
988368
Mon, Jul 6, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 615-626 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ali Hosseini S, Mohammadi F, Borzuo S R, Khazaei S, Masoumi S Z. Group Play Therapy for Children with Hearing Loss. Iranian Rehabilitation Journal 2024; 22 (4) :615-626
URL: http://irj.uswr.ac.ir/article-1-2045-en.html
URL: http://irj.uswr.ac.ir/article-1-2045-en.html
Sima Ali Hosseini1 

 , Fateme Mohammadi *2 , Seyed Reza Borzuo3 , Salman Khazaei4 , Seyedeh Zahra Masoumi5
, Fateme Mohammadi *2 , Seyed Reza Borzuo3 , Salman Khazaei4 , Seyedeh Zahra Masoumi5
, Fateme Mohammadi *2 , Seyed Reza Borzuo3 , Salman Khazaei4 , Seyedeh Zahra Masoumi5
1- Student Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
2- Department of Pediatric Nursing, Chronic Diseases (Home Care) Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
3- Department of Medical Surgical Nursing, Chronic Diseases (Home Care) Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
4- Health Sciences Research Center, Health Sciences & Technology Research Institute, Hamadan University of Medical Science, Hamadan, Iran.
5- Department of Midwifery, Mother and Child Care Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
2- Department of Pediatric Nursing, Chronic Diseases (Home Care) Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
3- Department of Medical Surgical Nursing, Chronic Diseases (Home Care) Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
4- Health Sciences Research Center, Health Sciences & Technology Research Institute, Hamadan University of Medical Science, Hamadan, Iran.
5- Department of Midwifery, Mother and Child Care Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
Full-Text [PDF 587 kb]
(1390 Downloads)
| Abstract (HTML) (5736 Views)
Full-Text: (979 Views)
Introduction
Hearing loss is among the most significant and widespread chronic conditions affecting school-age children. It can be congenital or caused by physical injury or certain medications, leading to varying degrees of hearing loss and deafness [1, 2]. Hearing loss is the inability to perceive sounds above a threshold of 30 dB, while deafness is the inability to hear any sound [3].
According to a World Health Organization (WHO) report, around 5% of the world’s population is affected by hearing loss, including 34 million children. This number may double by the year 2050 [4]. In Iran, about 520000 people are deaf or hard of hearing, and the country identifies about 1500 new cases of hearing impairment every year. Of these cases, about 7% are children, and about 21% are teenagers [5].
Children with hearing loss have difficulty maintaining social interactions and making friends because they cannot listen and speak. In addition, their lack of attention to others can lead to the development of paranoid thoughts and pessimistic behaviors. As a result, these negative traits contribute to these children becoming more withdrawn, depressed, and having difficulty adapting to society [1-7].
Social adjustment refers to human engagement with others, satisfaction with one’s actions, and navigation of roles, likely influenced by personality, culture, and family relationships [8, 9]. The main elements influencing social adjustment are personal characteristics, skills, attitudes, values, physical well-being, and environmental conditions [8]. Meanwhile, the inability to socialize in teenagers with hearing loss impacts their performance and social adjustment significantly [9]. The study results show that people with hearing impairment exhibit more antisocial behaviors and have low social adjustment [3, 7, 10-15]. Low social adjustment has a negative impact on the academic performance, self-efficacy, and self-esteem of these teenagers [7, 12, 16].
Self-esteem is crucial in guiding behavior and is a fundamental aspect of shaping childhood personality. It is defined as confidence in one’s abilities and the right to be successful, live happily, and be valuable [11]. High self-esteem can create a good sense of self-efficacy in people who face problems and adversity so that these people adopt better behaviors and coping strategies when faced with problems [7, 11].
In this regard, Verdugo and Sanchez-Sandoval reported a statistically significant and positive correlation between self-esteem and life satisfaction, self-efficacy, and hope for the future in young people [10]. In contrast, most studies state that the self-esteem of children with hearing impairment is low (several references on deaf self-esteem). In this regard. Jaiyeola et al. reported that deaf and hard-of-hearing students experience mental stress, low self-esteem, and poor quality of life (QoL) [15]. Therefore, effective therapeutic interventions are necessary to reduce mental stress and improve the QoL of these children.
One of the most important therapeutic interventions to reduce psychological tensions, improve understanding, and increase children’s ability against diseases and disabilities is using children’s natural language, i.e. playing games [17]. Play therapy constitutes a therapeutic intervention designed to facilitate secure communication between the child and the therapist [18]. Play therapy has become a specialized approach because play is a key instrument for comprehending issues and addressing childhood disorders. In this method, a skilled play therapist leverages play dynamics to support and enhance children’s functioning, thus fostering optimal growth and development [19]. By engaging in play, children express emotions, disturbances, and confusion, acquiring the skills to manage and adapt to challenges [20] effectively. Indeed, through play, children attain emotional equilibrium, make more reasoned decisions, and increase their self-esteem, self-concept, and overall QoL [21]. In this regard, William Li et al. concluded that play therapy reduces anxiety and negative emotions in hospitalized children [22].
Hence, therapists, particularly pediatric nurses, should endeavor to assist children and their families in effectively managing mental and psychological tensions, isolation, depression, aggression, and other related challenges. This method involves prompt identification and intervention, adopting a realistic approach to prevailing conditions, and making more rational decisions to enhance interactions, boost self-esteem, and improve social adaptation. Pediatric nurses are responsible for providing educational and counseling support to children with chronic illnesses and their families. This service enhances treatment, promotes social adjustment, and improves overall care [16, 23-25]. No research has been conducted on the effectiveness of play therapy for children with hearing loss or its influence on their social adjustment and self-esteem. This study examines the impact of play therapy on the self-esteem and social adjustment of children with hearing loss. The hypotheses for this study are as follows:
Play therapy is efficacious in improving the self-esteem of children with hearing loss.
Play therapy is effective in the social adjustment of children with hearing loss.
Materials and Methods
Study design
The current investigation comprised a quasi-experimental study featuring an intervention and a control group. The study took place in collaboration with Hamadan University of Medical Sciences in Western Iran from March to November 2023.
Sample size
In the research conducted by Alaei Fard et al. (2020), 16 samples were determined for each group with a power of 80% and α of 0.05 [25]. Using the sample’s Mean±SD scores, it was calculated that approximately 28 samples were required. To account for a potential loss of around 20% of the samples during the study, the final sample size was set at 31 children in each group.
Study participants
After determining the sample size, 71 children were assessed for eligibility. Out of these, 9 children were found to be ineligible. Eventually, 62 children who provided written informed consent were enrolled and divided into two groups by the corresponding author. The groups were assigned using block randomization, with 31 subjects in the play therapy group and 31 in the control group. One child was removed from the intervention group due to not participating in two group game sessions, and one from the study’s control group due to unwillingness to continue the study (Figure 1).
