
988368
Wed, Jul 29, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 21-30 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Momeni A, Hatamizadeh N, Mehrkian S, Hosseinzadeh S. Experiences and Challenges of Educational-audiologists and Tele-rehabilitation During COVID-19. Iranian Rehabilitation Journal 2025; 23 (1) :21-30
URL: http://irj.uswr.ac.ir/article-1-2122-en.html
URL: http://irj.uswr.ac.ir/article-1-2122-en.html



1- Department of Rehabilitation Management, School of Rehabilitation Sciences,University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Clinical Medicine, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Clinical Medicine, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 649 kb]
(745 Downloads)
| Abstract (HTML) (3997 Views)
Full-Text: (550 Views)
Introduction
Hearing loss is one of the most common types of childhood disabilities. Approximately 34 million children with moderate, severe, or profound hearing loss live worldwide [1, 2, 3]. The prevalence rate of hearing loss among children and adolescents aged 3-17 years is 5 per 1000 children. Therefore, children and adolescents with hearing loss need rehabilitation [4]. The prevalence rate of hearing loss is 6 per 1000 among 5-10-year-old children and 19 per 1000 in the 11-20-year-old age group [5]. Providing audiology services can reduce the adverse effects of hearing loss. Educational-audiologists help reduce the academic gap between affected children and their normal-hearing peers. Providing audiology services in schools facilitates the communication of hearing-impaired students with their classmates and teachers and helps them benefit from school programs as much as possible [6].
Tele-audiology has been used in screening, diagnosis, intervention, and assessment of patient perceptions of service delivery to remote communities and to overcome audiology service shortages in different parts of the world for more than 25 years [7]. Feasibility studies on telerehabilitation implementation began before the COVID-19 pandemic in Iran [8]. However, tele-practice to provide rehabilitation services has dramatically increased since the beginning of the COVID-19 pandemic. The necessity for social distancing has caused the closure of many public places, including schools and rehabilitation clinics [9]. The provision of in-person audiology and hearing rehabilitation services for students with hearing loss has been disrupted. Thereafter, the conventional service delivery method was revised, and tele-rehabilitation was increasingly used worldwide, which increased the possibility of continuing rehabilitation services. However, the delivery of such services is challenging. For example, in Malaysia, Rashid et al. used a self-administered questionnaire, indicating that 14 audiologists had a moderate desire to provide tele-rehabilitation services and 22 were not willing to use tele-audiology for cochlear implant mapping and consulting new hearing aid users and primary school-aged children [10]. In another survey conducted in the United Kingdom, Parmar et al. used a self-administered questionnaire with 339 audiologists. Audiologists indicated that tele-audiology was difficult when dealing with patients with mental health difficulties, complex patients, performing diagnostics, pediatrics, mold adjustment, and verification of hearing aid fitting [11].
As the students with hearing loss needed rehabilitation services to improve linguistic skills, academic performance, social interaction, and their potential to learn and reach their educational goals, and as the services were provided in-person before lockdown, it was not known to what extent tele-audiology is used for various types of audiology services’ delivery at schools throughout the country and the degree of difficulty in providing each type of audiological services by this root. This information is crucial in planning rehabilitation provisions for students with hearing loss when barriers do not allow in-person rehabilitation.
Materials and Methods
In this descriptive study, all 62 audiologists working in the Ministry of Education, who were members of the WhatsApp social group of educational-audiologists in the country, were sent the questionnaire and invited to participate. They were asked to complete the questionnaire if they were involved in providing audiological services to students with hearing loss and agreed to participate in the study. Seven audiologists had other duties and positions. They did not provide hearing rehabilitation services at schools and 12 were excluded from the study because they did not agree to participate or did not return the completed questionnaire after receiving reminders three times. A total number of 43 audiologists who met the included criteria completed the questionnaire.
The online questionnaire ended with a question asking if the participants would like to share their experiences on telerehabilitation during lockdown by telephone or video call. Telephone and online interviews were conducted with 11 participants who agreed to participate.
Questionnaire
The self-administered questionnaire used in this study contained questions about personal and work characteristics, changes in service coverage, intensity (frequency) of providing hearing rehabilitation services, method of providing each service “in-person/remotely, online/offline” and the degree of difficulty in providing tele-services during lockdown. The audiological services included otoscopy, audiometry, tympanometry, electrophysiological tests, first-time assessment, and follow-up measurement of the levels of listening and language skills, providing auditory-training exercises, evaluation and adjustment of hearing aids, earmold impression, adjustment of the mold on the ear and tube replacement, following up on the preparation of the mold, checking for hearing aid frequency modulation (FM) system, free-field evaluation of cochlear implant device, child and family counseling and training on hearing aid/cochlear implant care, and informing families about hearing and hearing loss. The questionnaire contained 104 questions, and its face and content validity was confirmed by 13 audiologists with MSc or PhD familiar with providing tele-rehabilitation services experienced in child rehabilitation, professionals, and experts in designing questionnaires and survey studies for comments on the face and content validity. The content validity ratio (CVR) was calculated for all questions using the Lawsche method. After corrections to improve the clarity of questions based on comments and omitting questions with CVR<0.56, the final version of the questionnaire was sent to the 12 audiologists to assess content validity. The content validity index (CVI) of the questionnaire was 0.70. The time required to complete the questionnaire was approximately 20 minutes.
