
988368
Thu, Jul 30, 2026

Volume 23, Issue 2 (June 2025)
Iranian Rehabilitation Journal 2025, 23(2): 201-208 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Vongsirinavarat M, Jitmal R, Nuntapornsak A. The Interrater Reliability of REEDCO Posture Score Among Thai Healthy Adolescents. Iranian Rehabilitation Journal 2025; 23 (2) :201-208
URL: http://irj.uswr.ac.ir/article-1-2132-en.html
URL: http://irj.uswr.ac.ir/article-1-2132-en.html



1- Faculty of Physical Therapy, Mahidol University, Nakhon Pathom, Thailand.
Full-Text [PDF 473 kb]
(817 Downloads)
| Abstract (HTML) (4462 Views)
Full-Text: (1253 Views)
Introduction
With a prevalence of 2-5%, scoliosis has become a major concern for adolescent health. School screening programs are recommended to timely capture the condition, and are routinely practiced as a health prevention protocol in many countries [1]. The SOSORT consensus paper on scoliosis school screening has justified the program to detect even mild and reversible spinal curvatures at an early stage. This would benefit children with adolescent idiopathic scoliosis (AIS) by providing a less invasive method of treatment or surgery [1]. There are recommendations for a standard protocol for using the forward bending test (FBT) and the degrees of axial trunk rotation (ATR) measured with a scoliometer for AIS detection [1, 2]. However, the criteria for testing results have been debated regarding their effectiveness and the threat of over-referral rates [3, 4].
In addition to FBT and ATR, posture assessment is crucial to the screening process. Incorrect posture is defined as deviations of the upright posture that disturb the stability and normal function of tissues and organs [5]. The prevalence of abnormal posture was reported as high as 65.3% in a population-based study of school students in China. Yang et al. [5] proposed a model of “incorrect posture,” including 10 indicators related to changes in the visually inspected body appearance, the FBT, and the ATR for the complete screening process in children and adolescents. They reported a better positive predictive value of 83.8% for identifying AIS patients with a Cobb angle ≥10◦ in a large-scale school scoliosis screening [6]. Thus, an incorrect posture is a feasible and effective identificatory measure for school scoliosis screening in China [6].
Incorrect posture has been indicated to be associated with the risk of developing scoliosis [3, 7, 8]. The shoulder height difference, scapula tilt, lumbar concave, pelvic tilt, flat back, and thoracic kyphosis were significantly higher in children with AIS than in the non-AIS group [9, 10]. Also, abnormal posture can lead to several health problems, such as headaches and pain in the cervical and lumbar spine [3]. Adolescents with poor posture also reported a lower health-related quality of life than those without incorrect posture [11].
Several methods assessed incorrect posture and AIS. Although motion analysis systems and Moiré topography are accurate, they are expensive and limited to use in the community [3]. In general practice, simple observation with specific reference point monitoring is recommended for incorrect posture screening. Designed tools are available to guide clinicians in improving the precision of postural assessments. Examples include the New York posture rating (NYPR), which was the original version of the REEDCO postural scale (RPS) [12], a questionnaire based on functional individual therapy of scoliosis [13], and a postural error chart of 15 body postures [14]. These tools have been reported to have been used by physical therapists (PT) or rehabilitation experts [12-14].
The RPS is a standard tool developed to detect abnormal postures in the frontal and sagittal planes from head to feet. It provides both qualitative and quantitative data. The RPS includes 10 postural characteristics: Head, neck, shoulders, upper back, trunk, abdomen, lower back, spine, hips, and ankles. The quality of posture was scored as 0, 5, and 10 for each item, with a total score of 100. A score of <60 indicates postural dysfunction [12]. The RPS is an inexpensive instrument that is easy to use in the community [15]. Previous studies have demonstrated that the RPS has good intra- and interrater reliability in many populations, such as post-menopausal women with osteoporosis, workers, patients with idiopathic scoliosis, and the elderly [12, 16-18]. However, information on RPS in healthy adolescents remains limited.
School screening has been conducted by several health personnel, including school nurses, physiotherapists, and orthopedic or pediatric physicians [2]. The SOSORT consensus paper on school screening for scoliosis recommended that scoliosis screeners should be individuals who have been trained to perform scoliosis screening by a certified instructor who is a licensed health practitioner [1]. Therefore, non-health professionals could be included in the screening team after training.
To save time and cost, non-health professionals, such as parents or schoolteachers, may perform the initial screening of incorrect postures. However, the consistency of observations of layperson groups has not been reported in the literature. Also, the agreement of postural evaluation between trained health personnel and laypersons should be confirmed. Therefore, this study aimed to investigate the interrater reliability of the RPS assessment between a physiotherapist and a schoolteacher in healthy adolescents. The results of this study can guide the school screening protocol for detecting abnormal postures in adolescents for use in the community.
