
988368
Mon, Jul 27, 2026

Volume 23, Issue 3 (September 2025)
Iranian Rehabilitation Journal 2025, 23(3): 277-286 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Pourmohamadreza-Tajrishi M, Mirzaee R, Ghobari Bonab B. The Efficacy of Cognitive-behavioral Play Therapy on Internalizing Behavior Problems. Iranian Rehabilitation Journal 2025; 23 (3) :277-286
URL: http://irj.uswr.ac.ir/article-1-2320-en.html
URL: http://irj.uswr.ac.ir/article-1-2320-en.html



1- Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Psychology and Education of Exceptional Children, Faculty of Psychology and Educational Sciences, Tehran University, Tehran, Iran.
2- Department of Psychology and Education of Exceptional Children, Faculty of Psychology and Educational Sciences, Tehran University, Tehran, Iran.
Full-Text [PDF 520 kb]
(1044 Downloads)
| Abstract (HTML) (3293 Views)
Full-Text: (574 Views)
Introduction
Behavioral and emotional problems in children refer to conditions in which there is a disparity between children’s behaviors in educational and domestic settings compared to societal norms. These conditions have a detrimental impact on children’s academic performance, social interactions, adaptability, and self-preservation [1]. Achenbach and Rescorla [2] introduced the most renowned classification of these issues, categorizing them into internalizing and externalizing problems. Internalizing problems encompass interpersonal challenges, such as social withdrawal, inhibition, anxiety, depression, and somatic complaints (SC) [2]. Statistics indicate that 17.8% to 34.4% of school-aged children [3], 10% to 20% [4], and 20.3% in Iran [5] suffer from internalizing problems. These problems typically manifest early in childhood [6] and can have enduring negative repercussions if left unresolved, even in adolescence and adulthood [1].
Due to the high prevalence and long-term effects of internalizing disorders in recent years, mental health professionals have been diligently seeking effective strategies and interventions to prevent and ameliorate issues in at-risk children. Various methodologies have been employed to mitigate these problems, with play therapy emerging as a prominent solution. Knell [7] extended the theoretical frameworks of Beck, Ellis, and Bandura by incorporating play techniques to address children’s emotional and behavioral challenges, fostering improved social interactions and problem-solving skills. Efficacious treatments for childhood disorders exist, supported by empirical evidence, with cognitive-behavioral play therapy (CBPT) being a notable intervention for anxiety and depression. CBPT, tailored for young children, integrates theories pertinent to psychopathology, emotional growth, and cognitive development [8]. This approach involves personalized assessments and interventions designed to enhance behavioral competence. Therapists utilize simulated scenarios from child’s life, employing modeling, role-playing, and desensitization techniques to facilitate behavioral modifications. Adapting cognitive therapy to suit child’s developmental stage without complex language is a key challenge faced by CBPT practitioners. As described by Knell [7], therapists can employ accessible tools, such as puppets, stuffed animals, and age-appropriate books, to demonstrate cognitive strategies for problem-solving in children.
Knell [7] conceptualized CBPT with a focus on developmental issues and cognitive and behavioral therapies, emphasizing its empirical validation. Playing offers numerous benefits for children by providing a platform for expressing emotions straightforwardly and effectively and helping them confront unpleasant experiences. Play helps children enhance and fortify their internal resources through verbal and nonverbal communication. Through play therapy, children experience emotional release and gain control over their environment, thereby fostering increased motivation to continue playing while deriving enjoyment from it [1, 9].
A review of the literature demonstrates that several studies have highlighted the effectiveness of play therapy in reducing anxiety, phobias, suicide risk, depression, internalizing problems, and emotional/behavioral disorders [9], while also enhancing self-concept, cognitive abilities, social skills, and self-confidence in children. Another study revealed that play therapy decreased depression, anxiety, and worry in children [10, 11]. Given the various studies in the realm of play therapy and the potential overlooking of covert internalizing issues without necessary follow-up, further research is warranted to explore CBPT as an effective approach for addressing internalizing problems in boys. While parental social support serves as a buffer against internalizing problems in girls, the same protective effect is not observed in boys [12]. As behavioral issues commonly manifest in school-aged children and peak between the ages of 8-15 [13], intervening to curb or prevent behavioral and emotional problems in boys can secure their social well-being. This study aimed to assess the efficacy of CBPT in addressing internalizing problems (and their facets) in 8-10-year-old boys, while also investigating its impact on reducing depression and anxiety levels in this demographic.
Materials and Methods
This study adopted a quasi-experimental design with pre-test and post-test structures. The study sample consisted of 391 boys aged 8-10, selected through cluster sampling during the 2017-18 academic year. Children and their parents who expressed a willingness to participate were requested to complete the questionnaires. Adherence to ethical guidelines, including obtaining informed consent, ensuring confidentiality of participant information, and offering the option to withdraw from the study, was maintained.
Guided by prior research, the sample size was determined using the sample size formula, targeting a test power of 0.90, a test error of 0.05, and accounting for potential sample loss, resulting in the selection of 42 participants. The inclusion criteria included achieving a score of T ≥63 on the children’s behavior checklist, (CBCL) a score of ≥60 on the multidimensional anxiety scale (MASC) for children, a score of ≥18 on the children’s depression inventory (CDI), a diagnosis of internalizing disorders through psychiatric assessment, the absence of sensory impairments or neurodevelopmental disorders, and no concurrent engagement in play therapy sessions. All participants were randomly assigned to the experimental or control group. The experimental group underwent 14 therapeutic sessions involving CBPT once a week for 45 minutes per session, whereas the control group received the standard school program. The data collection tools included the CBCL, MASC for children, and CDI.
CBCL
The CBCL was utilized to assess internalizing problems in children. The CBCL comprises two sections, with this study focusing on the second section, which pertains to symptoms associated with internalizing behaviors. The overall reliability of the CBCL, as indicated by Cronbach’s α, was 0.97. Minaee [14] translated the CBCL into Persian, establishing a cutoff point of T=63 for identifying internalizing disorders. Test, re-test results over a 5 to 8-week interval ranged from 0.32 to 0.67, indicating the instrument’s stability over time. This 113-item checklist is specifically designed for individuals aged 6-18 and can be completed by parents or legal guardians. Internalizing problems are derived from the cumulative scores across three scales: Anxious/depressed (AD), withdrawn/depressed (WD), and SC. In a previous study, the internalizing behaviors scale exhibited a Cronbach’s α of 0.65 [15].
MASC for children
The MASC developed by March [16], is a standardized self-report questionnaire comprising 39 items designed to assess anxiety levels in individuals aged 8-19 years. Principal component analysis revealed four distinct scales within the MASC: social anxiety, separation anxiety, harm avoidance, and physical symptoms, which collectively contribute to the overall measure of anxiety [16]. Anxiety levels are categorized into three tiers based on scores: Mild (zero to 40), moderate (40-60), and high (≥60). The reliability and internal consistency of the MASC in assessing total anxiety yielded values ranging from 0.48-0.79. Factor analysis conducted on the Iranian population confirmed the adequacy of the four-factor model of the MASC, with a reported Cronbach’s α coefficient of 0.77 [17].
CDI
The CDI is a 27-item self-report questionnaire designed to differentiate depression from other disorders. The CDI offers two forms, including the original 27-item version. Each item presents three options, and the child is required to select the option that most accurately reflects their emotions over the preceding two weeks using a 4-point Likert scale.
To assess the various components of depression, the CDI includes five subscales: Anhedonia, ineffectiveness, interpersonal problems, negative mood, and negative self-esteem. The CDI is considered a reliable tool for evaluating depression in children, with a cut-off point typically falling within the range of 19 to 20; individual circumstances should also be considered.
A score of 36 or higher indicates a relatively severe level of depression. The CDI exhibits a Cronbach’s α ranging from 0.71 to 0.89 [18], affirming its internal consistency. Additionally, the instrument’s construct and discriminant validity have been established [19].
