
988368
Sat, Feb 21, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 673-680 |
Back to browse issues page


Ethics code: IR.SEMUMS.REC.1396.43
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahmadizadeh Z, Samaei S A, Alibakhshi H, Pahlevanian A, Binesh M. Factors Associated with Occupational Performance in Older People with Stroke. Iranian Rehabilitation Journal 2024; 22 (4) :673-680
URL: http://irj.uswr.ac.ir/article-1-1964-en.html
URL: http://irj.uswr.ac.ir/article-1-1964-en.html
Zahra Ahmadizadeh1 

 , Seyed Afshin Samaei2 , Hossein Alibakhshi1 , Aliakbar Pahlevanian1 , Maryam Binesh *3
, Seyed Afshin Samaei2 , Hossein Alibakhshi1 , Aliakbar Pahlevanian1 , Maryam Binesh *3
, Seyed Afshin Samaei2 , Hossein Alibakhshi1 , Aliakbar Pahlevanian1 , Maryam Binesh *3
1- Neuromuscular Rehabilitation Research Center, Semnan University of Medical Sciences, Semnan, Iran.
2- Department of Internal Medicine, Neuromuscular Rehabilitation Research Center, School of Medicine, Semnan, University of Medical Sciences, Semnan, Iran.
3- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, Semnan University of Medical Sciences, Semnan, Iran.
2- Department of Internal Medicine, Neuromuscular Rehabilitation Research Center, School of Medicine, Semnan, University of Medical Sciences, Semnan, Iran.
3- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, Semnan University of Medical Sciences, Semnan, Iran.
Keywords: Stroke, Occupational performance, Cognition, Participation, Activity of daily living (ADL)
Full-Text [PDF 467 kb]
(1193 Downloads)
| Abstract (HTML) (5743 Views)
Full-Text: (506 Views)
Introduction
Stroke is a complex neurological dysfunction resulting from ischemic or hemorrhagic cerebrovascular disorders [1]. Fallahzadeh et al. reported that in Iran, the number of strokes was 963512 (53.6% females), and the number of stroke incident cases was 102778 in 2019 [2]. This medical condition is one of the leading causes of disability, causing a range of sensory, motor, emotional, and cognitive impairments. As a result of these problems, stroke limits one’s independent performance in daily occupations [3] and intact occupational performance [4].
Occupational performance is defined as a dynamic interaction among the client, the occupation, and the contexts that result in the achievement of the occupation [5]. The three areas of occupational performance are leisure, self-care, and productivity. Good performance in occupational performance domains needs a person’s physical, spiritual, mental, sensorimotor, perceptual, and sociocultural components [6]. Therefore, people with stroke experience problems in their occupational performance. Occupational performance is a self-perception of the activity performance, and occupational satisfaction is the satisfaction with the performance of activities [7]. According to the experience of patients with stroke, occupational performance is trying to return to meaningful occupation, problem-solving occupational concerns, and finding a good purpose [8]. Therefore, one of the essential goals for occupational therapists is planning to improve occupational performance problems after a stroke.
Recently, there has been a shift toward occupational performance for people with ongoing disabilities or chronic health issues [9]. Based on the evidence, occupational performance decreases in patients with stroke [8], and some of the interventions could improve occupational performance in stroke patients with motor difficulties [10]. However, a few studies have investigated factors associated with occupational performance in stroke patients [11]. There is no consensus about practical factors for improving occupational performance in stroke survivors. It seems necessary to find the components that could be correlated with occupational performance so that they can enhance occupational performance by identifying and improving factors associated with it.
Increased awareness of components related to occupational performance could guide therapists’ intervention. Therefore, the current study aimed to investigate the relationship between motor function, cognitive status, and activities of daily living (ADL) associated with occupation performance and satisfaction in stroke patients.
Materials and Methods
Study design and setting
This cross-sectional study was conducted in the Neuromuscular Rehabilitation Research Center of Semnan University of Medical Sciences, Semnan, Iran.
Study participants
The study participants were 55 stroke patients selected by the simple non-probability sampling method from the rehabilitation clinics in Semnan, Iran. The inclusion criteria were as follows: Being over 60 years old, a diagnosis of ischemic or hemorrhagic stroke by a physician, having independence in the ADL before their stroke based on the patient and family report, having a lesion only in one of the cerebral hemispheres, and a post-stroke duration of 3 to 6 months. The exclusion criteria included any neurological or orthopedic diseases along with stroke, having more than one stroke, having a severe cognitive deficit based on the medical records, and inability to complete the study.
The sample size in this study was calculated using G*Power software, version 3.1. For a linear multiple regression: Fixed model, R² deviation from zero, an effect size of 0.25, a 95%confidence level, a test power of 0.8, and four predictors, the calculated sample size was 53 patients.
Study procedure
Fulfillment of the inclusion criteria was checked, and then the participants were informed about the aim and process of the study and signed the consent forms. An expert with an MS in occupational therapy evaluated each participant for about 40 minutes. The participant’s personal information was recorded in a demographic questionnaire. Their occupational performance and satisfaction were assessed using the Canadian occupational performance measure (COPM). The Montreal cognitive assessment (MoCA), Barthel index, and Brunnstrom recovery stage (BRS) assessed one’s cognitive status, ADL, and the stage of post-stroke motor recovery, respectively. All assessments were conducted in a quiet room, and their order was random for different participants. The assessor also considered the participants’ fatigue and gave them a short rest if required. Data collection was done from February to September 2018.
