
988368
Tue, Jul 28, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 547-556 |
Back to browse issues page


Ethics code: IR.USWR.REC.1401.018-3735
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sattari Z, Hatamizadeh N, Shahshahani S, Hosseinzadeh S. Assistive Technology Assessment and Barriers to Access It in Children with Disability. Iranian Rehabilitation Journal 2024; 22 (4) :547-556
URL: http://irj.uswr.ac.ir/article-1-2118-en.html
URL: http://irj.uswr.ac.ir/article-1-2118-en.html



1- Department of Rehabilitation Management, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Rehabilitation Management, Pediatric Neurorehabilitation Research Center, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Rehabilitation Management, Pediatric Neurorehabilitation Research Center, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Disability, Children, Assistive technology (AT), Rapid assessment of assistive technology rATA, World Health Organization (WHO)
Full-Text [PDF 533 kb]
(1195 Downloads)
| Abstract (HTML) (4577 Views)
References
Full-Text: (1090 Views)
Introduction
It is estimated that 207.4 million (12.5%) people aged 5-19 years old worldwide suffer from some form of moderate-to-severe disability [1]. Many children with disabilities are deprived of education due to their health conditions and environmental barriers. Providing medical care, rehabilitation, appropriate assistive technology (AT), and improving accessibility can help them achieve full participation in educational and social integration [2]. Disabilities can restrict children’s active learning, leading to delayed physical, motor, cognitive, social, and adaptive development. Some children with disabilities require more or easier-to-use devices for active learning and skill development. They may need more attractive or colorful devices to encourage their use. These devices are called AT devices [3]. They help people with disabilities do activities that would be difficult or impossible without them [4]. Some children need AT devices for extended periods, while others require them for short-term use following trauma or illness until their recovery [5]. However, according to the World Health Organization (WHO), AT devices are accessible to only 1 in 10 people who need them. To fulfill the goals of the convention on the rights of persons with disabilities and ensure that all people with disabilities have access to AT devices, it is necessary to identify unmet needs for AT devices [5]. Rehabilitation services in Iran are mainly provided as center-based or community-based rehabilitation. In rehabilitation centers, therapists assess the AT needs of people with disabilities, while in the community-based rehabilitation program, experts in the Medical Commission of the Welfare Organization perform these assessments. Although Iran is one of 35 countries that measures the population’s access to AT [6], no specific tool is routinely used for AT needs assessment and reporting. Studies have shown that the prevalence of AT needs varies with regard to different countries, socioeconomic status, age groups, and genders [6].
This study focuses on AT usage, unmet needs, accessibility, and barriers to using AT devices in primary school-aged children, as this is a critical period for developing a range of academic and social competencies. The WHO’s rapid AT tool (rATA) is used in this study. This article also addresses the strengths and weaknesses of using this general AT assessment tool for the subgroup of children with disabilities.
Materials and Methods
The inclusion criterion for the interviewees was being parents of 6- to 12-year-old children with any physical, mental, visual, hearing, or speech disabilities living in Chaharmahal and Bakhtiari Province, Iran. The exclusion criterion was the unwillingness of parents to stay until the end of the interview. The list of people with disabilities registered by the Welfare Organization was used for sampling, including 1443 people with disabilities in this age group—informed consent was obtained from parents who participated in this study before interviews. Parents of children were randomly selected from the list of children with disabilities in each province area. The total sample size was 217, and the sample from each region was proportional to the number of children with disabilities living in that area. The questionnaire was filled by face-to-face interviews in the waiting rooms of rehabilitation centers when the parents and children came for therapy or by audio-visual tele-interviewing parents using cell phones. All interviews lasted for three months, from June to the end of August 2022.
The sample size was calculated as follows (Equation 1):

Study measurements
The assessment was done using the rATA tool, a household survey tool, which consists of seven parts: 1) Preliminary information, 2) Demographics, 3) Needs, 4) Demand and supply, 5) Satisfaction, 6) Recommendation (optional), and 7) Surveyor’s comments. WHO has developed this tool, and its face and content validities have been examined by distributing the draft among WHO regional and country offices and external AT experts, refining the tool based on their feedback [7, 8]. Each part consisted of multiple choice questions, and in case of asking about need and supply, the questionnaire included a list of predefined assistive devices along with pictures of those devices. It should be used to interview people with disabilities or by parental proxy when assessing children. The Persian version of the rATA questionnaire used in this study passed the translation, back translation, and adaptation process by Shirazikhah et al. in collaboration with the technical rATA committee of WHO [6]. The questionnaire takes an average of 20-30 minutes to complete.
Data analysis
Data analysis was performed using SPSS software, version 26, using the questionnaire’s instructions.
Results
Data were gathered from 217 children with disabilities aged 6-12 years, with an average age of 8.87±2.01 years. The male-to-female ratio was 3:2, and 60% of the children lived in rural areas. Table 1 presents the prevalence of different functional limitations among the participants.