The questions about “service coverage” have three answer options: “This service has not been provided before and during the COVID-19 pandemic; “this service was provided before but not during the pandemic”; “this service has been provided before and continued during the pandemic as well”. The questions about “changes in the number of services provided during the pandemic” had a 7-point Likert scale: “1=same as before,” “2=a little less,” “3=about two-thirds of before,” and “4=almost half of before.” “5=about a third of before,” “6=very little” and “7=insignificant.”
The researchers designed a questionnaire based on a literature review and their experiences. They then sent it to 12 audiologists with an MSc or PhD in child rehabilitation. The questionnaire was provided to the participants based on their preference as a “Google Form” or via email/WhatsApp.
Interview
After collecting the completed questionnaires, the participants who declared their willingness to share their experiences in providing tele-rehabilitation services and expressed their consent to participate in the interview were interviewed via telephone or video calls. Each interview lasted between 20 and 30 minutes. The interviewees were asked to talk about the barriers they faced in providing different services to students remotely and their practical solutions to those barriers, which allowed them to cover students with hearing loss during the school closure.
Data were analyzed using SPSS software, version 26. The data gathered through the questionnaire are summarized in the tables and shown in the figures. The information obtained from the interviews is summarized in a short description.
Results
Most participants (88.4%) were female and 76.7% had a bachelor’s degree. The participants’ work experience was 20.2±6.4 years in audiology and 18±5.5 years in auditory training. While all participants covered 1639 students in 106 special schools in their city, only 8 of them served 57 students with hearing loss in mainstream settings.
Audiological services (tele-rehabilitation and in-person audiology) provided in schools can be classified into two groups.
First: Hearing assessment services using specialized tools
Owing to technological limitations, these services were provided only in-person during the COVID-19 pandemic. Figure 1 shows the number of audiologists providing each service and changes in the number of services provided during the same period.
 As shown in Figure 1, during the lockdown, decrements in the otoscopy (from 95.3% to 67.7%) and audiometric (from 93% to 67.4%) services were higher than other services, and more than a quarter of the audiologists stopped performing these two types of evaluation during this period.
As shown in Figure 1, during the lockdown, decrements in the otoscopy (from 95.3% to 67.7%) and audiometric (from 93% to 67.4%) services were higher than other services, and more than a quarter of the audiologists stopped performing these two types of evaluation during this period.
On average, the number of different services provided by these services decreased to less than half. As shown in Table 1, the decrement amount varied from 4.25 to 6.13 on a 7-point scale,and the standard deviation of the changes was more than 2 points.

Second: Listening, speech and language skills assessment and hearing rehabilitation
Before the pandemic, all educational-audiologists provided these services to students under their coverage. Figure 2 shows how these services continued during the lockdown.
 According to Figure 2, 0-12% of audiologists stopped providing this group of services. Among others, the most common method for providing these services was a combination of tele-practice and in-person services. However, 49% of audiologists did not use tele-practice for listening skills assessment and 38% did not use this speech and language assessment method.
According to Figure 2, 0-12% of audiologists stopped providing this group of services. Among others, the most common method for providing these services was a combination of tele-practice and in-person services. However, 49% of audiologists did not use tele-practice for listening skills assessment and 38% did not use this speech and language assessment method.
Table 2 presents the changes in the number of services provided during the lockdown period.
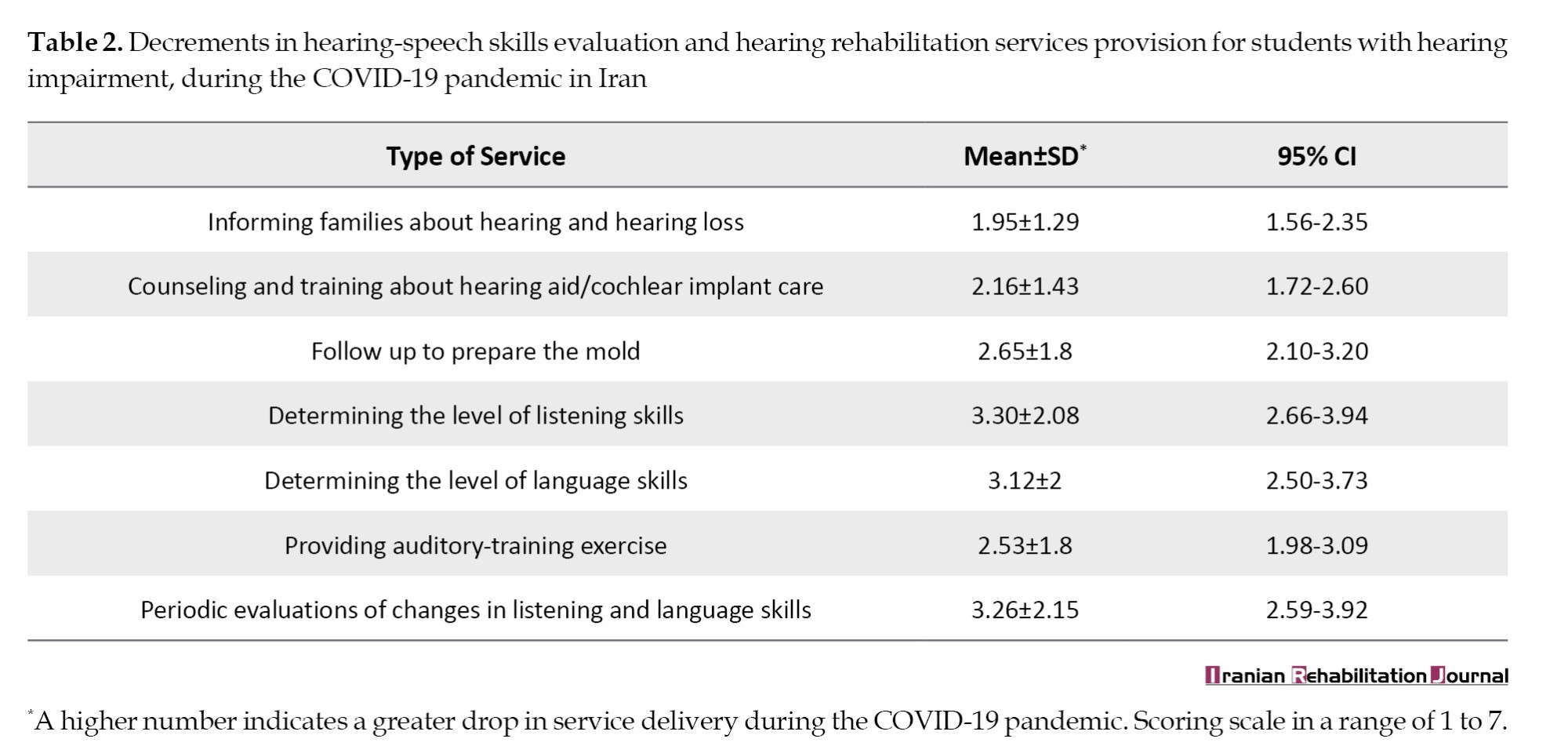
On a 7-point scale, these kinds of services have been reduced by 1.95-3.30 during this period.