Materials and Methods
This cross-sectional study investigated the inter-tester reliability of the RPS screening tool in adolescents. The participants were secondary school students aged 10-15 years. The guardians of all participants signed an informed consent before study enrollment. Students with musculoskeletal and neurological conditions that could influence body structure were excluded. The sample size calculation was performed with the following criteria: A two-tailed test with an alpha level of 0.05, a minimal kappa of clinical significance of 0.40, an expected kappa between testers of 0.70, and an expected dropout rate of 5%. The estimated sample size with 80% power was 85.
The assessors in this study were a PT with two years of clinical experience in the musculoskeletal field and a physical education teacher. Both assessors were trained to use the RPS tool before actual data collection. Each item of the tool was explained, and then they tried to assess the students until they could independently and confidently assess posture. The training period took around one hour to complete.
Assessment tool
The RPS assessment tool comprises 10 items divided into assessments in the posterior and lateral views. In the posterior view, five areas are assessed: Head, shoulder level, spine, hip level, and ankle. The lateral view included the neck, upper back, trunk, abdomen, and lower back. The ratings were as follows: 10 (normal position), 5 (slight to moderate deviation from the normal position), and 0 (deviation from the normal line until noticeable). A maximum score of 100 indicates good posture, and a score of less than 60 demonstrates postural dysfunction [12, 19].
Assessment procedure
Demographic data, including sex, age, weight, and height, were recorded by research assistants. During the postural assessment, the participants were required to expose their thoracic and lumbar spine regions in a private room. The male participants removed their shirts, and the female participants rolled up their shirttails and clipped them with a pin. They were barefoot and wore shorts. During the assessment session, the participants were asked to stand habitually on a marked spot located 1 m behind the postural grid and look straight forward. The assessors stood in the same line, 2 m away from the participants, and independently rated the REEDCO. The teacher assessed first, followed by the PT. After both assessors completed the assessment in the posterior view, the participants were asked to turn to the left side to assess the lateral view. All results were recorded in an online form on tablets, and the two assessors were not allowed to discuss the results.
Statistical analysis
SPSS software, version 23 was used for data analysis. Descriptive statistics were applied to the demographic data and each assessor’s rating frequency. The Kappa coefficient and percentage agreement were used to represent interrater reliability. The interpretation of kappa values was as follows: <0.20, slight agreements; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and >0.80, almost perfect agreement [20]. Also, the difference in scoring for each item was analyzed using the chi-square test. An independent sample t test compared the total RPS scores. The significant level was set at P<0.05.
Results
86 participants, 40 males and 46 females, were enrolled in this study. The mean age was 13.36±0.80 years. Table 1 presents the weights, heights, and body mass index (BMI).
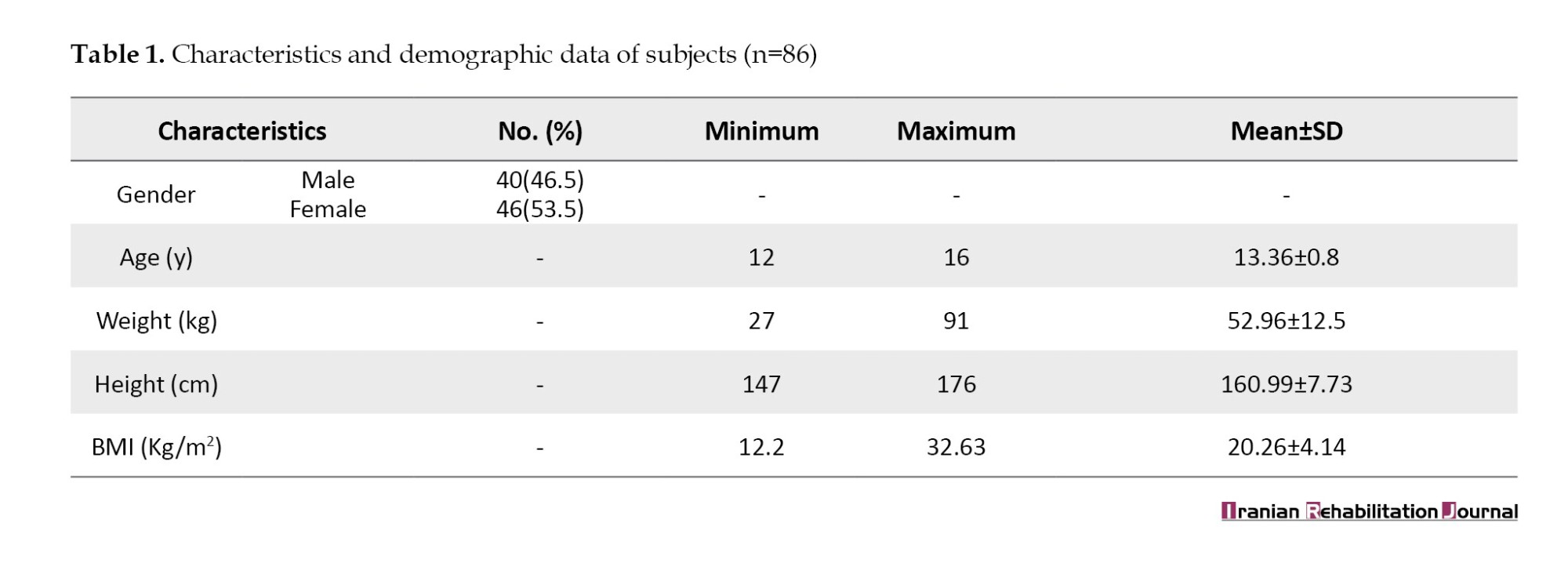
Table 2 presents the interrater reliability of RPS. The kappa coefficients of all assessment items were slight to fair. Furthermore, no significant agreement was observed between testers for the seven items, including the head, shoulders, spine, and hip in the posterior view and the upper back, abdomen, and lower back in the lateral view. The highest percentage agreement was for the head in the posterior view (80.23%), followed by the trunk in the lateral view (73.26%).