Study instruments
A demographic questionnaire was used to collect data on sex, age, education, and right or left hemisphere stroke recording.
COPM is standardized to identify one’s occupational priorities, perspectives on performance, and satisfaction with performance in three domains: Leisure, self-care, and productivity. In this study, the participants were asked to use a 10-point Likert scale to measure their satisfaction and performance [12]. COPM is valid and reliable in stroke patients [13]. Pan et al. reported that COPM was valid and reliable for people with physical disabilities [14]. The re-test-re-test reliability of the Persian version of COPM was 0.87 and 0.84 for satisfaction and performance, respectively [15].
The MoCA is a scale to screen mild cognitive impairments (MCI) and Alzheimer disease [16]. This tool evaluates different cognitive domains of visuospatial function, working memory, short-term memory recall, executive function, attention, language, concentration, and orientation to time and space [17]. The MoCA is a 30-point test with a cut-off point <26 for detecting MCI [18]. MoCA was translated and validated in Persian. The Cronbach α of MoCA was 0.80, and the interclass correlation coefficient between the baseline and repeated measurement was 0.99. This scale has acceptable validity [19].
The Barthel index assesses independence in daily living activities, including grooming, bathing, dressing, feeding, climbing the stairs, bowel and bladder management, transfer from bed to chair, mobility, and toilet use [20]. The total score on the scale is from 1 to 100, and higher scores indicate better physical performance and independence in ADL [21]. The Barthel index Persian version is valid and reliable for use in the stroke population (test re-test Cronbach α was 0.93 and reliability was 0.98) [22].
BRS is a measure to assess stroke patients’ upper and lower extremity motor impairment on the affected side. The test assesses recovery of the paresis side by determining associated reactions and synergy patterns on a 6-point scale from 1 (severe impairment) to 6 (normal movement pattern) [23]. The BRS classifies the recovery process into 6 stages: 1) Flaccidity, 2) Developing spasticity, 3) Maximum spasticity, 4) Decreasing spasticity, 5) Decreased spasticity, and 6) Normal. Naghdi et al. reported that the BRS is a valid test for motor impairment assessment in patients with stroke [24].
Statistical analysis
Data were analyzed using SPSS software, version 22 after confirming the normality of data by the Kolmogorov-Smirnov test and drawing histograms for variables. Parametric tests were used, including the Pearson correlation coefficient and multiple linear regressions. The significance level was set at P<0.05 in all the analyses.
Results
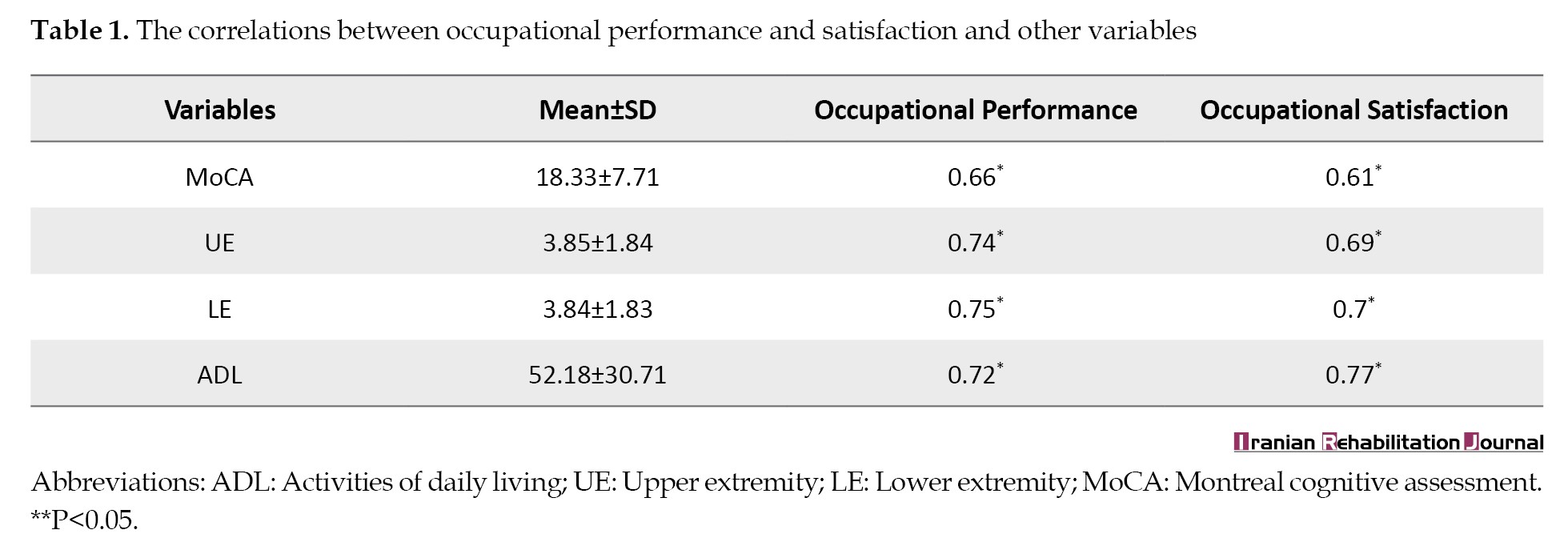
Five of the 60 stroke patients selected for the study were excluded because they could not complete all assessments. Therefore, 19 women and 36 men with a mean age of 68.98±5.37 years and a mean post-stroke duration of 15.49±12.97 months participated in the study. Also, 66.1% of the participants had left hemisphere stroke, and all of them lived at home. Table 1 presents the study participants’ mean and standard deviation and the Pearson correlation coefficient results between occupational performance and satisfaction, cognition level, ADL, and upper and lower extremity impairment.