CBPT
The CBPT intervention protocol was originally conceptualized by Knell [20] based on cognitive behavioral therapy and tailored for children. The complexity of the CBPT was simplified to align with the child’s developmental stage. Young children are encouraged to understand the connection between their behavior and emotions, enabling them to express their feelings more adaptively and effectively. Through play, the child communicates his needs, and the therapist acknowledges and values these moments of communication.
To establish goals for the child, the therapist engages both the child and the family, guiding the child to achieve these goals and monitoring progress over time. The therapist selects play materials, such as animal puppets and stuffed animals, and engages in activities, such as role-playing, modeling, drawing, and storytelling. Additionally, themes and psychoeducational aspects of the treatment are introduced to assist the child in replacing ineffective methods with positive coping skills. Ultimately, CBPT helps child articulate their conflicts, problems, and their connection to behavior through verbal expression.
The CBPT program consists of 14 sessions, each structured into different stages (introduction and preparation, assessment, intermediate, and final stages) to support children in recognizing their role in changing behaviors. Following preparation, the evaluation phase begins, where the child’s abilities and challenges are assessed, leading to the development of a treatment plan aimed at enhancing self-control, progressive tension, and coping strategies to acquire new beneficial skills. The therapeutic journey concludes with the child and family preparing for the end of the session [21]. The CBPT intervention utilized in the current research is drawn from Knell’s model [20] and tailored for children with anxiety.
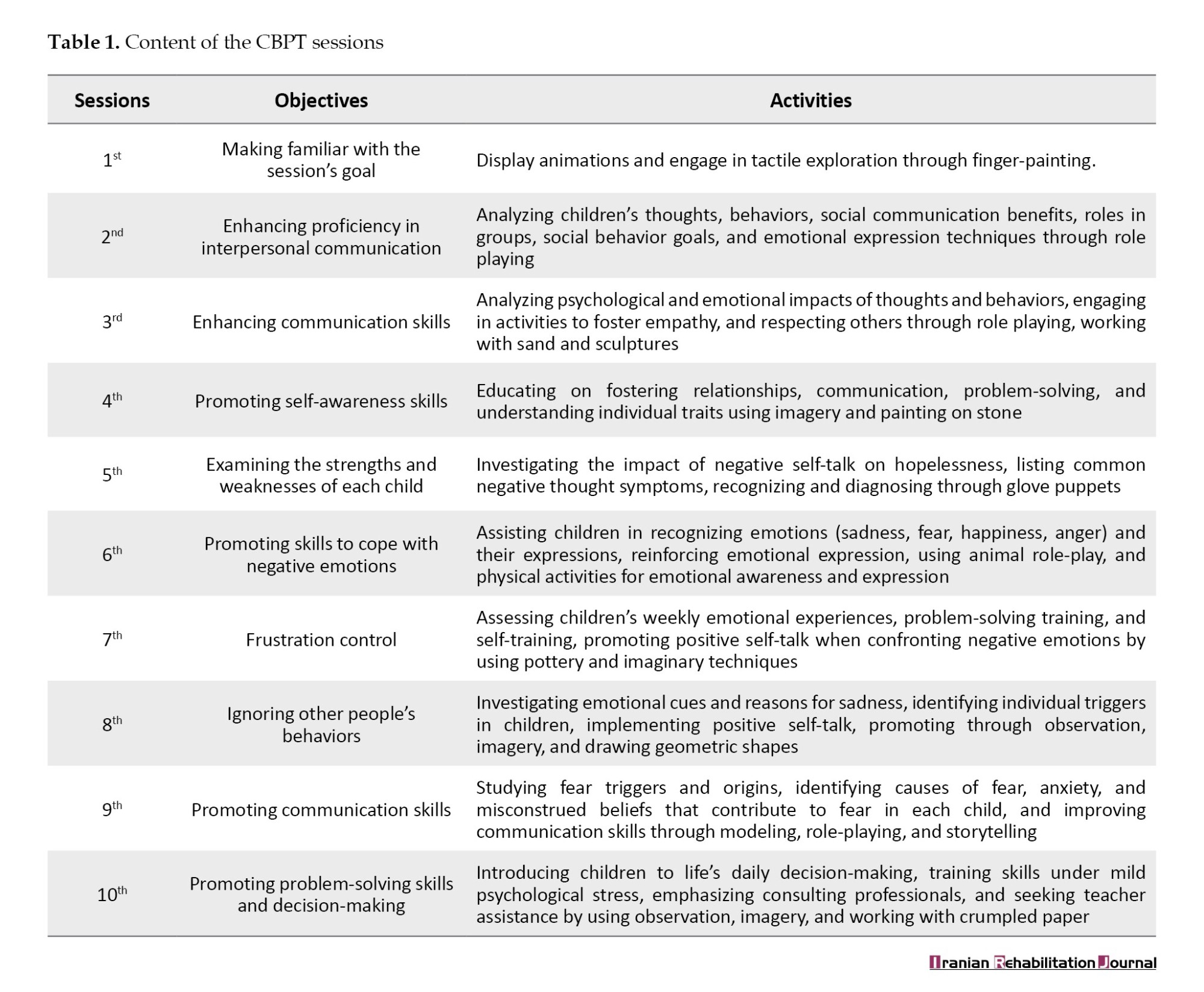
After collecting the data, SPSS software, version 21 was used to describe the data (Mean±SD) and to analyze the data, including the multivariate analysis of covariance (MANCOVA) method. Table 1 presents the content of the CBPT intervention for each session.
Results
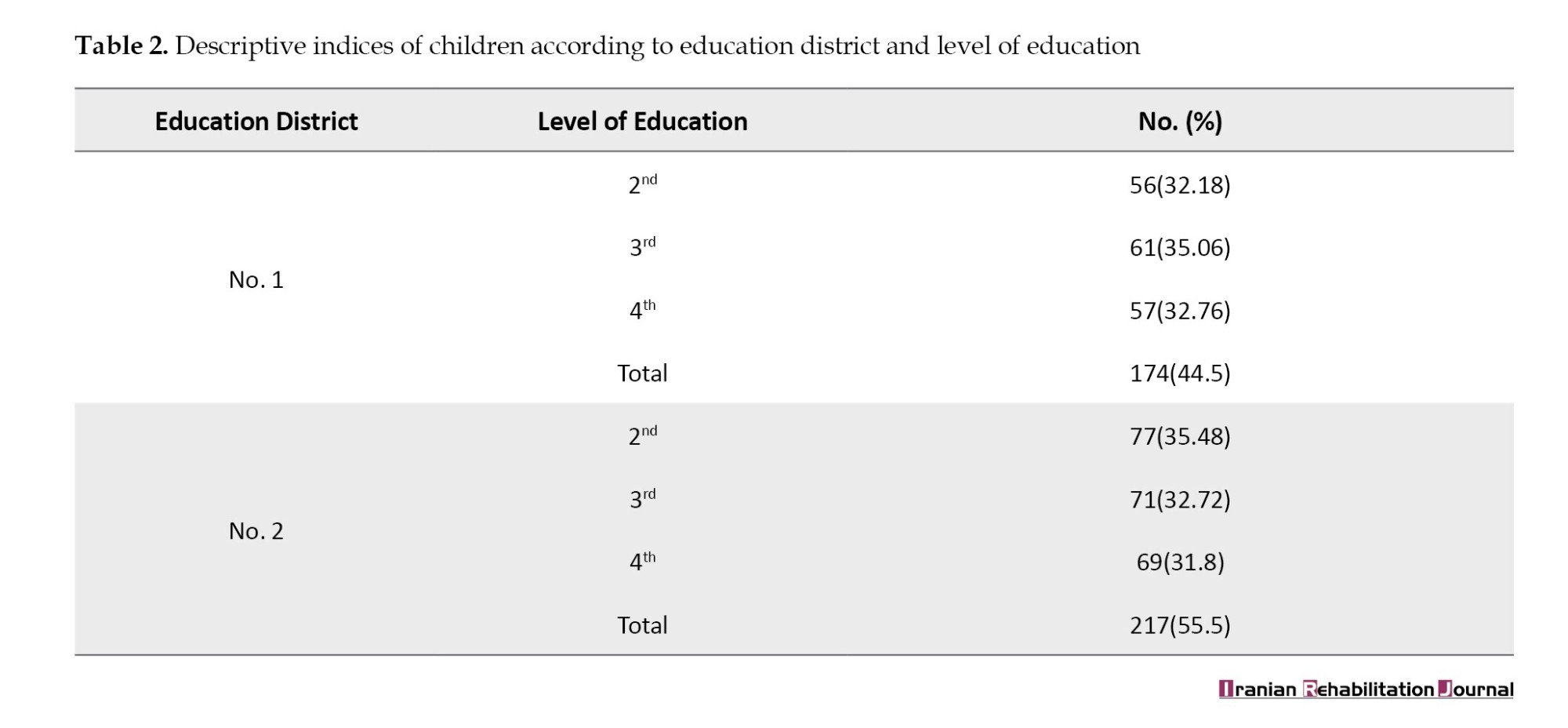
The mean age of the experimental group was 9.24±0.77, slightly higher than the control group’s average of 9.05±0.87. This data is presented in Table 2, which illustrates the frequency and percentage of total students categorized by education district and educational level. In Table 2, it is evident that out of the selected students, 174(44.5%) were male from education district No. 1, while 217(55.5%) were from education district No. 2. The majority of participants were enrolled in the third grade (35.06%) and second grade (35.46%) within their respective education districts. Among the 391 male students, 53 individuals from the second to fourth grades (16, 18, and 19, respectively) who scored above the cut-off points in the CBCL (≥63), MASC (≥60), and CDI (≥19) were interviewed by a psychiatrist. Subsequently, 42 students diagnosed with internalizing disorders were randomly chosen for further analysis.
