
988368
Tue, Jul 7, 2026

Volume 22, Issue 2 (June 2024)
Iranian Rehabilitation Journal 2024, 22(2): 307-320 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Brahmbhatt H. Need Assessment Study For Wheelchair Users In Gujarat, India. Iranian Rehabilitation Journal 2024; 22 (2) :307-320
URL: http://irj.uswr.ac.ir/article-1-1938-en.html
URL: http://irj.uswr.ac.ir/article-1-1938-en.html



Gujarat Technological University, Ahmedabad, India.
Full-Text [PDF 1549 kb]
(1786 Downloads)
| Abstract (HTML) (3373 Views)
Full-Text: (1823 Views)
Introduction
According to the World Health Organization (WHO) guidelines on the provision of manual wheelchairs in less-resourced settings [1], the appropriateness of a wheelchair for a specific user depends on the following factors: The physical needs of the users, the way and the environment in which the wheelchair will be used, the material and technology available where the wheelchair is being made and used.
Accordingly, users are central to developing and implementing any wheelchair design and further provision. They help to ensure that a wheelchair and its related services meet their need effectively. Hence, the WHO has described the role of users as follows: Participating in the planning, implementation, management and evaluation of wheelchair provisions, participating in the development and testing of wheelchair designs; Working within wheelchair services in clinical, technical, and training roles and supporting and training new users.
This article describes a need assessment study conducted on wheelchair users in the semi-urban area of Ahmedabad City, India, in 2018 to develop and prototype a wheelchair made from local resources for the local users. Moreover, a further study was also conducted [2]. Accordingly, the subjects of the need assessment study in that article are women with disabilities in and around Ahmedabad City, India in 1998. One main reason for conducting a second study on the same region was that the old study was outdated. In the last 20 years, there has been an immense change in the standards of living in Ahmedabad City, India and nearby regions along with technological advancements in general. For instance, from 2019 to 2020, a total of 89.3% of urban households in Gujarat City, India, had improved access to toilets in their homes and do not use communal facilities anymore in comparison to just 36.4% of households in 2001 who had access to toilets, including shared toilets [3, 4]. There was 41% mud flooring in houses in the year 2001 while in 2011 the mud floored houses decreased to 28% and the houses with solid flooring (cement/tiles) increased from 57% to 71% [4, 5]. A more recent data will become available with the census in 2023. Further, the phone access penetration in India in the year 2020 was around 83% [6]. Meanwhile, the scope of the previous study was limited to women with disability in the region, and the women participants were engaged solely in housework. We expand the scope of the study by being gender inclusive and noting that some housework, such as drying, hanging clothes, or accessing wardrobes must be done by everyone along with cooking. With the advent of modern housing design, mobility needs have changed significantly to working just close to the ground.
The government of India conducted its last census in 2011, in which the data on broad classification of disability types, like speech, movement, hearing, and seeing were collected. Accordingly [5], India has 2.21% of its population disabled while Gujarat City has 1.81% of its population disabled. In absolute numbers, India has over 28600000 disabled people of which over 1086900 reside in Gujarat City. Moreover, India has above 5.4 million people with locomotion disability.
In 2018, the National Statistical Office, a governmental survey department, conducted a detailed national survey. The results [7] reported the prevalence and causes of various disabilities, education levels, living arrangements, availability of caregivers, whether they had a certificate of disability, labor force participation rate, and unemployment rates. It also reported that the main causes of loco-motor disabilities in India are accidents (road accidents and burns), assaults (acid attacks), and diseases (polio, cerebral palsy, leprosy). The leading cause of locomotion disability was diseases/disorders accounting for over 46% of individuals. Additionally, nearly 30% of the people had a disability since birth.
Moreover, the survey reported that over 11% of the population with locomotor disability who were advised a mobility aid could not acquire it due to difficulty in affording it or its unavailability. Of the 23% of the people who were advised and bought an assistive device, 72% purchased it directly, 13% via government aid, 2% via non-governmental aid, and the remaining 11% got it from a charity event. A healthy number of 84% of the people who acquired some assistive devices were using it regularly. The most common type of mobility assistive device acquired was a crutch (about 31%) followed by a manual wheelchair (about 10%), then a tricycle (about 4%).
With such a large population requiring various assistive mobility, there is an immediate necessity to understand whether the current devices meet all the required needs and are well suited to the users.
Accordingly, this study collects user feedback about the assistive technology the users are using and how comfortable and utilitarian the choices and needs that are not met by their current devices. This need assessment study leads to the development and prototyping of an assistive device [8].
Materials and Methods
The study was conducted in the urban metropolitan region of Ahmedabad City, India, from 2018 to 2019 as a part of the need assessment study for the PhD dissertation of the principal investigator (PI). The reason for choosing this area was twofold: First and main reason, the PI is based in this city and is fluent in the local languages and customs, so a translator would not be needed and the study participants would feel more comfortable in sharing details. Secondly, a previous study had been carried out in the same region about the needs of women with locomotion disabilities in [2] in the year 1998. This study compared the results of this survey with ours on the changes in the needs of disabled women.
Participant selection criteria
In the year 2018, the unique disability ID had just started and since there was not yet any central database of persons with disabilities, the study was conducted with the help of local resources available to the PI. The participants were contacted through an (non government organization) (NGO), Apang Manav Mandal. The PI contacted the NGO and they helped by introducing around 150 people associated with them. The PI briefed the participants about the purpose of the study and requested consent to conduct survey interviews with the 150 people; However, only 69 interested people gave consent to participate. The PI then collected the primary information about the places the participants lived, their income, their locomotion difficulties, their needs and the mobility devices they were using. The PI further asked for consent from the participants to study their daily activities with a video recording. Only 9 of the 69 participants consented to such an interview. These interviews were conducted by the PI with the help of diploma students Dhruvin Patel, Smit Sompura, Jay Patel, Om Panchal, and Dhruv Chavada at LJ University, Ahmedabad City, India. The participants’ full daily routine was to be observed. Some participants only consented for parts of their daily activities to be recorded or just consented to a short video interview. However, they consented the student to observe them without recording along with them providing a description or explanation when needed. Further two more people who were work colleagues of the PI were also interviewed and their activities were video recorded. The video recordings were taken on a mobile device as it was most convenient to use while following the interviewee on their daily tasks around the city. Compensation in kind (e.g. first aid kits, wall clock) was given to the participants of video interviews for their valuable time and response.
Study methodology
The interviews were semi-structured since we wanted to explore all the different difficulties faced by the interviewees in using their current movement aid devices. The data of 69 participants having physical disabilities were collected through survey interviews. The preliminary analysis was conducted to understand the physical and socio-economic environment of the participants. Meanwhile, 9 out of 69 participants consented to the video interviews. The qualitative thematic analysis was carried out for the video interviews. A sample questionnaire is presented in the Appendix 1. The interviews were carried out mostly in the local languages (Gujarati/Hindi) and later translated into English by the PI. The thematic analysis of the interviews was carried out to identify common needs not met by the mobility devices used currently.
Results
The results begin by first summarizing the data collected from the preliminary interaction with the study participants. For such data, we do a descriptive analysis, since it suits our purpose the best. Then we describe the findings from the individual interview interactions with the select group.
