
988368
Thu, Jul 23, 2026

Volume 23, Issue 2 (June 2025)
Iranian Rehabilitation Journal 2025, 23(2): 165-174 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abed Laftah S, Kadhim Abdul-Hameed A, Zair Balat K, Malih Radhi M. Barriers and Facilitators in Rehabilitative Nursing Care for Disabilities and Mediating Roles of Nurse-related Factors. Iranian Rehabilitation Journal 2025; 23 (2) :165-174
URL: http://irj.uswr.ac.ir/article-1-2501-en.html
URL: http://irj.uswr.ac.ir/article-1-2501-en.html



1- Department of Community Health Nursing, College of Nursing, University of Thi-Qar, Thi-Qar, Iraq.
2- Department of Adult Nursing, College of Nursing, University of Thi-Qar, Thi-Qar, Iraq.
3- Community Health Nursing, College of Health and Medical Techniques, Kufa/Al-Furat Al-Awsat Technical University, Babylon, Iraq.
2- Department of Adult Nursing, College of Nursing, University of Thi-Qar, Thi-Qar, Iraq.
3- Community Health Nursing, College of Health and Medical Techniques, Kufa/Al-Furat Al-Awsat Technical University, Babylon, Iraq.
Keywords: Rehabilitative nursing care, Disabilities, Barriers, Facilitators, Organizational support, Self-efficacy, Workplace empowerment
Full-Text [PDF 527 kb]
(555 Downloads)
| Abstract (HTML) (3208 Views)
 Introduction
Introduction
Rehabilitative nursing care is crucial for enhancing the functional independence and exceptional lives of people with disabilities [1]. The World Health Organization (WHO) emphasizes the importance of rehabilitation as a critical healthcare issue, especially for individuals with physical, sensory, or cognitive impairments [2]. However, regardless of the growing recognition of its importance, numerous boundaries preclude the powerful implementation of rehabilitative nursing care, restricting patients’ capacity to achieve the most efficient healing outcomes. These barriers range from systemic healthcare barriers to person-nurse-related elements that affect the transport of rehabilitation offerings [3].
The existing literature has recognized multiple systemic and institutional barriers that impede rehabilitative nursing care. For instance, aid constraints, including insufficient staffing, lack of specialized rehabilitation schooling, and inadequate investment, are frequently pronounced as barriers in rehabilitation settings [4]. Furthermore, communication-demanding situations between healthcare professionals and patients with disabilities can negatively impact the affected person’s engagement and adherence to rehabilitative interventions [5]. These barriers are exacerbated by social determinants of health, including socioeconomic status, geographical location, and healthcare accessibility, which similarly affect the exceptional rehabilitation services acquired by individuals with disabilities [6].
In addition to systemic boundaries, nurse-associated elements play a pivotal role in the effectiveness of rehabilitative nursing care. Studies have proven that nurses’ attitudes, knowledge, and competencies appreciably affect the best rehabilitation services provided to patients with disabilities [7]. For example, nurses with a positive attitude toward incapacity and rehabilitation are likelier to implement patient-targeted care strategies and suggest complete rehabilitative interventions [8]. On the contrary, a lack of self-assurance or insufficient education in rehabilitative strategies can also cause suboptimal care transport and decreased affected person outcomes [9]. Furthermore, nurse-related elements, including job satisfaction, workload, and emotional resilience, also affect their capacity to provide effective rehabilitative care [10].
Facilitators of rehabilitative nursing care have also been extensively documented, with research emphasizing the significance of interdisciplinary collaboration, continuous expert development, and supportive healthcare regulations [11]. For instance, interdisciplinary teamwork among nurses, bodily therapists, occupational therapists, and physicians has improved rehabilitation results by ensuring holistic and coordinated care of clients with disabilities [1]. Moreover, ongoing schooling and education applications tailored to rehabilitative nursing can improve nurses’ abilities, increase self-assurance, and improve patient outcomes [12]. Additionally, healthcare policies that prioritizing rehabilitation services and allocating adequate resources to rehabilitation units can significantly enhance rehabilitative care delivery [1].
