
988368
Sat, Jul 11, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 117-126 |
Back to browse issues page


Ethics code: ID: IR.USWR.REC. 1400.191
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Akbarfahimi N, Kaviani P, Taheri M, Vahedi M, Torabian M. The Iranian Version of the Fullerton Advanced Balance Scale in Children With Cerebral Palsy: Psychometric Properties. Iranian Rehabilitation Journal 2025; 23 (1) :117-126
URL: http://irj.uswr.ac.ir/article-1-2036-en.html
URL: http://irj.uswr.ac.ir/article-1-2036-en.html



1- Department of Occupational Therapy, School of Rehabilitation Sciences, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Occupational Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- -Department of Occupational Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Biostatistics and Epidemiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Clinical Research Development Center, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Science, Tehran, Iran.
2- Department of Occupational Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- -Department of Occupational Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Biostatistics and Epidemiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Clinical Research Development Center, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Science, Tehran, Iran.
Keywords: Cerebral palsy (CP), Fullerton advanced balance (FAB) scale, Reliability, Validity, Receiver operating curve
Full-Text [PDF 614 kb]
(682 Downloads)
| Abstract (HTML) (2964 Views)
Full-Text: (394 Views)
Introduction
Cerebral palsy (CP) is a stable neurological impairment with critical impairments in muscle tone, postural control and balance [1]. Balance is the capacity to manage the mass centroid in association with the supporting base [2]. Various requirements are needed to control balance: Musculoskeletal elements, internal representation, cognitive process, adaptive procedures, anticipatory process, sensory strategies, individual sensory organizations, and neuromuscular systems [3]. Balance is vital for all movements and poor balance control is a major underlying factor of limitation in activity (school function, independence in activity of daily living and manipulatory skills), increased risk of falls and participation restriction (social events, playground and school) in children with CP [3]; therefore, a balanced assessment that is sound, easy to administer, reliable, valid and can estimate multiple dimensions of balance, necessitates justification and illustration of the effectiveness of balance intervention, and other functional skills and predict the risk of falls in children with CP [3].
Several clinical and technological assessments have been utilized to evaluate balance in these children. Technological tests are expensive and complicated to administer in clinical practice [4]. Many clinical balance assessments have been designed for adults, however, they have acceptable content and set up for evaluating balance skills in children, are easily applicable and need few pieces of equipment, but have critical limitations for application in children with CP; for instance, time up and go test assesses the dynamic balance in walking not static balance; functional reach tests only measure anticipatory control in forward reach [5]. Berg balance scale (BBS) [6] or pediatric BBS (PBBS) [3] are reliable tools to evaluate balance in children with neurological impairments which are translated into several languages, but they cannot measure balance in higher functioning children aged more than 6 years related to their inclination to exhibit ceiling effects, furthermore, they cannot evaluate numerous dimensions of balance such as impairments in sensory systems like vestibular or visual systems have an essential role in balance control [3, 7].
Rose et al. developed the Fullerton advanced balance (FAB) [8]. The FAB is a performance and functional-based measure to determine proper changes in the balance abilities. It consists of items to assess static and dynamic balance situations, besides anticipatory and reactive postural control of balance [8, 9]. It has ten items with five subscales ordinal scale, the scores range from 0 to 40: A score of 40 is considered perfect balance and a score of 25 or less is conveyed as poor balance or a high risk of falling [8].
The Persian [10], Korean [11], German [12] and Turkish [13] for evaluating balance skills in high-performing older individuals [14], breast cancer [15], Parkinson [16] and children with CP are translated versions of FAB [17, 18].
Nevertheless, Iranian version of the FAB is a proper tool for evaluating balance function in adult or elderly people; evidence of the psychometric criteria of the Iranian version of the FAB scale for children with CP has not been verified yet. Consequently, it is essential to evaluate the reliability and validity of the Iranian version of the FAB to ensure it is a proper test for the estimation of balance function in children with CP.
Materials and Methods
A cross-sectional study was designed to examine the validity and reliability of the Iranian version of the FAB in children with CP. This study was performed in three steps: 1) Translation (final step of the Beaton guideline) [19]; 2) The internal consistency (Cronbach α coefficient), test re-test (intraclass correlation coefficient [ICC]) reliability and 3) Content, discriminate (receiver operating curve analysis) and concurrent (compared to the PBBS) validity.
Study participants
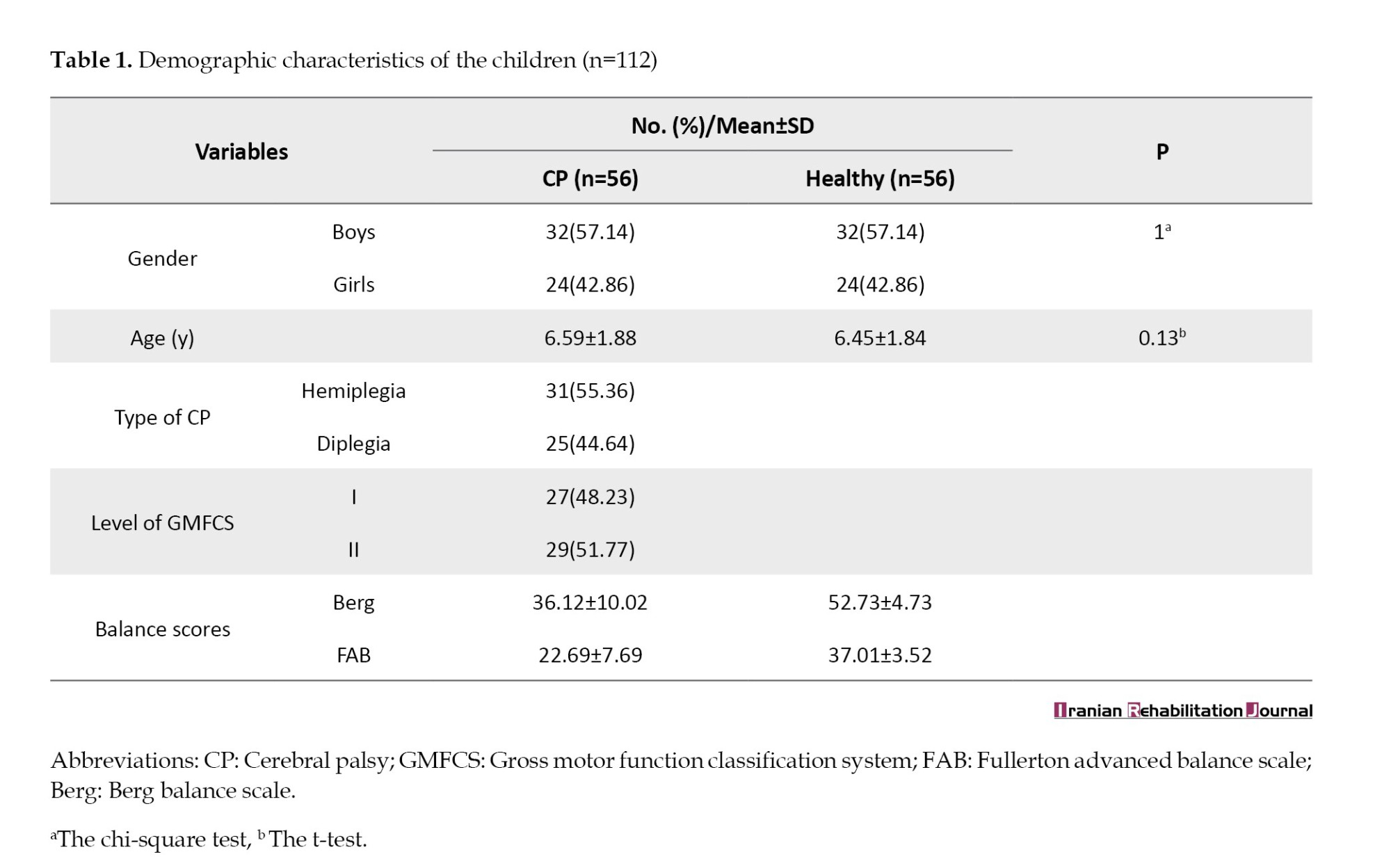
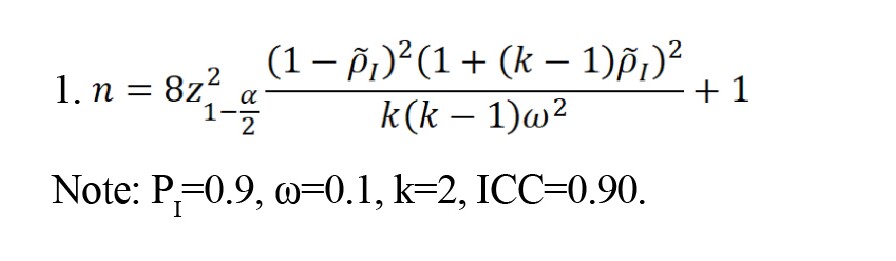