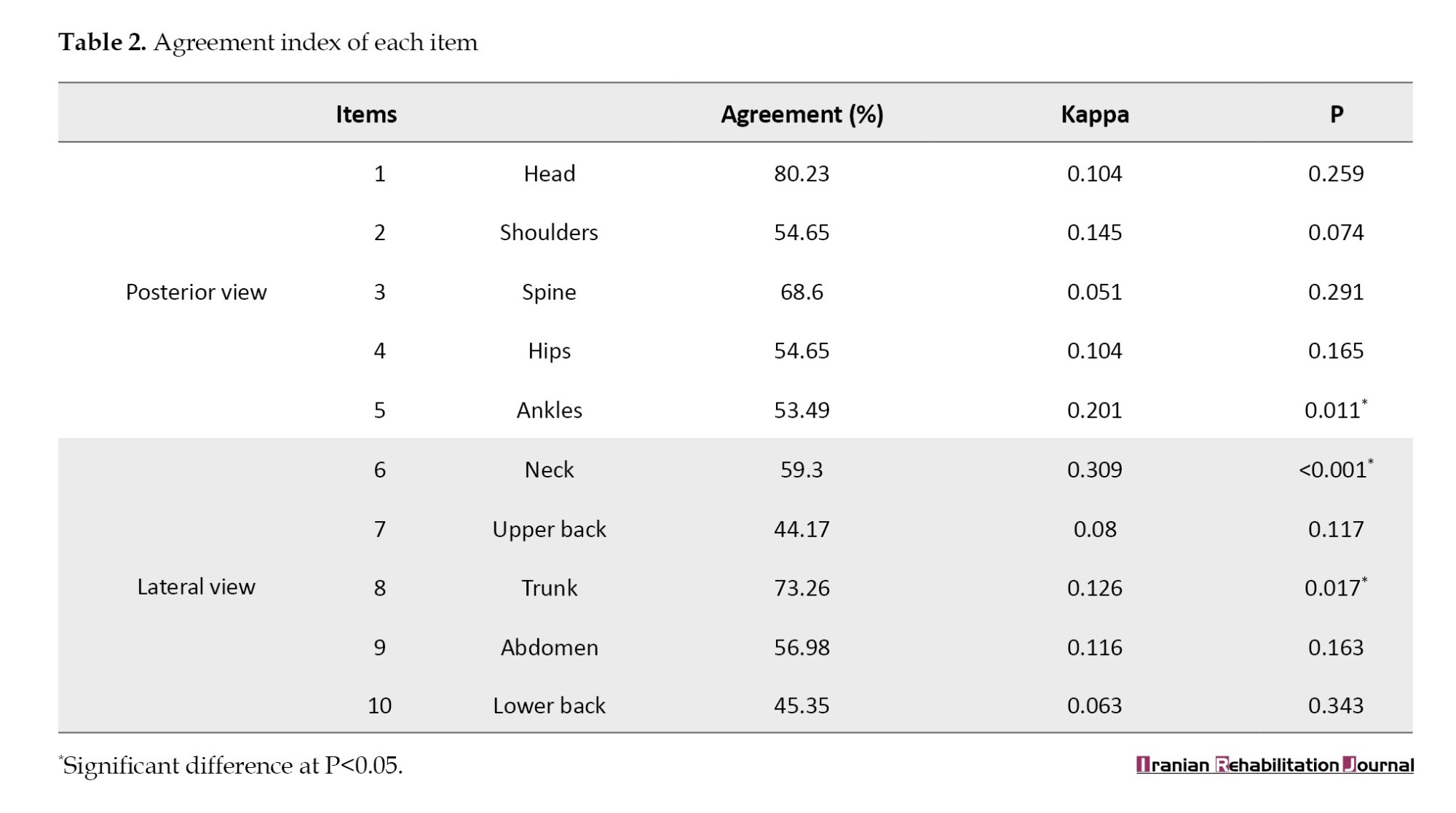
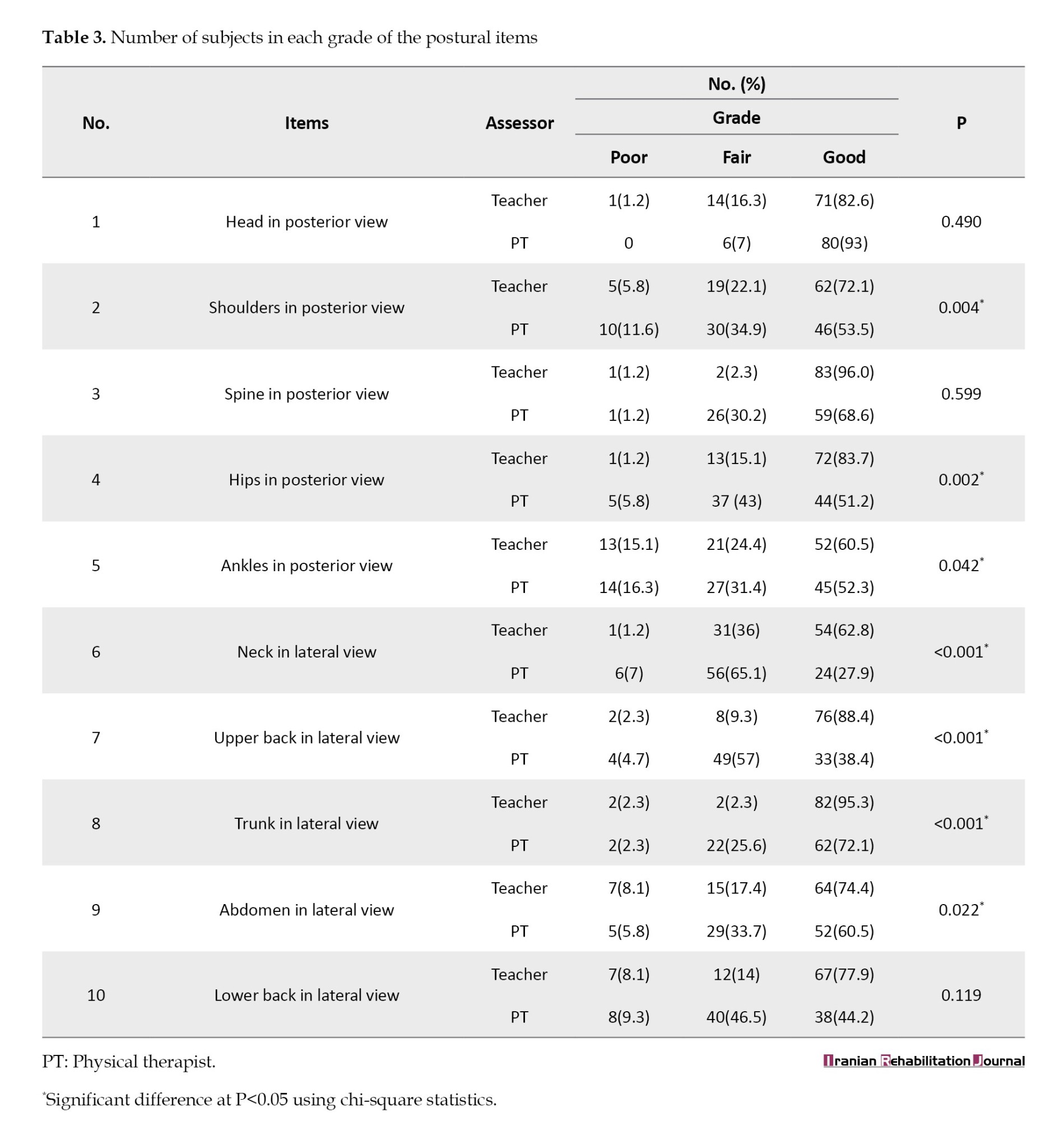
Table 3 compares the grading between the PT and schoolteachers. Significant differences were observed in the grading results between the two assessors for seven items, including the shoulders, hips, and ankles in the posterior view and the neck, upper back, trunk, and abdomen in the lateral view. The apparent trend was that the PT rated these items as good less frequently than the schoolteacher.
Finally, the total RPS score was significantly different between PT and schoolteachers. (P<0.001) The score rated by the schoolteacher (87.38±10.73) was higher than that of a physiotherapist (74.88±11.81).
Discussion
This is the first study to investigate the interrater reliability of the RPS in healthy adolescents. This pilot study evaluated the reliability between trained laypeople (schoolteacher) and health professionals (PT). The interrater reliability, presented as kappa coefficients, between the PT and schoolteacher showed significant agreement, ranging from poor to fair levels for only three out of ten items assessed. The ankles in the posterior view and neck in the lateral view showed a fair agreement. A poor level of agreement was observed for the trunk in the lateral view item. The other seven items, including the shoulders, hips, and ankles in the posterior view and the neck, upper back, trunk, and abdomen in the lateral view, were graded differently between assessors. Furthermore, the total RPS score was significantly different. These results imply that schoolteachers with rapid training might not be the best choice to replace the PT when a postural screening project is run in schools.