Given the interplay among systemic barriers, facilitators, and nurse-related factors in rehabilitative nursing care, comprehensive research is needed. This study aimed to investigate the barriers and facilitators of rehabilitative nursing care and nurse-related factors, including self-efficacy, organizational aid, and job empowerment, in influencing care results.
Materials and Methods
Study design and sitting
This study utilized a cross-sectional, descriptive-correlational design to investigate the barriers and facilitators of rehabilitative nursing care for clients with disabilities and the mediating roles of nurse-associated elements. The studies were conducted at the Babylon Center for the Rehabilitation of disabled persons in Babylon Governorate, Iraq, between November 3, 2024, and March 15, 2025. The center was chosen due to its pivotal function in providing rehabilitative services to a diverse population of clients with disabilities.
Study sample
A stratified random sampling method was used to select members among the nurses and rehabilitation care beneficiaries. The center receives approximately 2052 registered visitors monthly, so a representative pattern was determined using Cochrane measures for the expected population. With a confidence level of 90% and a margin of error of 0.5, the survey included 385 participants. The sample included 192 nurses providing rehabilitation care and 193 patients receiving services. The inclusion criteria for nurses required at least six months of experience in rehabilitation nursing. At the same time, patients must be 18 years or older and have received rehabilitation care for at least one month.
Cochran’s method supports calculating the pattern length required to ensure the effects are statistically significant, with a 95% confidence level and a 0.5 margin of error. After calculating the system’s use, a sample size of 385 contributors (192 nurses and 193 clients) was determined. This sample size guarantees that the findings concerning barriers and facilitators in rehabilitative nursing care are strong and representative of the population at the Babylon Center for Rehabilitation of the Disabled.
Study instruments
Barriers and facilitators in rehabilitation nursing care
Three demonstrated instruments were applied to examine the barriers and facilitators of rehabilitation nursing care for individuals with disabilities. The barriers to providing patient-centered rehabilitation care scale (BPRCS) is a tool designed to evaluate the boundaries that healthcare carriers, especially rehabilitation nurses, face in delivering patient-centered care. This scale has been widely used in healthcare settings. It demonstrates sturdy reliability, with a Cronbach’s α of 0.87 [13] and an intraclass correlation coefficient (ICC) of 0.85, indicating excellent stability in evaluating barriers to patient-centered rehabilitation care. The facilitators and barriers scale measures elements that beautify care transport, including support systems, teamwork, and useful resource availability. This tool has been confirmed in previous studies, displaying true internal consistency (Cronbach’s α=0.91) [14]. This scale showed excellent reliability in the Arabic version, with an ICC of 0.89, confirming consistent measurements of facilitators and barriers in the nursing care environment. Additionally, the perceived organizational support (POS) scale was administered to evaluate the extent to which nurses experienced support from their establishments. The POS has been considerably demonstrated, with a Cronbach’s α of 0.88, and is a dependable degree of organizational support in healthcare settings [15]. The Arabic modification of the POS scale achieved an ICC of 0.86, reflecting high reliability in measuring POS among nurses.
Nurse-related factors (mediator variables)
Four scales were employed to explore the mediating roles of nurse-associated elements. The nurse self-efficacy for rehabilitation care (NSERC) scale was used to measure nurses’ self-belief in providing rehabilitation care. This scale has established strong reliability, with a Cronbach’s α of 0.89, and has been tested in numerous nursing populations [16]. The NSERC Arabic scale demonstrated an ICC of 0.88, demonstrating strong agreement in responses across repeated administrations and confirming its reliability for measuring nurse self-efficacy. The professional quality of life (ProQOL) scale assessed three key dimensions: Burnout, compassion, pleasure, and secondary disturbing pressure. The ProQOL is a properly mounted device with a Cronbach’s α ranging from 0.75 to 0.88 throughout its subscales [5]. The Arabic version of the ProQOL scale showed acceptable to excellent test re-test reliability, with ICC values ranging from 0.78 to 0.87 across the burnout, compassion satisfaction, and secondary psychological distress subscales. The nursing attitudes towards disability (NATD) scale assesses nurses’ attitudes towards individuals with disabilities. This scale has proven true reliability, with a Cronbach’s α of 0.85, and has been used in multiple studies to evaluate disability-associated attitudes among healthcare experts [17]. The Arabic NATD scale demonstrated an ICC of 0.83, consistently capturing nurses’ attitudes toward individuals with disabilities. Finally, the workplace empowerment scale (WES) was employed to assess nurses’ perceptions of empowerment in decision-making and resources access. The WES has been proven in nursing populations, with a Cronbach’s α of 0.82, indicating excellent reliability [18]. The Arabic version of the women’s WES showed an ICC of 0.81, supporting its reliability in assessing perceptions of workplace empowerment among rehabilitation nurses.
