
988368
Thu, Jul 30, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 95-104 |
Back to browse issues page


Ethics code: IR.SSRC.REC. 1402.283
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shahani O, Shamsi Majelan A, Khoshraftar Yazdi N. Enhancing Balance in Athletes With Chronic Ankle Instability: The Power of Visual Feedback. Iranian Rehabilitation Journal 2025; 23 (1) :95-104
URL: http://irj.uswr.ac.ir/article-1-2230-en.html
URL: http://irj.uswr.ac.ir/article-1-2230-en.html



1- Department of Sport Injury and Corrective Exercise, Faculty of Physical Education and Sports Sciences, University of Guilan, Rasht, Iran.
2- Department of Exercise Physiology and Sport Injuries and Corrective Movements, Faculty of Sport Sciences, Ferdowsi University of Mashhad, Mashhad, Iran.
2- Department of Exercise Physiology and Sport Injuries and Corrective Movements, Faculty of Sport Sciences, Ferdowsi University of Mashhad, Mashhad, Iran.
Keywords: Stork balance, Feedback, Single-leg hop-stabilization, Athlete, Chronic ankle instability (CAI)
Full-Text [PDF 816 kb]
(1347 Downloads)
| Abstract (HTML) (3227 Views)
Program exercise
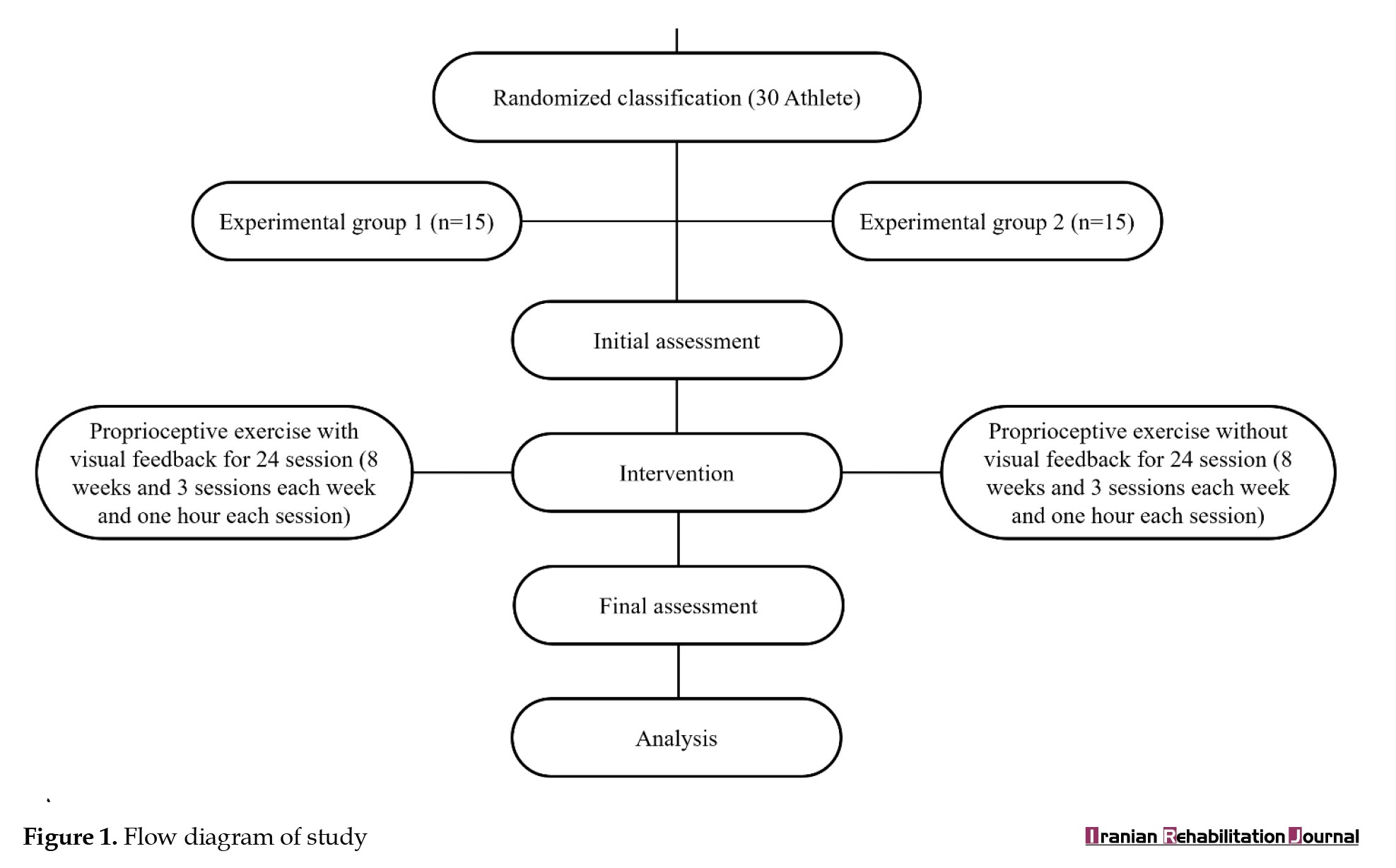
The research protocol was selected from Hupperets et al.’s research [17], which lasted for eight weeks in such a way that the exercises were performed in three 1-h sessions per week. In the first group, which performed proprioceptive exercises with visual feedback, all exercises were performed in front of a mirror to use their movement feedback, and the second group, which consisted of proprioceptive exercises without feedback, was performed in the same way. The intended proprioceptive exercises are presented in Table 1.
FAAM and FAAM-sport
FAAM questionnaire comprises 26 questions, with four about pain and 22 focusing on activity. In contrast, the FAAM-sports questionnaire consisted of eight questions. Every question was evaluated using a 5-point Likert scale that ranges from 0 to 4. Individual scores were assigned to each indicator. The maximum score achievable for the FAAM index was 104, whereas that for the FAAM-sports index was 32. Subsequently, scores were converted into percentages [19].
Dominant leg
To identify the dominant leg, athletes were asked to kick a ball, the dominant leg was the leg used to kick the ball [20].
Balance
Static balance (stork balance)
The Stork balance method is done in such a way that the subject placed the opposite leg of the injured leg on the inner edge of their knee placed both hands on their hip and with the command “Go” raised the heel of the stationary leg on the ground and the position. It preserves as much as possible when it is balance impaired, the foot is removed from the kneecap, the hands are removed from the hips, or the heel of the foot is near the ground and touch. Static balance was evaluated in two conditions with eyes open and closed [21].
