
988368
Wed, May 27, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 43-52 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Homaie Rad E, Shirazikhah M, Shirazikhah A, Sajadi H S. Inequality in Access to Rehabilitation Services for People With Disability Across Iran. Iranian Rehabilitation Journal 2025; 23 (1) :43-52
URL: http://irj.uswr.ac.ir/article-1-2213-en.html
URL: http://irj.uswr.ac.ir/article-1-2213-en.html



1- Social Determinants of Health Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran.
2- Social Determinants of Health Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Knowledge Utilization Research Center, University Research & Development Center, Tehran University of Medical Sciences, Tehran, Iran.
2- Social Determinants of Health Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Knowledge Utilization Research Center, University Research & Development Center, Tehran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 502 kb]
(1065 Downloads)
| Abstract (HTML) (3317 Views)
Full-Text: (707 Views)
Introduction
Achieving universal health coverage (UHC), a key target of sustainable development goals, is essential for ensuring that health systems do not leave anyone behind in accessing quality health services. The health system cannot meet this target without focusing on vulnerable groups, including people with disabilities (PWDs). PWD are primarily poor, face widespread stigma, and often face a range of exclusions, including employment and education [1]. They are also more likely to experience poor health. They will have a greater need for health care in general and rehabilitation services in particular, including a wide range of diagnostic, therapeutic, and surgical services and rehabilitation assistive technologies to improve PWD’s performance [2]. Therefore, more focus on PWD is essential to achieve UHC, mainly since they constitute 16% of the global population [3], are often not fully covered by health services [4], and are vulnerable to financial hardship [5].
Despite the importance of considering PWD’s health needs, many health systems, particularly in middle- and low-income countries, have restricted capacity to provide the services PWD need, causing failure to meet the needs of PWD effectively and fairly. For instance, fewer than ten skilled rehabilitation physicians per million people in these countries [6] and only between 5% and 15% of people needing assistive devices have received them [2, 7]. Lack of access to services and inequality in receiving the required services, in combination with other underlying factors (such as sex and age), make PWD the most marginalized group [8, 9] that has an unpleasant experience with their disorder [2]. Many adverse health outcomes of PWD are not solely attributable to their underlying health conditions or impairments. However, they result from health inequities stemming from societal and health system injustices. These factors are referred to as health inequalities. A global report on health equity for PWD reported that despite substantial progress in many countries, the world is still far from realizing the right to the highest attainable level of health for PWD [3]. Inequality to access health worsened for PWD during and after the COVID-19 pandemic [10].
A recent review of barriers hindering equitable access to healthcare services for PWD has identified various obstacles globally, spanning different levels of the health system (e.g. healthcare costs, insufficiently trained healthcare professionals, challenges in delivering inclusive and coordinated services) and broader contributing factors to health inequities beyond the healthcare system (e.g. societal stigma, health literacy) [11]. Therefore, to achieve UHC, health systems must address these barriers through policies and reforms. More investment in health equity for PWD through stronger intersectoral collaboration is an obligation of the health system to promote health equity for PWD and advance global health priorities [3].
Approximately 12 million PWD are estimated to live in the Islamic Republic of Iran. Iran has undertaken several initiatives to improve PWD access to health services. These efforts led to significant improvements in PWD’s health status. Nevertheless, there are several challenges to fair access to healthcare. For instance, while an average of approximately 28.1% of PWD did not have access to the required rehabilitation services, those living in poorer provinces had more needs and less access to required rehabilitation services [12]. It has also been reported that there is inequality in the utilization of rehabilitation services in favor of wealthy Iranian households, and low-income households have less access to these services [13]. The wealth index was the most significant contributor (94.22%) to the observed socioeconomic inequalities in the use of rehabilitation services among PWD [14]. These inequalities are avoidable differences caused by many factors, including the distribution of health resources. Health resources and infrastructure are either in short supply or are distributed unequally between health needs and geographical regions. For instance, the rehabilitation bed density is 0.1 per 100000 people (compared to the standard of 6 per 100000), all located in cities [15]. It is worth noting that additional difficulties in accessing health services emerged for PWD due to sanctions. Recent sanctions have overshadowed the accessibility of medicine and assistance technologies to Iranians with disabilities and created countless problems [16]. In addition to sanctions, the COVID-19 pandemic has created more obstacles for PWD to access the health services they need. Hence, given the emphasis on eliminating inequalities [17, 18], it is necessary to take the required collaborative actions to reduce inequalities in access to health services for PWD.
Examining the extent of disparities in access to health services is an essential initial step in comprehending the scope of the issue and establishing a baseline for monitoring and evaluating measures to reduce inequality. However, there is limited evidence in Iran, particularly at the national level. Therefore, this study examined inequality in PWD’s access to physical rehabilitation services in Iran. Identifying the scope and nature of these disparities will enable policymakers to select suitable interventions.
Materials and Methods
Data source
The present study used Iran’s access to physical rehabilitation services survey (IAPRSS) data. The IAPRSS was a population-based cross-sectional survey conducted in 2019. Four validated questionnaires were used to collect the data. The demographic status of each PWD, type of disability, housing and living conditions, job, and income status were also gathered. The first questionnaire was about deprivation of access to rehabilitation services (DARS). Shirazikhah et al. developed and validated a questionnaire [19]. It has 17 Likert-type questions in four dimensions: Affordability (six questions), transport (five questions), social support (three questions), and information (three questions), with five answering options: Never, rarely, sometimes, often, and always. The selection of “always” meant more significant DARS. The second questionnaire was the World Health Organization (WHO) standard responsiveness questionnaire, which had seven domains, including prompt attention, dignity, choice, autonomy, confidentiality, communication, and basic amenities, with 35 Likert-type questions. Previous studies have examined the validity and reliability of questionnaires for PWD [20, 21].
The last two questionnaires were the Persian versions of activities of daily living (ADL) and instrumental activities of daily living (IADL). With eight questions, ADL assesses basic daily tasks typically performed by individuals, such as bathing, dressing, eating, toileting, transferring, self-care, walking and continence. These activities are vital for maintaining independence and function in daily life. On the other hand, the IADL, with seven questions, assesses more complex activities necessary for community-independent living. These activities include managing finances, shopping, meal preparation, housekeeping, transportation, medications, and effective communication. Previous studies examined the reliability and validity of the Persian versions of ADL and IADL [22].
Sample selection
The IAPRSS utilized a multistage cluster sampling method to gather nationwide data. The number of sample zones was determined by dividing the country into four zones based on the level of development and population distribution in each zone [23]. Two provinces were selected from each zone using systematic sampling. Subsequently, households in each province were randomly chosen. The total sample size of IAPRSS was 2177, with 2146 PWD responding to the survey. In this study, we analyzed data from 2117 PWD.
Study variables
While IAPRSS has different variables, we chose some variables for our analysis, including sex, age, marital status, literacy, employment, and the type of rehabilitation service PWD need as socioeconomic status (SES) variables. The Mean±SD of the scores of DARS and its four dimensions were also included. We converted the original survey scores between 0 and 100, with higher scores indicating more significant DARS. We also used the ADL score as a standard indicator to assess the level of independence of individuals as a proxy variable for the need for rehabilitation services in PWD. We also calculated the wealth index to rank SES. The wealth index was calculated using a set of questions included in the demographic questions. We calculated the wealth index for each household using principal component analysis [24] and household living asset data.
Data analysis
This study calculated inequality using the GINI index and Lorenz curves. The GINI measures disparities in social and economic studies and health distribution without considering their needs. The GINI coefficient ranges from 0 to 1, where 0 indicates equal distribution and 1 indicates total inequality. The present study calculated the GINI index for the DARS scores.
The GINI was calculated as Equation 1:
ri is the DARS score of person i and rj is the DARS score of person j. µ is the average DARS score in total samples, n is the sample size, a and b are=2.