In this study, 56 children with CP in the University rehabilitation centers (Equation 1) and 56 healthy children who matched with the first group by age and gender in kindergartens and elementary schools were recruited. The inclusion criteria for children with CP were the children diagnosed with spastic CP of level I-II according to the gross motor function classification system (GMFCS), aged between 3 and 9 years old, capable of walking independently with or without aids, with no history of surgical procedures or Botulinum toxin injection within the six months leading up to the study and not being a suitable candidate for such injections or surgeries. Additionally, they had to be able to comprehend oral statements. All children with vision or hearing defects and suffering from out-of-controlled epilepsy or other musculoskeletal and mental health disorders were excluded. Demographic and clinical characteristics of the children in the two groups are presented in Table 1.
Sample size estimation for the study (Equation 1)
Study measures
The demographic questionnaire which developed by the research team, contained demographic data, namely age, gender, level of GMFCS and type of CP.
PBBS
The PBBS consists of 14 items, featuring five ordinary scale options that span from 0 to 4 with a maximum score of 56, representing the intact balance [20]. The standard error of measurement (SEM) for both the inter-rater reliability (ICC=0.99) and the test re-test reliability (ICC=0.99), of the Persian version of PBBS, was acceptable [21].
The gross motor function classification system
The Persian-GMFCS was used to determine the gross motor level of children with CP [1]. The GMFCS includes five separate levels of motor skill: At level I children can walk without restriction, while those at level V require a wheelchair for mobility [22]. The test re-test reliability (G=0.79) and interrater reliability (G=0.93) of GMFCS were confirmed [22].
FAB scale
The FAB was designed as a multi-item balance evaluation tool for postural control evaluation in older adults with normal social activity. It encompasses a total of ten items scored based on a 5-point ordinal scale (ranging from 4 to 0), with ten tasks. The 40 scores indicate independent performance, while the 25 scores or less indicate an inability to perform the balance task which means the falling risk is at a high level. It is quick and easy to administer, requiring minimal space, and simple equipment, and takes 10–12 min to complete [8, 14, 23]. The original version of FAB for adults has shown high test re-test reliability (r=0.96) and inter-rater reliability (r=0.92), with good correlation with the BBS (r=0.75, P<0.001) [8, 14, 23]. In this study, the Iranian version of the FAB, which has excellent test re-test reliability (ICC=0.97, P<0.001, 95% CI, 0.90%, 0.98%) and inter-rater reliability (ICC=0.92, P<0.001, 95% CI, 0.89%, 0.96%) in older adults was used [10].
Statistical analysis
The data were analyzed at P<0.05 the statistical significance level by IBM SPSS software, version 21. Demographic data were shown as to frequency, percentage, mean, and standard deviation. Psychometric properties of the Iranian version of the FAB, containing internal consistency, test re-test reliability (ICC [95% CI]), content, concurrent (compared to the PBBS) validity, and discriminate ability, were also reported.
Translation for CP population
Azad et al. translated the FAB into the Persian language according to the international quality of life assessment [10]. In this study, the process of translation for FAB in children with CP was performed based on only the final step of the Beaton guideline (cognitive debriefing and pre-testing step) [19]. This step involved using the cognitive interview method to investigate each patient’s understanding of the Iranian version of the FAB items, determining cognitive equivalence, and conducting debriefing. The Iranian version of the FAB was tested on 10 children with CP (three boys and seven girls) to assess its relevance, comprehensiveness and clarity.
Reliability
ICC and Cronbach α were calculated for the determination of the reliability and internal consistency, respectively. Test re-test reliability was assessed by performing the Iranian version of the FAB two times at two-week intervals. ICC was scored on a range of 0-1, interpreted as good with >0.7 [24]. Meanwhile, the Cronbach α coefficient is interpreted as excellent (α>0.90), good (0.80-0.90), acceptable (0.70-0.80), questionable (0.60-0.70), poor (0.50-0.60) and unacceptable (α<0.50) [25]. Minimal detectable change (MDC=1.96 ×2√SEM). that is the smallest change score beyond random error, standard error measurement (SEM=SD√[1–ICC]) and the smallest detectable change (SDC=2.77×SEM) were computed [26].
Content and concurrent validity
Content validity was evaluated based on the Lawshe model by 12 experts (two physiotherapists and 10 occupational therapists) in convenience sampling [27]. The content validity was estimated by computing the content validity ratio (CVR) and content validity index (CVI) for all items [27]. The necessity of the questionnaire items was rated on a triple Likert scale from “it is necessary,” “it is useful but not necessary” and “unnecessary.” Meanwhile, the CVR was calculated using Equation 2.
Content validity ratio (Equation 2)
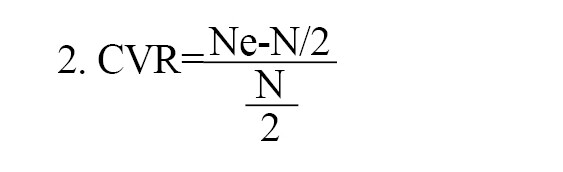
Note: Ne: The number of experts indicating “essential”; N: The total number of experts.
The experts analyzed the items about relativity, simplicity, and clarity using a 4-point Likert scale from 1 (the lowest) to 4 (the highest). Afterward, the CVI was computed for each item using Equation 3.
