
988368
Tue, Jul 14, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 1-12 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gandhi D B C, Sebastian I A, Mahmood A, Nayak P, Makkar M, Dawar D, et al . Investigating the Unmet Need and Future of Neurorehabilitation in India: A Scoping Review. Iranian Rehabilitation Journal 2025; 23 (1) :1-12
URL: http://irj.uswr.ac.ir/article-1-1937-en.html
URL: http://irj.uswr.ac.ir/article-1-1937-en.html
Dorcas B C Gandhi *1 

 , Ivy A Sebastian2 , Amreen Mahmood3 , Pradeepa Nayak3 , Mridul Makkar4 , Dimple Dawar5 , Nistara S Chawla5 , Jeyaraj Durai Pandian5
, Ivy A Sebastian2 , Amreen Mahmood3 , Pradeepa Nayak3 , Mridul Makkar4 , Dimple Dawar5 , Nistara S Chawla5 , Jeyaraj Durai Pandian5
, Ivy A Sebastian2 , Amreen Mahmood3 , Pradeepa Nayak3 , Mridul Makkar4 , Dimple Dawar5 , Nistara S Chawla5 , Jeyaraj Durai Pandian5
1- Department of Neurology, College of Physiotherapy, Christian Medical College & Hospital, Ludhiana, India.
2- Department of Neurology, St Stephens Hospital, New Delhi, India.
3- Department of Physiotherapy, Kasturba Medical College, Mangalore, India.
4- Department of Clinical Haematology, Christian Medical College & Hospital, Ludhiana, India.
5- Department of Neurology, Christian Medical College and Hospital, Ludhiana, India.
2- Department of Neurology, St Stephens Hospital, New Delhi, India.
3- Department of Physiotherapy, Kasturba Medical College, Mangalore, India.
4- Department of Clinical Haematology, Christian Medical College & Hospital, Ludhiana, India.
5- Department of Neurology, Christian Medical College and Hospital, Ludhiana, India.
Keywords: Neurorehabilitation, Neurological disorders, Burden, Prevalence, Disability, Health care models, Neurological services
Full-Text [PDF 823 kb]
(1638 Downloads)
| Abstract (HTML) (4350 Views)
Full-Text: (804 Views)
Introduction
It has been estimated that 1 in 7 people worldwide are living with a disability equating to 15% of the world’s population [1]. In the 2017 report by the Global Burden of Disease (GBD), low-and-middle-income countries (LMIC) have shown a 90.4% growth in their disability-adjusted life years; however, only 5.5% benefitted from physical rehabilitation in these 28 years (1990-2017) [2]. There are around 2.45 billion people needing rehabilitation which raises a counterargument against the common view that only a few require it [3]. Neurological disorders were identified as the third largest group with the highest contribution to prevalence in which stroke represented the greatest need. Meanwhile, 89.0% of stroke-related disability-adjusted life years happened in upper-middle-income and low-income nations, according to GBD 2019 [4]. Neurorehabilitation services are much needed in India, as in other LMICs, but the obstacles to providing them are specific to the Indian subcontinent [5].
In this review, we intend to discuss challenges in meeting the physical neurorehabilitation needs specific to India. According to the United Nations Millennium Development Goals, this is in keeping with the objectives of promoting the rights of people with disabilities, empowering them economically and socially and encouraging their active involvement [6]. Patients with neurological illnesses, particularly those residing in LMICs, face inequities in access to treatment and inadequate resources, according to the World Health Organization (WHO) [7]. Accordingly, there has to be a greater emphasis on the need for first-level and referral health institutions providing neurological treatment, as well as a heightened public and professional awareness of the worldwide burden [8]. With this background it is essential to understand country-specific challenges in meeting the neurorehabilitation needs and to strategize development and implementation of models of care essential for the same. We have defined neurorehabilitation as the delivery of a coordinated interdisciplinary care program comprising a set of measures that assist individuals who experience (or are likely to experience) disability to achieve and maintain optimal function in interaction with their environment [1].
Hence, the objectives of this study are to explore the barriers to implementing physical neurorehabilitation at in-hospital and community levels in India, to summarize the unmet needs of evidence-based physical neurorehabilitation in India and to explore the potential models/services that can enhance the delivery of physical neurorehabilitation in India.
Materials and Methods
The reporting of this scoping review is done following the preferred reporting items for systematic reviews and meta-analyses-scoping review reporting standard, which is described in detail below [9].
Identification and selection of trials
Two reviewers (Amreen Mahmood and Pradeepa Nayak) ran the online search in PubMed (2011 to 2021), EMBASE (2011 to 2021), Web of Science (2011 to 2021) and Cochrane (CENTRAL) databases for relevant studies. Search terms included keywords for different neurological disorders and conditions, physical rehabilitation, and India. Boolean operators, namely “OR” and “AND” were used in the search strategy. We used the search filter to include articles published in the English language and on human participants. Two independent reviewers (Mridul Makkar and Nistara S Chawla) screened the titles and abstracts of retrieved articles to identify pertinent studies. For full-text screening, the whole texts of pertinent, peer-reviewed publications were retrieved. The reference lists of the papers that were included were also searched for relevant studies. Disagreements or ambiguities for including any article were resolved by consensus after discussion with a third reviewer (Dorcas B C Gandhi). The following selection criteria were used to include or exclude a potential article.
Selection criteria
Articles were included if its participants suffered from any neurological disorders.
Study characteristics
Studies were included if they assessed the implementation of neurorehabilitation in India and were published between September 2011 and September 2021. The duration of studies was limited to the last ten years since a similar review was conducted by Mandaville Gourie-Devi previously. Studies that delivered or evaluated all components of physical neurorehabilitation (motor, sensory, functional/activities of daily living, occupational, recreational, physical activity, fatigue, speech-swallow) for all neurological conditions. All phases of neurorehabilitation (acute, subacute and chronic), at all levels of care primary/secondary/tertiary/home-based/community-based) were considered. Meanwhile, all types of articles were included such as scientific articles, chapters or books, registries, conference reports, editorials and any epidemiological data about neurorehabilitation in India.
Studies were excluded if they described non-physical components of neurorehabilitation, i.e. social, cognitive, psychological, visuo-perceptual or published in a language besides English or were opinion pieces or viewpoints or described rehabilitation for patients institutionalized in old-age homes, non-government organization, and so on.
Data extraction and analysis
Data extraction was performed by three reviewers (Dorcas B C Gandhi, Ivy A Sebastian and Dimple Dawar) to include information about the methods (i.e. design, participants, phase and type of intervention, rehab setting, physical domain of focus) and results (challenges in intervention delivery, advantages of intervention delivery, mention of a government policy or new program model, current needs for neurorehabilitation and other salient features relevant to the objective). The results were narratively synthesized and summarized under the subheadings of challenges in neurorehabilitation in India, current needs to improve neurorehabilitation in India, and potential models to improve neurorehabilitation delivery.
Results
We retrieved 713 articles (Figure 1) and after full-text screening included 28 studies for data extraction and synthesis (Table 1) based on the selection criteria.
