
988368
Mon, Jul 27, 2026

Volume 23, Issue 2 (June 2025)
Iranian Rehabilitation Journal 2025, 23(2): 183-190 |
Back to browse issues page


Ethics code: 703/UN.16.2/KEP-FK/2022
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fitria N, Agustina W, Sari Y O. Individuals’ Quality of Life Affected by Pulmonary Tuberculosis in and After Intensive Rehabilitation Therapy. Iranian Rehabilitation Journal 2025; 23 (2) :183-190
URL: http://irj.uswr.ac.ir/article-1-2058-en.html
URL: http://irj.uswr.ac.ir/article-1-2058-en.html



1- Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Andalas, Padang, Indonesia.
2- Bachelor Program, Faculty of Pharmacy, Universitas Andalas, Padang, Indonesia.
2- Bachelor Program, Faculty of Pharmacy, Universitas Andalas, Padang, Indonesia.
Keywords: Quality of life (QoL), Pulmonary tuberculosis (TB), World Health Organization’s quality of life questionnaire (WHOQOL-BREF)
Full-Text [PDF 493 kb]
(934 Downloads)
| Abstract (HTML) (4043 Views)
Full-Text: (358 Views)
Introduction
In 2019, the World Health Organization (WHO) reveal ed 10 million tuberculosis (TB) cases worldwide and an estimated 1.2 million deaths from TB cases globally. Based on the latest WHO 2020 data, Indonesia ranks second after India, with the number of TB cases increasing from 331 703 in 2015 to 562 049 cases in 2019 [1]. The prevalence of the Indonesian population diagnosed with TB by health workers reached 0.42% of the entire Indonesian population, with the highest rate occurring at the age of 65-74 years, reaching 1%, and the lowest at the age of <1 year with a value of 0.1% [2], where TB cases in West Sumatra reached 0.31% [3].
The main symptom of patients with pulmonary TB is coughing up phlegm for 2-3 weeks or more. Cough is usually followed by additional symptoms, such as coughing up blood, phlegm mixed with blood, shortness of breath, decreased appetite, weakness, decreased body weight, sweating at night without activity, and fever for over a month. Because the prevalence of TB in Indonesia is quite high, everyone who comes to the health service unit (UPK) with these symptoms is considered a patient diagnosed with TB and must undergo a direct microscopic examination of the sputum [4].
After a person is diagnosed with pulmonary TB, several impacts will appear in their life, both physically, psychologically, socially, and economically [5]. The identification and treatment of TB incur costs. However, patients must still pay for transportation, accommodation, food, or nutrition costs during treatment and loss of income due to being unable to work [6]. TB contributes to the exacerbation of social stigma and even to being ostracized from society [7]. A previous study by Kristina et al. among 156 respondents revealed that the mean quality of life (QoL) scores among TB patients in referral hospitals in Yogyakarta were lower than the normal range (60.45±12.23) [8]. A decrease in QoL is related to their health status because it causes delays in treatment and negatively impacts the continuity of treatment, which causes treatment to be interrupted or incomplete [9-11].
WHO recommends directly observed treatment short-course (DOTS) treatment accompanied by direct observation. The DOTS strategy is implemented at government health facilities, with Puskesmas as a parameter for program implementation success. Patient recovery is a parameter of the success of TB control efforts. This cure, besides reducing the number of sufferers, can also prevent transmission [12]. Efforts to control TB are made using medication. The treatment used is a combination therapy of several types of TB drugs, with a minimum span of six months, consisting of the first two months of the intensive phase of treatment consisting of isoniazid (INH), rifampin (RIF), pyrazinamide, and ethambutol, followed by four months with a daily regimen of INH and RIF [13].
The TB patients’ QoL is crucial to assess because it affects all aspects of a person’s QoL, including physical, social, psychological, and environmental health. QoL assessment is useful for assessing the success of health services in terms of prevention and treatment. A person with a chronic disease (i.e. pulmonary TB) can have extended periods despite the challenges of their illness, underscoring the importance of health services focusing on improving their QoL [14].
Based on a preliminary study conducted at the Pauh Health Center in Padang City, Indonesia, 78 patients with TB were treated from January 2021 to December 2021. Based on the description above, the incidence of TB is a major challenge for the health world, affecting the QoL of patients with TB. The effectiveness of TB patient treatment greatly depends on the patient’s routine in treatment and carrying out treatment based on the treatment that has been programmed to improve the patient’s health. Therefore, a study was conducted to observe the differences in the development of QoL among those diagnosed with pulmonary TB who received two months of treatment, encompassing intensive and follow-up post-intensive care at one of the primary centers in Padang City.
Materials and Methods
Setting, population, and sample
The samples from this study were part of or representative of the population studied, which comprised patients diagnosed with TB receiving two months of treatment, encompassing intensive and post-follow-up care, from October 2021 to February 2022. The sampling method involved purposive selection, which was non-random. All samples meeting the presence conditions were included without exception.
Research design
This investigation is a forthcoming cross-sectional study using the World Health Organization's QoL questionnaire (WHOQOL-BREF) inquiry form [14]. This study determined the patients’ QoL levels, consisting of 26 questions in five domains. The level of QoL of patients was determined using the WHOQOL-BREF questionnaire, which consists of 26 questionnaire items belonging to four domains. Several questions were used to assess each of these four domains. The answers were assessed using a Likert-style scale, allowing respondents to gauge their satisfaction or intensity by assigning ratings on a scale typically falling between 1 (indicating a high level of dissatisfaction or poor quality) and 5 (indicating a high level of satisfaction or good quality). The questionnaire can be accessed via the web [15]. For non-commercial purposes, the Indonesian version of the WHOQOL-BREF questionnaire was approved via a permissions, and the permission ID is 202300339 [16].