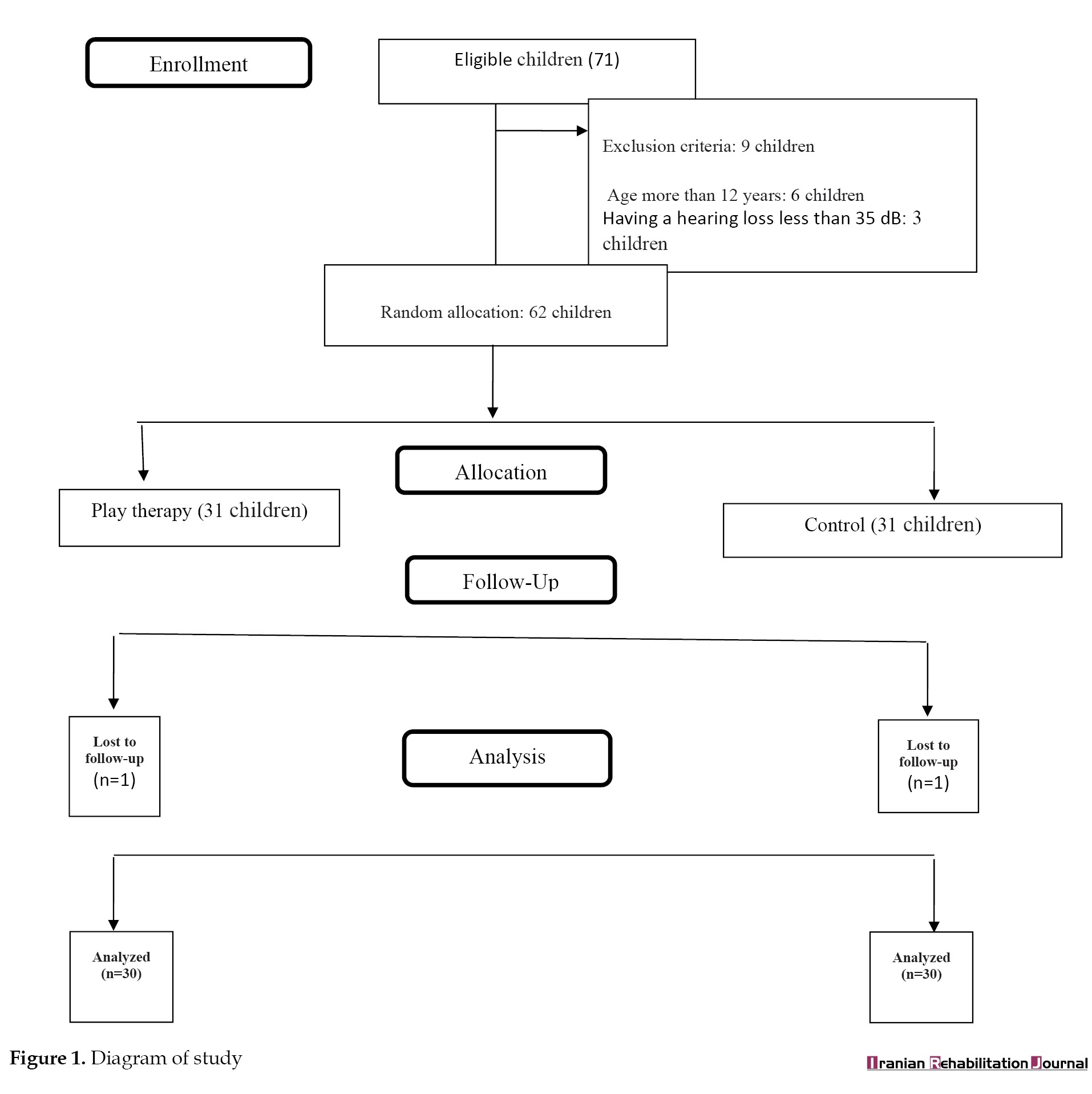 The inclusion criteria were children 8 to 12 years old, low hearing based on the auditory brainstem response test and children’s medical records, willingness to participate in this study, and lacking physical or mental disorders. The exclusion criteria were not wanting to continue the study and not participating in more than two play therapy sessions. The research assistant, blind to allocating individuals to the intervention and control groups, administered scales before and after executing the procedure for each child. Participants were excluded due to the children’s reluctance to continue their studies and frequent absence from multiple play therapy sessions throughout the study.
The inclusion criteria were children 8 to 12 years old, low hearing based on the auditory brainstem response test and children’s medical records, willingness to participate in this study, and lacking physical or mental disorders. The exclusion criteria were not wanting to continue the study and not participating in more than two play therapy sessions. The research assistant, blind to allocating individuals to the intervention and control groups, administered scales before and after executing the procedure for each child. Participants were excluded due to the children’s reluctance to continue their studies and frequent absence from multiple play therapy sessions throughout the study.
Study intervention
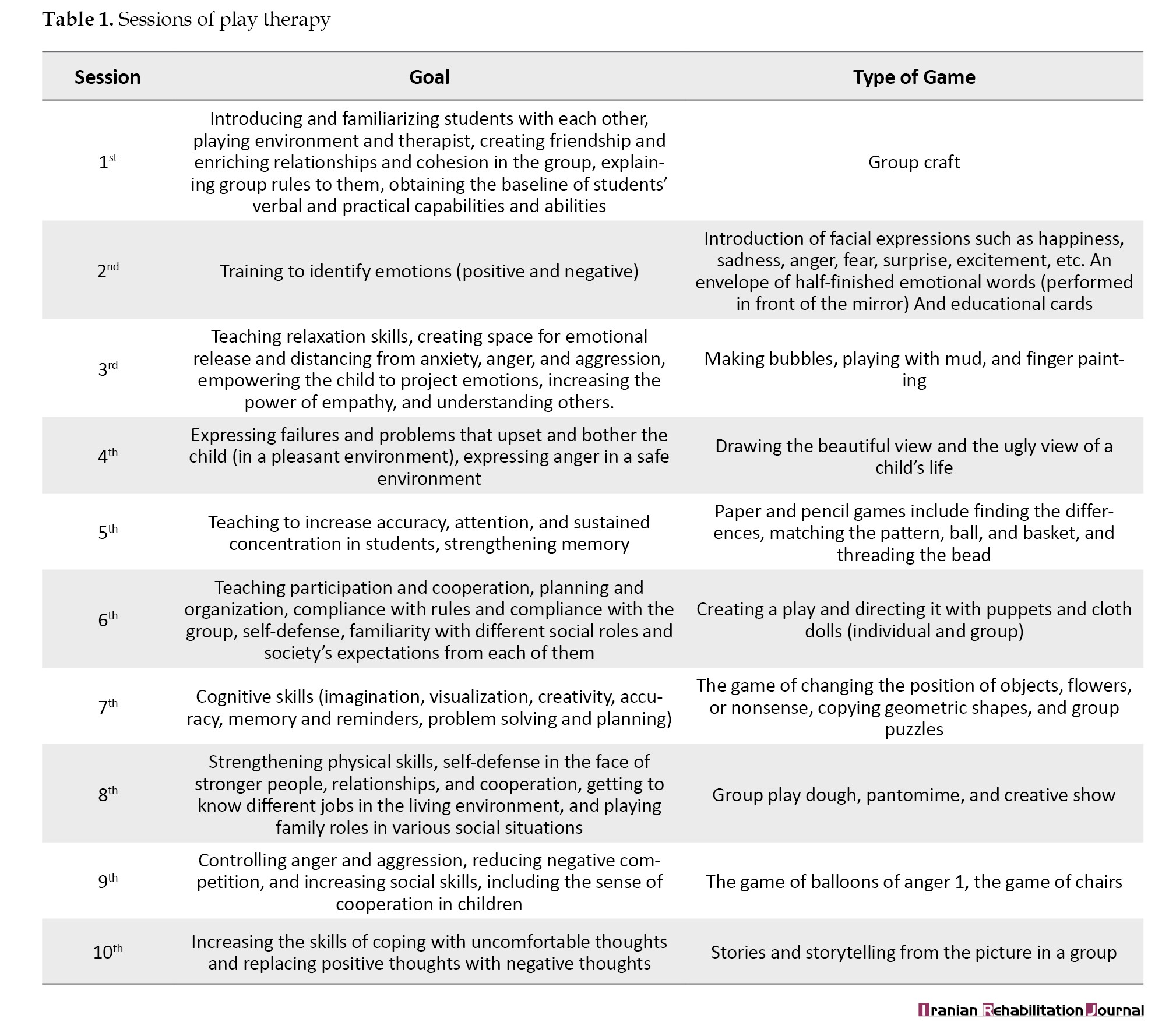
The intervention was done and written based on the TREND (the transparent reporting of evaluations with nonrandomized designs) checklist [26]. Children assigned to the intervention group were placed in a 6×6 game hall featuring a round table, chairs, bookshelves, and various game equipment. Initially, the topic was explained to the children, and once comprehension was achieved, they were organized into five groups of five individuals and one group of six. Over ten weeks, the children in the intervention group underwent training in 10 sessions per week, all conducted under the careful supervision of the researcher. At the start of every session, the researcher explained the game’s topic and proceeded to play it. The groups were then instructed to engage in a collaborative play of the same game. During this period, the researcher navigated the hall, moving among groups and providing guidance. Each gaming session lasted approximately 45 minutes, and the specific contents of these sessions are outlined in Table 1.
