
988368
Thu, Jul 30, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 605-614 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Almusawi A A H, Al-Hindy H A M. Exploring Back Pain Characteristics: Insights From Hilla, Iraq. Iranian Rehabilitation Journal 2024; 22 (4) :605-614
URL: http://irj.uswr.ac.ir/article-1-2179-en.html
URL: http://irj.uswr.ac.ir/article-1-2179-en.html



1- Department of Neurosurgery, Hammurabi College of Medicine, University of Babylon, Babylon, Iraq.
2- Department of Pharmacology and Toxicology, College of Pharmacy, University of Babylon, Babylon, Iraq.
2- Department of Pharmacology and Toxicology, College of Pharmacy, University of Babylon, Babylon, Iraq.
Full-Text [PDF 492 kb]
(915 Downloads)
| Abstract (HTML) (7135 Views)
Full-Text: (599 Views)
Introduction
Low back pain (LBP) is a prevalent illness that often prompts people to seek health care, usually results in job loss, and can cause disability worldwide [1]. LBP is frequently accompanied by neuropathic manifestations, including nociceptive, non-specific, and other pain kinds [2, 3]. Though several diagnostic techniques are available, their usefulness is still debatable since there are numerous contributing factors to LBP and imaging and diagnostic injections are not particularly specific [2]. The intricacy of lower back pain, which influences both the pain’s perception and the disability it causes, is influenced by biology, psychology, and society [4].
Non-specific LBP
Most cases of non-specific LBP lack a well-defined anatomical cause [5]. The hallmarks of non-specific pain are diminished physical function and pain. More severe cases are also linked to a marked decline in mental and physical health, in addition to a higher chance for the development of chronic illness and death from all causes [6].
Distinction of buttock region
The buttock region, which spans from both iliac crests down to the gluteal folds, is physiologically distinct from LBP, even though the two can occasionally coexist and be misdiagnosed. The iliac crest is the final anatomical marker in the lower back, starting from the 12th rib. Most people will suffer from severe LBP at certain times during the disease in their lives. This is usually a transient but often chronic disorder. Studies show that one year following the onset of mechanical lower back pain, more than 60% of persons with the condition would still be in pain or would experience it often [7].
A thorough analysis of the lower back pain situation would help clinicians better understand the heterogeneity in LBP and its implications [8]. Only a small number of cohorts have been performed on the general pattern of back pain patients in Iraq and the surgical management of these individuals.
Prognosis of LBP
The prognosis for LBP differs based on the patient and the particulars of the pain. The majority of people with new LBP episodes recover in a few weeks, but recurrences are frequent, and people with chronic, long-term LBP typically have a more protracted course. The back pain episode, individual and psychological traits, and social and professional environments influence the prognosis of back pain. A small percentage of patients with acute LBP may become chronic, although the majority see quick improvements in pain and impairment within the first month. On the other hand, individuals with non-radicular persistent LBP that has recently started have a favorable prognosis and a good chance of improving [9, 10, 11].
Our objective in doing this study on Iraqi patients is to close a significant knowledge gap. Iraq has a high incidence of LBP cases; however, there has not been much thorough research on the patterns and surgical care of these patients. This study makes a valuable contribution by providing a distinct viewpoint on the intricacies of LBP etiologies exclusive to the Iraqi population. Secondly, we hope to offer Iraqi medical professionals insightful information to help them design efficient treatment plans. Additionally, by diversifying our understanding of back pain globally, the study guarantees that medical interventions are appropriate for various cultural and regional contexts.
Materials and Methods
Setting and participants
This cross-sectional study was piloted on 200 patients (90 females and 110 males) aged 30-50 years. They were selected randomly from those attending the outpatient clinic in Imam Alsadiq Teaching Hospital, Hilla, Iraq. The study took two years, from January 2017 to February 2019. The sample size of patients was chosen after careful evaluation of the goals of the investigation and the realistic limitations imposed by our research setting. This decision was made to balance the distinctiveness of our study population, logistical viability, and statistical robustness. A sample size of 200 patients is substantiated for several reasons. Firstly, to allow for a thorough analysis of the various etiologies of LBP common in our target demographic, given the extent of our inquiry into LBP patterns in a specific location. Secondly, to guarantee adequate statistical power, significant inferences must be made following accepted standards for cross-sectional research in comparable settings. Thirdly, to make it easier to characterize LBP cases in depth while considering our study environment’s unique clinical and demographic details. Lastly, we aim to improve the study’s validity and help make our findings more broadly applicable within the particular parameters of our inquiry.
Inclusion criteria
All patients in this study complained of (acute or chronic) lower back pain, whether it was associated with radicular pain. The study also included those who complained of back pain resulting from poor posture, muscle overuse, and sprains and strains with normal magnetic resonance imaging (MRI). Muscle spasms are diagnosed by normal MRI of the spine and by clinical examination [12, 13]. All patients were evaluated for clinical tests, radiological, and MRI scanning [14, 15].
Exclusion criteria
Thirteen patients provided inadequate demographic information, while 27 refused to cooperate and take part in the study, those who were not seen again after the first visit, those with previous spinal injuries, those who were poorly followed up, those with spinal congenital dysraphism, radiological and MRI data archives, and those with spinal tumors were excluded from this cohort [16].
Clinical and radiological evaluation
Experienced neurosurgeons, including the authors, performed a comprehensive assessment of the patients’ neurological condition, clinical presentations, and medical histories [15, 16]. Moreover, MRI analyses, which are essential for precise anatomical understanding, were carried out by knowledgeable radiologists [14-16]. These experts followed prescribed study criteria and used cutting-edge imaging methods to obtain exact information pertinent to LBP etiologies. The synergy between radiologists and neurosurgeons guaranteed a comprehensive strategy, integrating radiological and clinical viewpoints in the case selection procedure. Our goal is to strengthen the validity and credibility of the study by enhancing the transparency and dependability of our data collection methods and offering clarification on the competence of the professionals participating and the standardized processes followed.
Surgical interventions
Under general anesthesia, a laminectomy was carried out in a prone posture. A lower midline skin incision was made at the level of the involved spine, a subperiosteal gauze dissection was carried out, and gel foam and coagulation cauterization were used to secure the hemostasis. After the spinous process was removed using spinal rongeurs and punches, the involved vertebra underwent a bilateral laminectomy. The protruding disk material was then removed using pituitary forceps, and the surgical site was cleaned with gentamicin 80 mg mixed with normal saline [17]. The wound was then closed in layers, hemostasis was secured, the dressing was applied with antiseptics, and the redivac drain was left in for 24 hours after the procedure. Neurosurgery is indicated for definite conditions in our patient cohort, including single-level and multiple levels of disk prolapse, as well as spinal stenosis. A total of 40 patients (20 with L5S1 disk prolapse, 12 with L4, L10 disks prolapse, and 8 with L3, L8 disks prolapse) have single-level disk prolapse. Moreover, 20 patients (6 with L4, L5, S1 disk prolapse, 8 with L3, L4, L5 disks prolapse, and 6 with L2, L3, L4 disks prolapse) had several levels of disk prolapse. Additionally, there are 28 individuals with spinal stenosis (10 with L4, L5 stenoses, 8 with L3, L4, and L5 stenoses, and 10 with L5 S1 stenosis).
Statistical analyses
The study data were compiled into an Excel sheet, Microsoft Office (2017), and the percentages and numbers were sorted and computed appropriately.
Ethical clearance
The Hammurabi College of Medicine’s Review Committee’s ethical criteria were closely followed during the consenting process. Before giving written consent, the participants were guaranteed to be fully informed about the study’s goals, methods, and possible dangers. The emphasis on ethical principles, autonomy, and confidentiality highlights the strong ethical integrity upheld throughout the study. We hope to provide transparency and assurance about the ethical standards maintained in our research by outlining these procedures.