Age and health status
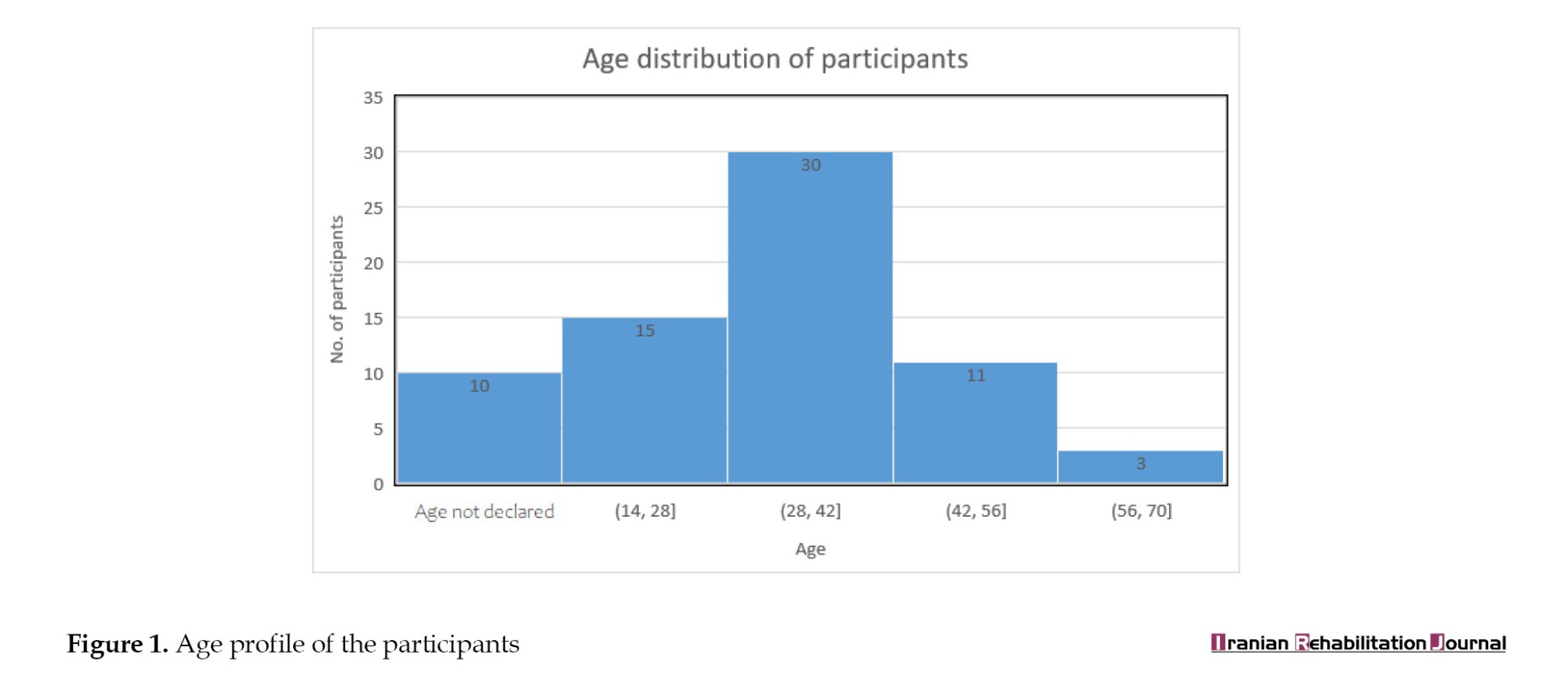
The age profile of the participants ranged between 18-70 years. Our study was focused on adults rather than children or adolescents for the reason that the needs of children/adolescents are usually different from the needs of adults who may no longer be fully dependent on their parents. 10 participants did not declare their age.
The weights of the participants are summarized in Table 1. The participants were asked to self-declare their weights. It was not feasible to measure the weights of the individuals on the spot. This set of data was collected to have an idea of how much weight the mobility device has to handle and the most appropriate weight range for which it should be designed.

To the best of our knowledge, (via a search on online databases, such as Google Scholar, Pubmed, and Scopus), no results about any study on the weights of disabled persons compared to the type of disability (even locomotor) in India exist. Therefore, we cannot comment if this weight profile is representative of the weight profile of persons with locomotor disabilities in India. However, the data shows a surprising trend towards the person’s being underweight given that these people have very limited scope for physical activity. This warrants an extensive study.
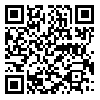
Table 2 summarizes the present mobility status of our study participants. Most of the study participants had a disability since birth. About 25% of the study participants had developed disability after accidents. Only one person had developed disability due to polio as she did not take polio vaccination as a child. This distribution can be compared with the leading causes of disability in India as recorded in the 2018 national sample survey (NSS) survey.
Education and economic status
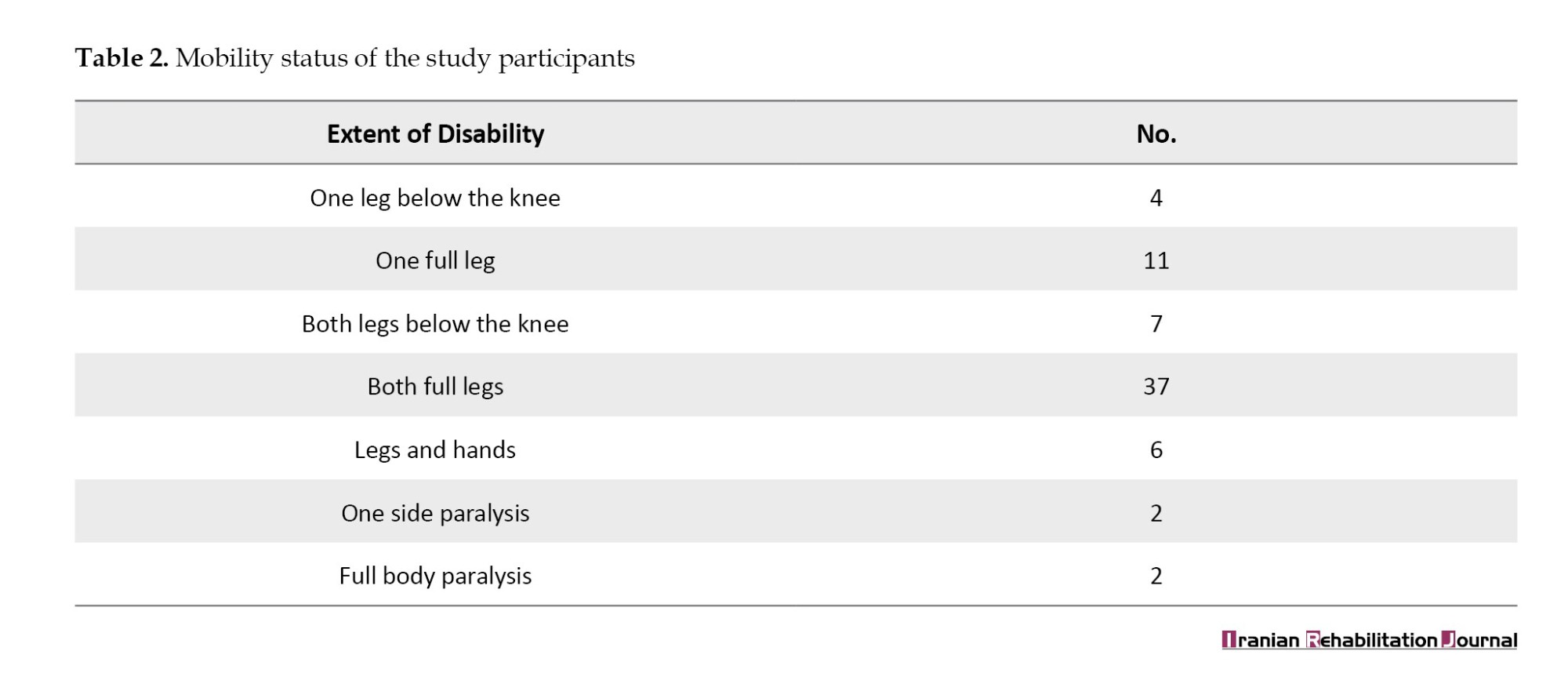
Access to education and the right to work are the fundamental rights guaranteed by the rights of persons with disabilities act of 2016. In our study, we found that all the study participants were literate with over 30% completing either undergraduate degree or higher. Although mostly they had pursued non-technical degrees. A few of them were pursuing under graduation. This is in stark contrast with the results of the census in 2011 as well as the NSS disability survey in 2018-2019, where the literacy rates are not that high in males but particularly low in females. The educational status of the study participants is summarized in the Table 3 along with the self-declared earnings of the study participants (Table 4).
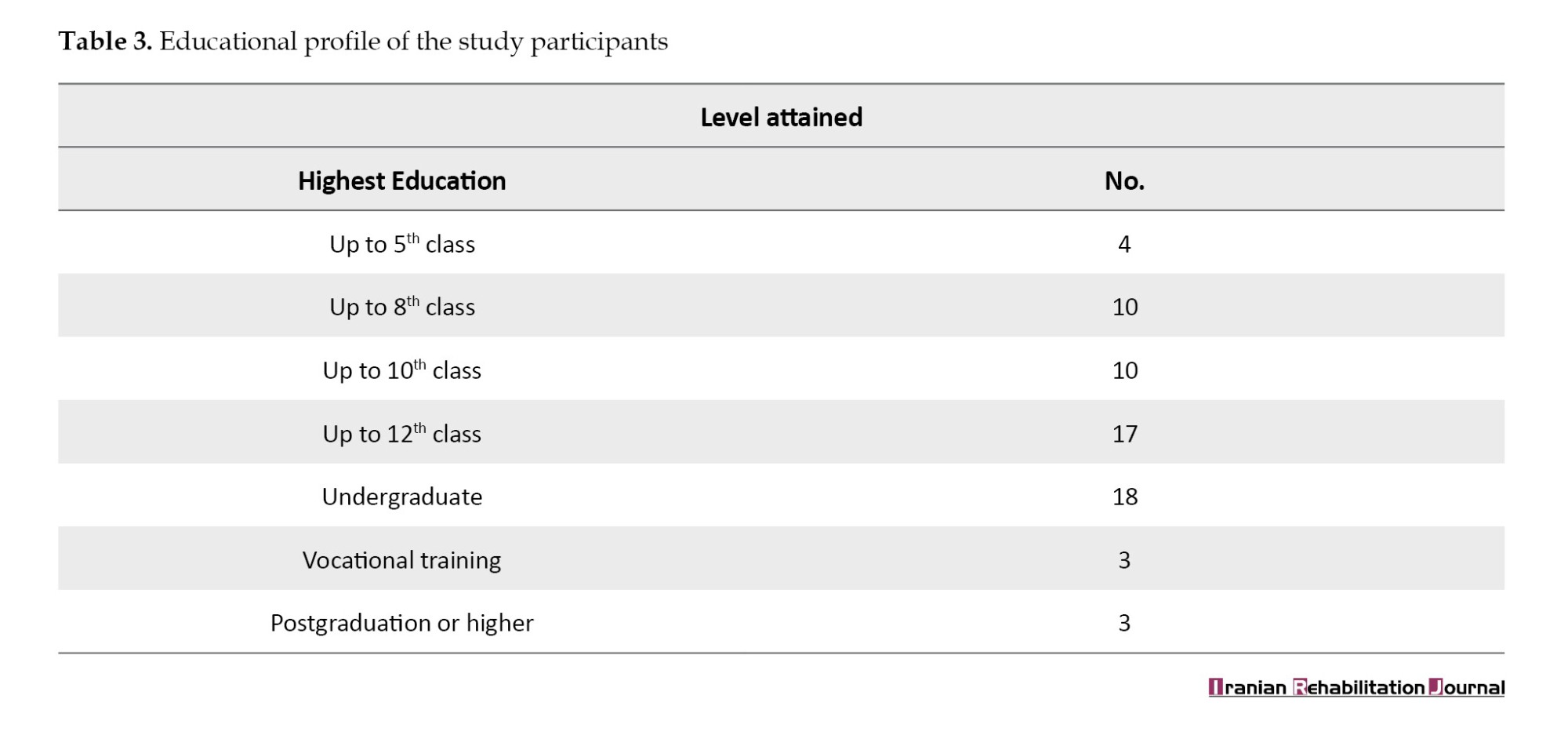
Even though the economic cost of the disability will not be apparent from our study, it is provided in the data in the NSS disability report.
