests in terms of skill and movement quality, may effectively involve these components when assessing athletes [8]. As previously mentioned, these functional tests could offer a more time and cost-effective alternative to clinical tests. For instance, given the significance of the hop tests, they enable us to efficiently assess performance factors, such as speed, explosive force, acceleration, stability, and balance within a short timeframe [15]. Hop tests are vital in ACL injury prevention and RTSs [11]. Different hop tests include the single-leg hop test for distance, the stair-hop test, the 6-meter single-leg hop test for time, and the triple jump test, of which three are measured based on the distance and one is measured based on time [41, 42].
Due to the complexity of identifying specific subjective and objective criteria for RTS after ACLR, a wide range of assessments were conducted to determine if individuals were prepared for a functional and quantifiable return to their previous levels of physical activity [14, 43, 44]. Most injury prevention protocols, such as 11+ and the Prevent Injury and Enhance Performance Program (PEP), include hop tests. Furthermore, hop tests are crucial and occupy a distinct position in the context of RTS after ACLR [11]. RTS outcomes following ACLR are disappointing [11]. Athletes who frequently experience ACL tears are often advised to undergo ACLR to ensure their fitness for sports [45]. RTS tests may include muscular strength and power, cardiovascular fitness, postural control, dynamic balance, movement quality, plyometric tests [8], and psychological readiness assessments using questionnaires [46, 47]. According to the studies, the RTS time has been reported as 6, 9, 12 months [48-50] and even more. Nevertheless, a significant disagreement is observed regarding the appropriate timeframe for safe return to competitive sports.
We hope that upcoming studies will focus on more up-to-date and effective functional tests that provide insights to clinicians, practitioners, and trainers so that they can better assess athletes for RTS after ACLR in the future.
Conclusion
According to the results of this study, the most common functional tests were the shuttle run, vertical jump, Carioca, and LEFT tests, especially the hop tests. These tests may be more appropriate functional tests for RTS after ACLR in terms of sensitivity and specificity, which were the main focus of this scoping review. We hope these tests will be useful for personal trainers, athletic trainers, practitioners, and clinicians when evaluating injured athletes.
Limitations
This review article’s limitation included studies in non-English languages, such as Chinese and Hindi, unpublished studies, and studies in other motor searches. The authors hope that future research will address these gaps.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to those who helped them prepare and write this manuscript.
One of the most common knee injuries is anterior cruciate ligament (ACL) injury, which occurs among patients aged 16-39 years [1-3]. ACL injuries can have short- and long-term consequences that encompass several factors. These consequences may include muscle weakness, physical deficits, decreased engagement in sports activities, an elevated risk of re-injury to the knee, and the potential development of osteoarthritis in the affected knee. These outcomes can significantly impact an individual’s overall physical function and quality of life. It is essential to consider these factors when evaluating the effects of ACL injuries and determining appropriate interventions for rehabilitation and return to sports (RTS) [4-7]. Deciding when an athlete is ready to RTS can be difficult as a physician or clinician. Various elements must be considered, such as muscle strength, cardiovascular fitness, balance, and psychological readiness. By tracking progress in these areas, practitioners can make more informed decisions and increase the likelihood that the athlete will RTS at an optimal performance level [8]. Owing to the latest technological developments, medical, rehabilitation, and performance professionals can now easily gather data that can be utilized to enhance the care and development of athletes as they prepare for RTS. Nevertheless, understanding the significance and application of collected data remains challenging [8]. The success of RTS after ACL injuries often relies on a comprehensive biopsychosocial approach to rehabilitation. This approach considers the biological aspects of injury and recovery, as well as the psychological and social factors that can influence an individual’s ability to RTS successfully. By addressing all these dimensions, including physical rehabilitation, psychological support, and social factors, the chances of a successful RTS can be significantly enhanced [9], and several factors likely affect its success. As a result, RTS assessments have become a vital and indispensable clinical and functional tool for determining readiness to RTS [10]. The selected papers and their results can be clinically crucial in advancing the RTS procedure and assessing the risk of reinjury after ACL reconstruction (ACLR). The findings from these studies can provide valuable insights and inform clinical decision-making to enhance the RTS process and minimize