Previous studies showed that PWD with severe disabilities and those who are poor may require more rehabilitation services [12-14]. The GINI index calculates inequality without considering needs or SES. Therefore, the GINI index cannot provide accurate results for inequity. Therefore, we used the concentration index (CI) to calculate inequity. We calculated inequity by ranking DARS based on ADL score and wealth index. CI range is between +1 and -1, in which negative values indicate that the DARS is intense among PWD with low SES or PWD with severe disability (low ADL score). Positive values indicate that the DARS is concentrated among PWD with high SES or PWD with weak disability (high ADL score). The measurement scale is a crucial criterion for selecting the method for calculating CI and GINI. The use of general CI and GINI estimators may have led to bias. In this study, the DARS scores were bounded and counted; therefore, we used the Erreygers [25] CI and GINI indices to avoid bias.
GINI and CI provide holistic and comparable results that can be used for interpretation and decision-making. These indices help compare the disparity findings between different studies and provide valid, flexible, and precise results [26].
Finally, a regression model was used to determine the causes of inequality in DARS scores. In the regression model, we used wealth and ADL scores, age, and education status as explanatory variables (because these factors may affect the inequity in DARS) and DARS as the dependent variable. Data were analyzed using STATA SE software, version 13.1.
Results
Of 2117 PWD, 996(47.0%) were women. Among them, 1172(55.4%) were married, 917(43.3%) were single, and some chose not to disclose their marital status. The mean age of the participants was 44.6±0.4 years. Additionally, 1184 of 2098 participants (56.4%) were not economically active. Among the 2124 participants, 281(13.2%) were illiterate, 1225(57.7%) had less than a high school degree, and the remaining held an academic degree. Furthermore, 909 participants (42.4%) required physiotherapy, 243(11.3%) required occupational therapy, 155(7.2%) required speech therapy, 320(14.9%) required audiology services, 449(20.9%) required optometry services, and 327(15.3%) required orthotic and prosthetic services.
Table 1 presents the DARS scores and GINI index for DARS.
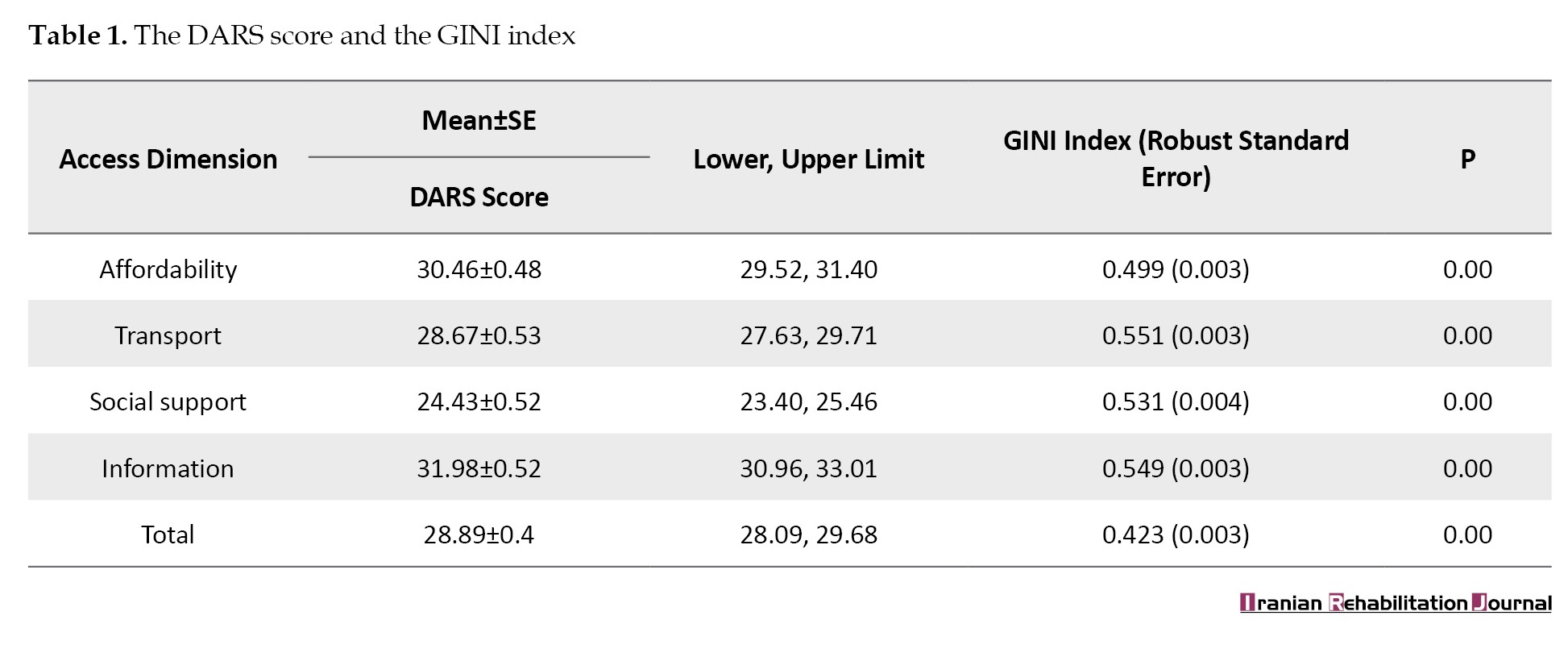
According to the Table 1, the overall DARS score averages 28.89±0.40. The highest score was observed in the information dimension at 31.98±0.52, while the lowest was in the social support dimension at 24.43±0.52. The overall GINI index for the DARS was 0.423±0.003. The highest GINI index was observed in the transport dimension at 0.551±0.003, while the lowest was associated with affordability at 0.499±0.003.
Table 2 presents the CI results for the DARS scores, considering ADL as a proxy variable for need.
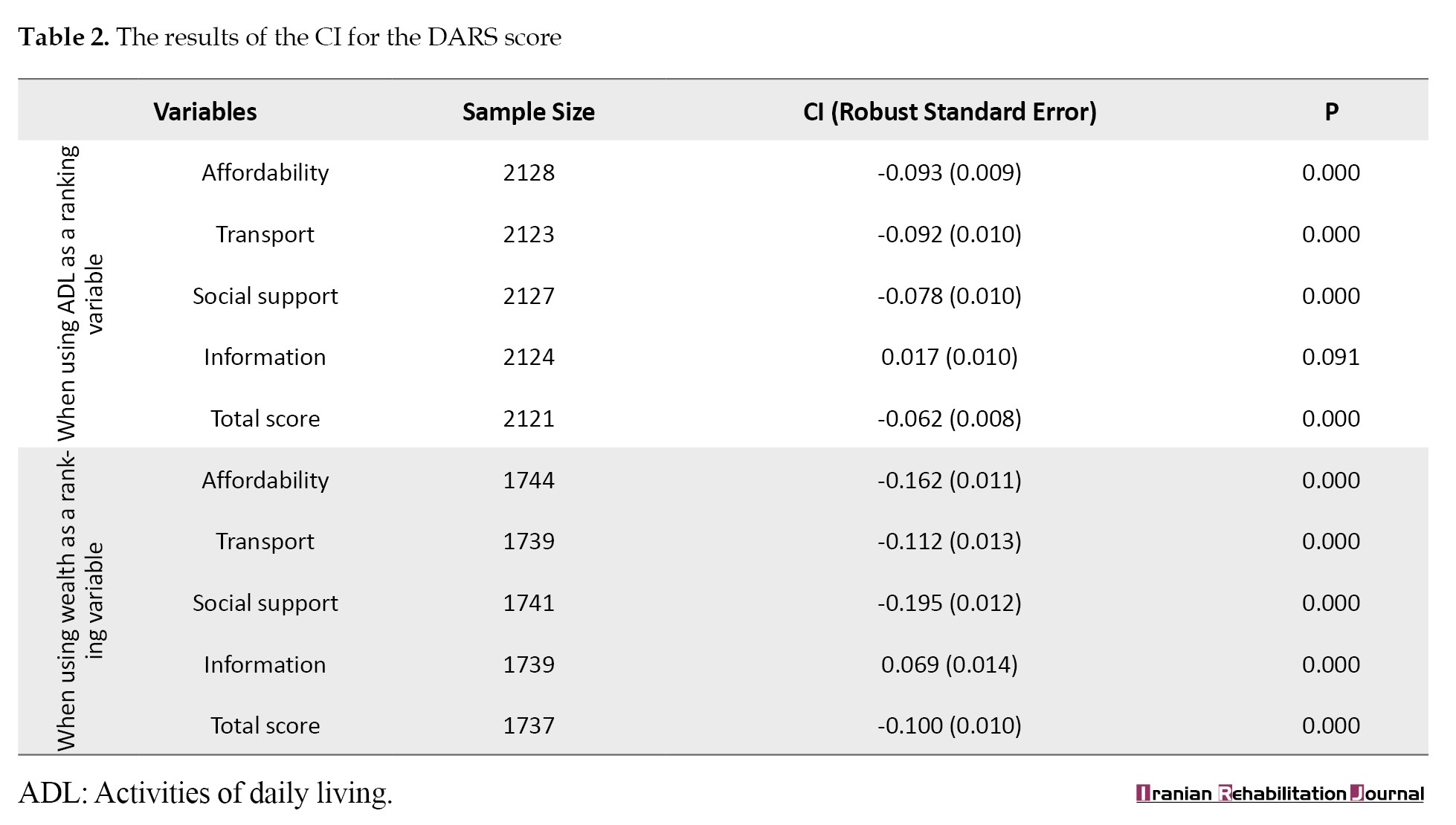
The CI for affordability, transport, and social support deprivation showed that PWD with higher ADL scores had less deprivation in these dimensions (-0.093±0.009; -0.092±0.010; -0.062±0.010). The CI for DARS is -0.062±0.008, indicating that PWD with lower ADL scores had more deprivation in access to rehabilitation services.
