
988368
Fri, May 17, 2024

Volume 21, Issue 4 (December 2023)
Iranian Rehabilitation Journal 2023, 21(4): 601-610 |
Back to browse issues page


Ethics code: IR. TUMS.FNM. REC.1399.174
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Amiri M, Dalvand H, Rassafiani M, Almasi A. The Relationship Between Manual Ability and Self-care in Children Aged 1-8 Years With Spastic Cerebral Palsy: A Cross-sectional Study. Iranian Rehabilitation Journal 2023; 21 (4) :601-610
URL: http://irj.uswr.ac.ir/article-1-1944-en.html
URL: http://irj.uswr.ac.ir/article-1-1944-en.html



1- Department of Occupational Therapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
2- School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Bathurst, Australia.
3- Department of Epidemiology, School of Health, Arak University of Medical Sciences, Arak, Iran.
2- School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Bathurst, Australia.
3- Department of Epidemiology, School of Health, Arak University of Medical Sciences, Arak, Iran.
Full-Text [PDF 552 kb]
(187 Downloads)
| Abstract (HTML) (933 Views)
Full-Text: (55 Views)
Introduction
Cerebral palsy (CP) includes a group of non-progressive and non-contagious neurological disorders that cause physical and cognitive disabilities in human development and influence performance, participation, mobility, posture, muscular strength and endurance, visual system, perception, communication and behavior [1, 2]. The prevalence of this disorder in Iran is reported to be 2.06 cases per 1000 live births [3]. Sensory-motor damage in the upper limb mainly causes problems in activities of daily living (ADLs) [4]. Compared to gross motor function, less attention is often paid to manual ability and statistics show that manual ability is challenging in approximately 50% of children with CP [4, 5]. Limitations in manual ability can cause restrictions in performing and completing ADLs [6]. Limitations in manual ability, regardless of gross motor function, have a crucial impact on the participation of people with CP [7]. The manual ability classification system (MACS) is directed at children with CP aged 4 to 18 years based on the way of using two hands when manipulating objects during ADLs [8]. Recently, this classification system has been expanded and can also check the manual ability of children with CP aged 1 to 4 years, which is called the mini-manual ability classification system (Mini-MACS) [9].
On the other hand, children must learn the ability to take care of themselves, and this develops at the age of 8 years. The pediatric evaluation of disability inventory (PEDI) is one of the most common tools to evaluate performance in children with CP [10]. PEDI indicates the functional status and occupational performance of children with disabilities in the self-care, mobility, and social function domains [11]. The study conducted by Kuijper et al. indicated an inverse relationship between the level of ability to perform self-care activities and the severity of the damage to manual ability [12]. The study results of Burges et al. showed that children who scored the highest in self-care based on the PEDI demonstrated the highest level of manual ability [13].
One of the crucial priorities of children with CP and their families is independence in performing ADLs, especially self-care. Therefore, it is required to know about the ability level of children and the expected level of these abilities in performing ADLs. Moreover, considering the difference in the level of providing rehabilitation and medical services in developing countries and developed countries and cultural differences regarding daily activities, such as going to the toilet, it is essential to determine the relationship between manual ability and self-care in children with spastic CP. So far, no study has been conducted on the use of the Mini-MACS. Therefore, this study was conducted to investigate the relationship between manual ability and self-care in children aged 1 to 8 years with spastic CP.
Materials and Methods
This study was a cross-sectional (descriptive and analytical) research. The study population included all children with spastic CP aged 1-8 years who were referred to public and private occupational therapy clinics in Tehran City in 2022 and were included in the study using the convenience sampling strategy. The inclusion criteria included the diagnosis of the spastic CP by a pediatric neurologist, age between 1 and 8 years, and having literate parents. The exclusion criteria included botulinum toxin injection in the last 6 months and surgery in the last 9 months. Evaluation tools were MACS, Mini-MACS scales, PEDI, and cognitive ability estimation forms designed in the SPARCLE project.
Manual ability classification system (MACS)
The MACS is designed based on the child’s performance in performing ADLs and how to use both hands when using objects for children with CP aged 4 to 18 years in five levels [8]. Children at level 1 control objects easily and without restrictions, and independence is maintained in ADLs. At level 5, the child cannot control objects [14]. This tool was translated into Persian by Riyahi et al. [14] and its validity and reliability were measured (intraclass correlation coefficient [ICC]=0.97). The MACS scale has recently been expanded and can also assess the manual ability of children with CP from 1 to 4 years old, which is called the mini-manual ability classification system [13]. The validity and reliability of this scale was cofirmed by Ryahi and et al. [15].
Pediatric evaluation of disability inventory (PEDI)
PEDI is one of the most common tools to assess occupational performance in children with CP [10]. PEDI indicates the functional status of children with disabilities in the self-care, mobility, and social function domains [11]. The PEDI evaluates these domains in three separate scales, including 197 items related to functional skills, 20 items related to caregiver assistance, and 20 items related to modification [11]. The validity and reliability of this inventory in the children with CP were confirmed by Moradi Abbasabadi et al. (Cronbach’s α 0.98-0.94) [16, 17].