Dynamic balance
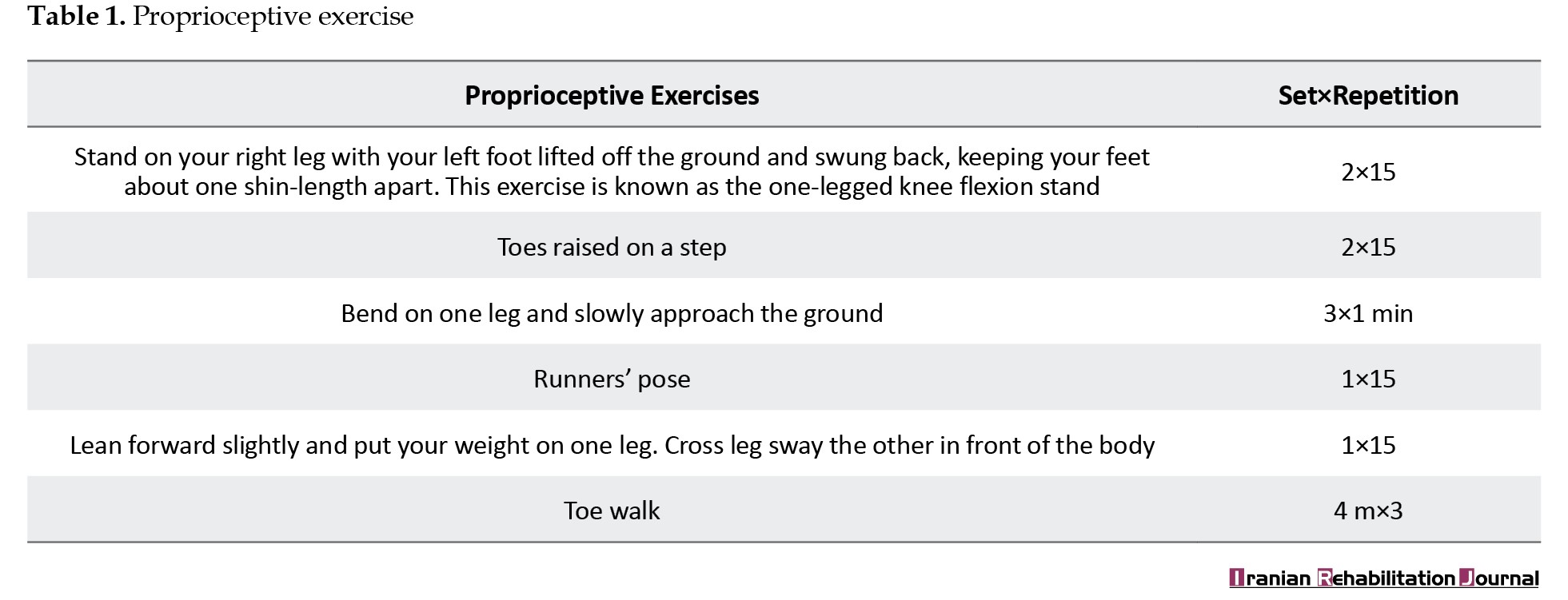
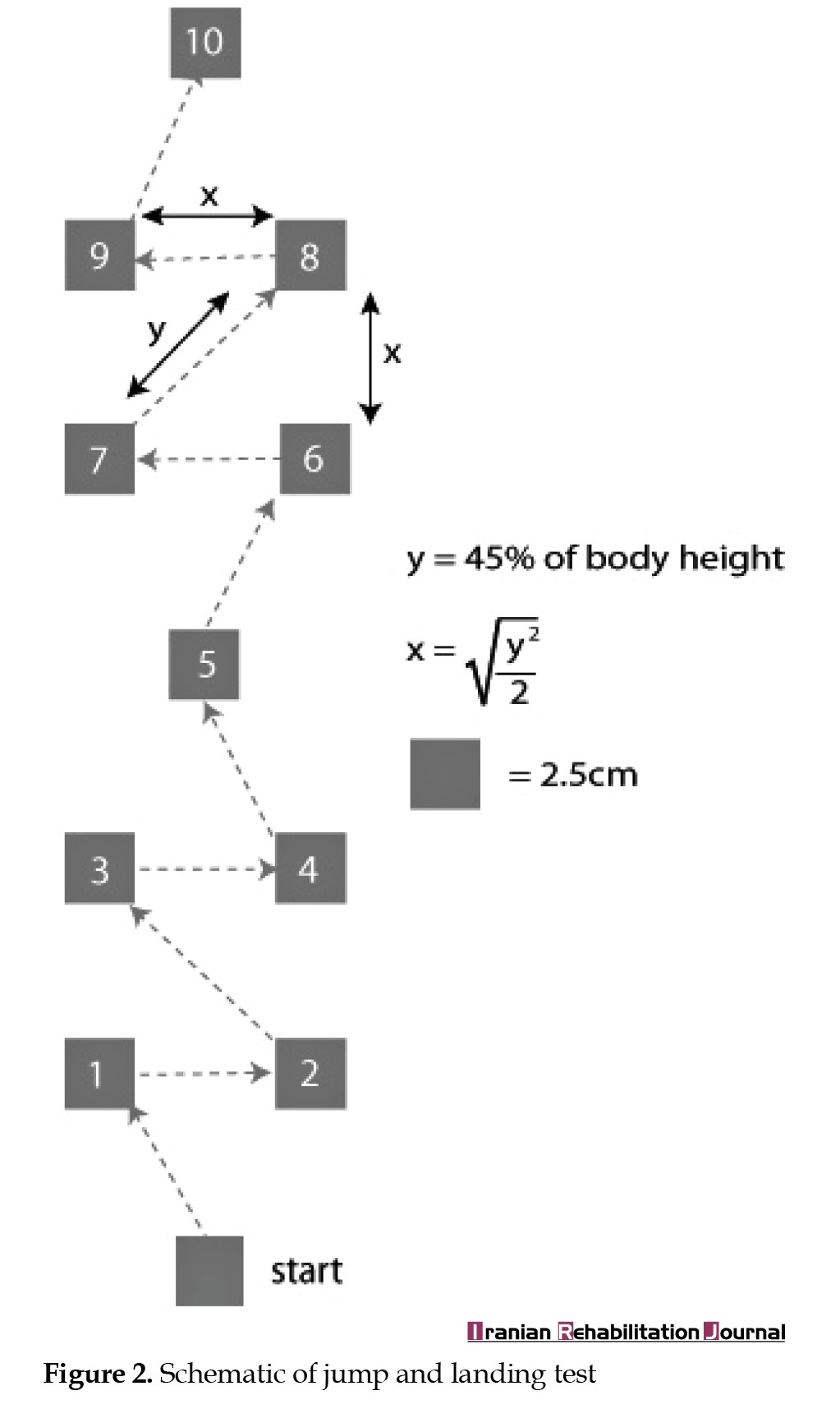
To evaluate dynamic balance, the jump and landing test was utilized. The procedure is as follows. The subject is placed in the starting position and the hands are on the iliac crest. The person’s gaze should be forward and then they will be placed on one leg and they will be asked to jump towards the prearranged squares and land on the same leg and then stop for 5 seconds and then perform the next jump. During the execution of the test, errors were counted and dynamic balance ability was evaluated by the number of errors.
Errors in the stop phase after landing include the bent leg hitting the ground, lifting the hands from the iliac crest, touching the weight-bearing limb, and moving the non-weight-bearing limb toward flexion, extension, or away, becoming excessive (>30 degrees).
Errors in the landing phase include removing the hands from the iliac crest, not covering the square with the leg, stumbling during landing, and the landing leg having more than 10 degrees of inversion or eversion [22].
The process of performing the jump and landing test is shown in Figure 2.
Full-Text: (734 Views)
Introduction
One of the injuries that commonly occurs in most sports is a sprained ankle [1]. Sports such as handball and volleyball, which have a landing on one leg, and sports that have the nature of a collision between two players, like football, can cause this type of injury [2]. In addition, if the rehabilitation process of this injury is not performed well and the complications remain, repeated ankle sprain will eventually lead to chronic instability in the ankle region and disrupt the stability and health of the athlete [3]. The remaining symptoms from the initial ankle sprain appear as chronic ankle instability (CAI). Around 70% of the general population will encounter an ankle sprain at some point in their lives [4]. CAI is a combination of mechanical and functional instability with residual symptoms of ankle sprains, such as pain, swelling, weakness, instability, and recurrences. These residual symptoms can impair people’s physical activity and ultimately negatively affect their overall health and quality of life [2, 5].
Balance deficits can lead to recurrent ankle sprains and decreased lower limb strength. The potential to maintain balance in different activities and uphold a natural posture is crucial for executing various movements effectively. Proper rehabilitation and strengthening exercises targeting balance and proprioception are often recommended to improve outcomes following ankle injuries [4, 6]. Ankle position sense is an important component of communication because it provides critical information for positioning the ankle to perform important multimodal motor tasks that play a vital role in control [7]. Visual feedback involves the momentary comprehension of errors, leading to an enhancement in decision-making abilities. The utilization of diverse tools to implement such feedback not only renders exercises more engaging but also increases their acceptability among individuals [8]. Specifically, the synergy between visual and sensory feedback assumes a crucial role in delivering information to the central nervous system (CNS), thereby facilitating the effective management of neuromuscular control during movements [9].
In this method, visual feedback to the CNS increases and creates an adaptive strategy. By relying on the more dependable information sources within these sensory systems, the body’s position stability is maintained. When people experience changes in sensory information due to an injured joint, they often reduce reliance on the somatosensory system and prioritize re-evaluating more dependable sensory inputs [10]. This optimization ensures superior motor control and bolsters the overall management of movement patterns, thereby contributing to the mitigation of potential injury risks. In a study conducted by Yalfani et al. on people suffering from CAI, it was concluded that it regulates brain wave feedback and can affect subcortical and cerebral motor loops [11]. Individuals with multiple sclerosis exhibit greater trust in their visual input when it comes to maintaining balance and stability [12]. Also, individuals who have undergone anterior cruciate ligament reconstruction exhibit heightened activity in the posterior inferior temporal gyrus of the brain, linked to visual processing. This change may manifest as altered sensations from textured shoe soles or numbness in the ankle joint. Nonetheless, there is currently insufficient proof of sensory reweighting in patients with CAI [9, 10, 13].
