
988368
Thu, Jul 30, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 375-388 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Masoudi Poorgholam L, Moghadas Tabrizi Y, Latifi S. The Effect of Body Balance on Working Memory, Muscle Spasms, and Fatigue in Multiple Sclerosis. Iranian Rehabilitation Journal 2025; 23 (4) :375-388
URL: http://irj.uswr.ac.ir/article-1-2488-en.html
URL: http://irj.uswr.ac.ir/article-1-2488-en.html



1- Iranian Research Center on Aging, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Sport Injuries and Biomechanics, Faculty of Sport Sciences and Health, University of Tehran, Tehran, Iran.
2- Department of Sport Injuries and Biomechanics, Faculty of Sport Sciences and Health, University of Tehran, Tehran, Iran.
Keywords: Multiple sclerosis (MS), Cognitive function, Balance training, N-back task, Fatigue severity, Muscle spasticity
Full-Text [PDF 592 kb]
(531 Downloads)
| Abstract (HTML) (2302 Views)
Full-Text: (300 Views)
Introduction
Multiple sclerosis (MS) is a chronic and complex disease of the central nervous system characterized by the degradation of the myelin sheath and neurons, resulting in widespread effects on affected individuals’ physical and cognitive functioning [1]. Individuals with MS face numerous challenges that impair their abilities across all dimensions of life [2]. A primary difficulty associated with this condition is the occurrence of symptom exacerbations, which manifest in 85-90% of cases and, due to their unpredictable nature, complicate disease management [3, 4]. Among the most prominent issues affecting the MS community are memory impairments, muscle spasm, and fatigue [5]. Approximately 60% of MS patients experience memory deficits, particularly impacting working memory and remote conscious memory [6]. These deficits are most evident in short-term memory, with patients struggling to recall details of recent conversations or events. However, their ability to remember distant past events typically remains intact [7]. Neuroimaging studies have shown that MS alters brain activation patterns associated with working memory. Patients often recruit additional or compensatory brain regions, such as prefrontal or parietal areas, to offset working memory impairments [8]. Fatigue, another prevalent and debilitating symptom of MS, is reported in 65% to 85% of patients and is defined as a pervasive sense of energy depletion [9, 10]. This condition, rooted in both physiological and psychological factors [11], is often exacerbated by sleep disturbances, depression, and medication side effects [12]. Additionally, muscle spasms, affecting at least 65 percent of MS patients, arise from damage to upper motor neurons and abnormal spinal reflex activity [13]. This condition is characterized by increased muscle tone, excessive stimulation, weakness, pain, and involuntary movements (spasms), which may progress to muscle contractures in severe cases [14]. While the body balance training in this study demonstrated promising improvements in working memory, muscle spasticity, and fatigue, it is important to note that the effectiveness of this intervention may vary depending on individual patient factors, such as disease severity, age, and response to exercise. While promising, this intervention is not a “quick fix” and should be considered part of a comprehensive, long-term therapeutic strategy. Previous research has suggested positive outcomes for exercise interventions in MS; however, the speed and extent of improvements can differ from patient to patient [15].
According to recent epidemiological studies, the number of individuals affected by MS has risen from 2.3 million in 2013 to 2.9 million in 2023, reflecting the increasing global burden of the disease [16]. In Iran, the annual incidence rate averages 6.5 per 100000 people, with some regions reporting rates as high as 12.8 per 100000 [17]. These alarming statistics, combined with limited accessibility to advanced pharmacological treatments, underscore the urgent need for affordable, non-pharmacological interventions. Recent research has increasingly focused on the potential of physical activity and exercise to manage MS symptoms [18]. Historically, physicians have advised patients with MS to avoid physical exertion, fearing potential exacerbation of symptoms. However,`suggests that, with appropriate guidance, exercise can serve as an effective non-pharmacological intervention. It can enhance aerobic capacity, muscle strength, flexibility, and balance and also plays a crucial role in managing fatigue levels, cognitive function, and memory [19-21]. In light of this growing body of evidence, exploring the specific effects of different exercise modalities on MS symptom progression is increasingly crucial, as regular physical activity has been shown to improve cardiopulmonary fitness, muscular strength and endurance, alleviate systemic fatigue, and positively influence mood and cognitive performance [22].
Suitable exercise options for patients with MS are yoga, Pilates, and Tai Chi [23]. Numerous studies have reported positive outcomes from these activities in addressing challenges faced by older adults and individuals with specific conditions, such as Parkinson’s disease and MS. For instance, research has shown that in women with MS receiving standard immunomodulatory treatments, yoga and hydrotherapy [24], without endurance or coordination exercises [25], produce comparable benefits in reducing fatigue, depression, and paresthesia. Similarly, Ozkul et al. (2020) identified beneficial effects of combining aerobic exercise and Pilates in patients with MS and cognitive impairment, noting positive correlations with improvements in cognition, mood, and quality of life (QoL) post-exercise [26]. Body balance training has emerged as a promising hybrid approach among these exercise interventions. Body balance is a gym-based holistic workout that includes both traditional methods, such as yoga and Tai Chi, and more recently developed methods, such as Pilates. A reasonable assumption is that body balance would also have similar benefits as its elements (yoga, Tai Chi, and pilates), such as improvement of balance, flexibility, mobility, posture, anxiety, and muscle strength [27, 28]. In this study, body balance training consisted of structured sessions incorporating a standardized sequence of yoga poses, Tai Chi movements, and Pilates-based exercises, focusing on core stability, flexibility, controlled breathing, and postural alignment, conducted three times a week over eight weeks. It is reasonable to assume that body balance offers benefits similar to its elements, such as improvements in balance, flexibility, mobility, posture, anxiety, and muscle strength [29].
Drawing from controlled, purposeful movements inspired by yoga, Tai Chi, and Pilates [29], these exercises emphasize balance, coordination, and physical strength, potentially mitigating mobility and impairments from MS-related neurological damage [30, 31]. Preliminary findings suggest that consistent engagement in body balance exercises reduces the frequency and severity of muscle spasms, alleviates severe fatigue and enhances patients’ capacity to perform daily tasks [32, 33]. Moreover, given the established link between physical activity and cognitive function, body balance training may positively influence working memory, although this aspect remains underexplored in the MS population. Despite the established benefits of yoga, Tai Chi, and Pilates, limited research has specifically examined the combined effects of body balance training on cognitive outcomes, particularly working memory, alongside physical symptoms in patients with MS. This study aimed to address this gap by evaluating the impact of body balance training on working memory, muscle spasms, and fatigue. Requiring minimal equipment and adaptable to various settings, these exercises offer a cost-effective and practical rehabilitation option.
Given the limitations of pharmacological treatments and the need for complementary approaches, this study aims to evaluate the effects of body balance training on three key domains in MS patients: Working memory, muscle spasticity, and fatigue. These domains were selected because they represent some of the most debilitating and commonly reported symptoms in individuals with MS, significantly impacting daily functioning and QoL. Moreover, previous research has indicated that exercise modalities incorporated into body balance, such as yoga, Tai Chi, and Pilates, can individually contribute to improvements in cognitive performance, reductions in spasticity, and alleviation of fatigue. Therefore, it is reasonable to hypothesize that an integrated body balance program may exert beneficial effects across these interrelated outcomes, ultimately improving QoL and overall health. Grounded in existing scientific frameworks and responsive to patients’ practical needs, this research aims to determine whether body balance training, as a non-pharmacological therapeutic strategy, can mitigate the debilitating symptoms of MS and improve the physical and cognitive capacities of affected individuals. We hypothesized that body balance training would lead to significant improvements in working memory, reductions in muscle spasticity, and decreases in fatigue compared to standard care.
Materials and Methods
This study utilized a single-blind, randomized controlled trial with a pre-test-post-test design, featuring an active intervention group and a control group. In this design, outcome assessors were blinded to group assignments to minimize assessment bias. Initially, 30 female participants diagnosed with relapsing-remitting MS (RRMS) (mean age=33.38±4.99 years) were recruited from the MS community in Karaj City, Iran, after obtaining informed consent. Participants were randomly allocated to either the intervention group (n=15) or the control group (n=15) using a computer-generated randomization sequence with allocation concealment ensured through sealed, opaque envelopes handled by an independent researcher. During the study, four participants dropped out, two from each group, due to relocation, engagement in alternative exercise programs, or loss of contact, resulting in a final sample of 26 participants (13 per group). No significant differences in dropout rates were observed between the experimental and control groups, and the reasons for dropout were consistent across both groups. Therefore, the dropout pattern is unlikely to influence the study’s overall results. Only data from participants who completed the study were included in the final analysis; no intention-to-treat approach was applied. The inclusion criteria included female patients aged 25–40 years. While the 15-year age range may introduce variability, this range was selected to capture a broad representation of adult women with RRMS, avoiding extreme age-related differences that could confound results. Additionally, potential age-related differences were considered and controlled for in the statistical analysis, ensuring that the effects observed are not significantly influenced by age. More inclusion criteria include a confirmed diagnosis of RRMS by a neurologist. Expanded disability status scale (EDSS) score below 4 (indicating mild to moderate disability) [34], no participation in body balance training for at least two months prior to the study, no engagement in other physical activities during the study period, no concurrent psychiatric, psychotherapeutic, or cognitive rehabilitation interventions, no diagnosis of additional neuromuscular disorders, no use of medications affecting muscle spasticity or fatigue, no participation in alternative treatment modalities during the study, no disease relapse within two months prior to study enrollment.
Written informed consent was obtained from all participants prior to the study. Demographic and clinical information, including age, disease duration, and medication history, was collected at baseline. The study protocol was approved by the Ethics Committee of the University of Tehran.
Assessment tools
Three primary outcome measures were evaluated: Working memory, muscle spasticity, and fatigue. All assessments, including the N-back, MS spasticity scale (MSSS-88), and fatigue severity scale (FSS), were administered under the supervision of trained researchers in a quiet research setting. The testing sessions took place between 9 AM and 12 PM to minimize potential variations in cognitive and fatigue responses due to time of day. A standardized protocol was followed to ensure consistency across all participants, and the environment was free of distractions to provide optimal testing conditions. Although the primary aim of the study was to assess cognitive and fatigue outcomes, future studies should incorporate motor tests, such as balance assessments, to evaluate the physical aspects of balance interventions in patients with MS. Given the nature of the body balance program, which integrates elements of yoga, Tai Chi, and Pilates, balance-related tests (e.g. Berg balance scale or timed up and go test) could provide essential data regarding the physical improvements resulting from the intervention, and thus should be part of the assessment protocol in future research.