Content validity index (Equation 3)

The concurrent validity of the Iranian version of the FAB was computed by calculating the Spearman rank correlation coefficients to quantify the relationship between Iranian version of the FAB and PBBS, which >0.7 was interpreted as good concurrent validity [28].
The area under the curve (AUC) derived from receiver operating curves (ROC) was used to discriminate the validity of the FAB to test the ability of the FAB to distinguish between the higher function children with CP and healthy children. The AUC values were explained as follows: AUC=0.50: No discrimination; 0.70≤AUC<0.80: Acceptable discrimination; 0.80≤AUC<0.90: Excellent discrimination; and AUC≥0.90: Outstanding discrimination [29]. The best cut-off value for the total score was calculated based on Youden’s index [30].
Study procedure
The agreement was received from Rose, developer of the FAB [8] and Azad [10], the translator of the FAB to the Persian language. The implementation of the study was explained to children and their parents, voluntary written consent was attained and assured them that all information would be maintained in strict confidentiality.
Two expert occupational therapists interviewed the parents of the children and gathered the demographic data, determined the children’s level of gross motor function using GMFCS. The children with CP eligibility were tested by the Iranian version of the FAB and PBBS in the center where they were treated. To investigate the scale’s discriminative validity, healthy children who matched with age and gender in kindergartens and elementary schools were also tested by the Iranian version of the FAB and PBBS. Finally, 17 children with CP were tested for the Iranian version of the FAB two weeks later again to study its test re-test reliability.