Of the 43 participants, 38(88%) stated that, during the pandemic, tele-education and tele-rehabilitation were provided in their schools. Most offline roots (86%) were used for tele-practice. Only one participant reported that the telephone and SMS were the only roots for the education and rehabilitation of the covered students. Audiologists use one or more software packages to communicate with parents. WhatsApp (19 people) and Shad (21 people) were the most commonly used software. Nine participants reported using other software.
Table 3 presents the problems faced by educational audiologists during the COVID-19 pandemic.

Tele-audiology services
Audiologists reported the following strategies to effectively overcome these problems and continue providing tele-rehabilitation services to students with hearing loss.
Solving hearing-aid problems
Telephone or online video calls between mothers or students and the educational audiologist were helpful in hearing-aid problems (such as discontinuity of sound, defects in the mold, or broken hook). The audiologist would see what had happened to the hearing aid through a video call and describe how to fix it to parents and students. During this online communication, some audiologists asked mothers to remove the hearing aid from their children’s ears to check the hearing aid’s sound remotely and train the mother to solve the problem.
If it was necessary to repair the hearing aid, some audiologists used a pick or post to transport it from the student’s home to check and repair it or send it to a repair facility.
Listening skills assessment
To assess listening skills, some audiologists performed an informal assessment by observing the child’s responses to the parents during training exercises with the child in videos they sent to the audiologist.
Teaching and advice to parents
Advice and teaching about how to care for hearing aids/molds or cochlear implants were provided by phone and ‘WhatsApp messenger.’ During the lockdown, some audiologists arranged group counseling for families of students with hearing loss by holding online group meetings at Messenger Shad. Also, they provided families with electronic versions of posters about hearing aids and cochlear implant care. They prepared electronic teaching materials on ear, hearing loss, types of hearing loss, ear diseases, hearing aids, and cochlear implantation in simple language for parents and shared them with families.
Discussion
Although the number of students with hearing loss in regular schools is several times that of those who study in schools for children with special needs, only 57 students in regular schools were covered by the services of the participating educational audiologists. The lack of resources, along with prioritizing policies, caused such different coverage in these two types of schools. If better efficiency of facilities is achieved, better coverage of students with hearing loss in mainstream schools, along with students at schools for children with special needs, may become possible. Although audiological services for children with hearing loss are also available at the community level, providing services at schools helps students maximize their potential in their learning environment. The results of the present study showed that all instrumental audiology assessments were provided in-person during the pandemic, and the number of services provided was reduced to approximately one-third. This result was unsurprising because, according to COVID-19 prevention measures, in-person service provision of less urgent and non-emergent rehabilitation services was postponed until the pandemic subsided. However, technical limitations exist in providing instrumental assessment in tele-practice. For other services, such as evaluation of listening and communication skills and hearing training and consulting, for which in-person and tele-services were used for delivery, a much lower drop in service provision occurred than specialized hearing assessments. On average, during the COVID-19 pandemic, the number of services provided was approximately two-thirds of that provided during the same period before the pandemic. However, a significant difference was observed among educational-audiologists in this regard, which showed a significant standard deviation of 2 points from 0-7 on a 7-point rating scale, indicating significant differences in the changes in the number of services provided. Sharing knowledge, skills, and experience among educational audiologists would help minimize the gap in receiving services among students with hearing loss nationwide.