Children in the control group underwent standard training, and no additional measures were implemented. Questionnaires were administered to children in both groups at the study’s outset, immediately post-intervention, and one month later.
Study measures
Demographic information
The demographic information form included gender, age, paternal age, educational background, parental occupation, and economic situation.
Adaptability questionnaire of elementary school children
This questionnaire was developed in India in 1993 by Sinha from Shankar University and Singh from Panta University to determine the level of social, emotional, and educational adjustment of students. It consists of 60 yes/no questions. A low score indicates a better adjustment, and a higher score indicates a lower adjustment person [27]. The findings from the study conducted by Jovanmard et al. (2018) demonstrated a commendable validity and reliability for this instrument, with a measure of 0.87 compared to Richardson’s approach [28].
Cooper Smith self-esteem inventory
Cooper Smith self-esteem questionnaire (1967) was created to measure students’ sense of self-worth in social and academic fields. This questionnaire has 58 yes/no questions. The four subscales are general self-esteem (26 items), social self-esteem (8 items), family self-esteem (8 items), and academic self-esteem (8 items). The subject’s overall score will vary between 0 and 50. The minimum score of the subscale will be general self-esteem (0-26), social self-esteem (0-8), academic self-esteem (0-8), and family self-esteem (0-8). Also, 8 questions serve as lie detectors. These questions are not taken into account when calculating the overall score. If the respondent scores more than 4 points on the aforementioned questions, it indicates a low test validity. It suggests that the subjects attempted to present themselves in a more favorable light than they genuinely were. A higher score indicates higher self-esteem [29]. The research results by Ahmadi et al. (2004) showed that this tool has a good validity and reliability of 0.79, as calculated by the Cronbach α method [30].
Data analysis
Descriptive and inferential statistical methods were utilized for data analysis using the SPSS statistical software, version 22. The demographic characteristics were assessed in three study groups using analysis of variance (ANOVA) and the chi-square test to determine any differences. According to the Kolmogorov-Smirnov test, the data were found to have a normal distribution. Thus, each group’s average scores before and after social coping and self-esteem were compared using repeated measurement tests. Average scores before and after social coping and self-esteem were compared using an independent t-test between the two groups. P<0.05 were considered statistically significant.
Results
Sample characteristics
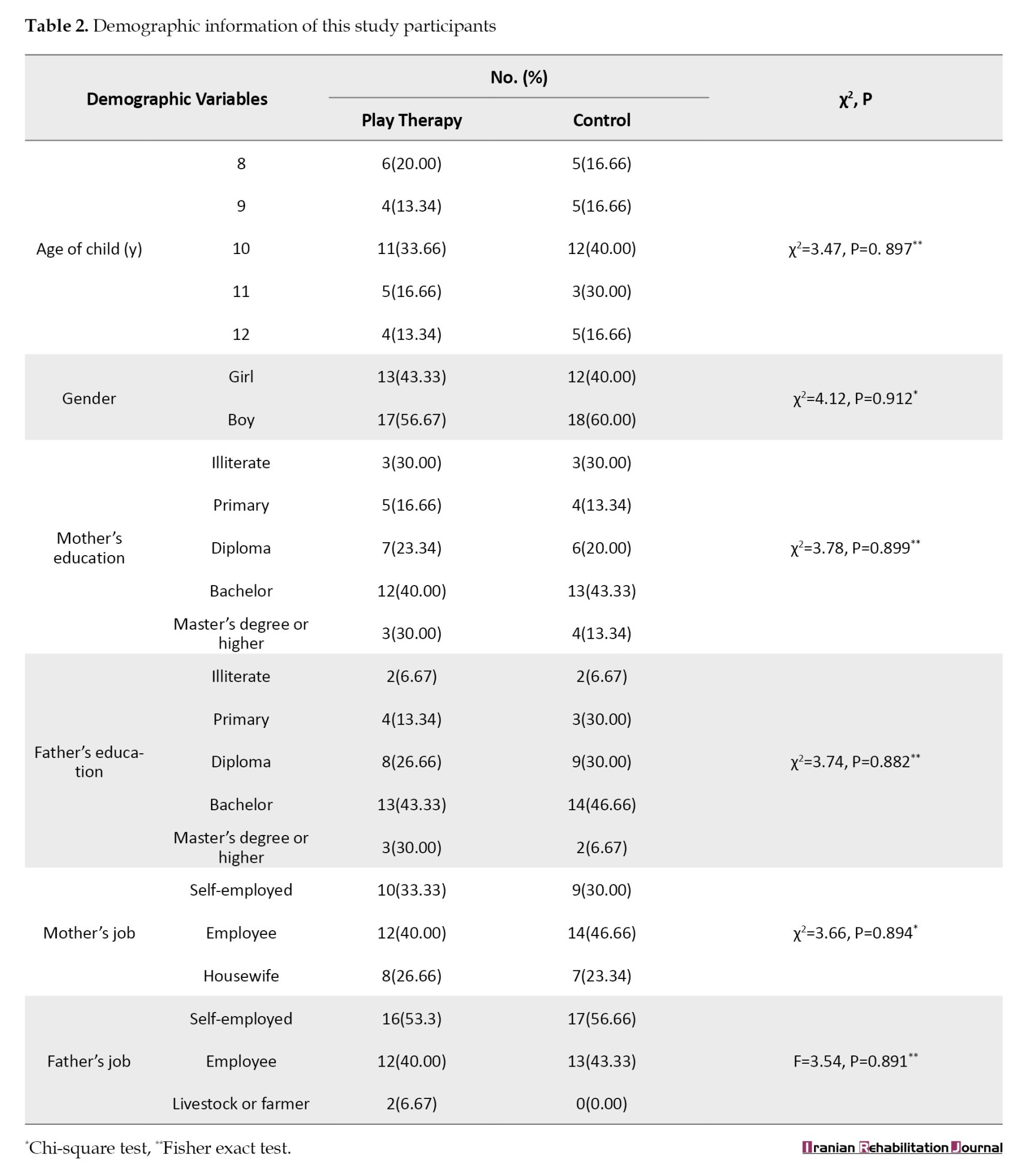
The mean age of children in the intervention group was 10.01±2.41 years, while in the control group, it was 10.22±2.54 years. Most children in both groups were boys and had a hearing of 60 dB. Additionally, the mean age of mothers in the intervention group was 36.27±2.24 years, and the mean age of fathers was 44.27±2.47 years. The control group consisted of mothers with a mean age of 36.225±2.15 years and fathers with a mean age of 41.43±2.37 years. In addition, most parents in both groups had at least a Bachelor’s degree and were employed. No significant difference was shown between the two groups regarding demographic characteristics. (Table 2).