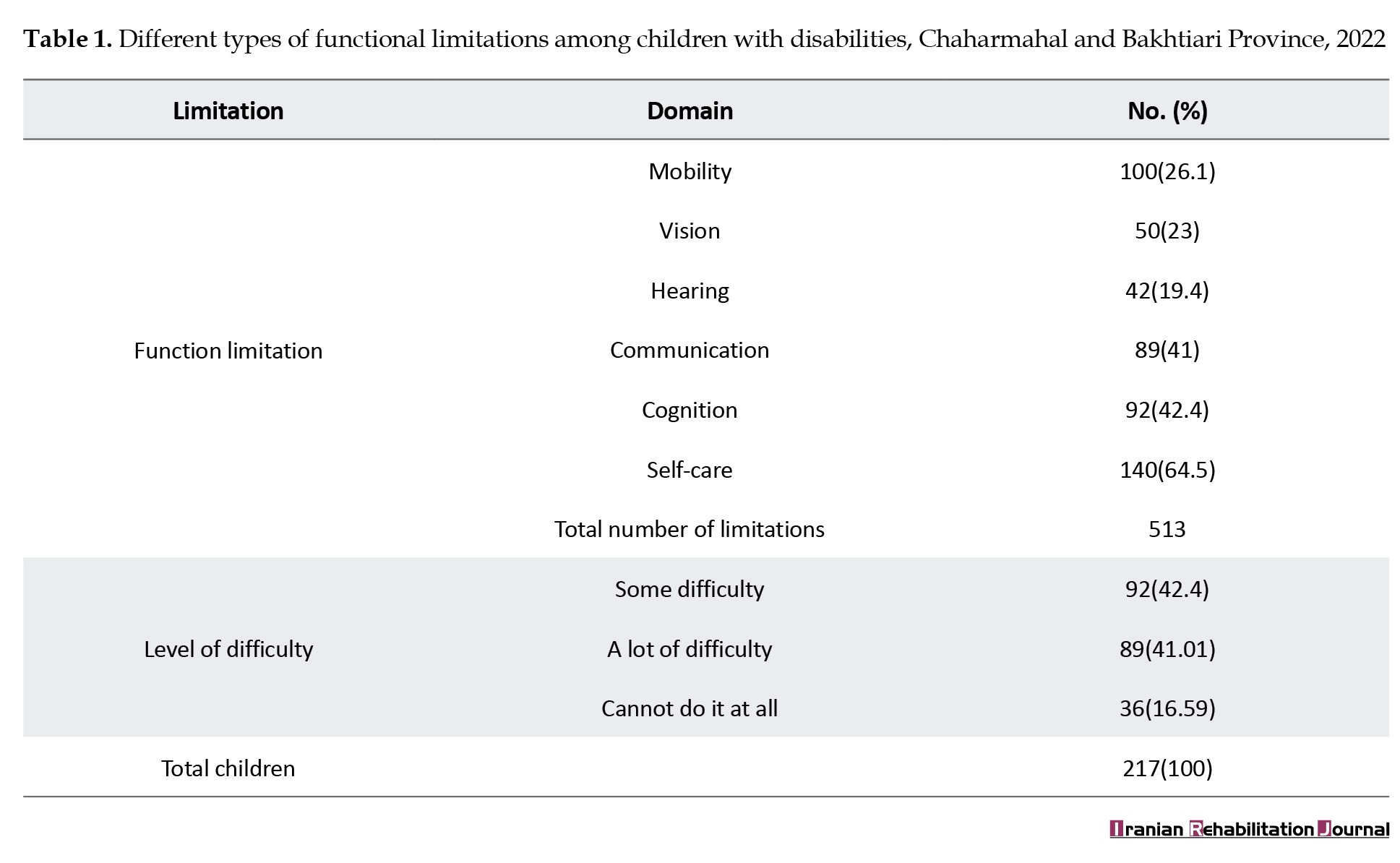
As shown in Table 1, parents of the 217 children with disabilities reported a total of 513 functional limitations. Mobility and communication limitations were the most commonly reported (26.1% and 41.0%, respectively) while hearing limitations were the least frequently reported (19.4%). Self-care limitations were reported in 64.5% of the children. The research population consisted of children with disabilities. All children had functional restrictions, and 16.6% could not perform some activities. The functional limitations varied from one to five among the studied children. Notably, the results showed that only 23.5% of children with disabilities had limitations confined to only one area.
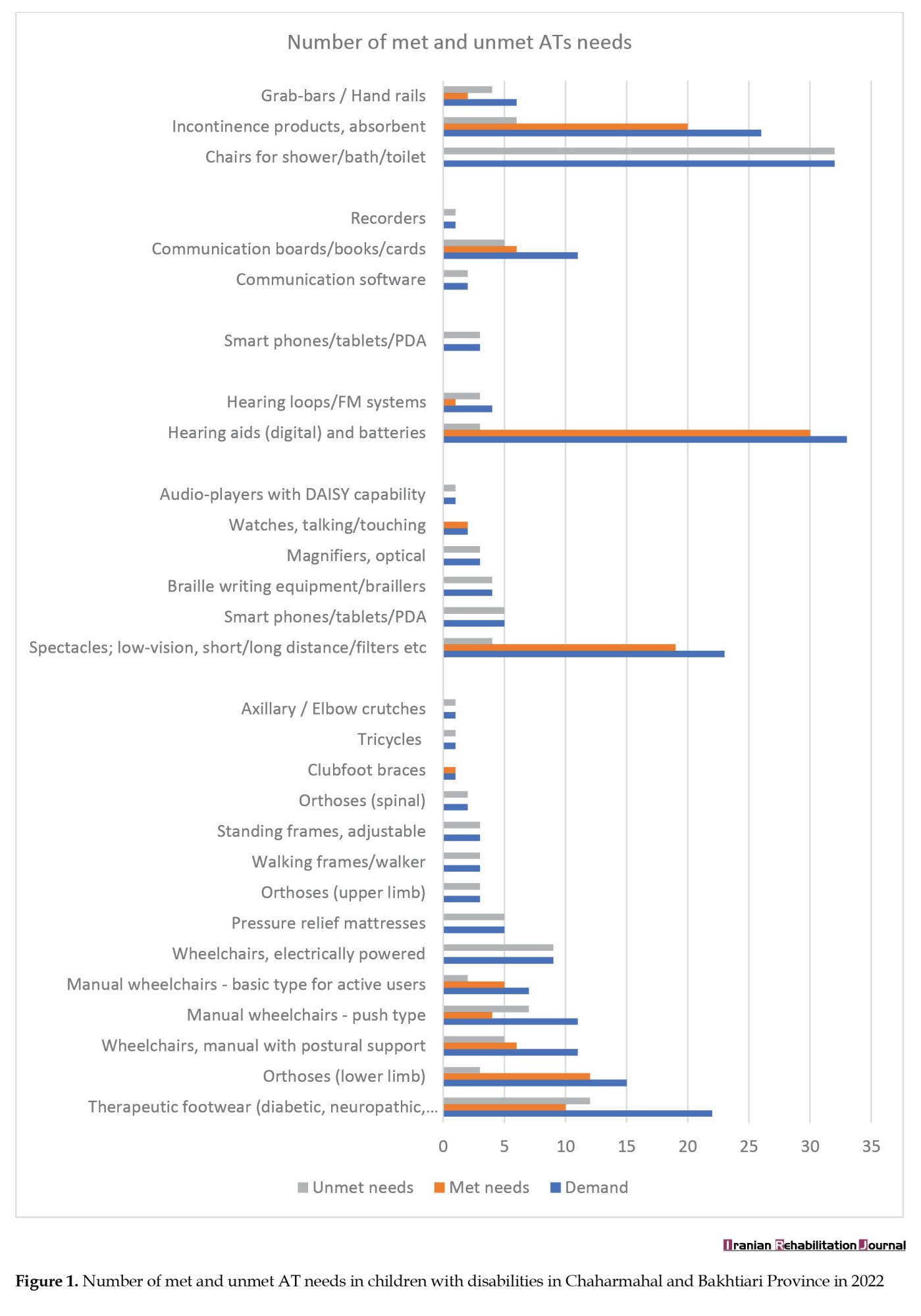
Among the 217 children with disabilities, 108(49.8%) used one or more assistive devices, and 102(47%) had one or more unmet AT needs. Some children use more than one AT device. So, in total, 125 AT devices were used by 108 children. Figure 1 shows the unmet needs for AT devices for children with disabilities.
It is estimated that 207.4 million (12.5%) people aged 5-19 years old worldwide suffer from some form of moderate-to-severe disability [1]. Many children with disabilities are deprived of education due to their health conditions and environmental barriers. Providing medical care, rehabilitation, appropriate assistive technology (AT), and improving accessibility can help them achieve full participation in educational and social integration [2]. Disabilities can restrict children’s active learning, leading to delayed physical, motor, cognitive, social, and adaptive development. Some children with disabilities require more or easier-to-use devices for active learning and skill development. They may need more attractive or colorful devices to encourage their use. These devices are called AT devices [3]. They help people with disabilities do activities that would be difficult or impossible without them [4]. Some children need AT devices for extended periods, while others require them for short-term use following trauma or illness until their recovery [5]. However, according to the World Health Organization (WHO), AT devices are accessible to only 1 in 10 people who need them. To fulfill the goals of the convention on the rights of persons with disabilities and ensure that all people with disabilities have access to AT devices, it is necessary to identify unmet needs for AT devices [5]. Rehabilitation services in Iran are mainly provided as center-based or community-based rehabilitation. In rehabilitation centers, therapists assess the AT needs of people with disabilities, while in the community-based rehabilitation program, experts in the Medical Commission of the Welfare Organization perform these assessments. Although Iran is one of 35 countries that measures the population’s access to AT [6], no specific tool is routinely used for AT needs assessment and reporting. Studies have shown that the prevalence of AT needs varies with regard to different countries, socioeconomic status, age groups, and genders [6].