Inclusion criteria
The inclusion criteria included patients 18 years old or above who were diagnosed with pulmonary TB and received category one anti-TB drugs at the Pauh Health Center, Padang City. The patient had received TB treatment for at least one month and communicated well. All patients with pulmonary TB were prepared to participate as respondents by completing an informed consent document. Both women and men were allowed to respond.
Statistical analysis
A chi-square was conducted to identify variances between the intensive and post-intensive phase groups for each sociodemographic variable [17]. Data normality in this study was assessed using the Shapiro-Wilk test (small sample size of 50). The normality test obtained a value of P>0.05; therefore, the relationship between the QoL of patients with intensive-post-intensive phase pulmonary TB was analyzed using the Mann-Whitney test. No missing, discarded, or outlier data were detected.
Results
Sociodemographic characteristics of pulmonary TB patients
An overview of the sociodemographic characteristics of the 40 patients interviewed (24 men and 16 women) (Table 1). In purposive sampling, the sample was saturated until the end of the study with 40 participants. Of the 40 respondents, the highest number of respondents was males (intensive [12], post-intensive [13]), followed by females (8 and 7, respectively) (Table 1). Based on the study results, most respondents were self-employed; the same proportion of self-employed jobs existed in both the intensive and post-intensive phases (35%).
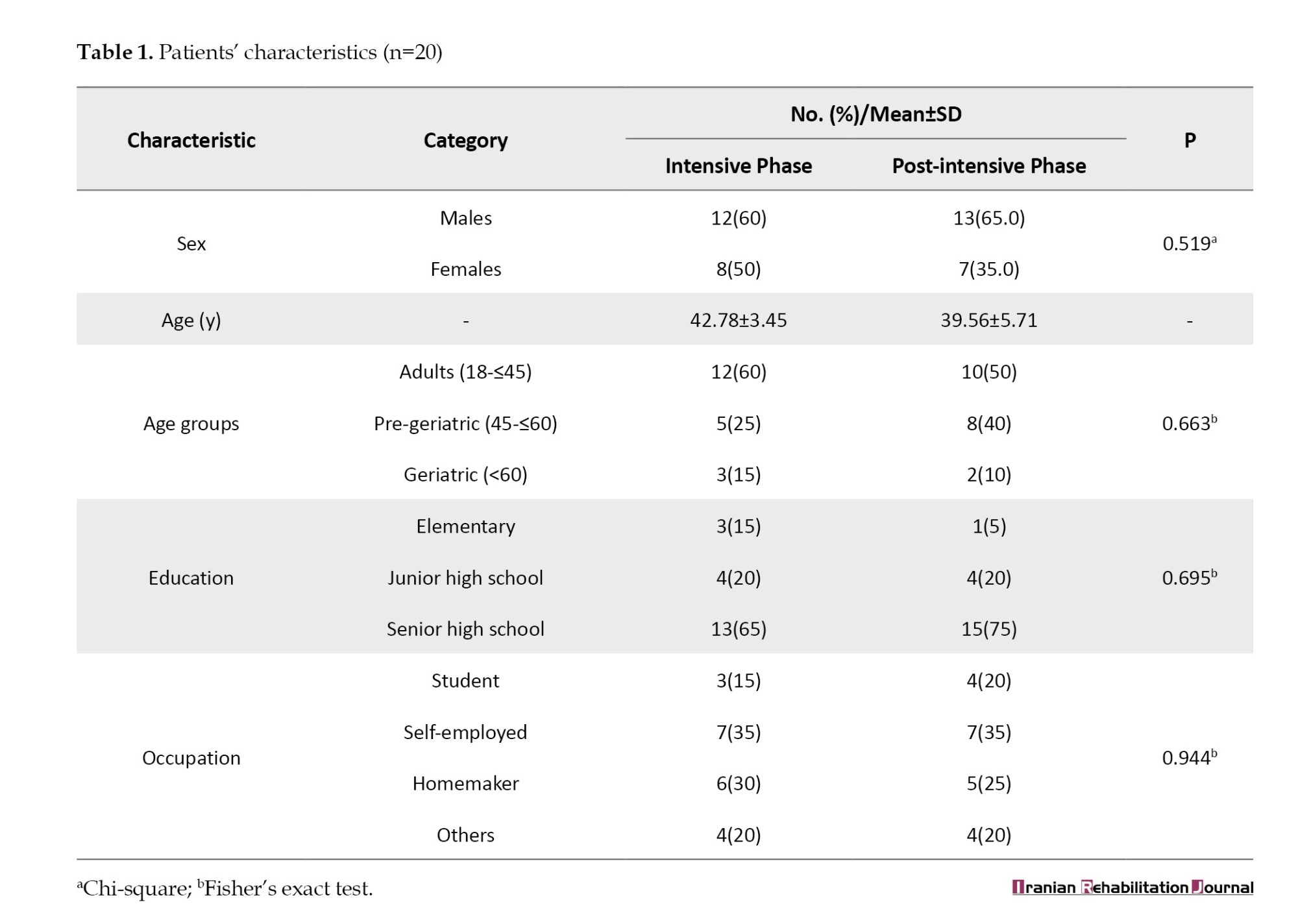
The statistical test used in this study was the chi-square test. Fisher’s test was used if the chi-square did not fulfill the cell on the characteristics of the research subjects [17, 18]. The variables of sex, age, education, and occupation had a value of P>0.05, indicating no difference in the proportion of each variable of the respondents’ sociodemographic characteristics between the group of respondents who underwent intensive care and the group of respondents who underwent continuation remedy.