Working memory assessment: N-back test
The N-Back test evaluates executive functions, with a particular focus on working memory. It requires participants to retain and manipulate information during task performance [35]. It has demonstrated high reliability, with validity coefficients ranging from 0.54 to 0.84 in previous studies [36]. The N-back test is considered a robust measure of working memory performance. Participants responded to a series of visual stimuli on a computer screen by pressing designated keys to indicate whether the current stimulus matched one presented n steps earlier in the sequence. The test consists of three levels: 1-back (matching the immediate prior stimulus), 2-back (matching the stimulus two steps back), and 3-back (matching the stimulus three steps back). A practice phase preceded the main test to ensure comprehension. The test lasted approximately 10 minutes, and the outcomes were measured in terms of accuracy (correct responses), reaction time for correct responses, incorrect responses, and unanswered items. For this study, accuracy (correct responses) was the primary outcome measure for working memory performance, with reaction time considered a secondary metric.
Muscle spasticity assessment: MSSS-88
Muscle spasticity was assessed using the MSSS-88, a patient-centered questionnaire comprising 88 items scored from 1 (no discomfort) to 4 (maximum discomfort), evaluating spasticity across eight distinct subscales [37, 38]. In this study, following a preliminary needs assessment and based on clinical recommendations from the physical activity guide for MS by Azad (2022), five subscales—muscle stiffness, pain and discomfort, muscle spasms, activities of daily living, and walking—were selected for analysis [39]. These subscales were prioritized because they most directly reflect the physical and functional impairments targeted by body balance training, particularly regarding mobility and daily function, which were central goals of the intervention. The MSSS-88 has demonstrated strong psychometric properties, with its validity and reliability confirmed in German [40], Serbian [41], and Persian [42] versions. It is important to note that if the guideline cited by Azad is unpublished, the recommendations are considered expert opinions based on clinical practice in the context of MS rehabilitation in Iran.
Fatigue assessment: FSS
Fatigue was assessed using the FSS, a 9-item self-report questionnaire developed by Krupp et al. in 1989 to measure the severity of fatigue symptoms in clinical populations, particularly in individuals with multiple sclerosis [43]. Each item is rated on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating greater severity of fatigue. The final score is calculated by averaging the responses across all nine items, with scores above four typically indicative of clinically significant fatigue. The FSS has demonstrated strong psychometric properties in MS populations, with reported validity of 0.78 and reliability of 0.93 [44]. This tool offers a simple, efficient, and reliable method for comprehensively assessing the impact of fatigue on daily functioning in MS patients.
Body balance training protocol
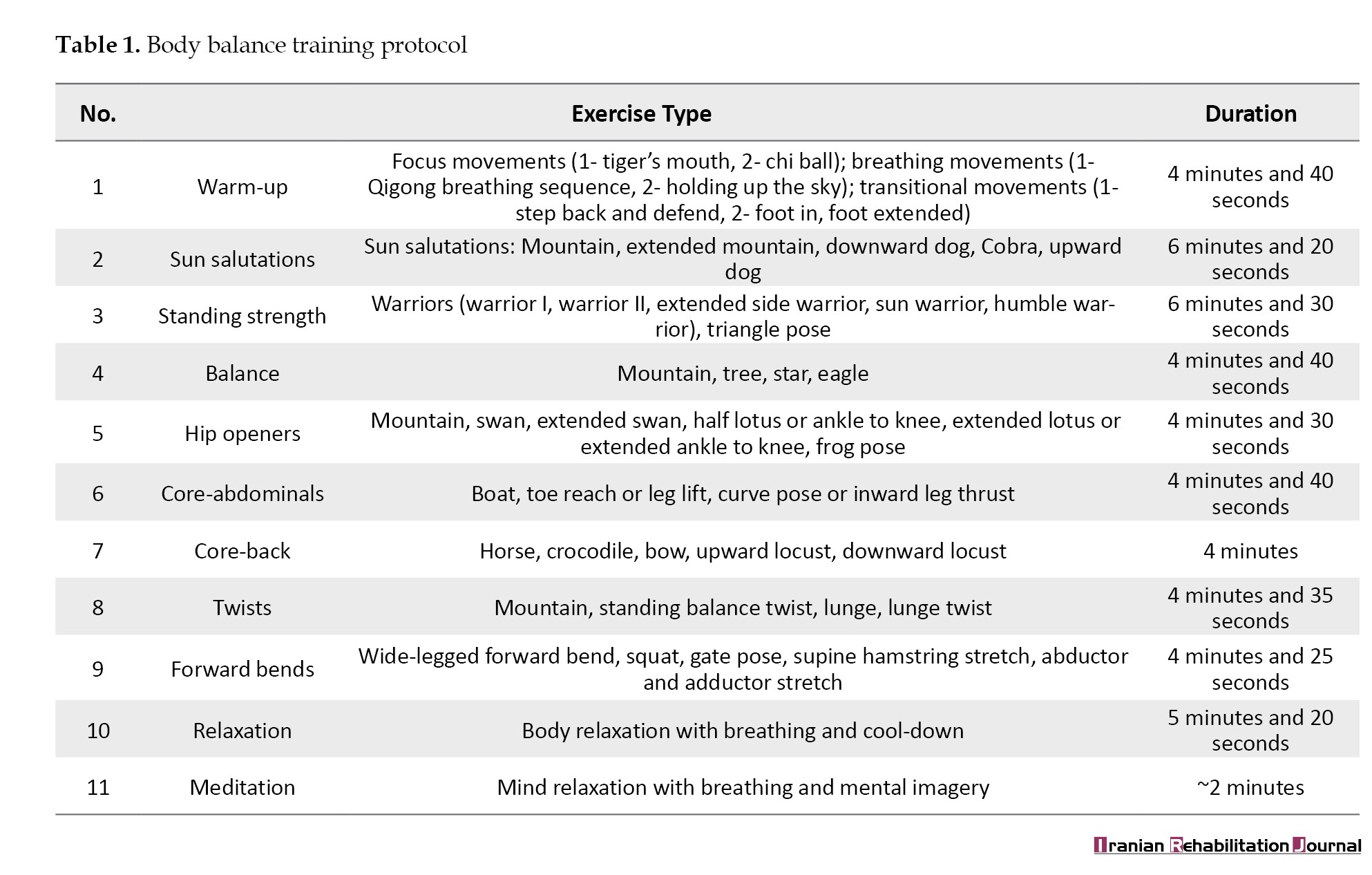
The body balance training protocol implemented in this study was adapted from a program by Khan et al. (2008), as referenced in the operational definition of body balance [28]. This protocol was selected because it combines elements of yoga, Tai Chi, and Pilates, specifically structured to improve balance, flexibility, and neuromuscular control, which are commonly impaired in patients with multiple sclerosis. Additionally, the exercises emphasized low-impact, controlled movements, making them particularly suitable for individuals with mild to moderate MS-related disability. The 8-week body balance training program consisted of 24 sessions, with participants attending three 60-minute sessions per week. Each session was organized into distinct phases: Warm-up, strength and core stability training, balance and flexibility exercises, and relaxation. The exercise protocol was progressively individualized throughout the intervention period in response to each participant’s performance capacity and tolerance levels. To promote gradual progression while minimizing the risk of injury, tailored modifications were implemented, including adjustments, such as limiting the range of motion, altering the base of support, or incorporating low-level challenges (e.g. performing balance exercises with eyes closed). Table 1 presents a detailed summary of the training components.
In this protocol, modifications were made for patients with MS, taking into account their physical limitations and ensuring their safety. For example, balance poses were performed with support (using a chair or wall) when necessary, and the intensity of strength exercises was adjusted to the individual’s capacity. Additionally, the protocol was designed to be flexible, allowing gradual progression of exercises as participants gained strength and stability over the 8-week period. For future adaptations, the original 12-week protocol was condensed to 8 weeks, reducing the overall volume of each session and focusing on key exercises that could be easily modified to accommodate the specific needs of patients with MS. Weekly progression was carefully monitored to ensure participants’ safety and maximize benefit. The control groJdard care, which included adherence to prescribed disease-modifying therapies, routine follow-up visits with neurologists, and general health advice regarding nutrition, sleep hygiene, and stress management. No additional structured physical activity or exercise interventions were introduced during the study period. Both groups continued their regular MS medications as prescribed.
Procedure
Baseline assessments were conducted one week prior to the start of the intervention at the Rehabilitation Research Laboratory, University of Tehran. These assessments included working memory (via the N-back test), muscle spasticity (via selected MSSS-88 subscales), and fatigue (via the FSS questionnaire). All assessments were conducted by trained evaluators with experience in neuropsychological testing in MS populations. Following baseline evaluations, participants were randomly assigned to either the intervention or control group. The intervention group participated in an 8-week body balance training program, held three times per week at a standardized local sports facility equipped with accessible flooring, temperature control (21-23 °C), and MS-friendly infrastructure. Each 60-minute session was structured into distinct phases: Warm-up, strength, balance, flexibility, core strengthening, and relaxation, with progressive adaptations based on participant feedback and performance. The program was supervised by a certified physiotherapist with specialization in neurorehabilitation and at least five years of experience working with MS patients. Exercises were drawn from yoga, Tai Chi, and Pilates, and were tailored to individual physical limitations using support tools (e.g. chairs, walls) when necessary. Participants who demonstrated ≥80% success in task completion or self-reported comfort were advanced to slightly more challenging versions of the same exercises. The control group received standard care, which consisted of adherence to prescribed MS medications, neurologist follow-ups every 8–12 weeks, and general lifestyle guidance. No structured exercise or physiotherapy programs were included in the standard care. All participants completed the post-test immediately after the intervention, using the same measures and blinded procedures as in the pre-test. Adverse events were monitored using session checklists and weekly self-reports. No serious adverse events occurred. No follow-up assessments were planned beyond the immediate post-intervention phase; however, future research is recommended to explore long-term effects. Statistical analysis was conducted using SPSS software, version 27, employing paired t-tests for within-group comparisons and analysis of covariance (ANCOVA) for between-group comparisons, adjusting for baseline scores. A significance level of P<0.05 was used.
Results
Table 2 presents a descriptive summary of the participants’ demographic characteristics. This table provides an overview of key variables for the intervention (body balance training) and control groups, including age, height, weight, body mass index (BMI), disease duration, and EDSS scores. All participants were patients with the relapsing-remitting subtype of MS, receiving routine MS pharmacotherapy and performing usual daily activities (without regular physical activity).