Results
In the current study, patients were classified as follows:
1) Degenerative spinal disorders affect 88 people; 40 cases with isolated disk prolapse; 20 patients suffer from multiple-level disk prolapse; 12 patients have L4, L5 disks prolapse; 8 patients have L3, L4 disks prolapse; and 20 patients have L5S1 disk prolapse. There are 6 patients with L4, 5, and S1 disk prolapse, 8 with L3, 4, and 5 with prolapse, and 6 with L2, 3, and 4. Additionally, there are 28 patients with lumber stenosis, 10 with L4, 5 stenoses, 8 with L3, 4, 5 stenoses, and 10 with L5, S1 stenosis.
2) Patients with mild disk prolapse make up 40.
3) Forty patients have normal lumbosacral spine MRIs but exhibit muscle spasms.
4) Twenty-six people experience back pain as a result of a laminectomy or a prior spinal operation.
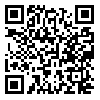
A clear and organized presentation of the demographic data in Table 1 helps clarify possible factors linked to LBP in the group under study.
The representation was broad in terms of age groups. The mean age displayed a narrow range of ages with slight variation. The gender distribution shows a higher percentage of men (63.5%), offering a fair assessment of the effects of LBP on both sexes. The distribution of residences between rural and urban areas provides information about possible lifestyle or environmental issues. The occupational distribution sheds light on potential factors contributing to LBP by highlighting a significant proportion of heavy job workers (55%). The awareness of LBP across various lifestyles is enhanced by the range of jobs, which includes homemakers, retirees, and official workers. The smoking rate among LBP patients reveals a notable percentage of smokers (62.5%). Comorbid conditions such as type 2 diabetes, bronchial asthma, chronic obstructive pulmonary disease (COPD), and hypertension are listed, giving a thorough picture of the population under study’s health.
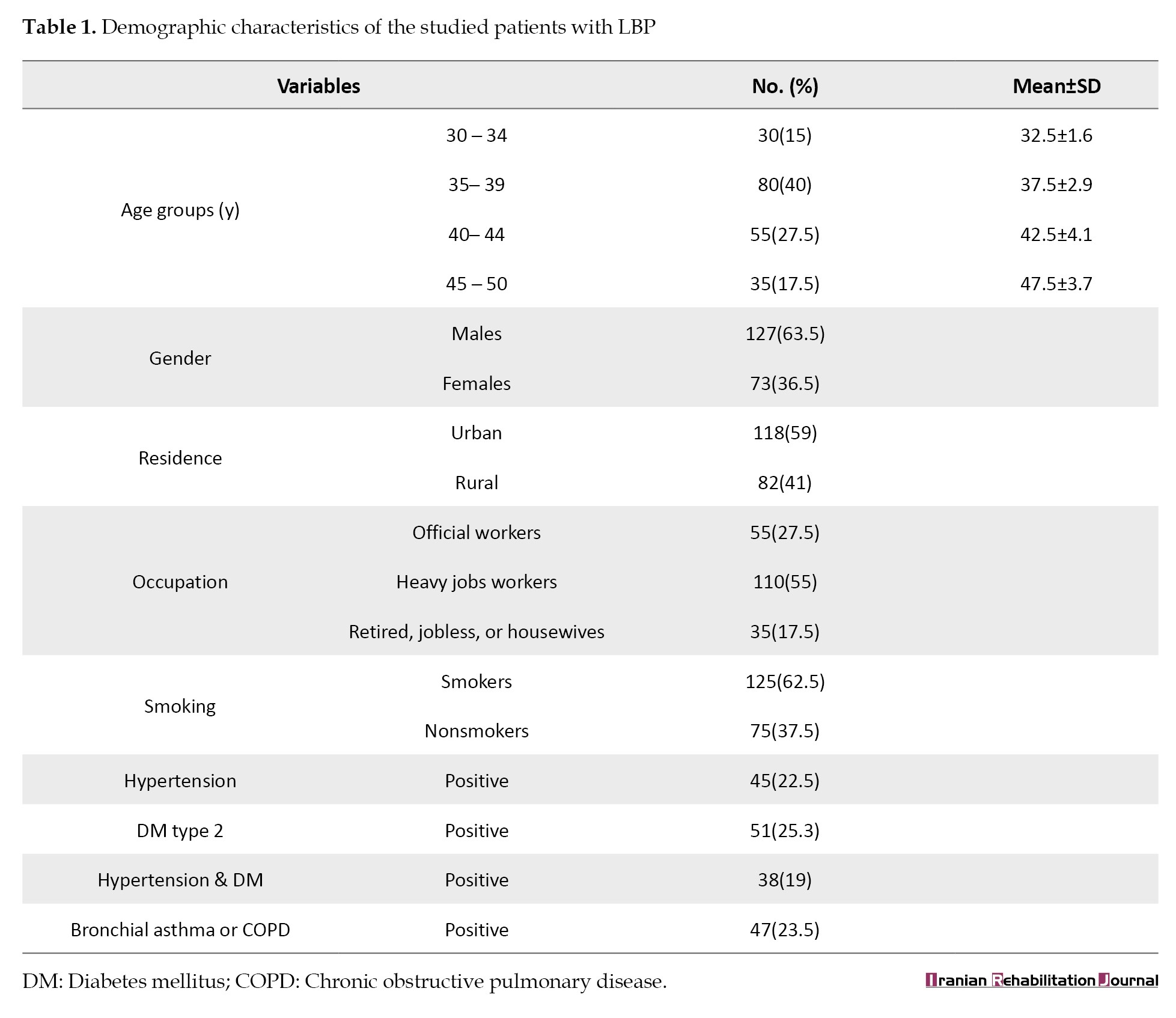
The numerous causes of back pain among the 200 study participants are briefly depicted in Table 2.
It gives a useful overview of the distribution of back pain etiologies in the population under study. It clearly and concisely breaks down the number of patients and the associated percentages for each cause. A more nuanced knowledge of the various variables causing back pain is provided by including categories such as spinal stenosis, muscle spasm, disc prolapse at different levels, and prior spinal procedures. These additions improve the study. According to the results, single-level disk prolapses, mild disk prolapses, and multiple-level disk prolapses account for half of the disc-related LBP.
Additionally common, accounting for 20% and 14% of cases, respectively, are spinal stenosis and muscular spasms. Remarkably, 13% of individuals have a history of prior spine procedures, including laminectomy. In 3% of cases, albeit less common, spinal tumors are found.