Domain-based QoL levels in intensive and post-intensive phase groups
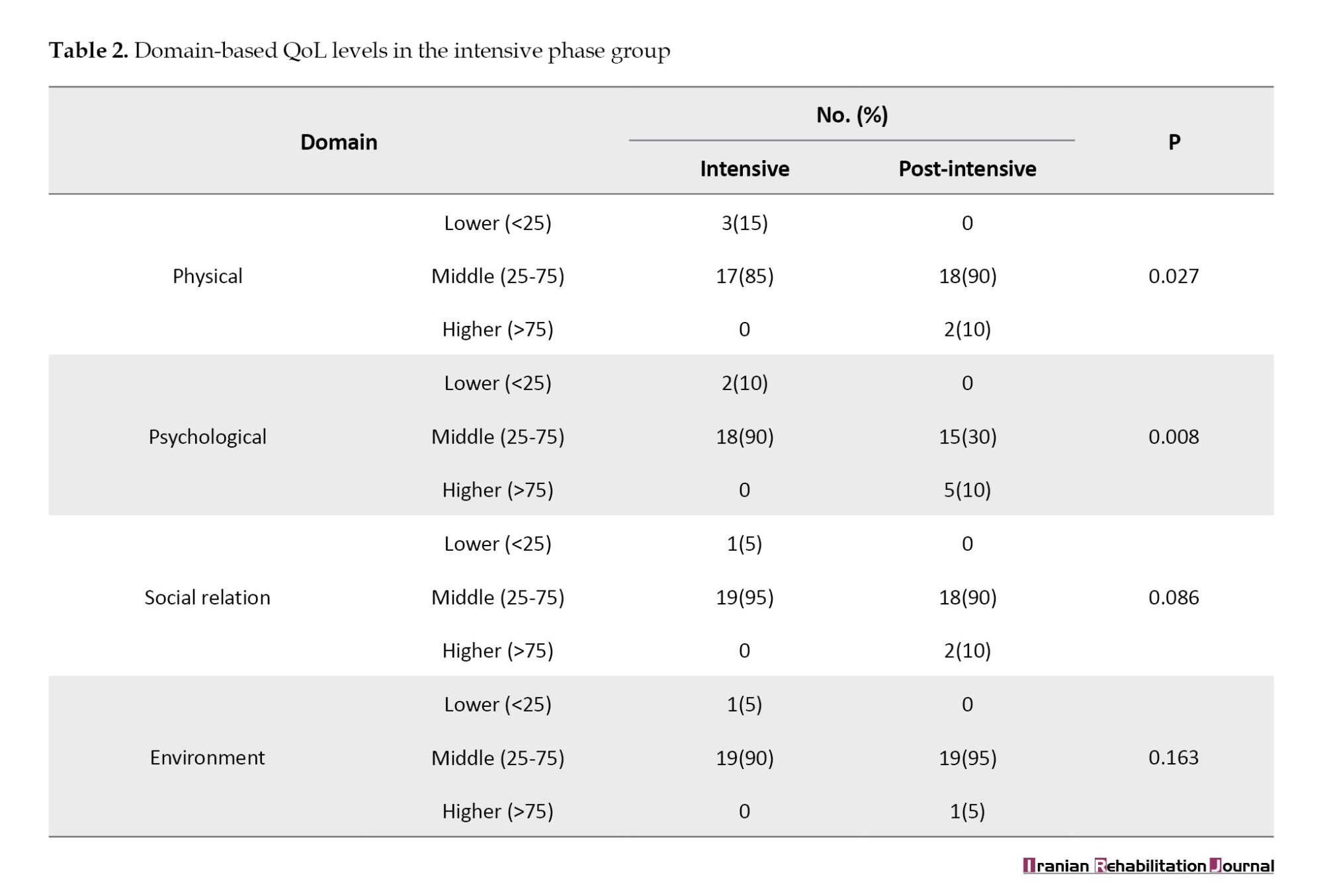
Based on research conducted on patients with pulmonary TB undergoing intensive initial treatment, as many as 20 respondents filled out the WHOQOL-BREF questionnaire; the results obtained are the patients’ QoL at the Pauh Health Center, Padang City, in each domain. Table 2 presents the QoL level for patients with pulmonary TB in the intensive and post-intensive rehabilitation phases.
In this study, the QoL for patients with TB in each domain of both groups showed a moderate category. Based on Table 2, the results of this study indicate that in the physical and psychological realms, the value is P<0.05. In the social relations and environmental domain, the value was P>0.05; in the environmental domains, the value was P>0.05. This study revealed no distinction in QoL concerning social and environmental aspects among patients with pulmonary TB undergoing intensive treatment compared to those in the continuation phase. However, significant transformations were observed in the physical and psychological health domains of patients with pulmonary TB undergoing intensive and continuation treatment.
Discussion
The results of this study are based on Indonesian health profile data, and the number of TB cases in male patients was 1.4 times greater than that in female patients [2]. This is in step with comprehensive research, which shows that more patients suffer from males than females [19]. Based on gender, pulmonary TB tends to be higher in males than females, because males are more susceptible to exposure than females [19]. The high incidence of pulmonary TB in men compared to women is because men have smoking habits [20]. Smokers have a higher risk of contracting pulmonary TB than non-smokers, with 28.1% of active smokers suffering from TB [20, 21].
The childbearing stage (35-44 years) has a greater risk of exposure to pulmonary TB because people tend to be more active and interact with many people; therefore, the possibility of exposure to TB is higher [22]. At a productive age, people will work to fulfill their life needs. However, the type of work does not substantially associate with pulmonary TB [22]. The work environment was significantly associated with the incidence of pulmonary TB (P=0.024). The work environment, which is at risk of pulmonary TB, affects the number of pulmonary TB incidents by 83.3% [20]. This is consistent with Papeo’s study, which stated that most cases of TB (65.3%) were in patients with self-employed jobs. The study also indicated no significant correlation between the nature of employment and the occurrence of TB [23].