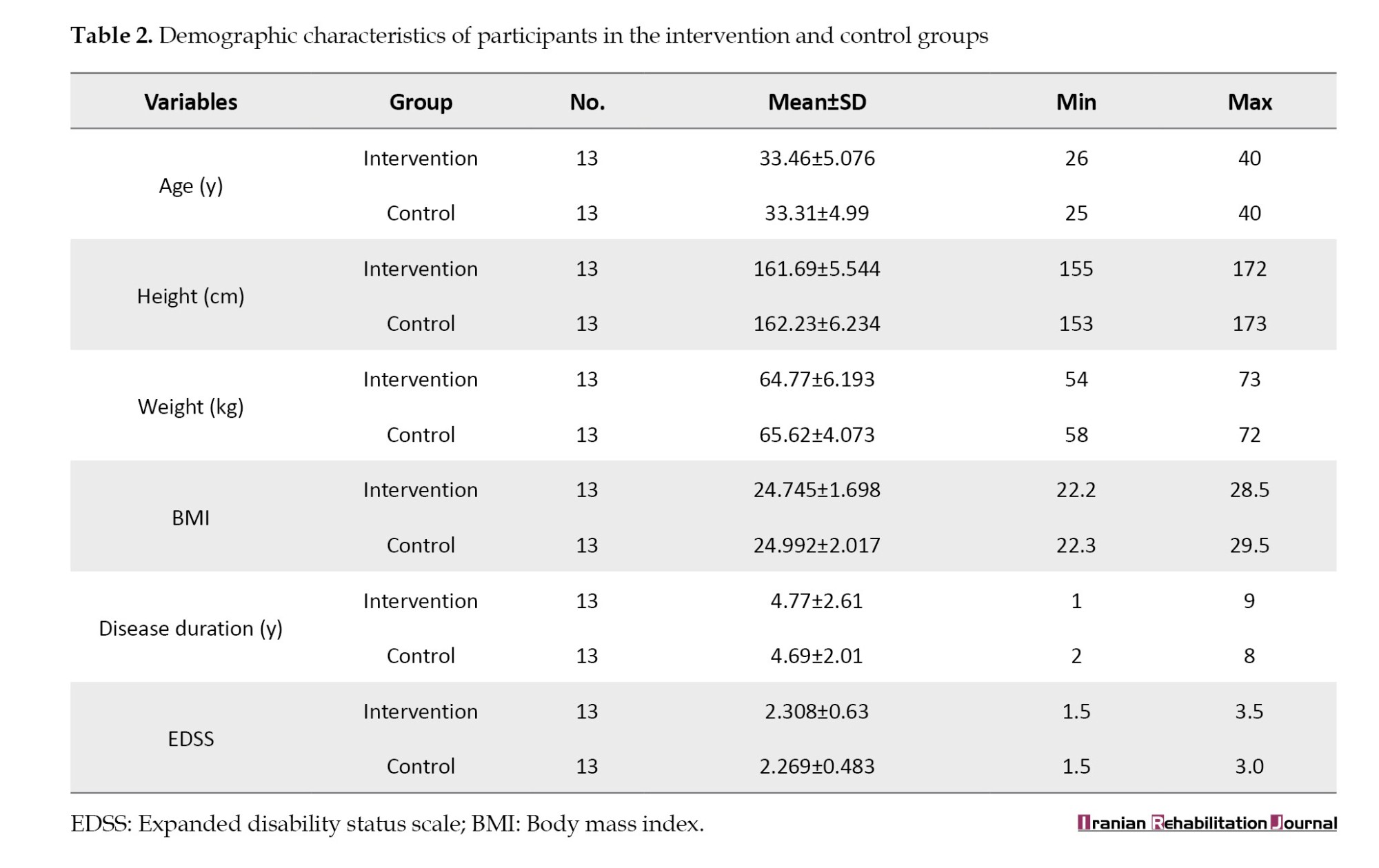
As shown in Table 2, the mean values of demographic variables were closely aligned between the intervention and control groups, indicating a high degree of similarity. Statistical comparisons of these demographic characteristics revealed no significant differences between the two groups, confirming that the intervention and control groups were comparable at baseline.
Before conducting the statistical analyses, assumptions required for parametric testing were evaluated. The Shapiro-Wilk test confirmed that all variables exhibited normal distribution (P>0.05). Homogeneity of variances was assessed using Levene’s test, confirming equality of error variances across groups (P>0.05). For ANCOVA, the assumption of homogeneity of regression slopes was tested and met, indicating that the relationship between pre-test scores and post-test outcomes was consistent across groups. Subsequently, paired t-tests were employed to assess within-group changes between pre- and post-intervention scores for the intervention (body balance training) and control groups. Cohen’s d effect sizes were also calculated to determine the magnitude of change within each group. Table 3 presents the results of paired t-tests analyzing the effects of body balance training on working memory, muscle spasticity, and fatigue. For the N-back test assessing working memory, three levels of task difficulty were examined: Level 1 (1-back: Comparison with the immediately preceding stimulus), level 2 (2-back: Comparison with the stimulus two steps earlier), and level 3 (3-back: Comparison with the stimulus three steps earlier). Outcomes included the number of correct responses and mean response time for correct responses at each level. Significant improvements were observed in the intervention group across all levels, both in increasing correct responses and decreasing response times, whereas the control group showed no significant changes. Similarly, for muscle spasticity (measured via selected subscales of the MSSS-88) and fatigue (measured via FSS), the intervention group demonstrated significant reductions post-intervention, while the control group exhibited no meaningful changes.
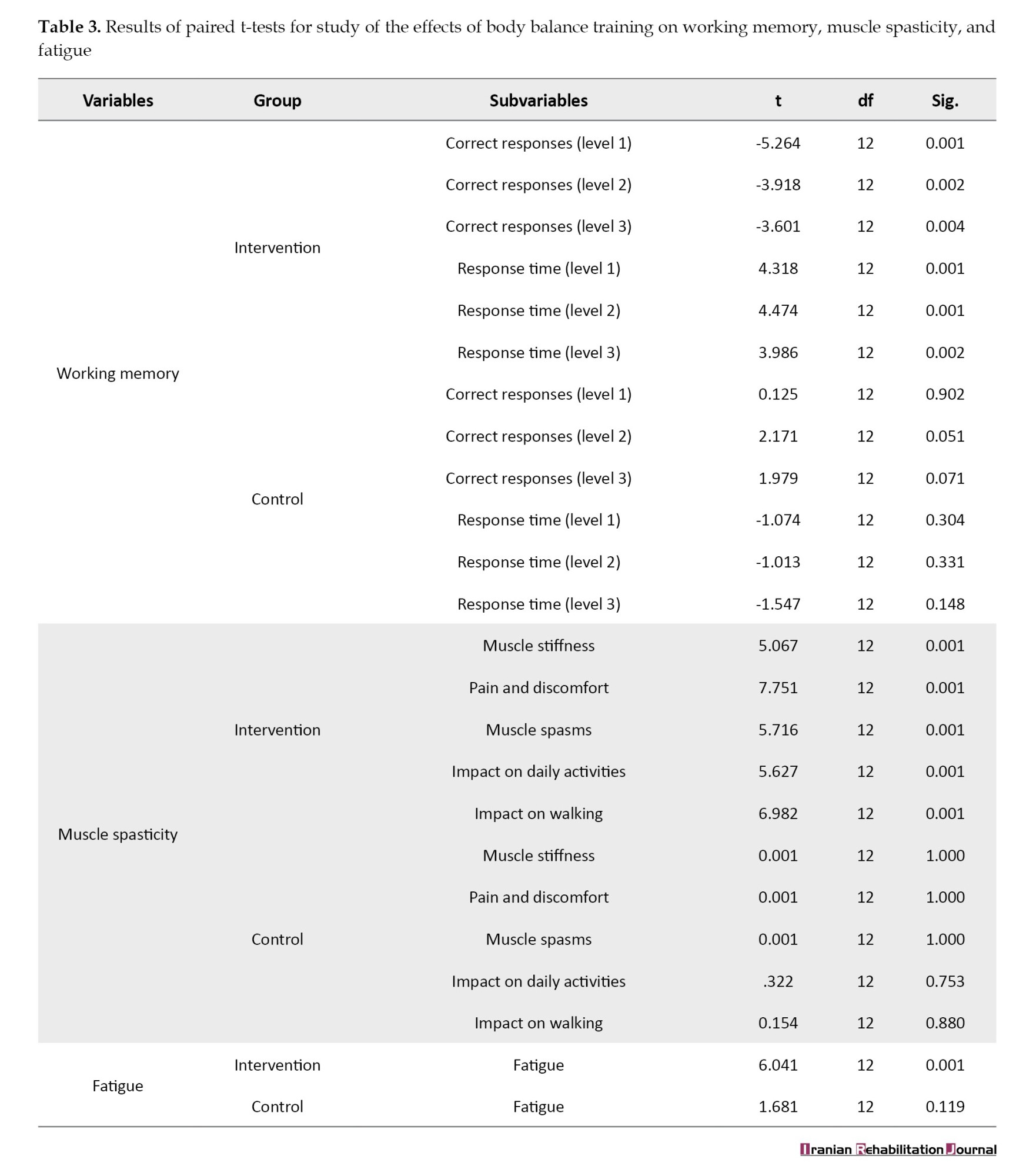
The paired t-test results (Table 3) indicated significant within-group improvements in the intervention group across all measured variables following the 8-week body balance training program.