Chi-square test analysis indicated no significant difference in age between the experimental and control groups (P=0.909, χ2=0.545). Similarly, no significant difference was observed between the two groups in terms of educational level (grade) (P=0.881, χ2=0.254).
Table 3 presents descriptive indices of internalizing problems (including their dimensions), anxiety, and depression symptoms for two groups in both pre-test and post-test scenarios.
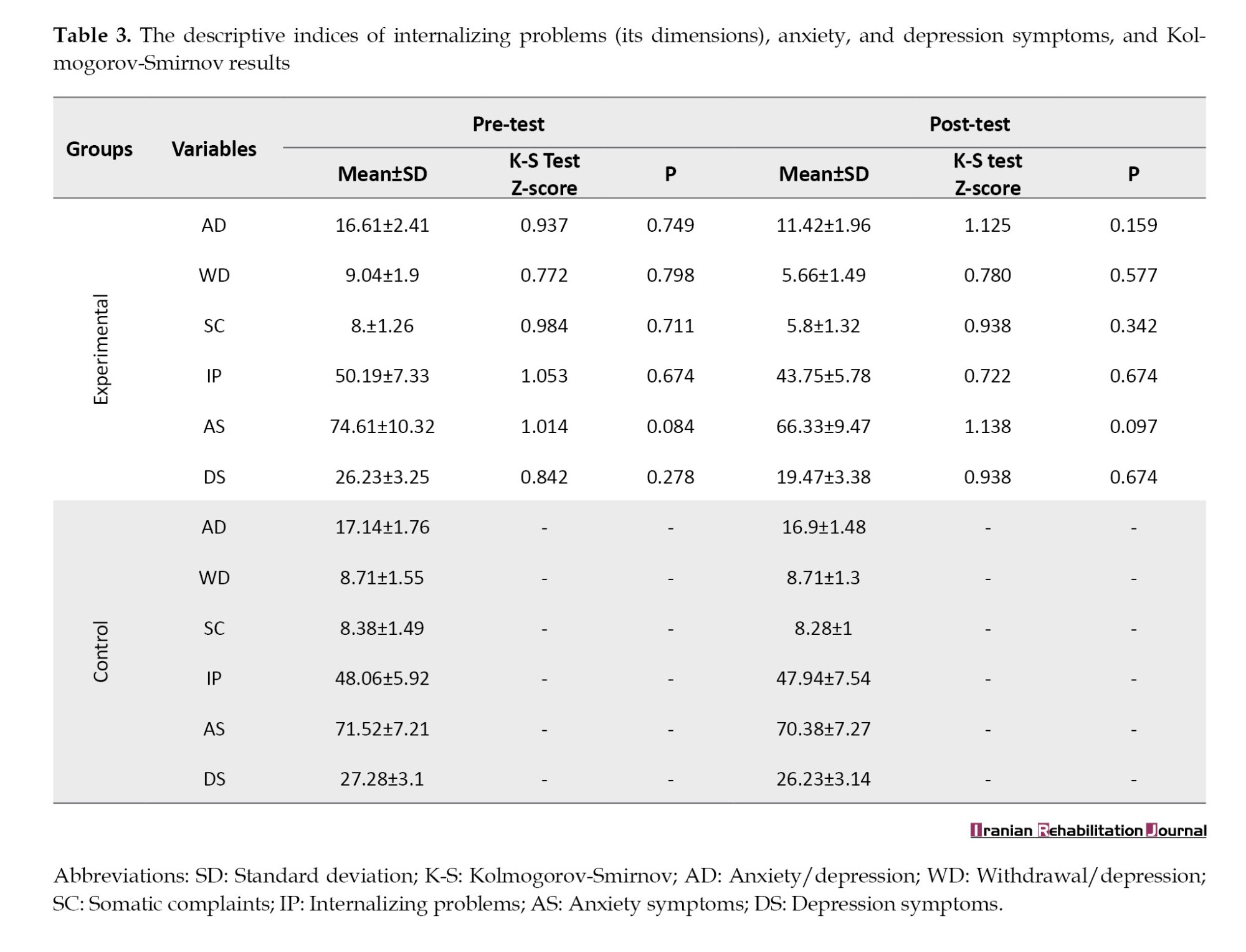
Table 4 presents the descriptive statistics for the indices derived from MASC, CBCL, and CDI in the pre-test and post-test situations. The normality of the variables was assessed using the Kolmogorov-Smirnov (K-S) test, confirming the assumption of MANCOVA (Table 3).