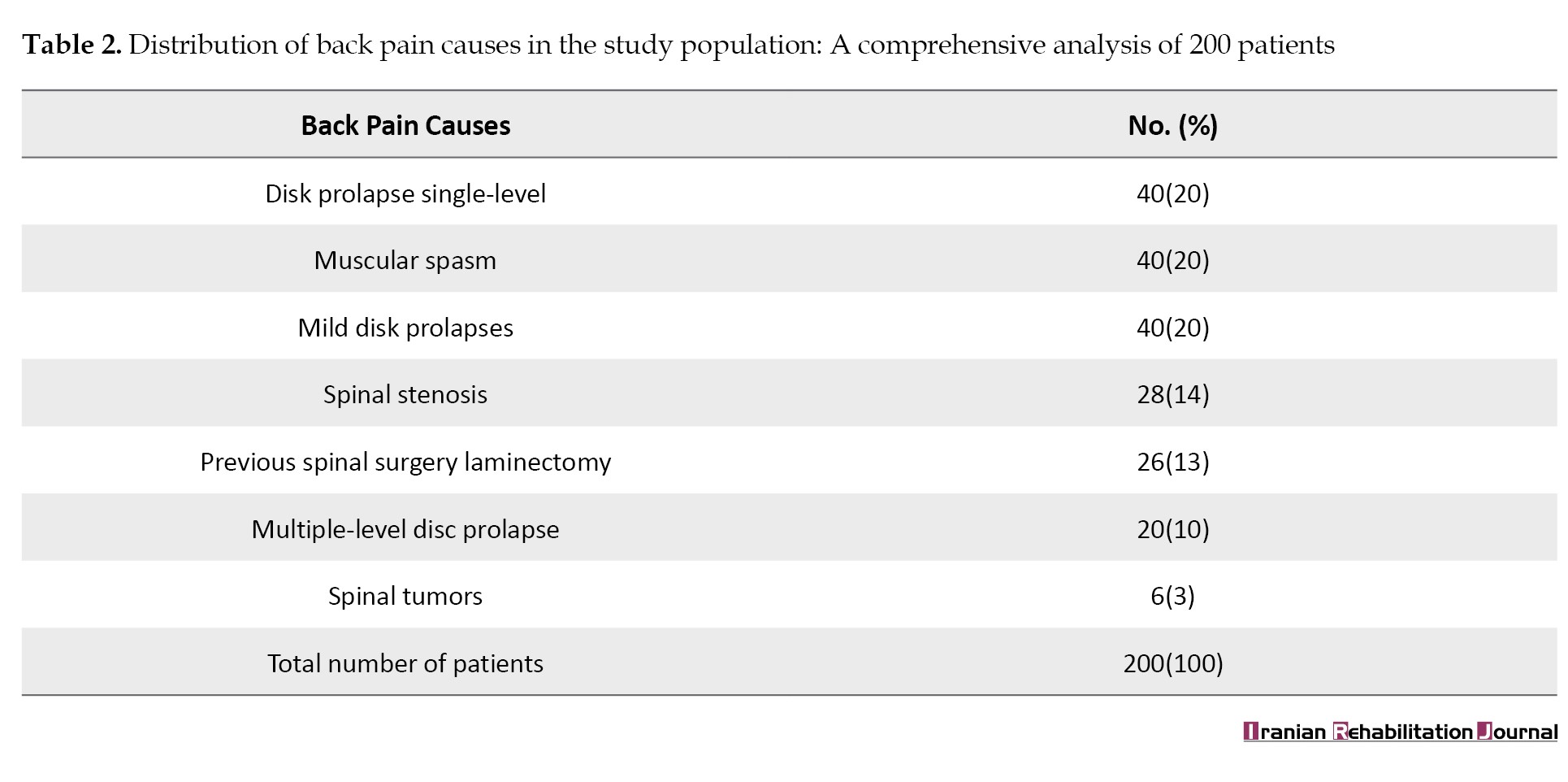
A targeted and detailed analysis of the number of patients with single-level disk prolapse at various spinal levels may be found in Table 3.
It effectively conveys the case distribution, showing that the L5, S1 level (20 patients) had the highest occurrence, followed by L4, L5 (12 patients), and L3, L4 (8 patients). There are forty individuals in total with single-level disk prolapse at all levels.
The number of patients with multiple-level disk prolapse at various spinal levels and the related percentages are effectively presented in Table 4.
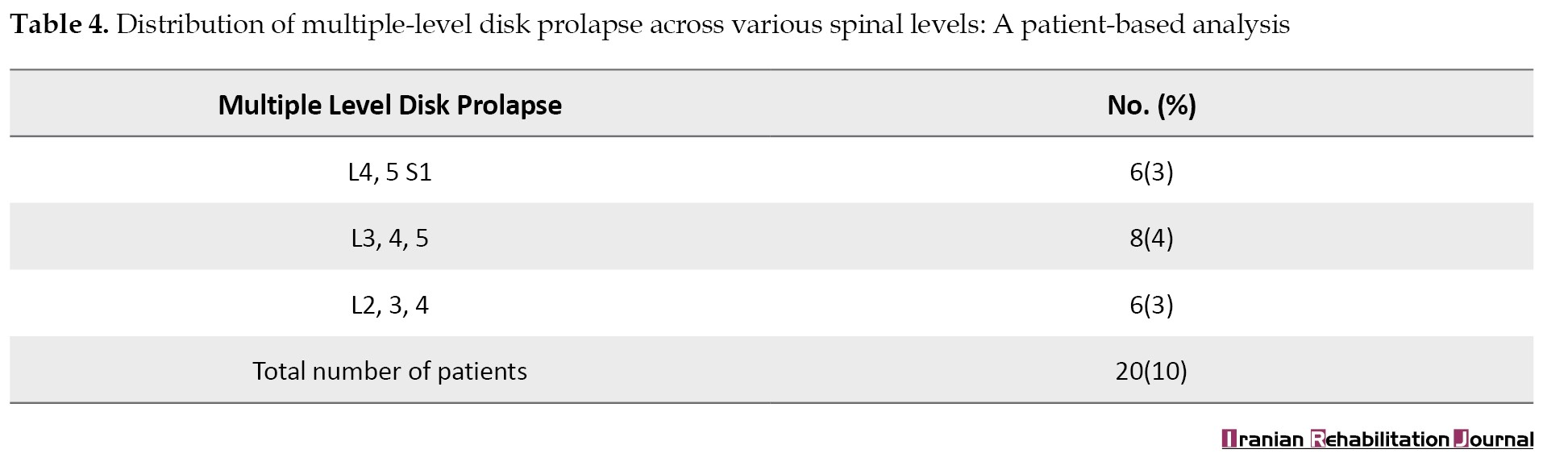
Six patients (3%) at L4, 5, S1, 8(4%) at L3, 4, 5, and 6(3%) at L2, 3, and 4 have disk prolapse, according to the distribution. Notably, 10% of the patients, or 20, lack a recognized spinal level.
The distribution of patients with spinal stenosis at various spinal levels is clearly shown in Table 5.
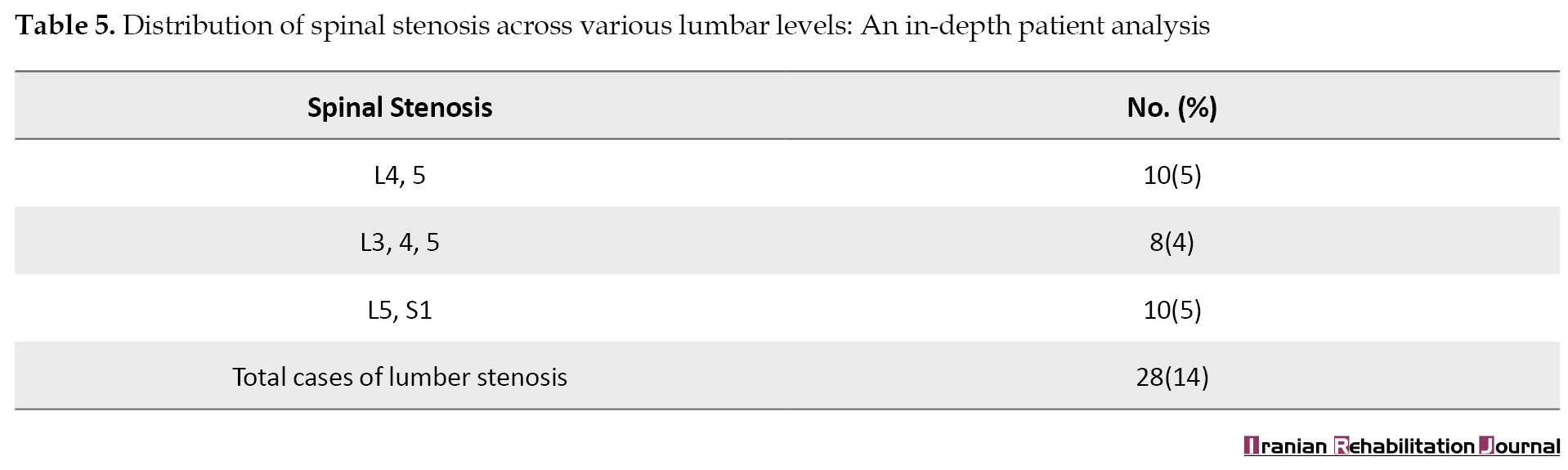
It shows that spinal stenosis affects 10 patients (5%) at L4, 5, 8(4%) at L3, 4, 5, and 10(5%) at L5, S1. Of the total participants in the study, 28 cases of lumbar stenosis cumulatively occur throughout all indicated levels, accounting for 14% of the total.