Validity and reliability
All measures used in this study were subjected to cultural modeling and linguistic translation to ensure the importance and suitability of monitoring devices in the Iraqi healthcare context. Most original instruments, including BPRCS, POS, and NATD scales, were originally developed in English. They were translated into Arabic using a standard forward and back translation system by bilingual professionals familiar with healthcare terminology and the Iraqi cultural context. The translated versions were then reviewed and improved by a committee of five rehabilitation nursing and health research specialists to ensure content equivalence, cultural relevance, and conceptual clarity. Where Arabic versions were already available and tested, they were used with minor modifications based on expert feedback. The pilot study, which involved 30 participants, demonstrated the readability and relevance of the translated instruments. These steps ensured the linguistic validity and cultural appropriateness of the tools used to assess barriers, facilitators, and nurse-related factors in the context of Iraq’s rehabilitative nursing care. Therefore, the tools were administered in Arabic to facilitate the experience and correct responses among the participants, most of whom were Arabic speakers.
Data collection
Data were collected using self-administered questionnaires for nurses and interviewer-supported surveys for clients to assess literacy boundaries. Participants were approached during their routine visits to the rehabilitation center, and written informed consent was obtained before participation. The study lasted three months, from December 1, 2024, to February 26, 2025.
Data evaluation
Data were analyzed using SPSS software, version 27. Descriptive records, including Mean±SD, were used to summarize the demographic and examine the variables. Pearson’s correlation coefficient was used to examine the relationships among barriers, facilitators, and nurse-associated factors. Structural equation modeling (SEM) was used to check the mediating position of nurse-associated elements within the relationship among barriers, facilitators, and rehabilitative nursing care consequences. Statistical significance was set at a P<0.05.
Results
Table 1 presents the socio-demographic traits of the nurses and clients involved in the study. The implied age of nurses (Mean±SD) was 34.6±7.5 years, while the Mean±SD age of clients was 42.3±11.2 years. The nurses have a Mean±SD of 24.3±8.9 months of experience in rehabilitation. Key scales were also supplied, together with BPRCS, which had a Mean±SD of 3.85±0.68, and facilitators of care, with a Mean±SD of 4.12±0.75. Additionally, they assessed POS, NSERC, professional first-class of life (ProQOL), NATD, and administrative center empowerment WES, with scores ranging from 3.45 to 4.20, indicating diverse ranges of perception and involvement in these elements of nursing practice.