Cognitive level form
This form is derived from the impairment form in the SPARCLE project, which measures cognitive ability level based on ICD-10 in three categories, including cognitive ability level >70, between 50-70, and <50 [18]. This form is completed by the family of participants. If the cognitive ability level is 50-70, it is mild, and if the cognitive ability level is <50, it is severe [19]. Nobakht et al. investigated the validity of this test in children with CP [18].
After obtaining permission to conduct the research from the Research and Technology Vice-Chancellor of Tehran University of Medical Sciences, the authors referred to the public and private occupational therapy centers in Tehran City to collect data. Then, using the MACS and Mini-MACS scales, children were classified in the age groups of 1 to 2 years, 2 to 4 years, 4 to 6 years, and 6 to 8 years in five levels of MACS. Then, the PEDI was applied and caregivers part was completed by the children’s family, and the functional skills were completed by the occupational therapist, then, the score related to self-care was collected in two parts, functional skills and caregiver assistance. Each item of the PEDI in the self-care part was assigned two scores of 1 (ability) or 0 (disability). Also, a score of 0 (full assistance) to 5 (full independence) was considered for caregiver assistance items. The collected data was analyzed using Stata software, version 14 by descriptive statistics (frequency and Mean±SD) and analytical statistics (correlation coefficient, chi-square, independent t-test, Fisher’s test, and one-way analysis of variance and regression if the data was normal). Non-parametric tests were used in the case of non-normal distribution of the variables.
Results
In this study, 125 children aged 1 to 8 years with spastic CP were examined, and 71 of them (56.8%) were boys. The average age of the children was 54.2±15 months. Table 1 presents the demographic characteristics of children with spastic CP.

According to the results, the average level of MACS of children with spastic CP in this study was 3.01 in the range of 1 to 5. The average self-care in these children was 49.65 with a minimum and maximum of 2 and 113, respectively.
Table 2 presents the relationship between the gender and education level of the main caregiver with the levels of MACS in children with spastic CP.

The results of Table 2 indicated that a significant difference was observed between boys and girls in the levels of MACS (P=0.031). Also, no significant difference was observed in the levels of children’s MACS according to the education levels of the main caregiver (P=0.772). A significant difference was observed in the levels of MACS in these children according to cognitive ability level (P<0.001). A significant relationship was observed between the age of children with spastic CP and their levels of MACS.
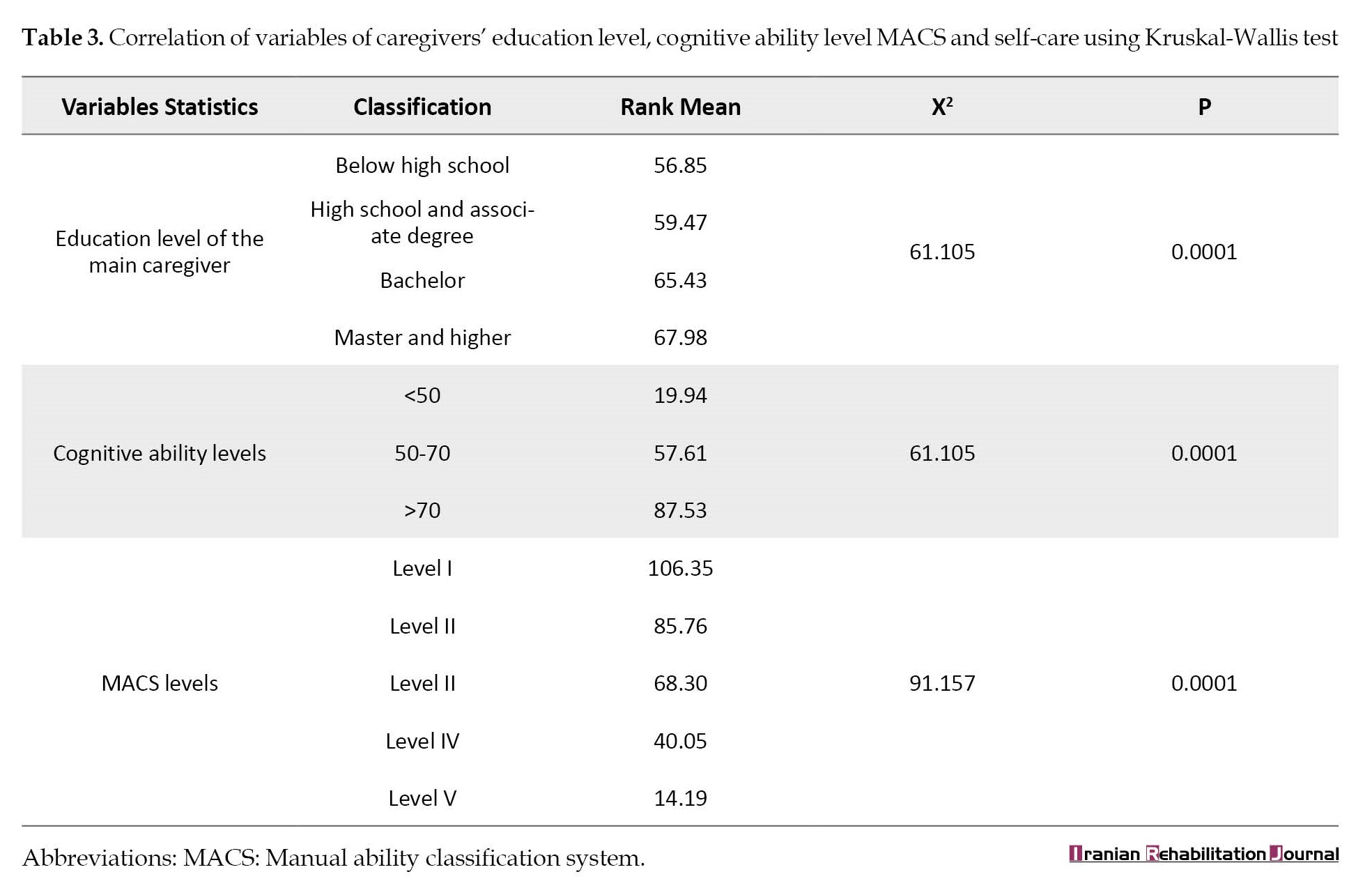
In this study, the relationship between the age of children with spastic CP and the children’s self-care was analyzed using the Spearman correlation test, and a statistically significant relationship was observed between the age and the variables of the children’s self-care (P<0.001); that is, as the age of the children increases, the ability to take care of themselves increases significantly. The relationship between gender and self-care in children with spastic CP was analyzed using the Mann-Whitney test, and no significant difference was observed between boys and girls in self-care (P=0.455). Based on the result of Table 3, with the change in the education level of the main caregiver, no significant difference was observed in the self-care of children with spastic CP (P=0.673); however, with the increase in children’s cognitive ability level, the levels of MACS, and in children with spastic CP, the ability to take care of themselves increased significantly (P<0.001).
The results test revealed a significant difference between different levels of cognitive ability level in terms of self-care (P<0.001). In comparing cognitive ability levels, a significant difference was observed among levels <50, between 50-70, below 50 and >70, between 50-70, and >70. Regarding the children’s MACS levels, no statistically significant difference was found in self-care between levels I and II, levels II and III, levels III and IV, and levels IV and V (Table 4).