Results
The demographic characteristics of the 112 participants in the two groups (CP group and healthy group) are given in Table 1.
Translation for CP population
The result of the final step of the Beaton guideline indicated that all children who participated in this study understood all the Iranian version of the FAB items with no difficulty.
Reliability
The ICC item was 0.98, >0.75, indicating good reliability of the test [24]. The Cronbach α coefficient in this study was found to be 0.99. This value is more than 0.70, which indicates the excellent internal consistency of the test [25]. The SEM: 1.86×0.11=0.22, MDC: 1.96×0.93=1.83, SDC: 2.77×0.22=0.61 were founded for Iranian version of the FAB.
Content, concurrent validity and discriminate ability
The results of CVI and CVR scores have been listed in Table 2.
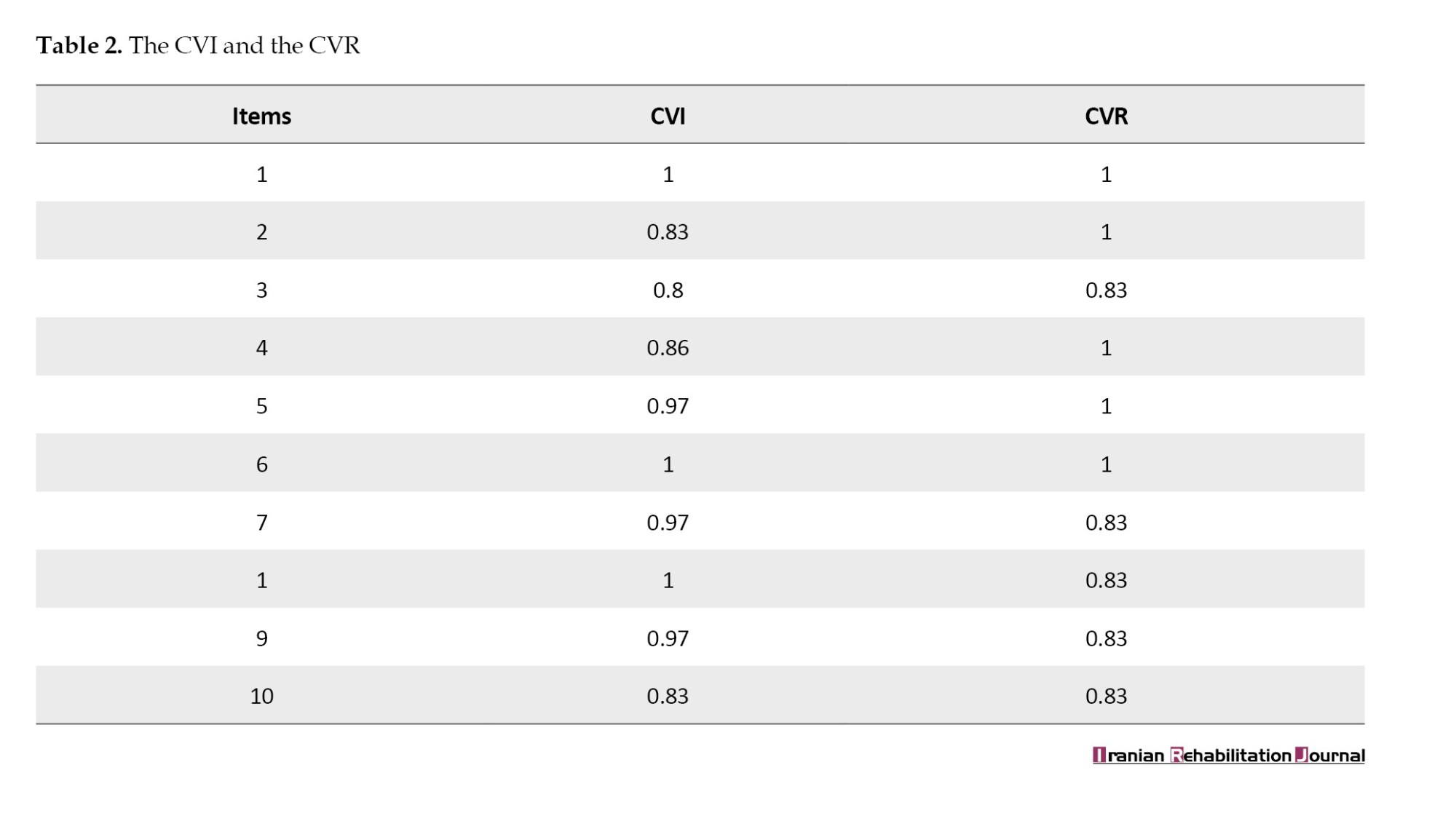
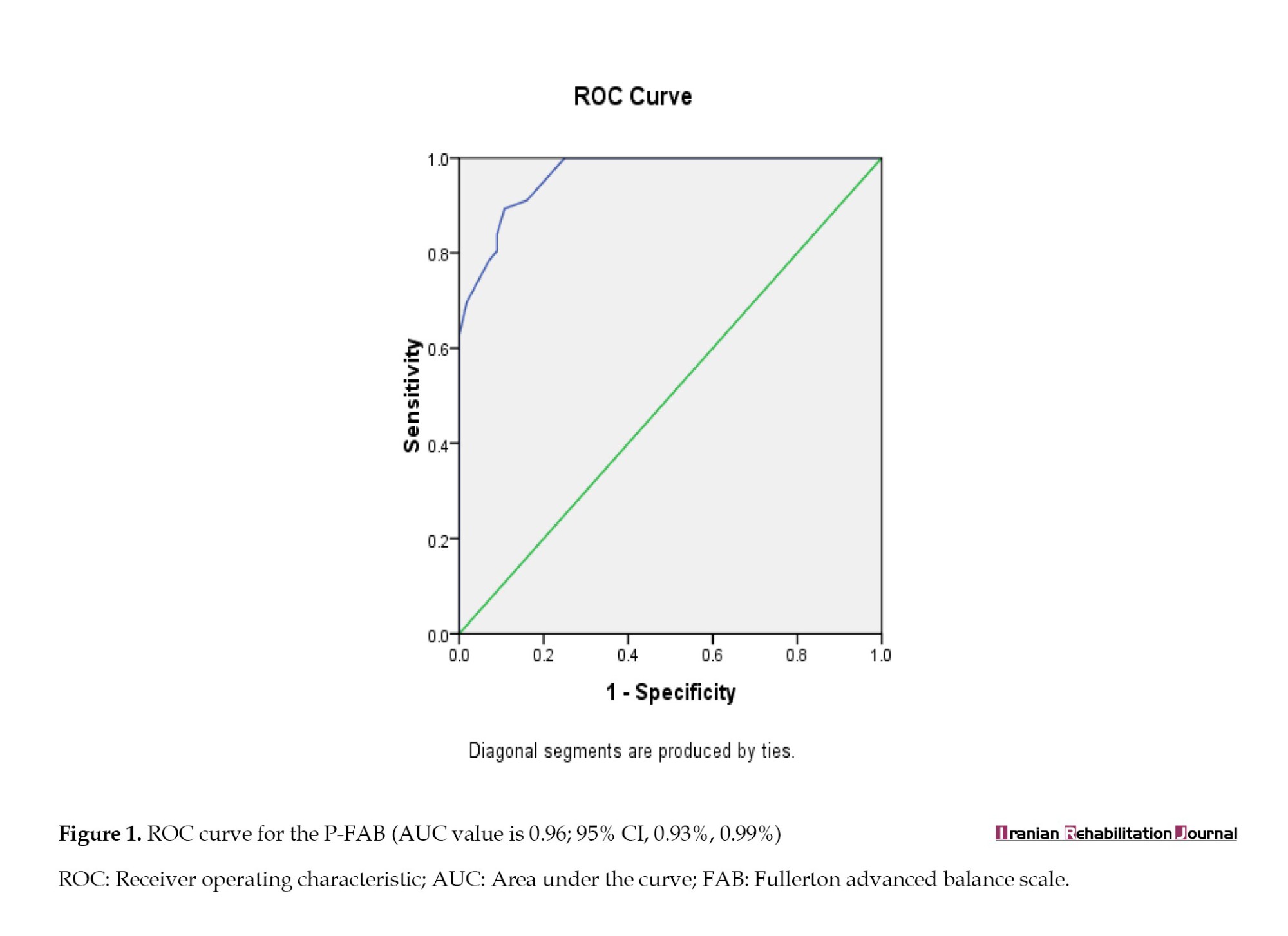
The CVI and CVR values were between 0.83 and 1, which is acceptable. Therefore, all items have good content validity. The Spearman rank correlation coefficients between the Iranian version of the FAB and PBBS indicated good concurrent validity of the Iranian version of the FAB (r=0.91, P<0.001). Regarding discriminate validity, the value of AUC was 0.96 (95% CI, 0.93%, 0.99%) which shows excellent discrimination, the score of 31.5 of the FAB had the best sensitivity (0.89), specificity (0.11) cut-off value to detect the higher function children with CP and healthy children (Figure 1).
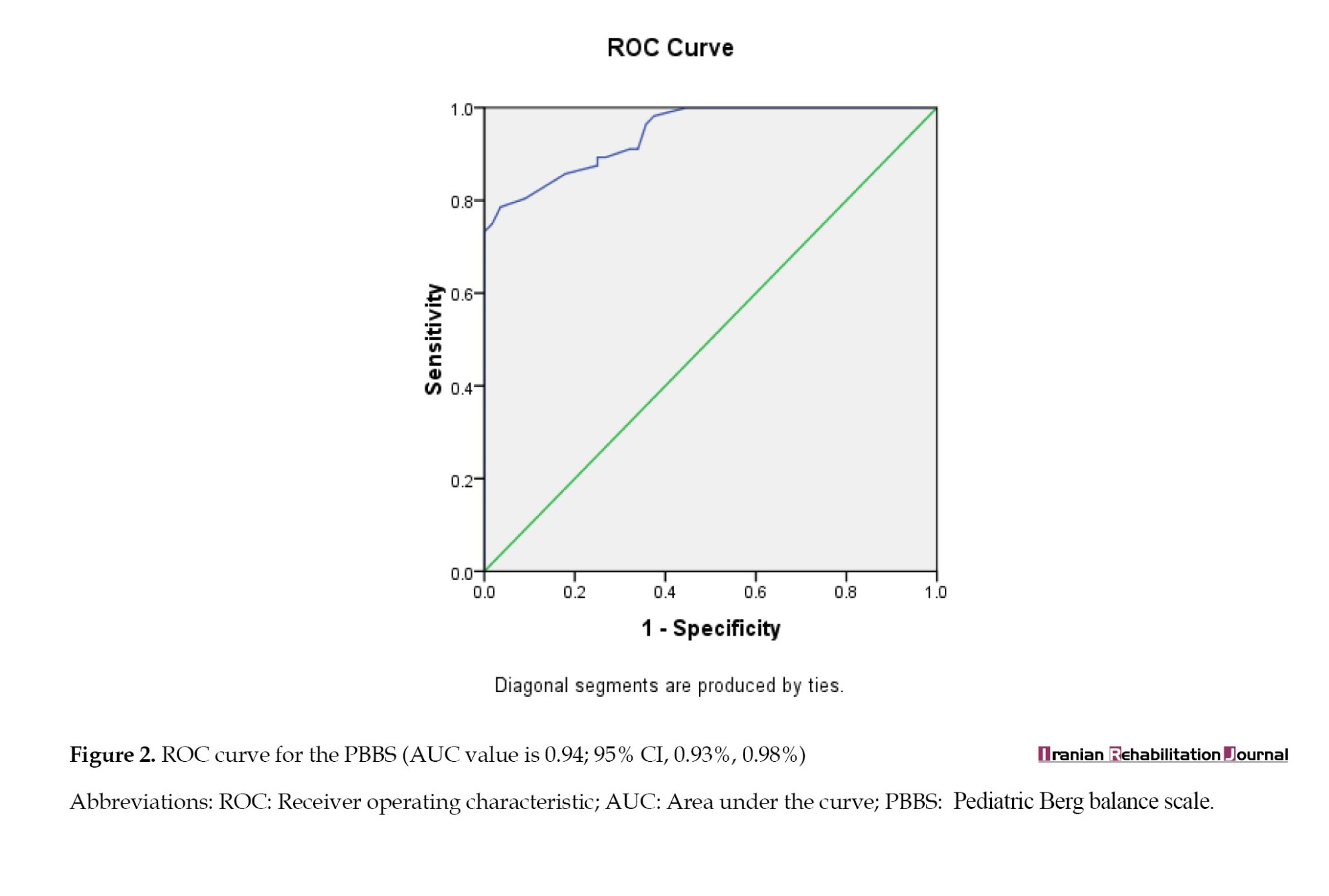
Furthermore, the value of AUC was 0.94 (95% CI, 0.93%, 0.98%) which shows excellent discrimination, the score of 49.5 of the P-PBS had the best sensitivity (0.78), specificity (0.04), cut-off value to detect the children with CP and healthy children (Figure 2).