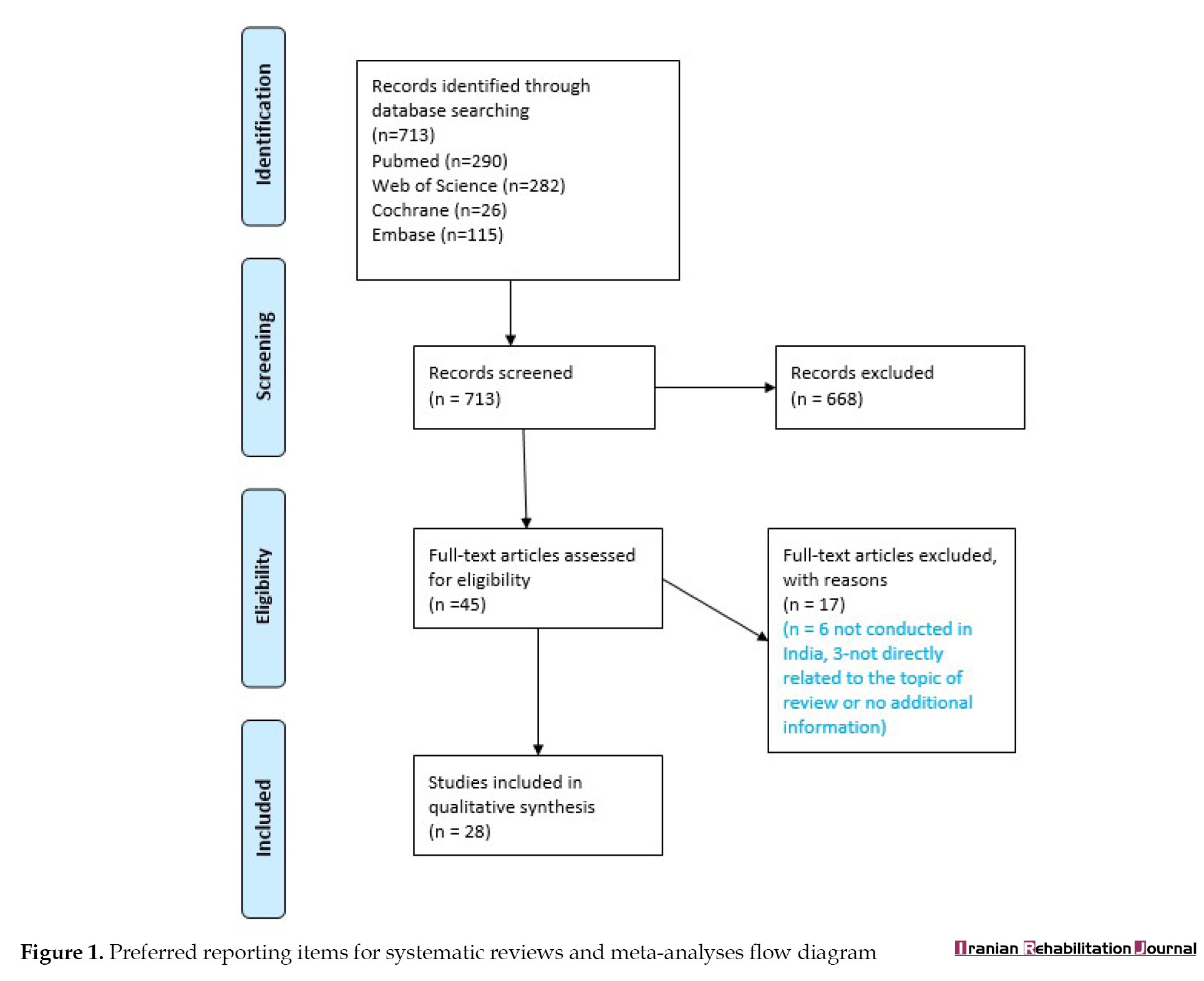
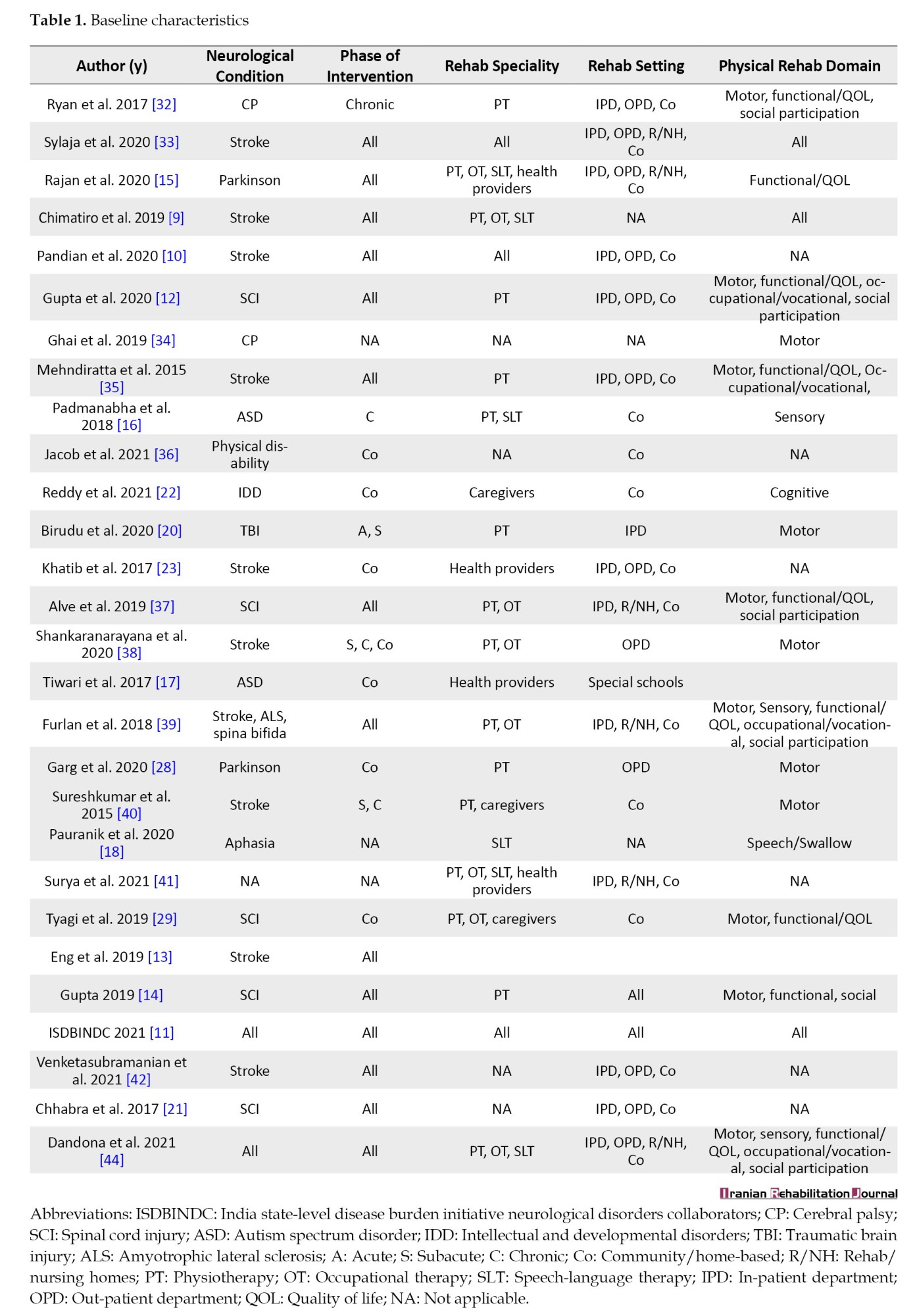
Of the included studies, 10 were on stroke, 5 on spinal cord injuries, 3 on autism spectrum disorders and the rest on cerebral palsy, traumatic brain injury, Parkinson, amyotrophic lateral sclerosis and Spina-Bifida. Meanwhile, two studies reported in general on those with neurological disorders causing physical disabilities. Most of the studies dealt with an adult population (>18 years of age) except for 6 studies that were on the pediatric population. Of the included studies, 13 were reviews, 7 were surveys, 2 were case reports and one was a cross-sectional study, feasibility study, guidelines and meta-analysis.
The results are summarized under the three following main categories: Challenges in neurorehabilitation in India, unmet needs to improve neurorehabilitation in India; potential models to improve neurorehabilitation delivery.
Categories 1 and 2 were further subdivided into data relevant to a) Rehabilitation; b) Rehabilitation provision; c) Rehabilitation research and d) Socioeconomic challenges or needs. The data extracted under category 3 was furnished into 8 potential models of neurorehabilitation that may help bridge the gaps in the existing systems of neurorehabilitation in India.
Challenges in neurorehabilitation in India
In our findings the most significant challenges (Table 2) that multiple authors have reported, are limited or lack of access to professional rehabilitation services which led to patients not availing any therapy or avail services from alternate branches of medicine like homeopathy, ayurveda, massage therapy, etc.
