
988368
Sun, Dec 7, 2025

Volume 22, Issue 1 (March 2024)
Iranian Rehabilitation Journal 2024, 22(1): 117-128 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Malih Radhi M, Zair Balat K. Health Literacy and Its Association With Medication Adherence in Patients With Hypertension: A Mediating Role of Social Support. Iranian Rehabilitation Journal 2024; 22 (1) :117-128
URL: http://irj.uswr.ac.ir/article-1-2146-en.html
URL: http://irj.uswr.ac.ir/article-1-2146-en.html



1- Department of Community Health, College of Health and Medical Technologies/Kufa, Al-Furat Al-Awsat Technical University, Babylon, Iraq.
2- Department of Community Health Nursing, College of Nursing, University of ThiQar, Thi-Qar, Iraq.
2- Department of Community Health Nursing, College of Nursing, University of ThiQar, Thi-Qar, Iraq.
Full-Text [PDF 588 kb]
(1569 Downloads)
| Abstract (HTML) (3101 Views)
Full-Text: (1728 Views)
Introduction
Hypertension, one of the most common chronic conditions, plays a significant role in global cardiovascular and public health mortality [1]. Several studies suggest that a variety of risk factors may exacerbate hypertension, increasing the risk of strokes, heart attacks, and kidney failure. Some risk factors are unchangeable, such as gender, age, and family history [2]. However, certain modifiable risk factors include smoking, poor dietary habits, excessive alcohol consumption, physical inactivity, obesity, high cholesterol levels, and diabetes [3]. The disease pattern in Iraq, as well as in other countries in the region, has shifted due to the rising incidence of non-communicable diseases. The most common cause of death in Iraq, according to national data registries, is still cardiovascular illnesses. According to statistics, it accounts for up to half of all sickness cases and one-third of all fatalities [4]. The nationwide diabetes and hypertension screening program was progressively extended to all primary healthcare facilities, including all 100 of Iraq’s health directorates, beginning in 2008. The screening system identified 860,000 cases of high blood pressure between the project’s initiation and 2017, with 150,000 cases confirmed [4]. Every human being has the fundamental right to health, and obtaining health requires having a suitable level of health knowledge and comprehension [5]. In many regions of the world, people struggle with health literacy because they cannot properly comprehend health information or follow treatment recommendations. This can exacerbate health issues in individuals with chronic illnesses, leading to a worsening of their conditions [6]. Social support appears to be a crucial factor in enhancing health literacy and improving medication adherence rates in such situations [7]. Patients with a strong social support system are better equipped to follow their treatment plans and develop skills related to health literacy [8]. Additionally, social support can provide guidance and educate patients, encouraging their active participation in self-care [9, 10]. One of the chronic illnesses for which a patient’s health depends on ongoing adherence to therapy is hypertension. The rise in these chronic illnesses necessitates a solid grasp of health and the capacity to successfully engage with health information. People with these diseases face significant challenges when it comes to health literacy [11]. “Health illiteracy” refers to the inability to understand and use health knowledge to make informed decisions about one’s health [12]. In many Iraqi communities, a lack of health literacy can exacerbate chronic illnesses, lead to injuries, and result in delays in receiving essential medical care. Individuals with long-term conditions like hypertension require close monitoring and must adhere to their doctor’s instructions and prescription schedules consistently [13]. The goal of science and research should be to comprehend health literacy and how it affects hypertension patients’ adherence to their medication. People with low health literacy may be more likely to forget to take their medications on time or misinterpret health instructions, which can worsen their condition and place additional strain on the healthcare system [14, 15]. Social support is a crucial component that can assist patients with low health literacy in improving their medication adherence. Social support from friends, family, and the local community can significantly enhance adherence to medication and healthy behaviors. Those who are more health literate can better absorb health information when they have the support of their social network [10].
The importance of medication adherence for individuals with hypertension cannot be overstated, since it is crucial for the management and control of this chronic condition. Hypertension is one of the main risk factors for cardiovascular diseases, such as heart attacks and strokes. Regular follow-up consultations with nurses, lifestyle modifications, and continuous adherence to prescribed drug regimens are crucial for the management of hypertension [16]. Patients who disregard their prescriptions face the danger of experiencing the negative effects of high blood pressure, which include damage to vital organs, such as the heart, kidneys, and blood vessels. Additionally, uncontrolled hypertension increases the cost of hospital and primary care treatments, which puts an additional burden on the healthcare system [16]. In order to better understand the relationship between medication adherence and health literacy in patients with hypertension, this study assessed the role that social support plays as a mediating factor in this relationship. We looked at the factors that influence medication adherence and how social support can help patients stick to their treatment plans and stay healthier overall.
Materials and Methods
Study design
This study followed the descriptive cross-sectional design since it is the best suitable method to accomplish its goals.
Study sample
A total of 450 participants with a diagnosis of hypertension who visited primary healthcare facilities in the Babylon Governorate were chosen as a non-probability convenience sample. Given that 25% of the research population has high blood pressure and because 1,803 visits to those health centers were made in a given month, this sample was chosen in part because of these factors.
The 25% of the study population is represented by selecting a quarter of the monthly visits for patients with hypertension.
Study tools
A questionnaire was utilized as the research tool, focusing on investigating the social and demographic characteristics of the individuals in the research sample. These characteristics encompassed various aspects such as age, gender, educational level, monthly income, occupation, and duration of hypertension. Specific metrics were employed in this study to analyze the collected data and information, including:
The Morisky medication adherence scale (MMAS-8), which comprises eight items and its Arabic version has been validated, was used to measure adherence to antihypertensive drugs [17]. In our study, its Cronbach’s α was 0.87, showing strong reliability in this particular setting.
The social support rating scale (SSRS) was used to assess patients’ social support, and its Arabic version has been validated [18]. This scale’s Cronbach’s α in this study was 0.79, indicating a satisfactory level of reliability.
Health literacy was assessed using the health literacy management scale (HeLMS), which was developed by Jordan et al. [19] and its Arabic version has been validated [20]. The scale’s Cronbach’s α in this study was 0.87, indicating improved reliability.