A comprehensive summary of the surgical techniques used in the study, broken down by levels of stenosis and disk prolapse, may be found in Table 6.
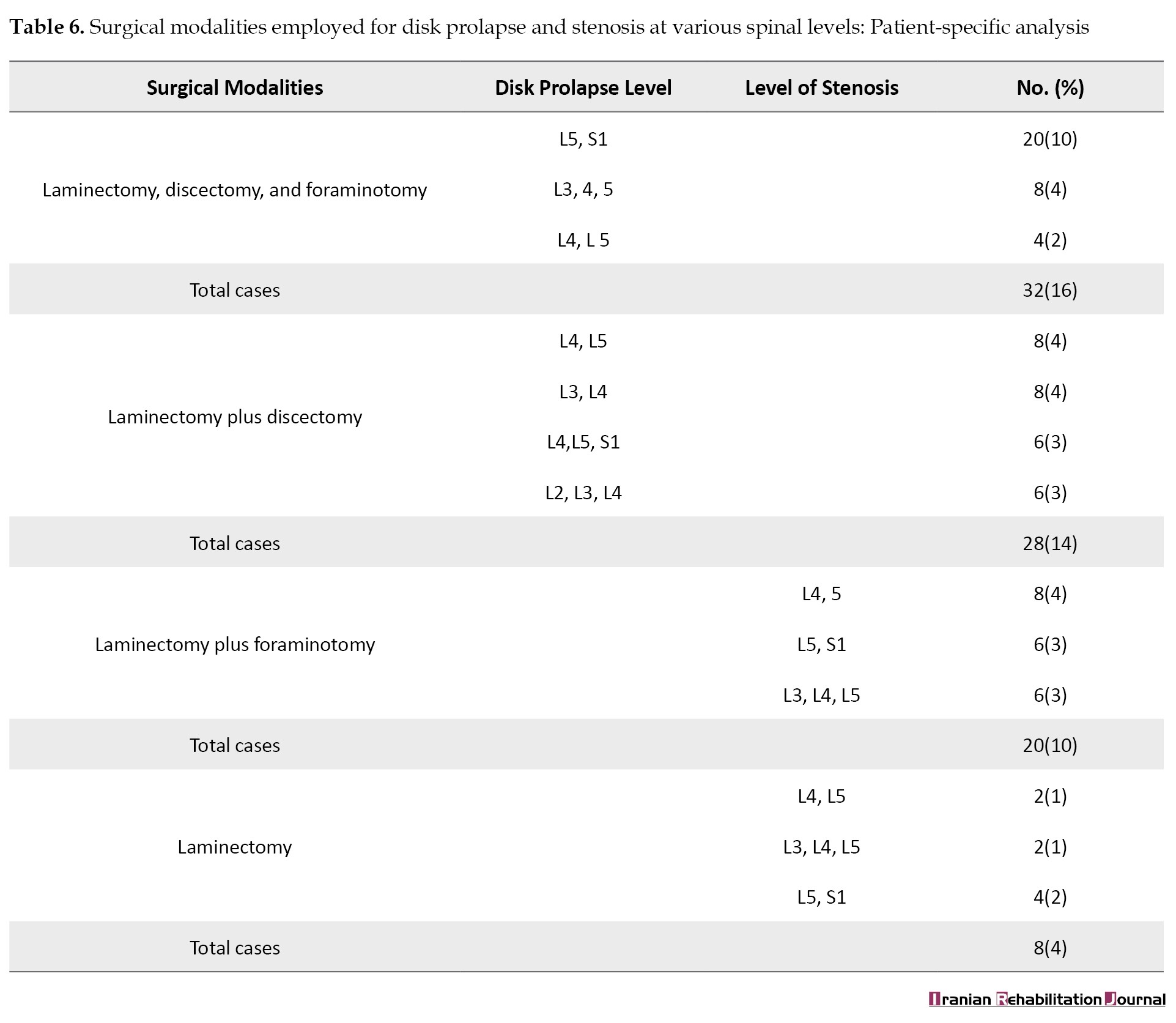
Specific spinal levels correspond to each surgical method. The table shows the number of patients and matching percentages for each category.
Many techniques are covered by the surgical modalities, such as laminectomy, discectomy, foraminotomy, and their combinations. The percentages show how each surgical technique is distributed compared to other disc prolapse and stenosis levels.
Discussion
The thorough examination of the etiologies of back pain, the distribution of disc prolapses, and the surgical techniques offered in this survey offer important new information about the features of the patient group under study. A detailed presentation of the demographic data in Table 1 helps clarify possible factors linked to LBP in the group under study. Table 2 lists the many reasons why people have back pain, with disk problems, muscle spasms, and laminectomy being the main culprits. Interestingly, many patients involve disk prolapse at a single level. Tables 3 and 4 provide detailed information on single-level and multiple-level disk prolapse, respectively, and the prevalence at various spine levels. Table 5 provides information on spinal stenosis incidence, highlighting differences across lumbar levels. Table 6 comprehensively analyzes the various surgical techniques used to treat disk prolapse and stenosis at different spine levels. The results highlight the intricacy of the etiologies of back pain and the sophisticated surgical methods used to treat these ailments. To personalize interventions based on the unique characteristics of patients, healthcare providers need to have this detailed understanding. This solution will help to improve therapy and patient care.
The annual incidence of disk prolapse is around 5-20/1000 adults [18], with a male/female ratio 2:1 [19]. However, other studies have reported female preponderance [20]. Similar to our outcome, almost in all cases of lumbar disk herniation, the L4-L5 and L5-S1 disks were affected [21]. Of the total participants in the present study, 28 cases of lumbar stenosis cumulatively occur throughout all indicated levels, accounting for 14%. Other studies have suggested spinal lumber stenosis ranges from 1.7% to 13.1% [22]. In the United States, lumbar spinal stenosis disturbs approximately 11% of older people. Studies have exposed that while 20% of people over 60 have spinal stenosis evident on imaging examinations, more than 80% do not cause manifestations and do not require therapy [23].
Similar to the findings of this study, many common comorbidities, including cerebrovascular, respiratory, and cardiovascular disorders among patients with LBP, were also reported. Research has indicated a higher likelihood of certain comorbidities in people with LBP than in people without back pain. Furthermore, comorbidities have been linked to subpar treatment for LBP. Comprehending the connection between comorbidities and back pain is crucial for enhancing patient care and developing guidelines [24]. These results highlight how crucial it is to consider and manage comorbidities in LBP patients to provide thorough and efficient therapy.