Only one previous study reported no significant difference in the total RPS scores among four PTs when rating the posture of five women with osteoporosis [16]. However, one item, the head in posterior view, was rated significantly differently among PTs.
The possible causes of the varied levels of agreement in our study might be mainly due to the different observation skills between the two assessors. Although the teacher in this study was trained to use RPS in practice, he might not have been accustomed to assessing adolescent body alignment. The perspectives on normal posture might also differ between health professionals and laypeople. Therefore, a formal intensive training program is necessary if a teacher is to be assigned as the screening personnel. Grivas et al. suggested a workshop designed to teach the principles and proper technique for the comprehensive steps of scoliosis screening. Assessors must formally attend the workshop and be certified before conducting fieldwork. Also, the assessor must recertify every five years to ensure assessment skills [1]. Because teachers are students’ first point of contact, they might be a good alternative if health professionals are unavailable. Furthermore, many countries demonstrated that school posture screening is beneficial and cost-effective. This policy is useful to decrease or prevent future posture symptoms, such as scoliosis or back pain [6, 21, 22].
Another possible factor that might have affected the results was the assessment sequence. In this study, the schoolteacher performed the assessment before PT without any random ordering. The students may have been fatigued and reformed their standing posture. Therefore, the scoring from the second tester (PT) might decrease since muscle fatigue might induce greater postural asymmetry [23, 24].
This study found poor to fair levels of kappa coefficient, but the percentage agreements between assessors was moderate to high. This could be due to the unequal distribution of subject characteristics. Therefore, the study’s main limitation was the subjects’ characteristics. In future studies, participants with a greater diversity of characteristics should be considered. Also, this study assigned only one PT and one schoolteacher as assessors. The results from only two assessors might be insufficient to summarize and draw conclusions from this assessment process. Additional studies with more assessors would provide more evidence of reliability issues. Furthermore, a validity test of the RPS compared with a standard test, such as a motion analysis system, would be beneficial.
Conclusion
A PT and a schoolteacher showed a poor to fair agreement for posture screening by RPS. Therefore, if schoolteachers are assigned this duty, they must undergo an intensive training course on posture screening. This screening is useful to decrease or prevent future posture symptoms such as scoliosis or back pain.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mahidol University, Nakhon Pathom, Thailand (Code: 2022/142.2912).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, investigation and resources: All authors; Writing the original draft: Rapeepat Jitmal; Supervision, review and editing: Mantana Vongsirinavarat and Amporn Nuntapornsak.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the participants, schoolteachers, and research assistants for their cooperation in this study.
References
With a prevalence of 2-5%, scoliosis has become a major concern for adolescent health. School screening programs are recommended to timely capture the condition, and are routinely practiced as a health prevention protocol in many countries [1]. The SOSORT consensus paper on scoliosis school screening has justified the program to detect even mild and reversible spinal curvatures at an early stage. This would benefit children with adolescent idiopathic scoliosis (AIS) by providing a less invasive method of treatment or surgery [1]. There are recommendations for a standard protocol for using the forward bending test (FBT) and the degrees of axial trunk rotation (ATR) measured with a scoliometer for AIS detection [1, 2]. However, the criteria for testing results have been debated regarding their effectiveness and the threat of over-referral rates [3, 4].
In addition to FBT and ATR, posture assessment is crucial to the screening process. Incorrect posture is defined as deviations of the upright posture that disturb the stability and normal function of tissues and organs [5]. The prevalence of abnormal posture was reported as high as 65.3% in a population-based study of school students in China. Yang et al. [5] proposed a model of “incorrect posture,” including 10 indicators related to changes in the visually inspected body appearance, the FBT, and the ATR for the complete screening process in children and adolescents. They reported a better positive predictive value of 83.8% for identifying AIS patients with a Cobb angle ≥10◦ in a large-scale school scoliosis screening [6]. Thus, an incorrect posture is a feasible and effective identificatory measure for school scoliosis screening in China [6].
Incorrect posture has been indicated to be associated with the risk of developing scoliosis [3, 7, 8]. The shoulder height difference, scapula tilt, lumbar concave, pelvic tilt, flat back, and thoracic kyphosis were significantly higher in children with AIS than in the non-AIS group [9, 10]. Also, abnormal posture can lead to several health problems, such as headaches and pain in the cervical and lumbar spine [3]. Adolescents with poor posture also reported a lower health-related quality of life than those without incorrect posture [11].
Several methods assessed incorrect posture and AIS. Although motion analysis systems and Moiré topography are accurate, they are expensive and limited to use in the community [3]. In general practice, simple observation with specific reference point monitoring is recommended for incorrect posture screening. Designed tools are available to guide clinicians in improving the precision of postural assessments. Examples include the New York posture rating (NYPR), which was the original version of the REEDCO postural scale (RPS) [12], a questionnaire based on functional individual therapy of scoliosis [13], and a postural error chart of 15 body postures [14]. These tools have been reported to have been used by physical therapists (PT) or rehabilitation experts [12-14].