A regression test was used to investigate the significant relationship between children’s mobility and their self-care, and the R2 value was equal to 0.773, which showed that 77% of changes in the self-care variable were described by children’s mobility variables. It showed the linearity of these relationships. Also, according to the regression coefficients and the beta coefficient, the mobility variable with an impact factor of 0.88 had a significant effect in predicting the self-care of children. To investigate the significant relationship between the variables of age, level of cognitive ability, level of MACS, and mobility of the studied children with their self-care, a regression test was performed and the R2 value was obtained equal to 0.881, which showed that 88% of changes in the self-care variable is described by these variables.
A significant relationship was observed between the variables of age, MACS level, and mobility of children with self-care ability (P<0.0001); however, the effect of children’s level of cognitive ability on their self-care ability was not significant (P=0.815) and did not affect on predicting the dependent variable. According to the beta coefficients and comparing its values, the factor of MACS level and mobility with the highest beta values (-0.530 and 0.512, respectively) had a greater contribution in predicting self-care ability compared to other variables (Table 5).

Discussion
Based on the result of this study, with the increase in the MACS level of children with spasitc CP, their performance in self-care increased significantly. Based on the study results of Kuijper et al. [12] and Burges et al. [13], an inverse relationship was observed between the level of self-care and the severity of injury in the MACS, which was consistent with the results of the present study. In the study conducted by Gunel et al. [20], the self-care of children with disabilities increased significantly with the increase in the level of MACS, which is consistent with our results.
According to the results of this study, with the increase in the level of cognitive ability of children aged 1 to 8 years with spastic CP, the self-care of these children was increased. The significant relationship between cognitive ability level and self-care has not been specifically investigated in children with CP; however, Himmelmann et al. [21] and Türkoğlu et al. [22] mentioned the relationship between the higher severity of CP and lower cognitive ability level in their studies. The critical difference of these studies is the dearth of reliable information in which the specific norms of society are considered for the intellectual evaluation of children with CP. For example, different assessment materials and tests are needed for children who have visual and communication problems with a high level of motor difficulty [23], and different systems for evaluating the cognitive ability level of children with CP and lead to different results.
The results of this study indicated that in children with spastic CP aged 1 to 8 years, no significant relationship was observed between the education level of the main caregiver and the child’s performance level in self-care. Studies that have assessed demographic variables about children with CP have examined the child’s education level or socioeconomic variables, and no similar study was found that examined the education level of the main caregiver about self-care in children with CP. Considering that it is expected that with the increase in the education level of the caregivers, their awareness and knowledge regarding the type of disease, the condition of the children, and the type of behavioral intervention will increase and consequently the ability of the children under their care in functional skills will be strengthened and increased. However, a different result was obtained and this relationship was not significant.
According to the results of the research, no significant difference was observed between boys and girls in self-care. Jarvis et al. reported a higher probability of birth of male infants with severe CP compared to female infants [24]. In the study conducted by Pfeifer et al., no significant difference was observed between gender and gross motor performance [25-27]. However, no independent studies were found that investigated the relationship between the gender of children with CP and self-care. The differences mentioned in this study can probably be due to cultural differences, different age ranges, scales, and different populations studied.