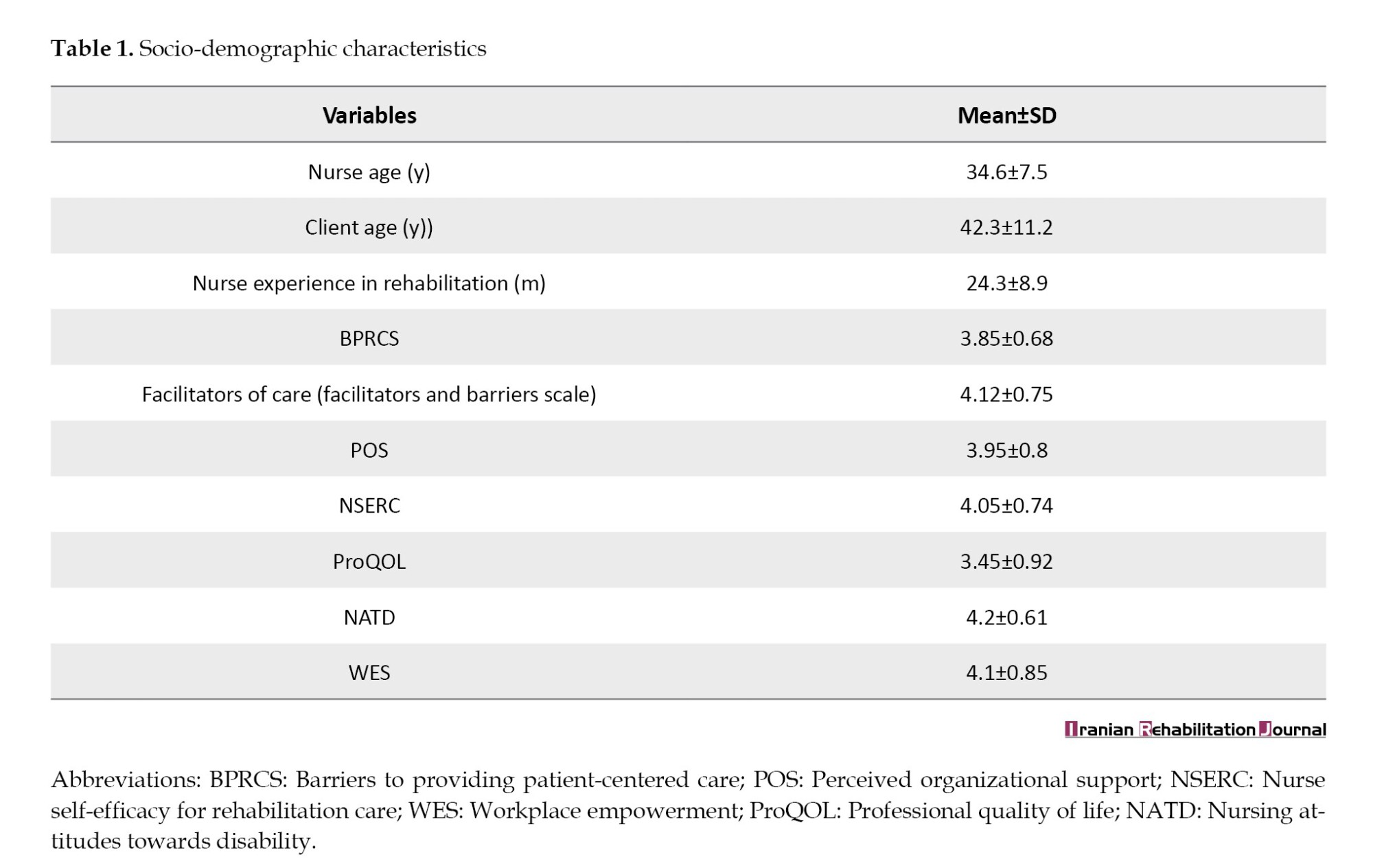
Table 2 presents the correlation analysis between barriers, facilitators, and nurse-related factors. Complete negative correlations were observed between BPRCS and each facilitator (-0.60), and numerous nurse-associated factors, including POS (-0.45), NSERC (0.53), ProQOL (-0.33), NATD (-0.40), and WES (-0.42). Conversely, facilitators displayed fine correlations with these equal factors, such as a sturdy advantageous correlation with POS (0.55) and NSERC (0.47). These correlations confirm that as facilitators increase, the positive factors associated with the nurse also improve, while barriers tend to negatively impact these factors.