Validity and reliability
Experts in the field of nursing evaluated the questionnaire for validity, and a pilot study was carried out on 20% of the research population to assess the instrument’s reliability. The researcher asked the participants to fill out a questionnaire with their comments in order to participate in the study after introducing themselves to them when they visited the primary health care centers. Subsequently, the investigator elucidated the study’s goals and title in order to assess the comprehensibility and simplicity of reading the questionnaire’s contents. The estimated time for completing each form was 20 minutes, and the pilot study was excluded from the sample without modification following data analysis. The study scales’ intraclass correlation coefficient (ICC) was 0.86, which denotes strong stability.
Data collection
The actual data collection process spanned nearly a month, during which the researchers conducted individual interviews with each study participant at primary healthcare facilities.
These interviews involved explaining the study’s objectives and obtaining verbal consent from each participant. Patients who met specific criteria, including having a hypertension diagnosis for more than six months and providing voluntary consent, were interviewed to gather information. The confidentiality of collected data and the privacy of participants were rigorously maintained. Participants were under no obligation to continue or discontinue their participation at any point in the study.
Statistical analysis
All statistical analyses were performed using SPSS software, version 20. Numeric values and percentages were used to rank the variables, while Mean±SD were employed to provide statistical descriptions of continuous variables. A straightforward linear regression test was employed to evaluate the hypothesis of the relationship between the study’s variables. The distribution of data was assessed using two common techniques: The Kolmogorov-Smirnov and Shapiro-Wilk tests. Additionally, the Mann-Whitney U and Kruskal-Wallis H tests were performed to assess any statistical differences between the groups. A significance threshold of 0.05 was applied.
Results
The mean age of participants was 47.61±14.84 years, with ages ranging from 22 to 74 years. Regarding gender, hypertension was more prevalent among females (54.7%) followed by males (45.3%). Concerning marital status, the majority were married (48.7%) and concerning education level, more than half of the studied sample had completed primary school (59.3%). Approximately one-third of the study sample did not have enough monthly income (65.8%). In terms of the duration of the disease, 53.8% were diagnosed with hypertension for less than one year.
The results in Table 1 revealed the socio-demographic characteristics of the participants in which the mean age was 47.61±14.84 years and ages ranged from 22 to 74 years. Relevant words for this essay may appear in purple. With respect to gender, hypertension was more common among females (54.7%) and the rest were males (45.3%). On the status on marital the married ones were majorities (48.7%). The related findings on education level, the majority of the studied sample were primary school graduates (59.3%). One-third of the respondents (65.8%) had low monthly income. With regard to duration of disease, (53.8%) were diagnosed with hypertension for less than one year.

Table 2 displays that 75.6% of patients with hypertension had low drug adherence. Additionally, 74.9% of hypertension patients reported receiving little social support, while 67.8% of these patients reported being highly illiterate in terms of health. The data given in Table 2 demonstrate the poor medication adherence rate (75.6 %) among patients with hypertension.
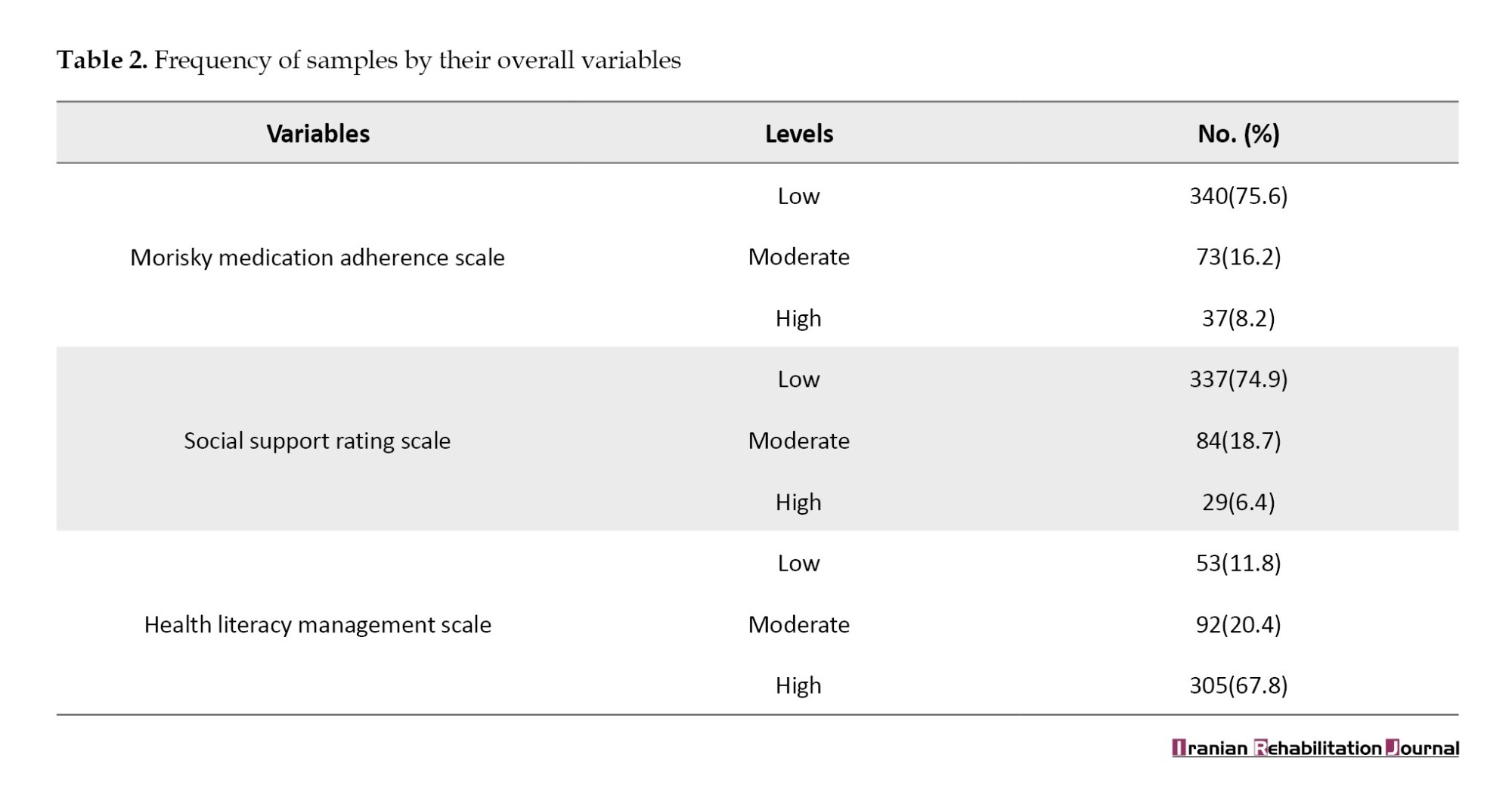
Further, social support provided to patients with hypertension was also low (74.9%). In addition, health literacy in patients with hypertension was recorded a high level (67.8%) (Figure s 1 and 2).