Teaching feedback and integrating it into training protocols to enhance the precision of movements and rectify errors during exercise involves utilizing feedback received either from one’s performance or stimulants provided by the systems visual, vestibular and somatosensory. This method aids in enhancing bodily functions, balance capabilities, and rectifying any asymmetry in posture [14]. Most studies on feedback have been conducted in controlled laboratory environments, where the feedback has been predominantly provided either by a professional therapist or through self-regulation mechanisms. However, leveraging this feedback within the training setting makes it more closely aligned with daily activities, thereby proving to be more impactful in enhancing performance outcomes [15]. This approach facilitates skill development and fosters a deeper understanding of one’s movements, leading to improved overall physical performance.
Hunt et al. compared the performance error during outward gait correction in Individuals with knee osteoarthritis utilizing three distinct forms of visual feedback: Mirror reflection, unedited video footage and real-time biofeedback displaying the outward angle. They stated that when real-time biofeedback was used, the performance error was significantly lower than the raw and mirror video errors [16]. Hupperets et al. used a protocol of proprioceptive exercises to prevent the recurrence of ankle sprain and the recurrence of this injury. Finally, the obtained results showed that the exercises can prevent the reoccurrence of the injury to an optimal extent and are effective [17]. Beydagı and Talu investigated the effect of proprioception exercises on balance in professional athletes. Finally, the desired effects of these exercises were observed [18]. Accordingly, this study examines the efficacy of visual feedback in proprioceptive training for athletes with CAI and determines if this approach can substantially improve the balance of this population.
Materials and Methods
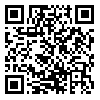
The research was semi experimental, with a pre and post-test in two groups. A total of 30 athletes were purposefully and available to participate in the research according to the score of the foot and ankle ability measure (FAAM) and the FAAM sports index (FAAM-sport) and after the physician confirmation Using medical records and physical examinations (anterior drawer test) that they were suffering from CAI, they entered the study. The inclusion criteria comprised the following items: In the past six months having a feeling of instability several times in the ankle joint and obtaining a score of ≤90% on the FAAM and a score of ≤80% on the FAAM-sport. Meanwhile, the exclusion criteria were having previous lower limb injury within the past six months, lower limb surgery, and balance and vision disorders, Afterwards, they were divided randomly into two groups. Each group included 15 athletes, the first group performed proprioceptive exercises with visual feedback (PF) and the second group performed proprioceptive exercises without feedback (P). Before starting the evaluation and exercises, a consent form for participating in the research was received from each subject. Initial evaluations, including height, mass, age, and static and dynamic balance, were performed. The research stages are depicted in Figure 1.
One of the injuries that commonly occurs in most sports is a sprained ankle [1]. Sports such as handball and volleyball, which have a landing on one leg, and sports that have the nature of a collision between two players, like football, can cause this type of injury [2]. In addition, if the rehabilitation process of this injury is not performed well and the complications remain, repeated ankle sprain will eventually lead to chronic instability in the ankle region and disrupt the stability and health of the athlete [3]. The remaining symptoms from the initial ankle sprain appear as chronic ankle instability (CAI). Around 70% of the general population will encounter an ankle sprain at some point in their lives [4]. CAI is a combination of mechanical and functional instability with residual symptoms of ankle sprains, such as pain, swelling, weakness, instability, and recurrences. These residual symptoms can impair people’s physical activity and ultimately negatively affect their overall health and quality of life [2, 5].
Balance deficits can lead to recurrent ankle sprains and decreased lower limb strength. The potential to maintain balance in different activities and uphold a natural posture is crucial for executing various movements effectively. Proper rehabilitation and strengthening exercises targeting balance and proprioception are often recommended to improve outcomes following ankle injuries [4, 6]. Ankle position sense is an important component of communication because it provides critical information for positioning the ankle to perform important multimodal motor tasks that play a vital role in control [7]. Visual feedback involves the momentary comprehension of errors, leading to an enhancement in decision-making abilities. The utilization of diverse tools to implement such feedback not only renders exercises more engaging but also increases their acceptability among individuals [8]. Specifically, the synergy between visual and sensory feedback assumes a crucial role in delivering information to the central nervous system (CNS), thereby facilitating the effective management of neuromuscular control during movements [9].
In this method, visual feedback to the CNS increases and creates an adaptive strategy. By relying on the more dependable information sources within these sensory systems, the body’s position stability is maintained. When people experience changes in sensory information due to an injured joint, they often reduce reliance on the somatosensory system and prioritize re-evaluating more dependable sensory inputs [10]. This optimization ensures superior motor control and bolsters the overall management of movement patterns, thereby contributing to the mitigation of potential injury risks. In a study conducted by Yalfani et al. on people suffering from CAI, it was concluded that it regulates brain wave feedback and can affect subcortical and cerebral motor loops [11]. Individuals with multiple sclerosis exhibit greater trust in their visual input when it comes to maintaining balance and stability [12]. Also, individuals who have undergone anterior cruciate ligament reconstruction exhibit heightened activity in the posterior inferior temporal gyrus of the brain, linked to visual processing. This change may manifest as altered sensations from textured shoe soles or numbness in the ankle joint. Nonetheless, there is currently insufficient proof of sensory reweighting in patients with CAI [9, 10, 13].
Teaching feedback and integrating it into training protocols to enhance the precision of movements and rectify errors during exercise involves utilizing feedback received either from one’s performance or stimulants provided by the systems visual, vestibular and somatosensory. This method aids in enhancing bodily functions, balance capabilities, and rectifying any asymmetry in posture [14]. Most studies on feedback have been conducted in controlled laboratory environments, where the feedback has been predominantly provided either by a professional therapist or through self-regulation mechanisms. However, leveraging this feedback within the training setting makes it more closely aligned with daily activities, thereby proving to be more impactful in enhancing performance outcomes [15]. This approach facilitates skill development and fosters a deeper understanding of one’s movements, leading to improved overall physical performance.
Hunt et al. compared the performance error during outward gait correction in Individuals with knee osteoarthritis utilizing three distinct forms of visual feedback: Mirror reflection, unedited video footage and real-time biofeedback displaying the outward angle. They stated that when real-time biofeedback was used, the performance error was significantly lower than the raw and mirror video errors [16]. Hupperets et al. used a protocol of proprioceptive exercises to prevent the recurrence of ankle sprain and the recurrence of this injury. Finally, the obtained results showed that the exercises can prevent the reoccurrence of the injury to an optimal extent and are effective [17]. Beydagı and Talu investigated the effect of proprioception exercises on balance in professional athletes. Finally, the desired effects of these exercises were observed [18]. Accordingly, this study examines the efficacy of visual feedback in proprioceptive training for athletes with CAI and determines if this approach can substantially improve the balance of this population.
Materials and Methods
The research was semi experimental, with a pre and post-test in two groups. A total of 30 athletes were purposefully and available to participate in the research according to the score of the foot and ankle ability measure (FAAM) and the FAAM sports index (FAAM-sport) and after the physician confirmation Using medical records and physical examinations (anterior drawer test) that they were suffering from CAI, they entered the study. The inclusion criteria comprised the following items: In the past six months having a feeling of instability several times in the ankle joint and obtaining a score of ≤90% on the FAAM and a score of ≤80% on the FAAM-sport. Meanwhile, the exclusion criteria were having previous lower limb injury within the past six months, lower limb surgery, and balance and vision disorders, Afterwards, they were divided randomly into two groups. Each group included 15 athletes, the first group performed proprioceptive exercises with visual feedback (PF) and the second group performed proprioceptive exercises without feedback (P). Before starting the evaluation and exercises, a consent form for participating in the research was received from each subject. Initial evaluations, including height, mass, age, and static and dynamic balance, were performed. The research stages are depicted in Figure 1.
Program exercise
The research protocol was selected from Hupperets et al.’s research [17], which lasted for eight weeks in such a way that the exercises were performed in three 1-h sessions per week. In the first group, which performed proprioceptive exercises with visual feedback, all exercises were performed in front of a mirror to use their movement feedback, and the second group, which consisted of proprioceptive exercises without feedback, was performed in the same way. The intended proprioceptive exercises are presented in Table 1.