The results of the multiple linear regression analysis to predict the participants’ occupational performance and satisfaction are shown in Table 2.
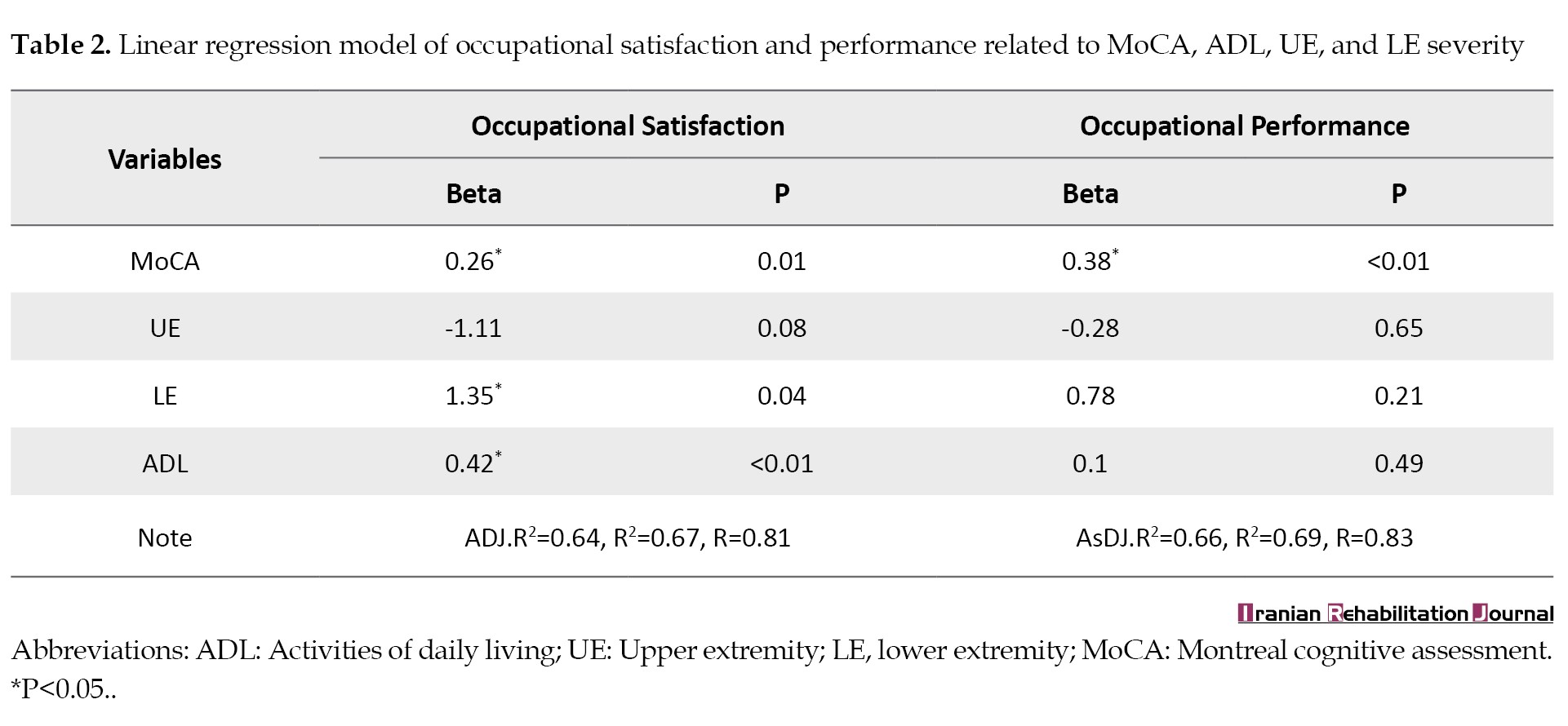
Evidently, the cognition level can significantly predict occupational performance, and cognition level, ADL, and lower extremity impairment can significantly predict occupational performance satisfaction in stroke patients (P<0.05).
Discussion
Our findings supports a significant correlation between occupational performance, ADL, cognitive problems, and severity of upper and lower extremity motor impairment after stroke. Results of linear regression analysis reveal that cognitive function could predict performance and satisfaction in daily occupations. ADL and lower extremity impairment can also be predictive of occupational performance satisfaction.