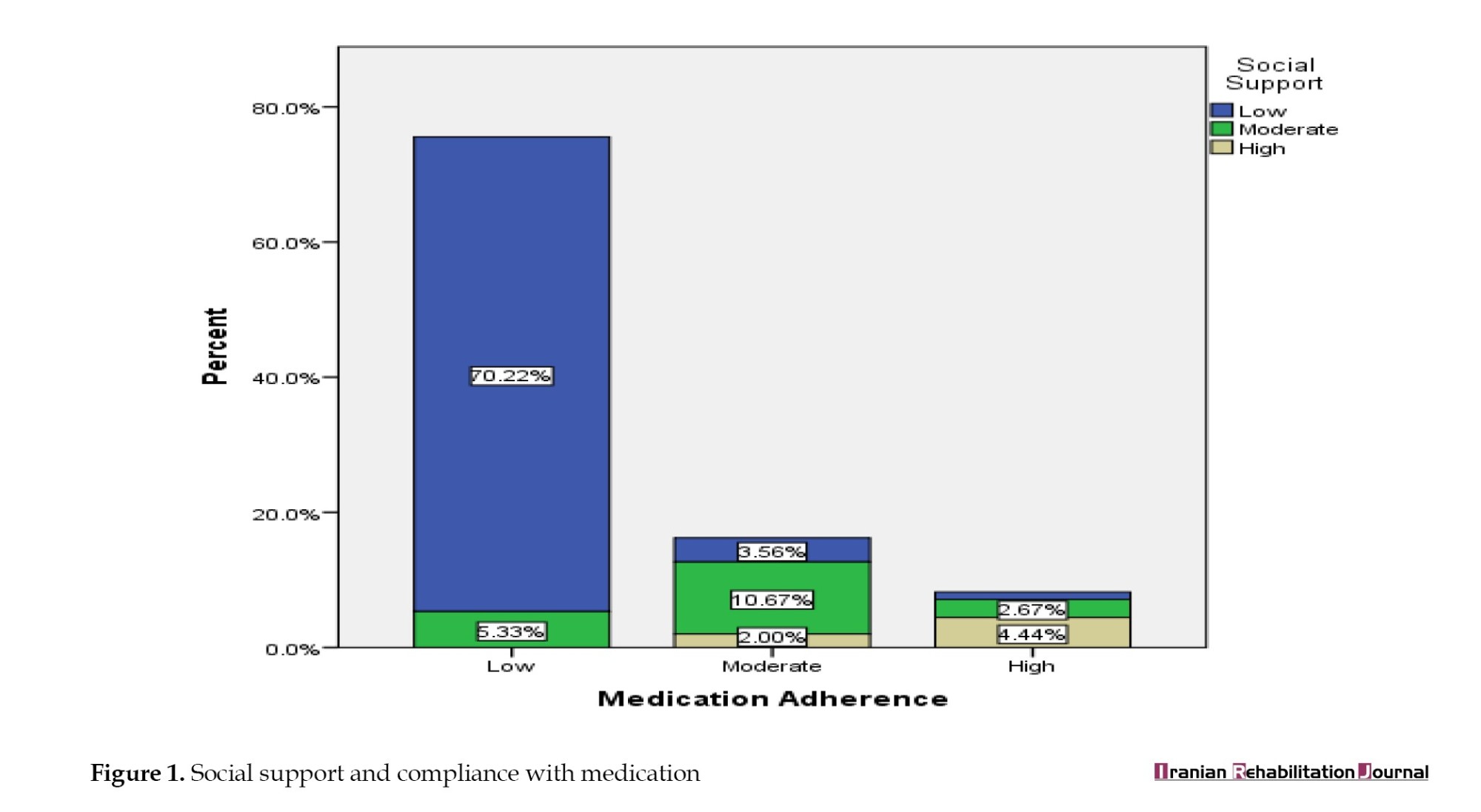

Table 3 presents the findings from a simple linear regression statistical analysis indicating that the degree of health education (β=-0.708; P=0.001) and the existence of social support (β=0.220; P=0.001) are predictive factors for medication adherence in hypertension patients.

According to Table 4, there were statistically significant differences in medication adherence among hypertensive patients based on their gender, marital status, education level, monthly income, and duration of hypertension (P=0.001 for all variables).

Discussion
Medication adherence is a crucial aspect of managing and treating hypertension, as it plays a vital role in maintaining cardiovascular health. Patients with hypertension experience elevated blood pressure in their arteries, which can have significant adverse effects on their well-being and increase the risk of cardiovascular diseases. It is imperative to emphasize to patients the importance of improving medication compliance, as treating hypertension with medication helps stabilize blood pressure, thereby reducing the risk of cardiovascular diseases.
According to the study’s findings, 75.6% of participants had low medication adherence, indicating that medication adherence is highly suboptimal among hypertension patients. This is concerning since there is a connection between a higher risk of cardiovascular disease and its complications with non-adherence to antihypertensive treatment [21]. Inadequate medication adherence has consequences that extend beyond individual health outcomes and affect the overall cost burden of hypertension on public health systems. Enhancing medication adherence is a primary goal of interventions aimed at reducing the potential consequences of poorly controlled hypertension.
These findings are in line with those of the Al-Khobar study and lower than those of the Saudi Arabian study [22, 23]. Discrepancies in adherence rates could be attributed to variations in healthcare systems, demographics, and tools used to measure medication adherence.