FAAM and FAAM-sport
FAAM questionnaire comprises 26 questions, with four about pain and 22 focusing on activity. In contrast, the FAAM-sports questionnaire consisted of eight questions. Every question was evaluated using a 5-point Likert scale that ranges from 0 to 4. Individual scores were assigned to each indicator. The maximum score achievable for the FAAM index was 104, whereas that for the FAAM-sports index was 32. Subsequently, scores were converted into percentages [19].
Dominant leg
To identify the dominant leg, athletes were asked to kick a ball, the dominant leg was the leg used to kick the ball [20].
Balance
Static balance (stork balance)
The Stork balance method is done in such a way that the subject placed the opposite leg of the injured leg on the inner edge of their knee placed both hands on their hip and with the command “Go” raised the heel of the stationary leg on the ground and the position. It preserves as much as possible when it is balance impaired, the foot is removed from the kneecap, the hands are removed from the hips, or the heel of the foot is near the ground and touch. Static balance was evaluated in two conditions with eyes open and closed [21].
Dynamic balance
To evaluate dynamic balance, the jump and landing test was utilized. The procedure is as follows. The subject is placed in the starting position and the hands are on the iliac crest. The person’s gaze should be forward and then they will be placed on one leg and they will be asked to jump towards the prearranged squares and land on the same leg and then stop for 5 seconds and then perform the next jump. During the execution of the test, errors were counted and dynamic balance ability was evaluated by the number of errors.
Errors in the stop phase after landing include the bent leg hitting the ground, lifting the hands from the iliac crest, touching the weight-bearing limb, and moving the non-weight-bearing limb toward flexion, extension, or away, becoming excessive (>30 degrees).
Errors in the landing phase include removing the hands from the iliac crest, not covering the square with the leg, stumbling during landing, and the landing leg having more than 10 degrees of inversion or eversion [22].
The process of performing the jump and landing test is shown in Figure 2.
Statistical analyses
SPSS software, version 27 was utilized for analyzing the collected data. The Shapiro-Wilk test was employed to check the normality of the subjects’ distribution. The paired sample t-test was conducted to examine within-group variations, while univariate analysis was used to compare the two groups. The Lune test was used to confirm the homogeneity of variance. A significance level of 0.05 was considered to interpret the results.
Results
Table 2 presents the descriptive statistics of the demographic characteristics of the subjects, such as mass, height, age, body mass index, FAAM index and FAAM sports index, individually for each group.
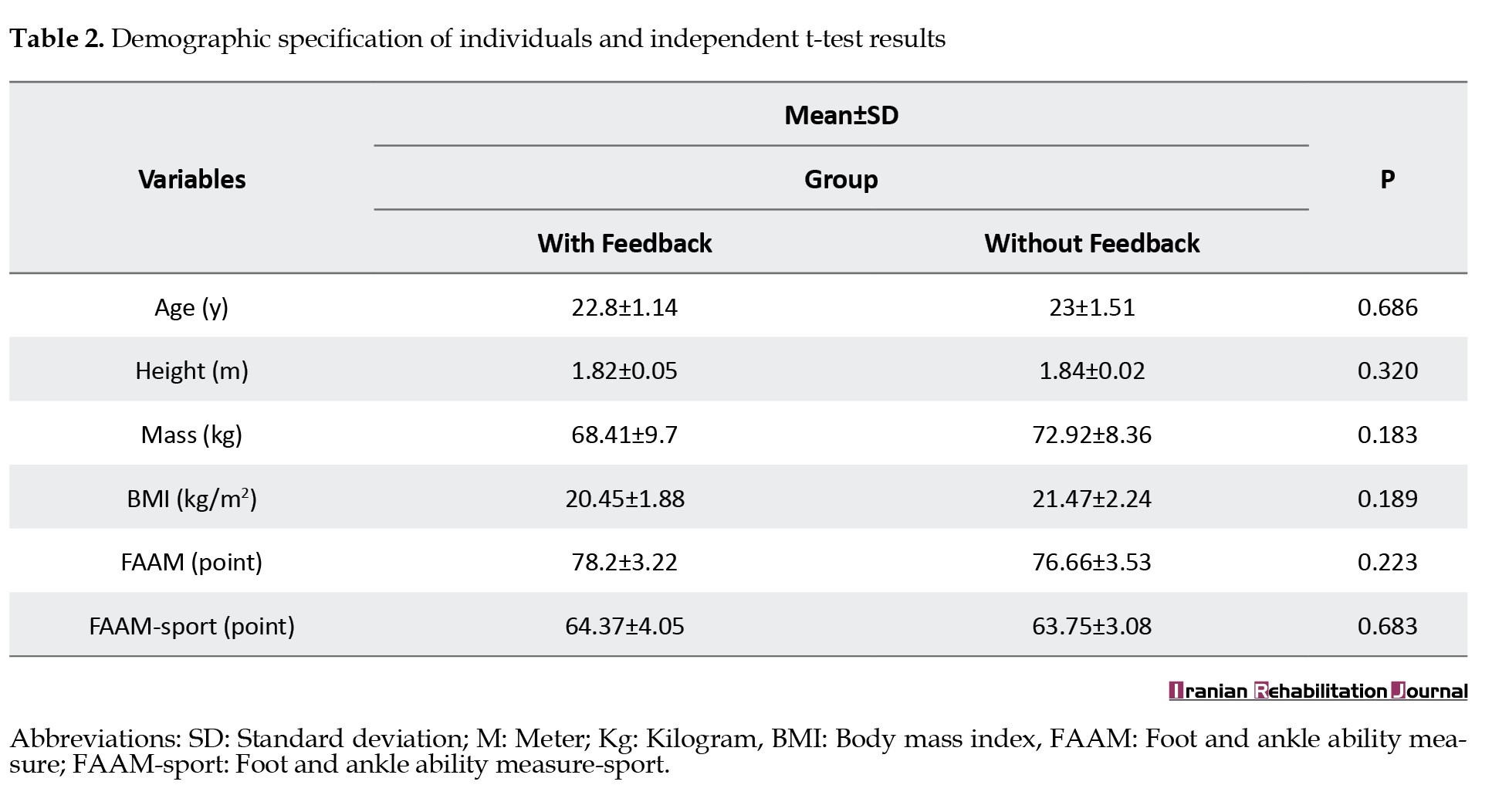
According to the results of the Shapiro-Wilk test, all the data follow a normal distribution. The independent t-test results revealed no significant difference across the demographic indicators, suggesting that the subjects exhibited homogeneity in these characteristics.
The comparison between groups was analyzed using univariate variance test and the results are reported in Table 3.