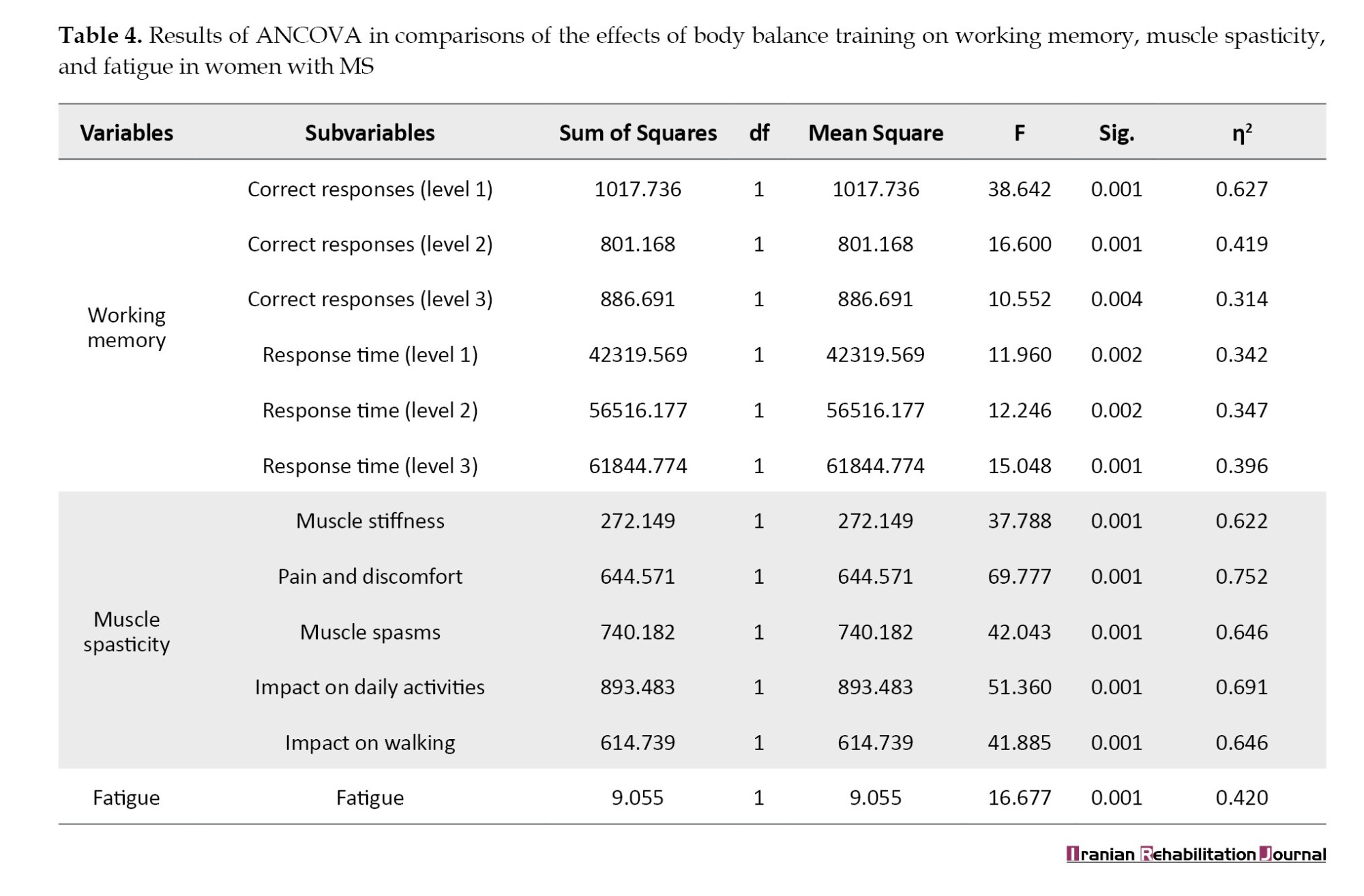
For between-group comparisons, ANCOVA was conducted, adjusting for baseline pre-test scores. No additional covariates (e.g. EDSS scores) were included because the baseline characteristics between groups were not significantly different. To control for the risk of type I error due to multiple comparisons, the Bonferroni correction was applied where necessary. Table 4 presents ANCOVA results.
The ANCOVA results (Table 4) revealed significant between-group differences across all measured variables, including working memory performance, muscle spasticity, and fatigue (P<0.05). Eta squared (η²) values indicated moderate to large effect sizes for all outcomes, suggesting a meaningful impact of the body balance intervention. Regarding safety monitoring, no adverse events were reported during the intervention period, supporting the feasibility and tolerability of the body balance training protocol for individuals with MS.
Discussion
This randomized controlled trial examined the effects of an 8-week body balance training program on working memory, muscle spasticity, and fatigue in women with RRMS. The intervention group demonstrated statistically significant improvements across all outcomes compared to the control group, underscoring the efficacy of this hybrid exercise modality—integrating yoga, Tai Chi, and Pilates—as a non-pharmacological approach to MS symptom management. Unlike traditional exercise programs focusing primarily on aerobic capacity or isolated muscle strengthening, body balance training emphasizes integrated movement patterns, postural control, and mind-body coordination. This holistic focus may explain its broader impact on both cognitive and physical domains in patients with MS. These findings contribute to the expanding evidence base supporting exercise interventions in MS, offering novel insights into the potential of Body Balance training to enhance overall functioning and QoL in this population.
The intervention group exhibited robust enhancements in working memory, as measured by the N-back test, with significant increases in correct responses and reductions in response times across all levels (1-back, 2-back, 3-back; P ranging from<0.001 to 0.004). No such changes were observed in the control group, affirming the intervention’s specific impact. These results align with a growing body of literature on exercise-induced cognitive benefits in MS. Ozkul et al. (2020) found that balance-focused exercises improve working memory by engaging attentional and executive functions, a mechanism likely amplified by body balance’s demand for sustained concentration and precise movement execution [26]. A recent systematic review by Chen et al. reported moderate-to-strong evidence that multimodal exercise enhances cognitive performance in MS, attributing these gains to increased cerebral blood flow, improved oxygenation, and enhanced neuroplasticity [45]. The prefrontal cortex, a critical region for working memory, may be particularly stimulated by body balance’s cognitive load [46], as participants must integrate sensory feedback, maintain focus, and coordinate complex sequences. This finding is consistent with the results of Abasıyanık et al. (2020), who noted that balance training’s attentional demands bolster cognitive outcomes [47], and Velikonja et al., who linked physical activity to improvements in memory in MS [48]. However, the unique contribution of body balance’s hybrid design, compared to standalone modalities, such as yoga or Pilates, remains underexplored. Future studies should directly compare body balance with single-modality interventions to delineate the added value of integrating multiple movement disciplines. Such comparisons are crucial to identify whether the observed cognitive benefits arise primarily from the diversity and complexity of the combined approach or if similar outcomes could be achieved with simpler, more targeted programs. Exploring these differences would refine exercise prescriptions for MS and optimize therapeutic outcomes. The potential mechanisms underlying body balance’s advantages may include enhanced neurovascular coupling, increased synaptic plasticity, and reduced stress-related cognitive interference, possibly mediated by lower cortisol levels [49].
Muscle spasticity, assessed via five MSSS-88 subscales (muscle stiffness, pain and discomfort, muscle spasms, impact on daily activities, and walking), significantly decreased in the intervention group (P<0.001 across all subscales), while the control group remained unchanged. These findings resonate with emerging research on exercise as a modulator of spasticity in MS. Tollár et al. (2021) demonstrated that multimodal training reduces spasticity by improving neuromuscular coordination and joint mobility [23], while Miller et al. reported that yoga-based interventions decrease muscle stiffness through enhanced relaxation and flexibility—outcomes mirrored in this study [50]. MS-related spasticity results from demyelination-induced hyperexcitability of motor pathways [51]; body balance’s slow, deliberate movements may counteract this by reducing muscle tone, enhancing proprioceptive input, and improving motor control [52]. These results align with Moghadasi et al., who observed improved muscle stiffness and range of motion following physical activity [53], and Gentile et al. who highlighted exercise’s role in functional gains [54]. Whether these improvements stem from direct neural modulation (e.g. reduced reflex hyperexcitability) or secondary effects of enhanced flexibility and strength remains unclear. Future research could explore this uncertainty by employing neurophysiological techniques such as electromyography (EMG) or transcranial magnetic stimulation to directly measure neural changes in response to body balance training. Additionally, comparing the effects of body balance to other exercise modalities targeting spasticity, such as strength training or stretching programs, could provide further insights into the specific mechanisms at play.
Fatigue, a debilitating MS symptom measured using the FSS, significantly decreased in the intervention group (P<0.001), with no notable changes in the control group. This finding is consistent with extensive evidence of exercise’s fatigue-reducing effects in MS. Torres-Costoso et al. identified combined exercise as a highly effective strategy [55], reporting effect sizes (η²≈0.42) comparable to ours, while Heine et al. noted moderate benefits from structured activity, linking them to improved energy metabolism and sleep quality [56]. A 2020 meta-analysis by Razazian et al. further confirmed that moderate-intensity exercise consistently mitigates fatigue in MS [11], contrasting with Hsieh et al. who found no effect from high-intensity mountaineering—likely due to its excessive demands exceeding MS patients’ energy reserves [57]. Body balance’s moderate intensity avoids overexertion, promoting energy restoration through enhanced mitochondrial efficiency, improved circulation, and stress reduction via endorphin release [45]. Its mindfulness and breathing components may further alleviate psychological fatigue by enhancing relaxation and sleep patterns, as suggested by Scott (2008) [49]. These multifaceted effects position body balance as a practical alternative to more physically taxing interventions, though its relative efficacy remains untested compared to aerobic or resistance training.
The novelty of the present study is a hybrid training program; body balance training, which offers distinct advantages over standalone modalities like yoga, Tai Chi, or Pilates, which require greater time, energy, and resources—often impractical for MS patients with limited physical capacity. By integrating these elements into a single, low-cost, equipment-light program, body balance delivers cognitive, motor, and symptomatic benefits within a feasible framework, as evidenced by its significant effects (P<0.05 for all outcomes). This practicality enhances its potential for clinical adoption, complementing pharmacological treatments and addressing the holistic needs of patients with MS.
While this study offers compelling evidence for the efficacy of body balance training in women with MS, several methodological constraints must be acknowledged to contextualize the findings. First, the sample size was modest (n=26), limited to female participants with RRMS, which restricts the applicability of results to men, individuals with progressive MS subtypes, or larger, more heterogeneous populations. This homogeneity may mask potential sex-specific or disease-stage-specific responses to the intervention. Second, the absence of a follow-up assessment beyond the 8-week intervention period precludes insights into the longevity of the benefits. Future studies could include follow-up assessments to evaluate the long-term effects of body balance training on MS symptoms. Third, reliance on self-reported measures, such as the FSS and MSSS-88, introduces subjectivity and recall bias, which may not fully capture physiological changes. Detailing how these tools were administered and whether any efforts were made to minimize bias (e.g. blinded assessment or standardized instructions) could enhance methodological transparency. In future research, it would be valuable to explore how body balance affects individuals with other MS subtypes, such as secondary progressive MS, and to compare responses by sex or disease severity. Moreover, clarifying the relative contribution of each component (yoga, Tai Chi, Pilates) and the mechanisms underlying their synergistic effects could help refine exercise prescriptions. Large-scale, longitudinal trials using objective neurophysiological and neuroimaging markers would also strengthen causal inferences and determine the sustainability of intervention effects over time.
Conclusion
This study provides compelling evidence that 8 weeks of body balance training significantly enhances working memory, reduces muscle spasticity, and alleviates fatigue in women with MS. These findings highlight its potential as a scalable, non-pharmacological intervention to improve QoL and functional outcomes in MS management. Larger, longitudinal trials are needed to confirm its efficacy, explore its sustained benefits, and refine its integration into comprehensive rehabilitation strategies.
