
988368
Wed, Jul 29, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 595-604 |
Back to browse issues page


Ethics code: IR.USWR.REC.1400.049
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Azimian M, Farazi M, Nilipour R, Sayad Nasiri M, Amrevani M, Hosseinzadeh S et al . Investigating the Effectiveness of Neuropsychological Rehabilitation on Stroke Patients. Iranian Rehabilitation Journal 2024; 22 (4) :595-604
URL: http://irj.uswr.ac.ir/article-1-2061-en.html
URL: http://irj.uswr.ac.ir/article-1-2061-en.html
Mojtaba Azimian1 

 , Morteza Farazi *2 , Reza Nilipour2 , Mohammad Sayad Nasiri3 , Marzieh Amrevani4 , Samaneh Hosseinzadeh5 , Zahra Valitabar Kerati2
, Morteza Farazi *2 , Reza Nilipour2 , Mohammad Sayad Nasiri3 , Marzieh Amrevani4 , Samaneh Hosseinzadeh5 , Zahra Valitabar Kerati2
, Morteza Farazi *2 , Reza Nilipour2 , Mohammad Sayad Nasiri3 , Marzieh Amrevani4 , Samaneh Hosseinzadeh5 , Zahra Valitabar Kerati2
1- Department of Clinical Since, School of Rehabilitation, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychiatry, School of Rehabilitation, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Department of Biostatistics and Epidemiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychiatry, School of Rehabilitation, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Department of Biostatistics and Epidemiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 478 kb]
(1031 Downloads)
| Abstract (HTML) (6274 Views)
Full-Text: (908 Views)
Introduction
In a stroke, an artery supplying blood to the brain is blocked by a blood clot (ischemic stroke), or a blood vessel in the brain bursts and cuts off blood flow to a portion of the brain (hemorrhagic stroke). Aphasia most frequently results from strokes, which sometimes is associated with dysarthria and dyspraxia. Every year, over 15 million people worldwide suffer from some degree of stroke and experience various complications, such as sensory-motor, cognitive, and language disabilities [1]. According to several studies, 23%-36% of stroke survivors experience various degrees of language-cognitive damage (aphasia) [2]. Aphasia is an acquired defect in language usage (expressive and perceptive language), which results from damage to specific language areas in the brain. Language impairment in aphasia depends on the type of damage, the location of the damage in the brain, and the severity of the problem, leading to different degrees of language comprehension and expression [3]. It also causes problems in naming, discussing, understanding concepts, repeating numbers and sentences, verbal fluency, verbal explanations, issues in defining words, and ambiguity in interpreting words and metaphors, especially metalinguistic disorders. Usually, communicating requires the ability to speak and use the appropriate language. Naturally, such injuries will destroy various aspects of a person’s life, such as communication, participation in daily activities, individual independence, economic status, and quality of life (QoL) [4, 5]. Therefore, these individuals are damaged to varying degrees in daily communication, meeting personal needs, and participating in society, depending on the effects of symbolic communication (including speaking, listening, reading, and writing) in aphasia patients [6, 7]. Word-finding defects are considered the main symptom of aphasia [8, 9].
Therefore, the most common language deficits in stroke patients are anomia or disorder in word retrieval, where word retrieval defects may be observed to express all concepts, including noun, verb, adjective, and adverb, and aphasia patients may have more difficulty in retrieving some grammatical concepts than other groups [10-12]. Studies have reported different morphological, phonological, gestural, and semantic methods for treating word retrieval impairments in aphasia caused by brain damage. The results of these treatments are not the same, but the improvement achieved in most treatments is specific to trained cases [13-15]. However, the provision of rehabilitation services based on the individual needs of stroke patients requires extensive screening and evaluation of the severity and type of language injuries.
Many standard tests have been developed in Western countries to evaluate different aspects of language, such as syntax, semantics, word search, listening comprehension, and reading. Some of these tests include the Western aphasia battery and Boston diagnostic aphasia examination [16]. In Iran, Dr. Nilipour et al. developed the clinical version of the Persian diagnostic aphasia battery bedside version (P-DAB-AQ1, 2016) to screen and assess the severity of acquired language disorders in Persian-speaking adults with brain injuries [17].
In neuropsychological rehabilitation, the neuropsychological principles that are effective in the severity of a stroke and aphasia include the severity of the disorder, type of stroke, extent of the lesion, location of the stroke, and whether it is unilateral or bilateral. A CT scan should determine whether a stroke is present, and other individual factors like age, sex, hand side, whether the patient is monolingual or bilingual, and length of hospital stay should also be considered. This study investigated all the cases of stroke patients receiving advanced rehabilitation in the speech therapy and neurology departments. The results of the clinical-linguistic evaluations of the patients were compared by a neurologist and a speech and language pathologist (SLP) in two stages: 1) Initial admission in the mentioned departments and 2) After discharge from the hospital. Notably, the comparative evaluation was based on an internationally standardized valid aphasia test for the Persian language (P-DAB-AQ1, 2016) and medical and paraclinical examination. This assessment comprises the severity of aphasia disorder, each patient’s recovery rate based on the treatment methods used, and the effect of various individual factors [17].
The World Health Organization (WHO) predicts that the number of strokes in the European :union:, Iceland, Norway, and Switzerland will rise from 1.1 million in 2000 to 1.5 million by 2025. Also, according to a systematic review conducted in South America, the crude score of stroke prevalence varies from 1.74 to 6.51 per 1000 people, and its annual incidence rate is 0.35 to 1.83 per 1000 people [2]. Numerous studies on aphasia treatment have been conducted and are ongoing. Falconer et al. subjected four aphasic patients to the treatment of semantic feature analysis (SFA) with continuous speech tasks. It was hypothesized that retrieving words during discourse would be more efficient and significantly impact communication. The results show that using SFA in group therapy can improve an individual’s communication performance [18]. Wambaugh et al. studied the effect of SFA treatment on verb naming performance in four English-speaking aphasic patients. Verbs were categorized into four groups of ten without semantic connection. After 12 therapy sessions, an increase in the accuracy of naming educational verbs was observed in 3/4 of the participants, no improvement in control verbs, and an increase in speech content was observed for one participant [19]. Kristensson et al. performed the intensive SFA treatment to increase speech and communication function content in three people with chronic aphasia. This treatment completed the naming task for 21 nouns and 21 verbs. The results showed that two participants had an increase in speech performance and an increase in self-correction. However, they did not show significant improvement in naming [20].
Mehri et al. investigated and compared the effect of semantic and phonetic guidance on facilitating the naming process in patients with aphasia and Alzheimer disease, considering the common impairments of comprehension and naming, as well as temporal and temporal lobe defects. The study was conducted cross-sectionally on seven patients with fluent aphasia and seven patients with Alzheimer disease. The study results showed that both types of patients benefited from semantic and phonetic guidance. Still, fluent aphasia patients benefited more from phonetic guidance. Alzheimer patients benefited more from semantic guidance, which shows that the damage of semantic representation in Alzheimer patients is more than in other patient groups [21]. Sadeghi et al. investigated and compared the effect of SFA and promoting aphasia communication efficacy (PACE) methods on the ability to name aphasia patients. A 2-week study was conducted on four patients with dyspraxia; after the intervention, the ability to name therapeutic words increased significantly in both methods, except for one participant with damage to the left basal ganglia, in whom the SFA method was ineffective. The observed changes in the PACE method were greater than those in SFA, and the ability to name control words, generate semantic coordinates, and transfer the message improved. One week after the interventions, the performance of the patients in naming therapeutic words was still above the baseline despite a slight decrease [22]. Parhoon et al. conducted a study on the effectiveness of cognitive rehabilitation on the executive functions of stroke patients. The cognitive rehabilitation program has re-learned mental actions, and based on brain flexibility, it has improved the patients’ functional memory and selective attention [23].