Considering the wealth index as the ranking variable, the CI is positive only for the information dimension 0.069±0.014, showing more information deprivation for PWD with high SES. The deprivation of affordability was -0.162±0.011, indicating that the rich had a lower affordability deprivation. The CI for the total DARS score was -0.100±0.010, showing better access to rehabilitation services for PWD with a better SES.
Table 3 presents the CI results regarding sex and the type of rehabilitation service that PWDs need.
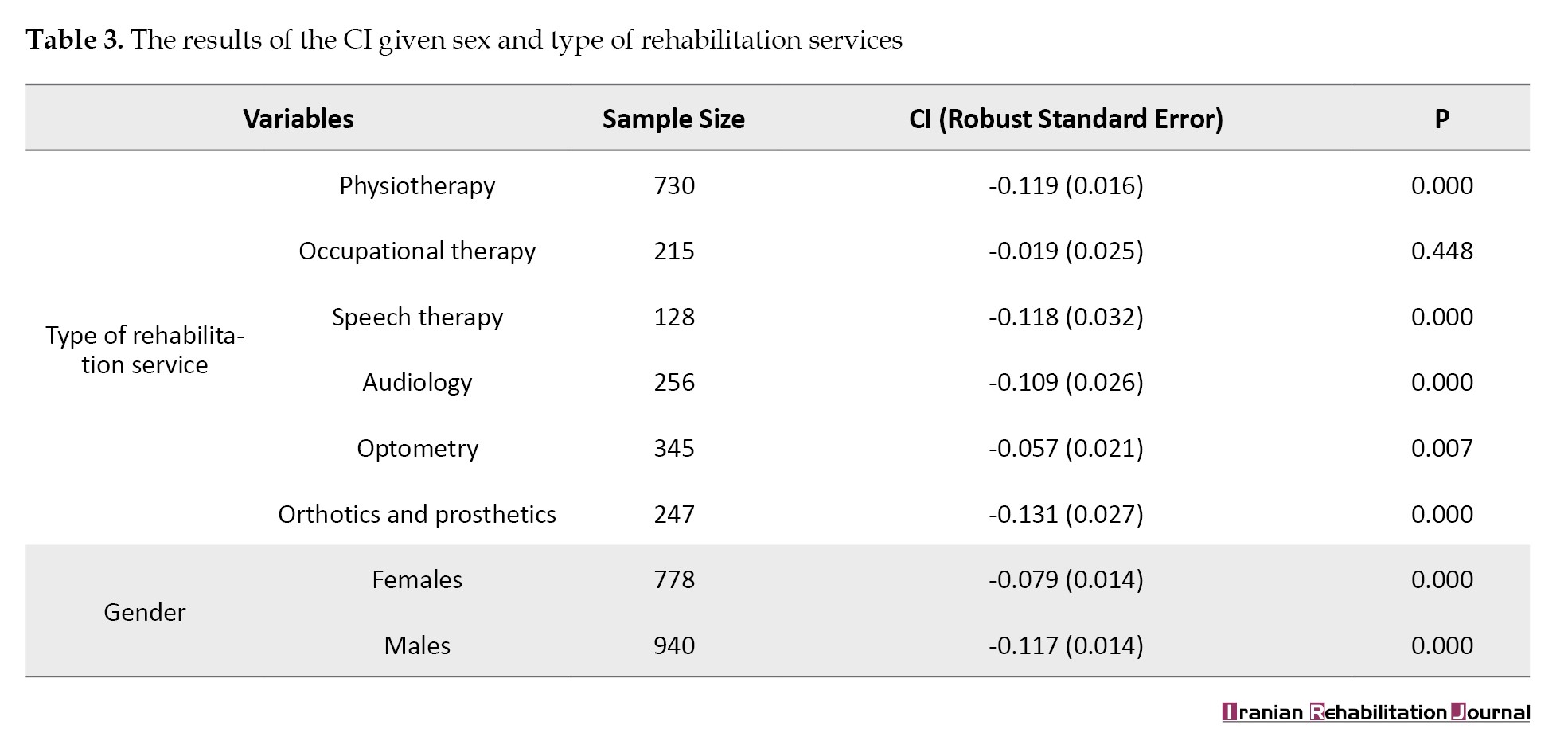
As shown in the Table 3, the CI was higher for orthotics and prosthetics services -0.131±0.027, indicating that the inequity of accessibility was higher in this type of rehabilitation service. In addition, inequity of accessibility was greater among men -0.117±0.014.
Table 4 presents the results of the regression model.