Meanwhile, the lower a person’s education level, the lower the level of health awareness, which affects the deterioration of health status, where patients with a low level of education tend not to know the risk factors, symptoms, and prevention of TB [24]. However, those with a high education level do not always have good knowledge of preventing disease transmission. This depends on how a person gains knowledge about preventing disease transmission, either through counseling or getting information themselves using available media [22, 25, 26].
The results of pulmonary TB patients have a moderate QoL of as much as 56.7% [27]. This condition occurs because the patient is still in the active treatment range for six months, where the first two months undergo the intensive treatment, followed by the next four months undergoing the continuation phase. Pulmonary TB patients in the intensive stage are still in the period of treatment adjustment; therefore, it impacts their QoL physically and psychologically. In the post-intensive phase, the patient is still in the process of completing treatment [10, 27, 28].
This study’s results align with those of a study conducted in Taiwan, which found significant differences in the psychological domain of patients undergoing the initial and post-intensive phases of treatment [29]. Previous research has shown that the treatment phase is one factor that affects the TB patients’ QoL; when the patient is still in the adjustment stage, physically and psychologically, it impacts their QoL [29]. A study by Tornu et al. found a significant relationship between the treatment stage and the QoL of patients with TB [27].
The results of this research indicated that pulmonary TB patients with a low QoL were found in patients experiencing intensive periods of treatment: Physical domain (15%), psychological domain (10%), and the domain of social and environmental relations (5%). The Mann-Whitney test showed that the physical and psychological realms had P=0.027 and 0.008 (P<0.05), respectively. Thus, a crucial change was observed in the survival of patients with pulmonary TB undergoing intensive and continuation stages of treatment. QoL is low during intensive treatment because it is carried out for two months by taking TB drugs every day. Therefore, patients are sometimes saturated with the drugs they are taking and stop their treatment, and this can worsen the QoL of patients with pulmonary TB [27, 30, 31]. This difference suggests that the QoL of patients with pulmonary TB during the intensive phase is inferior to that during the continuation phase.
Pulmonary TB affects the patient’s physical condition. Patients with pulmonary TB often become very vulnerable due to prolonged chronic illness, nutritional deficiencies, and weight loss occur in patients with pulmonary TB. The patient’s eating habits were disturbed by the severe coughing and chest pain experienced [19, 28]. Noticeable variances in the physical and psychological well-being of patients undergoing the intensive and continuation phases of treatment are influenced mainly by the symptoms experienced by the patients. The more symptoms the patient experiences, the higher their stress level. Therefore, it worsens the QoL of patients with pulmonary TB [5].
Stress can reduce psychological well-being and cause physical symptoms. Therefore, stress is believed to deteriorate both physical and mental health, diminishing overall QoL [30, 31]. An insufficient grasp of knowledge can affect the stress level of TB patients can be affected by. Hence, the provision of socialization regarding TB, especially the mode of transmission, is urgently needed to improve the QoL of TB patients [31].
The fallouts disclosed no significant difference between the QoL of patients with pulmonary TB undergoing intensive and continuation phases of treatment, both in social relations and the environmental realm. This is related to the positive perception of patients with pulmonary TB towards social support provided by family, friends, health workers, and the community. It leads to feelings of security and comfort because patients with pulmonary TB feel that other individuals pay attention to and accept them. Positive perceptions of social support can also help patients with pulmonary TB feel more accepted and not isolated. Positive perceptions can help eliminate feelings of inferiority in patients with pulmonary TB [22].
Patients with pulmonary TB claim to be satisfied with their access to health services, housing, and transportation in the environmental domain. Health services that are easily accessible to patients make it easy for them to obtain them. Hence, the factor influencing the treatment of TB patients is the ease of access to health services [32, 33].
This study has the advantage that direct research was conducted on patients with pulmonary TB, so that personal and participant bias can be avoided. This study has some limitations, including the difficulty of obtaining data on the patients’ QoL. Other potential factors influencing the QoL of pulmonary TB patients were not considered, such as the level of knowledge related to pulmonary TB, family history, marital status, and other characteristics that can affect the QoL of patients with pulmonary TB during treatment.
Conclusion
Pulmonary TB patients in this study experienced a drop in their QoL during the intensive and post-intensive phases. Patients with TB experienced similar QoL levels during both the intensive and post-intensive stages of care. Pulmonary TB patients as a whole experience a decrease in their QoL because they experience various conditions that impact biological, physical, psychological, social, and spiritual aspects and levels of productivity. TB is a curable illness, but its management is intricate and requires substantial patient assurance. Therefore, further research is necessary to determine the elements that may influence the QoL of patients with pulmonary TB, such as the level of acquaintance related to pulmonary TB, family history, and other characteristics that can affect the QoL of patients throughout treatment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Universitas Andalas, Padang, Indonesia (Code: 703/UN.16.2/KEP-FK/2022).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design, conceptualizing, and writing the manuscript: Najmiatul Fitria; Conducting fieldwork: Wince Agustina; Checking conceptual variables: Yelly Oktavia Sari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Faculty of Pharmacy, Universitas Andalas, for the research recommendation. Furthermore, the authors thank the Padang City Health Office for allowing the authors to collect data at the Pauh Health Center.
References
In 2019, the World Health Organization (WHO) reveal ed 10 million tuberculosis (TB) cases worldwide and an estimated 1.2 million deaths from TB cases globally. Based on the latest WHO 2020 data, Indonesia ranks second after India, with the number of TB cases increasing from 331 703 in 2015 to 562 049 cases in 2019 [1]. The prevalence of the Indonesian population diagnosed with TB by health workers reached 0.42% of the entire Indonesian population, with the highest rate occurring at the age of 65-74 years, reaching 1%, and the lowest at the age of <1 year with a value of 0.1% [2], where TB cases in West Sumatra reached 0.31% [3].