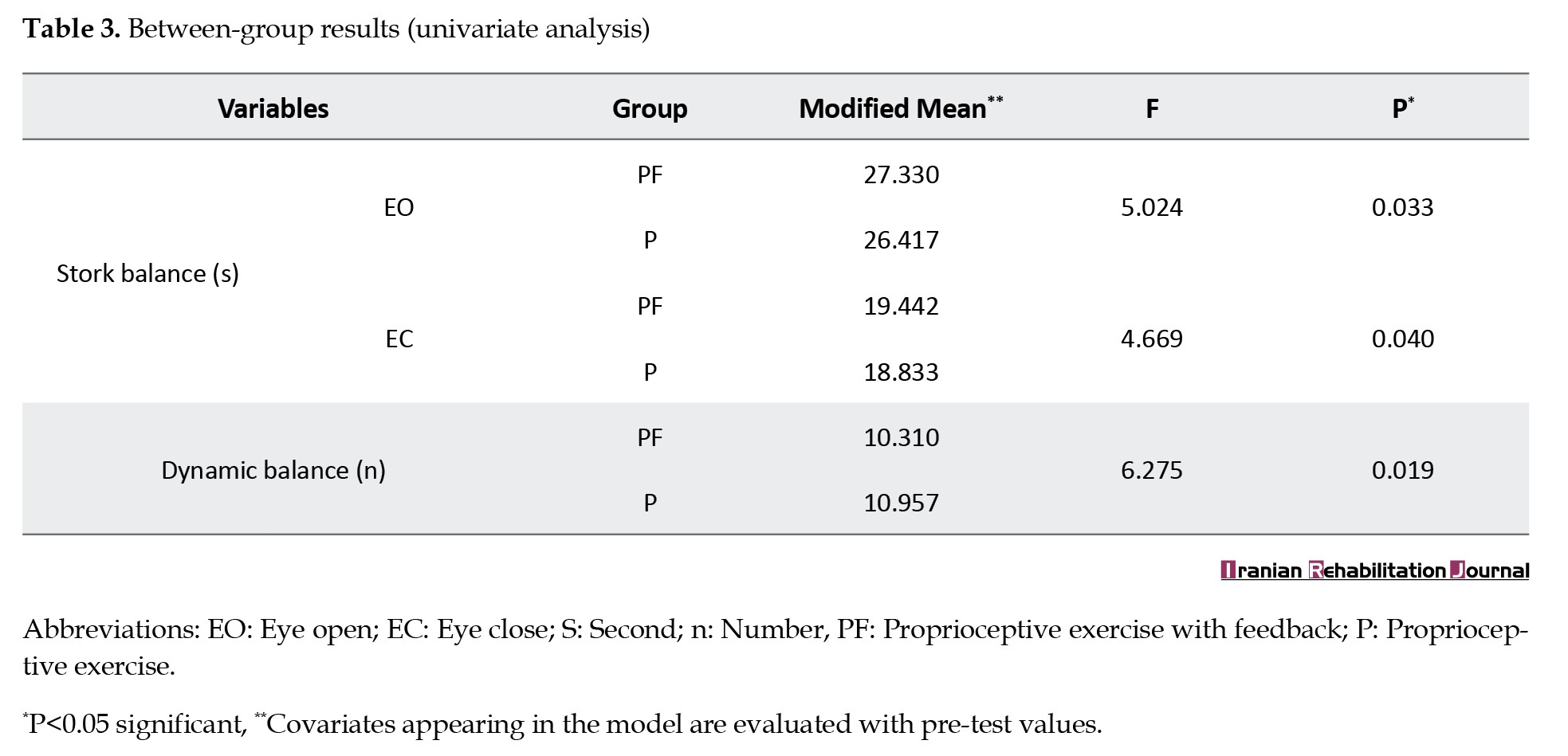
Meanwhile, the homogeneity of variances was assessed using Lune’s test. The results for static balance with eyes open (P=0.785, F=0.76), static balance with eyes closed (P=0.151, F=2.184), and dynamic balance (P=0.510, F=0.445) supported the hypothesis of homogeneity in variances.
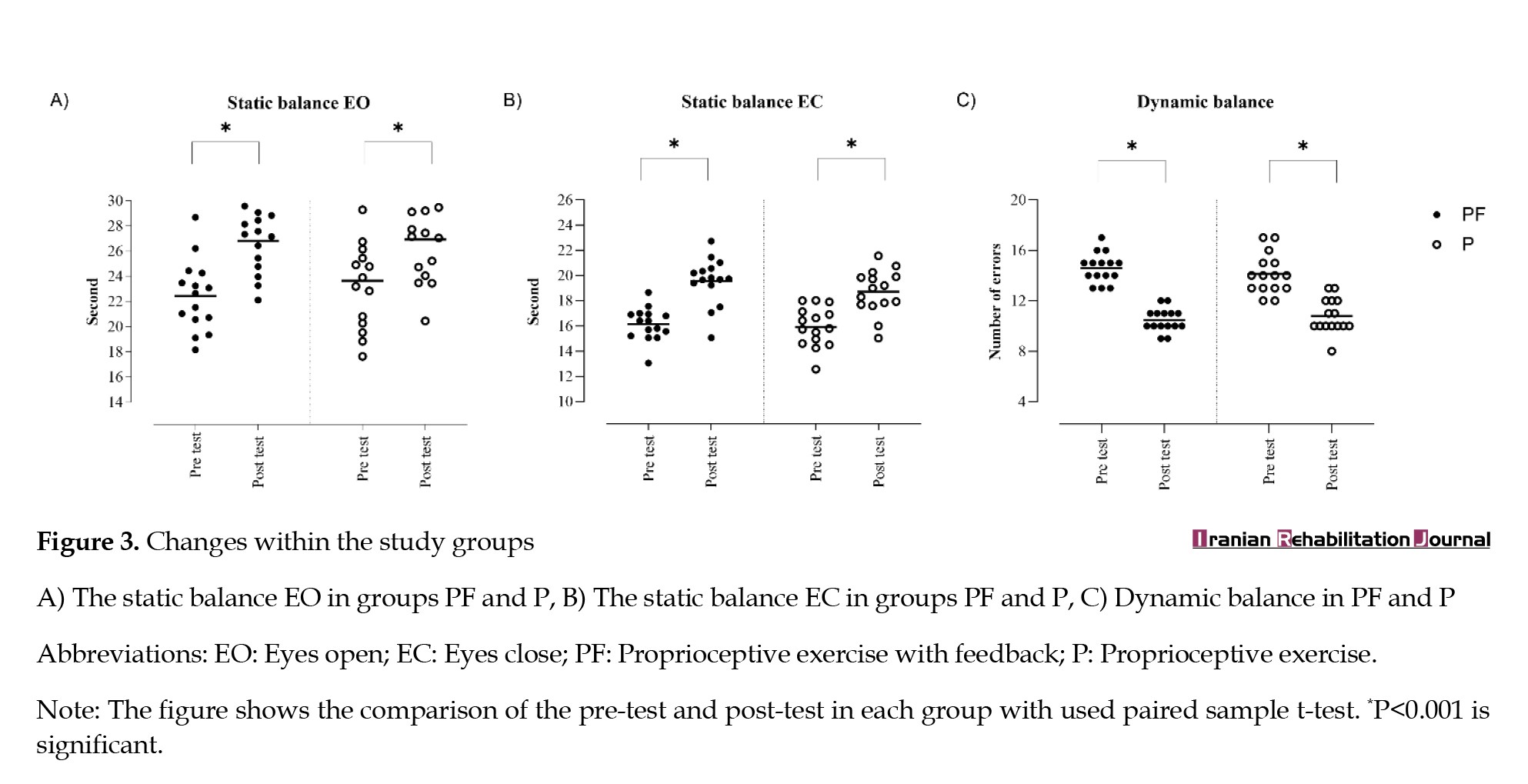
The mean difference is in static balance eyes open (-0.1) and eyes close (1.46), in dynamic balance (-0.33). The effect size of static balance in conditions with eyes open and closed, respectively (η²=0.157,η²=0.189) and in dynamic balance (η²=0.189), which shows that the effect size is weak. Comparing the intragroup changes in variables and changes within the group are shown in Figure 3.
SPSS software, version 27 was utilized for analyzing the collected data. The Shapiro-Wilk test was employed to check the normality of the subjects’ distribution. The paired sample t-test was conducted to examine within-group variations, while univariate analysis was used to compare the two groups. The Lune test was used to confirm the homogeneity of variance. A significance level of 0.05 was considered to interpret the results.
Results
Table 2 presents the descriptive statistics of the demographic characteristics of the subjects, such as mass, height, age, body mass index, FAAM index and FAAM sports index, individually for each group.
According to the results of the Shapiro-Wilk test, all the data follow a normal distribution. The independent t-test results revealed no significant difference across the demographic indicators, suggesting that the subjects exhibited homogeneity in these characteristics.
The comparison between groups was analyzed using univariate variance test and the results are reported in Table 3.
Meanwhile, the homogeneity of variances was assessed using Lune’s test. The results for static balance with eyes open (P=0.785, F=0.76), static balance with eyes closed (P=0.151, F=2.184), and dynamic balance (P=0.510, F=0.445) supported the hypothesis of homogeneity in variances.
The mean difference is in static balance eyes open (-0.1) and eyes close (1.46), in dynamic balance (-0.33). The effect size of static balance in conditions with eyes open and closed, respectively (η²=0.157,η²=0.189) and in dynamic balance (η²=0.189), which shows that the effect size is weak. Comparing the intragroup changes in variables and changes within the group are shown in Figure 3.
In the intra-group comparison section, the findings of the paired sample t-test demonstrate a notable discrepancy in both static and dynamic balances within each group. The mean difference is in exercises in each group in the static balance section with EO in the group of PF (-4.38), in the group P (-3.28), in the section of static balance with EC in the group PF (-3.42), in the group P (-2.78), and in the dynamic balance section, in the group PF (4.13) and the group P (3.33).