The study highlights the low levels of medication adherence rates and inadequate social support received by people with hypertension, with 74.9% reporting low levels. People with chronic illnesses need social support for self-care since it affects their motivation and ability to adhere to prescribed medication schedules and other healthy behaviors [24]. The low levels of social support reported by patients underscore the necessity for nurses and the community to offer interventions aimed at strengthening social support networks for individuals with hypertension. Some potential tactics include educational programs that inform friends and family about the illness, how to support it, and why it is crucial. These findings are in line with studies conducted in the Iraqi province of Babylon, which revealed that most patients with chronic conditions and illnesses needing rehabilitation do not obtain the necessary level of social assistance [10].
Additionally, the study sheds light on the issue of health illiteracy among hypertension patients, as 67.8% of them exhibited high levels of this knowledge deficit. Health literacy is a critical component when it comes to helping individuals with hypertension comprehend medical information, make essential decisions regarding medication adherence, and navigate healthcare systems successfully [25]. Insufficient health literacy can hinder the effective management of hypertension, leading to inadequate self-care practices and deteriorating overall health. Addressing health literacy through targeted educational initiatives and readily available health communication resources is essential for enabling individuals with hypertension to make informed decisions about their health and medication adherence.
The research emphasizes the various difficulties that people with hypertension encounter, such as poor medication compliance, insufficient social support, and elevated levels of health literacy. These results highlight the necessity of all-encompassing interventions that deal with the disease’s social, educational, and health-related aspects. Medication adherence among hypertensive patients should be encouraged through social support interventions provided by health care facilities (nurses), and increasing health literacy is crucial to improving patient outcomes and lowering the overall burden of hypertension on public health.
Social support vs medications adherence
Research has shown that social support is crucial for promoting medication compliance in individuals with long-term hypertension. The positive beta value (β=0.220) indicates a direct correlation between social support and medication adherence. This suggests that patients with high levels of social support networks are more likely to adhere to their prescribed medication regimens with a 0.220 increase in adherence for each incremental rise in social support. These findings demonstrate the extent to which emotional and practical support has a favorable impact on adherence habits, supporting the idea that social support is important in the management of chronic illnesses [26]. Additionally, social cognition theory, which holds that people learn by seeing and interacting with others, has supported the impact of social networks on behaviors related to health [27]. In the context of medication adherence, this may involve sharing experiences, acting as reminders, or providing assistance with medication administration in a socially supportive environment.
Health literacy vs medication adherence
The negative beta coefficient (β=-0.708) of health literacy indicates a negative relationship between health literacy and adherence to medication prescribed for hypertension patients. This suggests that for every unit improvement in health literacy, patients with hypertension have a 0.708-fold decrease in drug adherence. This finding is consistent with other studies emphasizing the significance of health literacy in understanding and applying medical guidance for chronic illnesses [28, 16]. Understanding and adhering to prescription instructions, possible side effects, and the significance of following pharmaceutical guidelines might be significantly hampered by high level of health literacy [29]. Patients with hypertension may find it challenging to absorb complicated medical information, which can result in misinterpretations and a disregard for recommended treatment plans. Therefore, it is critical to suggest initiatives aimed at enhancing health literacy in order to promote chronic condition medication adherence, including hypertension [30].
Differences in medication adherence according to patients’ characteristics
The results demonstrated that there were statistically gender-based differences in hypertension patients’ adherence to their medications (P=0.001). The results showed that males followed their hypertension treatment plans more religiously than women did. These findings are consistent with those of Radhi et al. [16]. Gender differences in adherence underscore the importance of developing intervention strategies that consider gender differences to address specific medication management needs.
Marital status can also influence medication adherence in patients with hypertension. The results showed a significant difference (P=0.000) in medication adherence levels between married patients and their single, divorced, and widowed counterparts. This observation can be attributed to the concept that shared responsibilities, spousal (social) support, and a more stable social environment positively impact the adherence of married individuals to their prescription regimens [31].
Another remarkable finding among the key factors affecting medication adherence in patients with hypertension is educational attainment. The results demonstrated that patients with different educational backgrounds adhere to treatment at significantly different rates (P=0.000), with college graduates adhering to treatment at the greatest rates. This underscores the critical role of health literacy. These differences may be explained by the fact that individuals with higher education levels may possess greater health awareness, understand the importance of following hypertension medication regimens, and have better relationships with community health nurses [32].
According to statistical analysis, patients with higher (sufficient) monthly incomes exhibited better medication adherence (P=0.001). This indicates a significant difference in adherence levels based on monthly income. Increased monthly income may facilitate more consistent adherence to blood pressure medication, underscoring the importance of targeted interventions for patients with lower incomes to address potential barriers to following their prescription drug regimens as prescribed [16].
The study results indicated statistically significant differences (P=0.001) in medication adherence levels based on the length of hypertension. These differences favored individuals with longer histories of hypertension, who demonstrated higher medication adherence than those with shorter durations. This observation suggests that individuals with a longer history of hypertension may have developed stronger medication adherence habits or possess a heightened awareness of the importance of consistent care [33].
Conclusion
The study’s striking finding is that individuals with hypertension exhibit low medication adherence, limited social support, and a high level of health illiteracy. Among the predictive factors for medication adherence, health literacy, and social support emerge as significant contributors. The complexity of this issue is underscored by the significance of variables such as patients’ gender, marital status, educational attainment, monthly income, and duration of hypertension. To address these concerns, interventions by community health nurses should prioritize strengthening patients’ social support networks and enhancing their health literacy levels.
Study limitation
Many patients declined to participate in the study due to time constraints, unwillingness, or lack of interest in the research. Additionally, the extensive questionnaire and large sample size made data collection a labor-intensive process.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Al-Awsat Technical University (No.: 713, dated 3/11/2023).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and data analysis: Mohammed Malih Radhi; Data collection, writing and supervision: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their thanks and gratitude to the Babylon Health Directorate for facilitating data collection, as well as to Al-Furat Al-Awsat Technical University.