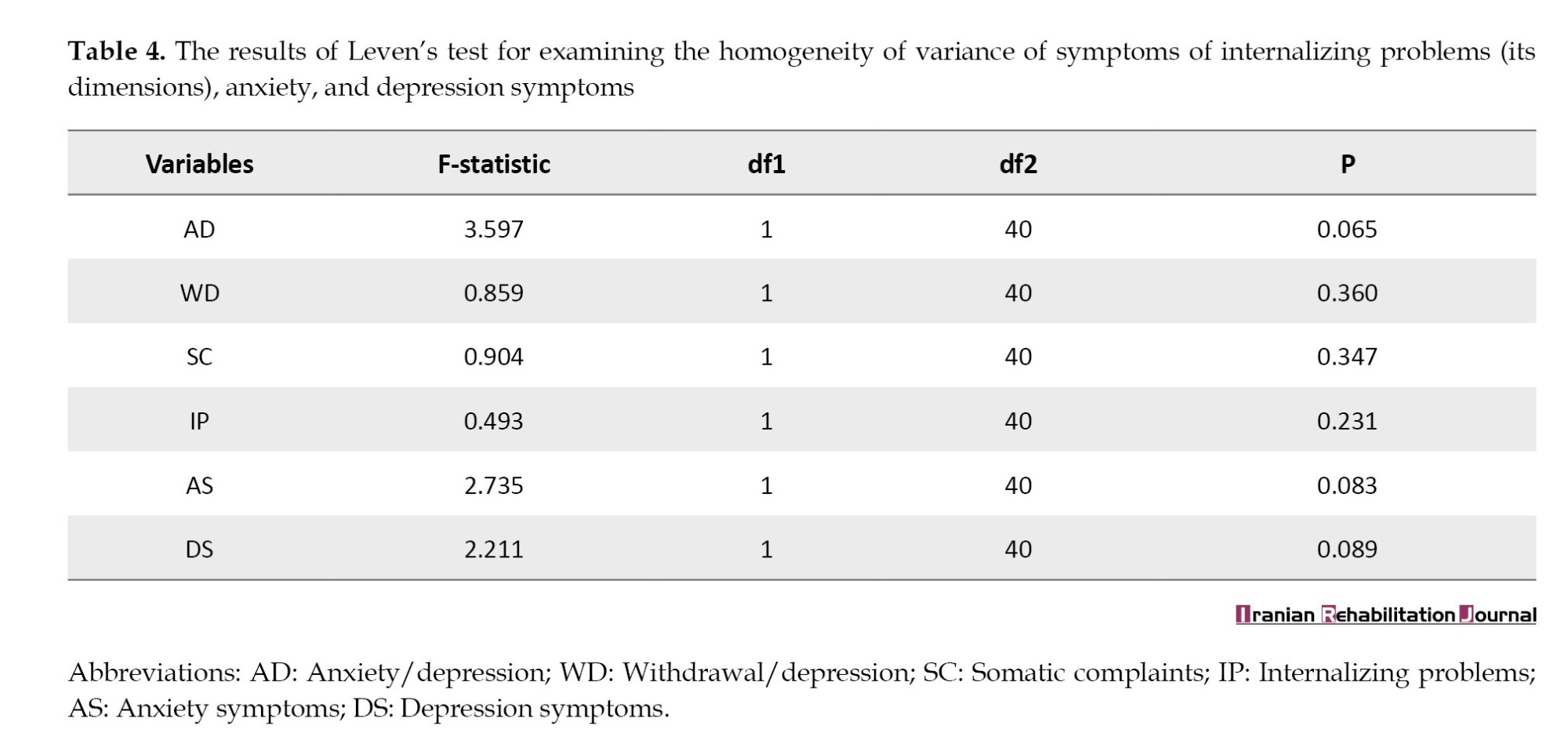
Table 3 reveals that no significant difference is observed between the pre-test and post-test scores in the control group. Furthermore, the scores of the experimental group decreased in the post-test compared to the pre-test. Considering a significance level of P<0.05 for all variables, we concluded that all scores exhibited a normal distribution. The outcomes of Levene’s test indicated that the variances in both groups were homogeneous (Table 4).
Having validated all the assumptions required for MANCOVA, it can be utilized to compare internalizing problems and their dimensions (anxiety/depression, isolation/depression, physical complaints) between the experimental and control groups. Table 5 presents the overall outcomes of the multivariate analysis of variance. To investigate the research hypothesis, which states “CBPT enhances internalizing problems (and its three dimensions), anxiety, and depression symptoms in children,” we employed MANCOVA (Table 5).
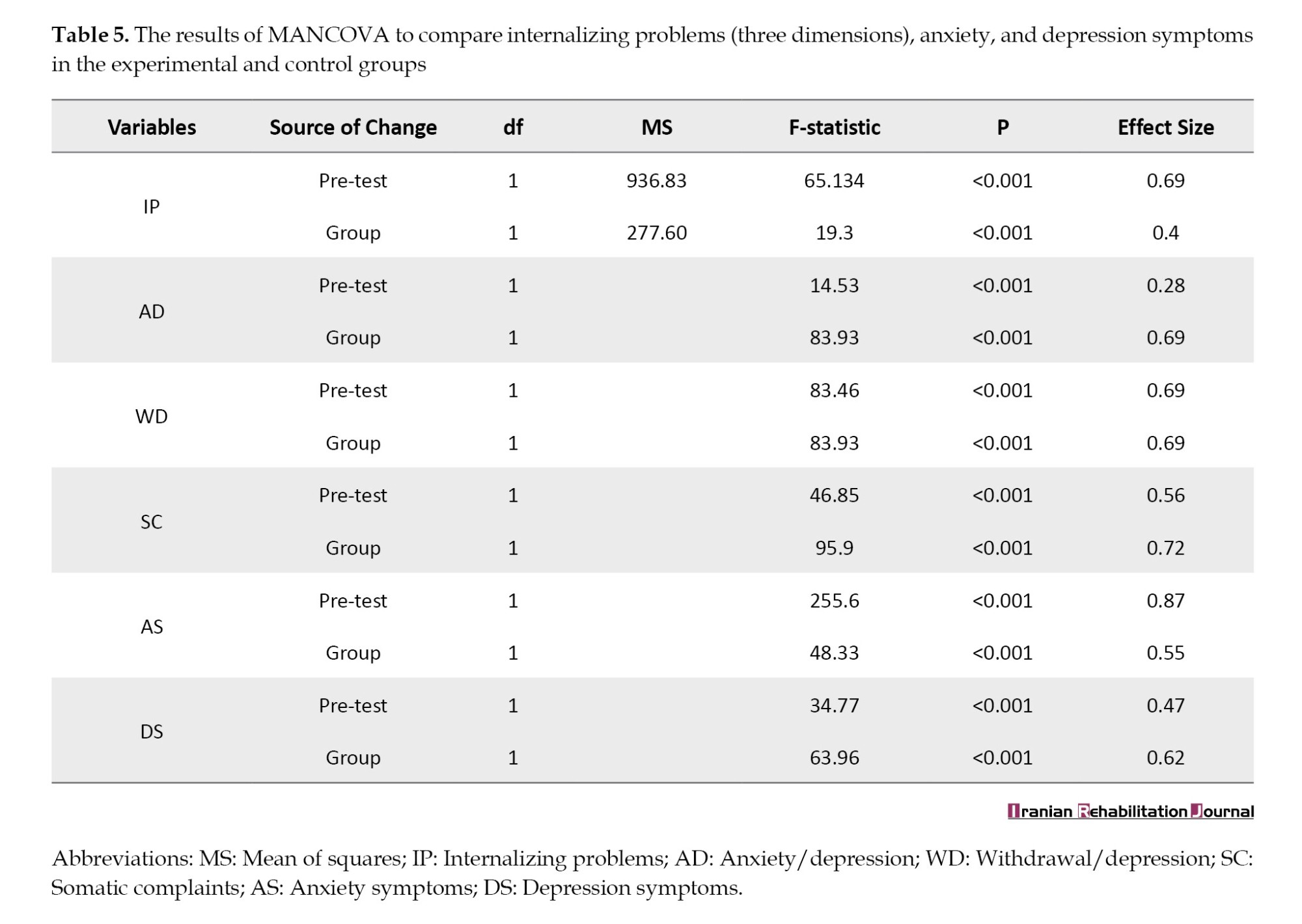
Based on the MANCOVA results, the F-statistics were 83.93, 83.93, 95.90, 19.30, 43.33, and 63.96, with P<0.001 for internalizing problems, anxiety/depression, withdrawal/depression, SC, anxiety symptoms, and depression symptoms, respectively, confirming the hypotheses. Consequently, the administration of CBPT to the experimental group led to a significant improvement in internalizing problems (anxiety/depression, withdrawal/depression, and SC), anxiety, and depression symptoms among male students. The effect sizes indicated that 0.40, 0.69, 0.69, and 0.72 of the variations in internalizing problems, anxiety/depression, withdrawal/depression, and SC in students were attributed to their participation in CBPT. Furthermore, a significant difference (P<0.001) was observed in anxiety and depression symptoms between the two groups in the post-test phase. It can be inferred that 0.55 and 0.62 of the changes in anxiety and depression symptoms in the experimental group were influenced by their engagement in CBPT sessions.
Discussion
This study investigated the potential positive impact of CBPT on internalizing problems (specifically anxiety/depression, withdrawal/depression, and SC), as well as anxiety and depression symptoms in boys aged 8–10 years. The results indicated a beneficial effect of CBPT in enhancing internalizing problems (including its various dimensions), anxiety, and depression symptoms. These findings are consistent with those of previous studies [22].