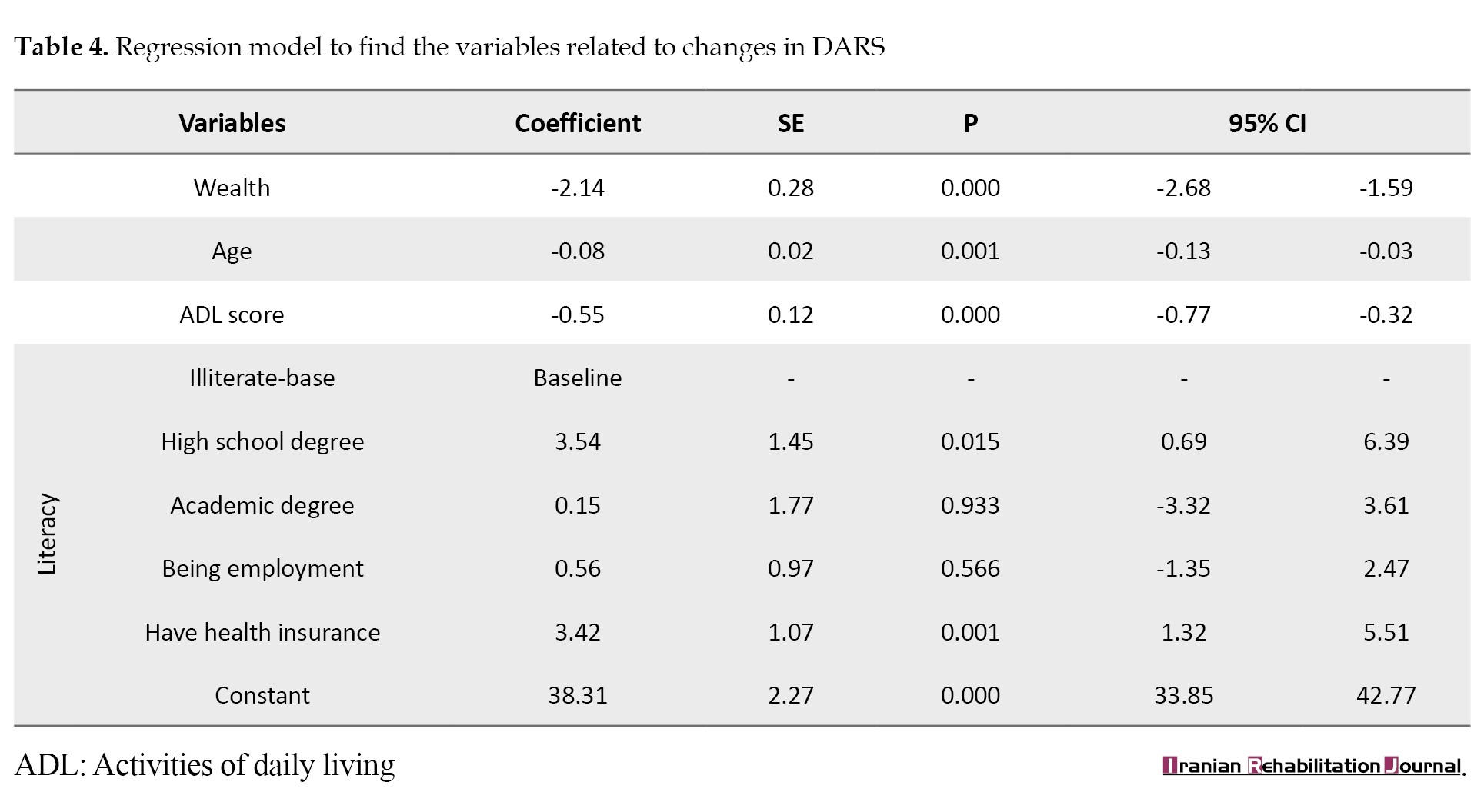
Regarding the wealth coefficient, PWD who were rich (coefficient=-2.14, %95 CI, -2.68%, -1.59%), younger (coefficient=-0.08, %95 CI, -0.775%, -0.32%) and had higher ADL scores (coefficient=-0.55, %95 CI, -0.77% -0.32%) had lower DARS scores. PWD with high school degrees (coefficient=3.54, 95 CI, 0.69%, 6.39%) and without health insurance coverage (coefficient=3.42, %95 CI, 1.32%, 5.51%) had higher DARS scores.
Discussion
This study investigated disparities in access to physical rehabilitation services among PWDs in a low-to-middle-income country, emphasizing the importance of planning and ensuring equitable access to rehabilitation services.
The results indicated that PWD encounter challenges when accessing rehabilitation services, particularly when seeking information about their required health and financial resources. Recent reviews highlighted that inadequate access to health information and financial support constitutes significant barriers for PWD seeking health services [27, 28]. Additionally, Sajadi et al. reported that accessing health information is a fundamental challenge for PWD during the COVID-19 pandemic. The WHO reports that over half of PWD face barriers to accessing health services due to financial constraints. However, these access challenges vary across low-income, medium-income, and high-income countries [29].
The results revealed significant disparities in access to rehabilitation services, raising considerable concerns. According to the global report on health equity for PWDs [3], health inequity is a pervasive challenge worldwide. Despite substantial advancements in numerous countries to mitigate this issue, many PWDs continue to encounter barriers to accessing necessary health services. This problem has been exacerbated after COVID-19 [10] and is particularly acute in Iran due to sanctions [16]. Consequently, immediate action is imperative to address these health disparities among PWDs, which entails progressing toward the universal realization of the right to the highest attainable standard of health for all. Paramount to this endeavor is to establish a national registry or database system for the systematic collection, analysis, interpretation, and utilization of data [30]. This system identifies PWD and their health needs, ensuring they receive timely and appropriate services. The recent national action plan for rehabilitation services in Iran outlines several interventions to reduce health disparities among PWDs [31]. It is anticipated that the effective implementation of this plan will ensure that no PWDs are excluded from receiving the necessary services. To develop targeted plans to reduce disparities in health access, particularly in rehabilitation, it is crucial to identify the primary drivers of these disparities. Our results highlight several key factors.
This study highlights disparities in access to rehabilitation services among PWD with severe impairments. This result is consistent with previous research by Sakellariouv and Rotarou, who demonstrated that people with severe disabilities face higher odds of encountering unmet needs [32]. When considering different dimensions of access, inequality seems to be minor regarding information for PWDs with severe disabilities. This suggests that these individuals may have better access to information through support organizations like the Iranian Welfare Organization but still face many other barriers. Therefore, it is crucial to develop specific interventions that identify and provide health services based on the needs of PWD.
Moreover, the results revealed pronounced disparities in access to diverse rehabilitation services, particularly orthotics and prosthetics. Previous research has also documented inequities in the availability of orthotic and prosthetic devices and related services [33, 34]. These disparities within the Iranian context may stem from the relatively elevated costs associated with orthotics and prosthetics compared to other rehabilitation services. Furthermore, a significant proportion of these services remain uncovered by health insurance packages, exacerbating financial challenges for persons with disabilities seeking access to them [35]. This underscores the imperative for enhanced efforts to expand coverage of rehabilitation services, considering cost-effectiveness analysis.
Our study revealed disparities in access to rehabilitation services among PWD lacking insurance coverage. These results are consistent with previous research that underscores the pivotal role of insurance coverage in determining health access for PWD [36]. Uninsured PWDs are more likely to have limited access to health services. In light of the national commitment to achieving UHC, targeted measures should be implemented to enhance adequate coverage of PWD, particularly in rehabilitation care.
SES analysis revealed significant disparities in access to rehabilitation services. These disparities are more pronounced in men than in women, individuals with lower educational attainment compared to those with higher education, older adults versus younger individuals, and PWD facing economic hardship compared to those in higher economic groups. Scholars have documented the critical role of SES in perpetuating health inequalities among PWD [37, 38]. Although previous studies have reported more significant disparities among women [40, 41], our results are contradictory. This gender-based disparity may stem from several factors. For instance, men may be less inclined to seek health services [42]. Additionally, health systems may inadvertently offer services that are more accessible to women [43].
Consistent with previous work, education, age, and economic status were identified as drivers of inequality in access to health services among PWD [28, 36, 37]. Regarding educational status, PWD with low educational levels had more difficulty accessing rehabilitation services. Lower educational attainment can impede health literacy, reduce awareness of available services, and complicate the navigation of healthcare systems. Furthermore, educational disparities often intersect with socioeconomic factors, further exacerbating inequities in less-educated PWD.
Regarding age differences, our study indicated that older adults face more significant challenges in accessing rehabilitation services than their younger counterparts. Accumulated health conditions and disabilities over time necessitate a more comprehensive rehabilitation program for older adults. Additionally, age-related mobility limitations or cognitive decline can impede the ability to effectively seek and utilize services.
Regarding income levels, we found that PWD from lower-income backgrounds encountered more disproportionate challenges than those from higher-income backgrounds. Low-income levels may result in limited access to essential resources, such as quality education and comprehensive healthcare, financial constraints that restrict their ability to afford necessary treatments or medications, and institutional barriers within the healthcare system that predominantly affect economically disadvantaged groups. Moreover, these communities may have limited access to information regarding available services and fewer advocacy opportunities, further intensifying inequities in-service distribution.
Efforts to reduce SES-related disparities in rehabilitation services for PWD should focus on policy reforms that enhance service accessibility and educational initiatives that improve health literacy among economically disadvantaged groups. Adopting approaches, such as the intersectional perspective, can be instrumental in identifying the most vulnerable groups and devising strategic plans to meet their specific needs [44]. Policymakers and healthcare practitioners must consider these insights when crafting inclusive rehabilitation programs to guarantee equitable access to PWD.