References
Hypertension, one of the most common chronic conditions, plays a significant role in global cardiovascular and public health mortality [1]. Several studies suggest that a variety of risk factors may exacerbate hypertension, increasing the risk of strokes, heart attacks, and kidney failure. Some risk factors are unchangeable, such as gender, age, and family history [2]. However, certain modifiable risk factors include smoking, poor dietary habits, excessive alcohol consumption, physical inactivity, obesity, high cholesterol levels, and diabetes [3]. The disease pattern in Iraq, as well as in other countries in the region, has shifted due to the rising incidence of non-communicable diseases. The most common cause of death in Iraq, according to national data registries, is still cardiovascular illnesses. According to statistics, it accounts for up to half of all sickness cases and one-third of all fatalities [4]. The nationwide diabetes and hypertension screening program was progressively extended to all primary healthcare facilities, including all 100 of Iraq’s health directorates, beginning in 2008. The screening system identified 860,000 cases of high blood pressure between the project’s initiation and 2017, with 150,000 cases confirmed [4]. Every human being has the fundamental right to health, and obtaining health requires having a suitable level of health knowledge and comprehension [5]. In many regions of the world, people struggle with health literacy because they cannot properly comprehend health information or follow treatment recommendations. This can exacerbate health issues in individuals with chronic illnesses, leading to a worsening of their conditions [6]. Social support appears to be a crucial factor in enhancing health literacy and improving medication adherence rates in such situations [7]. Patients with a strong social support system are better equipped to follow their treatment plans and develop skills related to health literacy [8]. Additionally, social support can provide guidance and educate patients, encouraging their active participation in self-care [9, 10]. One of the chronic illnesses for which a patient’s health depends on ongoing adherence to therapy is hypertension. The rise in these chronic illnesses necessitates a solid grasp of health and the capacity to successfully engage with health information. People with these diseases face significant challenges when it comes to health literacy [11]. “Health illiteracy” refers to the inability to understand and use health knowledge to make informed decisions about one’s health [12]. In many Iraqi communities, a lack of health literacy can exacerbate chronic illnesses, lead to injuries, and result in delays in receiving essential medical care. Individuals with long-term conditions like hypertension require close monitoring and must adhere to their doctor’s instructions and prescription schedules consistently [13]. The goal of science and research should be to comprehend health literacy and how it affects hypertension patients’ adherence to their medication. People with low health literacy may be more likely to forget to take their medications on time or misinterpret health instructions, which can worsen their condition and place additional strain on the healthcare system [14, 15]. Social support is a crucial component that can assist patients with low health literacy in improving their medication adherence. Social support from friends, family, and the local community can significantly enhance adherence to medication and healthy behaviors. Those who are more health literate can better absorb health information when they have the support of their social network [10].
The importance of medication adherence for individuals with hypertension cannot be overstated, since it is crucial for the management and control of this chronic condition. Hypertension is one of the main risk factors for cardiovascular diseases, such as heart attacks and strokes. Regular follow-up consultations with nurses, lifestyle modifications, and continuous adherence to prescribed drug regimens are crucial for the management of hypertension [16]. Patients who disregard their prescriptions face the danger of experiencing the negative effects of high blood pressure, which include damage to vital organs, such as the heart, kidneys, and blood vessels. Additionally, uncontrolled hypertension increases the cost of hospital and primary care treatments, which puts an additional burden on the healthcare system [16]. In order to better understand the relationship between medication adherence and health literacy in patients with hypertension, this study assessed the role that social support plays as a mediating factor in this relationship. We looked at the factors that influence medication adherence and how social support can help patients stick to their treatment plans and stay healthier overall.
Materials and Methods
Study design
This study followed the descriptive cross-sectional design since it is the best suitable method to accomplish its goals.
Study sample
A total of 450 participants with a diagnosis of hypertension who visited primary healthcare facilities in the Babylon Governorate were chosen as a non-probability convenience sample. Given that 25% of the research population has high blood pressure and because 1,803 visits to those health centers were made in a given month, this sample was chosen in part because of these factors.
The 25% of the study population is represented by selecting a quarter of the monthly visits for patients with hypertension.
Study tools
A questionnaire was utilized as the research tool, focusing on investigating the social and demographic characteristics of the individuals in the research sample. These characteristics encompassed various aspects such as age, gender, educational level, monthly income, occupation, and duration of hypertension. Specific metrics were employed in this study to analyze the collected data and information, including:
The Morisky medication adherence scale (MMAS-8), which comprises eight items and its Arabic version has been validated, was used to measure adherence to antihypertensive drugs [17]. In our study, its Cronbach’s α was 0.87, showing strong reliability in this particular setting.
The social support rating scale (SSRS) was used to assess patients’ social support, and its Arabic version has been validated [18]. This scale’s Cronbach’s α in this study was 0.79, indicating a satisfactory level of reliability.
Health literacy was assessed using the health literacy management scale (HeLMS), which was developed by Jordan et al. [19] and its Arabic version has been validated [20]. The scale’s Cronbach’s α in this study was 0.87, indicating improved reliability.
Validity and reliability
Experts in the field of nursing evaluated the questionnaire for validity, and a pilot study was carried out on 20% of the research population to assess the instrument’s reliability. The researcher asked the participants to fill out a questionnaire with their comments in order to participate in the study after introducing themselves to them when they visited the primary health care centers. Subsequently, the investigator elucidated the study’s goals and title in order to assess the comprehensibility and simplicity of reading the questionnaire’s contents. The estimated time for completing each form was 20 minutes, and the pilot study was excluded from the sample without modification following data analysis. The study scales’ intraclass correlation coefficient (ICC) was 0.86, which denotes strong stability.
Data collection
The actual data collection process spanned nearly a month, during which the researchers conducted individual interviews with each study participant at primary healthcare facilities.
These interviews involved explaining the study’s objectives and obtaining verbal consent from each participant. Patients who met specific criteria, including having a hypertension diagnosis for more than six months and providing voluntary consent, were interviewed to gather information. The confidentiality of collected data and the privacy of participants were rigorously maintained. Participants were under no obligation to continue or discontinue their participation at any point in the study.
Statistical analysis
All statistical analyses were performed using SPSS software, version 20. Numeric values and percentages were used to rank the variables, while Mean±SD were employed to provide statistical descriptions of continuous variables. A straightforward linear regression test was employed to evaluate the hypothesis of the relationship between the study’s variables. The distribution of data was assessed using two common techniques: The Kolmogorov-Smirnov and Shapiro-Wilk tests. Additionally, the Mann-Whitney U and Kruskal-Wallis H tests were performed to assess any statistical differences between the groups. A significance threshold of 0.05 was applied.