In investigating the effectiveness of computer-based cognitive rehabilitation on enhancing the working memory of stroke patients in Tabriz, Ghorbanian et al. asserted that cognitive problems are one of the most prevalent issues among stroke patients. Also, the findings showed that computer-based cognitive rehabilitation improves working memory in stroke patients [24].
Considering the lack of research in this area, conducting related but underappreciated research seems essential. On this basis, the current study examined the efficacy of neurological rehabilitation for stroke patients with language and cognitive disorders. We emphasized the prevention and control of confounding factors, such as blood pressure and reducing mental stress in the cause of stroke, referring patients to neurologists after brain injuries, accurate diagnosis of the disorder, and prompt referral to speech therapy. Also, providing treatment-rehabilitation services, particularly during the first 6 months of a patient’s illness, and fostering family participation is essential. This study aimed to investigate the effectiveness of neurological rehabilitation on the cognitive status of stroke patients.
Materials and Methods
This research is a quasi-experimental study before and after the intervention. The study was conducted on 22 adult Persian-speaking stroke patients with an average age of 64.31 years. They were selected from 41 patients who visited Rofiedeh Rehabilitation Hospital between March 2020 and October 2021. These patients with various cognitive disorders, fluency, and non-fluent aphasia were chosen based on the inclusion criteria: Speaking Farsi language, lacking history of previous stroke, being adult patients with left hemisphere stroke, having fluent and non-fluent aphasia caused by stroke, starting treatment 2 to 8 months after the complication, being stroke patients with cognitive disorders based on the MMSE test with a score below 23, taking up to 75% correct answers in clinical questionnaire of Persian picture naming battery test, being conscious during evaluation and therapeutic interventions, having minimum reading and writing literacy, and having normal hearing and vision. The data collection tools and methods included an acceptance questionnaire, personal information of an adult stroke patient with aphasia, and the Iranian version of the Farsi aphasia diagnostic test (P-DAB-1 record form, AQ1). The method of execution and scoring of the P-DAB is based on the scores obtained from the execution of different versions of the test: Four different quantitative indicators can be calculated to determine the severity and type of linguistic-cognitive disorders. These quantitative indicators are as follows:
• Clinical prescription severity index for aphasia quotient screening (AQ1),
• Aphasia quotient (AQ2) severity index of oral language disorders,
• Aphasia quotient (AQ3) severity index of oral language disorder, and
• Aphasia cortical quotient (CQ1) severity index of oral and written language and cognitive disorders [17].
The components of this tool (P-DAB-1 record form, AQ1) include continuous speech content quality (4 items), fluency of speech (6 items), listening comprehension (10 items), comprehension of continuous commands (4 items), ability to repeat words (6 items), and naming ability (20 items). Dr Nilipour et al. checked and confirmed the validity and reliability of this tool in Iran [17].
The Persian picture naming battery clinical questionnaire contains 50 clear and distinct nominal images designed on a separate page. By presenting a picture, the therapist asks the patient to say the name of that picture. The answer sheet contains four options: No guidance, semantic guidance, phonetic guidance, and type of error. The severity of the disorder is mild, moderate, and severe. Up to 75% of correct answers are mild disorder severity, 50% to 75% are moderate, and less than 50% represent severe disorder severity.
The mini-mental state examination (MMSE) contains questions with 30 points that determine cognitive problems, especially memory in adults. In scoring, 0 is given for wrong answers and 1 for correct answers. Therefore, scores of 24 to 30 indicate a normal condition, and below 23 indicate a disorder and the need for psychiatric consultation. In internal studies by Kazazi et al., the degree of confidence and ability to do it are 95% and 80%, respectively [25].
The diagnostic tools for stroke patients include CT scans, MRI, and fMRI. In this study, the cause of the disease was determined solely by MRI findings. Also, after the patient’s visit and the neurologist’s diagnosis of a stroke, according to MRI findings and based on the referral form, aphasia patients were referred to a SLP to determine the cause of the complication. The treatment methods used in this study include treatment programs based on the damage mapping hypothesis, verb network strengthening therapy, treatment of underlying constructions, treatment of underlying forms, melodic intonation therapy, SFA, and treatment around cognitive components such as perception, attention, memory, language, and thinking. Neurological rehabilitation is a medically controlled process to heal a damaged part of the nervous system. Neurological rehabilitation often reduces disease symptoms, strengthens or stabilizes new behavioral patterns, and rehabilitates and empowers the damaged functions of the patient’s nervous system.
Each patient began treatment between 2 and 8 weeks after sustaining a brain injury. An SLP provided rehabilitation services four times weekly (one 30-minute daily session) for one year and seven months. Due to the nature of aphasia, this treatment period did not affect the spontaneous recovery of the disorder. The treatment of patients varied according to severity, disorder type, and individual requirements. After the treatment, the patients’ AQ1 and MMSE questionnaires were reviewed and completed. Finally, the collected data were analyzed. Data analysis was done using the SPSS software version 19. The characteristics of the study participants were summarized using the Mean±SD or number and percentage. The Shapiro-Wilk test was used to check the normal distribution of research variance. The Mann-Whitney and the Kruskal-Wallis non-parametric tests were applied to compare the means of the research variables in background variables with two groups, respectively. Wilcoxon’s non-parametric test was used to compare research variance before and after the intervention.
Results
According to the results, 54.5% of the participants are male, 45.5% female, 72.7% employed, 72.7% married, 31.8% educated, and 77.3% had an average economic status. Table 1 shows that 10 patients (equivalent to 45.45%) had fluent aphasia and 12 of them (equivalent to 54.55%) had non-fluent aphasia.
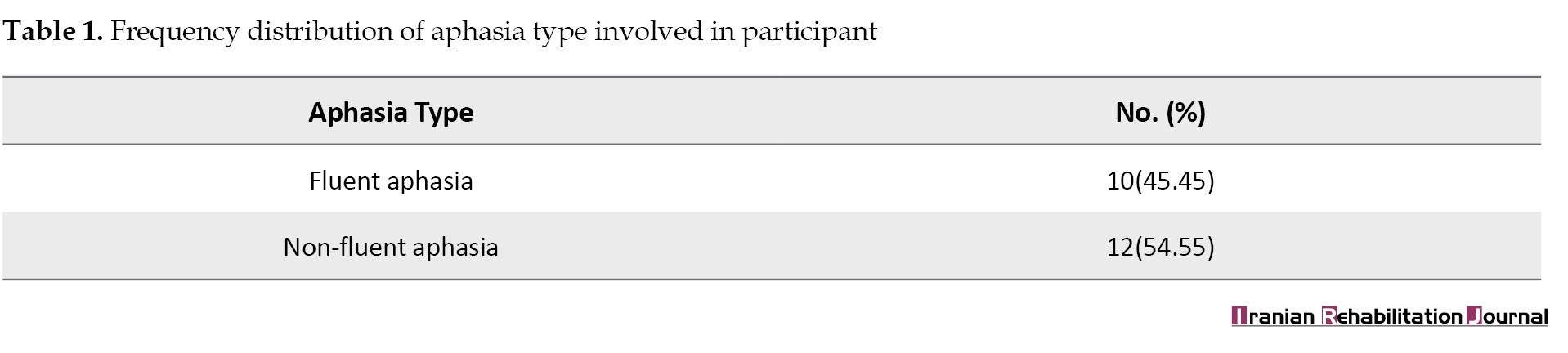
Table 2 shows that the average AQ1 score of the participants has increased from 74.80 to 80.12, and the average MMSE score has increased from 17 to 22.59.