Physical environment
The physical environment of the participants was semi-urban, given that we had interviewed the people who lived near and around Ahmedabad City, India and could come to meet us at Sabarmati Riverfront, which is almost in the middle of the city.
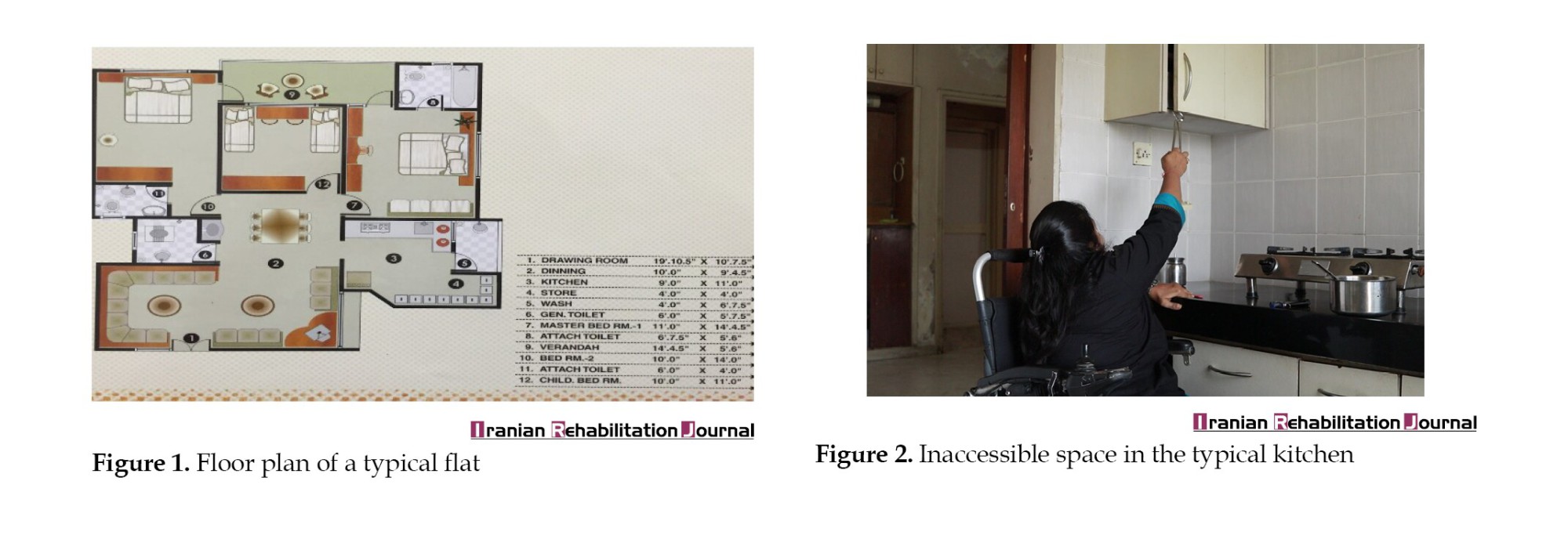
All the interviewed participants lived in either flats or houses. A typical 3 bedroom, hall, kitchen flat had the floor plan as shown in Figure 1. Usually, the houses/flats have the following rooms: Bedrooms (dependent upon the house vary from 1-3), hall cum dining room, bathrooms/toilets, kitchen, balcony/service balcony/drying area. The size and the number of rooms vary depending on the flat as well as the affordability of the house. The participants we interviewed owned or rented a flat or house. Below we will briefly discuss the places in the house where the participants faced a lot of difficulty.
Kitchen
The kitchens in city houses/flats are now modular in comparison with the study done before [2] in 1998, where the women worked in mud kitchens. This has led to more problems for disabled persons trying to work in the kitchen. Since the platforms are high, disabled people have to use their wheelchairs to see or work on the platform and while being in this position, they find it difficult to access the storage places made at a height, which usually are easily accessible in standing position for an adult of average height (Figure 2). Furthermore, the width of kitchens is not much sometimes and it becomes difficult to make a roundabout turn to access, either the second platform of back storage in the kitchen.
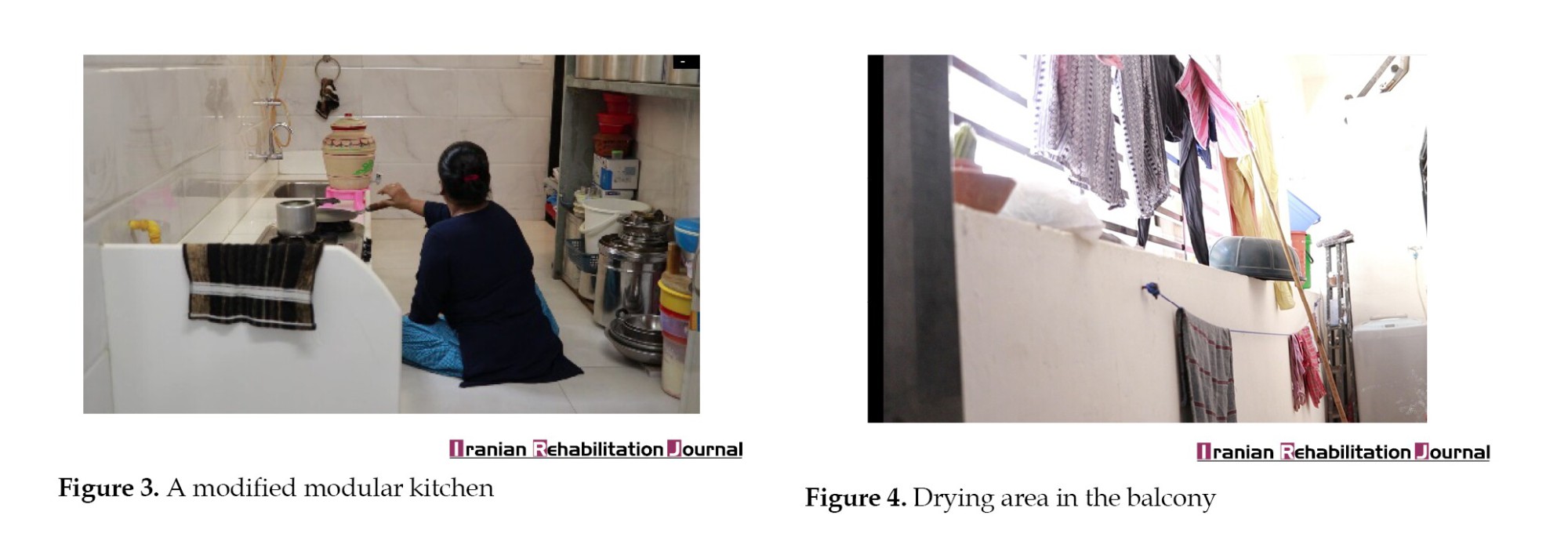
The cost associated with rebuilding the kitchen platform at a lower height; Therefore, it can be accessed with a ground-moving device, is usually quite high (approximately over 200000 INR). A few of our study participants had rebuilt their kitchen platform close to the ground. This helped improve its accessibility and they could easily turn around and use the back storage as can be seen in Figure 3, still not situated at much height. Another drawback of such a modification is that it decreases the usability of the kitchen for other family members. Meanwhile, these problems are not unique to kitchens but are faced a lot by disabled students/scientists trying to work in science laboratories, e.g. chemistry or biology labs. Again the option of rebuilding is not at all feasible or sensible in this case.