The RPS is a standard tool developed to detect abnormal postures in the frontal and sagittal planes from head to feet. It provides both qualitative and quantitative data. The RPS includes 10 postural characteristics: Head, neck, shoulders, upper back, trunk, abdomen, lower back, spine, hips, and ankles. The quality of posture was scored as 0, 5, and 10 for each item, with a total score of 100. A score of <60 indicates postural dysfunction [12]. The RPS is an inexpensive instrument that is easy to use in the community [15]. Previous studies have demonstrated that the RPS has good intra- and interrater reliability in many populations, such as post-menopausal women with osteoporosis, workers, patients with idiopathic scoliosis, and the elderly [12, 16-18]. However, information on RPS in healthy adolescents remains limited.
School screening has been conducted by several health personnel, including school nurses, physiotherapists, and orthopedic or pediatric physicians [2]. The SOSORT consensus paper on school screening for scoliosis recommended that scoliosis screeners should be individuals who have been trained to perform scoliosis screening by a certified instructor who is a licensed health practitioner [1]. Therefore, non-health professionals could be included in the screening team after training.
To save time and cost, non-health professionals, such as parents or schoolteachers, may perform the initial screening of incorrect postures. However, the consistency of observations of layperson groups has not been reported in the literature. Also, the agreement of postural evaluation between trained health personnel and laypersons should be confirmed. Therefore, this study aimed to investigate the interrater reliability of the RPS assessment between a physiotherapist and a schoolteacher in healthy adolescents. The results of this study can guide the school screening protocol for detecting abnormal postures in adolescents for use in the community.
Materials and Methods
This cross-sectional study investigated the inter-tester reliability of the RPS screening tool in adolescents. The participants were secondary school students aged 10-15 years. The guardians of all participants signed an informed consent before study enrollment. Students with musculoskeletal and neurological conditions that could influence body structure were excluded. The sample size calculation was performed with the following criteria: A two-tailed test with an alpha level of 0.05, a minimal kappa of clinical significance of 0.40, an expected kappa between testers of 0.70, and an expected dropout rate of 5%. The estimated sample size with 80% power was 85.
The assessors in this study were a PT with two years of clinical experience in the musculoskeletal field and a physical education teacher. Both assessors were trained to use the RPS tool before actual data collection. Each item of the tool was explained, and then they tried to assess the students until they could independently and confidently assess posture. The training period took around one hour to complete.
Assessment tool
The RPS assessment tool comprises 10 items divided into assessments in the posterior and lateral views. In the posterior view, five areas are assessed: Head, shoulder level, spine, hip level, and ankle. The lateral view included the neck, upper back, trunk, abdomen, and lower back. The ratings were as follows: 10 (normal position), 5 (slight to moderate deviation from the normal position), and 0 (deviation from the normal line until noticeable). A maximum score of 100 indicates good posture, and a score of less than 60 demonstrates postural dysfunction [12, 19].
Assessment procedure
Demographic data, including sex, age, weight, and height, were recorded by research assistants. During the postural assessment, the participants were required to expose their thoracic and lumbar spine regions in a private room. The male participants removed their shirts, and the female participants rolled up their shirttails and clipped them with a pin. They were barefoot and wore shorts. During the assessment session, the participants were asked to stand habitually on a marked spot located 1 m behind the postural grid and look straight forward. The assessors stood in the same line, 2 m away from the participants, and independently rated the REEDCO. The teacher assessed first, followed by the PT. After both assessors completed the assessment in the posterior view, the participants were asked to turn to the left side to assess the lateral view. All results were recorded in an online form on tablets, and the two assessors were not allowed to discuss the results.
Statistical analysis
SPSS software, version 23 was used for data analysis. Descriptive statistics were applied to the demographic data and each assessor’s rating frequency. The Kappa coefficient and percentage agreement were used to represent interrater reliability. The interpretation of kappa values was as follows: <0.20, slight agreements; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and >0.80, almost perfect agreement [20]. Also, the difference in scoring for each item was analyzed using the chi-square test. An independent sample t test compared the total RPS scores. The significant level was set at P<0.05.
Results
86 participants, 40 males and 46 females, were enrolled in this study. The mean age was 13.36±0.80 years. Table 1 presents the weights, heights, and body mass index (BMI).
Table 2 presents the interrater reliability of RPS. The kappa coefficients of all assessment items were slight to fair. Furthermore, no significant agreement was observed between testers for the seven items, including the head, shoulders, spine, and hip in the posterior view and the upper back, abdomen, and lower back in the lateral view. The highest percentage agreement was for the head in the posterior view (80.23%), followed by the trunk in the lateral view (73.26%).
Table 3 compares the grading between the PT and schoolteachers. Significant differences were observed in the grading results between the two assessors for seven items, including the shoulders, hips, and ankles in the posterior view and the neck, upper back, trunk, and abdomen in the lateral view. The apparent trend was that the PT rated these items as good less frequently than the schoolteacher.