Ethical Considerations
Compliance with ethical guidelines
All stages of the research were conducted with the approval of the Ethics Committee of the University of Tehran, Tehran, Iran (Code: ETHIC-20244-1199 [R1]).
Funding
The present study is extracted from the master’s thesis of Leila Pourgholam Masoudi approved by the Department of Biomechanics and sports injury, Faculty of Health and Sport Sciences, University of Tehran, Tehran, Iran.
Authors' contributions
All authors contributed equally to the preparation of this manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all patients for participating in this study.
References
Multiple sclerosis (MS) is a chronic and complex disease of the central nervous system characterized by the degradation of the myelin sheath and neurons, resulting in widespread effects on affected individuals’ physical and cognitive functioning [1]. Individuals with MS face numerous challenges that impair their abilities across all dimensions of life [2]. A primary difficulty associated with this condition is the occurrence of symptom exacerbations, which manifest in 85-90% of cases and, due to their unpredictable nature, complicate disease management [3, 4]. Among the most prominent issues affecting the MS community are memory impairments, muscle spasm, and fatigue [5]. Approximately 60% of MS patients experience memory deficits, particularly impacting working memory and remote conscious memory [6]. These deficits are most evident in short-term memory, with patients struggling to recall details of recent conversations or events. However, their ability to remember distant past events typically remains intact [7]. Neuroimaging studies have shown that MS alters brain activation patterns associated with working memory. Patients often recruit additional or compensatory brain regions, such as prefrontal or parietal areas, to offset working memory impairments [8]. Fatigue, another prevalent and debilitating symptom of MS, is reported in 65% to 85% of patients and is defined as a pervasive sense of energy depletion [9, 10]. This condition, rooted in both physiological and psychological factors [11], is often exacerbated by sleep disturbances, depression, and medication side effects [12]. Additionally, muscle spasms, affecting at least 65 percent of MS patients, arise from damage to upper motor neurons and abnormal spinal reflex activity [13]. This condition is characterized by increased muscle tone, excessive stimulation, weakness, pain, and involuntary movements (spasms), which may progress to muscle contractures in severe cases [14]. While the body balance training in this study demonstrated promising improvements in working memory, muscle spasticity, and fatigue, it is important to note that the effectiveness of this intervention may vary depending on individual patient factors, such as disease severity, age, and response to exercise. While promising, this intervention is not a “quick fix” and should be considered part of a comprehensive, long-term therapeutic strategy. Previous research has suggested positive outcomes for exercise interventions in MS; however, the speed and extent of improvements can differ from patient to patient [15].
According to recent epidemiological studies, the number of individuals affected by MS has risen from 2.3 million in 2013 to 2.9 million in 2023, reflecting the increasing global burden of the disease [16]. In Iran, the annual incidence rate averages 6.5 per 100000 people, with some regions reporting rates as high as 12.8 per 100000 [17]. These alarming statistics, combined with limited accessibility to advanced pharmacological treatments, underscore the urgent need for affordable, non-pharmacological interventions. Recent research has increasingly focused on the potential of physical activity and exercise to manage MS symptoms [18]. Historically, physicians have advised patients with MS to avoid physical exertion, fearing potential exacerbation of symptoms. However,`suggests that, with appropriate guidance, exercise can serve as an effective non-pharmacological intervention. It can enhance aerobic capacity, muscle strength, flexibility, and balance and also plays a crucial role in managing fatigue levels, cognitive function, and memory [19-21]. In light of this growing body of evidence, exploring the specific effects of different exercise modalities on MS symptom progression is increasingly crucial, as regular physical activity has been shown to improve cardiopulmonary fitness, muscular strength and endurance, alleviate systemic fatigue, and positively influence mood and cognitive performance [22].
Suitable exercise options for patients with MS are yoga, Pilates, and Tai Chi [23]. Numerous studies have reported positive outcomes from these activities in addressing challenges faced by older adults and individuals with specific conditions, such as Parkinson’s disease and MS. For instance, research has shown that in women with MS receiving standard immunomodulatory treatments, yoga and hydrotherapy [24], without endurance or coordination exercises [25], produce comparable benefits in reducing fatigue, depression, and paresthesia. Similarly, Ozkul et al. (2020) identified beneficial effects of combining aerobic exercise and Pilates in patients with MS and cognitive impairment, noting positive correlations with improvements in cognition, mood, and quality of life (QoL) post-exercise [26]. Body balance training has emerged as a promising hybrid approach among these exercise interventions. Body balance is a gym-based holistic workout that includes both traditional methods, such as yoga and Tai Chi, and more recently developed methods, such as Pilates. A reasonable assumption is that body balance would also have similar benefits as its elements (yoga, Tai Chi, and pilates), such as improvement of balance, flexibility, mobility, posture, anxiety, and muscle strength [27, 28]. In this study, body balance training consisted of structured sessions incorporating a standardized sequence of yoga poses, Tai Chi movements, and Pilates-based exercises, focusing on core stability, flexibility, controlled breathing, and postural alignment, conducted three times a week over eight weeks. It is reasonable to assume that body balance offers benefits similar to its elements, such as improvements in balance, flexibility, mobility, posture, anxiety, and muscle strength [29].
Drawing from controlled, purposeful movements inspired by yoga, Tai Chi, and Pilates [29], these exercises emphasize balance, coordination, and physical strength, potentially mitigating mobility and impairments from MS-related neurological damage [30, 31]. Preliminary findings suggest that consistent engagement in body balance exercises reduces the frequency and severity of muscle spasms, alleviates severe fatigue and enhances patients’ capacity to perform daily tasks [32, 33]. Moreover, given the established link between physical activity and cognitive function, body balance training may positively influence working memory, although this aspect remains underexplored in the MS population. Despite the established benefits of yoga, Tai Chi, and Pilates, limited research has specifically examined the combined effects of body balance training on cognitive outcomes, particularly working memory, alongside physical symptoms in patients with MS. This study aimed to address this gap by evaluating the impact of body balance training on working memory, muscle spasms, and fatigue. Requiring minimal equipment and adaptable to various settings, these exercises offer a cost-effective and practical rehabilitation option.
Given the limitations of pharmacological treatments and the need for complementary approaches, this study aims to evaluate the effects of body balance training on three key domains in MS patients: Working memory, muscle spasticity, and fatigue. These domains were selected because they represent some of the most debilitating and commonly reported symptoms in individuals with MS, significantly impacting daily functioning and QoL. Moreover, previous research has indicated that exercise modalities incorporated into body balance, such as yoga, Tai Chi, and Pilates, can individually contribute to improvements in cognitive performance, reductions in spasticity, and alleviation of fatigue. Therefore, it is reasonable to hypothesize that an integrated body balance program may exert beneficial effects across these interrelated outcomes, ultimately improving QoL and overall health. Grounded in existing scientific frameworks and responsive to patients’ practical needs, this research aims to determine whether body balance training, as a non-pharmacological therapeutic strategy, can mitigate the debilitating symptoms of MS and improve the physical and cognitive capacities of affected individuals. We hypothesized that body balance training would lead to significant improvements in working memory, reductions in muscle spasticity, and decreases in fatigue compared to standard care.
Materials and Methods
This study utilized a single-blind, randomized controlled trial with a pre-test-post-test design, featuring an active intervention group and a control group. In this design, outcome assessors were blinded to group assignments to minimize assessment bias. Initially, 30 female participants diagnosed with relapsing-remitting MS (RRMS) (mean age=33.38±4.99 years) were recruited from the MS community in Karaj City, Iran, after obtaining informed consent. Participants were randomly allocated to either the intervention group (n=15) or the control group (n=15) using a computer-generated randomization sequence with allocation concealment ensured through sealed, opaque envelopes handled by an independent researcher. During the study, four participants dropped out, two from each group, due to relocation, engagement in alternative exercise programs, or loss of contact, resulting in a final sample of 26 participants (13 per group). No significant differences in dropout rates were observed between the experimental and control groups, and the reasons for dropout were consistent across both groups. Therefore, the dropout pattern is unlikely to influence the study’s overall results. Only data from participants who completed the study were included in the final analysis; no intention-to-treat approach was applied. The inclusion criteria included female patients aged 25–40 years. While the 15-year age range may introduce variability, this range was selected to capture a broad representation of adult women with RRMS, avoiding extreme age-related differences that could confound results. Additionally, potential age-related differences were considered and controlled for in the statistical analysis, ensuring that the effects observed are not significantly influenced by age. More inclusion criteria include a confirmed diagnosis of RRMS by a neurologist. Expanded disability status scale (EDSS) score below 4 (indicating mild to moderate disability) [34], no participation in body balance training for at least two months prior to the study, no engagement in other physical activities during the study period, no concurrent psychiatric, psychotherapeutic, or cognitive rehabilitation interventions, no diagnosis of additional neuromuscular disorders, no use of medications affecting muscle spasticity or fatigue, no participation in alternative treatment modalities during the study, no disease relapse within two months prior to study enrollment.
Written informed consent was obtained from all participants prior to the study. Demographic and clinical information, including age, disease duration, and medication history, was collected at baseline. The study protocol was approved by the Ethics Committee of the University of Tehran.
Assessment tools
Three primary outcome measures were evaluated: Working memory, muscle spasticity, and fatigue. All assessments, including the N-back, MS spasticity scale (MSSS-88), and fatigue severity scale (FSS), were administered under the supervision of trained researchers in a quiet research setting. The testing sessions took place between 9 AM and 12 PM to minimize potential variations in cognitive and fatigue responses due to time of day. A standardized protocol was followed to ensure consistency across all participants, and the environment was free of distractions to provide optimal testing conditions. Although the primary aim of the study was to assess cognitive and fatigue outcomes, future studies should incorporate motor tests, such as balance assessments, to evaluate the physical aspects of balance interventions in patients with MS. Given the nature of the body balance program, which integrates elements of yoga, Tai Chi, and Pilates, balance-related tests (e.g. Berg balance scale or timed up and go test) could provide essential data regarding the physical improvements resulting from the intervention, and thus should be part of the assessment protocol in future research.
Working memory assessment: N-back test
The N-Back test evaluates executive functions, with a particular focus on working memory. It requires participants to retain and manipulate information during task performance [35]. It has demonstrated high reliability, with validity coefficients ranging from 0.54 to 0.84 in previous studies [36]. The N-back test is considered a robust measure of working memory performance. Participants responded to a series of visual stimuli on a computer screen by pressing designated keys to indicate whether the current stimulus matched one presented n steps earlier in the sequence. The test consists of three levels: 1-back (matching the immediate prior stimulus), 2-back (matching the stimulus two steps back), and 3-back (matching the stimulus three steps back). A practice phase preceded the main test to ensure comprehension. The test lasted approximately 10 minutes, and the outcomes were measured in terms of accuracy (correct responses), reaction time for correct responses, incorrect responses, and unanswered items. For this study, accuracy (correct responses) was the primary outcome measure for working memory performance, with reaction time considered a secondary metric.