According to the results, as the age of the children increased, their self-care increased significantly (P<0.05). Öhrvall et al. realized a significant relationship between age and self-care, which was consistent with the results of the present study [28]. In another study conducted by Phipps and Roberts, a significant relationship was found between age and self-care [26], which was consistent with our results, although a smaller age range was examined in the present study. Østensjø et al. recognized that preschool children with CP were unable to perform functions individually [27]. However, when older children and adolescents were examined in the analyses, children’s MACS and gross motor function classification system (GMFCS E & R), and subsequently self-care and mobility skills increased significantly with increasing age [28].
The regression analysis results showed that 88% of the changes in the self-care variable were described by the variables of age, MACS level, level of cognitive ability, and mobility of the children. According to the regression analysis results, the variables of age, MACS level, and mobility of children were significant with self-care (P<0.05), while the effect of children’s level of cognitive ability on their self-care was not significant (P>0.05), and it did not affect predicting the dependent variable. Finally, MACS level and mobility had a greater contribution to the prediction of self-care compared to other variables, respectively. In the study conducted by Öhrvall et al., the level of MACS (66%) was the strongest predictor for self-care [28], which is consistent with the results of this study. Based on the results, the level of MACS describes 53% of changes in the self-care. This may be partly explained by the item content of the PEDI. It can be assumed that these results originate from the fact that self-care includes items that do not measure manual ability. In addition, several factors that were not examined in this study affect the achievement of functional skills, such as cognition, motivation, and attention [9, 27, 29, 30, 31].
The limitations of this study included the problems of access to children with spastic CP and the cooperation of clinic managers, which their satisfaction and cooperation were obtained to a large extent by justifying and explaining the importance of research and the application of the results to promote and improve the condition of children. The data collection period coincided with the outbreak of COVID-19, which caused problems in children’s access and completing the data, and the data was collected by following the protocols. The long time for the tests and the problems of the clients’ traveling were among the other limitations of the study.
Conclusion
According to the results, self-care was promoted significantly as children aged 1-8 years with CP increased; however, gender did not show a significant effect. By increasing children’s level of cognitive ability and increasing the level of children’s MACS, self-care increased significantly. Furthermore, the self-care was greatly influenced by the level of MACS and mobility. The results of this study showed that by strengthening manual skills, we hope to improve the conditions of children with CP by improving self-care. It is suggested that future studies investigate manual function ability, self-care, and mobility compared to the healthy or control group. Also, it is recommended to examine the effectiveness of intervention occupational therapy in enhancing the self-care, mobility, and social function of children, adolescents, and young adults with CP.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Tehran University of Medical Sciences (Code: TUMS.FNM. REC.1399.174). The information of the participants remained confidential, and if they did not want to participate in the study, their information was removed from the research data set.
Funding
This article extracted from master's thesis of Mohammad Amiri, approved by School of Rehabilitation, Tehran University of Medical Sciences. This study was financially supported by the Tehran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The authors of the article highly appreciate the children’s parents and healthcare providers who participated in the study.
References
Cerebral palsy (CP) includes a group of non-progressive and non-contagious neurological disorders that cause physical and cognitive disabilities in human development and influence performance, participation, mobility, posture, muscular strength and endurance, visual system, perception, communication and behavior [1, 2]. The prevalence of this disorder in Iran is reported to be 2.06 cases per 1000 live births [3]. Sensory-motor damage in the upper limb mainly causes problems in activities of daily living (ADLs) [4]. Compared to gross motor function, less attention is often paid to manual ability and statistics show that manual ability is challenging in approximately 50% of children with CP [4, 5]. Limitations in manual ability can cause restrictions in performing and completing ADLs [6]. Limitations in manual ability, regardless of gross motor function, have a crucial impact on the participation of people with CP [7]. The manual ability classification system (MACS) is directed at children with CP aged 4 to 18 years based on the way of using two hands when manipulating objects during ADLs [8]. Recently, this classification system has been expanded and can also check the manual ability of children with CP aged 1 to 4 years, which is called the mini-manual ability classification system (Mini-MACS) [9].
On the other hand, children must learn the ability to take care of themselves, and this develops at the age of 8 years. The pediatric evaluation of disability inventory (PEDI) is one of the most common tools to evaluate performance in children with CP [10]. PEDI indicates the functional status and occupational performance of children with disabilities in the self-care, mobility, and social function domains [11]. The study conducted by Kuijper et al. indicated an inverse relationship between the level of ability to perform self-care activities and the severity of the damage to manual ability [12]. The study results of Burges et al. showed that children who scored the highest in self-care based on the PEDI demonstrated the highest level of manual ability [13].
One of the crucial priorities of children with CP and their families is independence in performing ADLs, especially self-care. Therefore, it is required to know about the ability level of children and the expected level of these abilities in performing ADLs. Moreover, considering the difference in the level of providing rehabilitation and medical services in developing countries and developed countries and cultural differences regarding daily activities, such as going to the toilet, it is essential to determine the relationship between manual ability and self-care in children with spastic CP. So far, no study has been conducted on the use of the Mini-MACS. Therefore, this study was conducted to investigate the relationship between manual ability and self-care in children aged 1 to 8 years with spastic CP.