This study focuses on AT usage, unmet needs, accessibility, and barriers to using AT devices in primary school-aged children, as this is a critical period for developing a range of academic and social competencies. The WHO’s rapid AT tool (rATA) is used in this study. This article also addresses the strengths and weaknesses of using this general AT assessment tool for the subgroup of children with disabilities.
Materials and Methods
The inclusion criterion for the interviewees was being parents of 6- to 12-year-old children with any physical, mental, visual, hearing, or speech disabilities living in Chaharmahal and Bakhtiari Province, Iran. The exclusion criterion was the unwillingness of parents to stay until the end of the interview. The list of people with disabilities registered by the Welfare Organization was used for sampling, including 1443 people with disabilities in this age group—informed consent was obtained from parents who participated in this study before interviews. Parents of children were randomly selected from the list of children with disabilities in each province area. The total sample size was 217, and the sample from each region was proportional to the number of children with disabilities living in that area. The questionnaire was filled by face-to-face interviews in the waiting rooms of rehabilitation centers when the parents and children came for therapy or by audio-visual tele-interviewing parents using cell phones. All interviews lasted for three months, from June to the end of August 2022.
The sample size was calculated as follows (Equation 1):
Study measurements
The assessment was done using the rATA tool, a household survey tool, which consists of seven parts: 1) Preliminary information, 2) Demographics, 3) Needs, 4) Demand and supply, 5) Satisfaction, 6) Recommendation (optional), and 7) Surveyor’s comments. WHO has developed this tool, and its face and content validities have been examined by distributing the draft among WHO regional and country offices and external AT experts, refining the tool based on their feedback [7, 8]. Each part consisted of multiple choice questions, and in case of asking about need and supply, the questionnaire included a list of predefined assistive devices along with pictures of those devices. It should be used to interview people with disabilities or by parental proxy when assessing children. The Persian version of the rATA questionnaire used in this study passed the translation, back translation, and adaptation process by Shirazikhah et al. in collaboration with the technical rATA committee of WHO [6]. The questionnaire takes an average of 20-30 minutes to complete.