Discussion
The main goals of this research were to investigate the reliability and validity of Iranian version of the FAB for children with CP. The results showed an acceptable internal consistency, and test re-test reliability for the Iranian version of the FAB. The FAB has been translated and validated in different languages: Korean [18], Turkish [13] and German [12]. Our results revealed similar or close internal consistency and test re-test reliability compared to the Korean study on children with CP (test re-test=0.99, internal consistency with Cronbach α=0.92) [18], as well as the Turkish version for children with CP (test re-test=0.99, internal consistency with Cronbach α=0.94) [17] and other studies with elderly on originally version (test re-test=0.96) [8], Persian version (test re-test=0.97, internal consistency with Kappa coefficient=0.8) [10] and German version (test re-test=0.96, internal consistency with Cronbach α=0.98) [12]. These results could be related to the appropriated time-space of the test re-test [23], good structure of questions for understanding and performing, and easy scoring instruction of the FAB [31].
We found a good correlation between Iranian version of the FAB and PBBS (r=0.91) for children with CP in a manner similar to that reported in the Turkish version (r=0.91) [17] and Korean version (r=0.60) for children with CP [18]. These findings indicated that the FAB and PBBS represent a similar structure due to containing the similar items. However, five items of FAB (items 1, 2, 3, 5, 6) are within the PBBS items, but they have different purposes. The PBB generally assesses static balance and anticipatory postural control, whereas the FAB assesses static and dynamic balance control, sensory orientation, anticipatory and reactive postural control [8]. The FAB was developed as a multinational balance scale for functionally independent older adults [8]. The results of factor analysis and Rasch analysis model in an earlier study explained two dominant factors as stationary and semi-dynamic balance and stability of gait for children with CP [18], as well as Erturan et al. reported all 10 items of FAB for the higher function children with CP define a one-dimensional scale of balance [17]. Moreover, the result of our study lined up with other previous studies: Regarding total scores of the PBBS was higher them the total score of the FAB which stated that FAB includes items to assess reactive postural control, vestibular, visual and tactile sense, in additional items of BBS and PBBS (in all version and population) are relatively easier than the FAB’s items.
The Iranian version of the FAB indicated high sensitivity to discriminate children with CP and healthy children in our study. The PBBS and FAB scales’ comparable accuracy identified functional balance ability between the higher function children with CP and healthy children with AUC of 0.94 and 0.96, respectively. In the PBBS a cut of point 49.5 points provided optimal sensitivity of 0.78 and specificity of 0.04. In the FAB scale, a cut of point 31.5 points provided an optimal sensitivity of 0.89 and a specificity of 0.11.
Kim et al. reported an AUC value of 0.79, the optimal cut-off point of 45.5 points (sensitivity=0.90, specificity=0.64) of PBBS in children with CP. However the AUC value of 0.76, the optimal cut of point of 21.5 points (sensitivity=0.90, specificity=0.62) of FAB in children with CP (age of 11.4±3.5 to 11.4±2.5 years) [32]. Franjoine et al. showed a cut of points from 23.3 points to 54.6 points (age of 2 years 4 months 13 years 7 months) in healthy children [7]. These controversies may be related to the age and balance level of participants. These studies demonstrated that the FAB with the more challenging and more difficult items than PBBS, furthermore both scales show high sensitivity versus low specificity. In this study, the higher cut of points of FAB may be related to the age of children (3-9 years).
Conclusion
This study was performed to investigate the reliability and validity of Iranian version of the FAB in higher gross motor function children with CP. The Iranian version of the FAB as a valid and reliable test can evaluate the balance of children functionally; nevertheless, it is more concise and requires less time and space for administration. This scale had a good positive correlation with PBBS.
Study limitations
This study had some limitations. We did not assess the floor and ceiling effects, whereas all items of the Turkish version of FAB were found adjust to the Rasch model, we did not reanalysis of the on the whole model and individual item fit. Conducting more comprehensive investigations is essential to recognize the item difficulty of the Iranian version of the FAB in children with CP in different types and different levels of balance function. Moreover, this question has remained whether the Iranian version of the FAB scale significant predictive measure of fall risk in the higher function children with CP.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC. 1400.191).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
This study was supported by a grant from the Clinical Research Development center, Rofeideh Rehabilitation Hospital, University Of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Grant No.: 2643).
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their sincere thanks to the Association for the Support of Children and their parents who provided their support during data collection and the Clinical Research Development Center of Rofeideh Rehabilitation Hospital, Tehran, Iran.
References
Cerebral palsy (CP) is a stable neurological impairment with critical impairments in muscle tone, postural control and balance [1]. Balance is the capacity to manage the mass centroid in association with the supporting base [2]. Various requirements are needed to control balance: Musculoskeletal elements, internal representation, cognitive process, adaptive procedures, anticipatory process, sensory strategies, individual sensory organizations, and neuromuscular systems [3]. Balance is vital for all movements and poor balance control is a major underlying factor of limitation in activity (school function, independence in activity of daily living and manipulatory skills), increased risk of falls and participation restriction (social events, playground and school) in children with CP [3]; therefore, a balanced assessment that is sound, easy to administer, reliable, valid and can estimate multiple dimensions of balance, necessitates justification and illustration of the effectiveness of balance intervention, and other functional skills and predict the risk of falls in children with CP [3].
Several clinical and technological assessments have been utilized to evaluate balance in these children. Technological tests are expensive and complicated to administer in clinical practice [4]. Many clinical balance assessments have been designed for adults, however, they have acceptable content and set up for evaluating balance skills in children, are easily applicable and need few pieces of equipment, but have critical limitations for application in children with CP; for instance, time up and go test assesses the dynamic balance in walking not static balance; functional reach tests only measure anticipatory control in forward reach [5]. Berg balance scale (BBS) [6] or pediatric BBS (PBBS) [3] are reliable tools to evaluate balance in children with neurological impairments which are translated into several languages, but they cannot measure balance in higher functioning children aged more than 6 years related to their inclination to exhibit ceiling effects, furthermore, they cannot evaluate numerous dimensions of balance such as impairments in sensory systems like vestibular or visual systems have an essential role in balance control [3, 7].
Rose et al. developed the Fullerton advanced balance (FAB) [8]. The FAB is a performance and functional-based measure to determine proper changes in the balance abilities. It consists of items to assess static and dynamic balance situations, besides anticipatory and reactive postural control of balance [8, 9]. It has ten items with five subscales ordinal scale, the scores range from 0 to 40: A score of 40 is considered perfect balance and a score of 25 or less is conveyed as poor balance or a high risk of falling [8].
The Persian [10], Korean [11], German [12] and Turkish [13] for evaluating balance skills in high-performing older individuals [14], breast cancer [15], Parkinson [16] and children with CP are translated versions of FAB [17, 18].
Nevertheless, Iranian version of the FAB is a proper tool for evaluating balance function in adult or elderly people; evidence of the psychometric criteria of the Iranian version of the FAB scale for children with CP has not been verified yet. Consequently, it is essential to evaluate the reliability and validity of the Iranian version of the FAB to ensure it is a proper test for the estimation of balance function in children with CP.