Materials and Methods
This study was a cross-sectional (descriptive and analytical) research. The study population included all children with spastic CP aged 1-8 years who were referred to public and private occupational therapy clinics in Tehran City in 2022 and were included in the study using the convenience sampling strategy. The inclusion criteria included the diagnosis of the spastic CP by a pediatric neurologist, age between 1 and 8 years, and having literate parents. The exclusion criteria included botulinum toxin injection in the last 6 months and surgery in the last 9 months. Evaluation tools were MACS, Mini-MACS scales, PEDI, and cognitive ability estimation forms designed in the SPARCLE project.
Manual ability classification system (MACS)
The MACS is designed based on the child’s performance in performing ADLs and how to use both hands when using objects for children with CP aged 4 to 18 years in five levels [8]. Children at level 1 control objects easily and without restrictions, and independence is maintained in ADLs. At level 5, the child cannot control objects [14]. This tool was translated into Persian by Riyahi et al. [14] and its validity and reliability were measured (intraclass correlation coefficient [ICC]=0.97). The MACS scale has recently been expanded and can also assess the manual ability of children with CP from 1 to 4 years old, which is called the mini-manual ability classification system [13]. The validity and reliability of this scale was cofirmed by Ryahi and et al. [15].
Pediatric evaluation of disability inventory (PEDI)
PEDI is one of the most common tools to assess occupational performance in children with CP [10]. PEDI indicates the functional status of children with disabilities in the self-care, mobility, and social function domains [11]. The PEDI evaluates these domains in three separate scales, including 197 items related to functional skills, 20 items related to caregiver assistance, and 20 items related to modification [11]. The validity and reliability of this inventory in the children with CP were confirmed by Moradi Abbasabadi et al. (Cronbach’s α 0.98-0.94) [16, 17].
Cognitive level form
This form is derived from the impairment form in the SPARCLE project, which measures cognitive ability level based on ICD-10 in three categories, including cognitive ability level >70, between 50-70, and <50 [18]. This form is completed by the family of participants. If the cognitive ability level is 50-70, it is mild, and if the cognitive ability level is <50, it is severe [19]. Nobakht et al. investigated the validity of this test in children with CP [18].
After obtaining permission to conduct the research from the Research and Technology Vice-Chancellor of Tehran University of Medical Sciences, the authors referred to the public and private occupational therapy centers in Tehran City to collect data. Then, using the MACS and Mini-MACS scales, children were classified in the age groups of 1 to 2 years, 2 to 4 years, 4 to 6 years, and 6 to 8 years in five levels of MACS. Then, the PEDI was applied and caregivers part was completed by the children’s family, and the functional skills were completed by the occupational therapist, then, the score related to self-care was collected in two parts, functional skills and caregiver assistance. Each item of the PEDI in the self-care part was assigned two scores of 1 (ability) or 0 (disability). Also, a score of 0 (full assistance) to 5 (full independence) was considered for caregiver assistance items. The collected data was analyzed using Stata software, version 14 by descriptive statistics (frequency and Mean±SD) and analytical statistics (correlation coefficient, chi-square, independent t-test, Fisher’s test, and one-way analysis of variance and regression if the data was normal). Non-parametric tests were used in the case of non-normal distribution of the variables.
Results
In this study, 125 children aged 1 to 8 years with spastic CP were examined, and 71 of them (56.8%) were boys. The average age of the children was 54.2±15 months. Table 1 presents the demographic characteristics of children with spastic CP.
According to the results, the average level of MACS of children with spastic CP in this study was 3.01 in the range of 1 to 5. The average self-care in these children was 49.65 with a minimum and maximum of 2 and 113, respectively.
Table 2 presents the relationship between the gender and education level of the main caregiver with the levels of MACS in children with spastic CP.
The results of Table 2 indicated that a significant difference was observed between boys and girls in the levels of MACS (P=0.031). Also, no significant difference was observed in the levels of children’s MACS according to the education levels of the main caregiver (P=0.772). A significant difference was observed in the levels of MACS in these children according to cognitive ability level (P<0.001). A significant relationship was observed between the age of children with spastic CP and their levels of MACS.
In this study, the relationship between the age of children with spastic CP and the children’s self-care was analyzed using the Spearman correlation test, and a statistically significant relationship was observed between the age and the variables of the children’s self-care (P<0.001); that is, as the age of the children increases, the ability to take care of themselves increases significantly. The relationship between gender and self-care in children with spastic CP was analyzed using the Mann-Whitney test, and no significant difference was observed between boys and girls in self-care (P=0.455). Based on the result of Table 3, with the change in the education level of the main caregiver, no significant difference was observed in the self-care of children with spastic CP (P=0.673); however, with the increase in children’s cognitive ability level, the levels of MACS, and in children with spastic CP, the ability to take care of themselves increased significantly (P<0.001).
The results test revealed a significant difference between different levels of cognitive ability level in terms of self-care (P<0.001). In comparing cognitive ability levels, a significant difference was observed among levels <50, between 50-70, below 50 and >70, between 50-70, and >70. Regarding the children’s MACS levels, no statistically significant difference was found in self-care between levels I and II, levels II and III, levels III and IV, and levels IV and V (Table 4).