Muscle spasticity assessment: MSSS-88
Muscle spasticity was assessed using the MSSS-88, a patient-centered questionnaire comprising 88 items scored from 1 (no discomfort) to 4 (maximum discomfort), evaluating spasticity across eight distinct subscales [37, 38]. In this study, following a preliminary needs assessment and based on clinical recommendations from the physical activity guide for MS by Azad (2022), five subscales—muscle stiffness, pain and discomfort, muscle spasms, activities of daily living, and walking—were selected for analysis [39]. These subscales were prioritized because they most directly reflect the physical and functional impairments targeted by body balance training, particularly regarding mobility and daily function, which were central goals of the intervention. The MSSS-88 has demonstrated strong psychometric properties, with its validity and reliability confirmed in German [40], Serbian [41], and Persian [42] versions. It is important to note that if the guideline cited by Azad is unpublished, the recommendations are considered expert opinions based on clinical practice in the context of MS rehabilitation in Iran.
Fatigue assessment: FSS
Fatigue was assessed using the FSS, a 9-item self-report questionnaire developed by Krupp et al. in 1989 to measure the severity of fatigue symptoms in clinical populations, particularly in individuals with multiple sclerosis [43]. Each item is rated on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating greater severity of fatigue. The final score is calculated by averaging the responses across all nine items, with scores above four typically indicative of clinically significant fatigue. The FSS has demonstrated strong psychometric properties in MS populations, with reported validity of 0.78 and reliability of 0.93 [44]. This tool offers a simple, efficient, and reliable method for comprehensively assessing the impact of fatigue on daily functioning in MS patients.
Body balance training protocol
The body balance training protocol implemented in this study was adapted from a program by Khan et al. (2008), as referenced in the operational definition of body balance [28]. This protocol was selected because it combines elements of yoga, Tai Chi, and Pilates, specifically structured to improve balance, flexibility, and neuromuscular control, which are commonly impaired in patients with multiple sclerosis. Additionally, the exercises emphasized low-impact, controlled movements, making them particularly suitable for individuals with mild to moderate MS-related disability. The 8-week body balance training program consisted of 24 sessions, with participants attending three 60-minute sessions per week. Each session was organized into distinct phases: Warm-up, strength and core stability training, balance and flexibility exercises, and relaxation. The exercise protocol was progressively individualized throughout the intervention period in response to each participant’s performance capacity and tolerance levels. To promote gradual progression while minimizing the risk of injury, tailored modifications were implemented, including adjustments, such as limiting the range of motion, altering the base of support, or incorporating low-level challenges (e.g. performing balance exercises with eyes closed). Table 1 presents a detailed summary of the training components.
In this protocol, modifications were made for patients with MS, taking into account their physical limitations and ensuring their safety. For example, balance poses were performed with support (using a chair or wall) when necessary, and the intensity of strength exercises was adjusted to the individual’s capacity. Additionally, the protocol was designed to be flexible, allowing gradual progression of exercises as participants gained strength and stability over the 8-week period. For future adaptations, the original 12-week protocol was condensed to 8 weeks, reducing the overall volume of each session and focusing on key exercises that could be easily modified to accommodate the specific needs of patients with MS. Weekly progression was carefully monitored to ensure participants’ safety and maximize benefit. The control groJdard care, which included adherence to prescribed disease-modifying therapies, routine follow-up visits with neurologists, and general health advice regarding nutrition, sleep hygiene, and stress management. No additional structured physical activity or exercise interventions were introduced during the study period. Both groups continued their regular MS medications as prescribed.
Procedure
Baseline assessments were conducted one week prior to the start of the intervention at the Rehabilitation Research Laboratory, University of Tehran. These assessments included working memory (via the N-back test), muscle spasticity (via selected MSSS-88 subscales), and fatigue (via the FSS questionnaire). All assessments were conducted by trained evaluators with experience in neuropsychological testing in MS populations. Following baseline evaluations, participants were randomly assigned to either the intervention or control group. The intervention group participated in an 8-week body balance training program, held three times per week at a standardized local sports facility equipped with accessible flooring, temperature control (21-23 °C), and MS-friendly infrastructure. Each 60-minute session was structured into distinct phases: Warm-up, strength, balance, flexibility, core strengthening, and relaxation, with progressive adaptations based on participant feedback and performance. The program was supervised by a certified physiotherapist with specialization in neurorehabilitation and at least five years of experience working with MS patients. Exercises were drawn from yoga, Tai Chi, and Pilates, and were tailored to individual physical limitations using support tools (e.g. chairs, walls) when necessary. Participants who demonstrated ≥80% success in task completion or self-reported comfort were advanced to slightly more challenging versions of the same exercises. The control group received standard care, which consisted of adherence to prescribed MS medications, neurologist follow-ups every 8–12 weeks, and general lifestyle guidance. No structured exercise or physiotherapy programs were included in the standard care. All participants completed the post-test immediately after the intervention, using the same measures and blinded procedures as in the pre-test. Adverse events were monitored using session checklists and weekly self-reports. No serious adverse events occurred. No follow-up assessments were planned beyond the immediate post-intervention phase; however, future research is recommended to explore long-term effects. Statistical analysis was conducted using SPSS software, version 27, employing paired t-tests for within-group comparisons and analysis of covariance (ANCOVA) for between-group comparisons, adjusting for baseline scores. A significance level of P<0.05 was used.
Results
Table 2 presents a descriptive summary of the participants’ demographic characteristics. This table provides an overview of key variables for the intervention (body balance training) and control groups, including age, height, weight, body mass index (BMI), disease duration, and EDSS scores. All participants were patients with the relapsing-remitting subtype of MS, receiving routine MS pharmacotherapy and performing usual daily activities (without regular physical activity).
As shown in Table 2, the mean values of demographic variables were closely aligned between the intervention and control groups, indicating a high degree of similarity. Statistical comparisons of these demographic characteristics revealed no significant differences between the two groups, confirming that the intervention and control groups were comparable at baseline.
Before conducting the statistical analyses, assumptions required for parametric testing were evaluated. The Shapiro-Wilk test confirmed that all variables exhibited normal distribution (P>0.05). Homogeneity of variances was assessed using Levene’s test, confirming equality of error variances across groups (P>0.05). For ANCOVA, the assumption of homogeneity of regression slopes was tested and met, indicating that the relationship between pre-test scores and post-test outcomes was consistent across groups. Subsequently, paired t-tests were employed to assess within-group changes between pre- and post-intervention scores for the intervention (body balance training) and control groups. Cohen’s d effect sizes were also calculated to determine the magnitude of change within each group. Table 3 presents the results of paired t-tests analyzing the effects of body balance training on working memory, muscle spasticity, and fatigue. For the N-back test assessing working memory, three levels of task difficulty were examined: Level 1 (1-back: Comparison with the immediately preceding stimulus), level 2 (2-back: Comparison with the stimulus two steps earlier), and level 3 (3-back: Comparison with the stimulus three steps earlier). Outcomes included the number of correct responses and mean response time for correct responses at each level. Significant improvements were observed in the intervention group across all levels, both in increasing correct responses and decreasing response times, whereas the control group showed no significant changes. Similarly, for muscle spasticity (measured via selected subscales of the MSSS-88) and fatigue (measured via FSS), the intervention group demonstrated significant reductions post-intervention, while the control group exhibited no meaningful changes.
The paired t-test results (Table 3) indicated significant within-group improvements in the intervention group across all measured variables following the 8-week body balance training program.
For between-group comparisons, ANCOVA was conducted, adjusting for baseline pre-test scores. No additional covariates (e.g. EDSS scores) were included because the baseline characteristics between groups were not significantly different. To control for the risk of type I error due to multiple comparisons, the Bonferroni correction was applied where necessary. Table 4 presents ANCOVA results.
The ANCOVA results (Table 4) revealed significant between-group differences across all measured variables, including working memory performance, muscle spasticity, and fatigue (P<0.05). Eta squared (η²) values indicated moderate to large effect sizes for all outcomes, suggesting a meaningful impact of the body balance intervention. Regarding safety monitoring, no adverse events were reported during the intervention period, supporting the feasibility and tolerability of the body balance training protocol for individuals with MS.
Discussion
This randomized controlled trial examined the effects of an 8-week body balance training program on working memory, muscle spasticity, and fatigue in women with RRMS. The intervention group demonstrated statistically significant improvements across all outcomes compared to the control group, underscoring the efficacy of this hybrid exercise modality—integrating yoga, Tai Chi, and Pilates—as a non-pharmacological approach to MS symptom management. Unlike traditional exercise programs focusing primarily on aerobic capacity or isolated muscle strengthening, body balance training emphasizes integrated movement patterns, postural control, and mind-body coordination. This holistic focus may explain its broader impact on both cognitive and physical domains in patients with MS. These findings contribute to the expanding evidence base supporting exercise interventions in MS, offering novel insights into the potential of Body Balance training to enhance overall functioning and QoL in this population.
The intervention group exhibited robust enhancements in working memory, as measured by the N-back test, with significant increases in correct responses and reductions in response times across all levels (1-back, 2-back, 3-back; P ranging from<0.001 to 0.004). No such changes were observed in the control group, affirming the intervention’s specific impact. These results align with a growing body of literature on exercise-induced cognitive benefits in MS. Ozkul et al. (2020) found that balance-focused exercises improve working memory by engaging attentional and executive functions, a mechanism likely amplified by body balance’s demand for sustained concentration and precise movement execution [26]. A recent systematic review by Chen et al. reported moderate-to-strong evidence that multimodal exercise enhances cognitive performance in MS, attributing these gains to increased cerebral blood flow, improved oxygenation, and enhanced neuroplasticity [45]. The prefrontal cortex, a critical region for working memory, may be particularly stimulated by body balance’s cognitive load [46], as participants must integrate sensory feedback, maintain focus, and coordinate complex sequences. This finding is consistent with the results of Abasıyanık et al. (2020), who noted that balance training’s attentional demands bolster cognitive outcomes [47], and Velikonja et al., who linked physical activity to improvements in memory in MS [48]. However, the unique contribution of body balance’s hybrid design, compared to standalone modalities, such as yoga or Pilates, remains underexplored. Future studies should directly compare body balance with single-modality interventions to delineate the added value of integrating multiple movement disciplines. Such comparisons are crucial to identify whether the observed cognitive benefits arise primarily from the diversity and complexity of the combined approach or if similar outcomes could be achieved with simpler, more targeted programs. Exploring these differences would refine exercise prescriptions for MS and optimize therapeutic outcomes. The potential mechanisms underlying body balance’s advantages may include enhanced neurovascular coupling, increased synaptic plasticity, and reduced stress-related cognitive interference, possibly mediated by lower cortisol levels [49].