Adaptability in children
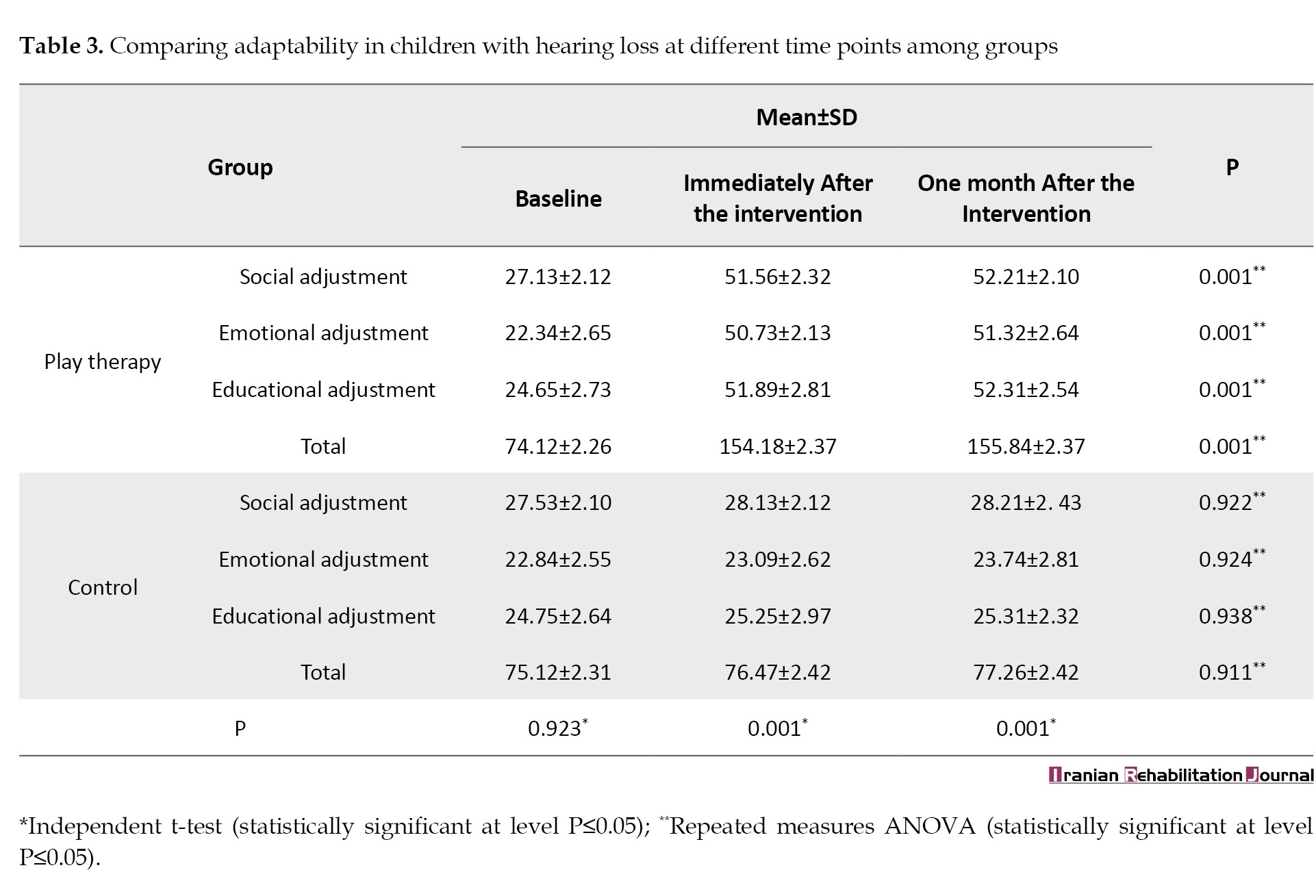
The two groups’ adaptability was compared using a dependent t-test. Initially, this test indicated no significant difference between the two groups (P=0.92). However, upon concluding the study, a statistically significant difference was observed (P<0.001). Furthermore, the intervention group exhibited a significant difference, evidenced by the repeated measures ANOVA. This test demonstrated that play therapy effectively increased adaptability immediately after the intervention and one month later (P<0.001) (Table 3).
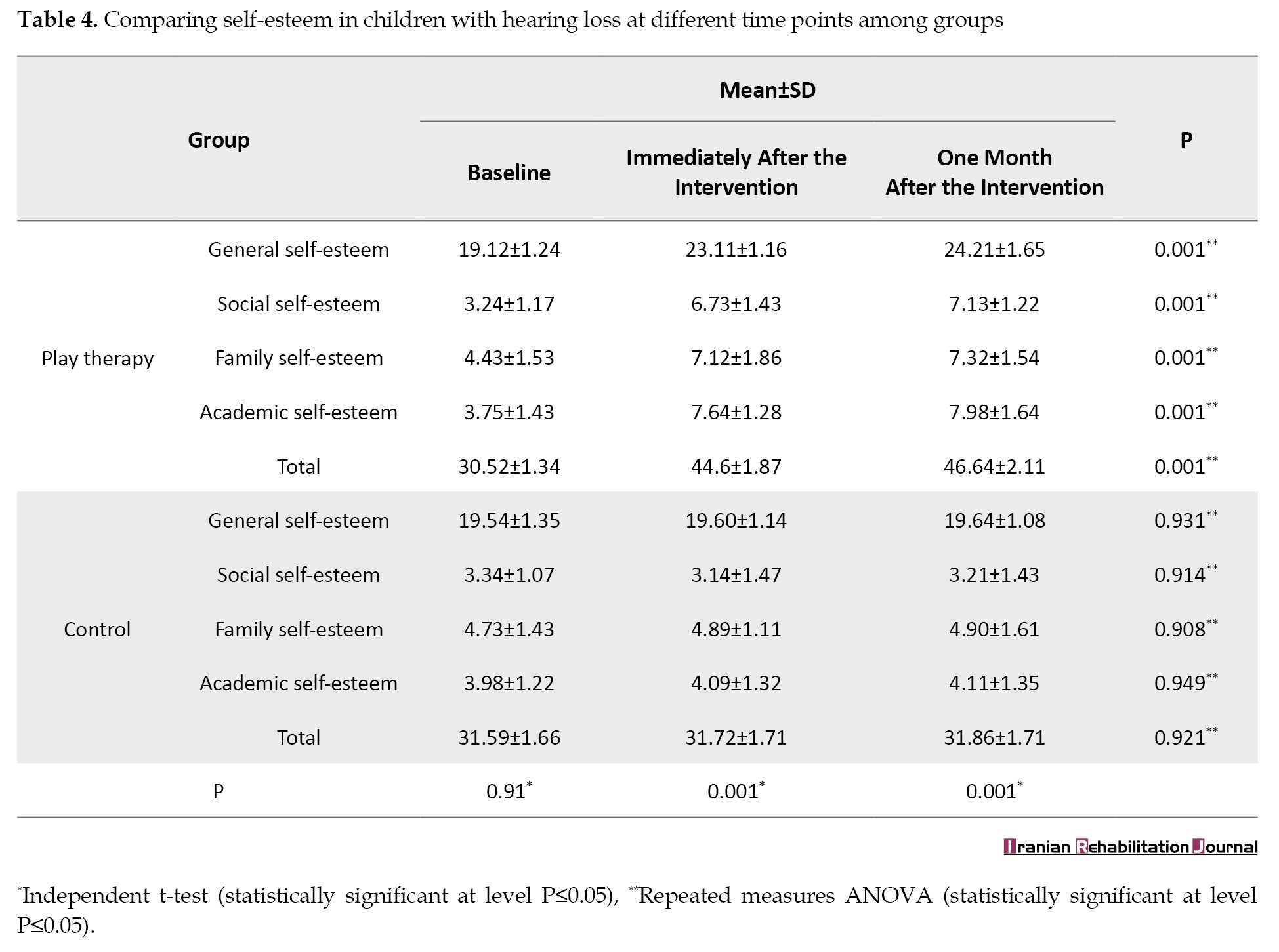
Self-esteem in children
In the first study, children in both groups had low self-esteem. There was no significant statistical difference between the two groups (P=0.91). However, the study results indicated a significant distinction between the play therapy and control groups, as demonstrated by the dependent t-test results (P=0.001). Furthermore, repeated measures ANOVA showed that self-esteem in the play therapy group compared with the control group increased immediately after the intervention and one month later (P<0.001) (Table 4).