One possible explanation for these findings is that young children, due to their limited flexibility and insufficient cognitive skills in the preoperational stage of development, may struggle to follow rational sequences and differentiate between logical and illogical thinking. During this stage, children tend to think egocentrically, concretely, and irrationally, often acting impulsively or without adequate cognitive maturity [20]. Consequently, they may act before thinking things through. However, it is feasible for young children to learn to associate their behaviors with their emotions and express their feelings in more adaptive ways. This capability enables them to develop a sense of control and receive positive reinforcement from their environment. Play serves as a natural avenue through which children can communicate [23]. Numerous evidence-based studies have supported the positive effects [20] and long-term benefits [24] of CBPT on behavioral problems.
This finding is consistent with that of a previous research [9]. This can be explained by the fact that internalizing problems, anxiety, and depression symptoms can exacerbate aggressive and rule-breaking behaviors [24]. Ensuring the child’s continuous engagement is crucial, as CBPT should offer an engaging platform that allows children to fully experience therapy. The level of engagement between children and CBPT plays a pivotal role in the success of a child’s therapy. Factors to concentrate on to enhance continuous engagement [25] include motivation, relaxation, attention, the child’s willingness to repeat, ease of learning, and problem-solving capabilities throughout CBPT sessions. Moreover, low parental involvement has been positively correlated with improvements in internalizing problems, anxiety, and depression symptoms in children. This finding suggests that when parents are less involved in treatment, children may express anxious and arousing behaviors more freely while the therapist provides guidance. Conversely, high parental involvement may trigger previous patterns of child-parent interaction, making it difficult to test new behaviors beneficial for reducing internalizing problems or anxiety and depression symptoms in children. Previous studies have yielded varied results regarding the role of parental involvement in CBPT [8].
The second finding supports the effectiveness of CBPT in improving anxiety symptoms, consistent with previous research [26]. One possible explanation is that the child actively engages in mastering and addressing issues. During CBPT sessions, child may intentionally place themselves in stressful scenarios and communicate their needs through role-playing exercises. Through these interactions, child can enhance their communication skills and develop a close rapport with the therapist. This process allows the child to recall and reinterpret significant themes and events from their life, leading to increased awareness and the ability to approach conflicts more adaptively [27, 28]. Moreover, acquiring strategies to regulate negative emotions enables children to acknowledge and embrace their feelings. The therapist’s emphasis on confronting negative self-talk and instructing children to replace maladaptive thoughts with more positive self-talk helps alleviate their concerns and foster emotional well-being.
The third finding validates the effectiveness of CBPT in addressing SC in children, consistent with previous research [29]. This finding can be explained by the high prevalence of SC among many children in our sample, leading to prolonged school absences and disruptions to daily activities. The study participants often sought medical consultation, underwent expensive diagnostic procedures, and relied on medication. A significant proportion of the sample exhibited psychosomatic symptoms or widespread pain linked to anxiety-provoking situations. Consequently, conventional intervention approaches that view SC as expressions of anxiety may fall short. Tailoring CBPT to directly target persistent physical discomfort could enhance its therapeutic efficacy in such cases. Furthermore, a challenge arises when applying CBPT to families seeking treatment for physical complaints rather than psychological symptoms, perceiving the condition as a medical issue. Therefore, the limited involvement of parents can potentially reinforce the validity of using CBPT in addressing children’s SC. Moreover, children learn to identify physical discomfort, challenge maladaptive thoughts associated with pain using imagery techniques, directly address SC, and dispel misconceptions related to them.
The latest findings validate the effectiveness of CBPT in reducing depression symptoms in children, consistent with existing research [30]. This outcome can be explained by the process in CBPT sessions where children externalize their negative emotions towards their environment and express them directly through play. CBPT focuses on enhancing self-control, fostering a sense of achievement, and cultivating adaptive responses to manage challenging situations. Consequently, CBPT helps prevent a decrease in children’s self-esteem and encourages them to take responsibility for their feelings of sadness. The therapist’s focus is on helping children modify maladaptive thoughts and behaviors. Furthermore, children learn to recognize and effectively manage their negative self-talk. Given that cognitive factors contribute to the persistence of depressive symptoms, CBPT appears to ameliorate depression in children by targeting strategies that correct unhelpful attitudes and thoughts. Additionally, children develop a more realistic self-perception and understanding of the world, enhancing their ability to regulate emotions and behaviors effectively.
Our study has several limitations. First, we did not incorporate a sample of girls, which precludes a comparison of the effectiveness of CBPT based on gender. Second, the absence of a follow-up in the study was due to interference with final exams during the school year. Third, the use of self-report measures to evaluate all variables represented another limitation of the study. Therefore, it is suggested that this study be replicated with girls experiencing internalizing issues concurrently to gather additional evidence supporting the obtained results. Additionally, it is recommended that supplementary methodologies be employed to gather data.
Conclusion
The results indicate that CBPT is a promising intervention for addressing internalizing issues in children. Furthermore, they suggest that professionals can have confidence in the efficacy of CBPT in school environments. Several factors contribute to the effectiveness of CBPT, including the ability to connect behavior and emotions, express feelings verbally in an adaptive way, and engage in positive self-talk. As a result, this intervention may prevent the persistence of psychological symptoms and social communication difficulties in the future. Additionally, the findings suggest that researchers to develop a comprehensive intervention program that considers all factors contributing to the maintenance of internalizing disorders and addresses them effectively.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1393.121). Informed consent was obtained from all mothers of the children included in the study.
Funding
This study was extracted from the project of Masoume Pourmohamadreza-Tajrishiresearch, funded by the Deputy of Research and Technology of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Project No.: 1890).
Authors' contributions
Conceptualization: All authors; Methodology, analysis, and supervision: Masoume Pourmohamadreza-Tajrishi and Bagher Ghobari Bonab; Investigation: Rohollah Mirzaee; Validation and writing: Masoume Pourmohamadreza-Tajrishi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the students and their parents for participating in this study.
References
Behavioral and emotional problems in children refer to conditions in which there is a disparity between children’s behaviors in educational and domestic settings compared to societal norms. These conditions have a detrimental impact on children’s academic performance, social interactions, adaptability, and self-preservation [1]. Achenbach and Rescorla [2] introduced the most renowned classification of these issues, categorizing them into internalizing and externalizing problems. Internalizing problems encompass interpersonal challenges, such as social withdrawal, inhibition, anxiety, depression, and somatic complaints (SC) [2]. Statistics indicate that 17.8% to 34.4% of school-aged children [3], 10% to 20% [4], and 20.3% in Iran [5] suffer from internalizing problems. These problems typically manifest early in childhood [6] and can have enduring negative repercussions if left unresolved, even in adolescence and adulthood [1].
Due to the high prevalence and long-term effects of internalizing disorders in recent years, mental health professionals have been diligently seeking effective strategies and interventions to prevent and ameliorate issues in at-risk children. Various methodologies have been employed to mitigate these problems, with play therapy emerging as a prominent solution. Knell [7] extended the theoretical frameworks of Beck, Ellis, and Bandura by incorporating play techniques to address children’s emotional and behavioral challenges, fostering improved social interactions and problem-solving skills. Efficacious treatments for childhood disorders exist, supported by empirical evidence, with cognitive-behavioral play therapy (CBPT) being a notable intervention for anxiety and depression. CBPT, tailored for young children, integrates theories pertinent to psychopathology, emotional growth, and cognitive development [8]. This approach involves personalized assessments and interventions designed to enhance behavioral competence. Therapists utilize simulated scenarios from child’s life, employing modeling, role-playing, and desensitization techniques to facilitate behavioral modifications. Adapting cognitive therapy to suit child’s developmental stage without complex language is a key challenge faced by CBPT practitioners. As described by Knell [7], therapists can employ accessible tools, such as puppets, stuffed animals, and age-appropriate books, to demonstrate cognitive strategies for problem-solving in children.