Muscle spasticity, assessed via five MSSS-88 subscales (muscle stiffness, pain and discomfort, muscle spasms, impact on daily activities, and walking), significantly decreased in the intervention group (P<0.001 across all subscales), while the control group remained unchanged. These findings resonate with emerging research on exercise as a modulator of spasticity in MS. Tollár et al. (2021) demonstrated that multimodal training reduces spasticity by improving neuromuscular coordination and joint mobility [23], while Miller et al. reported that yoga-based interventions decrease muscle stiffness through enhanced relaxation and flexibility—outcomes mirrored in this study [50]. MS-related spasticity results from demyelination-induced hyperexcitability of motor pathways [51]; body balance’s slow, deliberate movements may counteract this by reducing muscle tone, enhancing proprioceptive input, and improving motor control [52]. These results align with Moghadasi et al., who observed improved muscle stiffness and range of motion following physical activity [53], and Gentile et al. who highlighted exercise’s role in functional gains [54]. Whether these improvements stem from direct neural modulation (e.g. reduced reflex hyperexcitability) or secondary effects of enhanced flexibility and strength remains unclear. Future research could explore this uncertainty by employing neurophysiological techniques such as electromyography (EMG) or transcranial magnetic stimulation to directly measure neural changes in response to body balance training. Additionally, comparing the effects of body balance to other exercise modalities targeting spasticity, such as strength training or stretching programs, could provide further insights into the specific mechanisms at play.
Fatigue, a debilitating MS symptom measured using the FSS, significantly decreased in the intervention group (P<0.001), with no notable changes in the control group. This finding is consistent with extensive evidence of exercise’s fatigue-reducing effects in MS. Torres-Costoso et al. identified combined exercise as a highly effective strategy [55], reporting effect sizes (η²≈0.42) comparable to ours, while Heine et al. noted moderate benefits from structured activity, linking them to improved energy metabolism and sleep quality [56]. A 2020 meta-analysis by Razazian et al. further confirmed that moderate-intensity exercise consistently mitigates fatigue in MS [11], contrasting with Hsieh et al. who found no effect from high-intensity mountaineering—likely due to its excessive demands exceeding MS patients’ energy reserves [57]. Body balance’s moderate intensity avoids overexertion, promoting energy restoration through enhanced mitochondrial efficiency, improved circulation, and stress reduction via endorphin release [45]. Its mindfulness and breathing components may further alleviate psychological fatigue by enhancing relaxation and sleep patterns, as suggested by Scott (2008) [49]. These multifaceted effects position body balance as a practical alternative to more physically taxing interventions, though its relative efficacy remains untested compared to aerobic or resistance training.
The novelty of the present study is a hybrid training program; body balance training, which offers distinct advantages over standalone modalities like yoga, Tai Chi, or Pilates, which require greater time, energy, and resources—often impractical for MS patients with limited physical capacity. By integrating these elements into a single, low-cost, equipment-light program, body balance delivers cognitive, motor, and symptomatic benefits within a feasible framework, as evidenced by its significant effects (P<0.05 for all outcomes). This practicality enhances its potential for clinical adoption, complementing pharmacological treatments and addressing the holistic needs of patients with MS.
While this study offers compelling evidence for the efficacy of body balance training in women with MS, several methodological constraints must be acknowledged to contextualize the findings. First, the sample size was modest (n=26), limited to female participants with RRMS, which restricts the applicability of results to men, individuals with progressive MS subtypes, or larger, more heterogeneous populations. This homogeneity may mask potential sex-specific or disease-stage-specific responses to the intervention. Second, the absence of a follow-up assessment beyond the 8-week intervention period precludes insights into the longevity of the benefits. Future studies could include follow-up assessments to evaluate the long-term effects of body balance training on MS symptoms. Third, reliance on self-reported measures, such as the FSS and MSSS-88, introduces subjectivity and recall bias, which may not fully capture physiological changes. Detailing how these tools were administered and whether any efforts were made to minimize bias (e.g. blinded assessment or standardized instructions) could enhance methodological transparency. In future research, it would be valuable to explore how body balance affects individuals with other MS subtypes, such as secondary progressive MS, and to compare responses by sex or disease severity. Moreover, clarifying the relative contribution of each component (yoga, Tai Chi, Pilates) and the mechanisms underlying their synergistic effects could help refine exercise prescriptions. Large-scale, longitudinal trials using objective neurophysiological and neuroimaging markers would also strengthen causal inferences and determine the sustainability of intervention effects over time.
Conclusion
This study provides compelling evidence that 8 weeks of body balance training significantly enhances working memory, reduces muscle spasticity, and alleviates fatigue in women with MS. These findings highlight its potential as a scalable, non-pharmacological intervention to improve QoL and functional outcomes in MS management. Larger, longitudinal trials are needed to confirm its efficacy, explore its sustained benefits, and refine its integration into comprehensive rehabilitation strategies.
Ethical Considerations
Compliance with ethical guidelines
All stages of the research were conducted with the approval of the Ethics Committee of the University of Tehran, Tehran, Iran (Code: ETHIC-20244-1199 [R1]).
Funding
The present study is extracted from the master’s thesis of Leila Pourgholam Masoudi approved by the Department of Biomechanics and sports injury, Faculty of Health and Sport Sciences, University of Tehran, Tehran, Iran.
Authors' contributions
All authors contributed equally to the preparation of this manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all patients for participating in this study.
References
- Woo MS, Engler JB, Friese MA. The neuropathobiology of multiple sclerosis. Nature Reviews. Neuroscience. 2024; 25(7):493-513. [DOI:10.1038/s41583-024-00823-z] [PMID]
- Titlić M, Matijaca M, Marović A, Lusić I, Tonkić A, Jukić I, Karacić S, Capkun V. [Study of quality of life in patients with multiple sclerosis (Croatian)]. Acta Medica Croatica. 2007; 61(4):355-60. [PMID]
- Liu Y, Morgan C, Hornung L, Tyry T, Salter AR, Agashivala N, et al. Relationship between symptom change, relapse activity and disability progression in multiple sclerosis. Journal of the Neurological Sciences. 2016; 362:121-6. [DOI:10.1016/j.jns.2016.01.034] [PMID]
- Buljevac D, Hop WC, Reedeker W, Janssens AC, van der Meché FG, van Doorn PA, et al. Self reported stressful life events and exacerbations in multiple sclerosis: Prospective study. BMJ. 2003; 327(7416):646. [DOI:10.1136/bmj.327.7416.646] [PMID]
- Krupp LB. Fatigue in multiple sclerosis: A guide to diagnosis and management. New York: Demos Medical Publishing; 2004. [Link]
- Grafman J, Rao S, Bernardin L, Leo GJ. Automatic memory processes in patients with multiple sclerosis. Archives of Neurology. 1991; 48(10):1072-5. [DOI:10.1001/archneur.1991.00530220094025] [PMID]
- Antonis T. Memory disorders in multiple sclerosis. Open Journal of Case Reports. 2021; 2(4):1-2. [Link]
- Wishart HA, Saykin A, McDonald B, Mamourian A, Flashman L, Schuschu K, et al. Brain activation patterns associated with working memory in relapsing-remitting MS. Neurology. 2004; 62(2):234-8. [DOI:10.1212/01.WNL.0000103238.91536.5F] [PMID]
- Schwartz JE, Jandorf L, Krupp LB. The measurement of fatigue: A new instrument. Journal of Psychosomatic Research. 1993; 37(7):753-62. [DOI:10.1016/0022-3999(93)90104-N] [PMID]
- Fisk JD, Pontefract A, Ritvo PG, Archibald CJ, Murray T. The impact of fatigue on patients with multiple sclerosis. Canadian Journal of Neurological Sciences. 1994; 21(1):9-14. [DOI:10.1017/S0317167100048691]
- Razazian N, Kazeminia M, Moayedi H, Daneshkhah A, Shohaimi S, Mohammadi M, et al. The impact of physical exercise on the fatigue symptoms in patients with multiple sclerosis: A systematic review and meta-analysis. BMC Neurology. 2020; 20(1):93. [DOI:10.1186/s12883-020-01654-y] [PMID]
- Oliva Ramirez A, Keenan A, Kalau O, Worthington E, Cohen L, Singh S. Prevalence and burden of multiple sclerosis-related fatigue: A systematic literature review. BMC Neurology. 2021; 21(1):468. [DOI:10.1186/s12883-021-02396-1] [PMID]
- Rizzo M, Hadjimichael O, Preiningerova J, Vollmer T. Prevalence and treatment of spasticity reported by multiple sclerosis patients. Multiple Sclerosis Journal. 2004; 10(5):589-95. [DOI:10.1191/1352458504ms1085oa] [PMID]
- Close J, Vandercappellen J, King M, Hobart J. Measuring fatigue in multiple sclerosis: There may be trouble ahead. Neurology and Therapy. 2023; 12(5):1649-68. [DOI:10.1007/s40120-023-00501-9] [PMID]
- Flachenecker P, Henze T, Zettl U. Spasticity in patients with multiple sclerosis-clinical characteristics, treatment and quality of life. Acta Neurologica Scandinavica. 2014; 129(3):154-62. [DOI:10.1111/ane.12202] [PMID]