This finding shows that cognitive processes can predict occupational performance in older patients with stroke. It can be said that the cognition process is necessary to learn and use new information to improve occupational performance [25]. In addition, cognition has an essential role in occupations such as work, leisure, education, and home management [25]. The person-environment-occupation-performance (PEOP) model emphasizes cognition as one of the personal factors affecting occupational performance [26]. Therefore, this study shows cognition as an essential determinant of occupational performance. As such, the study’s results report that impaired cognition can predict difficulties in interpersonal relationships and ADL [27]. Kapoor et al. reported that the baseline cognition level could predict the long-term performance of patients with stroke in different domains regardless of age or severity of the stroke [28]. Wijst et al. also reported that cognitive problems were the determinants of occupational performance after a stroke [29]. Jokinen et al. reported complex cognitive abilities may be affected after stroke, and cognitive impairment is highly related to poor functional outcomes [30].
Despite a significant correlation between upper extremity motor impairment and occupational performance and satisfaction in our participants, motor impairment did not predict performance and satisfaction. When people with stroke experience difficulties in ADL, these difficulties are solved by using assistive devices or alternative strategies [31]. Therefore, it can be said that people with strokes on one side of the paresis learn to do most of their daily activities with the other extremities, change their strategy to do activities, or use assistive devices. Thus, it seems upper extremity motor impairment was not a predictor of occupational performance, but independence in doing ADL is a predictor of occupational performance.
As mentioned, independence in performing ADL and lower extremity function can predict occupational performance satisfaction. Life satisfaction is influenced by rumination on negative self-discrepancies based on differences in before and after stroke participation [32]. Maybe satisfaction with occupational performance has decreased due to the motor and sensory disability after the stroke [31] because of the inability to perform activities as before. It can be said that the psychological needs of people with stroke are not satisfied due to the inability to perform ADL, and independence in performing ADL has been identified as a predictor of occupational performance satisfaction.
Regarding the predictive role of lower extremity function, it can be said that normal gait requires healthy sensory and motor functions in both lower extremities [33]. After the stroke and one side sensory and motor dysfunction, the gait pattern will change, and performance satisfaction will change due to the inability to perform normal gait.
In a similar study, Mehdizade et al. reported that ADL activities, mobility, and crafts could affect the satisfaction and performance of stroke patients. Performing desired activities can also affect life satisfaction and quality [34]. Consistent with our study results, Hartman et al. reported that stroke patients’ satisfaction correlated with activity limitation and restricted participation [35]. Ghaffari et al. reported that stroke patients with more cognitive impairment are more dependent on instrumental ADL and have less participation [36].
Occupational performance may be affected by different health conditions, including stroke [37]. With restrictions on occupational performance, the person’s ability to participate in occupations is hindered that could negatively affect well-being [38]. The goal of rehabilitation is to maximize occupational performance and increase the participation of patients with stroke [39]. This study reports that cognitive impairment can predict occupational performance and satisfaction. In addition, independence in doing ADL activities and lower limb impairment can predict satisfaction with occupational performance. Therefore, occupational therapists must emphasize components that affect occupational performance and satisfaction to improve stroke patients’ participation in occupations.
Conclusion
Our study shows that cognition is a predictive factor of occupational performance and independence, and performing ADL and lower limb impairment can predict satisfaction with occupational performance. Therefore, occupational therapists are recommended to consider the practical and predictive factors of occupational performance during intervention planning for patients with stroke to increase their participation and decrease the adverse effects of social isolation.
Study limitations and suggestions for future research
One of the limitations of this study was the lack of a comparative study between patients with and without cognitive problems. Due to the small sample size of this study, it is suggested that similar studies be conducted with large sample sizes. Clinical trial studies are recommended to consider the factors affecting occupational performance. Future studies are also advised to assume the role of the environment on occupational performance.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Review Board of Semnan University of Medical Sciences (Code: IR.SEMUMS.REC.1396.43).
Funding
This study was funded by Semnan University of Medical Sciences (Grant No.: 1246).
Authors' contributions
Conceptualization and study design: Zahra Ahmadizadeh, Maryam Binesh, and Afshin Samaei; Data collection: Zahra Ahmadizadeh, and Afshin Samaei; Data analysis, interpretation and original draft preparation: Zahra Ahmadizadeh, Maryam Binesh, and Aliakbar Pahlevanian; Review and editing: Zahra Ahmadizadeh, Maryam Binesh, and Hossein Alibakhshi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Research Center of Neuromuscular Rehabilitation of Semnan University of Medical Sciences for cooperation and for providing facilities for this work.
References
Stroke is a complex neurological dysfunction resulting from ischemic or hemorrhagic cerebrovascular disorders [1]. Fallahzadeh et al. reported that in Iran, the number of strokes was 963512 (53.6% females), and the number of stroke incident cases was 102778 in 2019 [2]. This medical condition is one of the leading causes of disability, causing a range of sensory, motor, emotional, and cognitive impairments. As a result of these problems, stroke limits one’s independent performance in daily occupations [3] and intact occupational performance [4].
Occupational performance is defined as a dynamic interaction among the client, the occupation, and the contexts that result in the achievement of the occupation [5]. The three areas of occupational performance are leisure, self-care, and productivity. Good performance in occupational performance domains needs a person’s physical, spiritual, mental, sensorimotor, perceptual, and sociocultural components [6]. Therefore, people with stroke experience problems in their occupational performance. Occupational performance is a self-perception of the activity performance, and occupational satisfaction is the satisfaction with the performance of activities [7]. According to the experience of patients with stroke, occupational performance is trying to return to meaningful occupation, problem-solving occupational concerns, and finding a good purpose [8]. Therefore, one of the essential goals for occupational therapists is planning to improve occupational performance problems after a stroke.