The main symptom of patients with pulmonary TB is coughing up phlegm for 2-3 weeks or more. Cough is usually followed by additional symptoms, such as coughing up blood, phlegm mixed with blood, shortness of breath, decreased appetite, weakness, decreased body weight, sweating at night without activity, and fever for over a month. Because the prevalence of TB in Indonesia is quite high, everyone who comes to the health service unit (UPK) with these symptoms is considered a patient diagnosed with TB and must undergo a direct microscopic examination of the sputum [4].
After a person is diagnosed with pulmonary TB, several impacts will appear in their life, both physically, psychologically, socially, and economically [5]. The identification and treatment of TB incur costs. However, patients must still pay for transportation, accommodation, food, or nutrition costs during treatment and loss of income due to being unable to work [6]. TB contributes to the exacerbation of social stigma and even to being ostracized from society [7]. A previous study by Kristina et al. among 156 respondents revealed that the mean quality of life (QoL) scores among TB patients in referral hospitals in Yogyakarta were lower than the normal range (60.45±12.23) [8]. A decrease in QoL is related to their health status because it causes delays in treatment and negatively impacts the continuity of treatment, which causes treatment to be interrupted or incomplete [9-11].
WHO recommends directly observed treatment short-course (DOTS) treatment accompanied by direct observation. The DOTS strategy is implemented at government health facilities, with Puskesmas as a parameter for program implementation success. Patient recovery is a parameter of the success of TB control efforts. This cure, besides reducing the number of sufferers, can also prevent transmission [12]. Efforts to control TB are made using medication. The treatment used is a combination therapy of several types of TB drugs, with a minimum span of six months, consisting of the first two months of the intensive phase of treatment consisting of isoniazid (INH), rifampin (RIF), pyrazinamide, and ethambutol, followed by four months with a daily regimen of INH and RIF [13].
The TB patients’ QoL is crucial to assess because it affects all aspects of a person’s QoL, including physical, social, psychological, and environmental health. QoL assessment is useful for assessing the success of health services in terms of prevention and treatment. A person with a chronic disease (i.e. pulmonary TB) can have extended periods despite the challenges of their illness, underscoring the importance of health services focusing on improving their QoL [14].
Based on a preliminary study conducted at the Pauh Health Center in Padang City, Indonesia, 78 patients with TB were treated from January 2021 to December 2021. Based on the description above, the incidence of TB is a major challenge for the health world, affecting the QoL of patients with TB. The effectiveness of TB patient treatment greatly depends on the patient’s routine in treatment and carrying out treatment based on the treatment that has been programmed to improve the patient’s health. Therefore, a study was conducted to observe the differences in the development of QoL among those diagnosed with pulmonary TB who received two months of treatment, encompassing intensive and follow-up post-intensive care at one of the primary centers in Padang City.
Materials and Methods
Setting, population, and sample
The samples from this study were part of or representative of the population studied, which comprised patients diagnosed with TB receiving two months of treatment, encompassing intensive and post-follow-up care, from October 2021 to February 2022. The sampling method involved purposive selection, which was non-random. All samples meeting the presence conditions were included without exception.
Research design
This investigation is a forthcoming cross-sectional study using the World Health Organization's QoL questionnaire (WHOQOL-BREF) inquiry form [14]. This study determined the patients’ QoL levels, consisting of 26 questions in five domains. The level of QoL of patients was determined using the WHOQOL-BREF questionnaire, which consists of 26 questionnaire items belonging to four domains. Several questions were used to assess each of these four domains. The answers were assessed using a Likert-style scale, allowing respondents to gauge their satisfaction or intensity by assigning ratings on a scale typically falling between 1 (indicating a high level of dissatisfaction or poor quality) and 5 (indicating a high level of satisfaction or good quality). The questionnaire can be accessed via the web [15]. For non-commercial purposes, the Indonesian version of the WHOQOL-BREF questionnaire was approved via a permissions, and the permission ID is 202300339 [16].
Inclusion criteria
The inclusion criteria included patients 18 years old or above who were diagnosed with pulmonary TB and received category one anti-TB drugs at the Pauh Health Center, Padang City. The patient had received TB treatment for at least one month and communicated well. All patients with pulmonary TB were prepared to participate as respondents by completing an informed consent document. Both women and men were allowed to respond.
Statistical analysis
A chi-square was conducted to identify variances between the intensive and post-intensive phase groups for each sociodemographic variable [17]. Data normality in this study was assessed using the Shapiro-Wilk test (small sample size of 50). The normality test obtained a value of P>0.05; therefore, the relationship between the QoL of patients with intensive-post-intensive phase pulmonary TB was analyzed using the Mann-Whitney test. No missing, discarded, or outlier data were detected.
Results
Sociodemographic characteristics of pulmonary TB patients
An overview of the sociodemographic characteristics of the 40 patients interviewed (24 men and 16 women) (Table 1). In purposive sampling, the sample was saturated until the end of the study with 40 participants. Of the 40 respondents, the highest number of respondents was males (intensive [12], post-intensive [13]), followed by females (8 and 7, respectively) (Table 1). Based on the study results, most respondents were self-employed; the same proportion of self-employed jobs existed in both the intensive and post-intensive phases (35%).
The statistical test used in this study was the chi-square test. Fisher’s test was used if the chi-square did not fulfill the cell on the characteristics of the research subjects [17, 18]. The variables of sex, age, education, and occupation had a value of P>0.05, indicating no difference in the proportion of each variable of the respondents’ sociodemographic characteristics between the group of respondents who underwent intensive care and the group of respondents who underwent continuation remedy.