The results showed that listening and communication skills cannot be easily and precisely evaluated in tele-practice, and only half of the audiologists have ever used this root for evaluation. Therefore, it is mandatory to develop appropriate valid tests to measure children’s listening and communication skills more easily and accurately by tele-practice.
In the present study, 95.3% of audiologists reported not having high-quality audio and camera systems appropriate for online auditory training in primary-school children with hearing loss. Studies in other countries have demonstrated the existence of such problems. Ravi et al. reported a lack of facilities/infrastructure, training, reimbursement, reliability of results, licensure and reduced quality compared to face-to-face interactions in India [12]. In Brazil, Molini-Avejonas et al. identified barriers, such as the need for software information, the speed of the Internet, and technological limitations that limit the use of telehealth in speech, language and hearing sciences [13]. Monica et al. emphasized that the availability of high-speed Internet connections, video equipment and appropriate evaluation tools is vital for providing tele-audiology services [14].
According to the present study, 93% of the audiologists reported that it is challenging to measure listening skills in students with hearing loss at the beginning of their entrance to first-grade school by tele-practice, which is similar to the results of Saunders and Roughley in England [15].
In the current study, 90% of audiologists reported that it was challenging to consult parents about how to fix hearing aid problems through tele-practice. However, this problem caused fewer disturbances in the provision of hearing rehabilitation services than mentioned above. The results of the study by Parmar et al. indicated that during the COVID-19 pandemic in both public and private sectors in England, audiological evaluations of children were considered complex and emphasized that mold modifications cannot be carried out by phone or video [11]. Novak et al. stated that many hearing aid manufacturers include tele-monitoring and adjustment capabilities in their programming software to make adjustments during tele-consultation. They found this method successful and effective in face-to-face counseling of adult patients [16]. However, Muñoz et al. stated that more research is needed to assess this technique in the pediatric population and people with special needs. Remote programming of nucleus cochlear implants for patients aged >12 years is currently approved by the Food and Drug Administration (FDA) in the United States [17]. However, the number of studies on hearing aids and cochlear implantation programming by tele-audiology that include children under 18 years of age is limited, and more research is needed before considering applications of tele-audiology in children [17]. The British Academy of Audiology and Manchester Centre for Audiology and Deafness has produced several “remote working” documents introducing hearing conservation programs (HCPs) to tele-audiology and giving brief practical guidance for hearing assessment and fitting.
In October 2020, the French Society of Audiology published best practice recommendations for “telemedicine in audiology.” The guidance addresses remote consultation conditions for hearing assessment, training of HCPs and specific considerations for assessing and managing pediatric and elderly populations [18].
In the present study, 86% of the audiologists as specialists reported that they did not receive training on performing auditory training through telerehabilitation. This problem caused an almost moderate disturbance in service provision. Rangaswamy and Rao’s study in India showed that 73% of therapists believed that audiologists should have certifications in tele-therapy and that a short training course should be mandatory for audiologists who will provide tele-audiology services [19].
The changes in the number of services provided at similar times by different educational-audiologists in the present study were presumably due to differences in the availability of equipment and infrastructure in different regions of the country and schools. In addition, differences are observed between therapists in terms of motivation and creativity and the different approaches that educational-audiologists adopt to face the crisis of the pandemic shot down. Some audiologists try much more actively and with more creativity than others to overcome the condition and do their best to provide audiological services to children.
Sharing the solutions that some audiologists have successfully used for continuing service provision through tele-rehabilitation along with in-person services could enhance the use of those solutions widely, reduce the differences in service provision between audiologists and provinces, and increase service coverage under similar conditions.
Conclusion
Educational-audiologists acquired valuable experiences in tele-rehabilitation for students with hearing impairment during the COVID-19 pandemic, some of which are documented in the present article. In the presence of resource limitations as a barrier to rehabilitation service coverage for all children in mainstream and unique school settings, especially in distant areas, using these experiences and including tele-services to regular in-person ones would help increase service coverage in schools in distant areas and students with hearing impairment in mainstream settings.
The problems reported in tele-evaluation of hearing skills deserve special attention when designing valid and reliable tele-tests to measure children with hearing loss’s hearing and communication skills of children with hearing loss in providing tele-audiology services.
Limitations
The questionnaire contained 104 questions, all needed to gather relevant data; however, the length of the questionnaire may adversely affect the precision of answers. Also, for practical issues, information about the proportion of services provided as in-person or tele-rehabilitation, and the difference between the number of services provided during and before the pandemic was obtained using an interval scale. The exact number of services was not counted for data collection, resulting in a valuable but rough estimation of hearing rehabilitation services’ provision during the pandemic.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1400.218).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Ashrafsadat Momeni, Nikta Hatamizadeh and Saeideh Mehrkian; Methodology: Nikta Hatamizadeh and Samaneh Hosseinzadeh; Investigation: Ashrafsadat Momeni; Writing the original draft: Ashrafsadat Momeni and Nikta Hatamizadeh; Review and editing: All authors; Resources: Ashrafsadat Momeni; Supervision: Nikta Hatamizadeh, Saeideh Mehrkian, and Samaneh Hosseinzadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the educational-audiologists for sharing valuable information and experiences with the research group.