Patients who report radicular discomfort associated with root compression and a single degree of disk prolapse are treated with decompressive laminectomy or discectomy combined with foraminotomy [12]. Viewing the spinal root intraoperatively is vital to assess the extent of root pressure from the bone (osteophyte) or disk material. This method was based on the intraoperative findings of root pressure from disk material or osteophytes. This procedure may be necessary to alleviate pressure on the roots and release the spinal root (de roofing) of the intervertebral foramina since some patients continue to experience radicular discomfort following surgery due to intraoperatively undetected root pressure. Through what is known as “neural foramina,” apertures in the spinal vertebrae allow a bundle of spinal nerves (spinal roots) to emerge from the spinal cord. Narrowing of the nerve root apertures may cause pressure on the nerve. This condition is known medically as foraminal spinal stenosis, and a foraminotomy is necessary to decompress it [13]. Foraminotomy surgery may be taken into consideration if symptoms are severe enough to interfere with daily activities [25]. Symptoms could be experienced as thigh, calf, or lower back pain. Deep and often persistent agony is experienced. Pain is experienced when using the body in a particular way or when carrying out specific actions—numbness, tingling, and weakening of the muscles. MRI to verify that the symptoms are caused by foraminal stenosis [26].
The cases of major lumbar disk herniation can be successfully treated non-surgically, despite a revision by U et al. [27]. However, care must be taken to ensure that subjects are checked for cauda equina syndrome and were fully informed about the necessity to seek medical attention immediately if red-flag symptoms appear. In the patient in our study, a lumber disk herniation results in excruciating, uncontrollable pain and numbness in the leg, necessitating a diskectomy and improvement of the patient’s condition. A small number of individuals in our study require a decompressive laminectomy, and these patients gradually recover from their surgery and experience improved health during follow-up monitoring. After a laminectomy and fusion, spinal stenosis may manifest directly above or below the operative site. More spinal stenosis surgeries raise the risk of complications and spinal instability [28, 29]. For those with spinal stenosis, most medical specialists recommend against surgery. Surgical intervention for lumbar spinal stenosis usually reduces leg-specific discomfort, numbness, and weakness. Pain predominantly in the back may not respond well to surgery [30, 31]. Additionally, in this study, decompressive laminectomy, diskectomy, and foraminotomy managed the disk material and foraminal stenosis more effectively than endoscopic minimally invasive surgery, which had limited access to the spinal canal and spinal root foramen [32].
The results of this investigation shed light on the complex causes of back pain, with particular attention to disk prolapses, spinal stenosis, and the surgical methods used. These insights are essential for healthcare professionals who want to tailor interventions to each patient’s needs. The frequency of disk prolapse in our research is consistent with previous findings, highlighting the importance of L4-L5 and L5-S1 disks, and is consistent with trends worldwide. Although significantly higher in our sample (14%), the incidence of lumbar stenosis is consistent with published estimates. When it comes to controlling disc material and foraminal stenosis, our surgical approach—which prioritizes decompressive laminectomy, discectomy, and foraminotomy—works better than minimally invasive surgery. These results, which come from a particular community in Iraq, highlight the necessity for region-specific knowledge in treatment and add to the understanding of the etiology of back pain. The study’s ramifications go beyond influencing treatment choices to include bettering patient care and directing future research efforts, especially in diverse healthcare settings.
Recommendations and applications
The variety of reasons for back pain and the advanced surgical methods this study uncovered should be considered by healthcare professionals when formulating treatment plans. Optimizing therapy and patient care requires customizing therapies depending on individual features, such as the particular spinal level afflicted. Subsequent investigations must examine the varied forms of back discomfort and enhance surgical techniques to enhance results and minimize problems.
Conclusion
The lumbar disk degeneration is the most common cause of lower back pain. Males are more typically influenced by disk degeneration than females. Various disk levels are observed to be implicated per individual. Friction arthropathy, compression of the neural foramen, annular disk rupture, disk extrusion, disk herniation, spinal canal narrowing, and ligamentum flavum thickening are frequent at the L4 and L5 disk levels. Less usual conditions include spondylolisthesis and L1 and L2 disk involvement. MRI is the typical imaging method for identifying disk disorders because of its benefits, which include not requiring radioactivity, excellent spinal soft-tissue contrast, multiplanar imaging capability, and specific identification of intervertebral disc pathologies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of University of Babylon, Hammurabi College of Medicine Hammurabi (Code: IRB: HCM: 00231-21-AS-8/2019) criteria were closely followed during the consenting process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interests.
Acknowledgments
The authors gratefully appreciate the patients and relatives for their substantial assistance.
References
Low back pain (LBP) is a prevalent illness that often prompts people to seek health care, usually results in job loss, and can cause disability worldwide [1]. LBP is frequently accompanied by neuropathic manifestations, including nociceptive, non-specific, and other pain kinds [2, 3]. Though several diagnostic techniques are available, their usefulness is still debatable since there are numerous contributing factors to LBP and imaging and diagnostic injections are not particularly specific [2]. The intricacy of lower back pain, which influences both the pain’s perception and the disability it causes, is influenced by biology, psychology, and society [4].
Non-specific LBP
Most cases of non-specific LBP lack a well-defined anatomical cause [5]. The hallmarks of non-specific pain are diminished physical function and pain. More severe cases are also linked to a marked decline in mental and physical health, in addition to a higher chance for the development of chronic illness and death from all causes [6].
Distinction of buttock region
The buttock region, which spans from both iliac crests down to the gluteal folds, is physiologically distinct from LBP, even though the two can occasionally coexist and be misdiagnosed. The iliac crest is the final anatomical marker in the lower back, starting from the 12th rib. Most people will suffer from severe LBP at certain times during the disease in their lives. This is usually a transient but often chronic disorder. Studies show that one year following the onset of mechanical lower back pain, more than 60% of persons with the condition would still be in pain or would experience it often [7].
A thorough analysis of the lower back pain situation would help clinicians better understand the heterogeneity in LBP and its implications [8]. Only a small number of cohorts have been performed on the general pattern of back pain patients in Iraq and the surgical management of these individuals.
Prognosis of LBP
The prognosis for LBP differs based on the patient and the particulars of the pain. The majority of people with new LBP episodes recover in a few weeks, but recurrences are frequent, and people with chronic, long-term LBP typically have a more protracted course. The back pain episode, individual and psychological traits, and social and professional environments influence the prognosis of back pain. A small percentage of patients with acute LBP may become chronic, although the majority see quick improvements in pain and impairment within the first month. On the other hand, individuals with non-radicular persistent LBP that has recently started have a favorable prognosis and a good chance of improving [9, 10, 11].
Our objective in doing this study on Iraqi patients is to close a significant knowledge gap. Iraq has a high incidence of LBP cases; however, there has not been much thorough research on the patterns and surgical care of these patients. This study makes a valuable contribution by providing a distinct viewpoint on the intricacies of LBP etiologies exclusive to the Iraqi population. Secondly, we hope to offer Iraqi medical professionals insightful information to help them design efficient treatment plans. Additionally, by diversifying our understanding of back pain globally, the study guarantees that medical interventions are appropriate for various cultural and regional contexts.
Materials and Methods
Setting and participants
This cross-sectional study was piloted on 200 patients (90 females and 110 males) aged 30-50 years. They were selected randomly from those attending the outpatient clinic in Imam Alsadiq Teaching Hospital, Hilla, Iraq. The study took two years, from January 2017 to February 2019. The sample size of patients was chosen after careful evaluation of the goals of the investigation and the realistic limitations imposed by our research setting. This decision was made to balance the distinctiveness of our study population, logistical viability, and statistical robustness. A sample size of 200 patients is substantiated for several reasons. Firstly, to allow for a thorough analysis of the various etiologies of LBP common in our target demographic, given the extent of our inquiry into LBP patterns in a specific location. Secondly, to guarantee adequate statistical power, significant inferences must be made following accepted standards for cross-sectional research in comparable settings. Thirdly, to make it easier to characterize LBP cases in depth while considering our study environment’s unique clinical and demographic details. Lastly, we aim to improve the study’s validity and help make our findings more broadly applicable within the particular parameters of our inquiry.