A regression test was used to investigate the significant relationship between children’s mobility and their self-care, and the R2 value was equal to 0.773, which showed that 77% of changes in the self-care variable were described by children’s mobility variables. It showed the linearity of these relationships. Also, according to the regression coefficients and the beta coefficient, the mobility variable with an impact factor of 0.88 had a significant effect in predicting the self-care of children. To investigate the significant relationship between the variables of age, level of cognitive ability, level of MACS, and mobility of the studied children with their self-care, a regression test was performed and the R2 value was obtained equal to 0.881, which showed that 88% of changes in the self-care variable is described by these variables.
A significant relationship was observed between the variables of age, MACS level, and mobility of children with self-care ability (P<0.0001); however, the effect of children’s level of cognitive ability on their self-care ability was not significant (P=0.815) and did not affect on predicting the dependent variable. According to the beta coefficients and comparing its values, the factor of MACS level and mobility with the highest beta values (-0.530 and 0.512, respectively) had a greater contribution in predicting self-care ability compared to other variables (Table 5).
Discussion
Based on the result of this study, with the increase in the MACS level of children with spasitc CP, their performance in self-care increased significantly. Based on the study results of Kuijper et al. [12] and Burges et al. [13], an inverse relationship was observed between the level of self-care and the severity of injury in the MACS, which was consistent with the results of the present study. In the study conducted by Gunel et al. [20], the self-care of children with disabilities increased significantly with the increase in the level of MACS, which is consistent with our results.
According to the results of this study, with the increase in the level of cognitive ability of children aged 1 to 8 years with spastic CP, the self-care of these children was increased. The significant relationship between cognitive ability level and self-care has not been specifically investigated in children with CP; however, Himmelmann et al. [21] and Türkoğlu et al. [22] mentioned the relationship between the higher severity of CP and lower cognitive ability level in their studies. The critical difference of these studies is the dearth of reliable information in which the specific norms of society are considered for the intellectual evaluation of children with CP. For example, different assessment materials and tests are needed for children who have visual and communication problems with a high level of motor difficulty [23], and different systems for evaluating the cognitive ability level of children with CP and lead to different results.
The results of this study indicated that in children with spastic CP aged 1 to 8 years, no significant relationship was observed between the education level of the main caregiver and the child’s performance level in self-care. Studies that have assessed demographic variables about children with CP have examined the child’s education level or socioeconomic variables, and no similar study was found that examined the education level of the main caregiver about self-care in children with CP. Considering that it is expected that with the increase in the education level of the caregivers, their awareness and knowledge regarding the type of disease, the condition of the children, and the type of behavioral intervention will increase and consequently the ability of the children under their care in functional skills will be strengthened and increased. However, a different result was obtained and this relationship was not significant.
According to the results of the research, no significant difference was observed between boys and girls in self-care. Jarvis et al. reported a higher probability of birth of male infants with severe CP compared to female infants [24]. In the study conducted by Pfeifer et al., no significant difference was observed between gender and gross motor performance [25-27]. However, no independent studies were found that investigated the relationship between the gender of children with CP and self-care. The differences mentioned in this study can probably be due to cultural differences, different age ranges, scales, and different populations studied.
According to the results, as the age of the children increased, their self-care increased significantly (P<0.05). Öhrvall et al. realized a significant relationship between age and self-care, which was consistent with the results of the present study [28]. In another study conducted by Phipps and Roberts, a significant relationship was found between age and self-care [26], which was consistent with our results, although a smaller age range was examined in the present study. Østensjø et al. recognized that preschool children with CP were unable to perform functions individually [27]. However, when older children and adolescents were examined in the analyses, children’s MACS and gross motor function classification system (GMFCS E & R), and subsequently self-care and mobility skills increased significantly with increasing age [28].
The regression analysis results showed that 88% of the changes in the self-care variable were described by the variables of age, MACS level, level of cognitive ability, and mobility of the children. According to the regression analysis results, the variables of age, MACS level, and mobility of children were significant with self-care (P<0.05), while the effect of children’s level of cognitive ability on their self-care was not significant (P>0.05), and it did not affect predicting the dependent variable. Finally, MACS level and mobility had a greater contribution to the prediction of self-care compared to other variables, respectively. In the study conducted by Öhrvall et al., the level of MACS (66%) was the strongest predictor for self-care [28], which is consistent with the results of this study. Based on the results, the level of MACS describes 53% of changes in the self-care. This may be partly explained by the item content of the PEDI. It can be assumed that these results originate from the fact that self-care includes items that do not measure manual ability. In addition, several factors that were not examined in this study affect the achievement of functional skills, such as cognition, motivation, and attention [9, 27, 29, 30, 31].
The limitations of this study included the problems of access to children with spastic CP and the cooperation of clinic managers, which their satisfaction and cooperation were obtained to a large extent by justifying and explaining the importance of research and the application of the results to promote and improve the condition of children. The data collection period coincided with the outbreak of COVID-19, which caused problems in children’s access and completing the data, and the data was collected by following the protocols. The long time for the tests and the problems of the clients’ traveling were among the other limitations of the study.