Knell [7] conceptualized CBPT with a focus on developmental issues and cognitive and behavioral therapies, emphasizing its empirical validation. Playing offers numerous benefits for children by providing a platform for expressing emotions straightforwardly and effectively and helping them confront unpleasant experiences. Play helps children enhance and fortify their internal resources through verbal and nonverbal communication. Through play therapy, children experience emotional release and gain control over their environment, thereby fostering increased motivation to continue playing while deriving enjoyment from it [1, 9].
A review of the literature demonstrates that several studies have highlighted the effectiveness of play therapy in reducing anxiety, phobias, suicide risk, depression, internalizing problems, and emotional/behavioral disorders [9], while also enhancing self-concept, cognitive abilities, social skills, and self-confidence in children. Another study revealed that play therapy decreased depression, anxiety, and worry in children [10, 11]. Given the various studies in the realm of play therapy and the potential overlooking of covert internalizing issues without necessary follow-up, further research is warranted to explore CBPT as an effective approach for addressing internalizing problems in boys. While parental social support serves as a buffer against internalizing problems in girls, the same protective effect is not observed in boys [12]. As behavioral issues commonly manifest in school-aged children and peak between the ages of 8-15 [13], intervening to curb or prevent behavioral and emotional problems in boys can secure their social well-being. This study aimed to assess the efficacy of CBPT in addressing internalizing problems (and their facets) in 8-10-year-old boys, while also investigating its impact on reducing depression and anxiety levels in this demographic.
Materials and Methods
This study adopted a quasi-experimental design with pre-test and post-test structures. The study sample consisted of 391 boys aged 8-10, selected through cluster sampling during the 2017-18 academic year. Children and their parents who expressed a willingness to participate were requested to complete the questionnaires. Adherence to ethical guidelines, including obtaining informed consent, ensuring confidentiality of participant information, and offering the option to withdraw from the study, was maintained.
Guided by prior research, the sample size was determined using the sample size formula, targeting a test power of 0.90, a test error of 0.05, and accounting for potential sample loss, resulting in the selection of 42 participants. The inclusion criteria included achieving a score of T ≥63 on the children’s behavior checklist, (CBCL) a score of ≥60 on the multidimensional anxiety scale (MASC) for children, a score of ≥18 on the children’s depression inventory (CDI), a diagnosis of internalizing disorders through psychiatric assessment, the absence of sensory impairments or neurodevelopmental disorders, and no concurrent engagement in play therapy sessions. All participants were randomly assigned to the experimental or control group. The experimental group underwent 14 therapeutic sessions involving CBPT once a week for 45 minutes per session, whereas the control group received the standard school program. The data collection tools included the CBCL, MASC for children, and CDI.
CBCL
The CBCL was utilized to assess internalizing problems in children. The CBCL comprises two sections, with this study focusing on the second section, which pertains to symptoms associated with internalizing behaviors. The overall reliability of the CBCL, as indicated by Cronbach’s α, was 0.97. Minaee [14] translated the CBCL into Persian, establishing a cutoff point of T=63 for identifying internalizing disorders. Test, re-test results over a 5 to 8-week interval ranged from 0.32 to 0.67, indicating the instrument’s stability over time. This 113-item checklist is specifically designed for individuals aged 6-18 and can be completed by parents or legal guardians. Internalizing problems are derived from the cumulative scores across three scales: Anxious/depressed (AD), withdrawn/depressed (WD), and SC. In a previous study, the internalizing behaviors scale exhibited a Cronbach’s α of 0.65 [15].
MASC for children
The MASC developed by March [16], is a standardized self-report questionnaire comprising 39 items designed to assess anxiety levels in individuals aged 8-19 years. Principal component analysis revealed four distinct scales within the MASC: social anxiety, separation anxiety, harm avoidance, and physical symptoms, which collectively contribute to the overall measure of anxiety [16]. Anxiety levels are categorized into three tiers based on scores: Mild (zero to 40), moderate (40-60), and high (≥60). The reliability and internal consistency of the MASC in assessing total anxiety yielded values ranging from 0.48-0.79. Factor analysis conducted on the Iranian population confirmed the adequacy of the four-factor model of the MASC, with a reported Cronbach’s α coefficient of 0.77 [17].
CDI
The CDI is a 27-item self-report questionnaire designed to differentiate depression from other disorders. The CDI offers two forms, including the original 27-item version. Each item presents three options, and the child is required to select the option that most accurately reflects their emotions over the preceding two weeks using a 4-point Likert scale.
To assess the various components of depression, the CDI includes five subscales: Anhedonia, ineffectiveness, interpersonal problems, negative mood, and negative self-esteem. The CDI is considered a reliable tool for evaluating depression in children, with a cut-off point typically falling within the range of 19 to 20; individual circumstances should also be considered.
A score of 36 or higher indicates a relatively severe level of depression. The CDI exhibits a Cronbach’s α ranging from 0.71 to 0.89 [18], affirming its internal consistency. Additionally, the instrument’s construct and discriminant validity have been established [19].
CBPT
The CBPT intervention protocol was originally conceptualized by Knell [20] based on cognitive behavioral therapy and tailored for children. The complexity of the CBPT was simplified to align with the child’s developmental stage. Young children are encouraged to understand the connection between their behavior and emotions, enabling them to express their feelings more adaptively and effectively. Through play, the child communicates his needs, and the therapist acknowledges and values these moments of communication.
To establish goals for the child, the therapist engages both the child and the family, guiding the child to achieve these goals and monitoring progress over time. The therapist selects play materials, such as animal puppets and stuffed animals, and engages in activities, such as role-playing, modeling, drawing, and storytelling. Additionally, themes and psychoeducational aspects of the treatment are introduced to assist the child in replacing ineffective methods with positive coping skills. Ultimately, CBPT helps child articulate their conflicts, problems, and their connection to behavior through verbal expression.
The CBPT program consists of 14 sessions, each structured into different stages (introduction and preparation, assessment, intermediate, and final stages) to support children in recognizing their role in changing behaviors. Following preparation, the evaluation phase begins, where the child’s abilities and challenges are assessed, leading to the development of a treatment plan aimed at enhancing self-control, progressive tension, and coping strategies to acquire new beneficial skills. The therapeutic journey concludes with the child and family preparing for the end of the session [21]. The CBPT intervention utilized in the current research is drawn from Knell’s model [20] and tailored for children with anxiety.
After collecting the data, SPSS software, version 21 was used to describe the data (Mean±SD) and to analyze the data, including the multivariate analysis of covariance (MANCOVA) method. Table 1 presents the content of the CBPT intervention for each session.
Results
The mean age of the experimental group was 9.24±0.77, slightly higher than the control group’s average of 9.05±0.87. This data is presented in Table 2, which illustrates the frequency and percentage of total students categorized by education district and educational level. In Table 2, it is evident that out of the selected students, 174(44.5%) were male from education district No. 1, while 217(55.5%) were from education district No. 2. The majority of participants were enrolled in the third grade (35.06%) and second grade (35.46%) within their respective education districts. Among the 391 male students, 53 individuals from the second to fourth grades (16, 18, and 19, respectively) who scored above the cut-off points in the CBCL (≥63), MASC (≥60), and CDI (≥19) were interviewed by a psychiatrist. Subsequently, 42 students diagnosed with internalizing disorders were randomly chosen for further analysis.
Chi-square test analysis indicated no significant difference in age between the experimental and control groups (P=0.909, χ2=0.545). Similarly, no significant difference was observed between the two groups in terms of educational level (grade) (P=0.881, χ2=0.254).
Table 3 presents descriptive indices of internalizing problems (including their dimensions), anxiety, and depression symptoms for two groups in both pre-test and post-test scenarios.
Table 4 presents the descriptive statistics for the indices derived from MASC, CBCL, and CDI in the pre-test and post-test situations. The normality of the variables was assessed using the Kolmogorov-Smirnov (K-S) test, confirming the assumption of MANCOVA (Table 3).