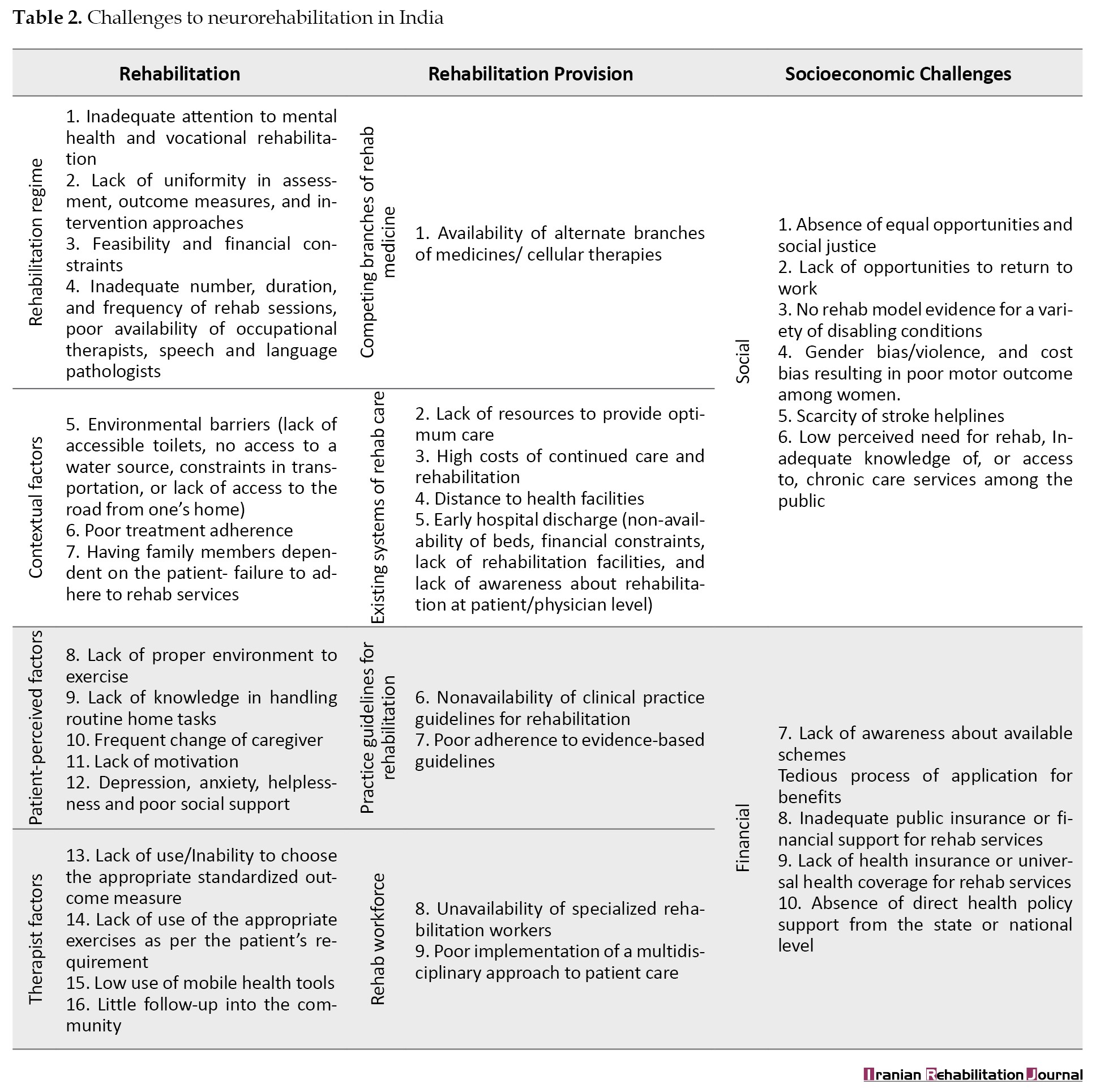
The various sociocultural beliefs among the Indian population facilitate social stigma attached to disability causing a percentage of the population to seek local god-men for functional recovery. Evidence-based rehabilitation is often the last priority and only if issues of accessibility, affordability, and the like are dealt with. Other significant challenges were the inability to provide adequate duration and intensity of rehabilitation, lack of proper environment for practicing achieved skills, poor adherence due to various factors, unavailability of occupational therapists, speech therapists commonly, lack of continued rehabilitation and supervision at patient homes after discharge and limited or almost nil focus of strengthening transitions in care with little follow-up of patients into the community and their social reintegration.
Challenges were also faced by the rehabilitation workforce, the numbers of whom are much less compared to those needing neurorehabilitation [10]. Studies have reported a vast percentage of unskilled professionals to handle neurorehabilitation in all phases of care (acute, subacute and chronic) [10-12]. Therapists have reported a lack of availability of standardized rehabilitation protocols for various neurological conditions like spinal cord injuries and Parkinson disease, lack of access to comprehensive clinical practice guidelines and [13] poor understanding of choice of suitable outcome measures [14, 15]. Even those with good expertise in neurorehabilitation do not find the opportunities to be part of multidisciplinary teams in corporate or public sector hospitals or primary health centers. Most hospitals do not incorporate advanced rehabilitation care in their care-delivery systems [10, 16]. Such challenges are also seen in primary and district health centers where a skilled rehabilitation workforce is a need, especially considering the strong need for continued therapy and supervision in the community of patients [17].
Unmet needs to improve neurorehabilitation in India
In line with the challenges, various needs (Table 3) highlighted were collaborative efforts by a multidisciplinary team (MDT) to promote functional improvement as well as vocational and social re-integration, use of trained non-rehab workforce to deliver and supervise rehabilitation at home/community levels, development of region-specific rehabilitation delivery models to cater to the considerable inter-state heterogeneity in disease burden and health-seeking behavior, [18-20] building capacity among rehabilitation professionals, non-rehabilitation workforce and caregivers apart from public awareness programs and policies to drive the importance of long-term continued and supervised neurorehabilitation and focus on empowering the public to understand the physiology behind recovery and early detection and accessing rehabilitation care [14, 21, 22].
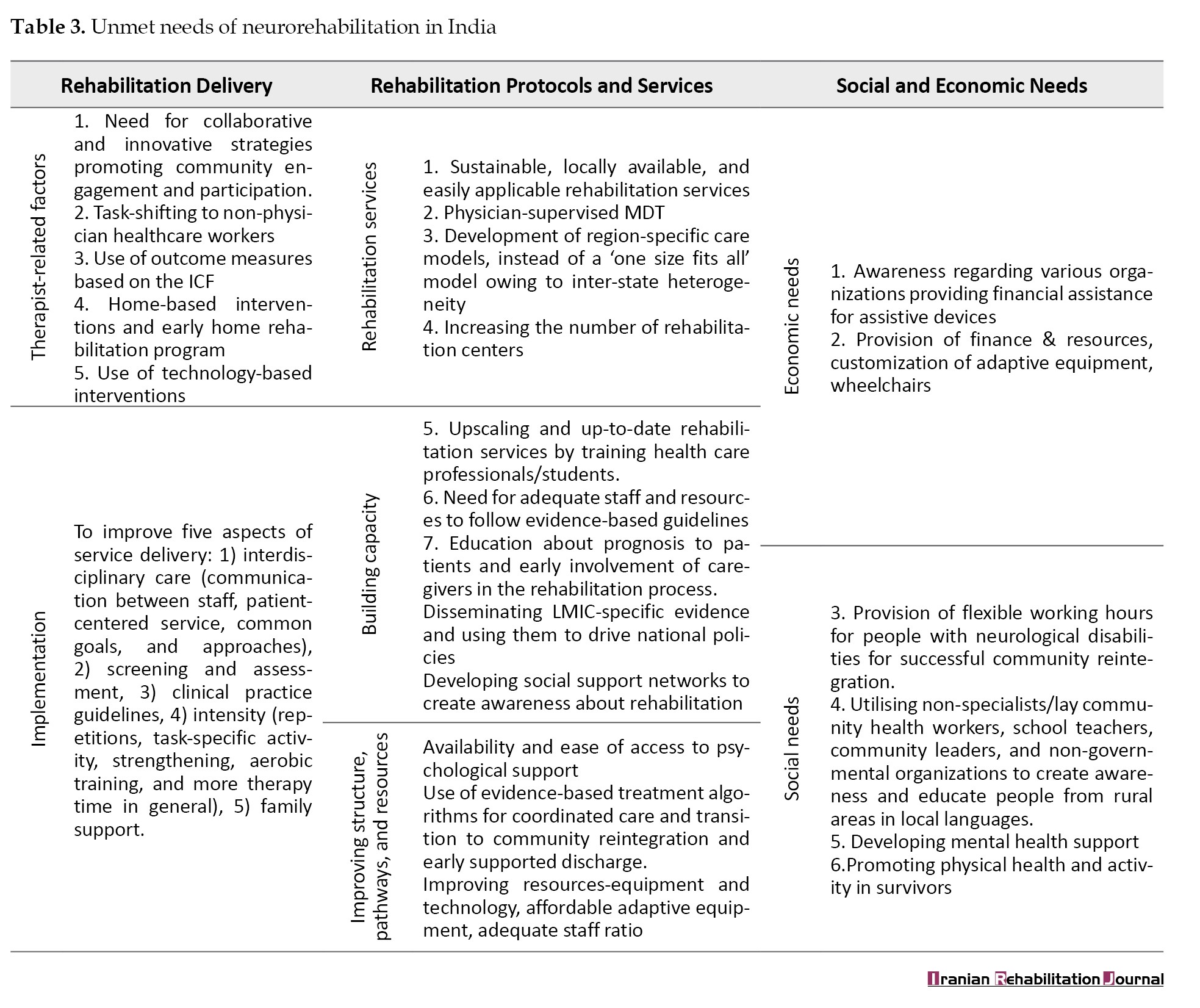
There is also a strong need for rehabilitation professionals to coordinate with other stakeholders like non-governmental organizations, government sectors taking disability-related policies, police, rehabilitation centers, community health volunteers, etc [23]. Non-specialist or lay community health workers, school teachers, and local leaders can all be successfully engaged in strengthening rehabilitation delivery and improve awareness among the public which would, in turn, facilitate positive health-seeking behavior and early identification of rehabilitation needs in patients [12] Coordinated transfer of care from hospital to community is another essential area to be developed in India [24]. In addition, there is a need to improve resources like rehabilitation space, equipment, technology to improve the intensity of rehabilitation, staffing, appropriate allocation of resources, and sufficient funding for all of the above [14].