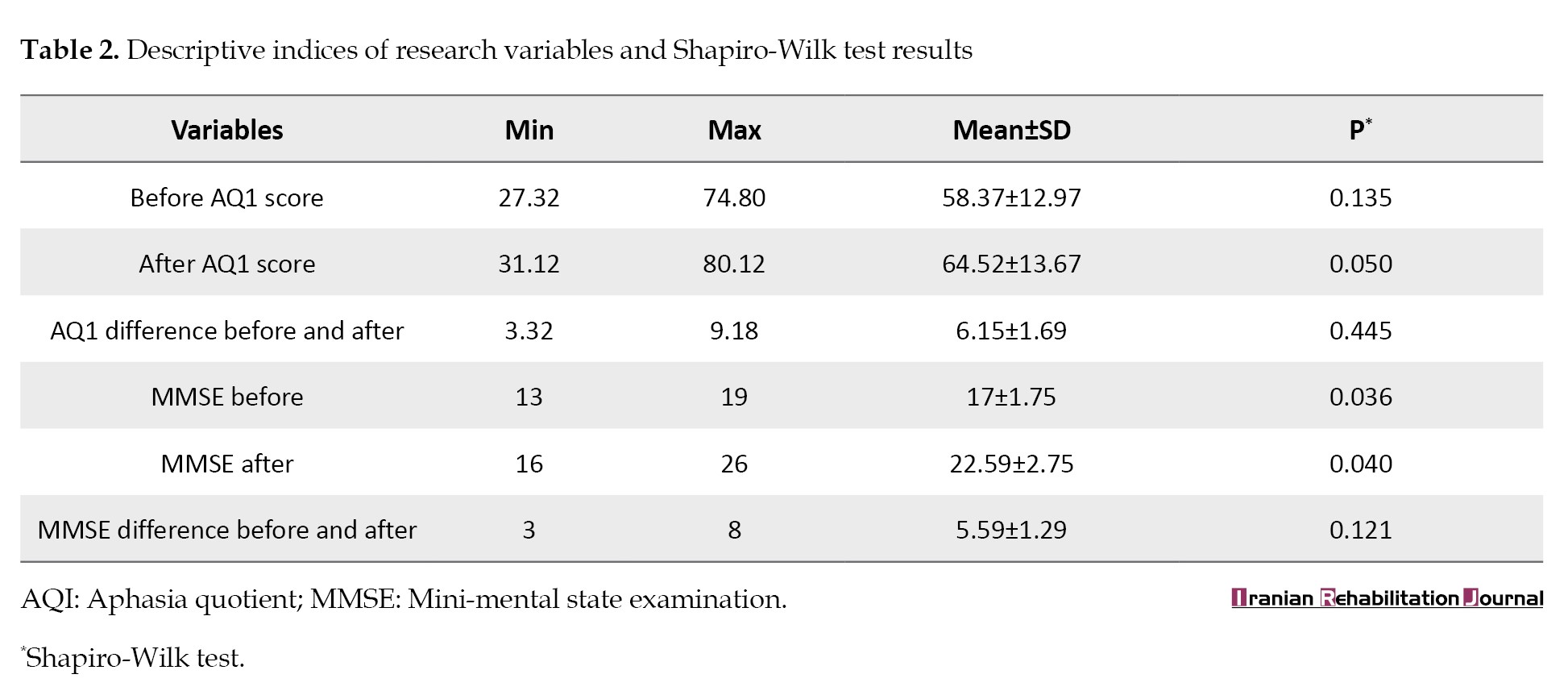
The main variables do not follow a normal distribution (P<0.05), but the difference between scores before and after the intervention follows a normal distribution (P<0.05).
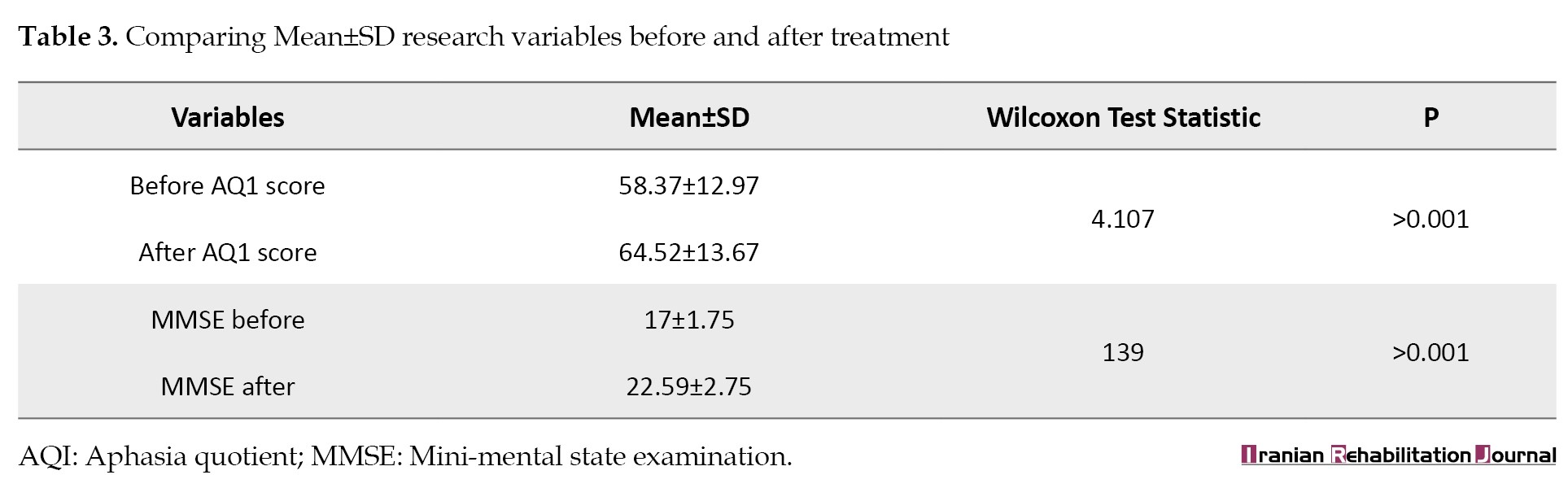
According to Table 3, the results of the Wilcoxon test, the mean score of AQ1, and MMSE before and after treatment had a significant difference.