Finally, the total RPS score was significantly different between PT and schoolteachers. (P<0.001) The score rated by the schoolteacher (87.38±10.73) was higher than that of a physiotherapist (74.88±11.81).
Discussion
This is the first study to investigate the interrater reliability of the RPS in healthy adolescents. This pilot study evaluated the reliability between trained laypeople (schoolteacher) and health professionals (PT). The interrater reliability, presented as kappa coefficients, between the PT and schoolteacher showed significant agreement, ranging from poor to fair levels for only three out of ten items assessed. The ankles in the posterior view and neck in the lateral view showed a fair agreement. A poor level of agreement was observed for the trunk in the lateral view item. The other seven items, including the shoulders, hips, and ankles in the posterior view and the neck, upper back, trunk, and abdomen in the lateral view, were graded differently between assessors. Furthermore, the total RPS score was significantly different. These results imply that schoolteachers with rapid training might not be the best choice to replace the PT when a postural screening project is run in schools.
Only one previous study reported no significant difference in the total RPS scores among four PTs when rating the posture of five women with osteoporosis [16]. However, one item, the head in posterior view, was rated significantly differently among PTs.
The possible causes of the varied levels of agreement in our study might be mainly due to the different observation skills between the two assessors. Although the teacher in this study was trained to use RPS in practice, he might not have been accustomed to assessing adolescent body alignment. The perspectives on normal posture might also differ between health professionals and laypeople. Therefore, a formal intensive training program is necessary if a teacher is to be assigned as the screening personnel. Grivas et al. suggested a workshop designed to teach the principles and proper technique for the comprehensive steps of scoliosis screening. Assessors must formally attend the workshop and be certified before conducting fieldwork. Also, the assessor must recertify every five years to ensure assessment skills [1]. Because teachers are students’ first point of contact, they might be a good alternative if health professionals are unavailable. Furthermore, many countries demonstrated that school posture screening is beneficial and cost-effective. This policy is useful to decrease or prevent future posture symptoms, such as scoliosis or back pain [6, 21, 22].
Another possible factor that might have affected the results was the assessment sequence. In this study, the schoolteacher performed the assessment before PT without any random ordering. The students may have been fatigued and reformed their standing posture. Therefore, the scoring from the second tester (PT) might decrease since muscle fatigue might induce greater postural asymmetry [23, 24].
This study found poor to fair levels of kappa coefficient, but the percentage agreements between assessors was moderate to high. This could be due to the unequal distribution of subject characteristics. Therefore, the study’s main limitation was the subjects’ characteristics. In future studies, participants with a greater diversity of characteristics should be considered. Also, this study assigned only one PT and one schoolteacher as assessors. The results from only two assessors might be insufficient to summarize and draw conclusions from this assessment process. Additional studies with more assessors would provide more evidence of reliability issues. Furthermore, a validity test of the RPS compared with a standard test, such as a motion analysis system, would be beneficial.
Conclusion
A PT and a schoolteacher showed a poor to fair agreement for posture screening by RPS. Therefore, if schoolteachers are assigned this duty, they must undergo an intensive training course on posture screening. This screening is useful to decrease or prevent future posture symptoms such as scoliosis or back pain.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mahidol University, Nakhon Pathom, Thailand (Code: 2022/142.2912).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, investigation and resources: All authors; Writing the original draft: Rapeepat Jitmal; Supervision, review and editing: Mantana Vongsirinavarat and Amporn Nuntapornsak.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the participants, schoolteachers, and research assistants for their cooperation in this study.