the chances of reinjury following ACLR [11]. The RTS process consists of several phases that pave the way and open the door for clinicians, practitioners, and trainers to focus on functional tests that play a crucial role in helping athletes after ACLR. Both clinical and functional tests are available. The term “sensitivity” is commonly used in medical testing and refers to the ability of a test to accurately identify individuals with the disease or condition being tested. In other words, a test’s sensitivity measures its ability to correctly recognize individuals with errors [12]. An assessment with 100% sensitivity accurately identifies all individuals with the errors, whereas a test with 80% sensitivity can identify 80% of those with the error, leaving 20% of cases unnoticed [12]. To pinpoint a significant yet avoidable mistake, a high level of sensitivity is particularly crucial [12]. Conversely, the term “specificity” pertains to the test’s capability to accurately exclude individuals who do not possess the disease or condition under examination [12]. Hence, a test with 100% sensitivity precisely identifies all individuals without errors [12]. An 80% specificity test correctly classifies 80% of individuals without errors as test negatives (true negatives), yet it erroneously categorizes 20% of error-free individuals as test positives (false positives) [12]. Herbst et al. [13] and Hildebrandt et al. as an example, [14] conducted seven functional assessments, which included the two-leg stability test, one-leg stability test, two-leg counter-movement jump, one-leg counter-movement jump, plyometric jumps, speedy test, and quick feet test. The results indicated that all the tests demonstrated moderate to substantial levels of reliability [15]. Although these functional tests’ validity and test, re-test reliability have been investigated and verified, they have limitations when used as a standardized set of measurements. This is primarily due to their time-consuming and intricate testing procedures [14, 16, 17]. When assessing sports-related performance, it is crucial to consider factors beyond the reliability and validity of functional tests. Considerations, such as cost, user-friendliness, and portability, are also significant. The single-leg hop test, which has consistently been suggested, serves as a valuable tool for evaluating athletic outcomes after ACLR [18, 19]. Hence, this study aimed to explore functional tests and assess their sensitivity and specificity in RTS after ACLR.
Materials and Methods
This scoping review was based on the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.
Search strategy
A thorough analysis of functional tests, encompassing their sensitivity and specificity for RTS after ACLR by searching the Web of Science, PEDRO, Google Scholar, PubMed, ScienceDirect, SCOPUS, CINAHL databases with the keywords using three groups of search terms: (group 1) “ACL RTS” OR “return to play” OR “return to competition” OR “return to activities” OR “return to participation;” AND (group 2) “lower extremity” OR “lower body” OR “lower limb” OR “ACL complex;” AND (group 3) “ACL functional tests” OR “ACL functional battery tests” OR “ACL functional assessment” OR “ACL functional evaluation.” These combinations (involving three groups) were investigated in the titles, abstracts, and keywords of studies published in indexed journals from 2000 to January 2023. Manual searches were conducted to identify articles that might not have appeared in online searches, and a thorough review of article sources was performed.
Eligibility criteria
The inclusion criteria included athletes or people who underwent rehabilitation programs, suffered ACL injuries, used functional tests to RTS; English-language articles, full-text studies were published, and also studies which were randomized control trial (RCT), cross-sectional, and cohort designs; other knee injuries, such as fractures of the proximal arm and articles that were published briefly in congresses and seminars. The exclusion criteria included non-English articles and tests that were not used for RTS.
Study selection
English was used for this search. The researchers screened all the texts. Finally, 127 articles were received from databases using relevant keywords. At first, the titles of the articles were examined, and 12 duplicate articles were removed. In the next step, the abstracts of 115 articles were examined, and, 78 articles were excluded from the survey because they did not meet the inclusion criteria. Next, 37 articles were thoroughly examined in their entirety. Subsequently, 23 of these articles were eliminated from consideration because they did not meet the inclusion criteria. For example, articles in Chinese (9 articles) and Hindi (5 articles) that did not use performance tests for returning to sports after ACLR were deleted. Finally, 14 articles were included in the present review and their results were fully reported. The final compilation of the acquired articles was reviewed by another prominent researcher to ensure that they aligned with the study objectives. The process of obtaining study 2 is illustrated in Figure 1. The structure adheres to the population, intervention, comparison, outcomes, and study (PICOS) framework (Table 1), which is connected to the survey question below.