According to the Mann-Whitney test in Table 4, the average score of AQ1 before and after treatment is not significantly different in the two types of aphasia.
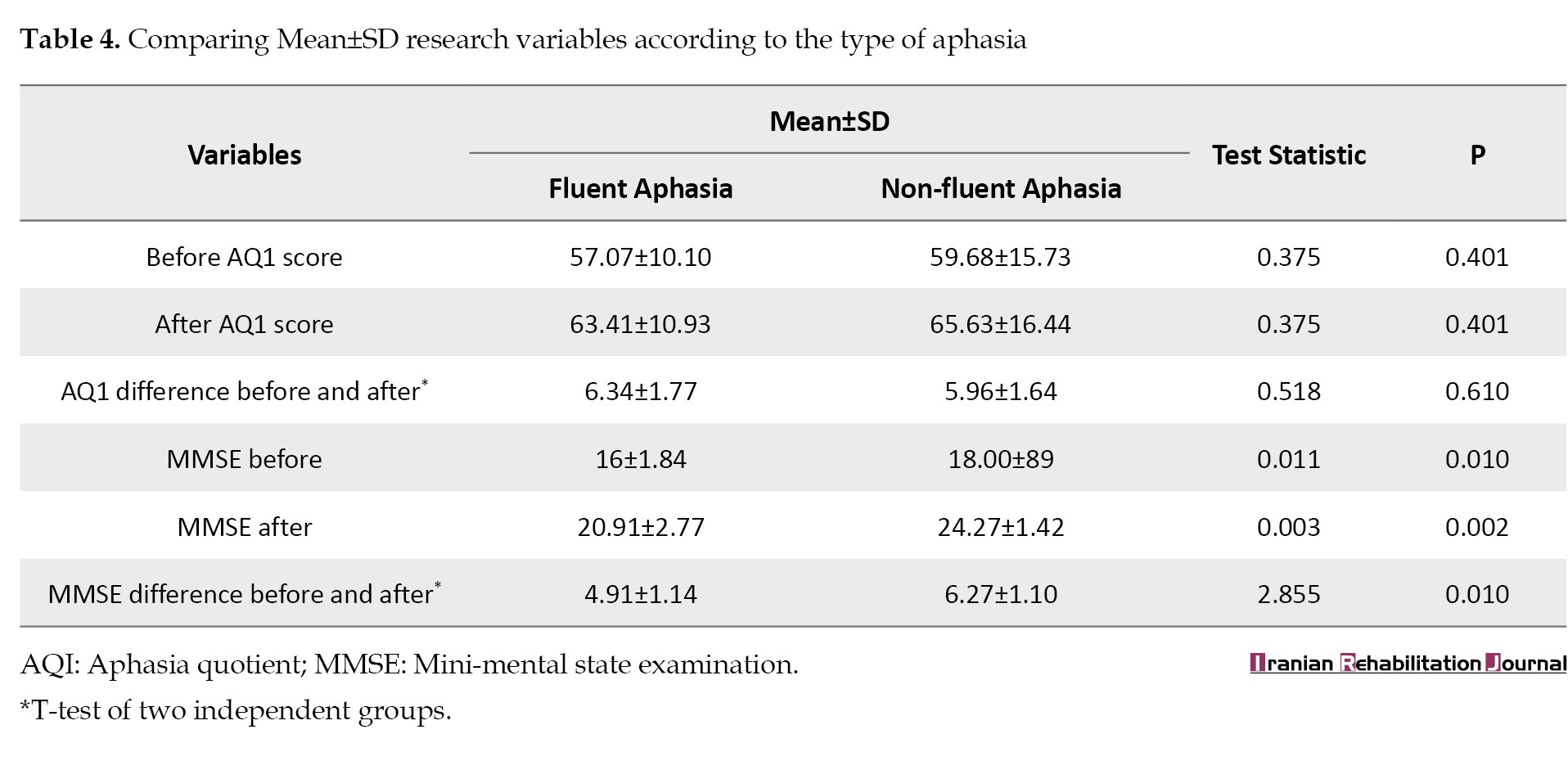
Still, MMSE recognition before and after treatment significantly differs in the two types of aphasia. The t test of two independent groups shows no significant difference in the AQ1 score in the fluent and non-fluent aphasia groups. Still, there is a significant difference in the MMSE score in the fluent and non-fluent aphasia groups. The MMSE increase was higher in the non-fluent aphasia group.
According to the Spearman correlation coefficient in Table 5, there is no significant association between research variables with age and the number of children.
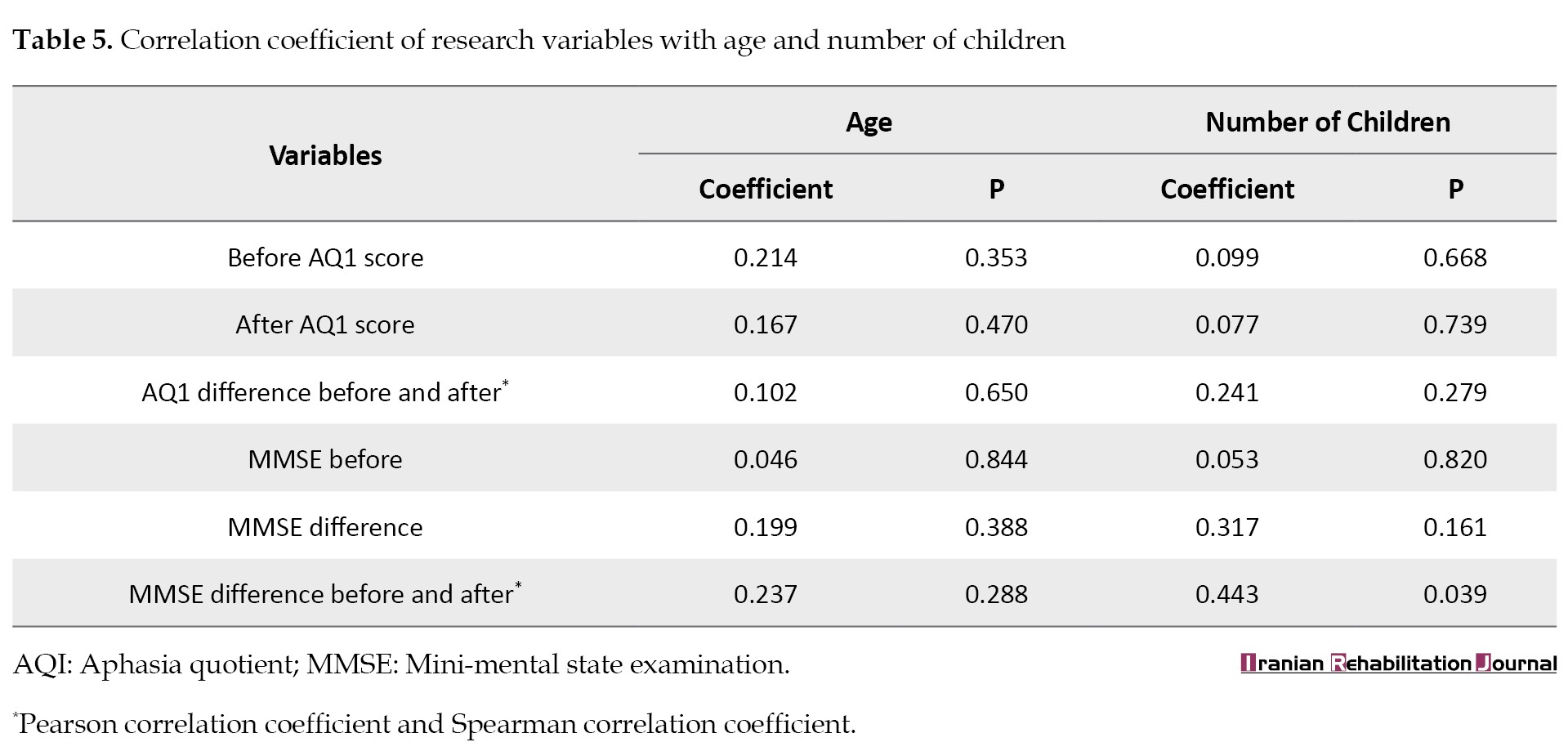
According to the Pearson correlation coefficient, the difference between the AQ1 score before and after treatment has no significant relationship with age and number of children. Still, a significant relationship exists between MMSE score before and after treatment and the number of children.