Data analysis
Data analysis was performed using SPSS software, version 26, using the questionnaire’s instructions.
Results
Data were gathered from 217 children with disabilities aged 6-12 years, with an average age of 8.87±2.01 years. The male-to-female ratio was 3:2, and 60% of the children lived in rural areas. Table 1 presents the prevalence of different functional limitations among the participants.
As shown in Table 1, parents of the 217 children with disabilities reported a total of 513 functional limitations. Mobility and communication limitations were the most commonly reported (26.1% and 41.0%, respectively) while hearing limitations were the least frequently reported (19.4%). Self-care limitations were reported in 64.5% of the children. The research population consisted of children with disabilities. All children had functional restrictions, and 16.6% could not perform some activities. The functional limitations varied from one to five among the studied children. Notably, the results showed that only 23.5% of children with disabilities had limitations confined to only one area.
Among the 217 children with disabilities, 108(49.8%) used one or more assistive devices, and 102(47%) had one or more unmet AT needs. Some children use more than one AT device. So, in total, 125 AT devices were used by 108 children. Figure 1 shows the unmet needs for AT devices for children with disabilities.
Figure 1 shows that 132 pieces of AT devices (51.4% of total needs) remained unmet. Thirty-two parents reported the need for ‘chairs for shower/bath/toilet’ for their children, but none had this device. Additionally, none of the 9 children who needed electric wheelchairs were already using them. The need for hearing aids had been met better than other AT devices, with 90.91% of those who needed hearing aids already using them. The second-highest met need was for glasses (82.6%). Only 3 out of 92 parents of children with cognitive disabilities stated the need for some cognitive assistive device for their children.
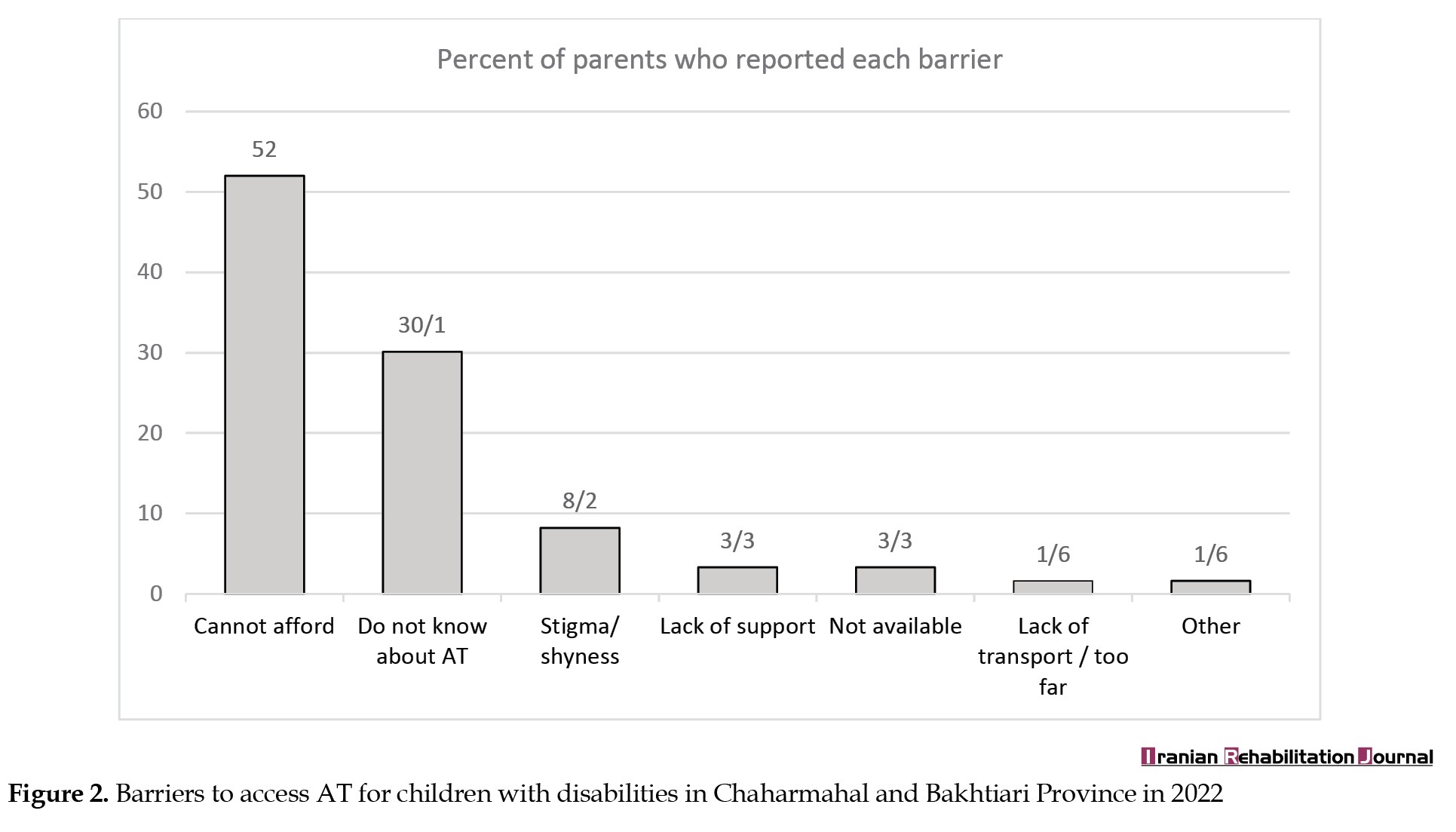
Figure 2 shows why children lack AT devices that are useful to them.
