
988368
Wed, Jul 29, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 639-644 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seemal P, Arshad J, Hameed S, Shafique S, Majeed M. Current Practice Patterns in the Management of Bell's Palsy Among Physiotherapists of Sargodha, Pakistan. Iranian Rehabilitation Journal 2024; 22 (4) :639-644
URL: http://irj.uswr.ac.ir/article-1-1949-en.html
URL: http://irj.uswr.ac.ir/article-1-1949-en.html



1- Department of Physical Therapy, Niazi Medical and Dental College, Sargodha, Pakistan.
2- Sargodha Institute of Health Sciences, Sargodha, Pakistan.
2- Sargodha Institute of Health Sciences, Sargodha, Pakistan.
Full-Text [PDF 522 kb]
(1203 Downloads)
| Abstract (HTML) (5772 Views)
Full-Text: (2678 Views)
Introduction
Bell’s palsy is a sudden-onset paralysis of the VII cranial nerve, characterized by a lower motor neuron lesion of the facial nerve, usually unilateral [1]. The reported incidence varies according to the geographical area. Its annual estimated incidence is around 30 per 100000 persons [2]. It is characterized by a lack of forehead wrinkles, incomplete lid closure, low eyebrow position (eyebrow ptosis), flattened nasolabial fold, and mouth corner droops [3]. The pathophysiology of Bell’s palsy includes vascular distension, edema with ischemia, and inflammation of the VII cranial nerve. Its etiology has remained unclear, but some causes have been proposed, such as vascular, autoimmune, inflammation, and viral infection, which includes reactivation of herpes zoster [4]. About 70% to 75% of patients fully recover without treatment, and early treatment enhances the chance of full recovery up to 82% [5]. A prompt diagnosis and therapy intervention seem essential for the best outcome in Bell’s palsy [6].
Bell’s palsy can be managed with both pharmaceutical and non-pharmacological treatments, as well as surgery. Corticosteroids (prednisolone), antivirals (acyclovir and valacyclovir), vitamin B12, non-steroidal anti-inflammatory drugs, and combination therapy are all examples of pharmacological treatments [7]. Non-pharmacological management includes physiotherapy, and surgical interventions include nerve decompression [8]. There is no explicit agreement on the treatment procedure for Bell’s palsy. The goal of therapy in its acute stage is to minimize inflammation with corticosteroids. After this period, antiviral drugs such as acyclovir or valacyclovir are administered to eliminate the human simplex virus. Rehabilitation treatment included electrical stimulation, neuromuscular facilitation technique, neuromuscular reeducation, infrared rays, acupuncture, facial exercise, and eye protection. If complete paralysis of the facial nerve occurs, it can be assessed by electromyography and electroneurography [9].
Physical therapy treatment for Bell’s palsy shows its effectiveness by depicting a notable increase in facial function and a quicker recovery. A combination of proprioceptive neuromuscular facilitation (PNF) and the Kabat technique with nerve stimulation improves facial asymmetry [10]. One of the previous studies about the efficacy of electrotherapy in treating Bell’s palsy shows that electrotherapy alone has unsatisfactory results but, when combined with other forms of treatment, significantly improves Bell’s palsy [11]. Evidence for managing Bell’s palsy in physical therapy is heterogeneous and limited. Descriptive data analysis from a previous study demonstrates that 78% of physiotherapists choose electrical stimulation, 34% favor mime therapy, and 72% adhere to the most recent evidence-based recommendations for treating Bell’s palsy [8]. There is ongoing discussion on the best course of therapy for Bell’s palsy, which varies from nation to nation and even between different institutions within a single country. Some commonly used physiotherapy techniques include massage therapy, mirror therapy, mime therapy, Kabat technique, infrared therapy, and low-level laser therapy. Bell’s palsy treatment varies; no consensus exists on what works best [9]. The recovery period varies according to the patient’s age, duration between treatment start and initial symptoms, severity of nerve damage, and rehabilitation after surgery [12].