Discussion
As mentioned previously, the communication and pathological problems of these patients become more and more severe in the advanced stages of stroke, so the reduction of social participation due to existing communication problems endangers the emotional and mental health of the patient. The pathology and language deficit in aphasia, depending on the type of damage, the location of the damage in the brain, and the severity of the problem, leads to different degrees of language comprehension and expression problems. Since the current study aimed to examine the efficacy of neurological rehabilitation in stroke patients, the findings are compared to those of similar research. In this study, it was found that the average research variables of the type of individual factors, such as gender, occupation, marital status, place of residence, income level, education level, cause and location of the complication, and the number of children before and after treatment did not differ significantly among the participants. Also, based on the MMSE test, the education level affects patients’ cognitive performance before and after treatment. This finding means that patients with a higher level of education had better performance in cognitive dimensions such as understanding, sustained attention, general memory, working memory, language, and thinking, which is in line with the study by Rahmani et al. [26]. According to this study, all participants showed functional improvement in continuous speech development and vocabulary retrieval. Thus, continuous speech and vocabulary retrieval are more efficient and possess a more meaningful communication aspect. This finding indicates that all participants showed improved performance in continuous speech tasks using SFA, and the results were consistent with Wambaugh and Falconer [15, 20]. The results of this study indicate that the average AQ1 score before and after treatment in two types of fluent and non-fluent aphasia is not significantly different. Based on the MMSE test before and after treatment, there is a significant difference in the treatment of two types of aphasia, and this variable is significantly less in the fluent aphasia group. It has been determined that word naming, language processing, word recall, working memory, and sustained attention are related to stroke patients’ performance. In addition, word-finding difficulties are a widespread symptom attributed to many factors. In fatigue, great stress, and taking many medications, healthy speakers can also experience difficulty recalling vocabulary.
At the end of the section, as a clinical point, it can be acknowledged that referring stroke patients to a neurologist and providing services during treatment-rehabilitation services by neurologists and SLPs would benefit these patients. The advantages of this teamwork include organization and familiarization with spatial-temporal position (orientation) and strengthening of respiratory support, awareness of the coordination of the breathing system and vocalization, strengthening of the facial and mouth muscles, increasing the phonological-semantic awareness of names and training to retrieve words with fluent expression and strengthening of functional memory and other cognitive dimensions increase linguistic and cognitive performance in stroke patients. In addition to being consistent with similar research, the important results of the research had innovations that include the effect of a regular and targeted treatment program on the rate of recovery of the patient’s speech and cognitive aspects, as well as the impact of early rehabilitation services (up to 6 months after the onset of stroke) on all-round progress of the patient.
Conclusion
The research results about the objectives of “the effectiveness of neurological rehabilitation in stroke patients” for 22 adult participants are only presented in the two fields of changes resulting from the AQ1 and MMSE tests. The mean scores of AQ1 and MMSE before and after treatment significantly differed. The average score of AQ1 before and after treatment is not significantly different in the two types of aphasia. Still, cognitive dimensions according to the MMSE test before and after treatment are significantly different in the two types of aphasia. Results indicate that gender, employment status, marital status, income level, and age have no significant relationship with changes in AQ1 and MMSE scores and the effect of the intervention on these two variables. In addition, it was observed that the changes in MMSE caused by the intervention significantly correlate with education level and the number of children.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1400.049).
Funding
The study was funded by the University of Social Welfare and Rehabilitation Sciences (Grant No.: 2407).
Authors' contributions
Conceptualization and study design: Mojtaba Azimian, Morteza Farazi and Reza Nilipour; Data acquisition: Morteza Farazi, Mohammad Sayad Nasiri, Marzieh Amrevani, and Zahra Valitabar Kerati; Data analysis and interpretation: Mojtaba Azimian, Morteza Farazi, Reza Nilipour and Mohammad Sayad Nasiri; Statistical analysis: Samaneh Hosseinzadeh; Initial draft preparation: Morteza Farazi; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patients participating in the study and the nurses of the Stroke Department of Rofeideh Rehabilitation Hospital.
In a stroke, an artery supplying blood to the brain is blocked by a blood clot (ischemic stroke), or a blood vessel in the brain bursts and cuts off blood flow to a portion of the brain (hemorrhagic stroke). Aphasia most frequently results from strokes, which sometimes is associated with dysarthria and dyspraxia. Every year, over 15 million people worldwide suffer from some degree of stroke and experience various complications, such as sensory-motor, cognitive, and language disabilities [1]. According to several studies, 23%-36% of stroke survivors experience various degrees of language-cognitive damage (aphasia) [2]. Aphasia is an acquired defect in language usage (expressive and perceptive language), which results from damage to specific language areas in the brain. Language impairment in aphasia depends on the type of damage, the location of the damage in the brain, and the severity of the problem, leading to different degrees of language comprehension and expression [3]. It also causes problems in naming, discussing, understanding concepts, repeating numbers and sentences, verbal fluency, verbal explanations, issues in defining words, and ambiguity in interpreting words and metaphors, especially metalinguistic disorders. Usually, communicating requires the ability to speak and use the appropriate language. Naturally, such injuries will destroy various aspects of a person’s life, such as communication, participation in daily activities, individual independence, economic status, and quality of life (QoL) [4, 5]. Therefore, these individuals are damaged to varying degrees in daily communication, meeting personal needs, and participating in society, depending on the effects of symbolic communication (including speaking, listening, reading, and writing) in aphasia patients [6, 7]. Word-finding defects are considered the main symptom of aphasia [8, 9].
Therefore, the most common language deficits in stroke patients are anomia or disorder in word retrieval, where word retrieval defects may be observed to express all concepts, including noun, verb, adjective, and adverb, and aphasia patients may have more difficulty in retrieving some grammatical concepts than other groups [10-12]. Studies have reported different morphological, phonological, gestural, and semantic methods for treating word retrieval impairments in aphasia caused by brain damage. The results of these treatments are not the same, but the improvement achieved in most treatments is specific to trained cases [13-15]. However, the provision of rehabilitation services based on the individual needs of stroke patients requires extensive screening and evaluation of the severity and type of language injuries.