Table 3 reveals that no significant difference is observed between the pre-test and post-test scores in the control group. Furthermore, the scores of the experimental group decreased in the post-test compared to the pre-test. Considering a significance level of P<0.05 for all variables, we concluded that all scores exhibited a normal distribution. The outcomes of Levene’s test indicated that the variances in both groups were homogeneous (Table 4).
Having validated all the assumptions required for MANCOVA, it can be utilized to compare internalizing problems and their dimensions (anxiety/depression, isolation/depression, physical complaints) between the experimental and control groups. Table 5 presents the overall outcomes of the multivariate analysis of variance. To investigate the research hypothesis, which states “CBPT enhances internalizing problems (and its three dimensions), anxiety, and depression symptoms in children,” we employed MANCOVA (Table 5).
Based on the MANCOVA results, the F-statistics were 83.93, 83.93, 95.90, 19.30, 43.33, and 63.96, with P<0.001 for internalizing problems, anxiety/depression, withdrawal/depression, SC, anxiety symptoms, and depression symptoms, respectively, confirming the hypotheses. Consequently, the administration of CBPT to the experimental group led to a significant improvement in internalizing problems (anxiety/depression, withdrawal/depression, and SC), anxiety, and depression symptoms among male students. The effect sizes indicated that 0.40, 0.69, 0.69, and 0.72 of the variations in internalizing problems, anxiety/depression, withdrawal/depression, and SC in students were attributed to their participation in CBPT. Furthermore, a significant difference (P<0.001) was observed in anxiety and depression symptoms between the two groups in the post-test phase. It can be inferred that 0.55 and 0.62 of the changes in anxiety and depression symptoms in the experimental group were influenced by their engagement in CBPT sessions.
Discussion
This study investigated the potential positive impact of CBPT on internalizing problems (specifically anxiety/depression, withdrawal/depression, and SC), as well as anxiety and depression symptoms in boys aged 8–10 years. The results indicated a beneficial effect of CBPT in enhancing internalizing problems (including its various dimensions), anxiety, and depression symptoms. These findings are consistent with those of previous studies [22].
One possible explanation for these findings is that young children, due to their limited flexibility and insufficient cognitive skills in the preoperational stage of development, may struggle to follow rational sequences and differentiate between logical and illogical thinking. During this stage, children tend to think egocentrically, concretely, and irrationally, often acting impulsively or without adequate cognitive maturity [20]. Consequently, they may act before thinking things through. However, it is feasible for young children to learn to associate their behaviors with their emotions and express their feelings in more adaptive ways. This capability enables them to develop a sense of control and receive positive reinforcement from their environment. Play serves as a natural avenue through which children can communicate [23]. Numerous evidence-based studies have supported the positive effects [20] and long-term benefits [24] of CBPT on behavioral problems.
This finding is consistent with that of a previous research [9]. This can be explained by the fact that internalizing problems, anxiety, and depression symptoms can exacerbate aggressive and rule-breaking behaviors [24]. Ensuring the child’s continuous engagement is crucial, as CBPT should offer an engaging platform that allows children to fully experience therapy. The level of engagement between children and CBPT plays a pivotal role in the success of a child’s therapy. Factors to concentrate on to enhance continuous engagement [25] include motivation, relaxation, attention, the child’s willingness to repeat, ease of learning, and problem-solving capabilities throughout CBPT sessions. Moreover, low parental involvement has been positively correlated with improvements in internalizing problems, anxiety, and depression symptoms in children. This finding suggests that when parents are less involved in treatment, children may express anxious and arousing behaviors more freely while the therapist provides guidance. Conversely, high parental involvement may trigger previous patterns of child-parent interaction, making it difficult to test new behaviors beneficial for reducing internalizing problems or anxiety and depression symptoms in children. Previous studies have yielded varied results regarding the role of parental involvement in CBPT [8].
The second finding supports the effectiveness of CBPT in improving anxiety symptoms, consistent with previous research [26]. One possible explanation is that the child actively engages in mastering and addressing issues. During CBPT sessions, child may intentionally place themselves in stressful scenarios and communicate their needs through role-playing exercises. Through these interactions, child can enhance their communication skills and develop a close rapport with the therapist. This process allows the child to recall and reinterpret significant themes and events from their life, leading to increased awareness and the ability to approach conflicts more adaptively [27, 28]. Moreover, acquiring strategies to regulate negative emotions enables children to acknowledge and embrace their feelings. The therapist’s emphasis on confronting negative self-talk and instructing children to replace maladaptive thoughts with more positive self-talk helps alleviate their concerns and foster emotional well-being.
The third finding validates the effectiveness of CBPT in addressing SC in children, consistent with previous research [29]. This finding can be explained by the high prevalence of SC among many children in our sample, leading to prolonged school absences and disruptions to daily activities. The study participants often sought medical consultation, underwent expensive diagnostic procedures, and relied on medication. A significant proportion of the sample exhibited psychosomatic symptoms or widespread pain linked to anxiety-provoking situations. Consequently, conventional intervention approaches that view SC as expressions of anxiety may fall short. Tailoring CBPT to directly target persistent physical discomfort could enhance its therapeutic efficacy in such cases. Furthermore, a challenge arises when applying CBPT to families seeking treatment for physical complaints rather than psychological symptoms, perceiving the condition as a medical issue. Therefore, the limited involvement of parents can potentially reinforce the validity of using CBPT in addressing children’s SC. Moreover, children learn to identify physical discomfort, challenge maladaptive thoughts associated with pain using imagery techniques, directly address SC, and dispel misconceptions related to them.
The latest findings validate the effectiveness of CBPT in reducing depression symptoms in children, consistent with existing research [30]. This outcome can be explained by the process in CBPT sessions where children externalize their negative emotions towards their environment and express them directly through play. CBPT focuses on enhancing self-control, fostering a sense of achievement, and cultivating adaptive responses to manage challenging situations. Consequently, CBPT helps prevent a decrease in children’s self-esteem and encourages them to take responsibility for their feelings of sadness. The therapist’s focus is on helping children modify maladaptive thoughts and behaviors. Furthermore, children learn to recognize and effectively manage their negative self-talk. Given that cognitive factors contribute to the persistence of depressive symptoms, CBPT appears to ameliorate depression in children by targeting strategies that correct unhelpful attitudes and thoughts. Additionally, children develop a more realistic self-perception and understanding of the world, enhancing their ability to regulate emotions and behaviors effectively.
Our study has several limitations. First, we did not incorporate a sample of girls, which precludes a comparison of the effectiveness of CBPT based on gender. Second, the absence of a follow-up in the study was due to interference with final exams during the school year. Third, the use of self-report measures to evaluate all variables represented another limitation of the study. Therefore, it is suggested that this study be replicated with girls experiencing internalizing issues concurrently to gather additional evidence supporting the obtained results. Additionally, it is recommended that supplementary methodologies be employed to gather data.
Conclusion
The results indicate that CBPT is a promising intervention for addressing internalizing issues in children. Furthermore, they suggest that professionals can have confidence in the efficacy of CBPT in school environments. Several factors contribute to the effectiveness of CBPT, including the ability to connect behavior and emotions, express feelings verbally in an adaptive way, and engage in positive self-talk. As a result, this intervention may prevent the persistence of psychological symptoms and social communication difficulties in the future. Additionally, the findings suggest that researchers to develop a comprehensive intervention program that considers all factors contributing to the maintenance of internalizing disorders and addresses them effectively.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1393.121). Informed consent was obtained from all mothers of the children included in the study.
Funding
This study was extracted from the project of Masoume Pourmohamadreza-Tajrishiresearch, funded by the Deputy of Research and Technology of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Project No.: 1890).
Authors' contributions
Conceptualization: All authors; Methodology, analysis, and supervision: Masoume Pourmohamadreza-Tajrishi and Bagher Ghobari Bonab; Investigation: Rohollah Mirzaee; Validation and writing: Masoume Pourmohamadreza-Tajrishi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the students and their parents for participating in this study.