Numerous studies have been done on the prevalence, risk factors, and treatment of Bell’s palsy. However, there is no study in the context of Pakistan regarding the identification of present clinical practice patterns regarding its management. So, this study aims to identify the type and number of common physiotherapy treatments for Bell’s palsy that physiotherapists of Sargodha, Pakistan, use.
Materials and Methods
A cross-sectional survey was conducted from May to August 2022. Data were obtained from 50 registered physiotherapists selected through a convenience sampling of those working in various clinical setups of Sargodha having more than 2 years of clinical experience. Novice practitioners and non-clinical physiotherapists were excluded [8]. A self-designed questionnaire was distributed to registered physiotherapists throughout Sargodha utilizing various internet platforms and by visiting their clinical setups in person. It was designed after searching literature with similar objectives for physiotherapists to assess current physical therapy practice patterns of Bell’s palsy by gathering all necessary information, including demographics, level of education, years of experience, and management strategies regarding physical therapy treatment of Bell’s palsy. Data were analyzed using SPSS software, version 20.1.0. Qualitative data, such as age, was presented as mean and standard deviation. Descriptive statistics were computed as frequency tables and graphs with percentages.
Results
In this cross-sectional observational study, 50 physiotherapists working in various clinical setups of Sargodha were included. The Mean±SD age of participants was 26.84±2.207 years. There were 42% male and 58% female physiotherapists. Almost 78% of physiotherapists had two years of clinical experience. About 18% had 2-5 years, and 2% had more than five years of clinical experience. Most physiotherapists work as general practitioners, and very few specialize in neurological physical therapy. About 80% of physiotherapists said they deal with 1-5 Bell’s palsy patients daily, with an average of 16 patients per month. According to most physiotherapists, the recovery period of patients was about 1-2 weeks.
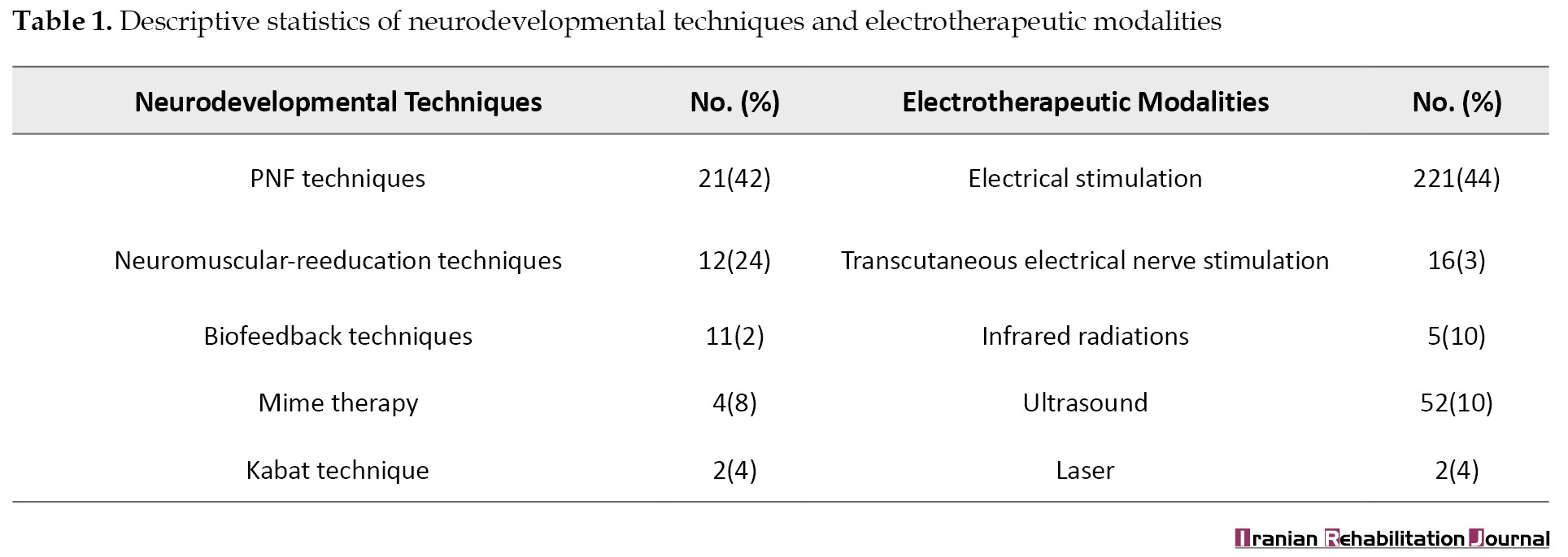
Results indicate that PNF (42%) is the preferred neurodevelopmental technique used in current practice patterns for the management of Bell’s palsy as compared to neuromuscular reeducation (24%), biofeedback (22%), mime therapy (8%), and Kabat technique (4%) (Table 1).