This study has some limitations. We analyzed the results using aggregated scores, such as GINI and CI, which were insufficient for detailed interpretation. The GINI and CI provide aggregated outcomes for calculating health and health service utilization inequity. The results are suitable for comparison studies; however, as aggregated outcomes are limited, they cannot be used for detailed analyses and interventions. Another limitation is that the study was related to its cross-sectional nature. Therefore, it is better to include the time of injury as an effective factor for ADL. We did not have access to the time variable and added it to the regression model. However, as we used ADL as the proxy variable for need, it was not crucial to add time as an explanatory variable for ADL.
Conclusion
In recent years, numerous initiatives have been undertaken to improve access to health for PWD, yet disparities in care persist in many low-income and middle-income countries. Advancing equity requires recognizing the drivers of these disparities and addressing them through health reforms and policies. This study revealed inequities in access to rehabilitation services, particularly among those with severe impairments, orthotics, and prosthetics, as well as among uninsured individuals. The disparities are more pronounced among men than women, individuals with lower educational levels versus those with higher education, older adults relative to younger people, and PWD experiencing economic hardship compared to those with higher economic levels. Policymakers are urged to consider these factors when developing health plans to tackle equity challenges and ensure equitable healthcare for all, especially disadvantaged groups. These results can be instrumental in planning purposes in similar contexts.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committees of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1400.059)
Funding
This research was supported by the research project funded by the University of Social Welfare and Rehabilitation Sciences University, Tehran, Iran (Project No.: 2600).
Authors' contributions
Project administration and funding acquisition: Marzieh Shirazikhah; Supervision: Haniye Sadat Sajadi; Conceptualization and validation: Enayatollah Homaie Rad, Marzieh Shirazikhah, and Haniye Sadat Sajadi; Software, data collection, Visualization and formal analysis: Enayatollah Homaie Rad; Writing the original draft: Enayatollah Homaie Rad and Haniye Sadat Sajadi; Methodology, resources, investigation, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank other contributors to the study who did not add themselves as authors. The University of Social Welfare and Rehabilitation Sciences, Tehran, Iran is appreciated for the financial support.
References
Achieving universal health coverage (UHC), a key target of sustainable development goals, is essential for ensuring that health systems do not leave anyone behind in accessing quality health services. The health system cannot meet this target without focusing on vulnerable groups, including people with disabilities (PWDs). PWD are primarily poor, face widespread stigma, and often face a range of exclusions, including employment and education [1]. They are also more likely to experience poor health. They will have a greater need for health care in general and rehabilitation services in particular, including a wide range of diagnostic, therapeutic, and surgical services and rehabilitation assistive technologies to improve PWD’s performance [2]. Therefore, more focus on PWD is essential to achieve UHC, mainly since they constitute 16% of the global population [3], are often not fully covered by health services [4], and are vulnerable to financial hardship [5].
Despite the importance of considering PWD’s health needs, many health systems, particularly in middle- and low-income countries, have restricted capacity to provide the services PWD need, causing failure to meet the needs of PWD effectively and fairly. For instance, fewer than ten skilled rehabilitation physicians per million people in these countries [6] and only between 5% and 15% of people needing assistive devices have received them [2, 7]. Lack of access to services and inequality in receiving the required services, in combination with other underlying factors (such as sex and age), make PWD the most marginalized group [8, 9] that has an unpleasant experience with their disorder [2]. Many adverse health outcomes of PWD are not solely attributable to their underlying health conditions or impairments. However, they result from health inequities stemming from societal and health system injustices. These factors are referred to as health inequalities. A global report on health equity for PWD reported that despite substantial progress in many countries, the world is still far from realizing the right to the highest attainable level of health for PWD [3]. Inequality to access health worsened for PWD during and after the COVID-19 pandemic [10].
A recent review of barriers hindering equitable access to healthcare services for PWD has identified various obstacles globally, spanning different levels of the health system (e.g. healthcare costs, insufficiently trained healthcare professionals, challenges in delivering inclusive and coordinated services) and broader contributing factors to health inequities beyond the healthcare system (e.g. societal stigma, health literacy) [11]. Therefore, to achieve UHC, health systems must address these barriers through policies and reforms. More investment in health equity for PWD through stronger intersectoral collaboration is an obligation of the health system to promote health equity for PWD and advance global health priorities [3].
Approximately 12 million PWD are estimated to live in the Islamic Republic of Iran. Iran has undertaken several initiatives to improve PWD access to health services. These efforts led to significant improvements in PWD’s health status. Nevertheless, there are several challenges to fair access to healthcare. For instance, while an average of approximately 28.1% of PWD did not have access to the required rehabilitation services, those living in poorer provinces had more needs and less access to required rehabilitation services [12]. It has also been reported that there is inequality in the utilization of rehabilitation services in favor of wealthy Iranian households, and low-income households have less access to these services [13]. The wealth index was the most significant contributor (94.22%) to the observed socioeconomic inequalities in the use of rehabilitation services among PWD [14]. These inequalities are avoidable differences caused by many factors, including the distribution of health resources. Health resources and infrastructure are either in short supply or are distributed unequally between health needs and geographical regions. For instance, the rehabilitation bed density is 0.1 per 100000 people (compared to the standard of 6 per 100000), all located in cities [15]. It is worth noting that additional difficulties in accessing health services emerged for PWD due to sanctions. Recent sanctions have overshadowed the accessibility of medicine and assistance technologies to Iranians with disabilities and created countless problems [16]. In addition to sanctions, the COVID-19 pandemic has created more obstacles for PWD to access the health services they need. Hence, given the emphasis on eliminating inequalities [17, 18], it is necessary to take the required collaborative actions to reduce inequalities in access to health services for PWD.
Examining the extent of disparities in access to health services is an essential initial step in comprehending the scope of the issue and establishing a baseline for monitoring and evaluating measures to reduce inequality. However, there is limited evidence in Iran, particularly at the national level. Therefore, this study examined inequality in PWD’s access to physical rehabilitation services in Iran. Identifying the scope and nature of these disparities will enable policymakers to select suitable interventions.
Materials and Methods
Data source
The present study used Iran’s access to physical rehabilitation services survey (IAPRSS) data. The IAPRSS was a population-based cross-sectional survey conducted in 2019. Four validated questionnaires were used to collect the data. The demographic status of each PWD, type of disability, housing and living conditions, job, and income status were also gathered. The first questionnaire was about deprivation of access to rehabilitation services (DARS). Shirazikhah et al. developed and validated a questionnaire [19]. It has 17 Likert-type questions in four dimensions: Affordability (six questions), transport (five questions), social support (three questions), and information (three questions), with five answering options: Never, rarely, sometimes, often, and always. The selection of “always” meant more significant DARS. The second questionnaire was the World Health Organization (WHO) standard responsiveness questionnaire, which had seven domains, including prompt attention, dignity, choice, autonomy, confidentiality, communication, and basic amenities, with 35 Likert-type questions. Previous studies have examined the validity and reliability of questionnaires for PWD [20, 21].
The last two questionnaires were the Persian versions of activities of daily living (ADL) and instrumental activities of daily living (IADL). With eight questions, ADL assesses basic daily tasks typically performed by individuals, such as bathing, dressing, eating, toileting, transferring, self-care, walking and continence. These activities are vital for maintaining independence and function in daily life. On the other hand, the IADL, with seven questions, assesses more complex activities necessary for community-independent living. These activities include managing finances, shopping, meal preparation, housekeeping, transportation, medications, and effective communication. Previous studies examined the reliability and validity of the Persian versions of ADL and IADL [22].
Sample selection
The IAPRSS utilized a multistage cluster sampling method to gather nationwide data. The number of sample zones was determined by dividing the country into four zones based on the level of development and population distribution in each zone [23]. Two provinces were selected from each zone using systematic sampling. Subsequently, households in each province were randomly chosen. The total sample size of IAPRSS was 2177, with 2146 PWD responding to the survey. In this study, we analyzed data from 2117 PWD.