Materials and Methods
A cross-sectional study was designed to examine the validity and reliability of the Iranian version of the FAB in children with CP. This study was performed in three steps: 1) Translation (final step of the Beaton guideline) [19]; 2) The internal consistency (Cronbach α coefficient), test re-test (intraclass correlation coefficient [ICC]) reliability and 3) Content, discriminate (receiver operating curve analysis) and concurrent (compared to the PBBS) validity.
Study participants
In this study, 56 children with CP in the University rehabilitation centers (Equation 1) and 56 healthy children who matched with the first group by age and gender in kindergartens and elementary schools were recruited. The inclusion criteria for children with CP were the children diagnosed with spastic CP of level I-II according to the gross motor function classification system (GMFCS), aged between 3 and 9 years old, capable of walking independently with or without aids, with no history of surgical procedures or Botulinum toxin injection within the six months leading up to the study and not being a suitable candidate for such injections or surgeries. Additionally, they had to be able to comprehend oral statements. All children with vision or hearing defects and suffering from out-of-controlled epilepsy or other musculoskeletal and mental health disorders were excluded. Demographic and clinical characteristics of the children in the two groups are presented in Table 1.
Sample size estimation for the study (Equation 1)
Study measures
The demographic questionnaire which developed by the research team, contained demographic data, namely age, gender, level of GMFCS and type of CP.
PBBS
The PBBS consists of 14 items, featuring five ordinary scale options that span from 0 to 4 with a maximum score of 56, representing the intact balance [20]. The standard error of measurement (SEM) for both the inter-rater reliability (ICC=0.99) and the test re-test reliability (ICC=0.99), of the Persian version of PBBS, was acceptable [21].
The gross motor function classification system
The Persian-GMFCS was used to determine the gross motor level of children with CP [1]. The GMFCS includes five separate levels of motor skill: At level I children can walk without restriction, while those at level V require a wheelchair for mobility [22]. The test re-test reliability (G=0.79) and interrater reliability (G=0.93) of GMFCS were confirmed [22].
FAB scale
The FAB was designed as a multi-item balance evaluation tool for postural control evaluation in older adults with normal social activity. It encompasses a total of ten items scored based on a 5-point ordinal scale (ranging from 4 to 0), with ten tasks. The 40 scores indicate independent performance, while the 25 scores or less indicate an inability to perform the balance task which means the falling risk is at a high level. It is quick and easy to administer, requiring minimal space, and simple equipment, and takes 10–12 min to complete [8, 14, 23]. The original version of FAB for adults has shown high test re-test reliability (r=0.96) and inter-rater reliability (r=0.92), with good correlation with the BBS (r=0.75, P<0.001) [8, 14, 23]. In this study, the Iranian version of the FAB, which has excellent test re-test reliability (ICC=0.97, P<0.001, 95% CI, 0.90%, 0.98%) and inter-rater reliability (ICC=0.92, P<0.001, 95% CI, 0.89%, 0.96%) in older adults was used [10].
Statistical analysis
The data were analyzed at P<0.05 the statistical significance level by IBM SPSS software, version 21. Demographic data were shown as to frequency, percentage, mean, and standard deviation. Psychometric properties of the Iranian version of the FAB, containing internal consistency, test re-test reliability (ICC [95% CI]), content, concurrent (compared to the PBBS) validity, and discriminate ability, were also reported.
Translation for CP population
Azad et al. translated the FAB into the Persian language according to the international quality of life assessment [10]. In this study, the process of translation for FAB in children with CP was performed based on only the final step of the Beaton guideline (cognitive debriefing and pre-testing step) [19]. This step involved using the cognitive interview method to investigate each patient’s understanding of the Iranian version of the FAB items, determining cognitive equivalence, and conducting debriefing. The Iranian version of the FAB was tested on 10 children with CP (three boys and seven girls) to assess its relevance, comprehensiveness and clarity.
Reliability
ICC and Cronbach α were calculated for the determination of the reliability and internal consistency, respectively. Test re-test reliability was assessed by performing the Iranian version of the FAB two times at two-week intervals. ICC was scored on a range of 0-1, interpreted as good with >0.7 [24]. Meanwhile, the Cronbach α coefficient is interpreted as excellent (α>0.90), good (0.80-0.90), acceptable (0.70-0.80), questionable (0.60-0.70), poor (0.50-0.60) and unacceptable (α<0.50) [25]. Minimal detectable change (MDC=1.96 ×2√SEM). that is the smallest change score beyond random error, standard error measurement (SEM=SD√[1–ICC]) and the smallest detectable change (SDC=2.77×SEM) were computed [26].
Content and concurrent validity
Content validity was evaluated based on the Lawshe model by 12 experts (two physiotherapists and 10 occupational therapists) in convenience sampling [27]. The content validity was estimated by computing the content validity ratio (CVR) and content validity index (CVI) for all items [27]. The necessity of the questionnaire items was rated on a triple Likert scale from “it is necessary,” “it is useful but not necessary” and “unnecessary.” Meanwhile, the CVR was calculated using Equation 2.
Content validity ratio (Equation 2)
Note: Ne: The number of experts indicating “essential”; N: The total number of experts.
The experts analyzed the items about relativity, simplicity, and clarity using a 4-point Likert scale from 1 (the lowest) to 4 (the highest). Afterward, the CVI was computed for each item using Equation 3.
Content validity index (Equation 3)
The concurrent validity of the Iranian version of the FAB was computed by calculating the Spearman rank correlation coefficients to quantify the relationship between Iranian version of the FAB and PBBS, which >0.7 was interpreted as good concurrent validity [28].
The area under the curve (AUC) derived from receiver operating curves (ROC) was used to discriminate the validity of the FAB to test the ability of the FAB to distinguish between the higher function children with CP and healthy children. The AUC values were explained as follows: AUC=0.50: No discrimination; 0.70≤AUC<0.80: Acceptable discrimination; 0.80≤AUC<0.90: Excellent discrimination; and AUC≥0.90: Outstanding discrimination [29]. The best cut-off value for the total score was calculated based on Youden’s index [30].
Study procedure
The agreement was received from Rose, developer of the FAB [8] and Azad [10], the translator of the FAB to the Persian language. The implementation of the study was explained to children and their parents, voluntary written consent was attained and assured them that all information would be maintained in strict confidentiality.
Two expert occupational therapists interviewed the parents of the children and gathered the demographic data, determined the children’s level of gross motor function using GMFCS. The children with CP eligibility were tested by the Iranian version of the FAB and PBBS in the center where they were treated. To investigate the scale’s discriminative validity, healthy children who matched with age and gender in kindergartens and elementary schools were also tested by the Iranian version of the FAB and PBBS. Finally, 17 children with CP were tested for the Iranian version of the FAB two weeks later again to study its test re-test reliability.
Results
The demographic characteristics of the 112 participants in the two groups (CP group and healthy group) are given in Table 1.
Translation for CP population
The result of the final step of the Beaton guideline indicated that all children who participated in this study understood all the Iranian version of the FAB items with no difficulty.