Hearing loss is one of the most common types of childhood disabilities. Approximately 34 million children with moderate, severe, or profound hearing loss live worldwide [1, 2, 3]. The prevalence rate of hearing loss among children and adolescents aged 3-17 years is 5 per 1000 children. Therefore, children and adolescents with hearing loss need rehabilitation [4]. The prevalence rate of hearing loss is 6 per 1000 among 5-10-year-old children and 19 per 1000 in the 11-20-year-old age group [5]. Providing audiology services can reduce the adverse effects of hearing loss. Educational-audiologists help reduce the academic gap between affected children and their normal-hearing peers. Providing audiology services in schools facilitates the communication of hearing-impaired students with their classmates and teachers and helps them benefit from school programs as much as possible [6].
Tele-audiology has been used in screening, diagnosis, intervention, and assessment of patient perceptions of service delivery to remote communities and to overcome audiology service shortages in different parts of the world for more than 25 years [7]. Feasibility studies on telerehabilitation implementation began before the COVID-19 pandemic in Iran [8]. However, tele-practice to provide rehabilitation services has dramatically increased since the beginning of the COVID-19 pandemic. The necessity for social distancing has caused the closure of many public places, including schools and rehabilitation clinics [9]. The provision of in-person audiology and hearing rehabilitation services for students with hearing loss has been disrupted. Thereafter, the conventional service delivery method was revised, and tele-rehabilitation was increasingly used worldwide, which increased the possibility of continuing rehabilitation services. However, the delivery of such services is challenging. For example, in Malaysia, Rashid et al. used a self-administered questionnaire, indicating that 14 audiologists had a moderate desire to provide tele-rehabilitation services and 22 were not willing to use tele-audiology for cochlear implant mapping and consulting new hearing aid users and primary school-aged children [10]. In another survey conducted in the United Kingdom, Parmar et al. used a self-administered questionnaire with 339 audiologists. Audiologists indicated that tele-audiology was difficult when dealing with patients with mental health difficulties, complex patients, performing diagnostics, pediatrics, mold adjustment, and verification of hearing aid fitting [11].
As the students with hearing loss needed rehabilitation services to improve linguistic skills, academic performance, social interaction, and their potential to learn and reach their educational goals, and as the services were provided in-person before lockdown, it was not known to what extent tele-audiology is used for various types of audiology services’ delivery at schools throughout the country and the degree of difficulty in providing each type of audiological services by this root. This information is crucial in planning rehabilitation provisions for students with hearing loss when barriers do not allow in-person rehabilitation.
Materials and Methods
In this descriptive study, all 62 audiologists working in the Ministry of Education, who were members of the WhatsApp social group of educational-audiologists in the country, were sent the questionnaire and invited to participate. They were asked to complete the questionnaire if they were involved in providing audiological services to students with hearing loss and agreed to participate in the study. Seven audiologists had other duties and positions. They did not provide hearing rehabilitation services at schools and 12 were excluded from the study because they did not agree to participate or did not return the completed questionnaire after receiving reminders three times. A total number of 43 audiologists who met the included criteria completed the questionnaire.
The online questionnaire ended with a question asking if the participants would like to share their experiences on telerehabilitation during lockdown by telephone or video call. Telephone and online interviews were conducted with 11 participants who agreed to participate.
Questionnaire
The self-administered questionnaire used in this study contained questions about personal and work characteristics, changes in service coverage, intensity (frequency) of providing hearing rehabilitation services, method of providing each service “in-person/remotely, online/offline” and the degree of difficulty in providing tele-services during lockdown. The audiological services included otoscopy, audiometry, tympanometry, electrophysiological tests, first-time assessment, and follow-up measurement of the levels of listening and language skills, providing auditory-training exercises, evaluation and adjustment of hearing aids, earmold impression, adjustment of the mold on the ear and tube replacement, following up on the preparation of the mold, checking for hearing aid frequency modulation (FM) system, free-field evaluation of cochlear implant device, child and family counseling and training on hearing aid/cochlear implant care, and informing families about hearing and hearing loss. The questionnaire contained 104 questions, and its face and content validity was confirmed by 13 audiologists with MSc or PhD familiar with providing tele-rehabilitation services experienced in child rehabilitation, professionals, and experts in designing questionnaires and survey studies for comments on the face and content validity. The content validity ratio (CVR) was calculated for all questions using the Lawsche method. After corrections to improve the clarity of questions based on comments and omitting questions with CVR<0.56, the final version of the questionnaire was sent to the 12 audiologists to assess content validity. The content validity index (CVI) of the questionnaire was 0.70. The time required to complete the questionnaire was approximately 20 minutes.
The questions about “service coverage” have three answer options: “This service has not been provided before and during the COVID-19 pandemic; “this service was provided before but not during the pandemic”; “this service has been provided before and continued during the pandemic as well”. The questions about “changes in the number of services provided during the pandemic” had a 7-point Likert scale: “1=same as before,” “2=a little less,” “3=about two-thirds of before,” and “4=almost half of before.” “5=about a third of before,” “6=very little” and “7=insignificant.”
The researchers designed a questionnaire based on a literature review and their experiences. They then sent it to 12 audiologists with an MSc or PhD in child rehabilitation. The questionnaire was provided to the participants based on their preference as a “Google Form” or via email/WhatsApp.