Study variables
While IAPRSS has different variables, we chose some variables for our analysis, including sex, age, marital status, literacy, employment, and the type of rehabilitation service PWD need as socioeconomic status (SES) variables. The Mean±SD of the scores of DARS and its four dimensions were also included. We converted the original survey scores between 0 and 100, with higher scores indicating more significant DARS. We also used the ADL score as a standard indicator to assess the level of independence of individuals as a proxy variable for the need for rehabilitation services in PWD. We also calculated the wealth index to rank SES. The wealth index was calculated using a set of questions included in the demographic questions. We calculated the wealth index for each household using principal component analysis [24] and household living asset data.
Data analysis
This study calculated inequality using the GINI index and Lorenz curves. The GINI measures disparities in social and economic studies and health distribution without considering their needs. The GINI coefficient ranges from 0 to 1, where 0 indicates equal distribution and 1 indicates total inequality. The present study calculated the GINI index for the DARS scores.
The GINI was calculated as Equation 1:
ri is the DARS score of person i and rj is the DARS score of person j. µ is the average DARS score in total samples, n is the sample size, a and b are=2.
Previous studies showed that PWD with severe disabilities and those who are poor may require more rehabilitation services [12-14]. The GINI index calculates inequality without considering needs or SES. Therefore, the GINI index cannot provide accurate results for inequity. Therefore, we used the concentration index (CI) to calculate inequity. We calculated inequity by ranking DARS based on ADL score and wealth index. CI range is between +1 and -1, in which negative values indicate that the DARS is intense among PWD with low SES or PWD with severe disability (low ADL score). Positive values indicate that the DARS is concentrated among PWD with high SES or PWD with weak disability (high ADL score). The measurement scale is a crucial criterion for selecting the method for calculating CI and GINI. The use of general CI and GINI estimators may have led to bias. In this study, the DARS scores were bounded and counted; therefore, we used the Erreygers [25] CI and GINI indices to avoid bias.
GINI and CI provide holistic and comparable results that can be used for interpretation and decision-making. These indices help compare the disparity findings between different studies and provide valid, flexible, and precise results [26].
Finally, a regression model was used to determine the causes of inequality in DARS scores. In the regression model, we used wealth and ADL scores, age, and education status as explanatory variables (because these factors may affect the inequity in DARS) and DARS as the dependent variable. Data were analyzed using STATA SE software, version 13.1.
Results
Of 2117 PWD, 996(47.0%) were women. Among them, 1172(55.4%) were married, 917(43.3%) were single, and some chose not to disclose their marital status. The mean age of the participants was 44.6±0.4 years. Additionally, 1184 of 2098 participants (56.4%) were not economically active. Among the 2124 participants, 281(13.2%) were illiterate, 1225(57.7%) had less than a high school degree, and the remaining held an academic degree. Furthermore, 909 participants (42.4%) required physiotherapy, 243(11.3%) required occupational therapy, 155(7.2%) required speech therapy, 320(14.9%) required audiology services, 449(20.9%) required optometry services, and 327(15.3%) required orthotic and prosthetic services.
Table 1 presents the DARS scores and GINI index for DARS.
According to the Table 1, the overall DARS score averages 28.89±0.40. The highest score was observed in the information dimension at 31.98±0.52, while the lowest was in the social support dimension at 24.43±0.52. The overall GINI index for the DARS was 0.423±0.003. The highest GINI index was observed in the transport dimension at 0.551±0.003, while the lowest was associated with affordability at 0.499±0.003.
Table 2 presents the CI results for the DARS scores, considering ADL as a proxy variable for need.
The CI for affordability, transport, and social support deprivation showed that PWD with higher ADL scores had less deprivation in these dimensions (-0.093±0.009; -0.092±0.010; -0.062±0.010). The CI for DARS is -0.062±0.008, indicating that PWD with lower ADL scores had more deprivation in access to rehabilitation services.
Considering the wealth index as the ranking variable, the CI is positive only for the information dimension 0.069±0.014, showing more information deprivation for PWD with high SES. The deprivation of affordability was -0.162±0.011, indicating that the rich had a lower affordability deprivation. The CI for the total DARS score was -0.100±0.010, showing better access to rehabilitation services for PWD with a better SES.
Table 3 presents the CI results regarding sex and the type of rehabilitation service that PWDs need.
As shown in the Table 3, the CI was higher for orthotics and prosthetics services -0.131±0.027, indicating that the inequity of accessibility was higher in this type of rehabilitation service. In addition, inequity of accessibility was greater among men -0.117±0.014.
Table 4 presents the results of the regression model.
Regarding the wealth coefficient, PWD who were rich (coefficient=-2.14, %95 CI, -2.68%, -1.59%), younger (coefficient=-0.08, %95 CI, -0.775%, -0.32%) and had higher ADL scores (coefficient=-0.55, %95 CI, -0.77% -0.32%) had lower DARS scores. PWD with high school degrees (coefficient=3.54, 95 CI, 0.69%, 6.39%) and without health insurance coverage (coefficient=3.42, %95 CI, 1.32%, 5.51%) had higher DARS scores.
Discussion
This study investigated disparities in access to physical rehabilitation services among PWDs in a low-to-middle-income country, emphasizing the importance of planning and ensuring equitable access to rehabilitation services.
The results indicated that PWD encounter challenges when accessing rehabilitation services, particularly when seeking information about their required health and financial resources. Recent reviews highlighted that inadequate access to health information and financial support constitutes significant barriers for PWD seeking health services [27, 28]. Additionally, Sajadi et al. reported that accessing health information is a fundamental challenge for PWD during the COVID-19 pandemic. The WHO reports that over half of PWD face barriers to accessing health services due to financial constraints. However, these access challenges vary across low-income, medium-income, and high-income countries [29].
The results revealed significant disparities in access to rehabilitation services, raising considerable concerns. According to the global report on health equity for PWDs [3], health inequity is a pervasive challenge worldwide. Despite substantial advancements in numerous countries to mitigate this issue, many PWDs continue to encounter barriers to accessing necessary health services. This problem has been exacerbated after COVID-19 [10] and is particularly acute in Iran due to sanctions [16]. Consequently, immediate action is imperative to address these health disparities among PWDs, which entails progressing toward the universal realization of the right to the highest attainable standard of health for all. Paramount to this endeavor is to establish a national registry or database system for the systematic collection, analysis, interpretation, and utilization of data [30]. This system identifies PWD and their health needs, ensuring they receive timely and appropriate services. The recent national action plan for rehabilitation services in Iran outlines several interventions to reduce health disparities among PWDs [31]. It is anticipated that the effective implementation of this plan will ensure that no PWDs are excluded from receiving the necessary services. To develop targeted plans to reduce disparities in health access, particularly in rehabilitation, it is crucial to identify the primary drivers of these disparities. Our results highlight several key factors.
This study highlights disparities in access to rehabilitation services among PWD with severe impairments. This result is consistent with previous research by Sakellariouv and Rotarou, who demonstrated that people with severe disabilities face higher odds of encountering unmet needs [32]. When considering different dimensions of access, inequality seems to be minor regarding information for PWDs with severe disabilities. This suggests that these individuals may have better access to information through support organizations like the Iranian Welfare Organization but still face many other barriers. Therefore, it is crucial to develop specific interventions that identify and provide health services based on the needs of PWD.
Moreover, the results revealed pronounced disparities in access to diverse rehabilitation services, particularly orthotics and prosthetics. Previous research has also documented inequities in the availability of orthotic and prosthetic devices and related services [33, 34]. These disparities within the Iranian context may stem from the relatively elevated costs associated with orthotics and prosthetics compared to other rehabilitation services. Furthermore, a significant proportion of these services remain uncovered by health insurance packages, exacerbating financial challenges for persons with disabilities seeking access to them [35]. This underscores the imperative for enhanced efforts to expand coverage of rehabilitation services, considering cost-effectiveness analysis.