Bathroom or toilet
All the study participants had a bathing and toilet area in their house. However, almost all the study participants usually faced a lot of problems in accessing the toilets. The pre-made toilets in the house had to be modified to suit their needs; For example, wall attachments had to be added so that they could hold on to them while bathing or when transferring onto the toilet seat. A few participants used Indian-style toilets, which were difficult to access with a wheelchair, and usually, they tried to access the toilets while sliding on the floor which also caused hygiene-related problems. This is one of the reasons that different hygiene-related diseases were common among them.
The people who could afford had special bathing and toilet chairs. Transferring to these chairs is a challenging task.
Moreover, in a typical house/flat the bathing and toilet areas usually have a height difference in the form of a low step for the bathing area. This adds to the difficulty when using a bathing chair. Moreover, the entry door to the bathroom usually has a small height barrier to prevent water from entering the room, which again adds to a lot of difficulty in accessing the toilet or bathroom in a wheelchair.
Furthermore, the washbasins and sinks in the washrooms are made with the idea that a person standing will be using them and thus it is not accessible for the person sitting in a wheelchair to access them, for example for brushing their teeth or washing their face. A few of our study participants had remodeled their bathroom sink to a slightly lower height. However, this decreases its usability for other family members.
During the interviews, women participants elaborated more on the difficulties in accessing toilets when they are outside their houses. Many of the female participants restricted their travel and outdoor time to less than 4 h so that they could come back home and use their toilets. This was one of the main reasons cited by women for not pursuing jobs/higher studies.
Drying area or service balcony
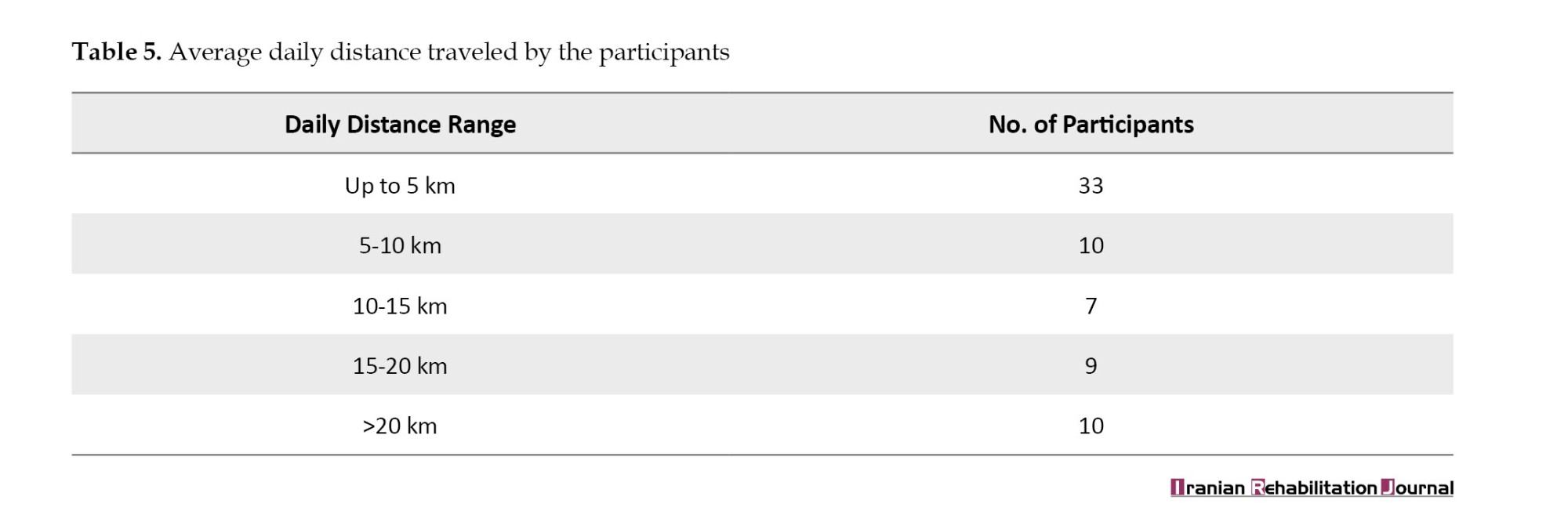
Dryers are extremely uncommon in India and are quite expensive to buy and use. Thus, drying of clothes in an apartment or flat is usually done under the sun in the service area or balcony on wires hung near the roof (Figure 4). Since the hanging wires are at a significant height, persons in wheelchairs cannot access them. However, a few of the study participants had developed indigenous solutions for hanging clothes using wooden sticks as can be seen in Figure 4.
Common area rooms and bedrooms
The major problems faced by study participants in these places were common and mostly related to transferring from wheelchair to bed, sofa, chair, or difficulty in accessing storage in high-height cupboard shelves.
Outdoor area
Most of the participants worked or studied. They lived quite close to the place of study/work and their daily travel was less than 5 km. A few of the study participants (all men) were traveling salespersons as well. Table 5 summarizes the daily travel distance commuted by the study participants.
For travelling almost all of the study participants used their means and did not travel much by public transport, if at all. The reasons were irregular timings and inaccessibility of public transport or public places via wheelchairs. This was also noted in the NSS survey. Mobility devices currently used by the study participants are summarized in Table 6. Out of the 69 study participants, 35 owned multiple mobility devices. The participants who owned motorized vehicles mostly owned a secondary mobility device, a wheelchair. A few of them also had calipers, which were useful for them to access stairs and get in and out of cars or their motor vehicle or tricycle.
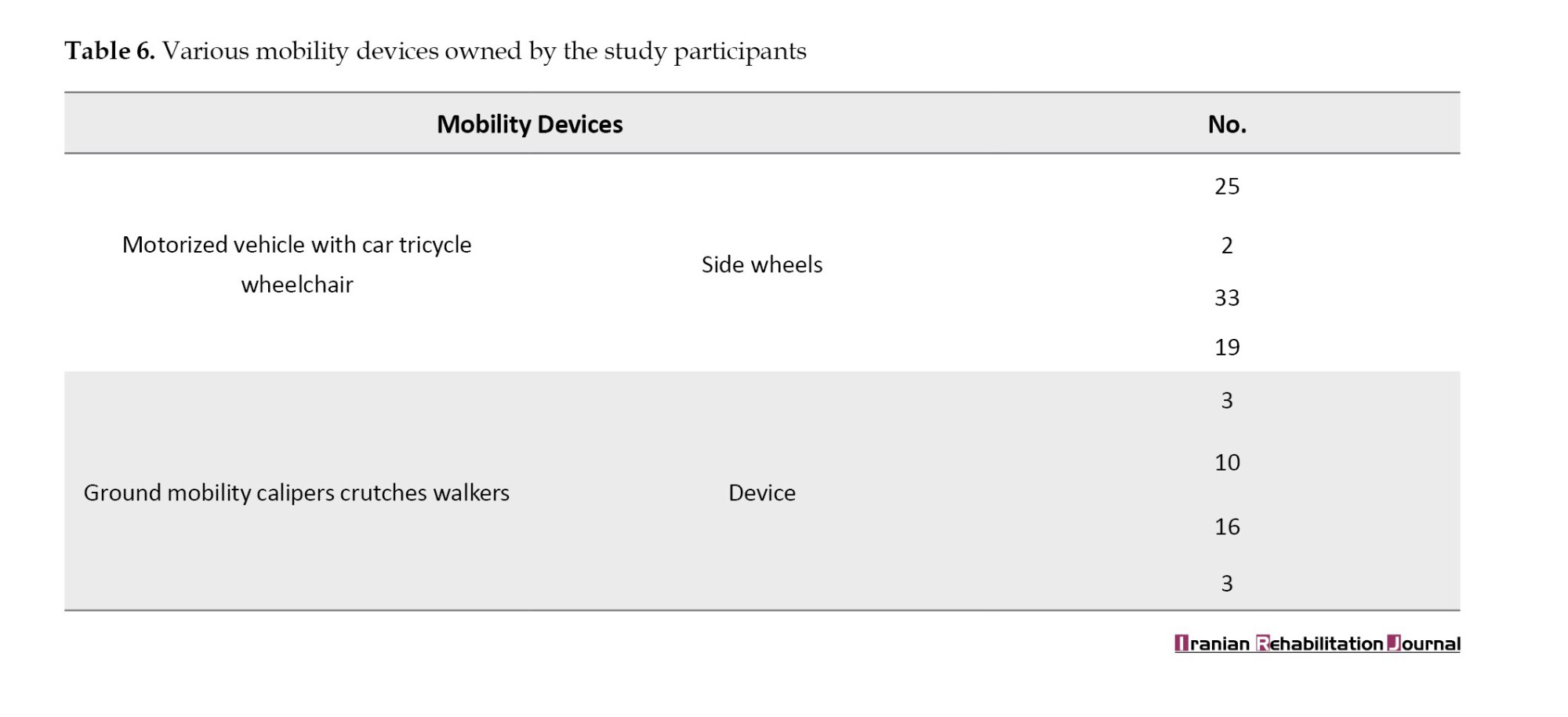
Even though over 80% of the study participants owned an outdoor mobility device (tricycle, motorized, two-wheeler with side wheels or car), the majority of the devices could not be used in all weather conditions.