References
- Kertz SJ, Petersen DR, Stevens KT. Cognitive and attentional vulnerability to depression in youth: A review. Clinical Psychology Review. 2019; 71:63-77. [DOI:10.1016/j.cpr.2019.01.004]
- Achenbach TM, Rescorla LA. Child behavior checklist for ages 6-18 (CBCL/6-18, ASEBA CBCL/6-18). 2001. [DOI:10.1037/t47452-000]
- Danielson ML, Bitsko RH, Holbrook JR, Charania SN, Claussen AH, McKeown RE, et al. Community-based prevalence of externalizing and internalizing disorders among school-aged children and adolescents in four geographically dispersed school districts in the United States. Child Psychiatry and Human Development. 2021; 52(3):500-14. [DOI:10.1007/s10578-020-01027-z] [PMID]
- Eaton NR, Krueger RF, Markon KE, Keyes KM, Skodol AE, Wall M, et al. The structure and predictive validity of the internalizing disorders. Journal of Abnormal Psychology. 2013; 122(1):86-92. [DOI:10.1037/a0029598]
- Ghobari-Bonab B, Parand A, Hossein Khanzadeh Firoozjah A, Movallali G, Nemati S. [Prevalence of children with behavioral disorders in primary schools in Tehran (Persian)]. Journal of Exceptional Children. 2009; 9(3):223-38. [Link]
- Perle JG, Levine AB, Odland AP, Ketterer JL, Cannon MA, Marker CD. The association between internalizing symptomology and risky behaviors. Journal of Child & Adolescent Substance Abuse. 2013; 22(1):1-24. [DOI:10.1080/1067828X.2012.724289]
- Knell SM. Cognitive-behavioral play therapy. Journal of Clinical Child Psychology. 1998; 27(1):28-33. [DOI:10.1207/s15374424jccp2701_3] [PMID]
- Dorsey S, McLaughlin KA, Kerns SEU, Harrison JP, Lambert HK, Briggs EC, et al. Evidence base update for psychosocial treatments for children and adolescents exposed to traumatic events. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53. 2017; 46(3):303-30. [DOI:10.1080/15374416.2016.1220309] [PMID]
- Seifi H, Tabrizi M, Asadzade H. Teaching cognitive behavioral techniques on attachment styles, mental health, and optimism in medical students at Islamic Azad University, Mashhad Branch, Iran. Journal of Practice in Clinical Psychology. 2024;12(2):189-200. [Link]
- Jafarzade M, Mohammadpanah Ardakan A, Rezapour Mir Saleh Y. The effectiveness of play therapy combined with a trauma-focused cognitive behavioral therapy on trauma symptoms and the loneliness feeling. Journal of Practice in Clinical Psychology. 2023; 11(3):211-22. [DOI:10.32598/jpcp.11.3.614.2]
- Poursadoughi A, Dadkhah A, Pourmohamadreza-Tajrishi M, Biglarian A. Psycho-Rehabilitation Method (Dohsa-Hou) and Quality of Life in Children with Cerebral Palsy. Iranian-Rehabilitation-Journal. 2015; 13(2):28-33. [Link]
- Lyell KM, Coyle S, Malecki CK, Santuzzi AM. Parent and peer social support compensation and internalizing problems in adolescence. Journal of School Psychology. 2020; 83:25-49. [DOI:10.1016/j.jsp.2020.08.003] [PMID]
- Kakabraee K, Emami Ale Agha S. [Effectiveness of problem solving training on behavioral problems of preschool children with behavioral disorder (Persian)]. Empowering Exceptional Children. 2018; 9(1):51-64. [DOI:10.22034/ceciranj.2018.68957]
- Minaee A. [Adaptation and standardization of child behavior checklist, youth self-report, and teacher’s report forms (Persian)]. Journal of Exceptional Children. 2006; 6(1):529-58. [Link]
- Ahadi B. [Comparison of behavior problems and school achievement between children with and without motor problems (Persian)]. Archives of Rehabilitation. 2009; 10(1):32-6. [Link]
- March JS, Parker JD, Sullivan K, Stallings P, Conners CK. The multidimensional anxiety scale for children (MASC): Factor structure, reliability, and validity. Journal of the American Academy of Child and Adolescent Psychiatry. 1997; 36(4):554-65. [DOI:10.1097/00004583-199704000-00019] [PMID]
- Mashhadi A, Soltani Shal R, Mirdoraghi F, Bahrami B. [Psychometric properties of the multidimensional anxiety scale for Iranian children (Persian)]. Applied Psychology. 2012; 6(1):70-8. [Link]
- Kovacs M. The Children's Depression, Inventory (CDI). Psychopharmacology Bulletin. 1985; 21(4):995-8. [PMID]
- Hodges K. Depression and anxiety in children: A comparison of self-report questionnaires to clinical interview. Psychological Assessment: A Journal of Consulting and Clinical Psychology. 1990; 2(4):376. [DOI:10.1037/1040-3590.2.4.376]
- Knell SM. Cognitive-Behavioral Play Therapy. In: O'Connor KJ, Schaefer CE, Braverman LD, editors. Handbook of play therapy. New Jersey: John Wiley & Sons; 2015. [Link]
- Gallagher HM, Rabian BA, McCloskey MS. A brief group cognitive-behavioral intervention for social phobia in childhood. Journal of Anxiety Disorders. 2004; 18(4):459-79. [DOI:10.1016/S0887-6185(03)00027-6]
- Hossein Khanzadeh AA, Imankhah F. The effect of music therapy along with play therapy on social behaviors and stereotyped behaviors of children with Autism. Practice in Clinical Psychology. 2017; 5(4):251-62. [DOI:10.29252/nirp.jpcp.5.4.251]
- Senko K, Bethany H. Play Therapy: An illustrative case. Innovations in Clinical Neuroscience. 2019; 16(5-6):38-40. [PMID]
- Daryabeigi M, Pourmohamdreza-Tajrishi M, Dolatshahi B, Bakhshi E. The effectiveness of cognitive-behavioral therapy on internalizing problems of children with externalizing disorders. Iranian Rehabilitation Journal. 2020; 18(2):193-202. [DOI:10.32598/irj.18.2.948.1]
- Drus ZAM, Singh D, Mokhtar MR, Abd Rashid R. Critical Review on Factors That Influence Continuous Engagement Towards CCBT. Pertanika Journal of Scholarly Research Reviews. 2018; 4(2):36-42. [Link]
- Baggerly J. The effects of child-centered group play therapy on self-concept, depression, and anxiety of children who are homeless. International Journal of Play Therapy. 2004; 13(2):31-51. [DOI:10.1037/h0088889]
- Grant RJ, Stone J, Mellenthin C. Do you have a primary play therapy theory or approach you use the most and why? In: Grant RJ, Stone J, Mellenthin C, editors. Play therapy theories and perspectives. New York: Routledge; 2020.[DOI:10.4324/9780367816452-3]
- Kaduson HG, Schaefer CE. Play therapy with children: Modalities for Change. Washington, D.C: American Psychological Association; 2021. [DOI:10.1037/0000217-000]
- Schottelkorb A, Swan K, Jahn L, Haas S, Hacker J. Effectiveness of play therapy on problematic behaviors of preschool children with somatization. Journal of Child and Adolescent Counseling. 2015; 1(1):3-16. [DOI:10.1080/23727810.2015.1015905]
- Chatoor I, Webb LE, Kerzner B. Anorexia nervosa and depression in a 5-year-old girl: Treatment with focused family play therapy and medication. The International Journal of Eating Disorders. 2019; 52(9):1065-9. [DOI:10.1002/eat.23129] [PMID]
Article type: Original Research Articles |
Subject:
Psychology
Received: 2024/07/16 | Accepted: 2024/12/31 | Published: 2025/09/1
Received: 2024/07/16 | Accepted: 2024/12/31 | Published: 2025/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