Discussion
The present study results highlight a significantly effective improvement in adjustment and a notable upturn in the self-esteem of children with hearing impairments in the intervention group throughout the study. In addition, play therapy resulted in a noteworthy enhancement in the adjustment and self-esteem of these children compared to the control group. However, a study that simultaneously investigated the effect of play therapy on the self-esteem and adaptation of children with hearing loss is not available to the researchers. Furthermore, there is insufficient research examining the impact of play therapy on school children with hearing impairments. Consequently, the discussion incorporated studies that explored the effects of play therapy and alternative behavior management techniques on the adjustment and self-esteem of children with hearing loss. The present study findings showed that the compatibility of these children was 74.12±2.26 at the beginning of the study, which became 154.18±2.37 during the 1-month study, and 154.18±2.37 one month after the study, showing the effectiveness of this method over time in the intervention group. Also, there was a statistically significant difference in the consistency score between the intervention group and the control group both during the intervention period and one month after the intervention. Pahlavi and Ashori also reported that play therapy in the gestalt and logotherapy methods would improve the social competence and adaptation of deaf children. Although this study is in line with the current study, the study of 3- to 6-year-old deaf children and different educational content is probably the reason for the difference in children’s self-esteem from the current study [31]. Tapia-Fuselier and Ray. stated that play therapy improves language skills and subsequently improves interactions and adaptation of children with hearing disorders. While this study aligns with the current research, the variation in play therapy approaches may account for the disparity in adjustment scores among these children [32]. Zeinali Dehrajabi et al., in line with the present study, concluded that play therapy in the Axalin method would increase resilience and improve social-emotional values and, subsequently, the adaptability of children with hearing loss. Although the effective result of play therapy in promoting adaptation is in line with the present study, the difference in the adaptation score can be due to the difference in play therapy methods and the different ages of the children under study [33]. Barimani et al. also stated in their study that play therapy could improve the communication and social adaptation of deaf children. Although it confirms the effectiveness of play therapy, it has examined different variables compared to the present study in adolescents [34].
Additionally, the initial self-esteem score of the children involved in the study was 30.52±1.34 throughout the one-month study. This score increased to 46.64±2.11 one month after the study, and the self-esteem score remained high at 44.6±1.87. The results indicate that the intervention method used in the experimental group had a lasting impact. Additionally, there was a notable difference in self-esteem scores between the intervention and control groups during the one-month intervention period and even one month after the intervention. Mahmoudi et al. found that group play positively impacted the self-esteem of deaf children compared to the control group. While the previous study also demonstrated the effectiveness of play therapy on self-esteem, the present study showed even greater improvements. This disparity may be attributed to the inclusion of children with hearing loss in the present study, the larger sample size, and longer training sessions for the children involved [35].
In line with the present study findings, Yazdanipour et al. reported that group play therapy would increase resilience and improve children’s social emotions, which subsequently increase the self-esteem of these children. However, the higher self-esteem of children in this study compared to the above study can be due to the difference in the age under study [36]. In line with the present study, Ioannou et al. concluded that playing with a robot would increase the learning self-esteem and self-confidence of children with hearing disorders; however, the play therapy approach of the above study is different from the present study, which can affect the difference in outcomes [37]. In their study, Adeniyi et al. reported that behavioral self-management would reduce behavioral distress and improve the self-esteem of adolescents with hearing disorders. Although this study shows the effectiveness of behavior training and behavior management on self-esteem in children with hearing impairment, the type of intervention and the age group of the investigated male is different from the current study, which can be the possible reason for the difference in the self-esteem score [38]. Awori et al. also reported that the self-esteem of girls with hearing disorders is low, which strongly affects their academic progress, and the need for behavioral management therapeutic interventions is felt in this regard. This finding is similar to the self-esteem score of children with hearing loss at the beginning of the study and highlights the importance of behavioral training and behavioral management [39]. It is recommended that similar treatments be used in combination with group play therapy for children in Iran.
Conclusion
Play therapy has been proven to enhance adaptability and self-esteem in children with hearing loss. Therefore, policymakers and healthcare providers, particularly nurses working in service centers for the deaf and hard of hearing, should consider play therapy as a therapeutic approach to alleviate their distress and promote better social adjustment and self-assurance.
The study limitations
The low number of participants in the present study was a significant drawback. To overcome this limitation, larger sample sizes are recommended for future investigations to enhance the precision of estimates regarding the impact of play therapy on adaptability and self-esteem. Also, the study was limited to school-aged children, so it is advisable to include pre-school-aged children in future assessments to gather more accurate information regarding the effectiveness of play therapy on adaptation and self-esteem in this specific age group.
Ethical Considerations
Compliance with ethical guidelines
Ethical considerations were approved by the institutional review board of medical universities in the Western region of Iran (IR.UMSHA.REC.1401.1045). At the beginning of the study, the researcher introduced herself and explained the research objectives. Written explanations were provided to the parents of the children, who then gave their informed consent. The parents were given reassurance that their information would be kept confidential. Furthermore, the researcher emphasized that the parents could withdraw from the study without facing any adverse consequences or affecting their participation.
Funding
This research has received grants from Hamadan University of Medical Sciences.
Authors' contributions
Conceptualization, study design, and data collection: Fateme Mohammadi, Seyed Reza Borzuo, Sima Ali Hosseini, and Seyed Reza Borzuo; Data analysis: Fateme Mohammadi and Salman Khazaei; Writing and final approval: Fateme Mohammadi and Seyedeh Zahra Masoumi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Hamadan University of Medical Sciences, School of Nursing and Midwifery authorities, the participants, and others who provided valuable cooperation and assistance.
Hearing loss is among the most significant and widespread chronic conditions affecting school-age children. It can be congenital or caused by physical injury or certain medications, leading to varying degrees of hearing loss and deafness [1, 2]. Hearing loss is the inability to perceive sounds above a threshold of 30 dB, while deafness is the inability to hear any sound [3].
According to a World Health Organization (WHO) report, around 5% of the world’s population is affected by hearing loss, including 34 million children. This number may double by the year 2050 [4]. In Iran, about 520000 people are deaf or hard of hearing, and the country identifies about 1500 new cases of hearing impairment every year. Of these cases, about 7% are children, and about 21% are teenagers [5].
Children with hearing loss have difficulty maintaining social interactions and making friends because they cannot listen and speak. In addition, their lack of attention to others can lead to the development of paranoid thoughts and pessimistic behaviors. As a result, these negative traits contribute to these children becoming more withdrawn, depressed, and having difficulty adapting to society [1-7].
Social adjustment refers to human engagement with others, satisfaction with one’s actions, and navigation of roles, likely influenced by personality, culture, and family relationships [8, 9]. The main elements influencing social adjustment are personal characteristics, skills, attitudes, values, physical well-being, and environmental conditions [8]. Meanwhile, the inability to socialize in teenagers with hearing loss impacts their performance and social adjustment significantly [9]. The study results show that people with hearing impairment exhibit more antisocial behaviors and have low social adjustment [3, 7, 10-15]. Low social adjustment has a negative impact on the academic performance, self-efficacy, and self-esteem of these teenagers [7, 12, 16].
Self-esteem is crucial in guiding behavior and is a fundamental aspect of shaping childhood personality. It is defined as confidence in one’s abilities and the right to be successful, live happily, and be valuable [11]. High self-esteem can create a good sense of self-efficacy in people who face problems and adversity so that these people adopt better behaviors and coping strategies when faced with problems [7, 11].