Ahmedabad City and surrounding areas have semi-arid weather conditions with three main seasons, namely summer, rainy, and winter. Summers are dry and hot with temperatures in the range of 28◦C to 48◦C. They last from March-June and September-October intervening in between the monsoon/rainy season during July-August.
Rainy season witness heavy rainfall which mostly leads to water-logging of roads, rendering them completely inaccessible by most vehicles. Even on days of moderate rainfall or days of hot summer with very bright sun, it is difficult to use the tricycle or motorized two-wheeler with side wheels, since they lack a roof.
The winter season is mild and usually lasts from November to February. The temperature ranges from 12◦C −33◦C, with nights being colder than the days which are mostly sunny. The visibility is over 1 km in the region during the summer and winter seasons. It can decrease to less than 50 m during the rainy season especially during moderate to heavy rainfall spells. Thus, visibility is not a serious issue for most of the year.
Given that roads in and around Ahmedabad can be quite busy with traffic with narrow passages or unpaved, wheelchairs are quite unsafe as well as inconvenient for outdoor use. Tricycles were a quite popular means of transport due to their affordability, even though they are quite slow, physically draining to use, and difficult to maneuver as told by our interviewees.
A motorized two-wheeler with side wheels being slightly expensive is the second most popular outdoor mobility device after the tricycle. Most of our study participants had bought it after they had used the tricycle for a few years and had become more economically stable. However, a few study participants faced problems while using it.
One study participant had a deformed spinal cord so their body height was smaller compared to normal users and he found the steering height high which is designed for a normal person. His arms even pained due to the force required to steer the motor vehicle with attached side wheels.
Another study participant would lose a bit of body stability when applying brakes, since he could not use his feet to maintain his balance, even with the side wheels. Transferring onto and out of all three outdoor mobility devices is quite challenging as well.
Object transportation
The ability to store and carry objects of daily use and shopping safely and conveniently is an important and necessary function of an outdoor mobility device. Cars are the most convenient and secure for object transportation and have the added benefit of being able to share the ride with co-passengers. The motorized two-wheeler has a limited storage capacity, it is especially difficult to carry heavy items or items of large sizes or secure them, although they take with them one co-passenger. The tricycles do not come with storage or any place to secure them and usually one cannot carry any co-passengers other than possibly small children but there are still some safety concerns for that. The study participants, mainly the users of the tricycles faced a lot of difficulty in carrying even lunch boxes or school bags/university textbooks with them on their tricycles.
Socio-cultural environment
Other than facing difficulties with the physical environment, the study participants faced numerous challenges because of the outright adverse attitude or ignorance of the people around them. There is a lack of sensitivity in society which does not support the social inclusion of persons with special needs to a larger extent.
A few study participants did not go out much on social occasions as the mobility devices made them feel uncomfortable. Also, they were not very welcome to participate in social or festive occasions as they were considered inauspicious. Moreover, one of the study participants explained that while using a wheelchair in social or public places she felt she was slow and could not match up with the pace of people and thus felt left out or out of place. Another (female) participant responded that they had difficulty in using their assistive devices with the traditional attire (a saree/lehenga), which they wanted to wear for a festive occasion. Thereby they felt a bit alienated.
Discussion
This study advances the work done in a previous article [2] in the region of Ahmedabad City, India in 1998 after over 20 years and fills in the gaps in studies identified in the literature [9] on the needs in indoor environment for persons with disability. Other than the above two cited articles no systematic study was conducted in India about the needs and user experience of the assisted devices. The results of this article identified many areas in which improvement is urgently needed to enhance the quality of life.
Accordingly, there are two main approaches in research to improve the quality of life of people living with locomotor disabilities. First, to create accessible infrastructure for example having ramps along with stairs or attaching elevators to access buildings, having doorways/hallways of sufficient width (in modern housing, there can be narrow doorways and passage or narrow balconies, due to high real estate prices), arrangement of furniture so that it does not hamper movement, accessibility of storage, we will call this generically as table height wheelchair accessible infrastructure. According to Saha et al. [10], this is how one should design indoor spaces.
The second approach is to introduce technological innovations in the design of assistive technologies that help in adapting to the available infrastructure.
In the Indian context, or even more generally in low-resourced settings, there is far better reach of adaptive assistive technologies than hoping for large-scale infrastructure changes. Even after it has been mandated by the Government of India to have accessible infrastructure, more than 63% of the persons who accessed public buildings faced difficulties in accessing them according to the NSS survey, a similar number exists for public transport. Long-distance journeys are virtually impossible for persons with disabilities on either trains or buses. Almost none have ramps to access the coach or seats on wheelchairs, passages are so narrow with no safety handles anywhere to keep steady. Toilets are inaccessible on most of the trains, with no wall attachments or any disability-friendly safety feature given that the trains also shake significantly. These problems are further aggravated by the issue that there are no standard guidelines on even manual wheelchairs that would fix the width range or basic features of the wheelchairs. Such guidelines are immediately needed so that most of the infrastructure (e.g. doorways of trains, houses) can be built keeping in mind the standard ranges for such devices. However, as the WHO guidelines have advised [1], such standards should be set according to the Indian context and further research is long due. As also highlighted in a study [2], wheelchairs should not restrict the sitting positions of a person to just one or two as various tasks require different seating positions.
Given that, not all infrastructure can be modified, nor would one want to modify it, given that everything at table height is not very convenient to use for a person standing a few technological innovations in the wheelchair technology would help us reach a good middle ground. For example, in offices, research labs, or working space environments, a space that has been ignored a lot in the context of disability-friendly designs, actually it is not quite feasible to have storage at sitting wheelchair height only. One would also require efficient use also high-height storage, for such needs it is better to modify the wheelchair can have adjustable height, as we have designed in [8]. Another such technological innovation is a standing wheelchair affordably designed in India [11] or a stair-climbing wheelchair [12]. The need assessment study of [2] also led to the development of a ground mobility device for women. A few of our study participants (actually both men and women) also owned a ground mobility device, it was quite helpful and convenient for them for indoor use but caused back pain after long-term use due to no back support. The problems highlighted above also occur in other countries, and the research done there can be adapted suitably in the Indian context, for example for the transfer of a wheelchair on to a train, a new assistive device has been developed in Japan [13].
As discussed in the results section above, mobility is severely restricted for everyone in monsoon, and so unless the infrastructure is improved at the level of planning of roads, we think it is not very beneficial to improvise on that part of the mobility device usability. Rather it would be greatly beneficial for persons with disability to have features on a wheelchair that will improve upon the ability to transfer from a wheelchair to another chair, bed, or toilet and to improve indoor accessibility features. Not much research has been done in the Indian context on this point.
Lastly, to improve the quality of life of a person with a disability, the stigma associated with disabilities has to be addressed at the level of society and the sensitivities of the general public have to be enhanced. Awareness drives by either NGOs or governmental organizations will benefit both the general public as well as persons with disabilities in knowing their rights and responsibilities as well as preparing the ground for their economic as well as social assimilation into society.
Conclusion
This study attempted to understand the everyday challenges of wheelchair users. It noted the educational background, assistive device preferences, health conditions, and socio-economic and physical environments of participants. The mixture of qualitative and quantitative data analysis showed that the major features that the Indian wheelchair users wanted were the ability to adjust the height of the chair, the ability to reach objects without too much maneuvering of the wheelchair, ease of transfer from wheelchair to toilet seat and back, a smaller number of transfers required and also to meet outdoor needs. This led us to conclude that a wheelchair which can be used in both indoor and outdoor settings was one of the most imminent needs for wheelchair users in the Indian context. Moreover, since the outdoor settings in India differ a lot from those of the more developed countries, these chairs should be developed and designed in India.
Limitations, methodological considerations, and future research
Some of the results of the survey are biased since our participant selection was not random and may not reflect the general needs of the disabled population. However, it does highlight a very important point; The independence and community participation that outdoor mobility devices bring and the positive effects it has on the user, namely access to education and economic independence.
Since one size fits all is not how wheelchair design should work [19], we confirm that even for this positively skewed education community, there are a lot of unmet needs that need to be addressed and other surveys should be conducted similarly in other Indian cities. Another factor for conducting such a study was to understand and find out the unmet needs of the knowledge workforce with disability so that when a person loses the ability to perform their previous work due to the disability due to some disease or injury, their transition (or upskill) to knowledge workforce with a bit more ease. They should not face difficulty due to a lack of suitable assistive devices for their economic and social independence.
The data we had collected had some gaps in between and it was self-reported, so there are chances for discrepancies, especially concerning medical facts or economic facts. A random study conducted out of participants selected from a database, which is fed information about the health status directly from the hospitals/medical facility would be of great help.