By searching databases, such as Web of Science, PEDRO, Google Scholar, PubMed, ScienceDirect, SCOPUS, and CINAHL, 127 papers were acquired. After removing duplicate titles, 115 abstracts were chosen for assessment. After reviewing these abstracts, 78 papers were excluded. Subsequently, 37 full-text papers were selected for further evaluation. After scrutinizing these full-text papers, 23 articles were disqualified, and 14 articles that met the criteria were included in the study. Table 2 shows the process of evaluating the quality of this study, and Figure 1 shows the process of evaluating and selecting research articles.
Results
The study included ACL functional tests, and the results were compared with those of existing studies. Approximately, 31 tests, including balance and postural control, agility, power, screening, and movement pattern tests, were included, each explained separately. Tables 3, 4, 5 and 6 present the RTS functional tests and their specificities and sensitivities.
Discussion
This review article was conducted to report the common functional tests and their sensitivity and specificity for RTS after ACLR. A significant finding of this review was that 60% of the articles showed that hop group tests are the most common functional tests after ACLR. Four tables were included: Balance and postural control, agility, power, screening, and movement pattern tests. The related explanation for each is discussed separately below.
Table 3 presents 20 tests of balance and postural control. Fifteen of 20 crucial tests were related to the hop group tests. The highest sensitivity was for the single-leg agility hop test and hopping obstacle course test (100% each) and the lowest sensitivity was for the balance error scoring system (BESS) test (34%). Also, the forward hop test and the hopping obstacle course test had the highest specificity (97% each), and the multiple single-leg hop stabilization test had the lowest specificity (63%). Finally, the sensitivity and specificity of the dynamic leap and balance (DLBT) test were unknown.
Table 4 presents the three agility tests. The shuttle run test had the highest sensitivity (80%), and the Illinois test had the lowest sensitivity (34%). Also, the shuttle run test had the highest specificity (68%), and the Illinois test had the lowest specificity (35%).
Table 5 presents three tests of power. The vertical jump test and the single-leg vertical jump test had the highest sensitivity (95% each), and the Carioca test had the lowest sensitivity (75%). Also, the Carioca test had the highest specificity (80%), while the vertical jump and single-leg vertical jump tests had the lowest specificity (46% each).
Table 6 presents six screening and movement pattern tests; one was a self-report questionnaire. The highest sensitivity was for the lower extremity functional test (LEFT) protocol (95%), and the lowest sensitivity was for the tuck jump test (52%). Also, the highest specificity was for the LEFT (95%), and the lowest specificity was for the tuck jump test (50%). Finally, the sensitivity and specificity of the self-report questionnaire adapted from de Bie et al. were unknown [20].
According to the above findings of each Table, it can be mentioned that the hop tests (Table 3), the shuttle run test (Table 4), the vertical jump tests and the Carioca test (Table 5), and the LEFT test may be more appropriate functional tests for RTS after ACLR in terms of sensitivity and specificity which were the main focus of this scoping review. Additionally, 10 of the 14 articles in this review assessed football players using hop tests, highlighting the importance of dynamic and static stability in football. However, others have focused on other components that are also crucial in sports. Considering the body as a whole and focusing on training principles, such as performing a task unilaterally in an open or closed kinetic chain with perturbation, along with dual tasks and focusing on movement pattern tests in terms of skill and movement quality, may effectively involve these components when assessing athletes [8]. As previously mentioned, these functional tests could offer a more time and cost-effective alternative to clinical tests. For instance, given the significance of the hop tests, they enable us to efficiently assess performance factors, such as speed, explosive force, acceleration, stability, and balance within a short timeframe [15]. Hop tests are vital in ACL injury prevention and RTSs [11]. Different hop tests include the single-leg hop test for distance, the stair-hop test, the 6-meter single-leg hop test for time, and the triple jump test, of which three are measured based on the distance and one is measured based on time [41, 42].