Discussion
This study assesses the impact of proprioceptive exercises incorporating visual feedback compared to proprioceptive exercises without feedback on the balance (static and dynamic) of athletes with CAI. The findings showed the effect of both training methods, but in the comparison between these two methods, the effect of proprioceptive exercises with visual feedback was greater than that of proprioceptive exercises without feedback, and there was a significant difference between these two training methods.
Proprioceptive exercises are the cornerstone of rehabilitation for patients with CAI, which have been used in many studies, and their effectiveness has been reported. On the other hand, the ankle joint receptors in the end range of the joint are stimulated, which requires dynamic exercises to improve and sends nerve information to the CNS to maintain stability [23]. When these exercises are combined with visual feedback, the sensory-motor system and the visual system send stimuli to the CNS and cause the entry of more accurate and better information, and the CNS also sends impulses to the organs. It sends messages that improve one’s balance. Learning more and using more effectively in exercises improves neuromuscular control and can affect a person’s balance [24]. Using multiple senses to maintain posture can increase environmental awareness and apply better information as quickly as possible to maintain balance. Among the research in line with this study, the research of Gidu et al. [24], the effect of exercises (P˃0.006, d˂0.610) which shows a moderate effect size of exercises in the results. The research of Parlakidis et al. [25] reported the variations between the experimental group and the control groups (the first group with training without feedback and the second group without training), respectively, P=0.040 and P=0.010 and in the research of Park et al. [26], the effect of proprioception exercises on static (P=0.001) and dynamic (P=0.001) balance was reported. These findings are consistent with the present study, and the reasons that can justify this consistency include proprioceptive exercises, the main purpose of which is to improve the balance of people with CAI. The subjects of these studies were within the same age bracket as this study, and in the two studies of Guido and Parlakides, the subjects were athletes.
The utilization of momentary feedback aids in correcting immediate movements, ensuring optimal conditions, and selecting the best course of action [27]. People with CAI employ a stepping strategy to sustain dynamic equilibrium across various scenarios. Following exercise sessions in both groups, a decline in the use of the stepping strategy was noted, with an enhanced reliance on the hip strategy for posture maintenance. Visual input enhances bilateral weight distribution, thereby enhancing balance [28]. Equitable weight distribution between limbs diminishes body sway during critical moments, optimizing positioning. Notably, individuals utilizing feedback exercises exhibited reduced balance fluctuations and achieved stability swiftly.
These exercises challenge the body’s sense of position and rely on vision and internal cues instead of touch, mechanoreceptors in muscles, and tendons, and stimulate the joints [29]. This increased sensory input is transmitted to the brain and improves its perception of the body’s position in space. Additionally, these exercises improve sensory integration by integrating proprioceptive cues with visual information By doing exercises with eyes closed and then opening them to observe any deviations, the brain learns to accurately perceive the posture and strengthens the neural pathways between the sensory and motor areas, allowing for more precise movement control and adjustments, in addition to optimizing the motor cortex; thus, proprioceptive exercises with visual feedback can indirectly enhance vestibular function [30]. As body position sense improves, the vestibular system receives more correct stimulus about head and body orientation and supports greater balance stability. By targeting these physiological processes, proprioceptive exercises with visual feedback create a positive feedback loop. Improved body awareness leads to better movement control, ultimately reducing the risk of falling and improving overall balance [31, 32].
In Han et al.’s research, the use of feedback is emphasized to maintain better balance, and the use of feedback during exercises is recommended. The use of feedback during performance creates a connection between two people. This relationship can have a significant effect on mental performance and cause motivation, reduce stress, and increase self-confidence [14].
In the research of Yalfani et al. [11], the effectiveness of eight weeks of exercises with and without neurofeedback was observed in the groups (in both experimental groups, the neuromuscular exercises group and the neuromuscular exercises group with neurofeedback, P˃0.001) but in the comparison two experimental groups no significant changes were apperceived in the balance section (except in the A-P direction in the dynamic balance section, P=0.031 and 95% CI, -0.56%, -0.02%). One of the reasons why this study was not aligned with the previous research was that they used neuromuscular exercises in combination with neurofeedback, while proprioceptive exercises are the cornerstone of rehabilitation for people with CAI. The next factor is the difference in the type of feedback, not all people react to the neurofeedback tool in the same way and it may be unpleasant for a group, while visual feedback applied through a mirror may be more user-friendly for subjects and the other hand. The feedback that appears is simpler than neurofeedback, and providing an appropriate response to them may be applied in less time.
In another study, Mohan et al. [33] performed two weeks of mirror therapy to improve balance in people with stroke. The obtained results showed that mirror therapy has no effect on the balance of this group of people does not cause a significant difference (P=0.358) and only leads to the improvement of their mobility. The short duration of training may be a factor that caused such a result. Mohan et al. used 12 rehabilitation sessions over two weeks. The large volume of exercises can take the chance of recovery from the subjects, and for this reason, the subjects may not be ready for the next session and may not do the exercises well. Another difference between this study and the present study was the target community. In the current study, athletes were used to perform exercises. In Mohan’s study, there were people with stroke, this group of people needs a longer intervention to improve the effects of stroke, so that the minimum results are achieved.
Visual feedback exercises spurred heightened motivation among the athletes in this study, influencing efforts to maintain equilibrium. The amalgamation of internal factors like motivation and external factors such as proprioceptive exercises with visual feedback delineates the disparities observed between the groups. Sensory re-weighting can compensate for limitations and defects by utilizing other sensory inputs to maintain optimal conditions. In cases of CAI, this process plays a crucial role in managing chronic injuries. On the other hand, because in people with CAI, the visual system carries more weight to establish balance, sensory reweighting helps a person a lot in chronic injury conditions [34].
The forthcoming study discusses the small impact of the findings but highlights that this approach can be a cost-effective and beneficial addition to achieving goals, including an expedited return to sports. This method not only adds variety to training in the long run, helping to sustain athlete motivation but also fosters a sense of safety and confidence during rehabilitation that can significantly enhance its quality.
Conclusion
The results show that both exercise methods, proprioceptive exercises with visual feedback and proprioceptive exercises without feedback, have affected the desired changes and caused improvement. In the review of the two methods, the results have shown that the method of proprioceptive exercises with feedback is more effective on balance. Proprioceptive exercises with visual feedback are effective in the rehabilitation of athletes with CAI and it is recommended that athletes and coaches use these exercises to reduce the complications of this injury so that they can observe the improvement of their performance after the exercises.
Study limitations
One of the limitations of the research is the lack of examination of the efficacy of exercises on the muscular activities of the lower extremities in the mechanisms of maintaining balance and the lack of access to female subjects to apply intervention on them.
It is suggested that Research comparisons include gender group analyses, especially since male athletes were the focus of the current study. Strengthening research with larger subject pools, diverse age ranges and additional controls can enhance its impact. Recording muscle activities can give us a better understanding of how exercises affect the balance of these people. Future studies should explore different feedback methods alongside comparison techniques to determine effectiveness and optimize rehabilitation processes. Combining feedback methods with various training approaches, such as resistance training, could also benefit the treatment of athletes with CAI.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Iran Institute of Sport Science, Tehran, Iran (Code: IR.SSRC.REC. 1402.283). This study was performed following the standards of ethics outlined in the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the subjects and all the people who somehow contributed to the completion of this study.
Discussion
This study assesses the impact of proprioceptive exercises incorporating visual feedback compared to proprioceptive exercises without feedback on the balance (static and dynamic) of athletes with CAI. The findings showed the effect of both training methods, but in the comparison between these two methods, the effect of proprioceptive exercises with visual feedback was greater than that of proprioceptive exercises without feedback, and there was a significant difference between these two training methods.