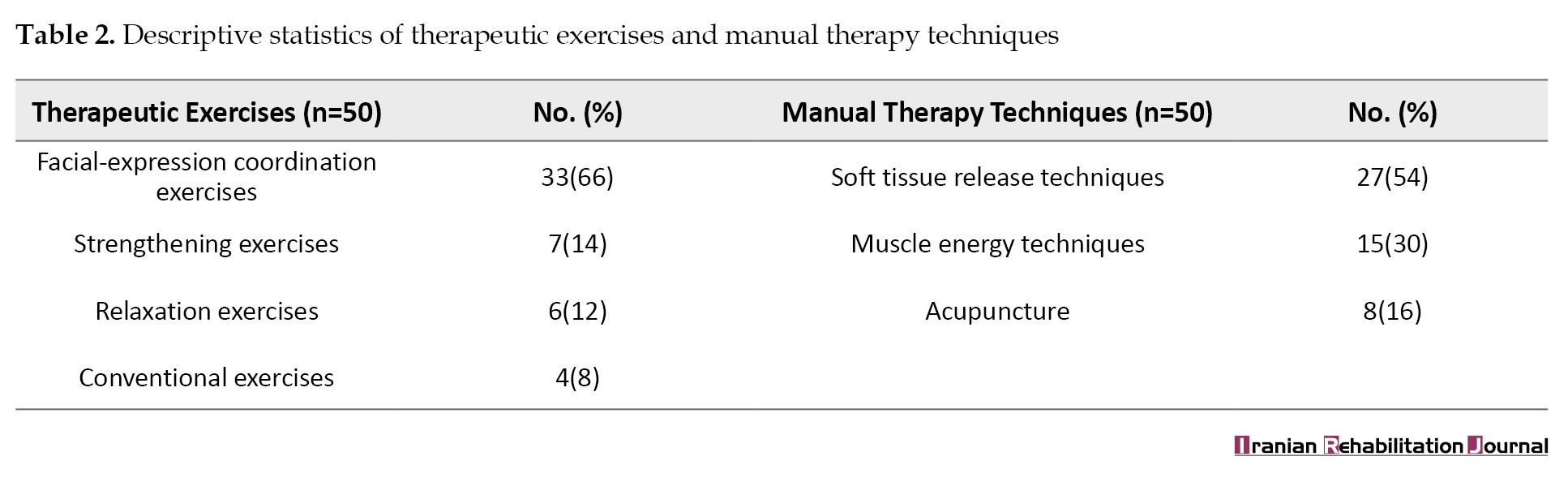
The most used therapeutic exercises by physiotherapists are facial expression coordination exercises (66%). Others used strengthening exercises (14%), relaxation exercises (12%), and convention exercises only for 8% of cases of Bell’s palsy. Manual therapy techniques used by physiotherapists for the management of Bell’s palsy are soft tissue release (54%), muscle energy techniques (30%), and acupuncture (16%) (Table 2).
Also, 44% of physiotherapists used electrical muscle stimulation as the preferred electrotherapeutic modality in their current practice. About 32% used transcutaneous electrical nerve stimulation, 10% ultrasound, 10% infrared radiation, and 4% laser (Table 1). Several combination therapies were also used. The combination of electrical muscle stimulation, facial exercises, and biofeedback was the most used (54%) among physiotherapists. Around 32% used a combination of ultrasound, facial exercises, and transcutaneous electrical nerve stimulation. In addition, 6% were using acupuncture and transcutaneous electrical nerve stimulation, and 6% were utilizing hot packs, soft tissue release, and relaxation exercises. Only 4% of physiotherapists chose other combinations (Figure 1).