Figure 2 shows why children lack AT devices that are useful to them.
As shown in Figure 2, the most common barriers to accessing AT devices were low affordability (52%), lack of knowledge about AT devices (30.1%), and feelings of stigma and shyness (8.2%). None of the parents reported lack of time or unsuitability of devices as barriers to accessing AT devices.
The most common sources of providing AT devices were the public sector (51.9%) followed by the private sector (38.5%). Families were the source of 7.45% of AT devices, and only 2% of AT devices were provided by NGOs. None of the parents reported using self-made AT devices.
Satisfaction with different aspects of AT services varied, with the highest satisfaction reported for ‘evaluation and training of the use of the AT device’ (92.3%) and the lowest for ‘repair and maintenance services of the AT devices’ (20.2%). Table 2 presents AT devices’ needs and uses in urban and rural areas.

According to Table 2, relatively more children with disabilities in urban areas use AT devices. Still, there was no significant difference between urban and rural areas regarding unmet needs, not fully met needs, or being far away from AT providers. Furthermore, none of the AT use, unmet needs, or not fully met needs were related to the gender of the children.
Discussion
This study focuses on the AT needs of children with disabilities and the use of the rATA tool in this age group. Since the introduction of the rATA by the WHO, some studies have assessed the need for ATs to use this tool in different countries. However, they have mainly focused on the general population, and only a few examined children with disabilities’ needs. As children with known disability were included in the survey, not the general population, a sample of 217 children was sufficient to answer the research questions.
The discussion is arranged in two parts: “Children’s assistive device needs” and “challenges in using the rATA for AT needs assessment in children with disabilities.”
Children’s assistive devices need
This study found that more than 65% of children with disabilities faced limitations in taking care of themselves, with these self-care limitations being associated with limitations in sensory, cognitive, or mobility performance. Mobility limitations and hearing impairments had the highest (46.08%) and lowest (19.35%) prevalence, respectively, among children with disabilities in this study. As the study population was children with a known disability, a relatively smaller sample size was sufficient for needs assessment compared to studies on the general population [9].
A total of 217 children reported 513 functional limitations, with 23.5% having a single functional limitation and others having limitations in two or more areas. In a separate AT assessment conducted in Ukraine in 2022 using the rATA tool, 45.4% of the 7125 participants across all age ranges had limitations in one or more areas, with approximately 40% experiencing vision and 40% mobility problems. The prevalence of mobility problems in Ukraine was similar to the present study. In contrast, the prevalence of low vision among children in the present study was much lower (23%) than that reported in Ukraine [10].
The most common reasons for not using the required AT devices in the present study were lack of financial resources (52.0%), lack of knowledge about AT devices (30.1%), and feelings of stigma (8.2%), as reported by parents. In a study by Saloojee et al. in South Africa, lack of knowledge about AT devices was among the most frequently reported reasons for not using AT devices among 156 children under 18 [11]. Similarly, in Hung et al’s study in South Taiwan in 2007, financial limitations and lack of information about AT devices were also prevalent barriers to using AT devices [12]. Although different barriers may be the leading cause for not using traditional devices as opposed to newly introduced digital ones, these differences could not be accessed in the present study using the rATA tool, which asks about all barriers that the family confronted with to obtain all needed devices, not for each device, one by one. Zamanpour et al. assessed the needs of 72 teenage students with hearing loss from the students’ and their parents’ points of view in Ahvaz City, Iran. The results indicated that more than 95% of the students were using digital hearing aids; however, almost all had difficulties performing one or more daily living activities for which there were AT devices to help them. Moreover, nearly none of the participants knew about other AT devices that could be helpful for their conditions. After being informed about the existence of AT devices, their need for each of the introduced aids ranged from 3% to 96% [13]. Informing the participants about the existence of different AT devices and their helpfulness might help them better appraise their needs, as pointed out in the literature [6].
In the present study, 49.8% of children with disabilities used an assistive device, and relatively more children in urban areas used AT devices; the difference was all due to AT devices being accessed from a private section, and parents paid for it out-of-pocket. About 47.0% of children with disability in this study had an unmet need for AT. In a needs assessment of AT devices in outpatient rehabilitation centers in Costa Rica using the rATA tool, 32% of the 615 participants were children and teenagers with disabilities. In that study, 68% of people used an AT, and 47% needed a replacement or a new one [14]. In South Africa in 2006, the relative prevalence of unmet need for ATs was 72% among children with disabilities [11]. Therefore, the prevalence of unmet needs in the present study was similar to that of Costa Rica but much lower than in South Africa.
In the present study, 125 out of 257 needed AT devices (48.6%) were met, while in the Saloojee study in South Africa, only 28% of AT needs in children were met [11]. Wheelchairs, seats, and standing frames were among the most commonly used rehabilitation aids by children in Africa [11]. In contrast, hearing aids, spectacles, various types of manual wheelchairs, and therapeutic footwear were the most used devices in the present study. Notably, the above-mentioned assistive devices are the ones Welfare Organization provides at reduced cost. In a regional survey on the use of ATs in children with physical disabilities in South Taiwan in 2007, 124 children with disabilities used 224 AT devices. About 90% of those children had AT devices, which included orthotics (62.10%), mobility aids (41.13%), therapy/training devices (16.94%), and AT devices for activities of daily living (2.42%). They modified the ‘nordic classification system on aids for disabled persons’ to classify the assistive devices [12].