Our study revealed disparities in access to rehabilitation services among PWD lacking insurance coverage. These results are consistent with previous research that underscores the pivotal role of insurance coverage in determining health access for PWD [36]. Uninsured PWDs are more likely to have limited access to health services. In light of the national commitment to achieving UHC, targeted measures should be implemented to enhance adequate coverage of PWD, particularly in rehabilitation care.
SES analysis revealed significant disparities in access to rehabilitation services. These disparities are more pronounced in men than in women, individuals with lower educational attainment compared to those with higher education, older adults versus younger individuals, and PWD facing economic hardship compared to those in higher economic groups. Scholars have documented the critical role of SES in perpetuating health inequalities among PWD [37, 38]. Although previous studies have reported more significant disparities among women [40, 41], our results are contradictory. This gender-based disparity may stem from several factors. For instance, men may be less inclined to seek health services [42]. Additionally, health systems may inadvertently offer services that are more accessible to women [43].
Consistent with previous work, education, age, and economic status were identified as drivers of inequality in access to health services among PWD [28, 36, 37]. Regarding educational status, PWD with low educational levels had more difficulty accessing rehabilitation services. Lower educational attainment can impede health literacy, reduce awareness of available services, and complicate the navigation of healthcare systems. Furthermore, educational disparities often intersect with socioeconomic factors, further exacerbating inequities in less-educated PWD.
Regarding age differences, our study indicated that older adults face more significant challenges in accessing rehabilitation services than their younger counterparts. Accumulated health conditions and disabilities over time necessitate a more comprehensive rehabilitation program for older adults. Additionally, age-related mobility limitations or cognitive decline can impede the ability to effectively seek and utilize services.
Regarding income levels, we found that PWD from lower-income backgrounds encountered more disproportionate challenges than those from higher-income backgrounds. Low-income levels may result in limited access to essential resources, such as quality education and comprehensive healthcare, financial constraints that restrict their ability to afford necessary treatments or medications, and institutional barriers within the healthcare system that predominantly affect economically disadvantaged groups. Moreover, these communities may have limited access to information regarding available services and fewer advocacy opportunities, further intensifying inequities in-service distribution.
Efforts to reduce SES-related disparities in rehabilitation services for PWD should focus on policy reforms that enhance service accessibility and educational initiatives that improve health literacy among economically disadvantaged groups. Adopting approaches, such as the intersectional perspective, can be instrumental in identifying the most vulnerable groups and devising strategic plans to meet their specific needs [44]. Policymakers and healthcare practitioners must consider these insights when crafting inclusive rehabilitation programs to guarantee equitable access to PWD.
This study has some limitations. We analyzed the results using aggregated scores, such as GINI and CI, which were insufficient for detailed interpretation. The GINI and CI provide aggregated outcomes for calculating health and health service utilization inequity. The results are suitable for comparison studies; however, as aggregated outcomes are limited, they cannot be used for detailed analyses and interventions. Another limitation is that the study was related to its cross-sectional nature. Therefore, it is better to include the time of injury as an effective factor for ADL. We did not have access to the time variable and added it to the regression model. However, as we used ADL as the proxy variable for need, it was not crucial to add time as an explanatory variable for ADL.
Conclusion
In recent years, numerous initiatives have been undertaken to improve access to health for PWD, yet disparities in care persist in many low-income and middle-income countries. Advancing equity requires recognizing the drivers of these disparities and addressing them through health reforms and policies. This study revealed inequities in access to rehabilitation services, particularly among those with severe impairments, orthotics, and prosthetics, as well as among uninsured individuals. The disparities are more pronounced among men than women, individuals with lower educational levels versus those with higher education, older adults relative to younger people, and PWD experiencing economic hardship compared to those with higher economic levels. Policymakers are urged to consider these factors when developing health plans to tackle equity challenges and ensure equitable healthcare for all, especially disadvantaged groups. These results can be instrumental in planning purposes in similar contexts.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committees of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1400.059)
Funding
This research was supported by the research project funded by the University of Social Welfare and Rehabilitation Sciences University, Tehran, Iran (Project No.: 2600).
Authors' contributions
Project administration and funding acquisition: Marzieh Shirazikhah; Supervision: Haniye Sadat Sajadi; Conceptualization and validation: Enayatollah Homaie Rad, Marzieh Shirazikhah, and Haniye Sadat Sajadi; Software, data collection, Visualization and formal analysis: Enayatollah Homaie Rad; Writing the original draft: Enayatollah Homaie Rad and Haniye Sadat Sajadi; Methodology, resources, investigation, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank other contributors to the study who did not add themselves as authors. The University of Social Welfare and Rehabilitation Sciences, Tehran, Iran is appreciated for the financial support.
References
- Banks LM, Kuper H, Polack S. Poverty and disability in low-and middle-income countries: A systematic review. PloS one. 2017; 12(12):e0189996. [DOI:10.1371/journal.pone.0189996] [PMID]
- WHO. World report on disability 2011. Geneva: World Health Organization; 2011. [Link]
- WHO. Global report on health equity for persons with disabilities. Geneva: World Health Organization; 2022. [Link]
- Soltani S. Unmet healthcare needs in people with disabilities: An evidence to make reforms in health insurance programs in Iran. Journal of Research in Medical Sciences. 2018; 23(1):74. [DOI:10.4103/jrms.JRMS_276_18]
- Soltani S. Hidden cost of disability: What policy makers usually forget. Journal of Research in Medical Sciences. 2018; 23:15. [DOI:10.4103/jrms.JRMS_760_17] [PMID]
- Briggs AM, Dreinhöfer KE. Rehabilitation 2030: A call to action relevant to improving musculoskeletal health care globally. The Journal of orthopaedic and Sports Physical Therapy. 2017; 47(5):297-300. [DOI:10.2519/jospt.2017.0105] [PMID]
- WHO. Global report on assistive technology. Geneva: World Health Organization; 2022. [Link]
- Soltani S, Takian A, Sari AA, Kamali M, Majdzadeh SR, Matin BK. [Disregarded health problems of people with disabilities: A qualitative study of policymakers’ perspective (Persian)]. Archives of Rehabilitation. 2019; 20(2):136-49. [DOI:10.32598/rj.20.2.136]
- Takamine Y. Disability issues in East Asia: Review and ways forward: Washington, DC: World Bank; 2004. [Link]
- Jumreornvong O, Tabacof L, Cortes M, Tosto J, Kellner CP, Herrera JE, et al. Ensuring equity for people living with disabilities in the age of COVID-19. Disability & Society. 2020; 35(10):1682-7. [DOI:10.1080/09687599.2020.1809350]
- Gréaux M, Moro MF, Kamenov K, Russell AM, Barrett D, Cieza A. Health equity for persons with disabilities: a global scoping review on barriers and interventions in healthcare services. International Journal for Equity in Health. 2023; 22(1):236. [DOI:10.1186/s12939-023-02035-w] [PMID]