Interview
After collecting the completed questionnaires, the participants who declared their willingness to share their experiences in providing tele-rehabilitation services and expressed their consent to participate in the interview were interviewed via telephone or video calls. Each interview lasted between 20 and 30 minutes. The interviewees were asked to talk about the barriers they faced in providing different services to students remotely and their practical solutions to those barriers, which allowed them to cover students with hearing loss during the school closure.
Data were analyzed using SPSS software, version 26. The data gathered through the questionnaire are summarized in the tables and shown in the figures. The information obtained from the interviews is summarized in a short description.
Results
Most participants (88.4%) were female and 76.7% had a bachelor’s degree. The participants’ work experience was 20.2±6.4 years in audiology and 18±5.5 years in auditory training. While all participants covered 1639 students in 106 special schools in their city, only 8 of them served 57 students with hearing loss in mainstream settings.
Audiological services (tele-rehabilitation and in-person audiology) provided in schools can be classified into two groups.
First: Hearing assessment services using specialized tools
Owing to technological limitations, these services were provided only in-person during the COVID-19 pandemic. Figure 1 shows the number of audiologists providing each service and changes in the number of services provided during the same period.
On average, the number of different services provided by these services decreased to less than half. As shown in Table 1, the decrement amount varied from 4.25 to 6.13 on a 7-point scale,and the standard deviation of the changes was more than 2 points.
Second: Listening, speech and language skills assessment and hearing rehabilitation
Before the pandemic, all educational-audiologists provided these services to students under their coverage. Figure 2 shows how these services continued during the lockdown.
Table 2 presents the changes in the number of services provided during the lockdown period.
On a 7-point scale, these kinds of services have been reduced by 1.95-3.30 during this period.
Of the 43 participants, 38(88%) stated that, during the pandemic, tele-education and tele-rehabilitation were provided in their schools. Most offline roots (86%) were used for tele-practice. Only one participant reported that the telephone and SMS were the only roots for the education and rehabilitation of the covered students. Audiologists use one or more software packages to communicate with parents. WhatsApp (19 people) and Shad (21 people) were the most commonly used software. Nine participants reported using other software.
Table 3 presents the problems faced by educational audiologists during the COVID-19 pandemic.
Tele-audiology services
Audiologists reported the following strategies to effectively overcome these problems and continue providing tele-rehabilitation services to students with hearing loss.
Solving hearing-aid problems
Telephone or online video calls between mothers or students and the educational audiologist were helpful in hearing-aid problems (such as discontinuity of sound, defects in the mold, or broken hook). The audiologist would see what had happened to the hearing aid through a video call and describe how to fix it to parents and students. During this online communication, some audiologists asked mothers to remove the hearing aid from their children’s ears to check the hearing aid’s sound remotely and train the mother to solve the problem.
If it was necessary to repair the hearing aid, some audiologists used a pick or post to transport it from the student’s home to check and repair it or send it to a repair facility.
Listening skills assessment
To assess listening skills, some audiologists performed an informal assessment by observing the child’s responses to the parents during training exercises with the child in videos they sent to the audiologist.
Teaching and advice to parents
Advice and teaching about how to care for hearing aids/molds or cochlear implants were provided by phone and ‘WhatsApp messenger.’ During the lockdown, some audiologists arranged group counseling for families of students with hearing loss by holding online group meetings at Messenger Shad. Also, they provided families with electronic versions of posters about hearing aids and cochlear implant care. They prepared electronic teaching materials on ear, hearing loss, types of hearing loss, ear diseases, hearing aids, and cochlear implantation in simple language for parents and shared them with families.
Discussion
Although the number of students with hearing loss in regular schools is several times that of those who study in schools for children with special needs, only 57 students in regular schools were covered by the services of the participating educational audiologists. The lack of resources, along with prioritizing policies, caused such different coverage in these two types of schools. If better efficiency of facilities is achieved, better coverage of students with hearing loss in mainstream schools, along with students at schools for children with special needs, may become possible. Although audiological services for children with hearing loss are also available at the community level, providing services at schools helps students maximize their potential in their learning environment. The results of the present study showed that all instrumental audiology assessments were provided in-person during the pandemic, and the number of services provided was reduced to approximately one-third. This result was unsurprising because, according to COVID-19 prevention measures, in-person service provision of less urgent and non-emergent rehabilitation services was postponed until the pandemic subsided. However, technical limitations exist in providing instrumental assessment in tele-practice. For other services, such as evaluation of listening and communication skills and hearing training and consulting, for which in-person and tele-services were used for delivery, a much lower drop in service provision occurred than specialized hearing assessments. On average, during the COVID-19 pandemic, the number of services provided was approximately two-thirds of that provided during the same period before the pandemic. However, a significant difference was observed among educational-audiologists in this regard, which showed a significant standard deviation of 2 points from 0-7 on a 7-point rating scale, indicating significant differences in the changes in the number of services provided. Sharing knowledge, skills, and experience among educational audiologists would help minimize the gap in receiving services among students with hearing loss nationwide.
The results showed that listening and communication skills cannot be easily and precisely evaluated in tele-practice, and only half of the audiologists have ever used this root for evaluation. Therefore, it is mandatory to develop appropriate valid tests to measure children’s listening and communication skills more easily and accurately by tele-practice.