In the present study, 47% of the children had an unmet need for assistive devices. The most common unmet need was for shower/bath/toilet chairs, followed by wheelchairs and medical shoes. Note that many parents were unfamiliar with ‘chair for shower/bath/toilet’ before demonstrating the picture of the device as a part of the interview process in the present study. The most prevalent unmet need in Ukraine was for complex products such as orthotics, hearing aids, and wheelchairs [10].
Challenges in using rATA for AT needs assessment in children with disability
Based on the rATA tool, parents were asked about their children’s met and unmet needs for 55 AT devices in the present study. However, only 14 items were used by some children, and some parents reported unmet needs for 30 out of 55 items, and the need for 25 items was not mentioned at all. There may be various reasons for this finding. Some items from the list of 55 AT devices might not be helpful for children. Another reason might be the indistinctness of the name and image of some other devices. For example, “travel aids, portable” is not clear enough, and there is no description of its application and usefulness. In the case of “smartphones/tablets,” parents might not know what software and programs could be installed on them or how the devices could be of use in helping their child with a disability. Some other studies have also mentioned this problem [10]. To overcome this problem of self-reporting needs assessment for AT devices, a solution might be to introduce them by showing pictures and a description of their application and usefulness to parents and children before asking if they need each device. This technique has been successfully used for assessing AT device needs in adolescents with hearing loss [13].
On the other hand, the rATA tool may not detect some of the important needs of people with disabilities. For example, this tool does not include environmental control units /remote controls, while some studies have shown that many people with disabilities need this group of AT devices. Shariatzadeh et al. assessed the rehabilitation needs of 152 people with physical-motor disabilities, aged 16-64, in Kohgiluyeh Province, Iran. They found that the unmet need for electronic devices to control the environment, such as door opening and remote controlling of televisions and air conditioners, was reported by more than 80% of respondents [15]. Additionally, some of the relatively essential needs of children with disabilities may not be detected by the rATA tool. Play and education are children’s two main ways of engagement and social participation, and these engagements are necessary for their development. However, the rATA tool does not focus on these devices, which are especially important in this age group. Therefore, it seems that developing a special version of the rATA tool to assess the AT needs of children with disabilities is necessary.
Conclusion
In this study, none of the children used AT devices for their cognitive problems, and only a few parents who had children with cognitive limitations stated their children’s need for some cognitive ATs. The need to introduce this category of ATs, their applications, and their usefulness should be given special attention as part of programs for increasing the coverage of AT devices.
Almost all parents declared their child’s need for devices that could quickly realize their function from the pictures in the rATA of the device or were commonly used in the community for many years. This issue highlights the need to review and improve the questions for introducing and asking about other less familiar devices.
Finally, as the most prevalent barrier to AT accessibility was financial shortcomings, researching to determine the most efficient and effective strategies to improve financial accessibility can be an essential step in improving the coverage of ATs among children with disabilities.
Study limitations
As many children with disability in this study were under 8 years old or had communication and or cognition limitations, interviews were done by proxy of parents, and the perceived needs of the children might not be similar to those mentioned by their parents. Furthermore, some data collection took place by tele-interview due to COVID-19 prevention measures. This condition may affect the precision of results. It should also be considered that the rATA is an interview-based survey tool that provides an overall estimation of AT needs. It is not intended to substitute the complete AT assessment process, which prescribes appropriate AT for people with disability [7].
Ethical Considerations
Compliance with ethical guidelines
This survey was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1401.018).
Funding
The current study received no financial support from any public, commercial, or non-for-profit organization.
Authors' contributions
Conceptualization: Zahra Satari, Nikta Hatamizadeh and Soheila Shahshahani; Methodology: Nikta Hatamizadeh and Samaneh Hosseinzadeh; Resources and investigation: Zahra Satari; Writing the original draft: Zahra Sattari and Nikta Hatamizadeh; Review and editing: All authors; Supervision: Nikta Hatamizadeh, Soheila Shahshahani and Samaneh Hosseinzadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors hereby express their appreciation to the officials and experts of the Welfare Organization of Chaharmahal and Bakhtiari Province and the children with disabilities and their families whose participation made this research possible.
The most common sources of providing AT devices were the public sector (51.9%) followed by the private sector (38.5%). Families were the source of 7.45% of AT devices, and only 2% of AT devices were provided by NGOs. None of the parents reported using self-made AT devices.
Satisfaction with different aspects of AT services varied, with the highest satisfaction reported for ‘evaluation and training of the use of the AT device’ (92.3%) and the lowest for ‘repair and maintenance services of the AT devices’ (20.2%). Table 2 presents AT devices’ needs and uses in urban and rural areas.
According to Table 2, relatively more children with disabilities in urban areas use AT devices. Still, there was no significant difference between urban and rural areas regarding unmet needs, not fully met needs, or being far away from AT providers. Furthermore, none of the AT use, unmet needs, or not fully met needs were related to the gender of the children.
Discussion
This study focuses on the AT needs of children with disabilities and the use of the rATA tool in this age group. Since the introduction of the rATA by the WHO, some studies have assessed the need for ATs to use this tool in different countries. However, they have mainly focused on the general population, and only a few examined children with disabilities’ needs. As children with known disability were included in the survey, not the general population, a sample of 217 children was sufficient to answer the research questions.
The discussion is arranged in two parts: “Children’s assistive device needs” and “challenges in using the rATA for AT needs assessment in children with disabilities.”