Due to the complexity of identifying specific subjective and objective criteria for RTS after ACLR, a wide range of assessments were conducted to determine if individuals were prepared for a functional and quantifiable return to their previous levels of physical activity [14, 43, 44]. Most injury prevention protocols, such as 11+ and the Prevent Injury and Enhance Performance Program (PEP), include hop tests. Furthermore, hop tests are crucial and occupy a distinct position in the context of RTS after ACLR [11]. RTS outcomes following ACLR are disappointing [11]. Athletes who frequently experience ACL tears are often advised to undergo ACLR to ensure their fitness for sports [45]. RTS tests may include muscular strength and power, cardiovascular fitness, postural control, dynamic balance, movement quality, plyometric tests [8], and psychological readiness assessments using questionnaires [46, 47]. According to the studies, the RTS time has been reported as 6, 9, 12 months [48-50] and even more. Nevertheless, a significant disagreement is observed regarding the appropriate timeframe for safe return to competitive sports.
We hope that upcoming studies will focus on more up-to-date and effective functional tests that provide insights to clinicians, practitioners, and trainers so that they can better assess athletes for RTS after ACLR in the future.
Conclusion
According to the results of this study, the most common functional tests were the shuttle run, vertical jump, Carioca, and LEFT tests, especially the hop tests. These tests may be more appropriate functional tests for RTS after ACLR in terms of sensitivity and specificity, which were the main focus of this scoping review. We hope these tests will be useful for personal trainers, athletic trainers, practitioners, and clinicians when evaluating injured athletes.
Limitations
This review article’s limitation included studies in non-English languages, such as Chinese and Hindi, unpublished studies, and studies in other motor searches. The authors hope that future research will address these gaps.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to those who helped them prepare and write this manuscript.
- Lynch TS, Parker RD, Patel RM, Andrish JT; MOON Group; Spindler KP, et al. The impact of the multicenter orthopaedic outcomes network (MOON) research on anterior cruciate ligament reconstruction and orthopaedic practice. The Journal of the American Academy of Orthopaedic Surgeons. 2015; 23(3):154-63. [DOI:10.5435/JAAOS-D-14-00005] [PMID]
- Kaeding CC, Léger-St-Jean B, Magnussen RA. Epidemiology and Diagnosis of Anterior Cruciate Ligament Injuries. Clinics in Sports Medicine. 2017; 36(1):1-8. [DOI:10.1016/j.csm.2016.08.001] [PMID]
- Granan LP, Bahr R, Steindal K, Furnes O, Engebretsen L. Development of a national cruciate ligament surgery registry: The Norwegian National Knee Ligament Registry. The American Journal of Sports Medicine. 2008; 36(2):308-15. [DOI:10.1177/0363546507308939] [PMID]
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clinical Journal of Sport Medicine. 2012; 22(2):116-21. [DOI:10.1097/JSM.0b013e318246ef9e] [PMID]
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. The American Journal of Sports Medicine. 2014; 42(7):1567-73. [DOI:10.1177/0363546514530088] [PMID]
- Øiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: A systematic review. The American Journal of Sports Medicine. 2009; 37(7):1434-43. [DOI:10.1177/0363546509338827] [PMID]
- Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or surgical treatment of ACL injuries: knee function, sports participation, and knee reinjury: The Delaware-Oslo ACL Cohort Study. The Journal of Bone and Joint Surgery. American Volume. 2014; 96(15):1233-41. [DOI:10.2106/JBJS.M.01054] [PMID]