Many standard tests have been developed in Western countries to evaluate different aspects of language, such as syntax, semantics, word search, listening comprehension, and reading. Some of these tests include the Western aphasia battery and Boston diagnostic aphasia examination [16]. In Iran, Dr. Nilipour et al. developed the clinical version of the Persian diagnostic aphasia battery bedside version (P-DAB-AQ1, 2016) to screen and assess the severity of acquired language disorders in Persian-speaking adults with brain injuries [17].
In neuropsychological rehabilitation, the neuropsychological principles that are effective in the severity of a stroke and aphasia include the severity of the disorder, type of stroke, extent of the lesion, location of the stroke, and whether it is unilateral or bilateral. A CT scan should determine whether a stroke is present, and other individual factors like age, sex, hand side, whether the patient is monolingual or bilingual, and length of hospital stay should also be considered. This study investigated all the cases of stroke patients receiving advanced rehabilitation in the speech therapy and neurology departments. The results of the clinical-linguistic evaluations of the patients were compared by a neurologist and a speech and language pathologist (SLP) in two stages: 1) Initial admission in the mentioned departments and 2) After discharge from the hospital. Notably, the comparative evaluation was based on an internationally standardized valid aphasia test for the Persian language (P-DAB-AQ1, 2016) and medical and paraclinical examination. This assessment comprises the severity of aphasia disorder, each patient’s recovery rate based on the treatment methods used, and the effect of various individual factors [17].
The World Health Organization (WHO) predicts that the number of strokes in the European :union:, Iceland, Norway, and Switzerland will rise from 1.1 million in 2000 to 1.5 million by 2025. Also, according to a systematic review conducted in South America, the crude score of stroke prevalence varies from 1.74 to 6.51 per 1000 people, and its annual incidence rate is 0.35 to 1.83 per 1000 people [2]. Numerous studies on aphasia treatment have been conducted and are ongoing. Falconer et al. subjected four aphasic patients to the treatment of semantic feature analysis (SFA) with continuous speech tasks. It was hypothesized that retrieving words during discourse would be more efficient and significantly impact communication. The results show that using SFA in group therapy can improve an individual’s communication performance [18]. Wambaugh et al. studied the effect of SFA treatment on verb naming performance in four English-speaking aphasic patients. Verbs were categorized into four groups of ten without semantic connection. After 12 therapy sessions, an increase in the accuracy of naming educational verbs was observed in 3/4 of the participants, no improvement in control verbs, and an increase in speech content was observed for one participant [19]. Kristensson et al. performed the intensive SFA treatment to increase speech and communication function content in three people with chronic aphasia. This treatment completed the naming task for 21 nouns and 21 verbs. The results showed that two participants had an increase in speech performance and an increase in self-correction. However, they did not show significant improvement in naming [20].
Mehri et al. investigated and compared the effect of semantic and phonetic guidance on facilitating the naming process in patients with aphasia and Alzheimer disease, considering the common impairments of comprehension and naming, as well as temporal and temporal lobe defects. The study was conducted cross-sectionally on seven patients with fluent aphasia and seven patients with Alzheimer disease. The study results showed that both types of patients benefited from semantic and phonetic guidance. Still, fluent aphasia patients benefited more from phonetic guidance. Alzheimer patients benefited more from semantic guidance, which shows that the damage of semantic representation in Alzheimer patients is more than in other patient groups [21]. Sadeghi et al. investigated and compared the effect of SFA and promoting aphasia communication efficacy (PACE) methods on the ability to name aphasia patients. A 2-week study was conducted on four patients with dyspraxia; after the intervention, the ability to name therapeutic words increased significantly in both methods, except for one participant with damage to the left basal ganglia, in whom the SFA method was ineffective. The observed changes in the PACE method were greater than those in SFA, and the ability to name control words, generate semantic coordinates, and transfer the message improved. One week after the interventions, the performance of the patients in naming therapeutic words was still above the baseline despite a slight decrease [22]. Parhoon et al. conducted a study on the effectiveness of cognitive rehabilitation on the executive functions of stroke patients. The cognitive rehabilitation program has re-learned mental actions, and based on brain flexibility, it has improved the patients’ functional memory and selective attention [23].
In investigating the effectiveness of computer-based cognitive rehabilitation on enhancing the working memory of stroke patients in Tabriz, Ghorbanian et al. asserted that cognitive problems are one of the most prevalent issues among stroke patients. Also, the findings showed that computer-based cognitive rehabilitation improves working memory in stroke patients [24].
Considering the lack of research in this area, conducting related but underappreciated research seems essential. On this basis, the current study examined the efficacy of neurological rehabilitation for stroke patients with language and cognitive disorders. We emphasized the prevention and control of confounding factors, such as blood pressure and reducing mental stress in the cause of stroke, referring patients to neurologists after brain injuries, accurate diagnosis of the disorder, and prompt referral to speech therapy. Also, providing treatment-rehabilitation services, particularly during the first 6 months of a patient’s illness, and fostering family participation is essential. This study aimed to investigate the effectiveness of neurological rehabilitation on the cognitive status of stroke patients.
Materials and Methods
This research is a quasi-experimental study before and after the intervention. The study was conducted on 22 adult Persian-speaking stroke patients with an average age of 64.31 years. They were selected from 41 patients who visited Rofiedeh Rehabilitation Hospital between March 2020 and October 2021. These patients with various cognitive disorders, fluency, and non-fluent aphasia were chosen based on the inclusion criteria: Speaking Farsi language, lacking history of previous stroke, being adult patients with left hemisphere stroke, having fluent and non-fluent aphasia caused by stroke, starting treatment 2 to 8 months after the complication, being stroke patients with cognitive disorders based on the MMSE test with a score below 23, taking up to 75% correct answers in clinical questionnaire of Persian picture naming battery test, being conscious during evaluation and therapeutic interventions, having minimum reading and writing literacy, and having normal hearing and vision. The data collection tools and methods included an acceptance questionnaire, personal information of an adult stroke patient with aphasia, and the Iranian version of the Farsi aphasia diagnostic test (P-DAB-1 record form, AQ1). The method of execution and scoring of the P-DAB is based on the scores obtained from the execution of different versions of the test: Four different quantitative indicators can be calculated to determine the severity and type of linguistic-cognitive disorders. These quantitative indicators are as follows:
• Clinical prescription severity index for aphasia quotient screening (AQ1),
• Aphasia quotient (AQ2) severity index of oral language disorders,
• Aphasia quotient (AQ3) severity index of oral language disorder, and
• Aphasia cortical quotient (CQ1) severity index of oral and written language and cognitive disorders [17].
The components of this tool (P-DAB-1 record form, AQ1) include continuous speech content quality (4 items), fluency of speech (6 items), listening comprehension (10 items), comprehension of continuous commands (4 items), ability to repeat words (6 items), and naming ability (20 items). Dr Nilipour et al. checked and confirmed the validity and reliability of this tool in Iran [17].