In this regard, Verdugo and Sanchez-Sandoval reported a statistically significant and positive correlation between self-esteem and life satisfaction, self-efficacy, and hope for the future in young people [10]. In contrast, most studies state that the self-esteem of children with hearing impairment is low (several references on deaf self-esteem). In this regard. Jaiyeola et al. reported that deaf and hard-of-hearing students experience mental stress, low self-esteem, and poor quality of life (QoL) [15]. Therefore, effective therapeutic interventions are necessary to reduce mental stress and improve the QoL of these children.
One of the most important therapeutic interventions to reduce psychological tensions, improve understanding, and increase children’s ability against diseases and disabilities is using children’s natural language, i.e. playing games [17]. Play therapy constitutes a therapeutic intervention designed to facilitate secure communication between the child and the therapist [18]. Play therapy has become a specialized approach because play is a key instrument for comprehending issues and addressing childhood disorders. In this method, a skilled play therapist leverages play dynamics to support and enhance children’s functioning, thus fostering optimal growth and development [19]. By engaging in play, children express emotions, disturbances, and confusion, acquiring the skills to manage and adapt to challenges [20] effectively. Indeed, through play, children attain emotional equilibrium, make more reasoned decisions, and increase their self-esteem, self-concept, and overall QoL [21]. In this regard, William Li et al. concluded that play therapy reduces anxiety and negative emotions in hospitalized children [22].
Hence, therapists, particularly pediatric nurses, should endeavor to assist children and their families in effectively managing mental and psychological tensions, isolation, depression, aggression, and other related challenges. This method involves prompt identification and intervention, adopting a realistic approach to prevailing conditions, and making more rational decisions to enhance interactions, boost self-esteem, and improve social adaptation. Pediatric nurses are responsible for providing educational and counseling support to children with chronic illnesses and their families. This service enhances treatment, promotes social adjustment, and improves overall care [16, 23-25]. No research has been conducted on the effectiveness of play therapy for children with hearing loss or its influence on their social adjustment and self-esteem. This study examines the impact of play therapy on the self-esteem and social adjustment of children with hearing loss. The hypotheses for this study are as follows:
Play therapy is efficacious in improving the self-esteem of children with hearing loss.
Play therapy is effective in the social adjustment of children with hearing loss.
Materials and Methods
Study design
The current investigation comprised a quasi-experimental study featuring an intervention and a control group. The study took place in collaboration with Hamadan University of Medical Sciences in Western Iran from March to November 2023.
Sample size
In the research conducted by Alaei Fard et al. (2020), 16 samples were determined for each group with a power of 80% and α of 0.05 [25]. Using the sample’s Mean±SD scores, it was calculated that approximately 28 samples were required. To account for a potential loss of around 20% of the samples during the study, the final sample size was set at 31 children in each group.
Study participants
After determining the sample size, 71 children were assessed for eligibility. Out of these, 9 children were found to be ineligible. Eventually, 62 children who provided written informed consent were enrolled and divided into two groups by the corresponding author. The groups were assigned using block randomization, with 31 subjects in the play therapy group and 31 in the control group. One child was removed from the intervention group due to not participating in two group game sessions, and one from the study’s control group due to unwillingness to continue the study (Figure 1).
Study intervention
The intervention was done and written based on the TREND (the transparent reporting of evaluations with nonrandomized designs) checklist [26]. Children assigned to the intervention group were placed in a 6×6 game hall featuring a round table, chairs, bookshelves, and various game equipment. Initially, the topic was explained to the children, and once comprehension was achieved, they were organized into five groups of five individuals and one group of six. Over ten weeks, the children in the intervention group underwent training in 10 sessions per week, all conducted under the careful supervision of the researcher. At the start of every session, the researcher explained the game’s topic and proceeded to play it. The groups were then instructed to engage in a collaborative play of the same game. During this period, the researcher navigated the hall, moving among groups and providing guidance. Each gaming session lasted approximately 45 minutes, and the specific contents of these sessions are outlined in Table 1.
Children in the control group underwent standard training, and no additional measures were implemented. Questionnaires were administered to children in both groups at the study’s outset, immediately post-intervention, and one month later.
Study measures
Demographic information
The demographic information form included gender, age, paternal age, educational background, parental occupation, and economic situation.
Adaptability questionnaire of elementary school children
This questionnaire was developed in India in 1993 by Sinha from Shankar University and Singh from Panta University to determine the level of social, emotional, and educational adjustment of students. It consists of 60 yes/no questions. A low score indicates a better adjustment, and a higher score indicates a lower adjustment person [27]. The findings from the study conducted by Jovanmard et al. (2018) demonstrated a commendable validity and reliability for this instrument, with a measure of 0.87 compared to Richardson’s approach [28].
Cooper Smith self-esteem inventory
Cooper Smith self-esteem questionnaire (1967) was created to measure students’ sense of self-worth in social and academic fields. This questionnaire has 58 yes/no questions. The four subscales are general self-esteem (26 items), social self-esteem (8 items), family self-esteem (8 items), and academic self-esteem (8 items). The subject’s overall score will vary between 0 and 50. The minimum score of the subscale will be general self-esteem (0-26), social self-esteem (0-8), academic self-esteem (0-8), and family self-esteem (0-8). Also, 8 questions serve as lie detectors. These questions are not taken into account when calculating the overall score. If the respondent scores more than 4 points on the aforementioned questions, it indicates a low test validity. It suggests that the subjects attempted to present themselves in a more favorable light than they genuinely were. A higher score indicates higher self-esteem [29]. The research results by Ahmadi et al. (2004) showed that this tool has a good validity and reliability of 0.79, as calculated by the Cronbach α method [30].
Data analysis
Descriptive and inferential statistical methods were utilized for data analysis using the SPSS statistical software, version 22. The demographic characteristics were assessed in three study groups using analysis of variance (ANOVA) and the chi-square test to determine any differences. According to the Kolmogorov-Smirnov test, the data were found to have a normal distribution. Thus, each group’s average scores before and after social coping and self-esteem were compared using repeated measurement tests. Average scores before and after social coping and self-esteem were compared using an independent t-test between the two groups. P<0.05 were considered statistically significant.
Results
Sample characteristics
The mean age of children in the intervention group was 10.01±2.41 years, while in the control group, it was 10.22±2.54 years. Most children in both groups were boys and had a hearing of 60 dB. Additionally, the mean age of mothers in the intervention group was 36.27±2.24 years, and the mean age of fathers was 44.27±2.47 years. The control group consisted of mothers with a mean age of 36.225±2.15 years and fathers with a mean age of 41.43±2.37 years. In addition, most parents in both groups had at least a Bachelor’s degree and were employed. No significant difference was shown between the two groups regarding demographic characteristics. (Table 2).
Adaptability in children
The two groups’ adaptability was compared using a dependent t-test. Initially, this test indicated no significant difference between the two groups (P=0.92). However, upon concluding the study, a statistically significant difference was observed (P<0.001). Furthermore, the intervention group exhibited a significant difference, evidenced by the repeated measures ANOVA. This test demonstrated that play therapy effectively increased adaptability immediately after the intervention and one month later (P<0.001) (Table 3).
Self-esteem in children
In the first study, children in both groups had low self-esteem. There was no significant statistical difference between the two groups (P=0.91). However, the study results indicated a significant distinction between the play therapy and control groups, as demonstrated by the dependent t-test results (P=0.001). Furthermore, repeated measures ANOVA showed that self-esteem in the play therapy group compared with the control group increased immediately after the intervention and one month later (P<0.001) (Table 4).