Conclusion
According to the results, self-care was promoted significantly as children aged 1-8 years with CP increased; however, gender did not show a significant effect. By increasing children’s level of cognitive ability and increasing the level of children’s MACS, self-care increased significantly. Furthermore, the self-care was greatly influenced by the level of MACS and mobility. The results of this study showed that by strengthening manual skills, we hope to improve the conditions of children with CP by improving self-care. It is suggested that future studies investigate manual function ability, self-care, and mobility compared to the healthy or control group. Also, it is recommended to examine the effectiveness of intervention occupational therapy in enhancing the self-care, mobility, and social function of children, adolescents, and young adults with CP.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Tehran University of Medical Sciences (Code: TUMS.FNM. REC.1399.174). The information of the participants remained confidential, and if they did not want to participate in the study, their information was removed from the research data set.
Funding
This article extracted from master's thesis of Mohammad Amiri, approved by School of Rehabilitation, Tehran University of Medical Sciences. This study was financially supported by the Tehran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The authors of the article highly appreciate the children’s parents and healthcare providers who participated in the study.
References
- Ashwal S, Russman BS, Blasco PA, Miller G, Sandler A, Shevell M, et al. Practice parameter: Diagnostic assessment of the child with cerebral palsy: Report of the quality standards subcommittee of the American academy of neurology and the practice committee of the child neurology society. Neurology. 2004; 62(6):851-63. [DOI:10.1212/01.WNL.0000117981.35364.1B] [PMID]
- te Velde A, Morgan C, Novak I, Tantsis E, Badawi N. Early diagnosis and classification of cerebral palsy: An historical perspective and barriers to an early diagnosis. Journal of Clinical Medicine. 2019; 8(10):1599. [DOI:10.3390/jcm8101599] [PMID]
- Joghataei M, Kazem M. [Assessment the level of community needs in welfare services on the whole country (Persian)]. Tehran: University of Social Welfare and Rehabilitation Sciences; 1990.
- Fedrizzi E, Pagliano E, Andreucci E, Oleari G. Hand function in children with hemiplegic cerebral palsy: Prospective follow-up and functional outcome in adolescence. Developmental Medicine and Child Neurology. 2003; 45(2):85-91. [DOI:10.1017/S0012162203000173] [PMID]
- Arner M, Eliasson AC, Nicklasson S, Sommerstein K, Hägglund G. Hand function in cerebral palsy. Report of 367 children in a population-based longitudinal health care program.The Journal of Hand Surgery. 2008; 33(8):1337-47. [DOI:10.1016/j.jhsa.2008.02.032] [PMID]
- Arnould C, Penta M, Thonnard JL. Hand impairments and their relationship with manual ability in children with cerebral palsy. Journal of Rehabilitation Medicine. 2007; 39(9):708-14. [DOI:10.2340/16151977-0111] [PMID]
- van Meeteren J, Roebroeck ME, Celen E, Donkervoort M, Stam HJ; Transition Research Group South West Netherlands. Functional activities of the upper extremity of young adults with cerebral palsy: A limiting factor for participation? Disability and Rehabilitation. 2008; 30(5):387-95. [DOI:10.1080/09638280701355504] [PMID]
- Riyahi A, Rassafiani M, Akbarfahimi N, Karimloo M. [Test-retest and inter-rater reliabilities of the of Manual Ability Classification System (MACS)-Farsi version in children with cerebral palsy (Persian)]. Journal of Research in Rehabilitation Sciences. 2012; 8(2):1-9. [DOI:10.22122/JRRS.V8I2.422]
- Eliasson AC, Ullenhag A, Wahlström U, Krumlinde-Sundholm L. Mini-MACS: Development of the Manual Ability Classification System for children younger than 4 years of age with signs of cerebral palsy. Developmental Medicine and Child Neurology. 2017; 59(1):72-8. [DOI:10.1111/dmcn.13162] [PMID]
- Schiariti V, Klassen AF, Cieza A, Sauve K, O'Donnell M, Armstrong R, et al. Comparing contents of outcome measures in cerebral palsy using the international classification of functioning (ICF-CY): A systematic review. European Journal of Paediatric Neurology. 2014; 18(1):1-12. [DOI:10.1016/j.ejpn.2013.08.001] [PMID]
- Haley SM. Pediatric Evaluation of Disability Inventory (PEDI): Development, standardization and administration manual. Charleston: PEDI Resarch Group; 1992. [Link]
- Kuijper MA, van der Wilden GJ, Ketelaar M, Gorter JW. Manual ability classification system for children with cerebral palsy in a school setting and its relationship to home self-care activities. The American Journal of Occupational Therapy. 2010; 64(4):614-20. [DOI:10.5014/ajot.2010.08087] [PMID]