Rehabilitation delivery encompasses various factors, such as multidisciplinary care, integrating different approaches, choosing between home-based or hospital-based care, utilizing technology and adherence to clinical practice guidelines. The administration of rehabilitation services and programs is entwined with a country’s healthcare infrastructure. This involves taking into account factors like the structuring and coordination of care, the accessibility of a qualified workforce, the creation of efficient health pathways and the distribution of suitable resources. These elements are essential to guarantee the availability, effectiveness and high caliber of rehabilitation services. Improving the state of rehabilitation-related research in the Indian subcontinent requires a major emphasis on promoting several aspects, such as improving study designs, raising the bar for methodological rigor and reporting requirements, analyzing cost-effectiveness, gauging the degree of interdisciplinary collaboration between healthcare providers and assessing the effectiveness of home-based rehabilitation programs [5, 11, 14].
Potential models to improve neurorehabilitation delivery
Various alternative models of rehabilitation have been studied previously in different neurological conditions with evidence of efficacy. Based on the needs identified from our study and the available literature, we have adapted 8 alternative models of rehabilitation delivery that have demonstrated evidence of effectiveness in low-resourced settings such as India (Figure 2).
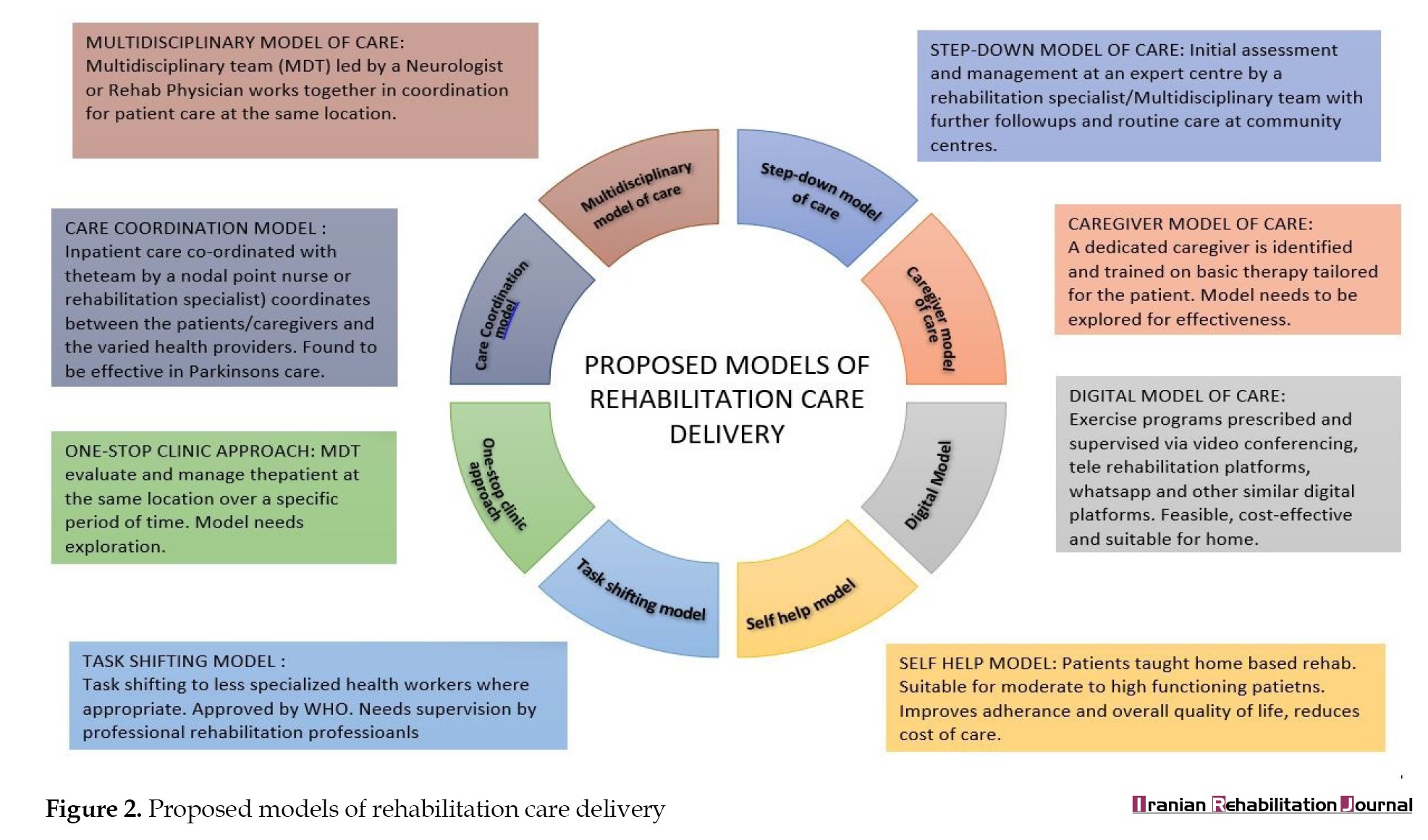 Multidisciplinary care model: The multidisciplinary model has been studied in patients with stroke, Parkinson disease, autism, cerebral palsy and spinal cord injuries and in place of its effectiveness has been incorporated as an essential component of clinical practice guidelines for various neurological conditions. However, its implementation in India is challenging, with multifactorial causes ranging from unavailability of sufficient rehab professionals and lack of awareness among neurologists/physicians, to funding issues and lack of appropriate staffing guidelines [11].
Multidisciplinary care model: The multidisciplinary model has been studied in patients with stroke, Parkinson disease, autism, cerebral palsy and spinal cord injuries and in place of its effectiveness has been incorporated as an essential component of clinical practice guidelines for various neurological conditions. However, its implementation in India is challenging, with multifactorial causes ranging from unavailability of sufficient rehab professionals and lack of awareness among neurologists/physicians, to funding issues and lack of appropriate staffing guidelines [11].
Step-down care model: The step-down care model entails initial assessment and management at an expert center by a rehabilitation specialist/multidisciplinary team followed by further follow-ups and routine care at community centers. Communication between the MDT and community level is maintained through an integrated network of professionals [25].
Care-coordination model: An in-patient model of care-coordination (found to be effective in those with Parkinson disease) [16] could also be useful in neurorehabilitation where a nodal point-of-contact (nurse or rehabilitation specialist) coordinates between the patients/caregivers and the varied health providers. This would not just eliminate the need for the whole MDT to be present at the same place and same time but also expedite and simplify the consultation process for the patients. However, this model like the multidisciplinary model of care, needs periodic MDT meetings to share information and common goals for patient recovery. Additional facilitation via information technology-based support may be of use [16].
One-stop clinic model: The one-stop clinic model of care allows for members of the MDT to gather together and evaluate and manage patients at the same location over a pre-specified period. This model can be adapted where MDT specialists can be available at the same location on pre-decided days/times for patients to access these services. This model also needs to be explored on a variety of neurological conditions and will need sufficient funding [16].
Task-shifting model: The task-shifting model is yet another evidence-based model of care that has been adopted by many LMICs where the task is delegated to less specialized health workers. One such example is found in Malawi, South East Africa, where community health workers were exposed to a rehabilitation training program over 5 years and significant improvements were found in their knowledge, skill, and competency to implement patient care [26]. Similarly in Punjab, India Accredited social health activist were trained to identify stroke cases in the community [27]. In Jharkhand, India a four-staged treatment delivery model was implemented via voluntary health workers for those with epilepsy in tribal areas. This example too resulted in trained volunteers influencing people to seek treatment for the same [12]. The task-shifting model is encouraged by the WHO among other international bodies.
Self-help/home-based model: The self-help/home-based model of care can lower healthcare costs, increase treatment compliance and enhance general quality of life. However, such programs must include evaluation and modification of environmental hazards, regular supervision and coaching, follow-up and feedback from the rehabilitation professionals. For patients with low levels of functioning, and requiring constant medical care, this model may not be suitable [28].
Digital model: A vast range of implementation systems where exercise programs can be prescribed and supervised via video-conferencing, official telerehabilitation platforms, WhatsApp and other similar digital platforms have been explored in the recent few years with adequate acceptability and efficacy [29, 30]. For instance, a home-based sensory intervention model where pre-decided exercises were prescribed, followed by weekly telephonic reinforcement and review of videotapes of home activities was found to be a feasible and cost-effective model among children with sensory issues [17].
Caregiver-led model: Lastly we describe the caregiver-led model of care where a dedicated caregiver is identified and trained on basic therapy tailored for the patient. Through the attend [31] and recover [32] trials, this model of care was found to have various loopholes, the major drawback being frequently changing caregivers and lack of continued supervision by professional physiotherapists [30]. More research would be needed for modified caregiver models, especially because such models were found to be safe, feasible, and satisfactory to all stakeholders involved.
While the efficacy of these adapted models has been studied, there is a need for further exploration of these systems at a larger scale and in more diverse groups of patients with neurological diseases.