Results
The mean age of participants was 47.61±14.84 years, with ages ranging from 22 to 74 years. Regarding gender, hypertension was more prevalent among females (54.7%) followed by males (45.3%). Concerning marital status, the majority were married (48.7%) and concerning education level, more than half of the studied sample had completed primary school (59.3%). Approximately one-third of the study sample did not have enough monthly income (65.8%). In terms of the duration of the disease, 53.8% were diagnosed with hypertension for less than one year.
The results in Table 1 revealed the socio-demographic characteristics of the participants in which the mean age was 47.61±14.84 years and ages ranged from 22 to 74 years. Relevant words for this essay may appear in purple. With respect to gender, hypertension was more common among females (54.7%) and the rest were males (45.3%). On the status on marital the married ones were majorities (48.7%). The related findings on education level, the majority of the studied sample were primary school graduates (59.3%). One-third of the respondents (65.8%) had low monthly income. With regard to duration of disease, (53.8%) were diagnosed with hypertension for less than one year.
Table 2 displays that 75.6% of patients with hypertension had low drug adherence. Additionally, 74.9% of hypertension patients reported receiving little social support, while 67.8% of these patients reported being highly illiterate in terms of health. The data given in Table 2 demonstrate the poor medication adherence rate (75.6 %) among patients with hypertension.
Further, social support provided to patients with hypertension was also low (74.9%). In addition, health literacy in patients with hypertension was recorded a high level (67.8%) (Figure s 1 and 2).
Table 3 presents the findings from a simple linear regression statistical analysis indicating that the degree of health education (β=-0.708; P=0.001) and the existence of social support (β=0.220; P=0.001) are predictive factors for medication adherence in hypertension patients.
According to Table 4, there were statistically significant differences in medication adherence among hypertensive patients based on their gender, marital status, education level, monthly income, and duration of hypertension (P=0.001 for all variables).
Discussion
Medication adherence is a crucial aspect of managing and treating hypertension, as it plays a vital role in maintaining cardiovascular health. Patients with hypertension experience elevated blood pressure in their arteries, which can have significant adverse effects on their well-being and increase the risk of cardiovascular diseases. It is imperative to emphasize to patients the importance of improving medication compliance, as treating hypertension with medication helps stabilize blood pressure, thereby reducing the risk of cardiovascular diseases.
According to the study’s findings, 75.6% of participants had low medication adherence, indicating that medication adherence is highly suboptimal among hypertension patients. This is concerning since there is a connection between a higher risk of cardiovascular disease and its complications with non-adherence to antihypertensive treatment [21]. Inadequate medication adherence has consequences that extend beyond individual health outcomes and affect the overall cost burden of hypertension on public health systems. Enhancing medication adherence is a primary goal of interventions aimed at reducing the potential consequences of poorly controlled hypertension.
These findings are in line with those of the Al-Khobar study and lower than those of the Saudi Arabian study [22, 23]. Discrepancies in adherence rates could be attributed to variations in healthcare systems, demographics, and tools used to measure medication adherence.
The study highlights the low levels of medication adherence rates and inadequate social support received by people with hypertension, with 74.9% reporting low levels. People with chronic illnesses need social support for self-care since it affects their motivation and ability to adhere to prescribed medication schedules and other healthy behaviors [24]. The low levels of social support reported by patients underscore the necessity for nurses and the community to offer interventions aimed at strengthening social support networks for individuals with hypertension. Some potential tactics include educational programs that inform friends and family about the illness, how to support it, and why it is crucial. These findings are in line with studies conducted in the Iraqi province of Babylon, which revealed that most patients with chronic conditions and illnesses needing rehabilitation do not obtain the necessary level of social assistance [10].
Additionally, the study sheds light on the issue of health illiteracy among hypertension patients, as 67.8% of them exhibited high levels of this knowledge deficit. Health literacy is a critical component when it comes to helping individuals with hypertension comprehend medical information, make essential decisions regarding medication adherence, and navigate healthcare systems successfully [25]. Insufficient health literacy can hinder the effective management of hypertension, leading to inadequate self-care practices and deteriorating overall health. Addressing health literacy through targeted educational initiatives and readily available health communication resources is essential for enabling individuals with hypertension to make informed decisions about their health and medication adherence.
The research emphasizes the various difficulties that people with hypertension encounter, such as poor medication compliance, insufficient social support, and elevated levels of health literacy. These results highlight the necessity of all-encompassing interventions that deal with the disease’s social, educational, and health-related aspects. Medication adherence among hypertensive patients should be encouraged through social support interventions provided by health care facilities (nurses), and increasing health literacy is crucial to improving patient outcomes and lowering the overall burden of hypertension on public health.
Social support vs medications adherence
Research has shown that social support is crucial for promoting medication compliance in individuals with long-term hypertension. The positive beta value (β=0.220) indicates a direct correlation between social support and medication adherence. This suggests that patients with high levels of social support networks are more likely to adhere to their prescribed medication regimens with a 0.220 increase in adherence for each incremental rise in social support. These findings demonstrate the extent to which emotional and practical support has a favorable impact on adherence habits, supporting the idea that social support is important in the management of chronic illnesses [26]. Additionally, social cognition theory, which holds that people learn by seeing and interacting with others, has supported the impact of social networks on behaviors related to health [27]. In the context of medication adherence, this may involve sharing experiences, acting as reminders, or providing assistance with medication administration in a socially supportive environment.
Health literacy vs medication adherence
The negative beta coefficient (β=-0.708) of health literacy indicates a negative relationship between health literacy and adherence to medication prescribed for hypertension patients. This suggests that for every unit improvement in health literacy, patients with hypertension have a 0.708-fold decrease in drug adherence. This finding is consistent with other studies emphasizing the significance of health literacy in understanding and applying medical guidance for chronic illnesses [28, 16]. Understanding and adhering to prescription instructions, possible side effects, and the significance of following pharmaceutical guidelines might be significantly hampered by high level of health literacy [29]. Patients with hypertension may find it challenging to absorb complicated medical information, which can result in misinterpretations and a disregard for recommended treatment plans. Therefore, it is critical to suggest initiatives aimed at enhancing health literacy in order to promote chronic condition medication adherence, including hypertension [30].