- Walton C, King R, Rechtman L, Kaye W, Leray E, Marrie RA, et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS. Multiple Sclerosis Journal. 2020; 26(14):1816-21. [DOI:10.1177/1352458520970841] [PMID]
- Hosseinzadeh A, Baneshi MR, Sedighi B, Kermanchi J, Haghdoost AA. Geographic variations of multiple sclerosis in Iran: A population-based study. Multiple Sclerosis and Related Disorders. 2019; 28:244-9. [DOI:10.1016/j.msard.2019.01.001] [PMID]
- Heesen C, Romberg A, Gold S, Schulz KH. Physical exercise in multiple sclerosis: Supportive care or a putative disease- modifying treatment. Expert Review of Neurotherapeutics. 2006; 6(3):347-55. [DOI:10.1586/14737175.6.3.347] [PMID]
- Edwards T, Pilutti LA. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: A systematic review and future research directions. Multiple sclerosis and Related Disorders. 2017; 16:31-9. [DOI:10.1016/j.msard.2017.06.003] [PMID]
- Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurology. 2017; 17(1):1-11. [DOI:10.1186/s12883-017-0960-9] [PMID]
- Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. The Lancet. 2018; 391(10130):1622-36. [DOI:10.1016/S0140-6736(18)30481-1] [PMID]
- White LJ, Dressendorfer RH. Exercise and multiple sclerosis. Sports Medicine. 2004; 34(15):1077-100. [DOI:10.2165/00007256-200434150-00005] [PMID]
- Tollár J, Nagy F, Tóth BE, Török K, Szita K, Csutorás B, et al. Exercise effects on multiple sclerosis quality of life and clinical-motor symptoms. Medicine and Science in Sports and Exercise. 2020; 52(5):1007-14. [DOI:10.1249/MSS.0000000000002228] [PMID]
- Razazian N, Yavari Z, Farnia V, Azizi A, Kordavani L, Bahmani DS, et al. Exercising impacts on fatigue, depression, and paresthesia in female patients with multiple sclerosis. Medicine and Science in Sports and Exercise. 2016; 48(5):796-803. [DOI:10.1249/MSS.0000000000000834] [PMID]
- Bahmani DS, Razazian N, Farnia V, Alikhani M, Tatari F, Brand S. Compared to an active control condition, in persons with multiple sclerosis two different types of exercise training improved sleep and depression, but not fatigue, paresthesia, and intolerance of uncertainty. Multiple Sclerosis and Related Disorders. 2019; 36:101356. [DOI:10.1016/j.msard.2019.07.032] [PMID]
- Ozkul C, Guclu-Gunduz A, Eldemir K, Apaydin Y, Yazici G, Irkec C. Combined exercise training improves cognitive functions in multiple sclerosis patients with cognitive impairment: A single-blinded randomized controlled trial. Multiple Sclerosis and Related Disorders. 2020; 45:102419. [DOI:10.1016/j.msard.2020.102419] [PMID]
- Nicholson VP, McKean MR, Burkett BJ. Twelve weeks of BodyBalance® training improved balance and functional task performance in middle-aged and older adults. Clinical Interventions in Aging. 2014; 9:1895-904. [DOI:10.2147/CIA.S71769] [PMID]
- Khan RS, Marlow C, Head A. Physiological and psychological responses to a 12-week bodybalance training programme. Journal of Science and Medicine in Sport. 2008; 11(3):299-307. [DOI:10.1016/j.jsams.2007.04.005] [PMID]
- TahmasabiBorojni S, Nazarifar N, MohammadShirazi R. [Improving the happiness of adult women as a result of a body balance training course (Persian)]. Paper presented at: The First National Conference of Developments in Sports Sciences in the Field Of Health, Prevention and Championship. 2016 May 12; Qazvin, Iran. [Link]
- Derewiecki T, Duda M, Majcher P, Chmiel-Derewiecka D. Effect of physiotherapy on body balance and quality of life in women suffering from multiple sclerosis-preliminary results. Hygeia Public Health. 2015; 50(1):203-9. [Link]
- Alanazi SA. Balance ability and postural adjustments in patients with multiple sclerosis [doctoral dissertation]. Coral Gables: University of Miami. [Link]
- Seo DK, Kim JS, Lee DY, Kwon OS, Lee SS, Kim JH. The relationship of abdominal muscles balance and body balance. Journal of Physical Therapy Science. 2013; 25(7):765-7. [DOI:10.1589/jpts.25.765] [PMID]
- Yu C. Analysis of jogging on muscle fatigue and body balance. Revista Brasileira de Medicina do Esporte. 2023; 29:e2022_0746. [DOI:10.1590/1517-8692202329012022_0746]
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology. 1983; 33(11):1444-52. [DOI:10.1212/WNL.33.11.1444] [PMID]
- Kane MJ, Conway ARA, Miura TK, Colflesh GJH. Working memory, attention control, and the N-back task: A question of construct validity. Journal of Experimental Psychology. Learning, Memory, and Cognition. 2007; 33(3):615-22. [DOI:10.1037/0278-7393.33.3.615] [PMID]
- Jacola LM, Willard VW, Ashford JM, Ogg RJ, Scoggins MA, Jones MM, et al. Clinical utility of the N-back task in functional neuroimaging studies of working memory. Journal of Clinical and Experimental Neuropsychology. 2014; 36(8):875-86. [DOI:10.1080/13803395.2014.953039] [PMID]
- Hobart JC, Riazi A, Thompson AJ, Styles IM, Ingram W, Vickery PJ, et al. Getting the measure of spasticity in multiple sclerosis: The multiple sclerosis spasticity scale (MSSS-88). Brain. 2006; 129(Pt 1):224-34. [DOI:10.1093/brain/awh675] [PMID]
- Pappalardo A, Castiglione A, Restivo DA, Calabrese A, Cimino V, Patti F. Pharmacologic management of spasticity in multiple sclerosis. Neurological Sciences. 2006; 27(Suppl 4):s310-5. [DOI:10.1007/s10072-006-0635-2]
- Azad A. [Physical activity guide for multiple sclerosis (Persian)]. Tehran: Mabani Publications; 2022.
- Henze T, von Mackensen S, Lehrieder G, Zettl UK, Pfiffner C, Flachenecker P. Linguistic and psychometric validation of the MSSS-88 questionnaire for patients with multiple sclerosis and spasticity in Germany. Health and Quality of Life Outcomes. 2014; 12:119. [DOI:10.1186/1477-7525-12-119] [PMID]
- Rodic SZ, Knezevic TI, Kisic-Tepavcevic DB, Dackovic JR, Dujmovic I, Pekmezovic TD, et al. Validation of the Serbian version of multiple sclerosis spasticity scale 88 (MSSS-88). Plos One. 2016; 11(1):e0147042. [DOI:10.1371/journal.pone.0147042] [PMID]
- Kiani I, Pouretezad M, Goharpey S, Salehi R, Negahban Siuki H, Majdi Nasab N. [Reliability and validity of the persian version of multiple sclerosis spasticity scale in iranian patients with multiple sclerosis (Persian)]. Jundishapur Scientific Medical Journal. 2017; 16(2):197-208. [DOI:10.22118/jsmj.2017.49250]
- Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale: application to patients with multiple sclerosis and systemic lupus erythematosus. Archives of Neurology. 1989; 46(10):1121-3. [DOI:10.1001/archneur.1989.00520460115022]
- Valko PO, Bassetti CL, Bloch KE, Held U, Baumann CR. Validation of the fatigue severity scale in a Swiss cohort. Sleep. 2008; 31(11):1601-7. [DOI:10.1093/sleep/31.11.1601] [PMID]
- Chen Y, Xu S, Shen J, Yang H, Xu W, Shao M, Pan F. Effect of exercise on fatigue in multiple sclerosis patients: A network meta-analysis. International Journal of Sports Medicine. 2021; 42(14):1250-9. [DOI:10.1055/a-1524-1935] [PMID]
- Monteiro PHM, Marcori AJ, da Conceição NR, Monteiro RLM, Coelho DB, Teixeira LA. Cortical activity in body balance tasks as a function of motor and cognitive demands: A systematic review. European Journal of Neuroscience. 2024; 60(10):6556-87. [DOI:10.1111/ejn.16574] [PMID]
- Abasıyanık Z, Ertekin Ö, Kahraman T, Yigit P, Özakbaş S. The effects of clinical pilates training on walking, balance, fall risk, respiratory, and cognitive functions in persons with multiple sclerosis: A randomized controlled trial. Explore. 2020; 16(1):12-20. [DOI:10.1016/j.explore.2019.07.010] [PMID]
- Velikonja O, Čurić K, Ožura A, Jazbec SŠ. Influence of sports climbing and yoga on spasticity, cognitive function, mood and fatigue in patients with multiple sclerosis. Clinical Neurology and Neurosurgery. 2010; 112(7):597-601. [DOI:10.1016/j.clineuro.2010.03.006] [PMID]
- Scott S. Able bodies balance training. Champaign: Human Kinetics; 2008. [Link]
- Miller NM. ‘Yoga is a way of life’exploring experiences of yoga as a treatment for substance use: An interpretative phenomenological analysis. Counselling and Psychotherapy Research. 2024; 24(4):1689-98. [DOI:10.1002/capr.12817]
- Dobson R, Giovannoni G. Multiple sclerosis-a review. European Journal of Neurology. 2019; 26(1):27-40. [DOI:10.1111/ene.13819] [PMID]
- Zavalishina SY, Karpov VY, Bakulina ED, Rysakova OG, Tagirova ND, Sibgatulina FR. The function of maintaining body balance in students involved in various sports. Journal of Biochemical Technology. 2021; 12(4-2021):94-8. [DOI:10.51847/bnyZig6kjI]
- Moghadasi A, Ghasemi G, Sadeghi-Demneh E, Etemadifar M. The effect of total body resistance exercise on mobility, proprioception, and muscle strength of the knee in people with multiple sclerosis. Journal of Sport Rehabilitation. 2020; 29(2):192-9. [DOI:10.1123/jsr.2018-0303] [PMID]
- Gentile A, Musella A, De Vito F, Rizzo FR, Fresegna D, Bullitta S, et al. Immunomodulatory effects of exercise in experimental multiple sclerosis. Frontiers in Immunology. 2019; 10:2197. [DOI:10.3389/fimmu.2019.02197] [PMID]
- Torres-Costoso A, Martínez-Vizcaíno V, Reina-Gutiérrez S, Álvarez-Bueno C, Guzmán-Pavón MJ, Pozuelo-Carrascosa DP, et al. Effect of exercise on fatigue in multiple sclerosis: A network meta-analysis comparing different types of exercise. Archives of Physical Medicine and Rehabilitation. 2022; 103(5):970-87. [DOI:10.1016/j.apmr.2021.08.008] [PMID]
- Heine M, van de Port I, Rietberg MB, van Wegen EE, Kwakkel G. Exercise therapy for fatigue in multiple sclerosis. The Cochrane Database of Systematic Reviews. 2015; 2015(9):CD009956. [DOI:10.1002/14651858.CD009956.pub2] [PMID]
- Hsieh DT, Warden GI, Butler JM, Nakanishi E, Asano Y. Multiple sclerosis exacerbation associated with high-altitude climbing exposure. Military Medicine. 2020; 185(7-8):e1322-5. [DOI:10.1093/milmed/usz421] [PMID]
Article type: Original Research Articles |
Subject:
Sport rehabilitation
Received: 2025/03/4 | Accepted: 2025/07/1 | Published: 2025/12/9
Received: 2025/03/4 | Accepted: 2025/07/1 | Published: 2025/12/9
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