Discussion
This study was done to identify the most popular treatment patterns currently used by most physiotherapists in Sargodha, Pakistan, for managing Bell’s palsy. PNF techniques, facial expression coordination exercises, soft tissue release, and electrical muscle stimulation have been used commonly from categories of neurodevelopmental techniques, therapeutic exercises, manual therapy techniques, and electrotherapeutic modalities. The most used combination was facial exercises, electrical stimulation, and biofeedback.
Regarding electrotherapeutic modalities, the practice pattern represented in the current study indicated the use of electrical stimulation (44%) by most physiotherapists compared to transcutaneous electrical nerve stimulation, ultrasound, infrared, and laser. Literature also verifies that most physiotherapists prefer electrical stimulation (78%) to manage Bell’s palsy [8]. It has been described in the past that infrared radiation releases heat that influences the superficial dermis and epidermis, which produces vasodilation, resulting in raised blood circulation and improved oxygen supply in the illuminated area. Moreover, it has the benefit of providing a warm and calm radiation effect [13]. Instead of its effectiveness, the present study demonstrated that only a small % of physiotherapists (10%) were using infrared radiation to manage Bell’s palsy.
The most preferred therapeutic exercises reported by physiotherapists are facial expression coordination and strengthening. At the same time, relaxation exercises are used by some physiotherapists and conventional exercises by a few. It is evident from previous studies that greater functional recovery is observed in patients performing facial exercises than in those who do not perform. This result emphasizes the positive effects of facial coordination exercises in patients with Bell’s palsy [14]. It was identified in the present study that soft tissue release is the most preferred treatment for hands-on techniques in Bell’s palsy patients as compared to muscle energy technique and acupuncture. Previous studies also reveal that massage therapy positively impacts facial muscle function due to relaxation as well as muscle tension thereby improving blood circulation [15].
The neurodevelopmental technique preferred by the current study’s physiotherapists is PNF compared to neuromuscular reeducation, biofeedback techniques, and mime therapy. This finding correlates with a previous study, which indicates that 4 weeks of a training program with PNF shows remarkable improvement in the functional independence of patients with Bell’s palsy, in contrast to the neuromuscular reeducation technique [16]. Evidence shows that about 34% of physiotherapists use mime therapy [8], but in this area of research, only 8% of physiotherapists go for mime therapy. Biofeedback through mirror therapy also benefits patients because it stimulates the brain through visual stimuli by observing the sound body part when the patient performs a series of movements [15]. Only 4% of physiotherapists included the Kabat technique in their treatment regime. However, a previous study found that the Kabat approach enhances social and physical function more effectively than the face exercise technique [17]. Physiotherapists have not selected this technique because of insufficient knowledge and lack of awareness regarding effectiveness of Kabat technique.
The most preferred combination therapies are electrical stimulation, biofeedback, and facial exercises. Afterward, physiotherapists utilized transcutaneous electrical nerve stimulation, ultrasound, and facial exercises in their clinical practice. Other combinations are least preferred. This finding correlates with a previous study, which concludes that the combined technique had a more significant impact than a customized Bell’s palsy therapy [18]. Another study reports that 70% of symptoms are resolved using electrical stimulation, facial muscle exercise, and massage in 2 weeks [19].
Conclusion
In conclusion, the current practice patterns in managing Bell’s palsy include PNF techniques, facial expression coordination exercises, soft tissue release, and electrical muscle stimulation by most physiotherapists in Sargodha. The most preferred combination was facial exercises, electrical stimulation, and biofeedback.
Study limitations
The small sample size and sample area of coverage make it hard to generalize the results. Moreover, there were fewer neuromuscular specialist physiotherapists, which will make a difference regarding practice behavior and preferences for managing Bell’s palsy.