- Draovitch P, Patel S, Marrone W, Grundstein MJ, Grant R, Virgile A, et al. The return-to-sport clearance continuum is a novel approach toward return to sport and performance for the professional athlete. Arthroscopy, Sports Medicine, and Rehabilitation. 2022; 4(1):e93-e101. [DOI:10.1016/j.asmr.2021.10.026] [PMID]
- Ardern CL, Kvist J, Webster KE Psychological aspects of anterior cruciate ligament injuries. Operative Techniques in Sports Medicine. 2016; 24(1):77-83. [DOI:10.1053/j.otsm.2015.09.006]
- Ashigbi EYK, Banzer W, Niederer D. Return to sport tests' prognostic value for reinjury risk after anterior cruciate ligament reconstruction: A systematic review. Medicine and Science in Sports and Exercise. 2020; 52(6):1263-71. [DOI:10.1249/MSS.0000000000002246] [PMID]
- Buckthorpe M. Optimising the Late-Stage Rehabilitation and Return-to-Sport Training and Testing Process After ACL Reconstruction. Sports Medicine. 2019; 49(7):1043-58.[DOI:10.1007/s40279-019-01102-z] [PMID]
- Lalkhen AG, McCluskey A. Clinical tests: Sensitivity and specificity. Continuing Education in Anaesthesia, Critical Care & Pain. 2008; 8(6):221-3. [DOI:10.1093/bjaceaccp/mkn041]
- Herbst E, Hoser C, Hildebrandt C, Raschner C, Hepperger C, Pointner H, et al. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part II: Clinical application of a new test battery. Knee Surgery, Sports Traumatology, Arthroscopy. 2015; 23(5):1283-91. [DOI:10.1007/s00167-015-3546-3] [PMID]
- Hildebrandt C, Müller L, Zisch B, Huber R, Fink C, Raschner C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part I: Development of a new test battery. Knee Surgery, Sports Traumatology, Arthroscopy. 2015; 23(5):1273-81. [DOI:10.1007/s00167-015-3529-4] [PMID]
- Lee DW, Yang SJ, Cho SI, Lee JH, Kim JG. Single-leg vertical jump test as a functional test after anterior cruciate ligament reconstruction. The Knee. 2018; 25(6):1016-26. [DOI:10.1016/j.knee.2018.07.014] [PMID]
- Lephart SM, Kocher MS, Harner CD, Fu FH. Quadriceps strength and functional capacity after anterior cruciate ligament reconstruction: patellar tendon autograft versus allograft. The American Journal of Sports Medicin. 1993; 21(5):738-43. [DOI:10.1177/036354659302100519] [PMID]
- Jang SH, Kim JG, Ha JK, Wang BG, Yang SJ. Functional performance tests as indicators of returning to sports after anterior cruciate ligament reconstruction. Knee. 2014; 21(1):95-101. [DOI:10.1016/j.knee.2013.08.017] [PMID]
- Fitzgerald GK, Lephart SM, Hwang JH, Wainner RS. Hop tests as predictors of dynamic knee stability. The Journal of Orthopaedic and Sports Physical Therapy. 2001; 31(10):588-97. [DOI:10.2519/jospt.2001.31.10.588] [PMID]
- Gustavsson A, Neeter C, Thomeé P, Silbernagel KG, Augustsson J, Thomeé R, et al. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 2006;14(8):778-88. [DOI:10.1007/s00167-006-0045-6] [PMID]
- de Bie RA, de Vet HC, van den Wildenberg FA, Lenssen T, Knipschild PG. The prognosis of ankle sprains. International Journal of Sports Medicine. 1997; 18(4):285-9. [PMID]
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. Journal of Epidemiology and Community Health. 1998; 52(6):377-84. [DOI:10.1136/jech.52.6.377] [PMID]
- Reiman MP, Manske RC. Functional testing in human performance. Champaign, IL: Human kinetics; 2009. [DOI:10.5040/9781492596882]
- Caffrey E, Docherty CL, Schrader J, Klossner J. The ability of 4 single-limb hopping tests to detect functional performance deficits in individuals with functional ankle instability. Journal of Orthopaedic & Sports Physical Therapy. 2009; 39(11):799-806. [DOI:10.2519/jospt.2009.3042] [PMID]