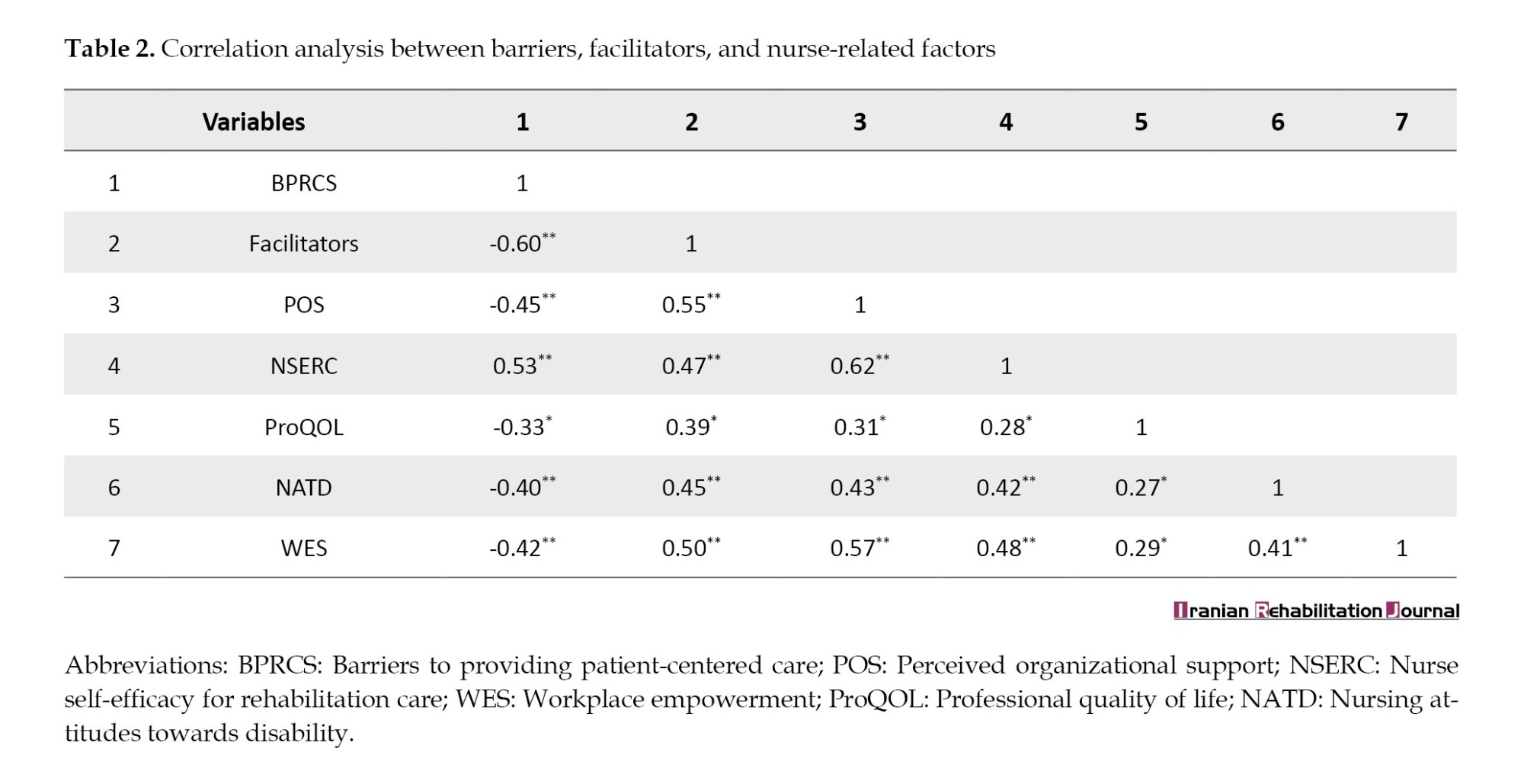
Table 3 presents the SEM path evaluation results, including course coefficients and significance values. The analysis revealed that barriers significantly negatively impacted rehabilitative care outcomes, with a route coefficient of -0.45 (P<0.01), which means that barriers strongly restricted care outcomes. In assessment, facilitators greatly impact care results (coefficient=0.60, P<0.01). NSERC (coefficient=0.35, P=0.02) and POS (coefficient=0.42, P<0.01) positively influenced rehabilitative care consequences. The mediator impact of nurse-related factors was sizeable, with a coefficient of 0.38 (P<0.01), indicating that these factors were key in mediating the relationship between barriers/facilitators and care consequences.