Discussion
The present state of affairs of neurorehabilitation in India is far from being adequate. This review attempts to throw light on the various unmet needs to improving Neurorehabilitation in India and propose adaptations for low-resourced settings such as ours. There is a flagrant imbalance between the existing burden of disability and the availability of and accessibility to resources and skilled multidisciplinary professionals in the country. The inadequate numbers of rehabilitation professionals, the poor accessibility to existent services, in addition to the gross rural-urban divide are some of the barriers to the provision of uniform and equitable multidisciplinary services across the country. Another unique but serious challenge our study yielded was the glaring gender discrepancy within the country in availing rehabilitation services. Women with disabilities rarely avail of rehabilitation services and only for a limited duration if at all, compared to men. Improving awareness among women and men, and providing opportunities for equal accessibility to care is essential. Accessibility to care can be improved by providing more rehabilitation services at the community level making access easier for women who may tend to be neglected by the family. Government schemes or programs for free or subsidized rehabilitation facilities for women need to be advocated.
There is a pressing need to develop standardized, accredited, and scalable training programs for rehabilitation professionals, registered with national bodies and councils for accountability. Periodic, formal upgradation of knowledge and skills should be undertaken from basic to advanced education levels with license exams and certifications to update and maintain the competency levels. Introducing a culture of research early into the educational curriculum will cultivate the temperament and attitude of implementing evidence-based practices among young professionals.
Several trials have explored the feasibility of alternate models of care for neuro-rehabilitation. The current models of neuro-rehab in India, include home-based care-giver-led models and telerehabilitation through WhatsApp or Zoom calls or exercise apps. The landmark attend trial (family-led rehabilitation after stroke in India: A randomized controlled trial) [31] did not find the home-based caregiver rehab model to be superior to routine care, however, such a model was safe and accepted by the patients and their caregivers. Exploring modified models of home-based care with periodic supervision by rehab professionals is a necessity. Similarly, technology-based rehab models like in the “care for u” study, did not find in-hospital game-based rehab to be feasible as most patients were unwilling and or unable to travel to the hospital for regular sessions. Application-based rehab delivery is another mode that is widely being researched [41]. Most of these apps are either not culturally specific or do not cater to impairments of all domains (motor, sensory, cognition, gait, etc). Socio-cultural and language-specific modifications are needed in such platforms.
While there is evidence for the efficacy of these proposed models, exploring these systems in more diverse groups of population is imperative to establish their effectiveness. It is important to note that these models of care are not mutually exclusive, but rather complimentary, and institutions of medical and rehabilitative care may need to utilize multiple such models to effectively deliver optimal rehabilitation services.
Recognizing the enormous burden of neurological disorders and the disability attributed to them as a public health problem is the first step towards alleviating the current situation in our country. Mobilizing the support of stakeholders, health planners and administrators, while also advocating for the value and role of rehabilitation among nongovernmental organizations is a principal component towards advancing the rehabilitation service provision within the country. In addition, there is also a need for improved data collection and reporting to better inform policy development.
Strengths of the present study
This study provided many examples of alternative rehabilitation models that have been explored and studied in different neurological conditions. Based on the myriad unmet needs and challenges identified in the study, the authors have proposed 8 alternative models of rehabilitation provision adapted from the previously studied model in the literature. Ranging from the multidisciplinary care model which involves the entire MDT actively involved in decision-making and care of the patient, to the task-shifting model and the caregiver-led model where other professionals or caregivers have delegated the task of care delivery, and finally to the self-help model where patient themselves are empowered, these models provide potential alternatives to rehabilitation service delivery in settings such as India where the need is over and above the availability.
Conclusion
Many different social and cultural traditions coexist in India. Due to the wide variety of problems and requirements in rehabilitation services in India, there is no universally applicable method. We have categorized the many unfulfilled neurorehabilitation requirements and obstacles to their implementation in our nation. Various alternative care models seem to have a good chance of succeeding in the future, despite the obstacles. Some basic steps towards progress include raising public awareness, enhancing the skills of current experts, and encouraging proactive engagement from state and federal governments and other interested parties. An integrated approach, whilst prioritizing the elements that will provide the most benefit is the need of the hour.
Concerning research, future researchers could focus on implementation studies of established interventions to improve the delivery of neurorehabilitation. In addition, there is a need to systematically develop condition-specific and regionally relevant clinical practice guidelines that may be more meaningful to users and improve functional outcomes. We also suggest using the co-design approach while conducting neurorehabilitation trials where all relevant stakeholders (patients, caregivers, policymakers, administrators, rehab and medical professionals, social workers, etc.) are involved in planning, implementing/conducting, and disseminating trials and their results. This would allow the development of comprehensive solutions targeted at specific needs with a holistic view of the whole team.
Limitations of the present study
This scoping review is limited in its scope for not including exact mechanisms and causes of the unmet needs and challenges. Although the paper describes various challenges, it does not provide details on the governmental policies or regulations and their merits/demerits that could address such challenges. The comprehensive searches on multiple databases did not search for information on national schemes for those with disabilities due to neurological conditions as the authors believe that such a section is beyond the scope of this paper. Lastly, the solutions provided in the form of probable models of care are general models and not condition-specific.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception, design, data collection, interpretation of results, and manuscript preparation. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
It has been estimated that 1 in 7 people worldwide are living with a disability equating to 15% of the world’s population [1]. In the 2017 report by the Global Burden of Disease (GBD), low-and-middle-income countries (LMIC) have shown a 90.4% growth in their disability-adjusted life years; however, only 5.5% benefitted from physical rehabilitation in these 28 years (1990-2017) [2]. There are around 2.45 billion people needing rehabilitation which raises a counterargument against the common view that only a few require it [3]. Neurological disorders were identified as the third largest group with the highest contribution to prevalence in which stroke represented the greatest need. Meanwhile, 89.0% of stroke-related disability-adjusted life years happened in upper-middle-income and low-income nations, according to GBD 2019 [4]. Neurorehabilitation services are much needed in India, as in other LMICs, but the obstacles to providing them are specific to the Indian subcontinent [5].
In this review, we intend to discuss challenges in meeting the physical neurorehabilitation needs specific to India. According to the United Nations Millennium Development Goals, this is in keeping with the objectives of promoting the rights of people with disabilities, empowering them economically and socially and encouraging their active involvement [6]. Patients with neurological illnesses, particularly those residing in LMICs, face inequities in access to treatment and inadequate resources, according to the World Health Organization (WHO) [7]. Accordingly, there has to be a greater emphasis on the need for first-level and referral health institutions providing neurological treatment, as well as a heightened public and professional awareness of the worldwide burden [8]. With this background it is essential to understand country-specific challenges in meeting the neurorehabilitation needs and to strategize development and implementation of models of care essential for the same. We have defined neurorehabilitation as the delivery of a coordinated interdisciplinary care program comprising a set of measures that assist individuals who experience (or are likely to experience) disability to achieve and maintain optimal function in interaction with their environment [1].
Hence, the objectives of this study are to explore the barriers to implementing physical neurorehabilitation at in-hospital and community levels in India, to summarize the unmet needs of evidence-based physical neurorehabilitation in India and to explore the potential models/services that can enhance the delivery of physical neurorehabilitation in India.
Materials and Methods
The reporting of this scoping review is done following the preferred reporting items for systematic reviews and meta-analyses-scoping review reporting standard, which is described in detail below [9].
Identification and selection of trials
Two reviewers (Amreen Mahmood and Pradeepa Nayak) ran the online search in PubMed (2011 to 2021), EMBASE (2011 to 2021), Web of Science (2011 to 2021) and Cochrane (CENTRAL) databases for relevant studies. Search terms included keywords for different neurological disorders and conditions, physical rehabilitation, and India. Boolean operators, namely “OR” and “AND” were used in the search strategy. We used the search filter to include articles published in the English language and on human participants. Two independent reviewers (Mridul Makkar and Nistara S Chawla) screened the titles and abstracts of retrieved articles to identify pertinent studies. For full-text screening, the whole texts of pertinent, peer-reviewed publications were retrieved. The reference lists of the papers that were included were also searched for relevant studies. Disagreements or ambiguities for including any article were resolved by consensus after discussion with a third reviewer (Dorcas B C Gandhi). The following selection criteria were used to include or exclude a potential article.
Selection criteria
Articles were included if its participants suffered from any neurological disorders.
Study characteristics
Studies were included if they assessed the implementation of neurorehabilitation in India and were published between September 2011 and September 2021. The duration of studies was limited to the last ten years since a similar review was conducted by Mandaville Gourie-Devi previously. Studies that delivered or evaluated all components of physical neurorehabilitation (motor, sensory, functional/activities of daily living, occupational, recreational, physical activity, fatigue, speech-swallow) for all neurological conditions. All phases of neurorehabilitation (acute, subacute and chronic), at all levels of care primary/secondary/tertiary/home-based/community-based) were considered. Meanwhile, all types of articles were included such as scientific articles, chapters or books, registries, conference reports, editorials and any epidemiological data about neurorehabilitation in India.