Inclusion criteria
All patients in this study complained of (acute or chronic) lower back pain, whether it was associated with radicular pain. The study also included those who complained of back pain resulting from poor posture, muscle overuse, and sprains and strains with normal magnetic resonance imaging (MRI). Muscle spasms are diagnosed by normal MRI of the spine and by clinical examination [12, 13]. All patients were evaluated for clinical tests, radiological, and MRI scanning [14, 15].
Exclusion criteria
Thirteen patients provided inadequate demographic information, while 27 refused to cooperate and take part in the study, those who were not seen again after the first visit, those with previous spinal injuries, those who were poorly followed up, those with spinal congenital dysraphism, radiological and MRI data archives, and those with spinal tumors were excluded from this cohort [16].
Clinical and radiological evaluation
Experienced neurosurgeons, including the authors, performed a comprehensive assessment of the patients’ neurological condition, clinical presentations, and medical histories [15, 16]. Moreover, MRI analyses, which are essential for precise anatomical understanding, were carried out by knowledgeable radiologists [14-16]. These experts followed prescribed study criteria and used cutting-edge imaging methods to obtain exact information pertinent to LBP etiologies. The synergy between radiologists and neurosurgeons guaranteed a comprehensive strategy, integrating radiological and clinical viewpoints in the case selection procedure. Our goal is to strengthen the validity and credibility of the study by enhancing the transparency and dependability of our data collection methods and offering clarification on the competence of the professionals participating and the standardized processes followed.
Surgical interventions
Under general anesthesia, a laminectomy was carried out in a prone posture. A lower midline skin incision was made at the level of the involved spine, a subperiosteal gauze dissection was carried out, and gel foam and coagulation cauterization were used to secure the hemostasis. After the spinous process was removed using spinal rongeurs and punches, the involved vertebra underwent a bilateral laminectomy. The protruding disk material was then removed using pituitary forceps, and the surgical site was cleaned with gentamicin 80 mg mixed with normal saline [17]. The wound was then closed in layers, hemostasis was secured, the dressing was applied with antiseptics, and the redivac drain was left in for 24 hours after the procedure. Neurosurgery is indicated for definite conditions in our patient cohort, including single-level and multiple levels of disk prolapse, as well as spinal stenosis. A total of 40 patients (20 with L5S1 disk prolapse, 12 with L4, L10 disks prolapse, and 8 with L3, L8 disks prolapse) have single-level disk prolapse. Moreover, 20 patients (6 with L4, L5, S1 disk prolapse, 8 with L3, L4, L5 disks prolapse, and 6 with L2, L3, L4 disks prolapse) had several levels of disk prolapse. Additionally, there are 28 individuals with spinal stenosis (10 with L4, L5 stenoses, 8 with L3, L4, and L5 stenoses, and 10 with L5 S1 stenosis).
Statistical analyses
The study data were compiled into an Excel sheet, Microsoft Office (2017), and the percentages and numbers were sorted and computed appropriately.
Ethical clearance
The Hammurabi College of Medicine’s Review Committee’s ethical criteria were closely followed during the consenting process. Before giving written consent, the participants were guaranteed to be fully informed about the study’s goals, methods, and possible dangers. The emphasis on ethical principles, autonomy, and confidentiality highlights the strong ethical integrity upheld throughout the study. We hope to provide transparency and assurance about the ethical standards maintained in our research by outlining these procedures.
Results
In the current study, patients were classified as follows:
1) Degenerative spinal disorders affect 88 people; 40 cases with isolated disk prolapse; 20 patients suffer from multiple-level disk prolapse; 12 patients have L4, L5 disks prolapse; 8 patients have L3, L4 disks prolapse; and 20 patients have L5S1 disk prolapse. There are 6 patients with L4, 5, and S1 disk prolapse, 8 with L3, 4, and 5 with prolapse, and 6 with L2, 3, and 4. Additionally, there are 28 patients with lumber stenosis, 10 with L4, 5 stenoses, 8 with L3, 4, 5 stenoses, and 10 with L5, S1 stenosis.
2) Patients with mild disk prolapse make up 40.
3) Forty patients have normal lumbosacral spine MRIs but exhibit muscle spasms.
4) Twenty-six people experience back pain as a result of a laminectomy or a prior spinal operation.
A clear and organized presentation of the demographic data in Table 1 helps clarify possible factors linked to LBP in the group under study.
The representation was broad in terms of age groups. The mean age displayed a narrow range of ages with slight variation. The gender distribution shows a higher percentage of men (63.5%), offering a fair assessment of the effects of LBP on both sexes. The distribution of residences between rural and urban areas provides information about possible lifestyle or environmental issues. The occupational distribution sheds light on potential factors contributing to LBP by highlighting a significant proportion of heavy job workers (55%). The awareness of LBP across various lifestyles is enhanced by the range of jobs, which includes homemakers, retirees, and official workers. The smoking rate among LBP patients reveals a notable percentage of smokers (62.5%). Comorbid conditions such as type 2 diabetes, bronchial asthma, chronic obstructive pulmonary disease (COPD), and hypertension are listed, giving a thorough picture of the population under study’s health.
The numerous causes of back pain among the 200 study participants are briefly depicted in Table 2.
It gives a useful overview of the distribution of back pain etiologies in the population under study. It clearly and concisely breaks down the number of patients and the associated percentages for each cause. A more nuanced knowledge of the various variables causing back pain is provided by including categories such as spinal stenosis, muscle spasm, disc prolapse at different levels, and prior spinal procedures. These additions improve the study. According to the results, single-level disk prolapses, mild disk prolapses, and multiple-level disk prolapses account for half of the disc-related LBP.
Additionally common, accounting for 20% and 14% of cases, respectively, are spinal stenosis and muscular spasms. Remarkably, 13% of individuals have a history of prior spine procedures, including laminectomy. In 3% of cases, albeit less common, spinal tumors are found.
A targeted and detailed analysis of the number of patients with single-level disk prolapse at various spinal levels may be found in Table 3.
It effectively conveys the case distribution, showing that the L5, S1 level (20 patients) had the highest occurrence, followed by L4, L5 (12 patients), and L3, L4 (8 patients). There are forty individuals in total with single-level disk prolapse at all levels.
The number of patients with multiple-level disk prolapse at various spinal levels and the related percentages are effectively presented in Table 4.
Six patients (3%) at L4, 5, S1, 8(4%) at L3, 4, 5, and 6(3%) at L2, 3, and 4 have disk prolapse, according to the distribution. Notably, 10% of the patients, or 20, lack a recognized spinal level.
The distribution of patients with spinal stenosis at various spinal levels is clearly shown in Table 5.
It shows that spinal stenosis affects 10 patients (5%) at L4, 5, 8(4%) at L3, 4, 5, and 10(5%) at L5, S1. Of the total participants in the study, 28 cases of lumbar stenosis cumulatively occur throughout all indicated levels, accounting for 14% of the total.
A comprehensive summary of the surgical techniques used in the study, broken down by levels of stenosis and disk prolapse, may be found in Table 6.
Specific spinal levels correspond to each surgical method. The table shows the number of patients and matching percentages for each category.
Many techniques are covered by the surgical modalities, such as laminectomy, discectomy, foraminotomy, and their combinations. The percentages show how each surgical technique is distributed compared to other disc prolapse and stenosis levels.