Study recommendations
Future studies must compare these current practice patterns with evidence-based practice guidelines to identify whether their management aligns with current evidence-based practice so treatment efficiency can be improved.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about study purpose & their consent was taken in written form.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Pakeeza Seemal; Methodology and analysis: Pakeeza Seemal, and Jibran Arshad; Investigation: Saba Hameed, Sabahat Shafique, and Maryum Majeed; Resources, data curation and writing the original draft: Saba Hameed, Sabahat Shafique, and Maryum Majeed; Review and editing: Pakeeza Seemal, Jibran Arshad.
Conflict of interest
All authors declared no conflict of interest.
References
Bell’s palsy is a sudden-onset paralysis of the VII cranial nerve, characterized by a lower motor neuron lesion of the facial nerve, usually unilateral [1]. The reported incidence varies according to the geographical area. Its annual estimated incidence is around 30 per 100000 persons [2]. It is characterized by a lack of forehead wrinkles, incomplete lid closure, low eyebrow position (eyebrow ptosis), flattened nasolabial fold, and mouth corner droops [3]. The pathophysiology of Bell’s palsy includes vascular distension, edema with ischemia, and inflammation of the VII cranial nerve. Its etiology has remained unclear, but some causes have been proposed, such as vascular, autoimmune, inflammation, and viral infection, which includes reactivation of herpes zoster [4]. About 70% to 75% of patients fully recover without treatment, and early treatment enhances the chance of full recovery up to 82% [5]. A prompt diagnosis and therapy intervention seem essential for the best outcome in Bell’s palsy [6].
Bell’s palsy can be managed with both pharmaceutical and non-pharmacological treatments, as well as surgery. Corticosteroids (prednisolone), antivirals (acyclovir and valacyclovir), vitamin B12, non-steroidal anti-inflammatory drugs, and combination therapy are all examples of pharmacological treatments [7]. Non-pharmacological management includes physiotherapy, and surgical interventions include nerve decompression [8]. There is no explicit agreement on the treatment procedure for Bell’s palsy. The goal of therapy in its acute stage is to minimize inflammation with corticosteroids. After this period, antiviral drugs such as acyclovir or valacyclovir are administered to eliminate the human simplex virus. Rehabilitation treatment included electrical stimulation, neuromuscular facilitation technique, neuromuscular reeducation, infrared rays, acupuncture, facial exercise, and eye protection. If complete paralysis of the facial nerve occurs, it can be assessed by electromyography and electroneurography [9].
Physical therapy treatment for Bell’s palsy shows its effectiveness by depicting a notable increase in facial function and a quicker recovery. A combination of proprioceptive neuromuscular facilitation (PNF) and the Kabat technique with nerve stimulation improves facial asymmetry [10]. One of the previous studies about the efficacy of electrotherapy in treating Bell’s palsy shows that electrotherapy alone has unsatisfactory results but, when combined with other forms of treatment, significantly improves Bell’s palsy [11]. Evidence for managing Bell’s palsy in physical therapy is heterogeneous and limited. Descriptive data analysis from a previous study demonstrates that 78% of physiotherapists choose electrical stimulation, 34% favor mime therapy, and 72% adhere to the most recent evidence-based recommendations for treating Bell’s palsy [8]. There is ongoing discussion on the best course of therapy for Bell’s palsy, which varies from nation to nation and even between different institutions within a single country. Some commonly used physiotherapy techniques include massage therapy, mirror therapy, mime therapy, Kabat technique, infrared therapy, and low-level laser therapy. Bell’s palsy treatment varies; no consensus exists on what works best [9]. The recovery period varies according to the patient’s age, duration between treatment start and initial symptoms, severity of nerve damage, and rehabilitation after surgery [12].
Numerous studies have been done on the prevalence, risk factors, and treatment of Bell’s palsy. However, there is no study in the context of Pakistan regarding the identification of present clinical practice patterns regarding its management. So, this study aims to identify the type and number of common physiotherapy treatments for Bell’s palsy that physiotherapists of Sargodha, Pakistan, use.