Domain-based QoL levels in intensive and post-intensive phase groups
Based on research conducted on patients with pulmonary TB undergoing intensive initial treatment, as many as 20 respondents filled out the WHOQOL-BREF questionnaire; the results obtained are the patients’ QoL at the Pauh Health Center, Padang City, in each domain. Table 2 presents the QoL level for patients with pulmonary TB in the intensive and post-intensive rehabilitation phases.
In this study, the QoL for patients with TB in each domain of both groups showed a moderate category. Based on Table 2, the results of this study indicate that in the physical and psychological realms, the value is P<0.05. In the social relations and environmental domain, the value was P>0.05; in the environmental domains, the value was P>0.05. This study revealed no distinction in QoL concerning social and environmental aspects among patients with pulmonary TB undergoing intensive treatment compared to those in the continuation phase. However, significant transformations were observed in the physical and psychological health domains of patients with pulmonary TB undergoing intensive and continuation treatment.
Discussion
The results of this study are based on Indonesian health profile data, and the number of TB cases in male patients was 1.4 times greater than that in female patients [2]. This is in step with comprehensive research, which shows that more patients suffer from males than females [19]. Based on gender, pulmonary TB tends to be higher in males than females, because males are more susceptible to exposure than females [19]. The high incidence of pulmonary TB in men compared to women is because men have smoking habits [20]. Smokers have a higher risk of contracting pulmonary TB than non-smokers, with 28.1% of active smokers suffering from TB [20, 21].
The childbearing stage (35-44 years) has a greater risk of exposure to pulmonary TB because people tend to be more active and interact with many people; therefore, the possibility of exposure to TB is higher [22]. At a productive age, people will work to fulfill their life needs. However, the type of work does not substantially associate with pulmonary TB [22]. The work environment was significantly associated with the incidence of pulmonary TB (P=0.024). The work environment, which is at risk of pulmonary TB, affects the number of pulmonary TB incidents by 83.3% [20]. This is consistent with Papeo’s study, which stated that most cases of TB (65.3%) were in patients with self-employed jobs. The study also indicated no significant correlation between the nature of employment and the occurrence of TB [23].
Meanwhile, the lower a person’s education level, the lower the level of health awareness, which affects the deterioration of health status, where patients with a low level of education tend not to know the risk factors, symptoms, and prevention of TB [24]. However, those with a high education level do not always have good knowledge of preventing disease transmission. This depends on how a person gains knowledge about preventing disease transmission, either through counseling or getting information themselves using available media [22, 25, 26].
The results of pulmonary TB patients have a moderate QoL of as much as 56.7% [27]. This condition occurs because the patient is still in the active treatment range for six months, where the first two months undergo the intensive treatment, followed by the next four months undergoing the continuation phase. Pulmonary TB patients in the intensive stage are still in the period of treatment adjustment; therefore, it impacts their QoL physically and psychologically. In the post-intensive phase, the patient is still in the process of completing treatment [10, 27, 28].
This study’s results align with those of a study conducted in Taiwan, which found significant differences in the psychological domain of patients undergoing the initial and post-intensive phases of treatment [29]. Previous research has shown that the treatment phase is one factor that affects the TB patients’ QoL; when the patient is still in the adjustment stage, physically and psychologically, it impacts their QoL [29]. A study by Tornu et al. found a significant relationship between the treatment stage and the QoL of patients with TB [27].
The results of this research indicated that pulmonary TB patients with a low QoL were found in patients experiencing intensive periods of treatment: Physical domain (15%), psychological domain (10%), and the domain of social and environmental relations (5%). The Mann-Whitney test showed that the physical and psychological realms had P=0.027 and 0.008 (P<0.05), respectively. Thus, a crucial change was observed in the survival of patients with pulmonary TB undergoing intensive and continuation stages of treatment. QoL is low during intensive treatment because it is carried out for two months by taking TB drugs every day. Therefore, patients are sometimes saturated with the drugs they are taking and stop their treatment, and this can worsen the QoL of patients with pulmonary TB [27, 30, 31]. This difference suggests that the QoL of patients with pulmonary TB during the intensive phase is inferior to that during the continuation phase.
Pulmonary TB affects the patient’s physical condition. Patients with pulmonary TB often become very vulnerable due to prolonged chronic illness, nutritional deficiencies, and weight loss occur in patients with pulmonary TB. The patient’s eating habits were disturbed by the severe coughing and chest pain experienced [19, 28]. Noticeable variances in the physical and psychological well-being of patients undergoing the intensive and continuation phases of treatment are influenced mainly by the symptoms experienced by the patients. The more symptoms the patient experiences, the higher their stress level. Therefore, it worsens the QoL of patients with pulmonary TB [5].
Stress can reduce psychological well-being and cause physical symptoms. Therefore, stress is believed to deteriorate both physical and mental health, diminishing overall QoL [30, 31]. An insufficient grasp of knowledge can affect the stress level of TB patients can be affected by. Hence, the provision of socialization regarding TB, especially the mode of transmission, is urgently needed to improve the QoL of TB patients [31].
The fallouts disclosed no significant difference between the QoL of patients with pulmonary TB undergoing intensive and continuation phases of treatment, both in social relations and the environmental realm. This is related to the positive perception of patients with pulmonary TB towards social support provided by family, friends, health workers, and the community. It leads to feelings of security and comfort because patients with pulmonary TB feel that other individuals pay attention to and accept them. Positive perceptions of social support can also help patients with pulmonary TB feel more accepted and not isolated. Positive perceptions can help eliminate feelings of inferiority in patients with pulmonary TB [22].