Ethical Considerations
Compliance with ethical guidelines
The consent of participants was taken for voluntary participation in the study. Each participant was briefed about the scope of the study. The confidentiality of the personal data of the participants was ensured. The participants were not subject to any harm during or after the study.
Funding
This article extracted from PhD dissertation of Harshul Brahmbhatt, approved by Gujarat Technological University. This study was financially supported by the Government of Gujarat under a startup grant.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Gujarat Technological University and the Government of Gujarat for their financial support.
References
According to the World Health Organization (WHO) guidelines on the provision of manual wheelchairs in less-resourced settings [1], the appropriateness of a wheelchair for a specific user depends on the following factors: The physical needs of the users, the way and the environment in which the wheelchair will be used, the material and technology available where the wheelchair is being made and used.
Accordingly, users are central to developing and implementing any wheelchair design and further provision. They help to ensure that a wheelchair and its related services meet their need effectively. Hence, the WHO has described the role of users as follows: Participating in the planning, implementation, management and evaluation of wheelchair provisions, participating in the development and testing of wheelchair designs; Working within wheelchair services in clinical, technical, and training roles and supporting and training new users.
This article describes a need assessment study conducted on wheelchair users in the semi-urban area of Ahmedabad City, India, in 2018 to develop and prototype a wheelchair made from local resources for the local users. Moreover, a further study was also conducted [2]. Accordingly, the subjects of the need assessment study in that article are women with disabilities in and around Ahmedabad City, India in 1998. One main reason for conducting a second study on the same region was that the old study was outdated. In the last 20 years, there has been an immense change in the standards of living in Ahmedabad City, India and nearby regions along with technological advancements in general. For instance, from 2019 to 2020, a total of 89.3% of urban households in Gujarat City, India, had improved access to toilets in their homes and do not use communal facilities anymore in comparison to just 36.4% of households in 2001 who had access to toilets, including shared toilets [3, 4]. There was 41% mud flooring in houses in the year 2001 while in 2011 the mud floored houses decreased to 28% and the houses with solid flooring (cement/tiles) increased from 57% to 71% [4, 5]. A more recent data will become available with the census in 2023. Further, the phone access penetration in India in the year 2020 was around 83% [6]. Meanwhile, the scope of the previous study was limited to women with disability in the region, and the women participants were engaged solely in housework. We expand the scope of the study by being gender inclusive and noting that some housework, such as drying, hanging clothes, or accessing wardrobes must be done by everyone along with cooking. With the advent of modern housing design, mobility needs have changed significantly to working just close to the ground.
The government of India conducted its last census in 2011, in which the data on broad classification of disability types, like speech, movement, hearing, and seeing were collected. Accordingly [5], India has 2.21% of its population disabled while Gujarat City has 1.81% of its population disabled. In absolute numbers, India has over 28600000 disabled people of which over 1086900 reside in Gujarat City. Moreover, India has above 5.4 million people with locomotion disability.
In 2018, the National Statistical Office, a governmental survey department, conducted a detailed national survey. The results [7] reported the prevalence and causes of various disabilities, education levels, living arrangements, availability of caregivers, whether they had a certificate of disability, labor force participation rate, and unemployment rates. It also reported that the main causes of loco-motor disabilities in India are accidents (road accidents and burns), assaults (acid attacks), and diseases (polio, cerebral palsy, leprosy). The leading cause of locomotion disability was diseases/disorders accounting for over 46% of individuals. Additionally, nearly 30% of the people had a disability since birth.
Moreover, the survey reported that over 11% of the population with locomotor disability who were advised a mobility aid could not acquire it due to difficulty in affording it or its unavailability. Of the 23% of the people who were advised and bought an assistive device, 72% purchased it directly, 13% via government aid, 2% via non-governmental aid, and the remaining 11% got it from a charity event. A healthy number of 84% of the people who acquired some assistive devices were using it regularly. The most common type of mobility assistive device acquired was a crutch (about 31%) followed by a manual wheelchair (about 10%), then a tricycle (about 4%).
With such a large population requiring various assistive mobility, there is an immediate necessity to understand whether the current devices meet all the required needs and are well suited to the users.
Accordingly, this study collects user feedback about the assistive technology the users are using and how comfortable and utilitarian the choices and needs that are not met by their current devices. This need assessment study leads to the development and prototyping of an assistive device [8].
Materials and Methods
The study was conducted in the urban metropolitan region of Ahmedabad City, India, from 2018 to 2019 as a part of the need assessment study for the PhD dissertation of the principal investigator (PI). The reason for choosing this area was twofold: First and main reason, the PI is based in this city and is fluent in the local languages and customs, so a translator would not be needed and the study participants would feel more comfortable in sharing details. Secondly, a previous study had been carried out in the same region about the needs of women with locomotion disabilities in [2] in the year 1998. This study compared the results of this survey with ours on the changes in the needs of disabled women.
Participant selection criteria
In the year 2018, the unique disability ID had just started and since there was not yet any central database of persons with disabilities, the study was conducted with the help of local resources available to the PI. The participants were contacted through an (non government organization) (NGO), Apang Manav Mandal. The PI contacted the NGO and they helped by introducing around 150 people associated with them. The PI briefed the participants about the purpose of the study and requested consent to conduct survey interviews with the 150 people; However, only 69 interested people gave consent to participate. The PI then collected the primary information about the places the participants lived, their income, their locomotion difficulties, their needs and the mobility devices they were using. The PI further asked for consent from the participants to study their daily activities with a video recording. Only 9 of the 69 participants consented to such an interview. These interviews were conducted by the PI with the help of diploma students Dhruvin Patel, Smit Sompura, Jay Patel, Om Panchal, and Dhruv Chavada at LJ University, Ahmedabad City, India. The participants’ full daily routine was to be observed. Some participants only consented for parts of their daily activities to be recorded or just consented to a short video interview. However, they consented the student to observe them without recording along with them providing a description or explanation when needed. Further two more people who were work colleagues of the PI were also interviewed and their activities were video recorded. The video recordings were taken on a mobile device as it was most convenient to use while following the interviewee on their daily tasks around the city. Compensation in kind (e.g. first aid kits, wall clock) was given to the participants of video interviews for their valuable time and response.
Study methodology
The interviews were semi-structured since we wanted to explore all the different difficulties faced by the interviewees in using their current movement aid devices. The data of 69 participants having physical disabilities were collected through survey interviews. The preliminary analysis was conducted to understand the physical and socio-economic environment of the participants. Meanwhile, 9 out of 69 participants consented to the video interviews. The qualitative thematic analysis was carried out for the video interviews. A sample questionnaire is presented in the Appendix 1. The interviews were carried out mostly in the local languages (Gujarati/Hindi) and later translated into English by the PI. The thematic analysis of the interviews was carried out to identify common needs not met by the mobility devices used currently.
Results
The results begin by first summarizing the data collected from the preliminary interaction with the study participants. For such data, we do a descriptive analysis, since it suits our purpose the best. Then we describe the findings from the individual interview interactions with the select group.
Age and health status
The age profile of the participants ranged between 18-70 years. Our study was focused on adults rather than children or adolescents for the reason that the needs of children/adolescents are usually different from the needs of adults who may no longer be fully dependent on their parents. 10 participants did not declare their age.
The weights of the participants are summarized in Table 1. The participants were asked to self-declare their weights. It was not feasible to measure the weights of the individuals on the spot. This set of data was collected to have an idea of how much weight the mobility device has to handle and the most appropriate weight range for which it should be designed.
To the best of our knowledge, (via a search on online databases, such as Google Scholar, Pubmed, and Scopus), no results about any study on the weights of disabled persons compared to the type of disability (even locomotor) in India exist. Therefore, we cannot comment if this weight profile is representative of the weight profile of persons with locomotor disabilities in India. However, the data shows a surprising trend towards the person’s being underweight given that these people have very limited scope for physical activity. This warrants an extensive study.
Table 2 summarizes the present mobility status of our study participants. Most of the study participants had a disability since birth. About 25% of the study participants had developed disability after accidents. Only one person had developed disability due to polio as she did not take polio vaccination as a child. This distribution can be compared with the leading causes of disability in India as recorded in the 2018 national sample survey (NSS) survey.
Education and economic status
Access to education and the right to work are the fundamental rights guaranteed by the rights of persons with disabilities act of 2016. In our study, we found that all the study participants were literate with over 30% completing either undergraduate degree or higher. Although mostly they had pursued non-technical degrees. A few of them were pursuing under graduation. This is in stark contrast with the results of the census in 2011 as well as the NSS disability survey in 2018-2019, where the literacy rates are not that high in males but particularly low in females. The educational status of the study participants is summarized in the Table 3 along with the self-declared earnings of the study participants (Table 4).
Even though the economic cost of the disability will not be apparent from our study, it is provided in the data in the NSS disability report.
Physical environment
The physical environment of the participants was semi-urban, given that we had interviewed the people who lived near and around Ahmedabad City, India and could come to meet us at Sabarmati Riverfront, which is almost in the middle of the city.