Materials and Methods
A cross-sectional survey was conducted from May to August 2022. Data were obtained from 50 registered physiotherapists selected through a convenience sampling of those working in various clinical setups of Sargodha having more than 2 years of clinical experience. Novice practitioners and non-clinical physiotherapists were excluded [8]. A self-designed questionnaire was distributed to registered physiotherapists throughout Sargodha utilizing various internet platforms and by visiting their clinical setups in person. It was designed after searching literature with similar objectives for physiotherapists to assess current physical therapy practice patterns of Bell’s palsy by gathering all necessary information, including demographics, level of education, years of experience, and management strategies regarding physical therapy treatment of Bell’s palsy. Data were analyzed using SPSS software, version 20.1.0. Qualitative data, such as age, was presented as mean and standard deviation. Descriptive statistics were computed as frequency tables and graphs with percentages.
Results
In this cross-sectional observational study, 50 physiotherapists working in various clinical setups of Sargodha were included. The Mean±SD age of participants was 26.84±2.207 years. There were 42% male and 58% female physiotherapists. Almost 78% of physiotherapists had two years of clinical experience. About 18% had 2-5 years, and 2% had more than five years of clinical experience. Most physiotherapists work as general practitioners, and very few specialize in neurological physical therapy. About 80% of physiotherapists said they deal with 1-5 Bell’s palsy patients daily, with an average of 16 patients per month. According to most physiotherapists, the recovery period of patients was about 1-2 weeks.
Results indicate that PNF (42%) is the preferred neurodevelopmental technique used in current practice patterns for the management of Bell’s palsy as compared to neuromuscular reeducation (24%), biofeedback (22%), mime therapy (8%), and Kabat technique (4%) (Table 1).
The most used therapeutic exercises by physiotherapists are facial expression coordination exercises (66%). Others used strengthening exercises (14%), relaxation exercises (12%), and convention exercises only for 8% of cases of Bell’s palsy. Manual therapy techniques used by physiotherapists for the management of Bell’s palsy are soft tissue release (54%), muscle energy techniques (30%), and acupuncture (16%) (Table 2).
Also, 44% of physiotherapists used electrical muscle stimulation as the preferred electrotherapeutic modality in their current practice. About 32% used transcutaneous electrical nerve stimulation, 10% ultrasound, 10% infrared radiation, and 4% laser (Table 1). Several combination therapies were also used. The combination of electrical muscle stimulation, facial exercises, and biofeedback was the most used (54%) among physiotherapists. Around 32% used a combination of ultrasound, facial exercises, and transcutaneous electrical nerve stimulation. In addition, 6% were using acupuncture and transcutaneous electrical nerve stimulation, and 6% were utilizing hot packs, soft tissue release, and relaxation exercises. Only 4% of physiotherapists chose other combinations (Figure 1).
Discussion
This study was done to identify the most popular treatment patterns currently used by most physiotherapists in Sargodha, Pakistan, for managing Bell’s palsy. PNF techniques, facial expression coordination exercises, soft tissue release, and electrical muscle stimulation have been used commonly from categories of neurodevelopmental techniques, therapeutic exercises, manual therapy techniques, and electrotherapeutic modalities. The most used combination was facial exercises, electrical stimulation, and biofeedback.
Regarding electrotherapeutic modalities, the practice pattern represented in the current study indicated the use of electrical stimulation (44%) by most physiotherapists compared to transcutaneous electrical nerve stimulation, ultrasound, infrared, and laser. Literature also verifies that most physiotherapists prefer electrical stimulation (78%) to manage Bell’s palsy [8]. It has been described in the past that infrared radiation releases heat that influences the superficial dermis and epidermis, which produces vasodilation, resulting in raised blood circulation and improved oxygen supply in the illuminated area. Moreover, it has the benefit of providing a warm and calm radiation effect [13]. Instead of its effectiveness, the present study demonstrated that only a small % of physiotherapists (10%) were using infrared radiation to manage Bell’s palsy.
The most preferred therapeutic exercises reported by physiotherapists are facial expression coordination and strengthening. At the same time, relaxation exercises are used by some physiotherapists and conventional exercises by a few. It is evident from previous studies that greater functional recovery is observed in patients performing facial exercises than in those who do not perform. This result emphasizes the positive effects of facial coordination exercises in patients with Bell’s palsy [14]. It was identified in the present study that soft tissue release is the most preferred treatment for hands-on techniques in Bell’s palsy patients as compared to muscle energy technique and acupuncture. Previous studies also reveal that massage therapy positively impacts facial muscle function due to relaxation as well as muscle tension thereby improving blood circulation [15].