Recently, there has been a shift toward occupational performance for people with ongoing disabilities or chronic health issues [9]. Based on the evidence, occupational performance decreases in patients with stroke [8], and some of the interventions could improve occupational performance in stroke patients with motor difficulties [10]. However, a few studies have investigated factors associated with occupational performance in stroke patients [11]. There is no consensus about practical factors for improving occupational performance in stroke survivors. It seems necessary to find the components that could be correlated with occupational performance so that they can enhance occupational performance by identifying and improving factors associated with it.
Increased awareness of components related to occupational performance could guide therapists’ intervention. Therefore, the current study aimed to investigate the relationship between motor function, cognitive status, and activities of daily living (ADL) associated with occupation performance and satisfaction in stroke patients.
Materials and Methods
Study design and setting
This cross-sectional study was conducted in the Neuromuscular Rehabilitation Research Center of Semnan University of Medical Sciences, Semnan, Iran.
Study participants
The study participants were 55 stroke patients selected by the simple non-probability sampling method from the rehabilitation clinics in Semnan, Iran. The inclusion criteria were as follows: Being over 60 years old, a diagnosis of ischemic or hemorrhagic stroke by a physician, having independence in the ADL before their stroke based on the patient and family report, having a lesion only in one of the cerebral hemispheres, and a post-stroke duration of 3 to 6 months. The exclusion criteria included any neurological or orthopedic diseases along with stroke, having more than one stroke, having a severe cognitive deficit based on the medical records, and inability to complete the study.
The sample size in this study was calculated using G*Power software, version 3.1. For a linear multiple regression: Fixed model, R² deviation from zero, an effect size of 0.25, a 95%confidence level, a test power of 0.8, and four predictors, the calculated sample size was 53 patients.
Study procedure
Fulfillment of the inclusion criteria was checked, and then the participants were informed about the aim and process of the study and signed the consent forms. An expert with an MS in occupational therapy evaluated each participant for about 40 minutes. The participant’s personal information was recorded in a demographic questionnaire. Their occupational performance and satisfaction were assessed using the Canadian occupational performance measure (COPM). The Montreal cognitive assessment (MoCA), Barthel index, and Brunnstrom recovery stage (BRS) assessed one’s cognitive status, ADL, and the stage of post-stroke motor recovery, respectively. All assessments were conducted in a quiet room, and their order was random for different participants. The assessor also considered the participants’ fatigue and gave them a short rest if required. Data collection was done from February to September 2018.
Study instruments
A demographic questionnaire was used to collect data on sex, age, education, and right or left hemisphere stroke recording.
COPM is standardized to identify one’s occupational priorities, perspectives on performance, and satisfaction with performance in three domains: Leisure, self-care, and productivity. In this study, the participants were asked to use a 10-point Likert scale to measure their satisfaction and performance [12]. COPM is valid and reliable in stroke patients [13]. Pan et al. reported that COPM was valid and reliable for people with physical disabilities [14]. The re-test-re-test reliability of the Persian version of COPM was 0.87 and 0.84 for satisfaction and performance, respectively [15].
The MoCA is a scale to screen mild cognitive impairments (MCI) and Alzheimer disease [16]. This tool evaluates different cognitive domains of visuospatial function, working memory, short-term memory recall, executive function, attention, language, concentration, and orientation to time and space [17]. The MoCA is a 30-point test with a cut-off point <26 for detecting MCI [18]. MoCA was translated and validated in Persian. The Cronbach α of MoCA was 0.80, and the interclass correlation coefficient between the baseline and repeated measurement was 0.99. This scale has acceptable validity [19].
The Barthel index assesses independence in daily living activities, including grooming, bathing, dressing, feeding, climbing the stairs, bowel and bladder management, transfer from bed to chair, mobility, and toilet use [20]. The total score on the scale is from 1 to 100, and higher scores indicate better physical performance and independence in ADL [21]. The Barthel index Persian version is valid and reliable for use in the stroke population (test re-test Cronbach α was 0.93 and reliability was 0.98) [22].
BRS is a measure to assess stroke patients’ upper and lower extremity motor impairment on the affected side. The test assesses recovery of the paresis side by determining associated reactions and synergy patterns on a 6-point scale from 1 (severe impairment) to 6 (normal movement pattern) [23]. The BRS classifies the recovery process into 6 stages: 1) Flaccidity, 2) Developing spasticity, 3) Maximum spasticity, 4) Decreasing spasticity, 5) Decreased spasticity, and 6) Normal. Naghdi et al. reported that the BRS is a valid test for motor impairment assessment in patients with stroke [24].
Statistical analysis
Data were analyzed using SPSS software, version 22 after confirming the normality of data by the Kolmogorov-Smirnov test and drawing histograms for variables. Parametric tests were used, including the Pearson correlation coefficient and multiple linear regressions. The significance level was set at P<0.05 in all the analyses.
Results
Five of the 60 stroke patients selected for the study were excluded because they could not complete all assessments. Therefore, 19 women and 36 men with a mean age of 68.98±5.37 years and a mean post-stroke duration of 15.49±12.97 months participated in the study. Also, 66.1% of the participants had left hemisphere stroke, and all of them lived at home. Table 1 presents the study participants’ mean and standard deviation and the Pearson correlation coefficient results between occupational performance and satisfaction, cognition level, ADL, and upper and lower extremity impairment.