Patients with pulmonary TB claim to be satisfied with their access to health services, housing, and transportation in the environmental domain. Health services that are easily accessible to patients make it easy for them to obtain them. Hence, the factor influencing the treatment of TB patients is the ease of access to health services [32, 33].
This study has the advantage that direct research was conducted on patients with pulmonary TB, so that personal and participant bias can be avoided. This study has some limitations, including the difficulty of obtaining data on the patients’ QoL. Other potential factors influencing the QoL of pulmonary TB patients were not considered, such as the level of knowledge related to pulmonary TB, family history, marital status, and other characteristics that can affect the QoL of patients with pulmonary TB during treatment.
Conclusion
Pulmonary TB patients in this study experienced a drop in their QoL during the intensive and post-intensive phases. Patients with TB experienced similar QoL levels during both the intensive and post-intensive stages of care. Pulmonary TB patients as a whole experience a decrease in their QoL because they experience various conditions that impact biological, physical, psychological, social, and spiritual aspects and levels of productivity. TB is a curable illness, but its management is intricate and requires substantial patient assurance. Therefore, further research is necessary to determine the elements that may influence the QoL of patients with pulmonary TB, such as the level of acquaintance related to pulmonary TB, family history, and other characteristics that can affect the QoL of patients throughout treatment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Universitas Andalas, Padang, Indonesia (Code: 703/UN.16.2/KEP-FK/2022).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design, conceptualizing, and writing the manuscript: Najmiatul Fitria; Conducting fieldwork: Wince Agustina; Checking conceptual variables: Yelly Oktavia Sari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Faculty of Pharmacy, Universitas Andalas, for the research recommendation. Furthermore, the authors thank the Padang City Health Office for allowing the authors to collect data at the Pauh Health Center.
References
- World Health Organization (WHO). Global Tuberculosis Report. Geneva: World Health Organization; 2020. [Link]
- National Institute of Health Research and Development. Laporan Nasional Riskesdas 2018. Jakarta: Kemenkes RI; 2019.
- National Institute of Health Research and Development. Laporan Provinsi Sumatera Barat Riskesdas 2018. Jakarta: Kemenkes RI; 2019.
- Rutherford ME, Ruslami R, Anselmo M, Alisjahbana B, Yulianti N, Sampurno H, et al. Management of children exposed to Mycobacterium tuberculosis: a public health evaluation in West Java, Indonesia. Bulletin of The World Health Organization. 2013; 91(12):932-41A. [DOI:10.2471/BLT.13.118414] [PMID]
- Johns B, Probandari A, Mahendradhata Y, Ahmad RA. An analysis of the costs and treatment success of collaborative arrangements among public and private providers for tuberculosis control in Indonesia. Health Policy. 2009; 93(2-3):214-24. [DOI:10.1016/j.healthpol.2009.08.004] [PMID]
- Fuady A, Houweling TAJ, Mansyur M, Richardus JH. Catastrophic total costs in tuberculosis-affected households and their determinants since indonesia’s implementation of universal health coverage. Infectious Diseases of Poverty. 2018; 7(1):3. [DOI:10.1186/s40249-017-0382-3] [PMID]
- Qiyaam N, Furqani N, Hartanti DJ. [Evaluasi Penggunaan Obat Antituberkulosis (OAT) Pada Pasien Tuberkulosis Paru di Puskesmas Kediri Lombok Barat Tahun 2018 (Indonesian)]. Lumbung Farmasi: Jurnal Ilmu Kefarmasian. 2020; 1(1):1-7. [DOI:10.31764/lf.v1i1.1197]
- Kristina SA, Mada UG, Lienaningrum AS, Mada UG. Quality of life among tuberculosis patients in Indonesia : A cross sectional survey. 2020. [Link]
- Idrus L, Fitria N, Hasan N, Postma M, Alffenaar JW. PIN53 The Usability Testing of the Integrated E-Healthcare Services (IEHS) Web-Based Application in the Therapy Management of HIV and Tuberculosis in Indonesia. Value In Health Regional Issues. 2020; 22(S57). [DOI:10.1016/j.vhri.2020.07.300]
- Juwita DA, Qalbi YA, Fitria N. The relationship between the time of use of Antiretroviral Therapy (Art) and the amount of viral load in acquired immunodeficiency syndrome. International Journal of Applied Pharmaceutics. 2023; 15(Special Issue 1):24-8. [DOI:10.22159/ijap.2023.v15s1.47502]
- Fitria N, Wulansari S, Sari YO. Potential interactions analysis of antihypertensive drugs used in geriatric. International Journal of Applied Pharmaceutics. 2023; 15(Special Issue 1):29-33. [DOI:10.22159/ijap.2023.v15s1.47503]
- Ministry of Health. [Health Profile 2020 Padang City (Indonesian)]. Padang: Padang City Health Office; 2021.
- Gafar F, Arifin H, Jurnalis YD, Yani FF, Fitria N, Alffenaar JWC, et al. Antituberculosis drug-induced liver injury in children: Incidence and risk factors during the two-month intensive phase of therapy. The Pediatric Infectious Disease Journal. 2019; 38(1):50-53. [DOI:10.1097/INF.0000000000002192] [PMID]
- Muniyandi M, Rajeswari R, Balasubramanian R, Nirupa C, Gopi PG, Jaggarajamma K, et al. Evaluation of post-treatment Health-Related Quality of Life (HRQoL) among tuberculosis patients. International Journal of Tuberculosis and Lung Disease. 2007; 11(8):887-92. [PMID]
- World Health Organization (WHO). WHO publication.WHOQOL: Measuring Quality of Life. Geneva: WHO; 2022.
- World Health Organization (WHO). Permission request [Internet]. Geneva: WHO; 2022.