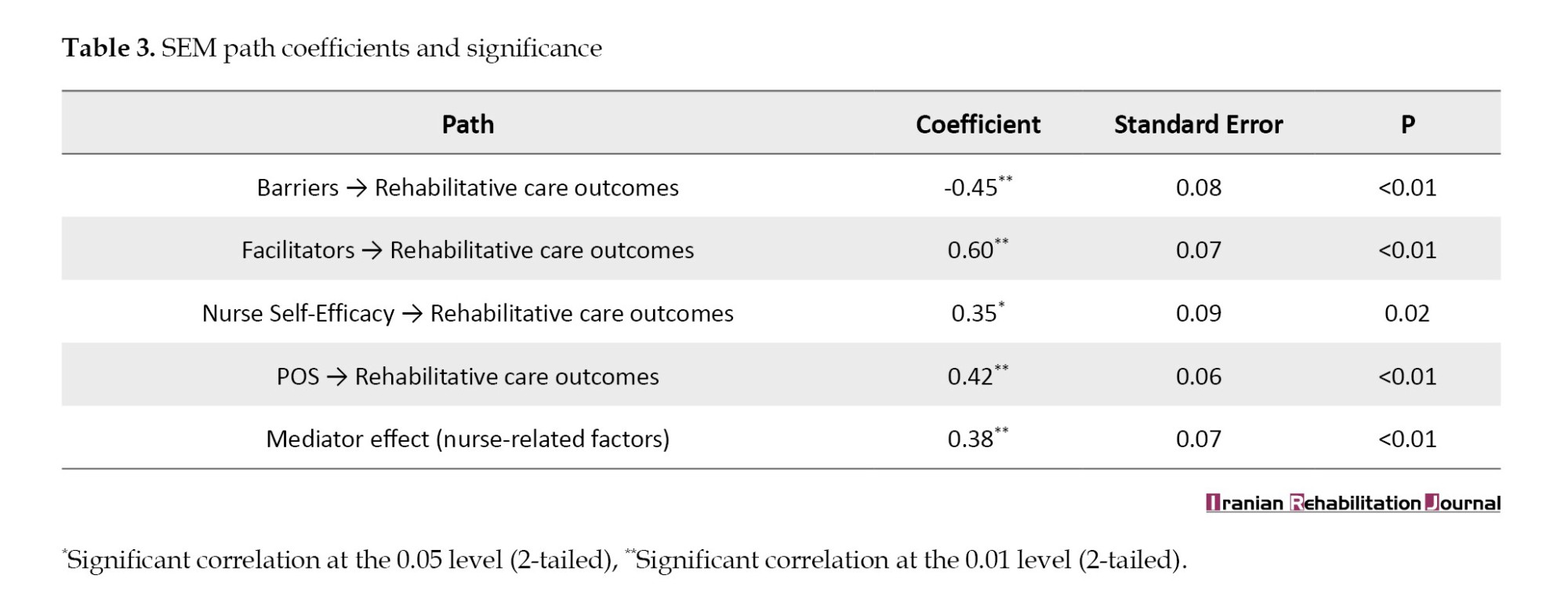
Table 4 presents the bootstrapped self-assurance periods for the mediation analysis, which examines the oblique outcomes of nurse-associated elements (self-efficacy and organizational support) within the relationship between obstacles/facilitators and rehabilitative care outcomes. The route from boundaries to effects, mediated by nurse-associated factors, indicates a considerable terrible effect (-0.13), with the 95% self-belief confidence interval from -0.25 to -0.03 and a P of 0.02, indicating a statistically significant indirect impact. Conversely, the path from facilitators to outcomes, mediated with the aid of the identical elements, demonstrated a considerable impact (0.18), with the confidence interval programming language between 0.10 and 0.30 and a P much less than 0.01, confirming a strong indirect effect. Additionally, the mediator’s direct effect on effects was vast (0.35), with a confidence interval ranging between 0.22 and 0.50, providing strong evidence of the mediating role of nurse-related elements in improving care effects. This mediation analysis reinforces the importance of nurse-related factors in influencing rehabilitative care outcomes and highlights their important position in the limitations and facilitators frameworks.