Reliability
The ICC item was 0.98, >0.75, indicating good reliability of the test [24]. The Cronbach α coefficient in this study was found to be 0.99. This value is more than 0.70, which indicates the excellent internal consistency of the test [25]. The SEM: 1.86×0.11=0.22, MDC: 1.96×0.93=1.83, SDC: 2.77×0.22=0.61 were founded for Iranian version of the FAB.
Content, concurrent validity and discriminate ability
The results of CVI and CVR scores have been listed in Table 2.
The CVI and CVR values were between 0.83 and 1, which is acceptable. Therefore, all items have good content validity. The Spearman rank correlation coefficients between the Iranian version of the FAB and PBBS indicated good concurrent validity of the Iranian version of the FAB (r=0.91, P<0.001). Regarding discriminate validity, the value of AUC was 0.96 (95% CI, 0.93%, 0.99%) which shows excellent discrimination, the score of 31.5 of the FAB had the best sensitivity (0.89), specificity (0.11) cut-off value to detect the higher function children with CP and healthy children (Figure 1).
Furthermore, the value of AUC was 0.94 (95% CI, 0.93%, 0.98%) which shows excellent discrimination, the score of 49.5 of the P-PBS had the best sensitivity (0.78), specificity (0.04), cut-off value to detect the children with CP and healthy children (Figure 2).
Discussion
The main goals of this research were to investigate the reliability and validity of Iranian version of the FAB for children with CP. The results showed an acceptable internal consistency, and test re-test reliability for the Iranian version of the FAB. The FAB has been translated and validated in different languages: Korean [18], Turkish [13] and German [12]. Our results revealed similar or close internal consistency and test re-test reliability compared to the Korean study on children with CP (test re-test=0.99, internal consistency with Cronbach α=0.92) [18], as well as the Turkish version for children with CP (test re-test=0.99, internal consistency with Cronbach α=0.94) [17] and other studies with elderly on originally version (test re-test=0.96) [8], Persian version (test re-test=0.97, internal consistency with Kappa coefficient=0.8) [10] and German version (test re-test=0.96, internal consistency with Cronbach α=0.98) [12]. These results could be related to the appropriated time-space of the test re-test [23], good structure of questions for understanding and performing, and easy scoring instruction of the FAB [31].
We found a good correlation between Iranian version of the FAB and PBBS (r=0.91) for children with CP in a manner similar to that reported in the Turkish version (r=0.91) [17] and Korean version (r=0.60) for children with CP [18]. These findings indicated that the FAB and PBBS represent a similar structure due to containing the similar items. However, five items of FAB (items 1, 2, 3, 5, 6) are within the PBBS items, but they have different purposes. The PBB generally assesses static balance and anticipatory postural control, whereas the FAB assesses static and dynamic balance control, sensory orientation, anticipatory and reactive postural control [8]. The FAB was developed as a multinational balance scale for functionally independent older adults [8]. The results of factor analysis and Rasch analysis model in an earlier study explained two dominant factors as stationary and semi-dynamic balance and stability of gait for children with CP [18], as well as Erturan et al. reported all 10 items of FAB for the higher function children with CP define a one-dimensional scale of balance [17]. Moreover, the result of our study lined up with other previous studies: Regarding total scores of the PBBS was higher them the total score of the FAB which stated that FAB includes items to assess reactive postural control, vestibular, visual and tactile sense, in additional items of BBS and PBBS (in all version and population) are relatively easier than the FAB’s items.
The Iranian version of the FAB indicated high sensitivity to discriminate children with CP and healthy children in our study. The PBBS and FAB scales’ comparable accuracy identified functional balance ability between the higher function children with CP and healthy children with AUC of 0.94 and 0.96, respectively. In the PBBS a cut of point 49.5 points provided optimal sensitivity of 0.78 and specificity of 0.04. In the FAB scale, a cut of point 31.5 points provided an optimal sensitivity of 0.89 and a specificity of 0.11.
Kim et al. reported an AUC value of 0.79, the optimal cut-off point of 45.5 points (sensitivity=0.90, specificity=0.64) of PBBS in children with CP. However the AUC value of 0.76, the optimal cut of point of 21.5 points (sensitivity=0.90, specificity=0.62) of FAB in children with CP (age of 11.4±3.5 to 11.4±2.5 years) [32]. Franjoine et al. showed a cut of points from 23.3 points to 54.6 points (age of 2 years 4 months 13 years 7 months) in healthy children [7]. These controversies may be related to the age and balance level of participants. These studies demonstrated that the FAB with the more challenging and more difficult items than PBBS, furthermore both scales show high sensitivity versus low specificity. In this study, the higher cut of points of FAB may be related to the age of children (3-9 years).
Conclusion
This study was performed to investigate the reliability and validity of Iranian version of the FAB in higher gross motor function children with CP. The Iranian version of the FAB as a valid and reliable test can evaluate the balance of children functionally; nevertheless, it is more concise and requires less time and space for administration. This scale had a good positive correlation with PBBS.
Study limitations
This study had some limitations. We did not assess the floor and ceiling effects, whereas all items of the Turkish version of FAB were found adjust to the Rasch model, we did not reanalysis of the on the whole model and individual item fit. Conducting more comprehensive investigations is essential to recognize the item difficulty of the Iranian version of the FAB in children with CP in different types and different levels of balance function. Moreover, this question has remained whether the Iranian version of the FAB scale significant predictive measure of fall risk in the higher function children with CP.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC. 1400.191).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
This study was supported by a grant from the Clinical Research Development center, Rofeideh Rehabilitation Hospital, University Of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Grant No.: 2643).
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their sincere thanks to the Association for the Support of Children and their parents who provided their support during data collection and the Clinical Research Development Center of Rofeideh Rehabilitation Hospital, Tehran, Iran.