The neurodevelopmental technique preferred by the current study’s physiotherapists is PNF compared to neuromuscular reeducation, biofeedback techniques, and mime therapy. This finding correlates with a previous study, which indicates that 4 weeks of a training program with PNF shows remarkable improvement in the functional independence of patients with Bell’s palsy, in contrast to the neuromuscular reeducation technique [16]. Evidence shows that about 34% of physiotherapists use mime therapy [8], but in this area of research, only 8% of physiotherapists go for mime therapy. Biofeedback through mirror therapy also benefits patients because it stimulates the brain through visual stimuli by observing the sound body part when the patient performs a series of movements [15]. Only 4% of physiotherapists included the Kabat technique in their treatment regime. However, a previous study found that the Kabat approach enhances social and physical function more effectively than the face exercise technique [17]. Physiotherapists have not selected this technique because of insufficient knowledge and lack of awareness regarding effectiveness of Kabat technique.
The most preferred combination therapies are electrical stimulation, biofeedback, and facial exercises. Afterward, physiotherapists utilized transcutaneous electrical nerve stimulation, ultrasound, and facial exercises in their clinical practice. Other combinations are least preferred. This finding correlates with a previous study, which concludes that the combined technique had a more significant impact than a customized Bell’s palsy therapy [18]. Another study reports that 70% of symptoms are resolved using electrical stimulation, facial muscle exercise, and massage in 2 weeks [19].
Conclusion
In conclusion, the current practice patterns in managing Bell’s palsy include PNF techniques, facial expression coordination exercises, soft tissue release, and electrical muscle stimulation by most physiotherapists in Sargodha. The most preferred combination was facial exercises, electrical stimulation, and biofeedback.
Study limitations
The small sample size and sample area of coverage make it hard to generalize the results. Moreover, there were fewer neuromuscular specialist physiotherapists, which will make a difference regarding practice behavior and preferences for managing Bell’s palsy.
Study recommendations
Future studies must compare these current practice patterns with evidence-based practice guidelines to identify whether their management aligns with current evidence-based practice so treatment efficiency can be improved.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about study purpose & their consent was taken in written form.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Pakeeza Seemal; Methodology and analysis: Pakeeza Seemal, and Jibran Arshad; Investigation: Saba Hameed, Sabahat Shafique, and Maryum Majeed; Resources, data curation and writing the original draft: Saba Hameed, Sabahat Shafique, and Maryum Majeed; Review and editing: Pakeeza Seemal, Jibran Arshad.
Conflict of interest
All authors declared no conflict of interest.
References
- Zhang W, Xu L, Luo T, Wu F, Zhao B, Li X. The etiology of Bell’s palsy: A review. Journal of Neurology. 2020; 267(7):1896-905. [DOI:10.1007/s00415-019-09282-4 ] [PMID]
- Kim MH, Park SY. Population-based study and a scoping review for the epidemiology and seasonality in and effect of weather on Bell's palsy. Scientific Reports. 2021; 11(1):16941.[DOI:10.1038/s41598-021-96422-4 ] [PMID]
- Heckmann JG, Urban PP, Pitz S, Guntinas-Lichius O, Gágyor I. The diagnosis and treatment of idiopathic facial paresis (Bell’s palsy). Deutsches Ärzteblatt International. 2019; 116(41):692-702. [DOI:10.3238/arztebl.2019.0692 ] [PMID]