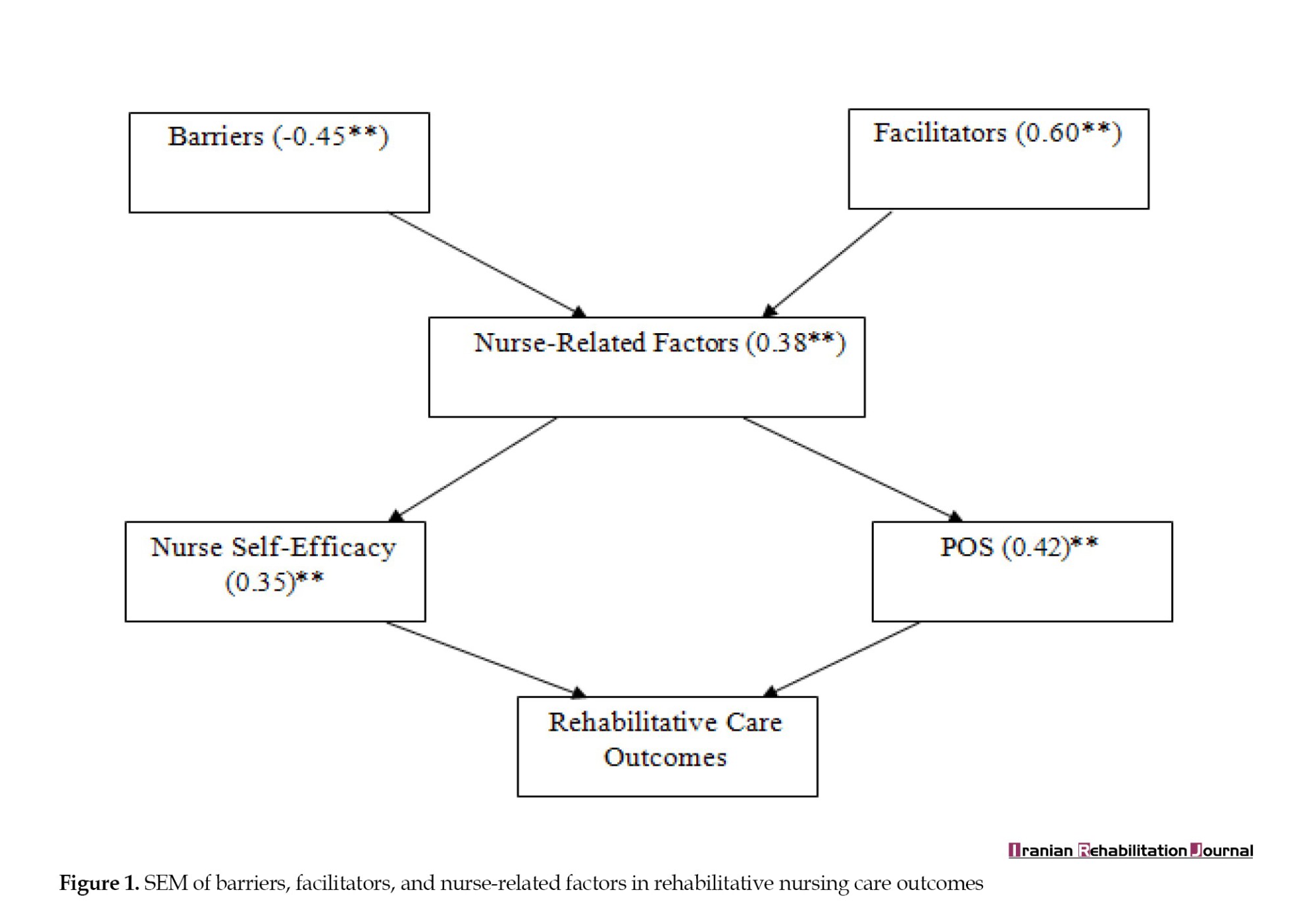
The SEM route model illustrates the relationships between barriers, facilitators, and rehabilitative care outcomes, incorporating nurse-related elements as mediators. Barriers negatively impacted the effects of rehabilitative care (β=-0.45, P<0.01), while facilitators had a robust and significant effect (β=0.60, P<0.01). Nurse-related factors, including nurse self-efficacy (β=0.35, P=0.02) and POS (β=0.42, P<0.01), affect rehabilitative care outcomes. These nurse-associated elements mediate the relationship (β=0.38, P<0.01), emphasizing their vital function in enhancing rehabilitative nursing care. Figure 1 underscores the significance of decreasing barriers, strengthening facilitators, and supporting nurses to improve outcomes for affected individuals.