- Richie DH, Izadi FE. Return to play after an ankle sprain: Guidelines for the podiatric physician. Clinics in Podiatric Medicine and Surgery. 2015; 32(2):195-215. [DOI:10.1016/j.cpm.2014.11.003] [PMID]
- Worrell TW, Booher LD, Hench KM. Closed kinetic chain assessment following inversion ankle sprain. Journal of Sport Rehabilitation. 1994; 3(3):197-203. [Link]
- Witchalls JB, Newman P, Waddington G, Adams R, Blanch P. Functional performance deficits associated with ligamentous instability at the ankle. Journal of Science and Medicine in Sport. 2013; 16(2):89-93. [DOI:10.1016/j.jsams.2012.05.018] [PMID]
- Halim-Kertanegara S, Raymond J, Hiller CE, Kilbreath SL, Refshauge KM. The effect of ankle taping on functional performance in participants with functional ankle instability. Physical Therapy in Sport. 2017; 23:162-7. [DOI:10.1016/j.ptsp.2016.03.005] [PMID]
- Demeritt KM, Shultz SJ, Docherty CL, Gansneder BM, Perrin DH. Chronic ankle instability does not affect lower extremity functional performance. Journal of Athletic Training. 2002; 37(4):507-11. [PMID]
- Munn J, Beard DJ, Refshauge KM, Lee RW. Do functional-performance tests detect impairment in subjects with ankle instability? Journal of Sport Rehabilitation. 2002; 11(1):40-50. [DOI:10.1123/jsr.11.1.40]
- Clanton TO, Matheny LM, Jarvis HC, Jeronimus AB. Return to play in athletes following ankle injuries. Sports Health. 2012; 4(6):471-4. [DOI:10.1177/1941738112463347] [PMID]
- Kim JG, Lee DW, Bae KC, Choi BC, Yang SJ, Cho SI, et al. Correlation of Y balance with clinical scores and functional tests after anterior cruciate ligament reconstruction in young and Middle-Aged Patients. Clinics in Orthopedic Surgery. 2023; 15(1):50-8. [DOI:10.4055/cios21131] [PMID]
- Beazell JR, Grindstaff TL, Sauer LD, Magrum EM, Ingersoll CD, Hertel J. Effects of a proximal or distal tibiofibular joint manipulation on ankle range of motion and functional outcomes in individuals with chronic ankle instability. Journal of Orthopaedic & Sports Physical Therapy. 2012; 42(2):125-34. [DOI:10.2519/jospt.2012.3729] [PMID]
- Jaffri AH, Newman TM, Smith BI, Vairo GL, Denegar CR, Buckley WE, et al. Dynamic leap and balance test (DLBT): Ability to discriminate balance deficits in individuals with chronic ankle instability. Journal of Sport Rehabilitation. 2020; 29(3):263-70. [DOI:10.1123/jsr.2018-0380] [PMID]
- Ross SE, Guskiewicz KM, Gross MT, Yu B. Assessment tools for identifying functional limitations associated with functional ankle instability. Journal of Athletic Training. 2008; 43(1):44-50. [DOI:10.4085/1062-6050-43.1.44] [PMID]
- Bisciotti GN, Quaglia A, Belli A, Carimati G, Volpi P. Return to sports after ACL reconstruction: a new functional test protocol. Muscles, Ligaments and Tendons Journal. 2016; 6(4):499-509. [PMID]
- Oleksy Ł, Mika A, Królikowska A, Kuchciak M, Stolarczyk M, Kielnar R, et al. Composite Score of Readiness (CSR) as holistic profiling of functional deficits in footballers following ACL Reconstruction. Journal of Clinical Medicine. 2021; 10(16):3570. [DOI:10.3390/jcm10163570] [PMID]
- Hoog P, Warren M, Smith CA, Chimera NJ. Functional hop tests and tuck jump assessment scores between female division I collegiate athletes participating in high versus low acl injury prone sports: A cross sectional analysis. International Journal of Sports Physical Therapy. 2016; 11(6):945-53. [PMID]
- Petushek E, Nilstad A, Bahr R, Krosshaug T. Drop jump? Single-leg squat? Not if you aim to predict anterior cruciate ligament injury from real-time clinical assessment: A prospective cohort study involving 880 elite female athletes. Journal of Orthopaedic & Sports Physical Therapy. 2021; 51(7):372-8. [DOI:10.2519/jospt.2021.10170] [PMID]