In the present study, 95.3% of audiologists reported not having high-quality audio and camera systems appropriate for online auditory training in primary-school children with hearing loss. Studies in other countries have demonstrated the existence of such problems. Ravi et al. reported a lack of facilities/infrastructure, training, reimbursement, reliability of results, licensure and reduced quality compared to face-to-face interactions in India [12]. In Brazil, Molini-Avejonas et al. identified barriers, such as the need for software information, the speed of the Internet, and technological limitations that limit the use of telehealth in speech, language and hearing sciences [13]. Monica et al. emphasized that the availability of high-speed Internet connections, video equipment and appropriate evaluation tools is vital for providing tele-audiology services [14].
According to the present study, 93% of the audiologists reported that it is challenging to measure listening skills in students with hearing loss at the beginning of their entrance to first-grade school by tele-practice, which is similar to the results of Saunders and Roughley in England [15].
In the current study, 90% of audiologists reported that it was challenging to consult parents about how to fix hearing aid problems through tele-practice. However, this problem caused fewer disturbances in the provision of hearing rehabilitation services than mentioned above. The results of the study by Parmar et al. indicated that during the COVID-19 pandemic in both public and private sectors in England, audiological evaluations of children were considered complex and emphasized that mold modifications cannot be carried out by phone or video [11]. Novak et al. stated that many hearing aid manufacturers include tele-monitoring and adjustment capabilities in their programming software to make adjustments during tele-consultation. They found this method successful and effective in face-to-face counseling of adult patients [16]. However, Muñoz et al. stated that more research is needed to assess this technique in the pediatric population and people with special needs. Remote programming of nucleus cochlear implants for patients aged >12 years is currently approved by the Food and Drug Administration (FDA) in the United States [17]. However, the number of studies on hearing aids and cochlear implantation programming by tele-audiology that include children under 18 years of age is limited, and more research is needed before considering applications of tele-audiology in children [17]. The British Academy of Audiology and Manchester Centre for Audiology and Deafness has produced several “remote working” documents introducing hearing conservation programs (HCPs) to tele-audiology and giving brief practical guidance for hearing assessment and fitting.
In October 2020, the French Society of Audiology published best practice recommendations for “telemedicine in audiology.” The guidance addresses remote consultation conditions for hearing assessment, training of HCPs and specific considerations for assessing and managing pediatric and elderly populations [18].
In the present study, 86% of the audiologists as specialists reported that they did not receive training on performing auditory training through telerehabilitation. This problem caused an almost moderate disturbance in service provision. Rangaswamy and Rao’s study in India showed that 73% of therapists believed that audiologists should have certifications in tele-therapy and that a short training course should be mandatory for audiologists who will provide tele-audiology services [19].
The changes in the number of services provided at similar times by different educational-audiologists in the present study were presumably due to differences in the availability of equipment and infrastructure in different regions of the country and schools. In addition, differences are observed between therapists in terms of motivation and creativity and the different approaches that educational-audiologists adopt to face the crisis of the pandemic shot down. Some audiologists try much more actively and with more creativity than others to overcome the condition and do their best to provide audiological services to children.
Sharing the solutions that some audiologists have successfully used for continuing service provision through tele-rehabilitation along with in-person services could enhance the use of those solutions widely, reduce the differences in service provision between audiologists and provinces, and increase service coverage under similar conditions.
Conclusion
Educational-audiologists acquired valuable experiences in tele-rehabilitation for students with hearing impairment during the COVID-19 pandemic, some of which are documented in the present article. In the presence of resource limitations as a barrier to rehabilitation service coverage for all children in mainstream and unique school settings, especially in distant areas, using these experiences and including tele-services to regular in-person ones would help increase service coverage in schools in distant areas and students with hearing impairment in mainstream settings.
The problems reported in tele-evaluation of hearing skills deserve special attention when designing valid and reliable tele-tests to measure children with hearing loss’s hearing and communication skills of children with hearing loss in providing tele-audiology services.
Limitations
The questionnaire contained 104 questions, all needed to gather relevant data; however, the length of the questionnaire may adversely affect the precision of answers. Also, for practical issues, information about the proportion of services provided as in-person or tele-rehabilitation, and the difference between the number of services provided during and before the pandemic was obtained using an interval scale. The exact number of services was not counted for data collection, resulting in a valuable but rough estimation of hearing rehabilitation services’ provision during the pandemic.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1400.218).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Ashrafsadat Momeni, Nikta Hatamizadeh and Saeideh Mehrkian; Methodology: Nikta Hatamizadeh and Samaneh Hosseinzadeh; Investigation: Ashrafsadat Momeni; Writing the original draft: Ashrafsadat Momeni and Nikta Hatamizadeh; Review and editing: All authors; Resources: Ashrafsadat Momeni; Supervision: Nikta Hatamizadeh, Saeideh Mehrkian, and Samaneh Hosseinzadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the educational-audiologists for sharing valuable information and experiences with the research group.