- Burgess A, Boyd RN, Ziviani J, Ware RS, Sakzewski L. Self-care and manual ability in preschool children with cerebral palsy: A longitudinal study. Developmental Medicine and Child Neurology. 2019; 61(5):570-8. [DOI:10.1111/dmcn.14049] [PMID]
- Riyahi A, Yazdani Ghadikolaii S, Kalantari M, Jalili N, Dalvand H. [Studying the occupational therapists prediction consistency of future manual ability of 4-18 years old cerebral palsy’s childrens with manual ability classification sysyem (MACS) (Persian)]. Journal of Arak University of Medical Sciences. 2016; 19(5):51-9. [Link]
- Riyahi A, Akbarfahimi N, Sarlak N, Abdolrazaghi H, Nobakht Z. Validating the reliability and validity of the Persian Version of the mini-manual ability classification system. Journal of Rehabilitation Sciences & Research. 2023; 10(4):203-8. [Link]
- Moradi Abbasabadi M, Hosseini SA, Rezasoltani P. [Content validity of the Persian version of the Pediatric Evaluation of Disability Inventory (PEDI) (Persian)]. Journal of Research in Rehabilitation Sciences. 2014; 10(1):35-45. [DOI:10.22122/JRRS.V10I1.1360]
- Moradi Abbasabadi M, Akbarfahimi N, Hosseini SA, Rezasoltani P. [Reliability of the Persian version of the pediatric evaluation of disability inventory in 3 to 9-year old children with cerebral palsy (Persian)]. Journal of Mazandaran University of Medical Sciences. 2015; 25(130):129-37. [Link]
- Nobakht Z, Rassafiani M, Rezasoltani P, Sahaf R, Yazdani F. Environmental barriers to social participation of children with cerebral palsy in Tehran Iranian Rehabilitation Journal 2013; 11(1):40-5. [Link]
- Colver A, SPARCLE Group. Study protocol: SPARCLE--a multi-centre European study of the relationship of environment to participation and quality of life in children with cerebral palsy. BMC Public Health. 2006; 6:105. [DOI:10.1186/1471-2458-6-105] [PMID]
- Gunel MK, Mutlu A, Tarsuslu T, Livanelioglu A. Relationship among the manual ability classification system (MACS), the gross motor function classification system (GMFCS), and the functional status (WeeFIM) in children with spastic cerebral palsy. European Journal of Pediatrics. 2009; 168(4):477-85. [DOI:10.1007/s00431-008-0775-1] [PMID]
- Himmelmann K, Beckung E, Hagberg G, Uvebrant P. Gross and fine motor function and accompanying impairments in cerebral palsy. Developmental Medicine and Child Neurology. 2006; 48(6):417-23. [DOI:10.1017/S0012162206000922] [PMID]
- Türkoğlu G, Türkoğlu S, Çelik C, Uçan H. Intelligence, functioning, and related factors in children with cerebral palsy. Noro Psikiyatri Arsivi. 2017; 54(1):33-7. [DOI:10.5152/npa.2015.12676] [PMID] [PMCID]
- Yin Foo R, Guppy M, Johnston LM. Intelligence assessments for children with cerebral palsy: A systematic review. Developmental Medicine and Child Neurology. 2013; 55(10):911-8. [DOI:10.1111/dmcn.12157] [PMID]
- Jarvis S, Glinianaia SV, Arnaud C, Fauconnier J, Johnson A, McManus V, et al. Case gender and severity in cerebral palsy varies with intrauterine growth. Archives of Disease in Childhood. 2005; 90(5):474-9. [DOI:10.1136/adc.2004.052670] [PMID]
- Pfeifer LI, Silva DB, Funayama CA, Santos JL. Classification of cerebral palsy: Association between gender, age, motor type, topography and gross motor function. Arquivos de Neuro-Psiquiatria. 2009; 67(4):1057-61. [DOI:10.1590/S0004-282X2009000600018] [PMID]
- Phipps S, Roberts P. Predicting the effects of cerebral palsy severity on self-care, mobility, and social function. The American Journal of Occupational Therapy. 2012; 66(4):422-9. [DOI:10.5014/ajot.2012.003921] [PMID]
- Ostensjø S, Carlberg EB, Vøllestad NK. Motor impairments in young children with cerebral palsy: Relationship to gross motor function and everyday activities. Developmental Medicine and Child Neurology. 2004; 46(9):580-9. [DOI:10.1017/S0012162204000994] [PMID]
- Öhrvall AM, Eliasson AC, Löwing K, Ödman P, Krumlinde-Sundholm L. Self-care and mobility skills in children with cerebral palsy, related to their manual ability and gross motor function classifications. Developmental Medicine and Child Neurology. 2010; 52(11):1048-55. [DOI:10.1111/j.1469-8749.2010.03764.x] [PMID]
- Henderson A, Pehoski C. Hand function in the child: Foundations for remediation. Elsevier Mosby; 2006. [Link]
- Pashmdarfard M, Shervin Badv R. The impact of manual ability level on participation of children with cerebral palsy in life areas: A cross-sectional study. Iranian Journal of Child Neurology. 2019; 13(3):83-91. [PMID] [PMCID]
- Pashmdarfard M, Richards LG, Amini M. Factors affecting participation of children with cerebral palsy in meaningful activities: Systematic review. Occupational Therapy in Health Care. 2021; 35(4):442-79. [DOI:10.1080/07380577.2021.1938339] [PMID]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2023/04/8 | Accepted: 2023/06/27 | Published: 2023/12/1
Received: 2023/04/8 | Accepted: 2023/06/27 | Published: 2023/12/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