- Gokeler A, Eppinga P, Dijkstra PU, Welling W, Padua DA, Otten E, et al. Effect of fatigue on landing performance assessed with the landing error scoring system (less) in patients after ACL reconstruction. A pilot study. International Journal of Sports Physical Therapy. 2014; 9(3):302-11. [PMID]
- Brumitt J, Heiderscheit BC, Manske RC, Niemuth PE, Rauh MJ. Lower extremity functional tests and risk of injury in division iii collegiate athletes. International Journal of Sports Physical Therapy. 2013; 8(3):216-27. [PMID]
- Booher LD, Hench KM, Worrell TW, Stikeleather J. Reliability of three single-leg hop tests. Journal of Sport Rehabilitation. 1993; 2(3):165-70. [DOI:10.1123/jsr.2.3.165]
- Kotsifaki A, Korakakis V, Whiteley R, Van Rossom S, Jonkers I. Measuring only hop distance during single leg hop testing is insufficient to detect deficits in knee function after ACL reconstruction: A systematic review and meta-analysis. British Journal of Sports Medicine. 2020; 54(3):139-53. [DOI:10.1136/bjsports-2018-099918] [PMID]
- Engelen-van Melick N, van Cingel RE, Tijssen MP, Nijhuis-van der Sanden MW. Assessment of functional performance after anterior cruciate ligament reconstruction: A systematic review of measurement procedures. Knee Surgery, Sports Traumatology, Arthroscopy. 2013; 21(4):869-79. [DOI:10.1007/s00167-012-2030-6] [PMID]
- Petersen W, Taheri P, Forkel P, Zantop T. Return to play following ACL reconstruction: A systematic review about strength deficits. Archives of Orthopaedic and Trauma Surgery. 2014; 134(10):1417-28. [DOI:10.1007/s00402-014-1992-x] [PMID]
- Marx RG, Jones EC, Angel M, Wickiewicz TL, Warren RF. Beliefs and attitudes of members of the American Academy of Orthopaedic Surgeons regarding the treatment of anterior cruciate ligament injury. Arthroscopy. 2003; 19(7):762-70.[DOI:10.1016/S0749-8063(03)00398-0] [PMID]
- Faleide AGH, Magnussen LH, Strand T, Bogen BE, Moe-Nilssen R, Mo IF, et al. The role of psychological readiness in return to sport assessment after anterior cruciate ligament reconstruction. The American Journal of Sports Medicine. 2021; 49(5):1236-43. [DOI:10.1177/0363546521991924] [PMID]
- Paster E, Sayeg A, Armistead S, Feldman MD. Rehabilitation using a systematic and holistic approach for the injured athlete returning to sport. Arthroscopy, Sports Medicine, and Rehabilitation,. 2022; 4(1):e215-9. [DOI:10.1016/j.asmr.2021.09.036] [PMID]
- Edwards PK, Ebert JR, Joss B, Ackland T, Annear P, Buelow JU, et al. Patient characteristics and predictors of return to sport at 12 months after anterior cruciate ligament reconstruction: The importance of patient age and postoperative rehabilitation. Orthopaedic Journal of Sports Medicine. 2018; 6(9):2325967118797575. [DOI:10.1177/2325967118797575] [PMID]
- Chicorelli AM, Micheli LJ, Kelly M, Zurakowski D, MacDougall R. Return to sport after anterior cruciate ligament reconstruction in the skeletally immature athlete. Clinical Journal of Sport Medicine. 2016; 26(4):266-271. [DOI:10.1097/JSM.0000000000000275] [PMID]
- Webster KE, Feller JA. Who passes return-to-sport tests, and which tests are most strongly associated with return to play after anterior cruciate ligament reconstruction? Orthopaedic Journal of Sports Medicine. 2020; 8(12):2325967120969425. [DOI:10.1177/2325967120969425] [PMID]
Article type: Reviews |
Subject:
Sport rehabilitation
Received: 2023/02/26 | Accepted: 2023/09/5 | Published: 2025/06/1
Received: 2023/02/26 | Accepted: 2023/09/5 | Published: 2025/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