- World Health Organization. Multi-country assessment of national capacity to provide hearing care. Geneva: WHO; 2013. [Link]
- Lynch P, Kaye T, Terlektsi E. Pakistan distance-learning topic brief: Primary-level deaf children. Victoria: EdTech Hub; 2020. [DOI:10.53832/edtechhub.0043]
- Olusanya BO, Newton VE. Global burden of childhood hearing impairment and disease control priorities for developing countries. Lancet. 2007; 369(9569):1314-7. [DOI:10.1016/S0140-6736(07)60602-3] [PMID]
- Subbiah K, Mason CA, Gaffney M, Grosse SD. Progress in documented early identification and intervention for deaf and hard of hearing infants: CDC’s Hearing Screening and Follow-up Survey, United States, 2006-2016. Journal of Early Hearing Detection and Intervention. 2018; 3(2):1-7. [doi:10.26077/6sj1-mw42] [PMID] [PMCID]
- Asghari A, Farhadi M, Daneshi A, Khabazkhoob M, Mohazzab-Torabi S, Jalessi M, et al. The prevalence of hearing impairment by age and gender in a population-based study. Iranian Journal of Public Health. 2017; 46(9):1237-46. [PMID] [PMCID]
- Autry S. An educational audiology model for Mississippi: Telepractice for direct service provision [MA theses]. Mississippi: University of Mississippi; 2020. [Link]
- Swanepoel de W, Hall JW 3rd. A systematic review of telehealth applications in audiology. Telemedicine Journal and E-health. 2010; 16(2):181-200. [DOI:10.1089/tmj.2009.0111] [PMID]
- Movahedazarhouligh S, Vameghi R, Hatamizadeh N, Bakhshi E, Moosavy Khatat SM. Feasibility of telerehabilitation implementation as a novel experience in rehabilitation academic centers and affiliated clinics in Tehran: Assessment of rehabilitation professionals' attitudes. International Journal of Telemedicine and Applications. 2015; 2015:468560. [DOI:10.1155/2015/468560] [PMID]
- Tohidast SA, Mansuri B, Bagheri R, Azimi H. Provision of speech-language pathology services for the treatment of speech and language disorders in children during the COVID-19 pandemic: Problems, concerns, and solutions. International Journal of Pediatric Otorhinolaryngology. 2020; 138:110262. [DOI:10.1016/j.ijporl.2020.110262] [PMID]
- Rashid MFNB, Quar TK, Chong FY, Maamor N. Are we ready for teleaudiology?: Data from Malaysia. Speech, Language and Hearing. 2020; 23(3):146-57. [DOI:10.1080/2050571X.2019.1622827]
- Parmar B, Beukes E, Rajasingam S. The impact of COVID-19 on provision of UK audiology services & on attitudes towards delivery of telehealth services. International Journal of Audiology. 2022; 61(3):228-38. [DOI:10.1080/14992027.2021.1921292] [PMID]
- Ravi R, Gunjawate DR, Yerraguntla K, Driscoll C. Knowledge and perceptions of teleaudiology among audiologists: A systematic review. Journal of Audiology & otology. 2018; 22(3):120-7. [DOI:10.7874/jao.2017.00353] [PMID]
- Molini-Avejonas DR, Rondon-Melo S, Amato CA, Samelli AG. A systematic review of the use of telehealth in speech, language and hearing sciences. Journal of telemedicine and Telecare. 2015; 21(7):367-76. [DOI:10.1177/1357633X15583215] [PMID]
- Monica SD, Ramkumar V, Krumm M, Raman N, Nagarajan R, Venkatesh L. School entry level tele-hearing screening in a town in South India-Lessons learnt. International Journal of Pediatric Otorhinolaryngology. 2017; 92:130-5. [DOI:10.1016/j.ijporl.2016.11.021] [PMID]
- Saunders GH, Roughley A. Audiology in the time of COVID-19: Practices and opinions of audiologists in the UK. International Journal of Audiology. 2021; 60(4):255-62. [DOI:10.1080/14992027.2020.1814432] [PMID]
- Novak RE, Cantu AG, Zappler A, Coco L, Champlin CA, Novak JC. The future of healthcare delivery: IPE/IPP audiology and nursing student/faculty collaboration to deliver hearing aids to vulnerable adults via telehealth. Journal of Nursing & Interprofessional Leadership in Quality & Safety. 2016; 1(1):1-11. [Link]
- Muñoz K, Nagaraj NK, Nichols N. Applied tele-audiology research in clinical practice during the past decade: A scoping review. International Journal of Audiology. 2021; 60(S 1):S4-12. [DOI:10.1080/14992027.2020.1817994] [PMID]
- Thai-Van H, Bakhos D, Bouccara D, Loundon N, Marx M, Mom T, et al. Telemedicine in audiology. Best practice recommendations from the French society of audiology (SFA) and the French society of otorhinolaryngology-head and neck surgery (SFORL). European Annals of Otorhinolaryngology, Head and Neck Diseases. 2021; 138(5):363-75. [DOI:10.1016/j.anorl.2020.10.007] [PMID]
- Rangaswamy Y, & Rao P. Tele speech-language pathology and audiology in India - A short report. Journal of the International Society for Telemedicine and EHealth. 2018; 6(1), e19 (1-8). [Link]
Article type: Original Research Articles |
Subject:
Audiology
Received: 2023/11/1 | Accepted: 2024/05/1 | Published: 2025/03/1
Received: 2023/11/1 | Accepted: 2024/05/1 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