References
- Grivas TB, Vasiliadis E, Savvidou OD, Triantafyllopoulos G. What a school screening program could contribute in clinical research of idiopathic scoliosis aetiology. Disability and Rehabilitation. 2008; 30(10):752-62. [DOI:10.1080/09638280802041086] [PMID]
- Fong DY, Lee CF, Cheung KM, Cheng JC, Ng BK, Lam TP, et al. A Meta-Analysis of the clinical effectiveness of school scoliosis screening. Spine. 2010; 35(10):1061-71. [PMID]
- Luk KD, Lee CF, Cheung KM, Cheng JC, Ng BK, Lam TP, et al. Clinical effectiveness of school screening for adolescent idiopathic scoliosis: A large population-based retrospective cohort study. Spine. 2010; 35(17):1607-14. [DOI:10.1097/BRS.0b013e3181c7cb8c] [PMID]
- Płaszewski M, Grantham W, Jespersen E. Screening for scoliosis - New recommendations, old dilemmas, no straight solutions. World Journal of Orthopedics. 2020; 11(9), 364-379. [DOI:10.5312/wjo.v11.i9.364] [PMID]
- Yang L, Lu X, Yan B, Huang Y. Prevalence of incorrect posture among children and adolescents: Finding from a large population-based study in China. iScience. 2020; 23(5):101043. [DOI:10.1016/j.isci.2020.101043] [PMID]
- Yan B, Lu X, Nie G, Huang Y. China urgently needs a nationwide scoliosis screening system. Acta Paediatrica. 2020; 109(11):2416-7. [DOI:10.1111/apa.15326] [PMID]
- Nissinen M, Heliövaara M, Seitsamo J, Poussa M. Trunk asymmetry, posture, growth, and risk of scoliosis. A three-year follow-up of Finnish prepubertal school children. Spine. 1993; 18(1):8-13. [DOI:10.1097/00007632-199301000-00002] [PMID]
- Nault ML, Allard P, Hinse S, Le Blanc R, Caron O, Labelle H, Sadeghi H. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine. 2002; 27(17):1911-7. [DOI:10.1097/00007632-200209010-00018] [PMID]
- Raso VJ, Lou E, Hill DL, Mahood JK, Moreau MJ, Durdle NG. Trunk distortion in adolescent idiopathic scoliosis. Journal of Pediatric Orthopedics. 1998; 18(2):222-6. [DOI:10.1097/01241398-199803000-00017] [PMID]
- Yan B, Lu X, Qiu Q, Nie G, Huang Y. Association between incorrect posture and adolescent idiopathic scoliosis among Chinese Adolescents: Findings from a large-scale population-based study. Frontiers in Pediatrics. 2020; 8:548. [DOI:10.3389/fped.2020.00548] [PMID]
- Biernat M, Bąk-Sosnowska M. The impact of body posture on self-image and psychosocial functioning during adolescence. Paediatrics and Family Medicine. 2018, 14(3):282-5. [DOI:10.15557/PiMR.2018.0031]
- McRoberts LB, Cloud RM, Black CM. Evaluation of the New York posture rating chart for assessing changes in postural alignment in a garment study. Clothing and Textiles Research Journal. 2013; 31(2):81-96. [DOI:10.1177/0887302X13480558]
- Baranowska A, Sierakowska M, Owczarczuk A, Olejnik BJ, Lankau A, Baranowski P. An analysis of the risk factors for postural defects among early school-aged children. Journal of Clinical Medicine. 2023; 12(14):4621. [DOI:10.3390/jcm12144621] [PMID]
- Maciałczyk-Paprocka K, Stawińska-Witoszyńska B, Kotwicki T, Sowińska A, Krzyżaniak A, Walkowiak J, et al. Prevalence of incorrect body posture in children and adolescents with overweight and obesity. European Journal of Pediatrics. 2017; 176(5):563-72. [DOI:10.1007/s00431-017-2873-4] [PMID]
- Thawinchai N, Funprom K. Effect of carrying style on posture score in adolescents with musculoskeletal pain. Chiang Mai University Journal of Natural Science. 2019; 18(4):553-61. [DOI:10.12982/CMUJNS.2019.0036]
- Gunther J, Kolodziej T, Bish C, Tiberi J. Test-retest and intertester reliability of two postural measures in post-menopausal women with osteoporosis. Journal of Geriatric Physical Therapy. 2005; 28(3):122. [DOI:10.1519/00139143-200512000-00044]
- Roman GA, Samar V. Workstation ergonomics improves posture and reduces musculoskeletal pain in video interpreters. Journal of Interpretation. 2015; 24(1):7. [Link]
- Wannakon T, Sriboonreung T, Thawinchai N, Pathumasut S, Peungsuwan P. Comparison of Postural Score Between Standing and Sitting in Female Adolescents with Idiopathic Scoliosis. 2020; 42(3):136-46. [Link]
- O'Neil MB, Woodard M, Sosa V, Hunter L, Mulrow CD, Gerety MB, et al. Physical therapy assessment and treatment protocol for nursing home residents. Physical Therapy. 1992; 72(8):596-604. [DOI:10.1093/ptj/72.8.596] [PMID]
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33(1):159-74. [DOI:10.2307/2529310] [PMID]
- Dunn J, Henrikson NB, Morrison CC, Blasi PR, Nguyen M, Lin JS. Screening for adolescent idiopathic scoliosis: Evidence report and systematic review for the US preventive services task force. JAMA. 2018; 319(2):173-87. [DOI:10.1001/jama.2017.11669] [PMID]
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders. 2018; 13:3.[DOI:10.1186/s13013-017-0145-8] [PMID]
- Schieppati M, Nardone A, Schmid M. Neck muscle fatigue affects postural control in man. Neuroscience. 2003; 121(2):277-85. [DOI:10.1016/s0306-4522(03)00439-1] [PMID]
- Penedo T, Polastri PF, Rodrigues ST, Santinelli FB, Costa EC, Imaizumi LFI, et al. Motor strategy during postural control is not muscle fatigue joint-dependent, but muscle fatigue increases postural asymmetry. Plos One. 2021;16(2): e0247395. [DOI:10.1371/journal.pone.0247395] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2023/11/12 | Accepted: 2024/02/17 | Published: 2025/06/1
Received: 2023/11/12 | Accepted: 2024/02/17 | Published: 2025/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