Differences in medication adherence according to patients’ characteristics
The results demonstrated that there were statistically gender-based differences in hypertension patients’ adherence to their medications (P=0.001). The results showed that males followed their hypertension treatment plans more religiously than women did. These findings are consistent with those of Radhi et al. [16]. Gender differences in adherence underscore the importance of developing intervention strategies that consider gender differences to address specific medication management needs.
Marital status can also influence medication adherence in patients with hypertension. The results showed a significant difference (P=0.000) in medication adherence levels between married patients and their single, divorced, and widowed counterparts. This observation can be attributed to the concept that shared responsibilities, spousal (social) support, and a more stable social environment positively impact the adherence of married individuals to their prescription regimens [31].
Another remarkable finding among the key factors affecting medication adherence in patients with hypertension is educational attainment. The results demonstrated that patients with different educational backgrounds adhere to treatment at significantly different rates (P=0.000), with college graduates adhering to treatment at the greatest rates. This underscores the critical role of health literacy. These differences may be explained by the fact that individuals with higher education levels may possess greater health awareness, understand the importance of following hypertension medication regimens, and have better relationships with community health nurses [32].
According to statistical analysis, patients with higher (sufficient) monthly incomes exhibited better medication adherence (P=0.001). This indicates a significant difference in adherence levels based on monthly income. Increased monthly income may facilitate more consistent adherence to blood pressure medication, underscoring the importance of targeted interventions for patients with lower incomes to address potential barriers to following their prescription drug regimens as prescribed [16].
The study results indicated statistically significant differences (P=0.001) in medication adherence levels based on the length of hypertension. These differences favored individuals with longer histories of hypertension, who demonstrated higher medication adherence than those with shorter durations. This observation suggests that individuals with a longer history of hypertension may have developed stronger medication adherence habits or possess a heightened awareness of the importance of consistent care [33].
Conclusion
The study’s striking finding is that individuals with hypertension exhibit low medication adherence, limited social support, and a high level of health illiteracy. Among the predictive factors for medication adherence, health literacy, and social support emerge as significant contributors. The complexity of this issue is underscored by the significance of variables such as patients’ gender, marital status, educational attainment, monthly income, and duration of hypertension. To address these concerns, interventions by community health nurses should prioritize strengthening patients’ social support networks and enhancing their health literacy levels.
Study limitation
Many patients declined to participate in the study due to time constraints, unwillingness, or lack of interest in the research. Additionally, the extensive questionnaire and large sample size made data collection a labor-intensive process.
Ethical Considerations
Compliance with ethical guidelines
This research approved by the Ethical Committee of Al-Awsat Technical University (No.: 713, dated 3/11/2023).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and data analysis: Mohammed Malih Radhi; Data collection, writing and supervision: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their thanks and gratitude to the Babylon Health Directorate for facilitating data collection, as well as to Al-Furat Al-Awsat Technical University.
References
- Guo A, Jin H, Mao J, Zhu W, Zhou Y, Ge X, et al. Impact of health literacy and social support on medication adherence in patients with hypertension: A cross-sectional community-based study. BMC Cardiovascular Disorders. 2023; 23(1):93. [DOI:10.1186/s12872-023-03117-x] [PMID] [PMCID]
- Khaleefah MA, Al-Badri HJ, Mousa NA. Hypertension control among adult Iraqis. Journal of the Faculty of Medicine Baghdad. 2022; 64(3):145-52. [DOI:10.32007/jfacmedbagdad.6431935]
- Hussain AM, Lafta RK. Burden of non-communicable diseases in Iraq after the 2003 war. Saudi Medical Journal. 2019; 40(1):72-8. [DOI:10.15537/smj.2019.1.23463] [PMID] [PMCID]
- Tailakh A, Evangelista LS, Mentes JC, Pike NA, Phillips LR, Morisky DE. Hypertension prevalence, awareness, and control in Arab countries: A systematic review. Nursing & Health Sciences. 2014; 16(1):126-30. [DOI:10.1111/nhs.12060] [PMID] [PMCID]
- Talbot L, Verrinder G. Promoting health: The primary health care approach. Edinburgh: Elsevier Health Sciences; 2017. [Link]
- Galvin B, Dalrymple PW. Growing community health literacy through libraries: Sharing global perspectives. Berlin: De Gruyter; 2020. [Link]
- Goldsmith DJ, Albrecht TL. Social support, social networks, and health. In: Thompson TL, Parrott R, Nussbaum JF, editors. The Routledge handbook of health communication. New York: Routledge; 2003. [Link]
- Dinh TTH, Bonner A. Exploring the relationships between health literacy, social support, self-efficacy and self-management in adults with multiple chronic diseases. BMC Health Services Research. 2023; 23(1):923. [DOI:10.1186/s12913-023-09907-5] [PMID] [PMCID]
- Zhu Y, Song Y, Wang Y, Ji H, Wang D, Cai S, et al. Relationships among patient activation, social support and online health information seeking of community-dwelling older adults living with coronary heart disease. Journal of Advanced Nursing. 2023; 79(1):161-9. [DOI:10.1111/jan.15428] [PMID]