The Persian picture naming battery clinical questionnaire contains 50 clear and distinct nominal images designed on a separate page. By presenting a picture, the therapist asks the patient to say the name of that picture. The answer sheet contains four options: No guidance, semantic guidance, phonetic guidance, and type of error. The severity of the disorder is mild, moderate, and severe. Up to 75% of correct answers are mild disorder severity, 50% to 75% are moderate, and less than 50% represent severe disorder severity.
The mini-mental state examination (MMSE) contains questions with 30 points that determine cognitive problems, especially memory in adults. In scoring, 0 is given for wrong answers and 1 for correct answers. Therefore, scores of 24 to 30 indicate a normal condition, and below 23 indicate a disorder and the need for psychiatric consultation. In internal studies by Kazazi et al., the degree of confidence and ability to do it are 95% and 80%, respectively [25].
The diagnostic tools for stroke patients include CT scans, MRI, and fMRI. In this study, the cause of the disease was determined solely by MRI findings. Also, after the patient’s visit and the neurologist’s diagnosis of a stroke, according to MRI findings and based on the referral form, aphasia patients were referred to a SLP to determine the cause of the complication. The treatment methods used in this study include treatment programs based on the damage mapping hypothesis, verb network strengthening therapy, treatment of underlying constructions, treatment of underlying forms, melodic intonation therapy, SFA, and treatment around cognitive components such as perception, attention, memory, language, and thinking. Neurological rehabilitation is a medically controlled process to heal a damaged part of the nervous system. Neurological rehabilitation often reduces disease symptoms, strengthens or stabilizes new behavioral patterns, and rehabilitates and empowers the damaged functions of the patient’s nervous system.
Each patient began treatment between 2 and 8 weeks after sustaining a brain injury. An SLP provided rehabilitation services four times weekly (one 30-minute daily session) for one year and seven months. Due to the nature of aphasia, this treatment period did not affect the spontaneous recovery of the disorder. The treatment of patients varied according to severity, disorder type, and individual requirements. After the treatment, the patients’ AQ1 and MMSE questionnaires were reviewed and completed. Finally, the collected data were analyzed. Data analysis was done using the SPSS software version 19. The characteristics of the study participants were summarized using the Mean±SD or number and percentage. The Shapiro-Wilk test was used to check the normal distribution of research variance. The Mann-Whitney and the Kruskal-Wallis non-parametric tests were applied to compare the means of the research variables in background variables with two groups, respectively. Wilcoxon’s non-parametric test was used to compare research variance before and after the intervention.
Results
According to the results, 54.5% of the participants are male, 45.5% female, 72.7% employed, 72.7% married, 31.8% educated, and 77.3% had an average economic status. Table 1 shows that 10 patients (equivalent to 45.45%) had fluent aphasia and 12 of them (equivalent to 54.55%) had non-fluent aphasia.
Table 2 shows that the average AQ1 score of the participants has increased from 74.80 to 80.12, and the average MMSE score has increased from 17 to 22.59.
The main variables do not follow a normal distribution (P<0.05), but the difference between scores before and after the intervention follows a normal distribution (P<0.05).
According to Table 3, the results of the Wilcoxon test, the mean score of AQ1, and MMSE before and after treatment had a significant difference.
According to the Mann-Whitney test in Table 4, the average score of AQ1 before and after treatment is not significantly different in the two types of aphasia.
Still, MMSE recognition before and after treatment significantly differs in the two types of aphasia. The t test of two independent groups shows no significant difference in the AQ1 score in the fluent and non-fluent aphasia groups. Still, there is a significant difference in the MMSE score in the fluent and non-fluent aphasia groups. The MMSE increase was higher in the non-fluent aphasia group.
According to the Spearman correlation coefficient in Table 5, there is no significant association between research variables with age and the number of children.
According to the Pearson correlation coefficient, the difference between the AQ1 score before and after treatment has no significant relationship with age and number of children. Still, a significant relationship exists between MMSE score before and after treatment and the number of children.
Discussion
As mentioned previously, the communication and pathological problems of these patients become more and more severe in the advanced stages of stroke, so the reduction of social participation due to existing communication problems endangers the emotional and mental health of the patient. The pathology and language deficit in aphasia, depending on the type of damage, the location of the damage in the brain, and the severity of the problem, leads to different degrees of language comprehension and expression problems. Since the current study aimed to examine the efficacy of neurological rehabilitation in stroke patients, the findings are compared to those of similar research. In this study, it was found that the average research variables of the type of individual factors, such as gender, occupation, marital status, place of residence, income level, education level, cause and location of the complication, and the number of children before and after treatment did not differ significantly among the participants. Also, based on the MMSE test, the education level affects patients’ cognitive performance before and after treatment. This finding means that patients with a higher level of education had better performance in cognitive dimensions such as understanding, sustained attention, general memory, working memory, language, and thinking, which is in line with the study by Rahmani et al. [26]. According to this study, all participants showed functional improvement in continuous speech development and vocabulary retrieval. Thus, continuous speech and vocabulary retrieval are more efficient and possess a more meaningful communication aspect. This finding indicates that all participants showed improved performance in continuous speech tasks using SFA, and the results were consistent with Wambaugh and Falconer [15, 20]. The results of this study indicate that the average AQ1 score before and after treatment in two types of fluent and non-fluent aphasia is not significantly different. Based on the MMSE test before and after treatment, there is a significant difference in the treatment of two types of aphasia, and this variable is significantly less in the fluent aphasia group. It has been determined that word naming, language processing, word recall, working memory, and sustained attention are related to stroke patients’ performance. In addition, word-finding difficulties are a widespread symptom attributed to many factors. In fatigue, great stress, and taking many medications, healthy speakers can also experience difficulty recalling vocabulary.
At the end of the section, as a clinical point, it can be acknowledged that referring stroke patients to a neurologist and providing services during treatment-rehabilitation services by neurologists and SLPs would benefit these patients. The advantages of this teamwork include organization and familiarization with spatial-temporal position (orientation) and strengthening of respiratory support, awareness of the coordination of the breathing system and vocalization, strengthening of the facial and mouth muscles, increasing the phonological-semantic awareness of names and training to retrieve words with fluent expression and strengthening of functional memory and other cognitive dimensions increase linguistic and cognitive performance in stroke patients. In addition to being consistent with similar research, the important results of the research had innovations that include the effect of a regular and targeted treatment program on the rate of recovery of the patient’s speech and cognitive aspects, as well as the impact of early rehabilitation services (up to 6 months after the onset of stroke) on all-round progress of the patient.
Conclusion
The research results about the objectives of “the effectiveness of neurological rehabilitation in stroke patients” for 22 adult participants are only presented in the two fields of changes resulting from the AQ1 and MMSE tests. The mean scores of AQ1 and MMSE before and after treatment significantly differed. The average score of AQ1 before and after treatment is not significantly different in the two types of aphasia. Still, cognitive dimensions according to the MMSE test before and after treatment are significantly different in the two types of aphasia. Results indicate that gender, employment status, marital status, income level, and age have no significant relationship with changes in AQ1 and MMSE scores and the effect of the intervention on these two variables. In addition, it was observed that the changes in MMSE caused by the intervention significantly correlate with education level and the number of children.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1400.049).
Funding
The study was funded by the University of Social Welfare and Rehabilitation Sciences (Grant No.: 2407).