Discussion
The present study results highlight a significantly effective improvement in adjustment and a notable upturn in the self-esteem of children with hearing impairments in the intervention group throughout the study. In addition, play therapy resulted in a noteworthy enhancement in the adjustment and self-esteem of these children compared to the control group. However, a study that simultaneously investigated the effect of play therapy on the self-esteem and adaptation of children with hearing loss is not available to the researchers. Furthermore, there is insufficient research examining the impact of play therapy on school children with hearing impairments. Consequently, the discussion incorporated studies that explored the effects of play therapy and alternative behavior management techniques on the adjustment and self-esteem of children with hearing loss. The present study findings showed that the compatibility of these children was 74.12±2.26 at the beginning of the study, which became 154.18±2.37 during the 1-month study, and 154.18±2.37 one month after the study, showing the effectiveness of this method over time in the intervention group. Also, there was a statistically significant difference in the consistency score between the intervention group and the control group both during the intervention period and one month after the intervention. Pahlavi and Ashori also reported that play therapy in the gestalt and logotherapy methods would improve the social competence and adaptation of deaf children. Although this study is in line with the current study, the study of 3- to 6-year-old deaf children and different educational content is probably the reason for the difference in children’s self-esteem from the current study [31]. Tapia-Fuselier and Ray. stated that play therapy improves language skills and subsequently improves interactions and adaptation of children with hearing disorders. While this study aligns with the current research, the variation in play therapy approaches may account for the disparity in adjustment scores among these children [32]. Zeinali Dehrajabi et al., in line with the present study, concluded that play therapy in the Axalin method would increase resilience and improve social-emotional values and, subsequently, the adaptability of children with hearing loss. Although the effective result of play therapy in promoting adaptation is in line with the present study, the difference in the adaptation score can be due to the difference in play therapy methods and the different ages of the children under study [33]. Barimani et al. also stated in their study that play therapy could improve the communication and social adaptation of deaf children. Although it confirms the effectiveness of play therapy, it has examined different variables compared to the present study in adolescents [34].
Additionally, the initial self-esteem score of the children involved in the study was 30.52±1.34 throughout the one-month study. This score increased to 46.64±2.11 one month after the study, and the self-esteem score remained high at 44.6±1.87. The results indicate that the intervention method used in the experimental group had a lasting impact. Additionally, there was a notable difference in self-esteem scores between the intervention and control groups during the one-month intervention period and even one month after the intervention. Mahmoudi et al. found that group play positively impacted the self-esteem of deaf children compared to the control group. While the previous study also demonstrated the effectiveness of play therapy on self-esteem, the present study showed even greater improvements. This disparity may be attributed to the inclusion of children with hearing loss in the present study, the larger sample size, and longer training sessions for the children involved [35].
In line with the present study findings, Yazdanipour et al. reported that group play therapy would increase resilience and improve children’s social emotions, which subsequently increase the self-esteem of these children. However, the higher self-esteem of children in this study compared to the above study can be due to the difference in the age under study [36]. In line with the present study, Ioannou et al. concluded that playing with a robot would increase the learning self-esteem and self-confidence of children with hearing disorders; however, the play therapy approach of the above study is different from the present study, which can affect the difference in outcomes [37]. In their study, Adeniyi et al. reported that behavioral self-management would reduce behavioral distress and improve the self-esteem of adolescents with hearing disorders. Although this study shows the effectiveness of behavior training and behavior management on self-esteem in children with hearing impairment, the type of intervention and the age group of the investigated male is different from the current study, which can be the possible reason for the difference in the self-esteem score [38]. Awori et al. also reported that the self-esteem of girls with hearing disorders is low, which strongly affects their academic progress, and the need for behavioral management therapeutic interventions is felt in this regard. This finding is similar to the self-esteem score of children with hearing loss at the beginning of the study and highlights the importance of behavioral training and behavioral management [39]. It is recommended that similar treatments be used in combination with group play therapy for children in Iran.
Conclusion
Play therapy has been proven to enhance adaptability and self-esteem in children with hearing loss. Therefore, policymakers and healthcare providers, particularly nurses working in service centers for the deaf and hard of hearing, should consider play therapy as a therapeutic approach to alleviate their distress and promote better social adjustment and self-assurance.
The study limitations
The low number of participants in the present study was a significant drawback. To overcome this limitation, larger sample sizes are recommended for future investigations to enhance the precision of estimates regarding the impact of play therapy on adaptability and self-esteem. Also, the study was limited to school-aged children, so it is advisable to include pre-school-aged children in future assessments to gather more accurate information regarding the effectiveness of play therapy on adaptation and self-esteem in this specific age group.
Ethical Considerations
Compliance with ethical guidelines
Ethical considerations were approved by the institutional review board of medical universities in the Western region of Iran (IR.UMSHA.REC.1401.1045). At the beginning of the study, the researcher introduced herself and explained the research objectives. Written explanations were provided to the parents of the children, who then gave their informed consent. The parents were given reassurance that their information would be kept confidential. Furthermore, the researcher emphasized that the parents could withdraw from the study without facing any adverse consequences or affecting their participation.
Funding
This research has received grants from Hamadan University of Medical Sciences.
Authors' contributions
Conceptualization, study design, and data collection: Fateme Mohammadi, Seyed Reza Borzuo, Sima Ali Hosseini, and Seyed Reza Borzuo; Data analysis: Fateme Mohammadi and Salman Khazaei; Writing and final approval: Fateme Mohammadi and Seyedeh Zahra Masoumi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Hamadan University of Medical Sciences, School of Nursing and Midwifery authorities, the participants, and others who provided valuable cooperation and assistance.
References
- Jalali MM, Nezamdoust F, Ramezani H, Pastadast M. Prevalence of hearing loss among school-age children in the north of Iran. Iranian Journal of Otorhinolaryngology. 2020; 32(109):85. [DOI: 10.22038/ijorl.2019.36090.2191]
- Tutuk HC, Gürgür H. Caregiver involvement in support services for a child with hearing loss? Journal of Childhood, Education & Society. 2024; 5(2):256-69. [DOI: 0.37291/2717638X.202452363]
- Jabeen T, Malik S. Level of depression, anxiety and stress among deaf adults: A literature review. ISRA Medical Journal. 2019; 11(4):345-8. [Link]
- WHO. Addressing the rising prevalence of hearing loss. Geneva: World Health Organization; 2018. [Link]
- Stevens G, Flaxman S, Brunskill E, Mascarenhas M, Mathers CD, Finucane M. Global and regional hearing impairment prevalence: An Analysis of 42 studies in 29 countries. The European Journal of Public Health. 2013 Feb 1;23(1):146-52.