Discussion
The thorough examination of the etiologies of back pain, the distribution of disc prolapses, and the surgical techniques offered in this survey offer important new information about the features of the patient group under study. A detailed presentation of the demographic data in Table 1 helps clarify possible factors linked to LBP in the group under study. Table 2 lists the many reasons why people have back pain, with disk problems, muscle spasms, and laminectomy being the main culprits. Interestingly, many patients involve disk prolapse at a single level. Tables 3 and 4 provide detailed information on single-level and multiple-level disk prolapse, respectively, and the prevalence at various spine levels. Table 5 provides information on spinal stenosis incidence, highlighting differences across lumbar levels. Table 6 comprehensively analyzes the various surgical techniques used to treat disk prolapse and stenosis at different spine levels. The results highlight the intricacy of the etiologies of back pain and the sophisticated surgical methods used to treat these ailments. To personalize interventions based on the unique characteristics of patients, healthcare providers need to have this detailed understanding. This solution will help to improve therapy and patient care.
The annual incidence of disk prolapse is around 5-20/1000 adults [18], with a male/female ratio 2:1 [19]. However, other studies have reported female preponderance [20]. Similar to our outcome, almost in all cases of lumbar disk herniation, the L4-L5 and L5-S1 disks were affected [21]. Of the total participants in the present study, 28 cases of lumbar stenosis cumulatively occur throughout all indicated levels, accounting for 14%. Other studies have suggested spinal lumber stenosis ranges from 1.7% to 13.1% [22]. In the United States, lumbar spinal stenosis disturbs approximately 11% of older people. Studies have exposed that while 20% of people over 60 have spinal stenosis evident on imaging examinations, more than 80% do not cause manifestations and do not require therapy [23].
Similar to the findings of this study, many common comorbidities, including cerebrovascular, respiratory, and cardiovascular disorders among patients with LBP, were also reported. Research has indicated a higher likelihood of certain comorbidities in people with LBP than in people without back pain. Furthermore, comorbidities have been linked to subpar treatment for LBP. Comprehending the connection between comorbidities and back pain is crucial for enhancing patient care and developing guidelines [24]. These results highlight how crucial it is to consider and manage comorbidities in LBP patients to provide thorough and efficient therapy.
Patients who report radicular discomfort associated with root compression and a single degree of disk prolapse are treated with decompressive laminectomy or discectomy combined with foraminotomy [12]. Viewing the spinal root intraoperatively is vital to assess the extent of root pressure from the bone (osteophyte) or disk material. This method was based on the intraoperative findings of root pressure from disk material or osteophytes. This procedure may be necessary to alleviate pressure on the roots and release the spinal root (de roofing) of the intervertebral foramina since some patients continue to experience radicular discomfort following surgery due to intraoperatively undetected root pressure. Through what is known as “neural foramina,” apertures in the spinal vertebrae allow a bundle of spinal nerves (spinal roots) to emerge from the spinal cord. Narrowing of the nerve root apertures may cause pressure on the nerve. This condition is known medically as foraminal spinal stenosis, and a foraminotomy is necessary to decompress it [13]. Foraminotomy surgery may be taken into consideration if symptoms are severe enough to interfere with daily activities [25]. Symptoms could be experienced as thigh, calf, or lower back pain. Deep and often persistent agony is experienced. Pain is experienced when using the body in a particular way or when carrying out specific actions—numbness, tingling, and weakening of the muscles. MRI to verify that the symptoms are caused by foraminal stenosis [26].
The cases of major lumbar disk herniation can be successfully treated non-surgically, despite a revision by U et al. [27]. However, care must be taken to ensure that subjects are checked for cauda equina syndrome and were fully informed about the necessity to seek medical attention immediately if red-flag symptoms appear. In the patient in our study, a lumber disk herniation results in excruciating, uncontrollable pain and numbness in the leg, necessitating a diskectomy and improvement of the patient’s condition. A small number of individuals in our study require a decompressive laminectomy, and these patients gradually recover from their surgery and experience improved health during follow-up monitoring. After a laminectomy and fusion, spinal stenosis may manifest directly above or below the operative site. More spinal stenosis surgeries raise the risk of complications and spinal instability [28, 29]. For those with spinal stenosis, most medical specialists recommend against surgery. Surgical intervention for lumbar spinal stenosis usually reduces leg-specific discomfort, numbness, and weakness. Pain predominantly in the back may not respond well to surgery [30, 31]. Additionally, in this study, decompressive laminectomy, diskectomy, and foraminotomy managed the disk material and foraminal stenosis more effectively than endoscopic minimally invasive surgery, which had limited access to the spinal canal and spinal root foramen [32].
The results of this investigation shed light on the complex causes of back pain, with particular attention to disk prolapses, spinal stenosis, and the surgical methods used. These insights are essential for healthcare professionals who want to tailor interventions to each patient’s needs. The frequency of disk prolapse in our research is consistent with previous findings, highlighting the importance of L4-L5 and L5-S1 disks, and is consistent with trends worldwide. Although significantly higher in our sample (14%), the incidence of lumbar stenosis is consistent with published estimates. When it comes to controlling disc material and foraminal stenosis, our surgical approach—which prioritizes decompressive laminectomy, discectomy, and foraminotomy—works better than minimally invasive surgery. These results, which come from a particular community in Iraq, highlight the necessity for region-specific knowledge in treatment and add to the understanding of the etiology of back pain. The study’s ramifications go beyond influencing treatment choices to include bettering patient care and directing future research efforts, especially in diverse healthcare settings.
Recommendations and applications
The variety of reasons for back pain and the advanced surgical methods this study uncovered should be considered by healthcare professionals when formulating treatment plans. Optimizing therapy and patient care requires customizing therapies depending on individual features, such as the particular spinal level afflicted. Subsequent investigations must examine the varied forms of back discomfort and enhance surgical techniques to enhance results and minimize problems.
Conclusion
The lumbar disk degeneration is the most common cause of lower back pain. Males are more typically influenced by disk degeneration than females. Various disk levels are observed to be implicated per individual. Friction arthropathy, compression of the neural foramen, annular disk rupture, disk extrusion, disk herniation, spinal canal narrowing, and ligamentum flavum thickening are frequent at the L4 and L5 disk levels. Less usual conditions include spondylolisthesis and L1 and L2 disk involvement. MRI is the typical imaging method for identifying disk disorders because of its benefits, which include not requiring radioactivity, excellent spinal soft-tissue contrast, multiplanar imaging capability, and specific identification of intervertebral disc pathologies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of University of Babylon, Hammurabi College of Medicine Hammurabi (Code: IRB: HCM: 00231-21-AS-8/2019) criteria were closely followed during the consenting process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interests.
Acknowledgments
The authors gratefully appreciate the patients and relatives for their substantial assistance.