The results of the multiple linear regression analysis to predict the participants’ occupational performance and satisfaction are shown in Table 2.
Evidently, the cognition level can significantly predict occupational performance, and cognition level, ADL, and lower extremity impairment can significantly predict occupational performance satisfaction in stroke patients (P<0.05).
Discussion
Our findings supports a significant correlation between occupational performance, ADL, cognitive problems, and severity of upper and lower extremity motor impairment after stroke. Results of linear regression analysis reveal that cognitive function could predict performance and satisfaction in daily occupations. ADL and lower extremity impairment can also be predictive of occupational performance satisfaction.
This finding shows that cognitive processes can predict occupational performance in older patients with stroke. It can be said that the cognition process is necessary to learn and use new information to improve occupational performance [25]. In addition, cognition has an essential role in occupations such as work, leisure, education, and home management [25]. The person-environment-occupation-performance (PEOP) model emphasizes cognition as one of the personal factors affecting occupational performance [26]. Therefore, this study shows cognition as an essential determinant of occupational performance. As such, the study’s results report that impaired cognition can predict difficulties in interpersonal relationships and ADL [27]. Kapoor et al. reported that the baseline cognition level could predict the long-term performance of patients with stroke in different domains regardless of age or severity of the stroke [28]. Wijst et al. also reported that cognitive problems were the determinants of occupational performance after a stroke [29]. Jokinen et al. reported complex cognitive abilities may be affected after stroke, and cognitive impairment is highly related to poor functional outcomes [30].
Despite a significant correlation between upper extremity motor impairment and occupational performance and satisfaction in our participants, motor impairment did not predict performance and satisfaction. When people with stroke experience difficulties in ADL, these difficulties are solved by using assistive devices or alternative strategies [31]. Therefore, it can be said that people with strokes on one side of the paresis learn to do most of their daily activities with the other extremities, change their strategy to do activities, or use assistive devices. Thus, it seems upper extremity motor impairment was not a predictor of occupational performance, but independence in doing ADL is a predictor of occupational performance.
As mentioned, independence in performing ADL and lower extremity function can predict occupational performance satisfaction. Life satisfaction is influenced by rumination on negative self-discrepancies based on differences in before and after stroke participation [32]. Maybe satisfaction with occupational performance has decreased due to the motor and sensory disability after the stroke [31] because of the inability to perform activities as before. It can be said that the psychological needs of people with stroke are not satisfied due to the inability to perform ADL, and independence in performing ADL has been identified as a predictor of occupational performance satisfaction.
Regarding the predictive role of lower extremity function, it can be said that normal gait requires healthy sensory and motor functions in both lower extremities [33]. After the stroke and one side sensory and motor dysfunction, the gait pattern will change, and performance satisfaction will change due to the inability to perform normal gait.
In a similar study, Mehdizade et al. reported that ADL activities, mobility, and crafts could affect the satisfaction and performance of stroke patients. Performing desired activities can also affect life satisfaction and quality [34]. Consistent with our study results, Hartman et al. reported that stroke patients’ satisfaction correlated with activity limitation and restricted participation [35]. Ghaffari et al. reported that stroke patients with more cognitive impairment are more dependent on instrumental ADL and have less participation [36].
Occupational performance may be affected by different health conditions, including stroke [37]. With restrictions on occupational performance, the person’s ability to participate in occupations is hindered that could negatively affect well-being [38]. The goal of rehabilitation is to maximize occupational performance and increase the participation of patients with stroke [39]. This study reports that cognitive impairment can predict occupational performance and satisfaction. In addition, independence in doing ADL activities and lower limb impairment can predict satisfaction with occupational performance. Therefore, occupational therapists must emphasize components that affect occupational performance and satisfaction to improve stroke patients’ participation in occupations.
Conclusion
Our study shows that cognition is a predictive factor of occupational performance and independence, and performing ADL and lower limb impairment can predict satisfaction with occupational performance. Therefore, occupational therapists are recommended to consider the practical and predictive factors of occupational performance during intervention planning for patients with stroke to increase their participation and decrease the adverse effects of social isolation.
Study limitations and suggestions for future research
One of the limitations of this study was the lack of a comparative study between patients with and without cognitive problems. Due to the small sample size of this study, it is suggested that similar studies be conducted with large sample sizes. Clinical trial studies are recommended to consider the factors affecting occupational performance. Future studies are also advised to assume the role of the environment on occupational performance.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Review Board of Semnan University of Medical Sciences (Code: IR.SEMUMS.REC.1396.43).
Funding
This study was funded by Semnan University of Medical Sciences (Grant No.: 1246).
Authors' contributions
Conceptualization and study design: Zahra Ahmadizadeh, Maryam Binesh, and Afshin Samaei; Data collection: Zahra Ahmadizadeh, and Afshin Samaei; Data analysis, interpretation and original draft preparation: Zahra Ahmadizadeh, Maryam Binesh, and Aliakbar Pahlevanian; Review and editing: Zahra Ahmadizadeh, Maryam Binesh, and Hossein Alibakhshi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Research Center of Neuromuscular Rehabilitation of Semnan University of Medical Sciences for cooperation and for providing facilities for this work.