Children’s assistive devices need
This study found that more than 65% of children with disabilities faced limitations in taking care of themselves, with these self-care limitations being associated with limitations in sensory, cognitive, or mobility performance. Mobility limitations and hearing impairments had the highest (46.08%) and lowest (19.35%) prevalence, respectively, among children with disabilities in this study. As the study population was children with a known disability, a relatively smaller sample size was sufficient for needs assessment compared to studies on the general population [9].
A total of 217 children reported 513 functional limitations, with 23.5% having a single functional limitation and others having limitations in two or more areas. In a separate AT assessment conducted in Ukraine in 2022 using the rATA tool, 45.4% of the 7125 participants across all age ranges had limitations in one or more areas, with approximately 40% experiencing vision and 40% mobility problems. The prevalence of mobility problems in Ukraine was similar to the present study. In contrast, the prevalence of low vision among children in the present study was much lower (23%) than that reported in Ukraine [10].
The most common reasons for not using the required AT devices in the present study were lack of financial resources (52.0%), lack of knowledge about AT devices (30.1%), and feelings of stigma (8.2%), as reported by parents. In a study by Saloojee et al. in South Africa, lack of knowledge about AT devices was among the most frequently reported reasons for not using AT devices among 156 children under 18 [11]. Similarly, in Hung et al’s study in South Taiwan in 2007, financial limitations and lack of information about AT devices were also prevalent barriers to using AT devices [12]. Although different barriers may be the leading cause for not using traditional devices as opposed to newly introduced digital ones, these differences could not be accessed in the present study using the rATA tool, which asks about all barriers that the family confronted with to obtain all needed devices, not for each device, one by one. Zamanpour et al. assessed the needs of 72 teenage students with hearing loss from the students’ and their parents’ points of view in Ahvaz City, Iran. The results indicated that more than 95% of the students were using digital hearing aids; however, almost all had difficulties performing one or more daily living activities for which there were AT devices to help them. Moreover, nearly none of the participants knew about other AT devices that could be helpful for their conditions. After being informed about the existence of AT devices, their need for each of the introduced aids ranged from 3% to 96% [13]. Informing the participants about the existence of different AT devices and their helpfulness might help them better appraise their needs, as pointed out in the literature [6].
In the present study, 49.8% of children with disabilities used an assistive device, and relatively more children in urban areas used AT devices; the difference was all due to AT devices being accessed from a private section, and parents paid for it out-of-pocket. About 47.0% of children with disability in this study had an unmet need for AT. In a needs assessment of AT devices in outpatient rehabilitation centers in Costa Rica using the rATA tool, 32% of the 615 participants were children and teenagers with disabilities. In that study, 68% of people used an AT, and 47% needed a replacement or a new one [14]. In South Africa in 2006, the relative prevalence of unmet need for ATs was 72% among children with disabilities [11]. Therefore, the prevalence of unmet needs in the present study was similar to that of Costa Rica but much lower than in South Africa.
In the present study, 125 out of 257 needed AT devices (48.6%) were met, while in the Saloojee study in South Africa, only 28% of AT needs in children were met [11]. Wheelchairs, seats, and standing frames were among the most commonly used rehabilitation aids by children in Africa [11]. In contrast, hearing aids, spectacles, various types of manual wheelchairs, and therapeutic footwear were the most used devices in the present study. Notably, the above-mentioned assistive devices are the ones Welfare Organization provides at reduced cost. In a regional survey on the use of ATs in children with physical disabilities in South Taiwan in 2007, 124 children with disabilities used 224 AT devices. About 90% of those children had AT devices, which included orthotics (62.10%), mobility aids (41.13%), therapy/training devices (16.94%), and AT devices for activities of daily living (2.42%). They modified the ‘nordic classification system on aids for disabled persons’ to classify the assistive devices [12].
In the present study, 47% of the children had an unmet need for assistive devices. The most common unmet need was for shower/bath/toilet chairs, followed by wheelchairs and medical shoes. Note that many parents were unfamiliar with ‘chair for shower/bath/toilet’ before demonstrating the picture of the device as a part of the interview process in the present study. The most prevalent unmet need in Ukraine was for complex products such as orthotics, hearing aids, and wheelchairs [10].
Challenges in using rATA for AT needs assessment in children with disability
Based on the rATA tool, parents were asked about their children’s met and unmet needs for 55 AT devices in the present study. However, only 14 items were used by some children, and some parents reported unmet needs for 30 out of 55 items, and the need for 25 items was not mentioned at all. There may be various reasons for this finding. Some items from the list of 55 AT devices might not be helpful for children. Another reason might be the indistinctness of the name and image of some other devices. For example, “travel aids, portable” is not clear enough, and there is no description of its application and usefulness. In the case of “smartphones/tablets,” parents might not know what software and programs could be installed on them or how the devices could be of use in helping their child with a disability. Some other studies have also mentioned this problem [10]. To overcome this problem of self-reporting needs assessment for AT devices, a solution might be to introduce them by showing pictures and a description of their application and usefulness to parents and children before asking if they need each device. This technique has been successfully used for assessing AT device needs in adolescents with hearing loss [13].
On the other hand, the rATA tool may not detect some of the important needs of people with disabilities. For example, this tool does not include environmental control units /remote controls, while some studies have shown that many people with disabilities need this group of AT devices. Shariatzadeh et al. assessed the rehabilitation needs of 152 people with physical-motor disabilities, aged 16-64, in Kohgiluyeh Province, Iran. They found that the unmet need for electronic devices to control the environment, such as door opening and remote controlling of televisions and air conditioners, was reported by more than 80% of respondents [15]. Additionally, some of the relatively essential needs of children with disabilities may not be detected by the rATA tool. Play and education are children’s two main ways of engagement and social participation, and these engagements are necessary for their development. However, the rATA tool does not focus on these devices, which are especially important in this age group. Therefore, it seems that developing a special version of the rATA tool to assess the AT needs of children with disabilities is necessary.