- Absalan A, Pirasteh I, Dashti Khavidaki GA, Asemi rad A, Nasr Esfahani AA, Nilforoush MH. A prevalence study of hearing loss among primary school children in the south east of Iran. International Journal of Otolaryngology. 2013; 2013(1):138935. [DOI: 10.1093/eurpub/ckr176] [PMID]
- Yigider AP, Yilmaz S, Ulusoy H, Kara T, Kufeciler L, Kaya KH. Emotional and behavioral problems in children and adolescents with hearing loss and their effects on quality of life. International Journal of Pediatric Otorhinolaryngology. 2020; 137:110245. [DOI: 10.1016/j.ijporl.2020.110245] [PMID]
- Terziev V. The dependence social adaptation-socialization. IJASOS-International E-journal of Advances in Social Sciences. 2019; 5(13):258-65. [DOI:10.18769/ijasos.531311]
- Adeniyi SO, Olufemi-Adeniyi OA, Raheem AW. Efficacy of cognitive therapy on the management of psychological distress among adolescents with hearing impairment in Oyo State. International Journal of Special Education (IJSE). 2021; 36(2):90–7. [DOI:10.52291/ijse.2021.36.21]
- Verdugo L, Sánchez-Sandoval Y. Psychological and social adjustment as antecedents of high school students’ future expectations. Journal of Psychologists and Counsellors in Schools. 2022; 32(1):39-53. [DOI: 10.1017/jgc.2020.1]
- Warner-Czyz AD, Loy BA, Evans C, Wetsel A, Tobey EA. Self-esteem in children and adolescents with hearing loss. Trends in hearing. 2015; 19:2331216515572615. [DOI: 10.1177/2331216515572615]
- Ishtiaq N, Mumtaz N, Saqulain G. Stress and coping strategies for parenting children with hearing impairment and autism. Pakistan Journal of Medical Sciences. 2020; 36(3):538. [DOI: 10.12669/pjms.36.3.1766] [PMID]
- Vovchenko OA. Emotional and behavioural reactions of high school students with special educational needs (hearing impairments) under stress. Scientific Bulletin of Mukachevo State University, Series Pedagogyand Psychology. 8(3):23-32. [DOI: 10.52534/msu-pp.8(2).2022.23-32]
- le Clercq CM, Labuschagne LJ, Franken MC, de Jong RJ, Luijk MP, Jansen PW, van der Schroeff MP. Association of slight to mild hearing loss with behavioral problems and school performance in children. JAMA Otolaryngology–Head & Neck Surgery. 2020 Feb 1;146(2):113-20. [DOI: 10.1001/jamaoto.2019.3585] [PMID]
- Jaiyeola MT, Adeyemo AA. Quality of life of deaf and hard of hearing students in Ibadan metropolis, Nigeria. PLoS One. 2018; 13(1):e0190130. [DOI:10.1371/journal.pone.0190130] [PMID]
- Awori BB, Karugu GK, Mugo J, Orodho JA. Self-esteem and academic achievement: What are the explanatory variables among girls with hearing impairment in selected secondary schools for the deaf in Kenya. Greener Journal of Educational Research. 2019; 9(1):16-26. [DOI:10.15580/GJER.2019.1.013119025]
- Ibrahim HA, Amal AA. The effectiveness of play therapy in hospitalized children with cancer: Systematic review. Journal Of Nursing Practice. 2020; 3(2):233-43. [DOI:10.30994/jnp.v3i2.92]
- Cochran NH, Nordling WJ, Cochran JL. Child-centered play therapy: A practical guide to therapeutic relationships with children. Oxfordshire: Routledge; 2023. [Link]
- Haas SC, Ray DC. Child-centered play therapy with children affected by adverse childhood experiences: A single-case design. International Journal of Play Therapy. 2020; 29(4):223-36. [DOI:10.1037/pla0000135]
- Wilson K, Ryan V. Play therapy: A non-directive approach for children and adolescents. Amsterdam: Elsevier Health Sciences; 2006. [Link]
- Elbeltagi R, Al-Beltagi M, Saeed NK, Alhawamdeh R. Play therapy in children with autism: Its role, implications, and limitations. World Journal of Clinical Pediatrics. 2023 Jan 1;12(1):1. [DOI: 10.5409/wjcp.v12.i1.1] [PMID]
- William Li HC, Lopez V, Lee TL. Effects of preoperative therapeutic play on outcomes of school‐age children undergoing day surgery. Research in nursing & health. 2007 Jun;30(3):320-32.
- Warner-Czyz AD, Loy B, Tobey EA, Nakonezny P, Roland PS. Health-related quality of life in children and adolescents who use cochlear implants. International Journal of Pediatric Otorhinolaryngology. 2011; 75(1):95-105. [DOI:10.1016/j.ijporl.2010.10.018] [PMID]
- Meyer A, Sie K, Skalicky A, Edwards TC, Schick B, Niparko J, et al. Quality of life in youth with severe to profound sensorineural hearing loss. JAMA Otolaryngology-Head & Neck Surgery. 2013; 139(3):294-300. [DOI:10.1001/jamaoto.2013.35] [PMID]
- Alaii Fard N, Ahadi H, Mehrvarz A, Jomehri F, Dolatabadi S. A comparative study on the effectiveness of play therapy and story therapy on depression and anxiety skills in children with leukemia. Razavi International Journal of Medicine. 2022; 10(4):9-14. [DOI: 10.30483/rijm.2022.254299.1131]
- Kruschke JK. Bayesian analysis reporting guidelines. Nature human behaviour. 2021; 5(10):1282-91. [DOI: 10.1038/s41562-021-01177-7] [PMID]
- Sinha AK, Singh RP. The adjustment inventory for school students (AISS). Agra: National Psychological Corporation. 1993. [Link]
- Javanmard J, Rajaee A, Khodrowpour F. [Effectiveness of Group Positive Psychotherapy on social, emotional and educational adaptability of junior high school maladaptive boy students (Persian)]. Quarterly of Applied Psychology. 2019; 13(2):209-27. [DOI: 10.29252/apsy.13.2.209]
- Johnson BW, Redfield DL, Miller RL, Simpson RE. The Coopersmith self-esteem inventory: A construct validation study. Educational and Psychological Measurement. 1983; 43(3):907-13. [DOI: 10.1177/0013164483043003]
- Ahmadi P, Zarean Z, Ebrahimpor M. [The effect of the flipped learning method on the self-esteem of elementary school students (Persian)]. Quarterly Journal of Education Studies. 2023; 9(34):35-48. [Link]
- Pahlavi M, Ashori M. [Comparing the effect of gestalt playtherapy and lego therapy on the socio-emotional competence in deaf children (Persian)]. Journal of Exceptional Children. 2021; 21(4):7-20. [Link]
- Tapia-Fuselier JL, Ray DC. Culturally and linguistically responsive playtherapy: Adapting child-centered play therapy for deaf children. International Journal of Play Therapy. 2019; 28(2):79-87. [DOI:10.1037/pla0000091]
- Zeinali Dehrajabi Z, Ashori M. [The effect of play therapybased on axline approach on the social-emotional assets and resilience of preschool children with hearing loss (Persian)]. Positive Psychology Research. 2021; 7(4):13-24.[DOI:10.22108/ppls.2022.130700.2194]
- Barimani S, Asadi J, Khajevand A. [The effectiveness of play therapy on deaf children’s social adaptation and communication skills (Persian)]. Archives of Rehabilitation. 2018; 19(3):250-61. [DOI:10.32598/rj.19.3.250]
- Mahmoodi A, Mashayekh M, Zam F, Shahnazari M, Peymani J. The effectiveness of group play therapy with cognitive-behavioral approach on anxiety and self-esteem of deaf students. Journal of Sabzevar University of Medical Sciences. 2022; 29(1):115-31. [Link]
- Yazdanipour M, Ashori M, Abedi A. Impact of group theraplay on the social-emotional assets and resilience in children with hearing loss. International Journal of Play Therapy. 2022; 31(2):107-18. [DOI:10.1037/pla0000175]
- Ioannou A, Andreva A. Play and learn with an intelligent robot: Enhancing the therapy of children with hearing loss. Paper presented at: IFIP Conference on Human-Computer Interaction. 2–6 September 2019; Paphos: Cyprus. [Link]
- Adeniyi SO, Olufemi-Adeniyi OA, Raheem AW. Efficacy of cognitive therapy on the management of psychological distress among adolescents with hearing impairment in Oyo State. International Journal of Special Education (IJSE). 2021; 36(2):90–7. [DOI:10.52291/ijse.2021.36.21]
- Awori BB, Karugu GK, Mugo J, Orodho JA. Self-esteem and academic achievement: What are the explanatory variables among girls with hearing impairment in selected secondary schools for the deaf in Kenya. Greener Journal of Educational Research. 2019; 9(1):16-26. [DOI:10.15580/GJER.2019.1.013119025]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2023/08/12 | Accepted: 2023/12/30 | Published: 2024/12/20
Received: 2023/08/12 | Accepted: 2023/12/30 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