All the interviewed participants lived in either flats or houses. A typical 3 bedroom, hall, kitchen flat had the floor plan as shown in Figure 1. Usually, the houses/flats have the following rooms: Bedrooms (dependent upon the house vary from 1-3), hall cum dining room, bathrooms/toilets, kitchen, balcony/service balcony/drying area. The size and the number of rooms vary depending on the flat as well as the affordability of the house. The participants we interviewed owned or rented a flat or house. Below we will briefly discuss the places in the house where the participants faced a lot of difficulty.
Kitchen
The kitchens in city houses/flats are now modular in comparison with the study done before [2] in 1998, where the women worked in mud kitchens. This has led to more problems for disabled persons trying to work in the kitchen. Since the platforms are high, disabled people have to use their wheelchairs to see or work on the platform and while being in this position, they find it difficult to access the storage places made at a height, which usually are easily accessible in standing position for an adult of average height (Figure 2). Furthermore, the width of kitchens is not much sometimes and it becomes difficult to make a roundabout turn to access, either the second platform of back storage in the kitchen.
The cost associated with rebuilding the kitchen platform at a lower height; Therefore, it can be accessed with a ground-moving device, is usually quite high (approximately over 200000 INR). A few of our study participants had rebuilt their kitchen platform close to the ground. This helped improve its accessibility and they could easily turn around and use the back storage as can be seen in Figure 3, still not situated at much height. Another drawback of such a modification is that it decreases the usability of the kitchen for other family members. Meanwhile, these problems are not unique to kitchens but are faced a lot by disabled students/scientists trying to work in science laboratories, e.g. chemistry or biology labs. Again the option of rebuilding is not at all feasible or sensible in this case.
Bathroom or toilet
All the study participants had a bathing and toilet area in their house. However, almost all the study participants usually faced a lot of problems in accessing the toilets. The pre-made toilets in the house had to be modified to suit their needs; For example, wall attachments had to be added so that they could hold on to them while bathing or when transferring onto the toilet seat. A few participants used Indian-style toilets, which were difficult to access with a wheelchair, and usually, they tried to access the toilets while sliding on the floor which also caused hygiene-related problems. This is one of the reasons that different hygiene-related diseases were common among them.
The people who could afford had special bathing and toilet chairs. Transferring to these chairs is a challenging task.
Moreover, in a typical house/flat the bathing and toilet areas usually have a height difference in the form of a low step for the bathing area. This adds to the difficulty when using a bathing chair. Moreover, the entry door to the bathroom usually has a small height barrier to prevent water from entering the room, which again adds to a lot of difficulty in accessing the toilet or bathroom in a wheelchair.
Furthermore, the washbasins and sinks in the washrooms are made with the idea that a person standing will be using them and thus it is not accessible for the person sitting in a wheelchair to access them, for example for brushing their teeth or washing their face. A few of our study participants had remodeled their bathroom sink to a slightly lower height. However, this decreases its usability for other family members.
During the interviews, women participants elaborated more on the difficulties in accessing toilets when they are outside their houses. Many of the female participants restricted their travel and outdoor time to less than 4 h so that they could come back home and use their toilets. This was one of the main reasons cited by women for not pursuing jobs/higher studies.
Drying area or service balcony
Dryers are extremely uncommon in India and are quite expensive to buy and use. Thus, drying of clothes in an apartment or flat is usually done under the sun in the service area or balcony on wires hung near the roof (Figure 4). Since the hanging wires are at a significant height, persons in wheelchairs cannot access them. However, a few of the study participants had developed indigenous solutions for hanging clothes using wooden sticks as can be seen in Figure 4.
Common area rooms and bedrooms
The major problems faced by study participants in these places were common and mostly related to transferring from wheelchair to bed, sofa, chair, or difficulty in accessing storage in high-height cupboard shelves.
Outdoor area
Most of the participants worked or studied. They lived quite close to the place of study/work and their daily travel was less than 5 km. A few of the study participants (all men) were traveling salespersons as well. Table 5 summarizes the daily travel distance commuted by the study participants.
For travelling almost all of the study participants used their means and did not travel much by public transport, if at all. The reasons were irregular timings and inaccessibility of public transport or public places via wheelchairs. This was also noted in the NSS survey. Mobility devices currently used by the study participants are summarized in Table 6. Out of the 69 study participants, 35 owned multiple mobility devices. The participants who owned motorized vehicles mostly owned a secondary mobility device, a wheelchair. A few of them also had calipers, which were useful for them to access stairs and get in and out of cars or their motor vehicle or tricycle.
Even though over 80% of the study participants owned an outdoor mobility device (tricycle, motorized, two-wheeler with side wheels or car), the majority of the devices could not be used in all weather conditions.
Ahmedabad City and surrounding areas have semi-arid weather conditions with three main seasons, namely summer, rainy, and winter. Summers are dry and hot with temperatures in the range of 28◦C to 48◦C. They last from March-June and September-October intervening in between the monsoon/rainy season during July-August.
Rainy season witness heavy rainfall which mostly leads to water-logging of roads, rendering them completely inaccessible by most vehicles. Even on days of moderate rainfall or days of hot summer with very bright sun, it is difficult to use the tricycle or motorized two-wheeler with side wheels, since they lack a roof.
The winter season is mild and usually lasts from November to February. The temperature ranges from 12◦C −33◦C, with nights being colder than the days which are mostly sunny. The visibility is over 1 km in the region during the summer and winter seasons. It can decrease to less than 50 m during the rainy season especially during moderate to heavy rainfall spells. Thus, visibility is not a serious issue for most of the year.
Given that roads in and around Ahmedabad can be quite busy with traffic with narrow passages or unpaved, wheelchairs are quite unsafe as well as inconvenient for outdoor use. Tricycles were a quite popular means of transport due to their affordability, even though they are quite slow, physically draining to use, and difficult to maneuver as told by our interviewees.
A motorized two-wheeler with side wheels being slightly expensive is the second most popular outdoor mobility device after the tricycle. Most of our study participants had bought it after they had used the tricycle for a few years and had become more economically stable. However, a few study participants faced problems while using it.
One study participant had a deformed spinal cord so their body height was smaller compared to normal users and he found the steering height high which is designed for a normal person. His arms even pained due to the force required to steer the motor vehicle with attached side wheels.
Another study participant would lose a bit of body stability when applying brakes, since he could not use his feet to maintain his balance, even with the side wheels. Transferring onto and out of all three outdoor mobility devices is quite challenging as well.
Object transportation
The ability to store and carry objects of daily use and shopping safely and conveniently is an important and necessary function of an outdoor mobility device. Cars are the most convenient and secure for object transportation and have the added benefit of being able to share the ride with co-passengers. The motorized two-wheeler has a limited storage capacity, it is especially difficult to carry heavy items or items of large sizes or secure them, although they take with them one co-passenger. The tricycles do not come with storage or any place to secure them and usually one cannot carry any co-passengers other than possibly small children but there are still some safety concerns for that. The study participants, mainly the users of the tricycles faced a lot of difficulty in carrying even lunch boxes or school bags/university textbooks with them on their tricycles.
Socio-cultural environment
Other than facing difficulties with the physical environment, the study participants faced numerous challenges because of the outright adverse attitude or ignorance of the people around them. There is a lack of sensitivity in society which does not support the social inclusion of persons with special needs to a larger extent.
A few study participants did not go out much on social occasions as the mobility devices made them feel uncomfortable. Also, they were not very welcome to participate in social or festive occasions as they were considered inauspicious. Moreover, one of the study participants explained that while using a wheelchair in social or public places she felt she was slow and could not match up with the pace of people and thus felt left out or out of place. Another (female) participant responded that they had difficulty in using their assistive devices with the traditional attire (a saree/lehenga), which they wanted to wear for a festive occasion. Thereby they felt a bit alienated.
Discussion
This study advances the work done in a previous article [2] in the region of Ahmedabad City, India in 1998 after over 20 years and fills in the gaps in studies identified in the literature [9] on the needs in indoor environment for persons with disability. Other than the above two cited articles no systematic study was conducted in India about the needs and user experience of the assisted devices. The results of this article identified many areas in which improvement is urgently needed to enhance the quality of life.
Accordingly, there are two main approaches in research to improve the quality of life of people living with locomotor disabilities. First, to create accessible infrastructure for example having ramps along with stairs or attaching elevators to access buildings, having doorways/hallways of sufficient width (in modern housing, there can be narrow doorways and passage or narrow balconies, due to high real estate prices), arrangement of furniture so that it does not hamper movement, accessibility of storage, we will call this generically as table height wheelchair accessible infrastructure. According to Saha et al. [10], this is how one should design indoor spaces.
The second approach is to introduce technological innovations in the design of assistive technologies that help in adapting to the available infrastructure.