Studies were excluded if they described non-physical components of neurorehabilitation, i.e. social, cognitive, psychological, visuo-perceptual or published in a language besides English or were opinion pieces or viewpoints or described rehabilitation for patients institutionalized in old-age homes, non-government organization, and so on.
Data extraction and analysis
Data extraction was performed by three reviewers (Dorcas B C Gandhi, Ivy A Sebastian and Dimple Dawar) to include information about the methods (i.e. design, participants, phase and type of intervention, rehab setting, physical domain of focus) and results (challenges in intervention delivery, advantages of intervention delivery, mention of a government policy or new program model, current needs for neurorehabilitation and other salient features relevant to the objective). The results were narratively synthesized and summarized under the subheadings of challenges in neurorehabilitation in India, current needs to improve neurorehabilitation in India, and potential models to improve neurorehabilitation delivery.
Results
We retrieved 713 articles (Figure 1) and after full-text screening included 28 studies for data extraction and synthesis (Table 1) based on the selection criteria.
Of the included studies, 10 were on stroke, 5 on spinal cord injuries, 3 on autism spectrum disorders and the rest on cerebral palsy, traumatic brain injury, Parkinson, amyotrophic lateral sclerosis and Spina-Bifida. Meanwhile, two studies reported in general on those with neurological disorders causing physical disabilities. Most of the studies dealt with an adult population (>18 years of age) except for 6 studies that were on the pediatric population. Of the included studies, 13 were reviews, 7 were surveys, 2 were case reports and one was a cross-sectional study, feasibility study, guidelines and meta-analysis.
The results are summarized under the three following main categories: Challenges in neurorehabilitation in India, unmet needs to improve neurorehabilitation in India; potential models to improve neurorehabilitation delivery.
Categories 1 and 2 were further subdivided into data relevant to a) Rehabilitation; b) Rehabilitation provision; c) Rehabilitation research and d) Socioeconomic challenges or needs. The data extracted under category 3 was furnished into 8 potential models of neurorehabilitation that may help bridge the gaps in the existing systems of neurorehabilitation in India.
Challenges in neurorehabilitation in India
In our findings the most significant challenges (Table 2) that multiple authors have reported, are limited or lack of access to professional rehabilitation services which led to patients not availing any therapy or avail services from alternate branches of medicine like homeopathy, ayurveda, massage therapy, etc.
The various sociocultural beliefs among the Indian population facilitate social stigma attached to disability causing a percentage of the population to seek local god-men for functional recovery. Evidence-based rehabilitation is often the last priority and only if issues of accessibility, affordability, and the like are dealt with. Other significant challenges were the inability to provide adequate duration and intensity of rehabilitation, lack of proper environment for practicing achieved skills, poor adherence due to various factors, unavailability of occupational therapists, speech therapists commonly, lack of continued rehabilitation and supervision at patient homes after discharge and limited or almost nil focus of strengthening transitions in care with little follow-up of patients into the community and their social reintegration.
Challenges were also faced by the rehabilitation workforce, the numbers of whom are much less compared to those needing neurorehabilitation [10]. Studies have reported a vast percentage of unskilled professionals to handle neurorehabilitation in all phases of care (acute, subacute and chronic) [10-12]. Therapists have reported a lack of availability of standardized rehabilitation protocols for various neurological conditions like spinal cord injuries and Parkinson disease, lack of access to comprehensive clinical practice guidelines and [13] poor understanding of choice of suitable outcome measures [14, 15]. Even those with good expertise in neurorehabilitation do not find the opportunities to be part of multidisciplinary teams in corporate or public sector hospitals or primary health centers. Most hospitals do not incorporate advanced rehabilitation care in their care-delivery systems [10, 16]. Such challenges are also seen in primary and district health centers where a skilled rehabilitation workforce is a need, especially considering the strong need for continued therapy and supervision in the community of patients [17].
Unmet needs to improve neurorehabilitation in India
In line with the challenges, various needs (Table 3) highlighted were collaborative efforts by a multidisciplinary team (MDT) to promote functional improvement as well as vocational and social re-integration, use of trained non-rehab workforce to deliver and supervise rehabilitation at home/community levels, development of region-specific rehabilitation delivery models to cater to the considerable inter-state heterogeneity in disease burden and health-seeking behavior, [18-20] building capacity among rehabilitation professionals, non-rehabilitation workforce and caregivers apart from public awareness programs and policies to drive the importance of long-term continued and supervised neurorehabilitation and focus on empowering the public to understand the physiology behind recovery and early detection and accessing rehabilitation care [14, 21, 22].
There is also a strong need for rehabilitation professionals to coordinate with other stakeholders like non-governmental organizations, government sectors taking disability-related policies, police, rehabilitation centers, community health volunteers, etc [23]. Non-specialist or lay community health workers, school teachers, and local leaders can all be successfully engaged in strengthening rehabilitation delivery and improve awareness among the public which would, in turn, facilitate positive health-seeking behavior and early identification of rehabilitation needs in patients [12] Coordinated transfer of care from hospital to community is another essential area to be developed in India [24]. In addition, there is a need to improve resources like rehabilitation space, equipment, technology to improve the intensity of rehabilitation, staffing, appropriate allocation of resources, and sufficient funding for all of the above [14].
Rehabilitation delivery encompasses various factors, such as multidisciplinary care, integrating different approaches, choosing between home-based or hospital-based care, utilizing technology and adherence to clinical practice guidelines. The administration of rehabilitation services and programs is entwined with a country’s healthcare infrastructure. This involves taking into account factors like the structuring and coordination of care, the accessibility of a qualified workforce, the creation of efficient health pathways and the distribution of suitable resources. These elements are essential to guarantee the availability, effectiveness and high caliber of rehabilitation services. Improving the state of rehabilitation-related research in the Indian subcontinent requires a major emphasis on promoting several aspects, such as improving study designs, raising the bar for methodological rigor and reporting requirements, analyzing cost-effectiveness, gauging the degree of interdisciplinary collaboration between healthcare providers and assessing the effectiveness of home-based rehabilitation programs [5, 11, 14].
Potential models to improve neurorehabilitation delivery
Various alternative models of rehabilitation have been studied previously in different neurological conditions with evidence of efficacy. Based on the needs identified from our study and the available literature, we have adapted 8 alternative models of rehabilitation delivery that have demonstrated evidence of effectiveness in low-resourced settings such as India (Figure 2).
Step-down care model: The step-down care model entails initial assessment and management at an expert center by a rehabilitation specialist/multidisciplinary team followed by further follow-ups and routine care at community centers. Communication between the MDT and community level is maintained through an integrated network of professionals [25].
Care-coordination model: An in-patient model of care-coordination (found to be effective in those with Parkinson disease) [16] could also be useful in neurorehabilitation where a nodal point-of-contact (nurse or rehabilitation specialist) coordinates between the patients/caregivers and the varied health providers. This would not just eliminate the need for the whole MDT to be present at the same place and same time but also expedite and simplify the consultation process for the patients. However, this model like the multidisciplinary model of care, needs periodic MDT meetings to share information and common goals for patient recovery. Additional facilitation via information technology-based support may be of use [16].
One-stop clinic model: The one-stop clinic model of care allows for members of the MDT to gather together and evaluate and manage patients at the same location over a pre-specified period. This model can be adapted where MDT specialists can be available at the same location on pre-decided days/times for patients to access these services. This model also needs to be explored on a variety of neurological conditions and will need sufficient funding [16].
Task-shifting model: The task-shifting model is yet another evidence-based model of care that has been adopted by many LMICs where the task is delegated to less specialized health workers. One such example is found in Malawi, South East Africa, where community health workers were exposed to a rehabilitation training program over 5 years and significant improvements were found in their knowledge, skill, and competency to implement patient care [26]. Similarly in Punjab, India Accredited social health activist were trained to identify stroke cases in the community [27]. In Jharkhand, India a four-staged treatment delivery model was implemented via voluntary health workers for those with epilepsy in tribal areas. This example too resulted in trained volunteers influencing people to seek treatment for the same [12]. The task-shifting model is encouraged by the WHO among other international bodies.
Self-help/home-based model: The self-help/home-based model of care can lower healthcare costs, increase treatment compliance and enhance general quality of life. However, such programs must include evaluation and modification of environmental hazards, regular supervision and coaching, follow-up and feedback from the rehabilitation professionals. For patients with low levels of functioning, and requiring constant medical care, this model may not be suitable [28].
Digital model: A vast range of implementation systems where exercise programs can be prescribed and supervised via video-conferencing, official telerehabilitation platforms, WhatsApp and other similar digital platforms have been explored in the recent few years with adequate acceptability and efficacy [29, 30]. For instance, a home-based sensory intervention model where pre-decided exercises were prescribed, followed by weekly telephonic reinforcement and review of videotapes of home activities was found to be a feasible and cost-effective model among children with sensory issues [17].