References
- Murphy SJ, Werring DJ. Stroke: Causes and clinical features. Medicine. 2020; 48(9):p561-6. [DOI:10.1016/j.mpmed.2020.06.002]
- Fallahzadeh A, Esfahani Z, Sheikhy A, Keykhaei M, Moghaddam SS, Tehrani YS, et al. National and subnational burden of stroke in Iran from 1990 to 2019. Annals of Clinical Translational Neurology. 2022; 9(5):669-83. [DOI:10.1002/acn3.51547]
- Lui SK, Nguyen MH. Elderly stroke rehabilitation: Overcoming the complications and its associated challenges. Current Gerontology and Geriatrics Research. 2018; 2018. [DOI:10.1155/2018/9853837]
- Paul P. The relationship between occupational performance and well-being of stroke survival in selected rehabilitation centre of Bangladesh (PhD dissertation). Dhaka: University of Dhaka; 2017. [Link]
- Association AOT. Occupational therapy practice framework: Domain and process. American Journal of Occupational Therapy. 2020; 74(2):7412410010p1–7412410010p87. [DOI:10.5014/ajot.2020.74S2001]
- Concepcion AV, Bosque FD, Delgado NM, Mojica IK, Charlie R, Reyes D. Documenting pediatric occupational therapy evaluation through the dollhouse model. Philippine Journal of Allied Health Sciences. 2023; 6(2):53-9. [DOI:10.36413/pjahs.0602.009]
- Eyssen I, Steultjens MP, Oud TA, Bolt EM, Maasdam A, Dekker J. Responsiveness of the Canadian occupational performance measure. Journal of Rehabilitation Research and Development. 2011; 48(5):517-28. [DOI:10.1682/jrrd.2010.06.0110] [PMID]
- Wijekoon S, Wilson W, Gowan N, Ferreira L, Phadke C, Udler E, et al. Experiences of occupational performance in survivors of stroke attending peer support groups. Canadian Journal of Occupational Therapy. Revue Canadienne D'ergotherapie 2020; 87(3):173-81. [DOI:10.1177/0008417420905707] [PMID]
- Graham F, Kennedy-Behr A, Ziviani J. Occupational performance coaching: A manual for practitioners and researchers. London: Routledge; 2020. [DOI:10.4324/9780429055805]
- Nilsen DM, Gillen G, Geller D, Hreha K, Osei E, Saleem GT. Effectiveness of interventions to improve occupational performance of people with motor impairments after stroke: An evidence-based review. American Journal of Occupational Therapy. 2015; 69(1):6901180030p1-9. [DOI:10.5014/ajot.2015.011965] [PMID]
- Chae GS, Chang M. The correlation between occupational performance and well-being in stroke patients. Journal of Physical Therapy Science. 2016; 28(6):1712-5. [DOI:10.1589/jpts.28.1712] [PMID]
- Law M, Baptiste S, Carswell A, McColl M, Polatajko H, Pollock N. The Canadian occupational performance measure. Ottawa: Canadian Association of Occupational Therapists Publications; 2014. [Link]
- Yang SY, Lin CY, Lee YC, Chang JH. The Canadian occupational performance measure for patients with stroke: A systematic review. Journal of Physical Therapy Science. 2017; 29(3):548-55. [PMID]
- Pan AW, Chung L, Hsin‐Hwei G. Reliability and validity of the Canadian Occupational Performance Measure for clients with psychiatric disorders in Taiwan. Occupational Therapy International. 2003; 10(4):269-77. [DOI:10.1002/oti.190]
- Dehghan L, Dalvand H, Pourshahbaz A. [Translation of Canadian occupational performance measure and testing Persian version validity and reliability among Iranian mothers of children with cerebral palsy (Persian)]. Journal of Modern Rehabilitation. 2015; 9(4):25-31. [Link]
- Chehrehnegar N, Shams F, Zarshenas S, Kazemi F. Evaluating the reliability of the montreal cognitive assessment test and its agreement with mini mental state examination among healthy elderly. Journal of Research in Rehabilitation Sciences. 2012; 7(5). [Link]
- Chiti G, Pantoni L. Use of Montreal Cognitive Assessment in patients with stroke. Stroke. 2014; 45(10):3135-40. [DOI:10.1161/STROKEAHA.114.004590]
- Arab Ahmadi M, Ashrafi F, Behnam B. Comparison of Montreal Cognitive Assessment test and Mini Mental State Examination in detecting cognitive impairment in relapsing-remitting multiple sclerosis patients. International Clinical Neuroscience Journal. 2016; 2(4):137-41. [Link]
- Badrkhahan SZ, Sikaroodi H, Sharifi F, Kouti L, Noroozian M. Validity and reliability of the Persian version of the Montreal Cognitive Assessment (MoCA-P) scale among subjects with Parkinson’s disease. Applied Neuropsychology. Adult. 2020; 27(5):431-9. [DOI:10.1080/23279095.2019.1565762] [PMID]
- Koohestani H, Baghcheghi N. [The prevalence of depression among caregivers of stroke survivors and related factors in Arak(Persian)]. Iranian Journal of Epidemiology. 2012; 8(3):66-72. [Link]