In the Indian context, or even more generally in low-resourced settings, there is far better reach of adaptive assistive technologies than hoping for large-scale infrastructure changes. Even after it has been mandated by the Government of India to have accessible infrastructure, more than 63% of the persons who accessed public buildings faced difficulties in accessing them according to the NSS survey, a similar number exists for public transport. Long-distance journeys are virtually impossible for persons with disabilities on either trains or buses. Almost none have ramps to access the coach or seats on wheelchairs, passages are so narrow with no safety handles anywhere to keep steady. Toilets are inaccessible on most of the trains, with no wall attachments or any disability-friendly safety feature given that the trains also shake significantly. These problems are further aggravated by the issue that there are no standard guidelines on even manual wheelchairs that would fix the width range or basic features of the wheelchairs. Such guidelines are immediately needed so that most of the infrastructure (e.g. doorways of trains, houses) can be built keeping in mind the standard ranges for such devices. However, as the WHO guidelines have advised [1], such standards should be set according to the Indian context and further research is long due. As also highlighted in a study [2], wheelchairs should not restrict the sitting positions of a person to just one or two as various tasks require different seating positions.
Given that, not all infrastructure can be modified, nor would one want to modify it, given that everything at table height is not very convenient to use for a person standing a few technological innovations in the wheelchair technology would help us reach a good middle ground. For example, in offices, research labs, or working space environments, a space that has been ignored a lot in the context of disability-friendly designs, actually it is not quite feasible to have storage at sitting wheelchair height only. One would also require efficient use also high-height storage, for such needs it is better to modify the wheelchair can have adjustable height, as we have designed in [8]. Another such technological innovation is a standing wheelchair affordably designed in India [11] or a stair-climbing wheelchair [12]. The need assessment study of [2] also led to the development of a ground mobility device for women. A few of our study participants (actually both men and women) also owned a ground mobility device, it was quite helpful and convenient for them for indoor use but caused back pain after long-term use due to no back support. The problems highlighted above also occur in other countries, and the research done there can be adapted suitably in the Indian context, for example for the transfer of a wheelchair on to a train, a new assistive device has been developed in Japan [13].
As discussed in the results section above, mobility is severely restricted for everyone in monsoon, and so unless the infrastructure is improved at the level of planning of roads, we think it is not very beneficial to improvise on that part of the mobility device usability. Rather it would be greatly beneficial for persons with disability to have features on a wheelchair that will improve upon the ability to transfer from a wheelchair to another chair, bed, or toilet and to improve indoor accessibility features. Not much research has been done in the Indian context on this point.
Lastly, to improve the quality of life of a person with a disability, the stigma associated with disabilities has to be addressed at the level of society and the sensitivities of the general public have to be enhanced. Awareness drives by either NGOs or governmental organizations will benefit both the general public as well as persons with disabilities in knowing their rights and responsibilities as well as preparing the ground for their economic as well as social assimilation into society.
Conclusion
This study attempted to understand the everyday challenges of wheelchair users. It noted the educational background, assistive device preferences, health conditions, and socio-economic and physical environments of participants. The mixture of qualitative and quantitative data analysis showed that the major features that the Indian wheelchair users wanted were the ability to adjust the height of the chair, the ability to reach objects without too much maneuvering of the wheelchair, ease of transfer from wheelchair to toilet seat and back, a smaller number of transfers required and also to meet outdoor needs. This led us to conclude that a wheelchair which can be used in both indoor and outdoor settings was one of the most imminent needs for wheelchair users in the Indian context. Moreover, since the outdoor settings in India differ a lot from those of the more developed countries, these chairs should be developed and designed in India.
Limitations, methodological considerations, and future research
Some of the results of the survey are biased since our participant selection was not random and may not reflect the general needs of the disabled population. However, it does highlight a very important point; The independence and community participation that outdoor mobility devices bring and the positive effects it has on the user, namely access to education and economic independence.
Since one size fits all is not how wheelchair design should work [19], we confirm that even for this positively skewed education community, there are a lot of unmet needs that need to be addressed and other surveys should be conducted similarly in other Indian cities. Another factor for conducting such a study was to understand and find out the unmet needs of the knowledge workforce with disability so that when a person loses the ability to perform their previous work due to the disability due to some disease or injury, their transition (or upskill) to knowledge workforce with a bit more ease. They should not face difficulty due to a lack of suitable assistive devices for their economic and social independence.
The data we had collected had some gaps in between and it was self-reported, so there are chances for discrepancies, especially concerning medical facts or economic facts. A random study conducted out of participants selected from a database, which is fed information about the health status directly from the hospitals/medical facility would be of great help.
Ethical Considerations
Compliance with ethical guidelines
The consent of participants was taken for voluntary participation in the study. Each participant was briefed about the scope of the study. The confidentiality of the personal data of the participants was ensured. The participants were not subject to any harm during or after the study.
Funding
This article extracted from PhD dissertation of Harshul Brahmbhatt, approved by Gujarat Technological University. This study was financially supported by the Government of Gujarat under a startup grant.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Gujarat Technological University and the Government of Gujarat for their financial support.
References
- World Health Organization. Guidelines on the provision of manual wheelchairs in less resourced settings. Genev: WHO; 2008. [Link]
- Mulholland SJ, Packer TL, Laschinger SJ, Olney SJ, Panchal V. The mobility needs of women with physical disabilities in India: A functional perspective. Disability and Rehabilitation. 1998; 20(5):168-78. [DOI:10.3109/09638289809166078] [PMID]
- Government of India Ministry of Health and Family Welfare. National family health survey (NFHS-5) 2019-21. New Delhi: Government of India Ministry of Health and Family Welfare; 2020. [Link]
- Office of the Registrar General and census Commissioner, India Ministry of Home and Affairs, Government of India. Census tables. New Delhi: Government of India; 2001. [Link]
- Office of the Registrar General and census Commissioner, India Ministry of Home and Affairs, Government of India. Census tables. New Delhi: Government of India; 2011. [Link]
- Telecom Regulatory Authority of India. The Indian telecom services performance indicators April – June, 2020. Telecom Regulatory Authority of India: New Delhi; 2020. [Link]
- Government of India. Persons with disabilities in India. NSS 76th round (July – December 2018). Government of India: New Delhi; 2020. [Link]
- Brahmbhatt HB, Design of indoor-outdoor mobility wheelchair for low resourced settings. Jordan Journal of Mechanical and Industrial Engineering. 2023; 17(04):461–9. [DOI: 10.59038/jjmie/170401]
- Borade N, Ingle A, Nagarkar A. Lived experiences of people with mobility-related disability using assistive devices. Disability and Rehabilitation: Assistive Technology. 2021; 16(7):730-4. [DOI:10.1080/17483107.2019.1701105] [PMID]
- Saha R, Dey A, Hatoj M, Podder S. Study of Wheelchair operations in Rural areas covered under the District Rehabilitation Centre (DRC) scheme. Indian Journal of Disability and Rehabilitation. 1990; 57-87. [Link]
- Shaikh-Mohammed J, Dash SS, Sarda V, Sujatha S. Design journey of an affordable manual standing wheelchair. Disability and Rehabilitation. Assistive Technology. 2023; 18(5):553-63. [PMID]
- Behera PK, Gupta A. Novel design of stair climbing wheelchair. Journal of Mechanical Science and Technology. 2018; 32:4903-8. [DOI:10.1007/s12206-018-0938-6]
- Kim K, Kobayashi H, Matsumoto K, Hashimoto T. Development of train-boarding assistance device for wheelchair. Journal of Robotics and Mechatronics. 2022; 34(1):167-76. [DOI:10.20965/jrm.2022.p0167]
- Kirby RL, Cooper RA. Applicability of Wheel-chair skills program to the Indian context. Disability and Rehabilitation. 2007; 29(11-12):969-72. [PMID]
- Desai S, Mantha S, Phalle V. Comprehensive needs assessment study and deployment of QFD targeted at new wheelchair design. Iranian Rehabilitation Journal. 2017; 15(4):377-88. [DOI:10.29252/nrip.irj.15.4.377]
- Magnusson L, Ghosh R, Jensen KR, Göbel K, Wågberg J, Wallén S, et al. Quality of life of prosthetic and orthotic users in South India: A cross-sectional study. Health and Quality of Life Outcomes. 2019; 17(1):50. [DOI:10.1186/s12955-019-1116-y] [PMID]
- Gupta N, Raja K. Expectations of persons with paraplegia regarding their care in India: A qualitative study. Spinal Cord Series and Cases. 2017; 3:17042. [DOI:10.1038/scsandc.2017.40] [PMID]
- Lysack JT, Mulholland SJ, Panchal V, Wyss UP, Packer TL. Designing a short range wheeled mobility device for women in India. Proceedings of the Rehabilitation Engineering Society of North America, 1996 Conference, Salt Lake City. 1996:405-7.
- Gupta S, Meershoek A, Witte L. A narrative review of the government wheelchair provision system in India. International Journal of Environmental Research and Public Health. 2021; 18(10):5109. [DOI:10.3390/ijerph18105109] [PMID]
Article type: Original Research Articles |
Subject:
methodology in rehabilitation
Received: 2023/04/2 | Accepted: 2023/07/25 | Published: 2024/06/1
Received: 2023/04/2 | Accepted: 2023/07/25 | Published: 2024/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