Proprioceptive exercises are the cornerstone of rehabilitation for patients with CAI, which have been used in many studies, and their effectiveness has been reported. On the other hand, the ankle joint receptors in the end range of the joint are stimulated, which requires dynamic exercises to improve and sends nerve information to the CNS to maintain stability [23]. When these exercises are combined with visual feedback, the sensory-motor system and the visual system send stimuli to the CNS and cause the entry of more accurate and better information, and the CNS also sends impulses to the organs. It sends messages that improve one’s balance. Learning more and using more effectively in exercises improves neuromuscular control and can affect a person’s balance [24]. Using multiple senses to maintain posture can increase environmental awareness and apply better information as quickly as possible to maintain balance. Among the research in line with this study, the research of Gidu et al. [24], the effect of exercises (P˃0.006, d˂0.610) which shows a moderate effect size of exercises in the results. The research of Parlakidis et al. [25] reported the variations between the experimental group and the control groups (the first group with training without feedback and the second group without training), respectively, P=0.040 and P=0.010 and in the research of Park et al. [26], the effect of proprioception exercises on static (P=0.001) and dynamic (P=0.001) balance was reported. These findings are consistent with the present study, and the reasons that can justify this consistency include proprioceptive exercises, the main purpose of which is to improve the balance of people with CAI. The subjects of these studies were within the same age bracket as this study, and in the two studies of Guido and Parlakides, the subjects were athletes.
The utilization of momentary feedback aids in correcting immediate movements, ensuring optimal conditions, and selecting the best course of action [27]. People with CAI employ a stepping strategy to sustain dynamic equilibrium across various scenarios. Following exercise sessions in both groups, a decline in the use of the stepping strategy was noted, with an enhanced reliance on the hip strategy for posture maintenance. Visual input enhances bilateral weight distribution, thereby enhancing balance [28]. Equitable weight distribution between limbs diminishes body sway during critical moments, optimizing positioning. Notably, individuals utilizing feedback exercises exhibited reduced balance fluctuations and achieved stability swiftly.
These exercises challenge the body’s sense of position and rely on vision and internal cues instead of touch, mechanoreceptors in muscles, and tendons, and stimulate the joints [29]. This increased sensory input is transmitted to the brain and improves its perception of the body’s position in space. Additionally, these exercises improve sensory integration by integrating proprioceptive cues with visual information By doing exercises with eyes closed and then opening them to observe any deviations, the brain learns to accurately perceive the posture and strengthens the neural pathways between the sensory and motor areas, allowing for more precise movement control and adjustments, in addition to optimizing the motor cortex; thus, proprioceptive exercises with visual feedback can indirectly enhance vestibular function [30]. As body position sense improves, the vestibular system receives more correct stimulus about head and body orientation and supports greater balance stability. By targeting these physiological processes, proprioceptive exercises with visual feedback create a positive feedback loop. Improved body awareness leads to better movement control, ultimately reducing the risk of falling and improving overall balance [31, 32].
In Han et al.’s research, the use of feedback is emphasized to maintain better balance, and the use of feedback during exercises is recommended. The use of feedback during performance creates a connection between two people. This relationship can have a significant effect on mental performance and cause motivation, reduce stress, and increase self-confidence [14].
In the research of Yalfani et al. [11], the effectiveness of eight weeks of exercises with and without neurofeedback was observed in the groups (in both experimental groups, the neuromuscular exercises group and the neuromuscular exercises group with neurofeedback, P˃0.001) but in the comparison two experimental groups no significant changes were apperceived in the balance section (except in the A-P direction in the dynamic balance section, P=0.031 and 95% CI, -0.56%, -0.02%). One of the reasons why this study was not aligned with the previous research was that they used neuromuscular exercises in combination with neurofeedback, while proprioceptive exercises are the cornerstone of rehabilitation for people with CAI. The next factor is the difference in the type of feedback, not all people react to the neurofeedback tool in the same way and it may be unpleasant for a group, while visual feedback applied through a mirror may be more user-friendly for subjects and the other hand. The feedback that appears is simpler than neurofeedback, and providing an appropriate response to them may be applied in less time.
In another study, Mohan et al. [33] performed two weeks of mirror therapy to improve balance in people with stroke. The obtained results showed that mirror therapy has no effect on the balance of this group of people does not cause a significant difference (P=0.358) and only leads to the improvement of their mobility. The short duration of training may be a factor that caused such a result. Mohan et al. used 12 rehabilitation sessions over two weeks. The large volume of exercises can take the chance of recovery from the subjects, and for this reason, the subjects may not be ready for the next session and may not do the exercises well. Another difference between this study and the present study was the target community. In the current study, athletes were used to perform exercises. In Mohan’s study, there were people with stroke, this group of people needs a longer intervention to improve the effects of stroke, so that the minimum results are achieved.
Visual feedback exercises spurred heightened motivation among the athletes in this study, influencing efforts to maintain equilibrium. The amalgamation of internal factors like motivation and external factors such as proprioceptive exercises with visual feedback delineates the disparities observed between the groups. Sensory re-weighting can compensate for limitations and defects by utilizing other sensory inputs to maintain optimal conditions. In cases of CAI, this process plays a crucial role in managing chronic injuries. On the other hand, because in people with CAI, the visual system carries more weight to establish balance, sensory reweighting helps a person a lot in chronic injury conditions [34].
The forthcoming study discusses the small impact of the findings but highlights that this approach can be a cost-effective and beneficial addition to achieving goals, including an expedited return to sports. This method not only adds variety to training in the long run, helping to sustain athlete motivation but also fosters a sense of safety and confidence during rehabilitation that can significantly enhance its quality.
Conclusion
The results show that both exercise methods, proprioceptive exercises with visual feedback and proprioceptive exercises without feedback, have affected the desired changes and caused improvement. In the review of the two methods, the results have shown that the method of proprioceptive exercises with feedback is more effective on balance. Proprioceptive exercises with visual feedback are effective in the rehabilitation of athletes with CAI and it is recommended that athletes and coaches use these exercises to reduce the complications of this injury so that they can observe the improvement of their performance after the exercises.
Study limitations
One of the limitations of the research is the lack of examination of the efficacy of exercises on the muscular activities of the lower extremities in the mechanisms of maintaining balance and the lack of access to female subjects to apply intervention on them.
It is suggested that Research comparisons include gender group analyses, especially since male athletes were the focus of the current study. Strengthening research with larger subject pools, diverse age ranges and additional controls can enhance its impact. Recording muscle activities can give us a better understanding of how exercises affect the balance of these people. Future studies should explore different feedback methods alongside comparison techniques to determine effectiveness and optimize rehabilitation processes. Combining feedback methods with various training approaches, such as resistance training, could also benefit the treatment of athletes with CAI.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Iran Institute of Sport Science, Tehran, Iran (Code: IR.SSRC.REC. 1402.283). This study was performed following the standards of ethics outlined in the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the subjects and all the people who somehow contributed to the completion of this study.