Caregiver-led model: Lastly we describe the caregiver-led model of care where a dedicated caregiver is identified and trained on basic therapy tailored for the patient. Through the attend [31] and recover [32] trials, this model of care was found to have various loopholes, the major drawback being frequently changing caregivers and lack of continued supervision by professional physiotherapists [30]. More research would be needed for modified caregiver models, especially because such models were found to be safe, feasible, and satisfactory to all stakeholders involved.
While the efficacy of these adapted models has been studied, there is a need for further exploration of these systems at a larger scale and in more diverse groups of patients with neurological diseases.
Discussion
The present state of affairs of neurorehabilitation in India is far from being adequate. This review attempts to throw light on the various unmet needs to improving Neurorehabilitation in India and propose adaptations for low-resourced settings such as ours. There is a flagrant imbalance between the existing burden of disability and the availability of and accessibility to resources and skilled multidisciplinary professionals in the country. The inadequate numbers of rehabilitation professionals, the poor accessibility to existent services, in addition to the gross rural-urban divide are some of the barriers to the provision of uniform and equitable multidisciplinary services across the country. Another unique but serious challenge our study yielded was the glaring gender discrepancy within the country in availing rehabilitation services. Women with disabilities rarely avail of rehabilitation services and only for a limited duration if at all, compared to men. Improving awareness among women and men, and providing opportunities for equal accessibility to care is essential. Accessibility to care can be improved by providing more rehabilitation services at the community level making access easier for women who may tend to be neglected by the family. Government schemes or programs for free or subsidized rehabilitation facilities for women need to be advocated.
There is a pressing need to develop standardized, accredited, and scalable training programs for rehabilitation professionals, registered with national bodies and councils for accountability. Periodic, formal upgradation of knowledge and skills should be undertaken from basic to advanced education levels with license exams and certifications to update and maintain the competency levels. Introducing a culture of research early into the educational curriculum will cultivate the temperament and attitude of implementing evidence-based practices among young professionals.
Several trials have explored the feasibility of alternate models of care for neuro-rehabilitation. The current models of neuro-rehab in India, include home-based care-giver-led models and telerehabilitation through WhatsApp or Zoom calls or exercise apps. The landmark attend trial (family-led rehabilitation after stroke in India: A randomized controlled trial) [31] did not find the home-based caregiver rehab model to be superior to routine care, however, such a model was safe and accepted by the patients and their caregivers. Exploring modified models of home-based care with periodic supervision by rehab professionals is a necessity. Similarly, technology-based rehab models like in the “care for u” study, did not find in-hospital game-based rehab to be feasible as most patients were unwilling and or unable to travel to the hospital for regular sessions. Application-based rehab delivery is another mode that is widely being researched [41]. Most of these apps are either not culturally specific or do not cater to impairments of all domains (motor, sensory, cognition, gait, etc). Socio-cultural and language-specific modifications are needed in such platforms.
While there is evidence for the efficacy of these proposed models, exploring these systems in more diverse groups of population is imperative to establish their effectiveness. It is important to note that these models of care are not mutually exclusive, but rather complimentary, and institutions of medical and rehabilitative care may need to utilize multiple such models to effectively deliver optimal rehabilitation services.
Recognizing the enormous burden of neurological disorders and the disability attributed to them as a public health problem is the first step towards alleviating the current situation in our country. Mobilizing the support of stakeholders, health planners and administrators, while also advocating for the value and role of rehabilitation among nongovernmental organizations is a principal component towards advancing the rehabilitation service provision within the country. In addition, there is also a need for improved data collection and reporting to better inform policy development.
Strengths of the present study
This study provided many examples of alternative rehabilitation models that have been explored and studied in different neurological conditions. Based on the myriad unmet needs and challenges identified in the study, the authors have proposed 8 alternative models of rehabilitation provision adapted from the previously studied model in the literature. Ranging from the multidisciplinary care model which involves the entire MDT actively involved in decision-making and care of the patient, to the task-shifting model and the caregiver-led model where other professionals or caregivers have delegated the task of care delivery, and finally to the self-help model where patient themselves are empowered, these models provide potential alternatives to rehabilitation service delivery in settings such as India where the need is over and above the availability.
Conclusion
Many different social and cultural traditions coexist in India. Due to the wide variety of problems and requirements in rehabilitation services in India, there is no universally applicable method. We have categorized the many unfulfilled neurorehabilitation requirements and obstacles to their implementation in our nation. Various alternative care models seem to have a good chance of succeeding in the future, despite the obstacles. Some basic steps towards progress include raising public awareness, enhancing the skills of current experts, and encouraging proactive engagement from state and federal governments and other interested parties. An integrated approach, whilst prioritizing the elements that will provide the most benefit is the need of the hour.
Concerning research, future researchers could focus on implementation studies of established interventions to improve the delivery of neurorehabilitation. In addition, there is a need to systematically develop condition-specific and regionally relevant clinical practice guidelines that may be more meaningful to users and improve functional outcomes. We also suggest using the co-design approach while conducting neurorehabilitation trials where all relevant stakeholders (patients, caregivers, policymakers, administrators, rehab and medical professionals, social workers, etc.) are involved in planning, implementing/conducting, and disseminating trials and their results. This would allow the development of comprehensive solutions targeted at specific needs with a holistic view of the whole team.
Limitations of the present study
This scoping review is limited in its scope for not including exact mechanisms and causes of the unmet needs and challenges. Although the paper describes various challenges, it does not provide details on the governmental policies or regulations and their merits/demerits that could address such challenges. The comprehensive searches on multiple databases did not search for information on national schemes for those with disabilities due to neurological conditions as the authors believe that such a section is beyond the scope of this paper. Lastly, the solutions provided in the form of probable models of care are general models and not condition-specific.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception, design, data collection, interpretation of results, and manuscript preparation. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- WHO. World report on disability. Geneva: World Health Organization; 2011. [Link]
- Jesus TS, Landry MD, Hoenig H. Global need for physical rehabilitation: Systematic analysis from the Global Burden of Disease Study 2017. International Journal of Environmental Research and Public Health. 2019; 16(6):980. [DOI:10.3390/ijerph16060980] [PMID]
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2021; 396(10267):2006-17. [DOI:10.1016/S0140-6736(20)32340-0] [PMID]
- Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet Neurology. 2021; 20(10):795-820. [Link]
- UN. Secretary-General. [Keeping the promise: realizing the Millennium Development Goals for persons with disabilities towards 2015 and beyond: Report of the Secretary-General (Arabic)] [Internet]. 2010. Available from: [Link]
- Janca A, Prilipko L, Costa e Silva JA. The World Health Organisation’s work on public health aspects of neurology. Journal of Neurology, Neurosurgery & Psychiatry. 1997; 63(S 1):6S-7. [DOI:10.1136/jnnp.63.2008.6S] [PMID]