References
- Rosenbaum P. The definition and classification of cerebral palsy: Are we any further ahead in 2006? NeoReviews. 2006; 7(11):e569-74. [DOI:10.1542/neo.7-11-e569]
- Woollacott MH, Shumway-Cook A. Postural dysfunction during standing and walking in children with cerebral palsy: what are the underlying problems and what new therapies might improve balance? Neural Plasticity. 2005; 12(2-3):211-9. [DOI:10.1155/NP.2005.211] [PMID]
- Franjoine MR, Gunther JS, Taylor MJ. Pediatric balance scale: A modified version of the berg balance scale for the school-age child with mild to moderate motor impairment. Pediatric Physical Therapy. 2003; 15(2):114-28. [DOI:10.1097/01.PEP.0000068117.48023.18] [PMID]
- Verbecque E, Lobo Da Costa PH, Vereeck L, Hallemans A. Psychometric properties of functional balance tests in children: A literature review. Developmental Medicine & Child Neurology. 2015; 57(6):521-9. [DOI:10.1111/dmcn.12657] [PMID]
- Gan SM, Tung LC, Tang YH, Wang CH. Psychometric properties of functional balance assessment in children with cerebral palsy. Neurorehabilitation and Neural Repair. 2008; 22(6):745-53. [DOI:10.1177/1545968308316474] [PMID]
- Kembhavi G, Darrah J, Magill-Evans J, Loomis J. Using the berg balance scale to distinguish balance abilities in children with cerebral palsy. Pediatric Physical Therapy. 2002; 14(2):92-9. [DOI:10.1097/00001577-200214020-00005] [PMID]
- Franjoine MR, Darr N, Held SL, Kott K, Young BL. The performance of children developing typically on the pediatric balance scale. Pediatric Physical Therapy. 2010; 22(4):350-9. [DOI:10.1097/PEP.0b013e3181f9d5eb] [PMID]
- Rose DJ, Lucchese N, Wiersma LD. Development of a multidimensional balance scale for use with functionally independent older adults. Archives of physical medicine and rehabilitation. 2006; 87(11):1478-85. [DOI:10.1016/j.apmr.2006.07.263] [PMID]
- Boulgarides LK, McGinty SM, Willett JA, Barnes CW. Use of clinical and impairment-based tests to predict falls by community-dwelling older adults. Physical therapy. 2003; 83(4):328-39. [DOI:10.1093/ptj/83.4.328] [PMID]
- Azad A, Sabet A, Taghizadeh G, Mohammadi-Nezhad T. Clinical assessment of Persian translation of Fullerton Advanced Balance Scale in community-dwelling older adults. Disability and Rehabilitation. 2020; 42(4):567-73. [DOI:10.1080/09638288.2018.1503731] [PMID]
- Kim GM. Content validity of a Korean-translated version of a Fullerton Advanced Balance Scale: A pilot study. Physical Therapy Korea. 2015; 22(4):51-61. [DOI:10.12674/ptk.2015.22.4.051]
- Schott N. [Assessment of balance in community dwelling older adults: Reliability and validity of the German version of the Fullerton Advanced Balance Scale (German)]. Zeitschrift fur Gerontologie und Geriatrie. 2011; 44(6):417-28. [DOI:10.1007/s00391-011-0236-8] [PMID]
- Iyigun G, Kirmizigil B, Angin E, Oksuz S, Can F, Eker L, et al. The reliability and validity of the Turkish version of Fullerton Advanced Balance (FAB-T) scale. Archives of Gerontology and Geriatrics. 2018; 78:38-44. [DOI:10.1016/j.archger.2018.05.022] [PMID]
- Hernandez D, Rose DJ. Predicting which older adults will or will not fall using the Fullerton Advanced Balance scale. Archives of Physical Medicine and Rehabilitation. 2008; 89(12):2309-15. [DOI:10.1016/j.apmr.2008.05.020] [PMID]
- Wampler MA, Topp KS, Miaskowski C, Byl NN, Rugo HS, Hamel K. Quantitative and clinical description of postural instability in women with breast cancer treated with taxane chemotherapy. Archives of Physical Medicine and Rehabilitation. 2007; 88(8):1002-8. [DOI:10.1016/j.apmr.2007.05.007] [PMID]
- Schlenstedt C, Brombacher S, Hartwigsen G, Weisser B, Möller B, Deuschl G. Comparing the Fullerton Advanced Balance Scale with the Mini-BESTest and Berg Balance Scale to assess postural control in patients with Parkinson disease. Archives of Physical Medicine and Rehabilitation. 2015; 96(2):218-25. [DOI:10.1016/j.apmr.2014.09.002] [PMID]
- Erturan S, Atalan P, Çimen YA, Gökmen D, Sert ÖA, Yılmaz K, et al. Reliability and validity of the Turkish version of Fullerton Advanced Balance Scale in cerebral palsy. Gait & Posture. 2022; 96:295-300. [DOI:10.1016/j.gaitpost.2022.06.007] [PMID]
- Sim YJ, Kim GM, Yi CH. The reliability and validity of the Korean version of the Fullerton Advanced Balance scale in children with cerebral palsy. Physiotherapy Theory and Practice. 2019; 35(11):1087-93. [DOI:10.1080/09593985.2018.1469058] [PMID]
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000; 25(24):3186-91. [DOI:10.1097/00007632-200012150-00014] [PMID]
- Yi SH, Hwang JH, Kim SJ, Kwon JY. Validity of Pediatric Balance Scales in children with spastic cerebral palsy. Neuropediatrics. 2012; 43(6):307-13. [DOI:10.1055/s-0032-1327774] [PMID]
- Alimi E, Kalantari M, Nazeri AR, Baghban AA. Test-retest & inter-rater reliability of Persian version of Pediatric Balance scale in children with spastic cerebral palsy. Iranian Journal of Child Neurology. 2019; 13(4):163-71. [PMCID] [PMID]
- Wood E, Rosenbaum P. The gross motor function classification system for cerebral palsy: A study of reliability and stability over time. Developmental Medicine and Child Neurology. 2000; 42(5):292-6. [DOI:10.1017/S0012162200000529] [PMID]
- Klein PJ, Fiedler RC, Rose DJ. Rasch analysis of the Fullerton Advanced Balance (FAB) scale. Physiotherapy Canada. 2011; 63(1):115-25. [DOI:10.3138/ptc.2009-51] [PMID]
- Prinsen CAC, Mokkink LB, Bouter LM, Alonso J, Patrick DL, De Vet HCW, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Quality of Life Research. 2018; 27(5):1147-57. [DOI:10.1007/s11136-018-1798-3] [PMID]
- Tavakol M, Dennick R. Making sense of Cronbach’s alpha. International Journal of Medical Education. 2011; 2:53-5. [DOI:10.5116/ijme.4dfb.8dfd] [PMID]
- Turner D, Schünemann HJ, Griffith LE, Beaton DE, Griffiths AM, Critch JN, et al. The minimal detectable change cannot reliably replace the minimal important difference. Journal of Clinical Epidemiology. 2010; 63(1):28-36. [DOI:10.1016/j.jclinepi.2009.01.024] [PMID]
- Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Bosco FA, Aguinis H, Singh K, Field JG, Pierce CA. Correlational effect size benchmarks. Journal of Applied Psychology. 2015; 100(2):431-49. [DOI:10.1037/a0038047] [PMID]
- Kumar R, Indrayan A. Receiver Operating Characteristic (ROC) curve for medical researchers. Indian Pediatrics. 2011; 48(4):277-87. [DOI:10.1007/s13312-011-0055-4] [PMID]
- Youden WJ. Index for rating diagnostic tests. Cancer. 1950; 3(1):32-5. [DOI:10.1002/1097-0142(1950)3:13.0.CO;2-3] [PMID]
- Won H, Singh DKA, Din NC, Badrasawi M, Manaf ZA, Tan ST, et al. Relationship between physical performance and cognitive performance measures among community-dwelling older adults. Clinical Epidemiology. 2014; 6:343-50. [DOI:10.2147/CLEP.S62392] [PMID]
- Kim KM. [Reliability and validity study on the korean version of the fullerton Advanced Balance Scale (Korean)]. Physical Therapy Korea. 2016; 23(1):31-7. [DOI:10.12674/ptk.2016.23.1.031]
Article type: Original Research Articles |
Subject:
methodology in rehabilitation
Received: 2023/07/31 | Accepted: 2024/08/27 | Published: 2025/03/27
Received: 2023/07/31 | Accepted: 2024/08/27 | Published: 2025/03/27
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