- Shirazikhah M, Ghaedamini Harouni GG, Shirazikhah A, Noroozi M, Sajadi HS. [Access to physical rehabilitation services among people with disabilities: results of a national study in Iran (Persian)]. Koomesh. 2022; 24(5):596-604. [Link]
- Yahyavi Dizaj J, Na’emani F, Fateh M, Soleimanifar M, Arab AM, Zali ME, et al. [Inequality in the utilization of rehabilitation services among Urban and Rural households in Iran: A cross-sectional study (Persian)]. Archives of Rehabilitation. 2020; 21(3):336-57. [DOI:10.32598/RJ.21.3.2893.1]
- Soltani S, Moghadam MM, Amani S, Akbari S, Shiani A, Soofi M. Socioeconomic disparities in using rehabilitation services among Iranian adults with disabilities: a decomposition analysis. BMC Health Services Research. 2022; 22(1):1449. [DOI:10.1186/s12913-022-08811-8] [PMID]
- Sajadi HS, Shirazikhah M, Joghataei M. [Need to expand rehabilitation facilities to improve access to health services for people with disabilities in Iran (Persian)]. Social Welfare Quarterly. 2021; 21(81):9-14. [Link]
- Shahabi S, Teymourlouy AA, Shabaninejad H, Kamali M, Lankarani KB, Mojgani P. Physical rehabilitation in Iran after international sanctions: explored findings from a qualitative study. Globalization and Health. 2020; 16(1):86. [DOI:10.1186/s12992-020-00618-8] [PMID]
- Sajadi HS, Gholamreza Kashi F, Majdzadeh R. Identifying national health priorities: Content analysis of the Islamic Republic of Iran’s General Health Policies (GHPs). World Medical & Health Policy. 2020; 12(2):123-36. [DOI:10.1002/wmh3.338]
- Wright S, Mabejane R. The 2019 UN high-level meeting on universal health coverage. Lancet. 2019; 393(10184):1931. [DOI:10.1016/S0140-6736(19)30349-6] [PMID]
- Shirazikhah M, Mirabzadeh A, Sajjadi H, Joghataei MT, Biglarian A, Mohammadi Shahboulaghi F, et al. Physical rehabilitation accessibility assessment questionnaire for people with physical disability: A development and validation study in Iran. Iranian Rehabilitation Journal. 2020; 18(2):211-22. [DOI:10.32598/irj.18.2.971.1]
- Alavi M, Forouzan AS, Moradi-Lakeh M, Ardakani MRK, Shati M, Noroozi M, et al. Inequality in responsiveness: A study of comprehensive physical rehabilitation centers in capital of Iran. Health Services Research and Managerial Epidemiology. 2018; 5:2333392818789026. [DOI:10.1177/2333392818789026] [PMID]
- Shirazikhah M, Ghaedamini Harouni G, Shirazikhah A, Noroozi M, Sajadi HS. [Iran health system responsiveness in regared to provision of physical rehabilitation: results of a national survey (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences 2023; 28(4):174-85. [DOI:10.61186/sjku.28.4.174]
- Taheri Tanjani P, Azadbakht M. [Psychometric properties of the Persian version of the activities of daily living scale and instrumental activities of daily living scale in elderly (Persian)]. Journal of Mazandaran University of Medical Sciences. 2016; 25(132):103-12. [Link]
- Farzadfar F, Danaei G, Namdaritabar H, Rajaratnam JK, Marcus JR, Khosravi A, et al. National and subnational mortality effects of metabolic risk factors and smoking in Iran: a comparative risk assessment. Population Health Metrics. 2011; 9(1):55. [DOI:10.1186/1478-7954-9-55] [PMID]
- Vyas S, Kumaranayake L. Constructing socioeconomic status indices: how to use principal components analysis. Health Policy and Planning. 2006; 21(6):459-68. [DOI:10.1093/heapol/czl029] [PMID]
- Erreygers G. Correcting the concentration index. Journal of Health Economics. 2009; 28(2):504-15. [DOI:10.1016/j.jhealeco.2008.12.001] [PMID]
- Schneider MC, Castillo-Salgado C, Bacallao J, Loyola E, Mujica OJ, Vidaurre M, et al. Methods for measuring health inequalities (Part III). Epidemiological Bulletin. 2005; 26(1):5-10. [DOI:10.1590/S1020-49892002001200006]
- Clemente KAP, Silva SVD, Vieira GI, Bortoli MC, Toma TS, Ramos VD, et al. Barriers to the access of people with disabilities to health services: A scoping review. Revista de Saude Publica. 2022; 56:64. [DOI:10.11606/s1518-8787.2022056003893] [PMID]
- Gibson J, O’Connor R. Access to health care for disabled people: a systematic review. Social Care and Neurodisability. 2010; 1(3):21-31. [DOI:10.5042/scn.2010.0599]
- WHO. WHO global disability action plan 2014-2021: Better health for all people with disability. Geneva: World Health Organization; 2015. [Link]
- Milićević M, Simeunović B. Founding process of a registry of people with disabilities-methodological challenges and overcoming strategies. Belgrades School of Defectology. 2020; 26(2):19-30. [Link]
- Sajadi HS, Nazari M, Shirazikhah M, Bahmanziari N. [Monitoring and evaluation indicators of the national plan of medical rehabilitation (Persian)]. Iranian Journal of Culture and Health Promotion. 2024; 8(3) :290-7. [DOI: 10.22034/8.3.12]
- Sakellariou D, Rotarou ES. Access to healthcare for men and women with disabilities in the UK: secondary analysis of cross-sectional data. BMJ Open. 2017; 7(8):e016614. [DOI:10.1136/bmjopen-2017-016614] [PMID]
- Baumann MF, Maria M. Improving access to prosthetic limbs in Germany: An explorative review. Prosthetics and orthotics international. 2023; 47(5):486-93. [DOI:10.1097/PXR.0000000000000254] [PMID]
- Lipski E, Waters WF, Kenworthy S, Mullen A. A disparity in prosthetic access for Ecuadorians with lower-limb amputation. Prosthetics and orthotics international. 2024; 48(6):694-9. [DOI:10.1097/PXR.0000000000000326] [PMID]
- Shahabi S, Pardhan S, Ahmadi Teymourlouy A, Skempes D, Shahali S, et al. Prioritizing solutions to incorporate Prosthetics and Orthotics services into Iranian health benefits package: Using an analytic hierarchy process. PLoS One. 2021; 16(6):e0253001. [DOI:10.1371/journal.pone.0253001] [PMID]
- Mahmoudi E, Meade MA. Disparities in access to health care among adults with physical disabilities: Analysis of a representative national sample for a ten-year period. Disability and Health Journal. 2015; 8(2):182-90. [DOI:10.1016/j.dhjo.2014.08.007] [PMID]
- Wang YR, Luo YN, Fan YL, Fan YY, Zheng XY. Impact of socioeconomic position on the utilization of rehabilitation services among the Chinese older adults disabled by injury. Frontiers in Public Health. 2023; 11:1034482. [DOI:10.3389/fpubh.2023.1034482] [PMID]
- Mitchell RJ, Ryder T, Matar K, Lystad RP, Clay-Williams R, Braithwaite J. An overview of systematic reviews to determine the impact of socio-environmental factors on health outcomes of people with disabilities. Health & Social Care in the Community. 2022; 30(4):1254-74. [DOI:10.1111/hsc.13665] [PMID]
- Nosek MA. Health disparities and equity: The intersection of disability, health, and sociodemographic characteristics among women. In: Miles-Cohen SE, Signore C, ediotors. Eliminating inequities for women with disabilities: An agenda for health and wellness. Massachusetts: American Psychological Association; 2016. [DOI:10.1037/14943-002]
- Smith DL, Ruiz MS. Perceived disparities in access to health care due to cost for women with disabilities. Journal of Rehabilitation. 2009; 75(4):3-10. [Link]
- Rotarou ES, Sakellariou D. Inequalities in access to health care for people with disabilities in Chile: the limits of universal health coverage. Critical Public Health. 2017; 27(5):604-16. [DOI:10.1080/09581596.2016.1275524]
- Baker P. Men’s health: time for a new approach. Physical Therapy Reviews. 2018; 23(2):144-50. [DOI:10.1080/10833196.2018.1452562]
- Beia T, Kielmann K, Diaconu K. Changing men or changing health systems? A scoping review of interventions, services and programmes targeting men’s health in sub-Saharan Africa. International journal for equity in health. 2021; 20:87. [DOI:10.1186/s12939-021-01428-z] [PMID]
- Kuran CHA, Morsut C, Kruke BI, Krüger M, Segnestam L, Orru K, et al. Vulnerability and vulnerable groups from an intersectionality perspective. International Journal of Disaster Risk Reduction. 2020; 50:101826. [DOI:10.1016/j.ijdrr.2020.101826]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2024/02/28 | Accepted: 2024/08/31 | Published: 2025/03/1
Received: 2024/02/28 | Accepted: 2024/08/31 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