References
- Medina McKeon JM, Hoch MC. The ankle-joint complex: A kinesiologic approach to lateral ankle sprains. Journal of Athletic Training. 2019; 54(6):589-602. [DOI:10.4085/1062-6050-472-17] [PMID]
- Cain MS, Ban RJ, Chen YP, Geil MD, Goerger BM, Linens SW. Four-week ankle-rehabilitation programs in adolescent athletes with chronic ankle instability. Journal of Athletic Training. 2020; 55(8):801-10. [DOI:10.4085/1062-6050-41-19] [PMID]
- Hertel J, Corbett RO. An updated model of chronic ankle instability. Journal of athletic training. 2019; 54(6):572-88. [DOI:10.4085/1062-6050-344-18] [PMID]
- Zhang P, Liu F, He X, Brooke-Wavell K, Song Q, Fong DTP. Effect of biophysical interventions on balance and postural control in patients with ankle instability: A systematic review. Medicine in Novel Technology and Devices. 2023; 18:100241. [DOI:10.1016/j.medntd.2023.100241]
- D’Hooghe P, Cruz F, Alkhelaifi K. Return to play after a lateral ligament ankle sprain. Current Reviews in Musculoskeletal Medicine. 2020; 13(3):281-8. [DOI:10.1007/s12178-020-09631-1] [PMID]
- Xue X, Ma T, Li Q, Song Y, Hua Y. Chronic ankle instability is associated with proprioception deficits: A systematic review and meta-analysis. Journal of Sport and Health Science. 2021; 10(2):182-91. [DOI:10.1016/j.jshs.2020.09.014] [PMID]
- Di Giulio I, Maganaris CN, Baltzopoulos V, Loram ID. The proprioceptive and agonist roles of gastrocnemius, soleus and tibialis anterior muscles in maintaining human upright posture. The Journal of Physiology. 2009; 587(Pt 10):2399-416. [DOI:10.1113/jphysiol.2009.168690] [PMID]
- Swaby L, Shu P, Hind D, Sutherland K. The use of cognitive task analysis in clinical and health services research-a systematic review. Pilot and Feasibility Studies. 2022; 8(1):57. [DOI:10.1186/s40814-022-01002-6] [PMID]
- Song K, Burcal CJ, Hertel J, Wikstrom EA. Increased visual use in chronic ankle instability: A meta-analysis. Medicine and Science in Sports and Exercise. 2016; 48(10):2046-56. [DOI:10.1249/MSS.0000000000000992] [PMID]
- Grooms D, Appelbaum G, Onate J. Neuroplasticity following anterior cruciate ligament injury: a framework for visual-motor training approaches in rehabilitation. Journal of Orthopaedic & Sports Physical Therapy. 2015; 45(5):381-93. [DOI:10.2519/jospt.2015.5549] [PMID]
- Yalfani A, Azizian M, Gholami-Borujeni B. Neurofeedback training can increase the effectiveness of neuromuscular training on balance and limit of stability of athletes with chronic ankle instability: three arms and single-blind randomized control trial. Sport Sciences for Health. 2024; 20:1343-52. [DOI:10.1007/s11332-024-01212-w]
- Van Emmerik REA, Remelius JG, Johnson MB, Chung LH, Kent-Braun JA. Postural control in women with multiple sclerosis: Effects of task, vision and symptomatic fatigue. Gait & posture. 2010; 32(4):608-14. [DOI:10.1016/j.gaitpost.2010.09.002] [PMID]
- Song K, Rhodes E, Wikstrom EA. Balance training does not alter reliance on visual information during static stance in those with chronic ankle instability: A systematic review with meta-analysis. Sports Medicine. 2018; 48(4):893-905. [DOI:10.1007/s40279-017-0850-8] [PMID]
- Han S, Lee H, Son SJ, Hopkins JT. The effects of visual feedback disruption on postural control with chronic ankle instability. Journal of Science and Medicine in Sport. 2022; 25(1):53-7. [DOI:10.1016/j.jsams.2021.07.014] [PMID]
- Kok M, Komen A, van Capelleveen L, van der Kamp J. The effects of self-controlled video feedback on motor learning and self-efficacy in a Physical Education setting: An exploratory study on the shot-put. Physical Education and Sport Pedagogy. 2020; 25(1):49-66. [DOI:10.1080/17408989.2019.1688773]
- Hunt MA, Takacs J, Hart K, Massong E, Fuchko K, Biegler J. Comparison of mirror, raw video, and real-time visual biofeedback for training toe-out gait in individuals with knee osteoarthritis. Archives of Physical Medicine and Rehabilitation. 2014; 95(10):1912-7. [DOI:10.1016/j.apmr.2014.05.016] [PMID]
- Hupperets MDW, Verhagen EALM, Heymans MW, Bosmans JE, van Tulder MW, Van Mechelen W. Potential savings of a program to prevent ankle sprain recurrence: Economic evaluation of a randomized controlled trial. The American Journal of Sports Medicine. 2010; 38(11):2194-200. [DOI:10.1177/0363546510373470] [PMID]
- Beydagı MG, Talu B. The effect of proprioceptive exercises on static and dynamic balance in professional athletes. Annals of Clinical and Analytical Medicine. 2021; 12(S 1):S49-53. [DOI:10.4328/ACAM.20327]
- Li Y, Tsang RCC, Liu D, Ruan B, Yu Y, Gao Q. Applicability of cutoff scores of Chinese Cumberland Ankle Instability Tool and Foot and Ankle Ability Measure as inclusion criteria for study of chronic ankle instability in Chinese individuals. Physical Therapy in Sport. 2021; 48:116-20. [DOI:10.1016/j.ptsp.2020.12.021] [PMID]
- Villarón-Casales C, Aladro-Gonzalvo AR, Gámez-Payá J, Pardo-Ibáñez A, Domínguez-Navarro F, Gallego D, et al. Static postural control during single-leg stance in endurance, team and combat athletes from the Spanish national sport technification program. International Journal of Environmental Research and Public Health. 2023; 20(5):4292. [DOI:10.3390/ijerph20054292] [PMID]
- Bouteraa I, Negra Y, Shephard RJ, Chelly MS. Effects of combined balance and plyometric training on athletic performance in female basketball players. The Journal of Strength & Conditioning Research. 2020; 34(7):1967-73. [DOI:10.1519/JSC.0000000000002546] [PMID]
- Sawle L, Freeman J, Marsden J. Intra-rater reliability of the multiple single-leg hop-stabilization test and relationships with age, leg dominance and training. International Journal of Sports Physical Therapy. 2017; 12(2):190-8. [PMID]
- Dhillon MS, Patel S, Baburaj V. Ankle sprain and chronic lateral ankle instability: Optimizing conservative treatment. Foot and Ankle Clinics. 2023; 28(2):297-307. [DOI:10.1016/j.fcl.2022.12.006] [PMID]
- Gidu DV, Badau D, Stoica M, Aron A, Focan G, Monea D, et al. The effects of proprioceptive training on balance, strength, agility and dribbling in adolescent male soccer players. International Journal of Environmental Research and Public Health. 2022; 19(4):2028. [DOI:10.3390/ijerph19042028] [PMID]
- Parlakidis K, Kontopoulos LA, Mandalidis D, Paraskevopoulos E, Papandreou M, Kapreli E, et al. The effectiveness of external verbal feedback on balance in athletes with chronic ankle instability. Journal of Functional Morphology and Kinesiology. 2024; 9(1):56. [DOI:10.3390/jfmk9010056] [PMID]
- Park YJ, Cho YH, Seo TB. Effect of two different exercises on balance, pain and ankle motor function in male college students with chronic ankle instability. Journal of Men’s Health. 2023; 19(2):51-7. [Link]
- Kim H, Kim H, Shin WS. Effects of vibrotactile Biofeedback providing real-time pressure information on static balance ability and Weight Distribution Symmetry Index in patients with chronic stroke. Brain Sciences. 2022; 12(3):358. [DOI:10.3390/brainsci12030358] [PMID]
- Pellegrino L, Giannoni P, Marinelli L, Casadio M. Effects of continuous visual feedback during sitting balance training in chronic stroke survivors. Journal of Neuroengineering and Rehabilitation. 2017; 14(1):107. [DOI:10.1186/s12984-017-0316-0] [PMID]
- Henry M, Baudry S. Age-related changes in leg proprioception: implications for postural control. Journal of Neurophysiology. 2019; 122(2):525-38. [DOI:10.1152/jn.00067.2019] [PMID]
- Ueta Y, Matsugi A, Oku K, Okuno K, Tamaru Y, Nomura S, et al. Gaze stabilization exercises derive sensory reweighting of vestibular for postural control. Journal of Physical Therapy Science. 2017; 29(9):1494-6. [DOI:10.1589/jpts.29.1494] [PMID]
- Maksimovic S, Neville KM, Cressman EK. Experiencing the cross-sensory error signal during movement leads to proprioceptive recalibration. Journal of Motor Behavior. 2020; 52(1):122-9. [DOI:10.1080/00222895.2019.1574258] [PMID]
- Peterka RJ. Sensory integration for human balance control. Handbook of Clinical Neurology. 2018; 159:27-42. [DOI:10.1016/B978-0-444-63916-5.00002-1] [PMID]
- Mohan U, Kumar KV, Suresh BV, Misri ZK, Chakrapani M. Effectiveness of mirror therapy on lower extremity motor recovery, balance and mobility in patients with acute stroke: A randomized sham-controlled pilot trial. Annals of Indian Academy of Neurology. 2013; 16(4):634-9. [DOI:10.4103/0972-2327.120496] [PMID]
- Sugimoto YA, McKeon PO, Rhea CK, Schmitz RJ, Henson R, Mattacola CG, et al. Sensory reweighting system differences on vestibular feedback with increased task constraints in individuals with chronic ankle instability compared to healthy controls. Journal of Athletic Training. 2024 ;59(7):713-23. [DOI:10.4085/1062-6050-0246.22] [PMID]
Article type: Original Research Articles |
Subject:
Sport rehabilitation
Received: 2024/03/27 | Accepted: 2024/07/1 | Published: 2025/03/1
Received: 2024/03/27 | Accepted: 2024/07/1 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