- Gagyor I, Madhok VB, Daly F, Sullivan F. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews. 2019; 9(9):CD001869. [DOI:10.1002/14651858.CD001869.pub9 ] [PMID]
- Efraimidis K, Lytras D, Paris Iakovidis A, Tsimerakis F, Kottaras A, Moutaftsis K. Efficacy of laser application for the rehabilitation of patients with Bell’s palsy. National Journal of Clinical Orthopaedics. 2021; 5(3):79-81. [Link]
- Fornaini C, Meng Z, Merigo E, Rocca JP. At-Home” Photobiomodulation: A new approach for bell’s palsy treatment.Case Reports in Neurological Medicine. 2021; 2021(1):5043458.[DOI:10.1155/2021/5043458 ]
- Mustafa AHK, Sulaiman AM. The epidemiology and management of Bell’s palsy in the Sudan. The Open Dentistry Journal. 2018; 12:827-36. [DOI:10.2174/1874210601812010827 ] [PMID]
- Limbu T, Nepal G. Current practice patterns in the management of bell’s palsy amongst physiotherapists in Nepal: A cross-sectional study. Annals of Physical and Rehabilitation Medicine. 2018; 61:e519. [DOI:10.1016/j.rehab.2018.05.1207 ]
- Rantung YH, Sengkey LS. Medical rehabilitation in patient with left bell’s palsy.Jurnal Medik Dan Rehabilitasi. 2021; 4(3). [Link]
- Gatidou AM, Kottaras A, Lytras D, Gatidou C, Iakovidis P, Kottaras I. Physiotherapy management of Bell’s palsy-A review of evidenced based physiotherapy practice. International Journal of Advanced Research in Medicine. 2021; 3(1):402-6. [DOI:10.22271/27069567.2021.v3.i1g.171 ]
- Burelo-Peregrino EG, Salas-Magaña M, Arias-Vázquez PI, Tovilla-Zarate CA, Bermudez-Ocaña DY, López-Narváez ML, et al. Efficacy of electrotherapy in Bell’s palsy treatment: A systematic review. Journal of Back and Musculoskeletal Rehabilitation. 2020; 33(5):865-74. [DOI:10.3233/BMR-171031 ]
- Menchetti I, McAllister K, Walker D, Donnan PT. Surgical interventions for the early management of Bell’s palsy. The Cochrane Database of Systematic Reviews. 2021; 1(1):CD007468.[DOI:10.1002/14651858.CD007468.pub4 ] [PMID]
- Ningsih D, Widodo A, Kusumawati A. Rehabilitation program for bell’s palsy patients-case report. Academic Physiotherapy Conference Proceeding. 2021; 563-71. [Link]
- Khan AJ, Szczepura A, Palmer S, Bark C, Neville C, Thomson D, et al. Physical therapy for facial nerve paralysis (Bell’s palsy): An updated and extended systematic review of the evidence for facial exercise therapy. Clinical Rehabilitation. 2022; 36(11):1424-49. [DOI:10.1177/02692155221110727] [PMID]
- Sofianata A, Susilo TE. Improving functional of facial ability for chronic bells palsy’s by using modalities massage and mirror exercise: A case report. Paper presented at: Academic Physiotherapy Conference Proceeding. 21-22 August 2021; Indonesia: Surakarta. [Link]
- Dhanya KV. Effectiveness of proprioceptive neuromuscular fecilitation and neuromuscular re-education for reducing facial disability and synkinesis in patients with bells palsy: A comparative study [PhD dissertation]. Coimbatore: PPG College of Physiotherapy; 2019. [Link]
- Khanzada K, Gondal MJI, Qamar MM, Basharat A, Ahmad W, Ali S. Comparison of efficacy of Kabat rehabilitation and facial exercises along with nerve stimulation in patients with Bell’s palsy. BLDE University Journal of Health Sciences. 2018; 3(1):31-5. [DOI:10.4103/bjhs.bjhs_35_17 ]
- Kumar S, Hashmi MA. Multiple approaches in management of bell’s palsy-A case study. Pakistan Journal of Rehabilitation. 2018; 7(2):52-4. [DOI:10.36283/pjr.zu.7.2/010 ]
- Javaid A, Waqas S, Asim HM. Recovery time in bell’s palsy after physical therapy treatment. Pakistan Journal of Medical and Health Sciences. 2021;15(3):473-4. [Link]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2023/04/12 | Accepted: 2023/11/25 | Published: 2024/12/20
Received: 2023/04/12 | Accepted: 2023/11/25 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