- Khan F, Amatya B, Mannan H, Rathore FA. Neurorehabilitation in developing countries: Challenges and the way forward. Physical Medicine and Rehabilitation - International. 2015; 2(9):1070. [Link]
- Rocco MV, Sink KM, Lovato LC, Wolfgram DF, Wiegmann TB, Wall BM, et al. Effects of intensive blood pressure treatment on acute kidney injury events in the Systolic Blood Pressure Intervention Trial (SPRINT). American Journal of Kidney Diseases. 2018; 71(3):352-61. [doi:10.1053/j.ajkd.2017.08.021]
- Chimatiro GL, Rhoda AJ. Scoping review of acute stroke care management and rehabilitation in low and middle-income countries. BMC Health Services Research. 2019; 19(1):789. [DOI:10.1186/s12913-019-4654-4] [PMID]
- Pandian JD, Kalkonde Y, Sebastian IA, Felix C, Urimubenshi G, Bosch J. Stroke systems of care in low-income and middle-income countries: Challenges and opportunities. Lancet. 2020; 396(10260):1443-51. [DOI:10.1016/S0140-6736(20)31374-X] [PMID]
- India State-Level Disease Burden Initiative Neurological Disorders Collaborators. The burden of neurological disorders across the states of India: The Global Burden of Disease Study 1990-2019. The Lancet. Global Health. 2021; 9(8):e1129-44. [DOI:10.1016/S2214-109X(21)00164-9] [PMID] [PMCID]
- Gupta N. Recommendations for standards of physiotherapy care following complete traumatic paraplegia in India. Spinal Cord Series and Cases. 2020; 6(1):14. [DOI:10.1038/s41394-020-0263-z] [PMID]
- Eng JJ, Bird ML, Godecke E, Hoffmann TC, Laurin C, Olaoye OA, et al. Moving stroke rehabilitation research evidence into clinical practice: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. International journal of Stroke. 2019; 14(8):766-73. [DOI:10.1177/1747493019873597] [PMID]
- Gupta N. Lack of adequate care post spinal cord injury-A case report. Spinal Cord Series and Cases. 2019; 5:22. [DOI:10.1038/s41394-019-0163-2] [PMID]
- Rajan R, Brennan L, Bloem BR, Dahodwala N, Gardner J, Goldman JG, et al. Integrated care in Parkinson’s disease: A systematic review and meta-analysis. Movement Disorders. 2020; 35(9):1509-31. [DOI:10.1002/mds.28097] [PMID]
- Padmanabha H, Singhi P, Sahu JK, Malhi P. Home-based sensory interventions in children with autism spectrum disorder: A randomized controlled trial. Indian journal of pediatrics. 2019; 86(1):18-25. [DOI:10.1007/s12098-018-2747-4] [PMID]
- Tiwari S, John J. Special educators’ knowledge and training on autism in Karnataka: A cross-sectional study. Indian journal of psychiatry. 2017; 59(3):359-65. [DOI:10.4103/psychiatry.IndianJPsychiatry_133_17] [PMID]
- Pauranik A, Pauranik N, Singh P, Lahiri D, Krishnan G. Aphasia in neurology practice: A survey about perceptions and practices. Annals of Indian Academy of Neurology. 2020; 23(S 2):S162-70. [DOI:10.4103/aian.AIAN_788_20] [PMID]
- Parmar ST, Kanitkar A, Sepehri N, Bhairannawar S, Szturm T. Computer game-based telerehabilitation platform targeting manual dexterity: Exercise is fun. “You are kidding-right?” Sensors. 2021; 21(17):5766. [DOI:10.3390/s21175766] [PMID]
- Birudu R, Kanmani TR, Devi BI. Management of rehabilitation needs of "unknown" traumatic brain injury survivors: A medical and psychiatric social work perspective. Neurology India. 2020; 68(3):603-8. [DOI:10.4103/0028-3886.288985] [PMID]
- Chhabra HS, Sharma S, Arora M. Challenges in comprehensive management of spinal cord injury in India and in the Asian Spinal Cord network region: Findings of a survey of experts, patients and consumers. Spinal Cord. 2018; 56(1):71-7. [DOI:10.1038/sc.2017.102] [PMID]
- Reddy SK, Jagnnathan A, Ashraf GH, Kumar CN, Thirthalli J, Banerjee R, et al. Barriers in accessing social welfare benefits for families of children with intellectual and developmental disorders in rural Karnataka: A situation analysis. Indian Journal of Psychological Medicine. 2021; 43(5):403-9. [DOI:10.1177/0253717621994706] [PMID]
- Khatib R, Jawaada AM, Arevalo YA, Hamed HK, Mohammed SH, Huffman MD. Implementing evidence-based practices for acute stroke care in Low- and Middle-Income countries. Current Atherosclerosis Reports. 2017; 19(12):61. [DOI:10.1007/s11883-017-0694-6] [PMID]
- van der Marck MA, Munneke M, Mulleners W, Hoogerwaard EM, Borm GF, Overeem S, et al. Integrated multidisciplinary care in Parkinson’s disease: A non-randomised, controlled trial (IMPACT). The Lancet Neurology. 2013; 12(10):947-56. [DOI:10.1016/S1474-4422(13)70196-0] [PMID]
- Wilson E, Lee L, Klas R, Nesbit KC. Technology and rehabilitation training for community health workers: Strengthening health systems in Malawi. Health & Social Care in the Community. 2020; 28(3):833-41. [DOI:10.1111/hsc.12914] [PMID]
- Nesbit KC, Clark A. Rehabilitation training for community health workers: A five-year study. International Journal of Health Promotion and Education. 2019; 57(1):3-12. [DOI:10.1080/14635240.2018.1538808]
- Gelaw AY, Janakiraman B, Gebremeskel BF, Ravichandran H. Effectiveness of home-based rehabilitation in improving physical function of persons with Stroke and other physical disability: A systematic review of randomized controlled trials. Journal of Stroke and Cerebrovascular Diseases. 2020; 29(6):104800. [DOI:10.1016/j.jstrokecerebrovasdis.2020.104800] [PMID]
- Garg D, Dhamija RK. Teleneurorehabilitation for Parkinson’s Disease: A panacea for the times to come? Annals of Indian Academy of Neurology. 2020; 23(5):592-7. [DOI:10.4103/aian.AIAN_566_20] [PMID]
- Tyagi N, Amar Goel S, Alexander M. Improving quality of life after spinal cord injury in India with telehealth. Spinal Cord Series and Cases. 2019; 5:70. [DOI:10.1038/s41394-019-0212-x] [PMID]
- ATTEND Collaborative Group. Family-led rehabilitation after stroke in India (ATTEND): A randomised controlled trial. Lancet. 2017; 390(10094):588-99. [DOI:10.1016/S0140-6736(17)31447-2] [PMID]
- Zhou B, Zhang J, Zhao Y, Li X, Anderson CS, Xie B, et al. Caregiver-delivered stroke rehabilitation in rural China. Stroke. 2019; 50(7):1825-30. [DOI:10.1161/STROKEAHA.118.021558] [PMID]
- Ryan JM, Cassidy EE, Noorduyn SG, O'Connell NE. Exercise interventions for cerebral palsy. The Cochrane Database of Systematic Reviews. 2017; 6(6):CD011660. [DOI:10.1002/14651858.CD011660.pub2] [PMID]
- Sylaja PN, Srivastava MVP, Shah S, Bhatia R, Khurana D, Sharma A, et al. The SARS-CoV-2/COVID-19 pandemic and challenges in stroke care in India. Annals of the New York Academy of Sciences. 2020; 1473(1):3-10. [DOI:10.1111/nyas.14379] [PMID]
- Ghai S, Ghai I. Virtual reality enhances gait in cerebral palsy: A training dose-response meta-analysis. Frontiers in neurology. 2019; 10:236. [DOI:10.3389/fneur.2019.00236] [PMID]
- Mehndiratta P, Wasay M, Mehndiratta MM. Implications of female sex on stroke risk factors, care, outcome and rehabilitation: An Asian perspective. Cerebrovascular Diseases. 2015; 39(5-6):302-8. [DOI:10.1159/000381832] [PMID]
- Jacob S, Alagirisamy M, Xi C, Balasubramanian V, Srinivasan R, R P, et al. AI and IoT-enabled smart exoskeleton system for rehabilitation of paralyzed people in connected communities. IEEE. 2021; 9:80340-50. [DOI:10.1109/ACCESS.2021.3083093]
- Alve YA, Bontje P. Factors influencing participation in daily activities by persons with spinal cord injury: Lessons learned from an international scoping review. Topics in Spinal Cord Injury Rehabilitation. 2019; 25(1):41-61. [DOI:10.1310/sci2501-41] [PMID]
- Shankaranarayana AM, Gururaj S, Natarajan M, Balasubramanian CK, Solomon JM. Gait training interventions for patients with stroke in India: A systematic review. Gait & posture. 2021; 83:132-40. [DOI:10.1016/j.gaitpost.2020.10.012] [PMID]
- Furlan AD, Irvin E, Munhall C, Giraldo-Prieto M, Fullerton L, McMaster R, et al. Rehabilitation service models for people with physical and/or mental disability living in low- and middle-income countries: A systematic review. Journal of Rehabilitation Medicine. 2018; 50(6):487-98. [DOI:10.2340/16501977-2325] [PMID]
- Sureshkumar K, Murthy GVS, Munuswamy S, Goenka S, Kuper H. ‘Care for Stroke’, a web-based, smartphone-enabled educational intervention for management of physical disabilities following stroke: Feasibility in the Indian context. BMJ Innovations. 2015; 1(3):127-36. [DOI:10.1136/bmjinnov-2015-000056]
- Surya N, Srivastava A, Nagda T, Palande D, Someshwar H. Education, training, and practices of neurorehabilitation in India during the Covid-19 pandemic. Frontiers in Neurology. 2021; 12:626399. [DOI:10.3389/fneur.2021.626399] [PMID]
- Venketasubramanian N, Anderson C, Ay H, Aybek S, Brinjikji W, de Freitas GR, et al. Stroke care during the COVID-19 pandemic: International expert panel review. Cerebrovascular Diseases. 2021; 50(3):245-61. [DOI:10.1159/000514155] [PMID]
- Alzamanan MZ, Lim KS, Akmar Ismail M, Abdul Ghani N. Self-management apps for people with Epilepsy: Systematic analysis. JMIR mHealth and uHealth. 2021; 9(5):e22489. [DOI:10.2196/22489] [PMID]
- Dandona L, Singh G, India State-Level Disease Burden Initiative Neurological Disorders Collaborators. Challenges in estimating the burden of neurological disorders across Indian states - Authors' reply. The Lancet. Global health, 9(11), e1504. [DOI:10.1016/S2214-109X(21)00412-5] [PMID]
Article type: Reviews |
Subject:
Neurorehabilitation
Received: 2023/03/31 | Accepted: 2024/04/27 | Published: 2025/03/1
Received: 2023/03/31 | Accepted: 2024/04/27 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