References
- Franchini M, Salvatori M, Denoth F, Molinaro S, Pieroni S. Participation in low back pain management: It Is Time for the To-Be Scenarios in Digital Public Health. International Journal of Environmental Research and Public Health. 2022; 19(13):7805. [DOI:10.3390/ijerph19137805]
- Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. The Lancet. 2021; 398(10294):78-92. [DOI:10.1016/S0140-6736(21)00733-9] [PMID]
- Sheeran L, Sparkes V, Whatling G, Biggs P, Holt C. Identifying non-specific low back pain clinical subgroups from sitting and standing repositioning posture tasks using a novel Cardiff Dempster-Shafer Theory Classifier. Clinical Biomechanics. 2019; 70:237-44. [DOI:10.1016/j.clinbiomech.2019.10.004] [PMID]
- Simula AS, Malmivaara A, Booth N, Karppinen J. A classification-based approach to low back pain in primary care - protocol for a benchmarking controlled trial. BMC Family Practice. 2020; 21(1):61. [DOI:10.1186/s12875-020-01135-8] [PMID]
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet. 2017; 389(10070):736-47. [DOI:10.1016/S0140-6736(16)30970-9] [PMID]
- Briggs AM, Cross MJ, Hoy DG, Sànchez-Riera L, Blyth FM, Woolf AD, et al. Musculoskeletal health conditions represent a global threat to healthy aging: A report for the 2015 World Health Organization World Report on Ageing and Health. The Gerontologist. 2016; 56(Suppl 2):S243-55. [DOI:10.1093/geront/gnw002] [PMID]
- Itz CJ, Geurts JW, van Kleef M, Nelemans P. Clinical course of non-specific low back pain: A systematic review of prospective cohort studies set in primary care. European Journal of Pain. 2013; 17(1):5-15. [DOI:10.1002/j.1532-2149.2012.00170.x]
- Kongsted A, Kent P, Hestbaek L, Vach W. Patients with low back pain had distinct clinical course patterns that were typically neither complete recovery nor constant pain. A latent class analysis of longitudinal data. The Spine Journal. 2015; 15(5):885-94. [DOI:10.1016/j.spinee.2015.02.012] [PMID]
- Stochkendahl MJ, Kjaer P, Hartvigsen J, Kongsted A, Aaboe J, Andersen M, et al. National clinical guidelines for non-surgical treatment of patients with recent onset low back pain or lumbar radiculopathy. European Spine Journal. 2018; 27(1):60-75. [DOI:10.1007/s00586-017-5099-2] [PMID]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392(10159):1789-858. [DOI:10.1016/S0140-6736(18)32279-7] [PMID]
- da C Menezes Costa L, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO. The prognosis of acute and persistent low-back pain: A meta-analysis. CMAJ : Canadian Medical Association journal. 2012; 184(11):E613-24. [DOI:10.1503/cmaj.111271] [PMID]
- Lee S, Lee JW, Yeom JS, Kim KJ, Kim HJ, Chung SK, et al. A practical MRI grading system for lumbar foraminal stenosis. AJR. American Journal of Roentgenology. 2010; 194(4):1095-8. [DOI:10.2214/AJR.09.2772] [PMID]
- Rydevik B, Brown MD, Lundborg G. Pathoanatomy and pathophysiology of nerve root compression. Spine (Phila Pa 1976). 1984; 9(1):7-15. [DOI:10.1097/00007632-198401000-00004] [PMID]
- Rao D, Scuderi G, Scuderi C, Grewal R, Sandhu SJ. The use of imaging in management of patients with low back pain. Journal of Clinical Imaging Science. 2018; 8:30. [DOI:10.4103/jcis.JCIS_16_18] [PMID]
- Yang H, Liu H, Li Z, Zhang K, Wang J, Wang H, et al. Low back pain associated with lumbar disc herniation: Role of moderately degenerative disc and annulus fibrous tears. International Journal of Clinical and Experimental Medicine. 2015; 8(2):1634-44. [PMID]
- Amundsen PA, Evans DW, Rajendran D, Bright P, Bjørkli T, Eldridge S, et al. Inclusion and exclusion criteria used in non-specific low back pain trials: A review of randomised controlled trials published between 2006 and 2012. BMC Musculoskeletal Disorders. 2018; 19(1):113. [DOI:10.1186/s12891-018-2034-6] [PMID]
- Agrawal A, Ramachandraiah MK, Shanthappa AH, Agarawal S. Effectiveness of gentamicin wound irrigation in preventing surgical site infection during lumbar spine surgery: A retrospective study at a rural teaching hospital in India. Cureus. 2023; 15(9):e46094. [DOI:10.7759/cureus.46094]
- McGill S. Low back disorders: Evidence based prevention and rehabilitation. Champaign: Human Kinetics; 2007. [Link]
- Manchikanti L, Abdi S, Atluri S, Benyamin RM, Boswell MV, Buenaventura RM, et al. An update of comprehensive evidence-based guidelines for interventional techniques in chronic spinal pain. Part II: Guidance and recommendations. Pain Physician. 2013; 16(2 Suppl):S49-283. [PMID]
- Mattiuzzi C, Lippi G, Bovo C. Current epidemiology of low back pain. Journal of Hospital Management and Health Policy. 2020; 4. [DOI:10.21037/jhmhp-20-17]
- Al Qaraghli MI, De Jesus O. Lumbar disc herniation. Treasure Island: StatPearls; 2024. [Link]
- Wu AM, Zou F, Cao Y, Xia DD, He W, Zhu B, et al. Lumbar spinal stenosis: An update on the epidemiology, diagnosis and treatment. AME Medical Journal. 2017; 2(5). [DOI:10.21037/amj.2017.04.13]
- Walter KL, O’Toole JE. Lumbar spinal stenosis. JAMA. 2022; 328(3):310. [DOI:10.1001/jama.2022.6137] [PMID]
- Ramanathan S, Hibbert P, Wiles L, Maher CG, Runciman W. What is the association between the presence of comorbidities and the appropriateness of care for low back pain? A population-based medical record review study. BMC Musculoskeletal Disorders. 2018; 19(1):391. [DOI:10.1186/s12891-018-2316-z] [PMID]
- Hasegawa T, An HS, Haughton VM, Nowicki BH. Lumbar foraminal stenosis: Critical heights of the intervertebral discs and foramina. A cryomicrotome study in cadavera. The Journal of Bone and Joint Surgery. American volume. 1995; 77(1):32-8. [DOI:10.2106/00004623-199501000-00005] [PMID]
- Kalichman L, Cole R, Kim DH, Li L, Suri P, Guermazi A, et al. Spinal stenosis prevalence and association with symptoms: The Framingham Study. The Spine Journal. 2009; 9(7):545-50. [DOI:10.1016/j.spinee.2009.03.005] [PMID]
- U ECY, Shetty A, Craig PRS, Chitgopkar SD. An observation of massive lumbar disc prolapse.Journal of Spine Surgery. 2018; 4(3):583-7. [DOI:10.21037/jss.2018.07.12] [PMID]
- O’Sullivan PB. Lumbar segmental ‘instability’: Clinical presentation and specific stabilizing exercise management. Manual Therapy. 2000; 5(1):2-12. [DOI:10.1054/math.1999.0213] [PMID]
- Al-Hindy HA, Al-Mumin AS, Mousa MJ. Association of dental caries in the era of COVID-19 with the number of occluded coronary vessels: A non-traditional risk factor in patients with acute coronary syndrome. Journal of Emergency Medicine, Trauma & Acute Care. 2023; 2023(3):8.[DOI:10.5339/jemtac.2023.midc.8]
- Williamson E, White L, Rushton A. A survey of post-operative management for patients following first-time lumbar discectomy. European Spine Journal. 2007; 16(6):795-802. [DOI:10.1007/s00586-006-0207-8] [PMID]
- Fadheel QJ, Naser RT, Al-Hindy HA. Evaluation of practice of prescribing and monitoring anticoagulants among hospitalized Iraqi patients. HIV Nursing. 2022; 22(1):71-6. [Link]
- Kleinpeter G, Markowitsch MM, Böck F. Percutaneous endoscopic lumbar discectomy: Minimally invasive, but perhaps only minimally useful? Surgical Neurology. 1995; 43(6):534-9; discussion 40-1. [DOI:10.1016/0090-3019(95)00051-8] [PMID]
Article type: Original Research Articles |
Subject:
chronic pain
Received: 2024/01/16 | Accepted: 2024/03/12 | Published: 2024/12/20
Received: 2024/01/16 | Accepted: 2024/03/12 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