- Hormozi S, Alizadeh-Khoei M, Sharifi F, Taati F, Aminalroaya R, Fadaee S, et al. Iranian version of barthel index: Validity and reliability in outpatients’ elderly. International Journal of Preventive Medicine. 2019; 10:130. [DOI:10.4103/ijpvm.IJPVM_579_18] [PMID]
- Oveisgharan S, Shirani S, Ghorbani A, Soltanzade A, Baghaei A, Hosseini S, et al. Barthel index in a Middle-East country: Translation, validity and reliability. Cerebrovascular Diseases. 2006; 22(5-6):350-4. [DOI:10.1159/000094850] [PMID]
- Koyama T, Koumo M, Uchiyama Y, Domen K. Utility of Fractional Anisotropy in Cerebral Peduncle for Stroke Outcome Prediction: Comparison of Hemorrhagic and Ischemic Strokes. Journal of Stroke and Cerebrovascular Diseases. 2018; 27(4):878-85. [DOI:10.1016/j.jstrokecerebrovasdis.2017.10.022] [PMID]
- Naghdi S, Ansari NN, Mansouri K, Hasson S. A neurophysiological and clinical study of Brunnstrom recovery stages in the upper limb following stroke. Brain Injury. 2010; 24(11):1372-8. [DOI:10.3109/02699052.2010.506860] [PMID]
- Giles GM, Radomski MV, Wolf TJ. Cognition, cognitive rehabilitation, and occupational performance. American Journal of Occupational Therapy. 2013; 67(6):S9. [Link]
- Smith D, Hudson S. Using the Person-Environment-Occupational Performance conceptual model as an analyzing framework for health literacy. 2013; 5(1):11-3. [DOI:10.1179/1753807611Y.0000000021]
- Saleem GT, Fitzpatrick JM. Impaired cognition impacts occupational performance and social relationships in survivors of intimate-partner-violence-related brain injury. The American Journal of Occupational Therapy. 2021; 75(Supplement_2):7512500071p1-p1. [DOI:10.5014/ajot.2021.75S2-RP71]
- Kapoor A, Lanctot K, Bayley M, Kiss A, Swartz R. Abstract TMP45: Predicting long-term body function, activity & participation after stroke: The prevailing role of cognition in determining functional outcome. Stroke. 2017; 48(suppl_1):ATMP45. [Link]
- van der Wijst E, Wright J, Steultjens E. The suitability of the Montreal Cognitive Assessment as a screening tool to identify people with dysfunction in occupational performance after mild stroke. British Journal of Occupational Therapy. 2014; 77(10):526-32. [DOI:10.4276/030802214X14122630932511]
- Jokinen H, Melkas S, Ylikoski R, Pohjasvaara T, Kaste M, Erkinjuntti T, et al. Post‐stroke cognitive impairment is common even after successful clinical recovery. European Journal of Neurology. 2015; 22(9):1288-94. [DOI:10.1111/ene.12743]
- Kristensen H, Postat A, Poulsen T, Jones D, Minet LR. Subjective experiences of occupational performance of activities of daily living in patients with mild stroke. International Journal of Therapy and Rehabilitation. 2014; 21(3):118-25. [DOI:10.12968/ijtr.2014.21.3.118]
- Hoyle M, Gustafsson L, Meredith P. Personal factors, participation, and satisfaction post-stroke: A qualitative exploration. Scandinavian Journal of Occupational Therapy. 2023; 30(4):572-84. [DOI:10.1080/11038128.2022.2154708]
- Pirker W, Katzenschlager R. Gait disorders in adults and the elderly: A clinical guide. Wiener klinische Wochenschrift. 2017; 129(3-4):81-95. [DOI:10.1007/s00508-016-1096-4]
- Mehdizadeh M, Hassani Mehraban A, Zahediyannasab R. The effect of group-based occupational therapy on performance and satisfaction of stroke survivors: Pilot trail, neuro-occupational view. Basic and clinical Neuroscience. 2017; 8(1):69-76. [DOI:10.15412/J.BCN.03080109] [PMID]
- Hartman-Maeir A, Soroker N, Ring H, Avni N, Katz N. Activities, participation and satisfaction one-year post stroke. Disability and Rehabilitation. 2007; 29(7):559-66. [DOI:10.1080/09638280600924996] [PMID]
- Ghaffari A, Rostami HR, Akbarfahimi M. Predictors of instrumental activities of daily living performance in patients with stroke. Occupational Therapy International. 2021; 2021:6675680. [DOI:10.1155/2021/6675680] [PMID]
- Yang SY, Lin CY. Using Canadian Model of Occupational Performance (CMOP) in a patient with stroke: Case report. Journal of Taiwan Occupational Therapy Research and Practice. 2015 ;11(2):109-19. [DOI:10.6534/jtotrp.2015.11(2).109]
- Christiansen CH, Bass J, Baum CM. Occupational therapy: Performance, participation, and well-being. Oxfordshire: Taylor & Francis; 2024. [Link]
- Chen HC. Contributions of neurological and neuropsychological functions to occupational performance in people with ischemic stroke [PhD dissertation]. Wisconsin: The University of Wisconsin-Madison; 2016. [Link]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2023/05/7 | Accepted: 2023/10/11 | Published: 2024/12/20
Received: 2023/05/7 | Accepted: 2023/10/11 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