- Juma Elywy G, Radhi MM, Khyoosh Al-Eqabi QA. Social support and its association with the quality of life (QoL) of amputees. Iranian Rehabilitation Journal. 2022; 20(2):253-60. [DOI:10.32598/irj.20.2.1784.1]
- Chen X, Zhou X, Li H, Li J, Jiang H. The value of WeChat application in chronic diseases management in China. Computer Methods and Programs in Biomedicine. 2020; 196:105710. [DOI:10.1016/j.cmpb.2020.105710] [PMID]
- Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health. 2017; 17(1):361. [DOI:10.1186/s12889-017-4365-x] [PMID] [PMCID]
- Uribe Guajardo MG, Slewa-Younan S, Kitchener BA, Mannan H, Mohammad Y, Jorm AF. Improving the capacity of community-based workers in Australia to provide initial assistance to Iraqi refugees with mental health problems: An uncontrolled evaluation of a Mental Health Literacy Course. International Journal of Mental Health Systems. 2018; 12:2. [DOI:10.1186/s13033-018-0180-8] [PMID] [PMCID]
- Saqlain M, Riaz A, Malik MN, Khan S, Ahmed A, Kamran S, et al. Medication adherence and its association with health literacy and performance in activities of daily livings among elderly hypertensive patients in Islamabad, Pakistan. Medicina. 2019; 55(5):163. [DOI:10.3390/medicina55050163] [PMID] [PMCID]
- Heizomi H, Iraji Z, Vaezi R, Bhalla D, Morisky DE, Nadrian H. Gender differences in the associations between health literacy and medication adherence in hypertension: A population-based survey in Heris County, Iran. Vascular Health And Risk Management. 2020; 16:157-66. [DOI:10.2147/VHRM.S245052] [PMID] [PMCID]
- Radhi MM, Niazy SM, Abed SN. Individual-related factors associated treatment adherence among hypertensive patients. Journal of Public Health in Africa. 2023; 24. [DOI:10.4081/jphia.2023.2466] [PMID] [PMCID]
- Ashur ST, Shamsuddin K, Shah SA, Bosseri S, Morisky DE. Reliability and known-group validity of the Arabic version of the 8-item Morisky Medication Adherence Scale among type 2 diabetes mellitus patients. Eastern Mediterranean Health Journal. 2015; 21(10):722-8. [DOI:10.26719/2015.21.10.722] [PMID]
- RM KS. Validation of the Arabic translation of the multidensional scale of social support (Arabic MSPSS) in a lebanese community sample. The Arab Journal of Psychiatry. 2012; 23(2):159-68. [Link]
- Jordan JE, Buchbinder R, Osborne RH. Conceptualising health literacy from the patient perspective. Patient Education and Counseling. 2010; 79(1):36-42. [DOI:10.1016/j.pec.2009.10.001] [PMID]
- Bergman L, Nilsson U, Dahlberg K, Jaensson M, Wångdahl J. Validity and reliability of the arabic version of the HLS-EU-Q16 and HLS-EU-Q6 questionnaires. BMC Public Health. 2023; 23(1):304. [DOI:10.1186/s12889-023-15519-9] [PMID] [PMCID]
- Mahmood S, Jalal Z, Hadi MA, Khan TM, Haque MS, Shah KU. Prevalence of non-adherence to antihypertensive medication in Asia: A systematic review and meta-analysis. International Journal of Clinical Pharmacy. 2021; 43(3):486-501. [DOI:10.1007/s11096-021-01236-z] [PMID]
- Elbur AI. Level of adherence to lifestyle changes and medications among male hypertensive patients in two hospitals in Taif; Kingdom of Saudi Arabia. International Journal of Pharmacy and Pharmaceutical Sciences. 2015; 7(4):168-72. [Link]
- Algabbani FM, Algabbani AM. Treatment adherence among patients with hypertension: Findings from a cross-sectional study. Clinical Hypertension. 2020; 26:18. [DOI:10.1186/s40885-020-00151-1] [PMID] [PMCID]
- Mohebi S, Parham M, Sharifirad G, Gharlipour Z, Mohammadbeigi A, Rajati F. Relationship between perceived social support and self-care behavior in type 2 diabetics: A cross-sectional study. Journal of Education and Health Promotion. 2018; 7:48. [DOI:10.4103/jehp.jehp_73_17] [PMID] [PMCID]
- Park NH, Song MS, Shin SY, Jeong JH, Lee HY. The effects of medication adherence and health literacy on health-related quality of life in older people with hypertension. International Journal of Older People Nursing. 2018; 13(3):e12196. [DOI:10.1111/opn.12196] [PMID]
- Vahedparast H, Mohammadi E, Ahmadi F, Farhadi A. The role of social support in adherence to treatment regimens: Experiences of patients with chronic diseases. Medical-Surgical Nursing Journal. 2018; 7(1):e69646. [DOI:10.5812/msnj.69646]
- Link E, Reifegerste D, Klimmt C. Family involvement in the context of chronic diseases: The role of social support in treatment decision-making for surgical procedures. Journal of Family Research. 2020; 32(1):45-71. [DOI:10.20377/jfr-160]
- van der Gaag M, Heijmans M, Spoiala C, Rademakers J. The importance of health literacy for self-management: A scoping review of reviews. Chronic Illness. 2022; 18(2):234-54. [DOI:10.1177/17423953211035472] [PMID]
- Kilic HF, Dag S. The relationship between health literacy and medication adherence in a hypertensive patient population. International Journal of Caring Sciences. 2020; 13(1):101-7. [Link]
- Lor M, Koleck TA, Bakken S, Yoon S, Dunn Navarra AM. Association between health literacy and medication adherence among hispanics with hypertension. Journal of Racial and Ethnic Health Disparities. 2019; 6(3):517-24. [DOI:10.1007/s40615-019-00588-7] [PMID] [PMCID]
- Ezeala-Adikaibe BA, Mbadiwe N, Okudo G, Nwosu N, Onyebueke G, Nwobodo M, et al. Factors associated with medication adherence among hypertensive patients in a tertiary health center: A cross-sectional study. Archives of Community Medicine and Public Health. 2017; 3(1):24-31. [DOI:10.17352/2455-5479.000021]
- Ayodapo AO, Elegbede OT, Omosanya OE, Monsudi KF. Patient education and medication adherence among hypertensives in a tertiary hospital, south western Nigeria. Ethiopian Journal of Health Sciences. 2020; 30(2):243-50. [DOI:10.4314/ejhs.v30i2.12] [PMID] [PMCID]
- Jhaj R, Gour PR, Kumari S, Sharma S. Association between medication adherence and blood pressure control in urban hypertensive patients in central India. International Journal of Noncommunicable Diseases. 2018; 3(1):9-14. [DOI:10.4103/jncd.jncd_29_16]
Article type: Original Research Articles |
Subject:
Nursing
Received: 2023/12/2 | Accepted: 2023/12/18 | Published: 2024/03/1
Received: 2023/12/2 | Accepted: 2023/12/18 | Published: 2024/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