Conclusion
In this study, none of the children used AT devices for their cognitive problems, and only a few parents who had children with cognitive limitations stated their children’s need for some cognitive ATs. The need to introduce this category of ATs, their applications, and their usefulness should be given special attention as part of programs for increasing the coverage of AT devices.
Almost all parents declared their child’s need for devices that could quickly realize their function from the pictures in the rATA of the device or were commonly used in the community for many years. This issue highlights the need to review and improve the questions for introducing and asking about other less familiar devices.
Finally, as the most prevalent barrier to AT accessibility was financial shortcomings, researching to determine the most efficient and effective strategies to improve financial accessibility can be an essential step in improving the coverage of ATs among children with disabilities.
Study limitations
As many children with disability in this study were under 8 years old or had communication and or cognition limitations, interviews were done by proxy of parents, and the perceived needs of the children might not be similar to those mentioned by their parents. Furthermore, some data collection took place by tele-interview due to COVID-19 prevention measures. This condition may affect the precision of results. It should also be considered that the rATA is an interview-based survey tool that provides an overall estimation of AT needs. It is not intended to substitute the complete AT assessment process, which prescribes appropriate AT for people with disability [7].
Ethical Considerations
Compliance with ethical guidelines
This survey was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1401.018).
Funding
The current study received no financial support from any public, commercial, or non-for-profit organization.
Authors' contributions
Conceptualization: Zahra Satari, Nikta Hatamizadeh and Soheila Shahshahani; Methodology: Nikta Hatamizadeh and Samaneh Hosseinzadeh; Resources and investigation: Zahra Satari; Writing the original draft: Zahra Sattari and Nikta Hatamizadeh; Review and editing: All authors; Supervision: Nikta Hatamizadeh, Soheila Shahshahani and Samaneh Hosseinzadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors hereby express their appreciation to the officials and experts of the Welfare Organization of Chaharmahal and Bakhtiari Province and the children with disabilities and their families whose participation made this research possible.
References
- Olusanya BO, Kancherla V, Shaheen A, Ogbo FA, Davis AC. Global and regional prevalence of disabilities among children and adolescents: Analysis of findings from global health databases. Frontiers in Public Health. 2022; 10:977453. [DOI:10.3389/fpubh.2022.977453] [PMID]
- WHO. Community-based rehabilitation: CBR guidelines. Geneva: WHO; 2010. [Link]
- Rhoads L, Doty M, Seiler R. Assistive technology for school age children with disabilities: A handbook for parents and caregivers. Moscow: University of Idaho; 2007. [Link]
- Barresi J. Technical assistance guide assistive technology for children and youth with disabilities IDEA part B. Oklahoma City: Oklahoma State Department of Education; 2014. [Link]
- Pryor W, Nguyen L, Islam QN, Jalal FA, Marella M. Unmet needs and use of assistive products in two districts of Bangladesh: Findings from a household survey. International Journal of Environmental Research Public Health. 2018; 15(12):2901. [DOI:10.3390/ijerph15122901] [PMID]
- WHO. Global report on assistive technology. Geneva: WHO; 2022. [Link]
- WHO. Measuring need and unmet need for assistive technology the rapid assistive technology assessment (rATA) tool for national representative survey enumeration: A manual. 2019: WHO; [Link]
- WHO. Rapid Assistive Technology Assessment tool (rATA). Geneva: WHO; 2021. [Link]
- Senjam SS, Manna S, Kishore J, Kumar A, Kumar R, Vashist P, et al. Assistive technology usage, unmet needs and barriers to access: A sub-population-based study in India. The Lancet Regional Health - Southeast Asia. 2023; 15:100213.[DOI:10.1016/j.lansea.2023.100213] [PMID]
- WHO. A situation assessment of assistive technology in Ukraine. Geneva: WHO; 2022. [Link]
- Saloojee G, Phohole M, Saloojee H, IJsselmuiden C. Unmet health, welfare and educational needs of disabled children in an impoverished South African peri-urban township. Child: Care, Health and Development. 2007; 33(3):230-5. [DOI:10.1111/j.1365-2214.2006.00645.x] [PMID]
- Hung JW, Wu YH, Wu WC, Leong CP, Lau YC. Regional survey of assistive devices use by children with physical disabilities in southern Taiwan. Chang Gung Medical Journal. 2007; 2007; 30(4):354-62. [PMID]
- Zaman-pour M, Hatami-zadeh N, Vameghi R, Bakhshi E. [Assistive technology needs assessment from adolescent students with hearing loss and their parents, Ahvaz City-2013 (Persian)]. Archives of Rehabilitation. 2015; 15(4):42-51. [Link]
- Coto-Solano B. Measuring access to assistive technology in the public rehabilitation outpatient setting in Costa Rica using the WHO Rapid Assistive Technology Assessment (rATA) Questionnaire. ICCHP-AAATE 2022 Open Access Compendium" Assistive Technology, Accessibility and (e) Inclusion" Part II. 2022. [Link]
- Shariatzadeh, A. [Rehabilitation needs assessment of adults with physical-motor disabilities and prioritizing needs in Kohgiluyeh City (Persian)] [MSc]. Tehran: University of Social Welfare and Rehabilitation Sciences; 2019. [Link]
Article type: Original Research Articles |
Subject:
Social Welfare
Received: 2023/10/30 | Accepted: 2024/01/28 | Published: 2024/12/20
Received: 2023/10/30 | Accepted: 2024/01/28 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