Authors' contributions
Conceptualization and study design: Mojtaba Azimian, Morteza Farazi and Reza Nilipour; Data acquisition: Morteza Farazi, Mohammad Sayad Nasiri, Marzieh Amrevani, and Zahra Valitabar Kerati; Data analysis and interpretation: Mojtaba Azimian, Morteza Farazi, Reza Nilipour and Mohammad Sayad Nasiri; Statistical analysis: Samaneh Hosseinzadeh; Initial draft preparation: Morteza Farazi; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patients participating in the study and the nurses of the Stroke Department of Rofeideh Rehabilitation Hospital.
References
- Truelsen T, Piechowski-Jóźwiak B, Bonita R, Mathers C, Bogousslavsky J, Boysen G. Stroke incidence and prevalence in Europe: A review of available data. European Journal of Neurology. 2006; 13(6):581-98. [DOI:10.1111/j.1468-1331.2006.01138.x] [PMID]
- Saposnik G, Del Brutto OH; Iberoamerican Society of Cerebrovascular Diseases. Stroke in South America: A systematic review of incidence, prevalence, and stroke subtypes. Stroke. 2003; 34(9):2103-7. [DOI:10.1161/01.STR.0000088063.74250.DB] [PMID]
- Bhogal SK, Teasell R, Speechley M. Intensity of aphasia therapy, impact on recovery. Stroke. 2003; 34(4):987-93. [DOI:10.1161/01.STR.0000062343.64383.D0] [PMID]
- Pernacchio AS. Treatment outcomes for semantic feature analysis in aphasia: A case study [MSc thesis]. New Haven: Southern Connecticut State University; 2010. [Link]
- Raymer AM, Ciampitti M, Holliway B, Singletary F, Blonder LX, Ketterson T, et al. Semantic-phonologic treatment for noun and verb retrieval impairments in aphasia. Neuropsychological Rehabilitation. 2007; 17(2):244-70. [DOI:10.1080/09602010600814661] [PMID]
- Cruice M, Hill R, Worrall L, Hickson L. Conceptualising quality of life for older people with aphasia. Aphasiology. 2010; 24(3):327-47. [DOI:10.1080/02687030802565849]
- Vigliocco G, Vinson DP, Druks J, Barber H, Cappa SF. Nouns and verbs in the brain: A review of behavioural, electrophysiological, neuropsychological and imaging studies. Neuroscience & Biobehavioral Reviews. 2011; 35(3):407-26. [DOI:10.1016/j.neubiorev.2010.04.007] [PMID]
- Jong-Hagelstein M. Word finding deficitsin aphasia: Diagnosis and treatment. Rotterdam Aphasia Therapy Study-2. Rotterdam: Erasmus University Rotterdam; 2011. [Link]
- LaPointe LL. Aphasia and related neurogenic language disorders. New York: Thieme; 2011. [DOI:10.1055/b-006-161009]
- Chapey R. Language intervention strategies in aphasia and related neurogenic communication disorders. Pennsylvania: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008. [Link]
- Kiran S. Complexity in the treatment of naming deficits. American Journal of Speech-Language Pathology. 2007; 16(1):18-29. [DOI:10.1044/1058-0360(2007/004)]
- Yadegari F, A’zimian M, Rahgozar M, Biglarian A. [Severity and co-occurrence of oral and verbal apraxias in left brain damaged adults (Persian)]. Archives of Rehabilitation. 2012; 13(1):8-16. [Link]
- Boo M, Rose ML. The efficacy of repetition, semantic, and gesture treatments for verb retrieval and use in Broca’s aphasia. Aphasiology. 2011; 25(2):154-75. [DOI:10.1080/02687031003743789]
- No author. What’s the difference between aphasia, dysphasia and dysarthria? [Internet]. 2018 [Updated 2024 October 22]. TTRS. Available from: [Link] .
- Boyle M. Semantic feature analysis treatment for aphasic word retrieval impairments: What’s in a name? Topics in Stroke Rehabilitation. 2010; 17(6):411-22. [DOI:10.1310/tsr1706-411]
- Wambaugh J, Cameron R, Kalinyak-Fliszar M, Nessler C, Wright S. Retrieval of action names in aphasia: Effects of two cueing treatments. Aphasiology. 2004; 18(11):979-1004. [DOI:10.1080/02687030444000471]
- Nilipour R, Pourshahbaz A, Ghoreyshi ZS. Reliability and validity of bedside version of Persian WAB (P-WAB-1). Basic and Clinical Neuroscience. 2014; 5(4):253-8. [PMID]
- Falconer C, Antonucci SM. Use of semantic feature analysis in group discourse treatment for aphasia: Extension and expansion. Aphasiology. 2012; 26(1):64-82. [DOI:10.1080/02687038.2011.602390]
- Wambaugh JL, Ferguson M. Application of semantic feature analysis to retrieval of action names in aphasia. Journal of Rehabilitation Research & Development. 2007; 44(3):381-94. [DOI:10.1682/JRRD.2006.05.0038] [PMID]
- Kristensson J, Behrns I, Saldert C. Effects on communication from intensive treatment with semantic feature analysis in aphasia. Aphasiology. 2015; 29(4):466-87. [DOI:10.1080/02687038.2014.973359]
- Mehri A, Jahani Y, Alemi R, Aramipour E. [Investigation of usage of semantic and phonological cues in naming of fluent aphasia and Alzheimer disease (Persian)]. Audiology. 2008; 16(2):51-6. [Link]
- Sadeghi Z, Baharloei N, Moddarres Zadeh A, Ghasisin L. Comparative effectiveness of semantic feature analysis (SFA) and phonological components analysis (PCA) for anomia treatment in Persian speaking patients with aphasia. Iranian Rehabilitation Journal 2017; 15 (3) :259-68. [DOI: 10.29252/nrip.irj.15.3.259]
- Parhoon H, Moradi A, Hasanabadi H, Akbari ME. [Effectiveness of cognitive rehabilitation on Executive Function and Self care Behavior in patients with Brest Cancer (Persian)]. Journal of Research in Behavioural Sciences. 2019; 16(3):365-78. [DOI:10.52547/rbs.16.3.365]
- Ghorbanian E, Alivandi Vafa M, Farhoudi M, Nazari MA. [Effectiveness of computer-based cognitive rehabilitation intervention on working memory of patients with stroke in Tabriz (Persian)]. Neuropsychology. 2019; 5(16):157-72. [DOI:10.30473/clpsy.2019.44834.1406]
- Kazazi L, Foroughan M, Nejati V, Shati M. Association between age associated cognitive decline and health related quality of life among Iranian older individuals. Electronic Physician. 2018; 10(4):6663-6671. [DOI: 10.19082/6663] [PMID]
- Rahmani F, Khanjani MS, Marsa R, Sharifi G, Bahadori E, Sarani EM. Learning strategies and verbal memory deficits on the Shiraz verbal learning test in patients with alzheimer’s disease and amnestic mild cognitive impairment. Iranian Journal of Psychiatry and Behavioral Sciences. 2022; 16(2). [DOI: 10.5812/ijpbs-118139]
Article type: Original Research Articles |
Subject:
Speech therapy
Received: 2023/08/31 | Accepted: 2023/12/30 | Published: 2024/12/20
Received: 2023/08/31 | Accepted: 2023/12/30 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