- Fitria N, Idrus L, Putri AR, Sari YO. The usability testing of the integrated electronic healthcare services for diabetes mellitus patients during the pandemic in Indonesia. Digital Health. 2023; 9:20552076231173227.[DOI:10.1177/20552076231173227] [PMID]
- Fitria N, Sari YO, Ananta FT, Husnia K. Adherence Assessment on Hypertension Therapy Using The Pill Count Method in Lubuk Kilangan Health Center, Indonesia. Jurnal Sains Farmasi & Klinis. 2023; 10(1):28-34. [DOI:10.25077/jsfk.10.1.28-34.2023]
- Lange C, Chesov D, Heyckendorf J, Leung CC, Udwadia Z, Dheda K. Drug-resistant tuberculosis: An update on disease burden, diagnosis and treatment. Respirology. 2018; 23(7):656-73. [DOI:10.1111/resp.13304] [PMID]
- Silva DR, Muñoz-Torrico M, Duarte R, Galvão T, Bonini EH, Arbex FF, et al. Risk factors for tuberculosis: Diabetes, smoking, alcohol use, and the use of other drugs. Jornal Brasileiro de Pneumologia: Publicacao Oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2018; 44(2):145-52. [DOI:10.1590/s1806-37562017000000443] [PMID]
- Sheikh S, Poursadeghian M, Rohaninasab M, Vatani J, Akhlaghi Pirposhteh E, Ahmadi-Mazhin S, et al. The incidence of lung cancer and smoking in Iran, Turkey, England, and the USA: A comparative study. Iranian Rehabilitation Journal. 2023; 21(2):231-8. [DOI:10.32598/irj.21.2.763.4]
- Kaaffah S, Kusuma IY, Renaldi FS, Lestari YE, Pratiwi ADE, Bahar MA. Knowledge, attitudes, and perceptions of tuberculosis in Indonesia: A multi-center cross-sectional study. Infection and Drug Resistance. 2023; 16:1787-800. [DOI:10.2147/IDR.S404171] [PMID]
- Papeo DRP, Immaculata M, Rukmawati I. [Hubungan Antara Kepatuhan Minum Obat (MMAS-8) Dan Kualitas Hidup (WHOQOL-BREF) Penderita Tuberkulosis Di Puskesmas Di Kota Bandung (Indonesian)]. Indonesian Journal of Pharmaceutical Education. 2021; 1(2):86-97. [DOI:10.37311/ijpe.v1i2.11143]
- Joesoef MR, Remington PL, Jiptoherijanto PT. Epidemiological model and cost-effectiveness analysis of tuberculosis treatment programmes in Indonesia. International Journal of Epidemiology. 1989; 18(1):174-9. [DOI:10.1093/ije/18.1.174] [PMID]
- Kausar MN, Fitriana E, Khairunnisa K, Faruque MO, Bahar MA, Alfian SD, et al. Development and Validation of the Knowledge, Attitude, and Practice Questionnaire for community pharmacy personnel in tuberculosis case detection, drug monitoring, and education: A study from Indonesia. Infection and Drug Resistance. 2023; 16:3729-41. [DOI:10.2147/IDR.S409107] [PMID]
- Fitria N, Sari YO, Putry AR, Putrizeti F, Sukma A. Future challenge on probiotics uses from fermented milk on the endocrine disorder in human. In: IOP Conference Series: Earth and Environmental Science. IOP Publishing Ltd; 2021. [DOI:10.1088/1755-1315/888/1/012047]
- Tornu E, Quarcoopome L. Correlates of quality of life among persons living with tuberculosis: A cross-sectional study. Plos One. 2022; 17(11):e0277192. [DOI:10.1371/journal.pone.0277192] [PMID]
- de Soldenhoff R. Community based programmes can help to manage tuberculosis more effectively. BMJ. 1998; 316(7134):864-5. [DOI:10.1136/bmj.316.7134.864b] [PMID]
- Chung WS, Lan YL, Yang MC. Psychometric testing of the short version of the world health organization quality of life (WHOQOL-BREF) questionnaire among pulmonary tuberculosis patients in Taiwan. BMC Public Health. 2012; 12:630. [DOI:10.1186/1471-2458-12-630] [PMID]
- Kittikraisak W, Kingkaew P, Teerawattananon Y, Yothasamut J, Natesuwan S, Manosuthi W, et al. Health related quality of life among patients with tuberculosis and HIV in Thailand. Plos One. 2012; 7(1):e29775. [DOI:10.1371/journal.pone.0029775] [PMID]
- Dhuria M, Sharma N, Narender Pal Singh, Ram Chander Jiloha, Saha R, et al. A study of the impact of tuberculosis on the quality of life and the effect after treatment with DOTS. Asia-Pacific Journal of Public Health. 2009; 21(3):312-20. [DOI:10.1177/1010539509336242] [PMID]
- Nhavoto JA, Grönlund Å, Chaquilla WP. SMSaúde: Design, development, and implementation of a remote/mobile patient management system to improve retention in care for HIV/AIDS and Tuberculosis Patients. JMIR mHealth and uHealth. 2015; 3(1):e26. [DOI:10.2196/mhealth.3854] [PMID]
- Adams S, Mulubwa M, van Huyssteen M, Bheekie A. Access to chronic medicines: Patients’ preferences for a last kilometre medicine delivery service in Cape Town, South Africa. BMC Family Practice. 2021; 22(1):43. [DOI:10.1186/s12875-021-01392-1] [PMID]
Article type: Original Research Articles |
Subject:
epidemiological studies
Received: 2023/08/27 | Accepted: 2024/02/17 | Published: 2025/06/1
Received: 2023/08/27 | Accepted: 2024/02/17 | Published: 2025/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