Discussion
The results of this study highlight the critical role of each barrier and facilitator in rehabilitative nursing care for clients with disabilities, while emphasizing the mediating impact of nurse-related elements. The socio-demographic characteristics show that the nurses in the study had an average of 24.3 months of rehabilitation experience, suggesting personnel with moderate exposure to rehabilitative care. This enjoyment stage is applicable, as previous studies have implied that expert exposure and experience significantly affect nurses’ ability to provide good rehabilitative care [19-21].
The correlation analysis showed that boundaries to affected person-targeted care (BPRCS) were negatively related to facilitators (-0.6) and numerous nurse-associated factors, along with POS (-0.45) and administrative center empowerment (-0.42). These results align with earlier research indicating that institutional and systemic barriers, including a lack of resources and administrative guidance, obstruct the capacity of nurses to provide the best care [22]. Furthermore, the negative correlation between BPRCS and professional quality of existence (-0.33) indicates that nurses with more boundaries experience decreased activity pride and better ranges of burnout, consistent with earlier studies highlighting the emotional toll of rehabilitative nursing [23].
Conversely, facilitators showed robust positive correlations with nurse-related factors, POS (0.55), and nurse self-efficacy (0.47). This indicates that supportive work environments, adequate training, and empowerment techniques enhance the nurses’ ability to provide powerful care. Prior literature confirms that nurses who perceive better organizational support are likelier to interact in proactive patient care, demonstrate resilience, and preserve long-term commitment to rehabilitation [24]. Additionally, the superb correlation between facilitators and nursing attitudes closer to incapacity (0.45) shows that supportive environments contribute to extra-inclusive, patient-centered care.
The SEM results enhance these findings by demonstrating that boundaries significantly preclude rehabilitative care effects (-0.45, P<0.01), while facilitators positively contribute to stepped-forward results (0.60, P<0.01). Nurse self-efficacy (0.35, P=0.02) and perceived organizational aid (0.42, P<0.01) positively influenced care results, supporting previous studies that emphasize the importance of confidence and institutional support in enhancing nursing performance [25]. The mediating impact of nurse-related factors (0.38, P<0.01) confirms that these variables function as essential mechanisms through which barriers and facilitators impact rehabilitative care.
Social cognitive theory (SCT), based on Bandura (1986), which emphasizes the interaction between personal, environmental, and behavioral elements in influencing human actions is an appropriate theoretical framework for this SEM scheme. Social cognitive theory (SCT) is especially applicable as it highlights the role of self-efficacy, a key mediating issue in the version, in which nurses’ self-belief in their capability to offer rehabilitative care substantially influences patient outcomes [26]. The theory also aligns with the effect of POS, as environmental factors, such as workplace resources and institutional backing, affect nurses’ behaviors and overall performance in delivering care.
Research supports that self-efficacy and organizational support improve healthcare vendors’ performance and patient results. For instance, Cherniss discusses the function of self-efficacy in expert settings [27], while Rubel et al. emphasize how POS fosters dedication and overall performance in healthcare [28]. This theoretical foundation justifies the mediating roles within the SEM model and provides a lens to improve rehabilitative nursing care.
These results have vast implications for healthcare policymakers. Addressing boundaries that include inadequate resources, schooling, and organizational constraints may enhance the effects of rehabilitative care [29, 30]. Simultaneously, improving facilitators, such as business empowerment, professional development, and psychological support, may also optimize nursing performance and affect personal consequences. Future studies should explore intervention techniques to strengthen facilitators while mitigating barriers to enhance the overall effectiveness of rehabilitative nursing care.
Conclusion
This study highlighted the main barriers and influencing factors in the rehabilitative nursing care of patients with disabilities, where nurse-related elements were mediating. The results showed that barriers negatively impacted care outcomes, while facilitating factors, such as organizational support, self-efficacy, and workplace empowerment, significantly improved nursing performance. Nurse-related factors, such as attitudes toward disability and professional well-being, strengthened these relationships, emphasizing their importance in improving care delivery. To improve rehabilitative nursing care, healthcare organizations should strengthen organizational support, provide focused education to improve nurses’ self-efficacy, and implement rules that promote empowerment and positive attitudes toward disability care.
Study limitation
Despite the valuable insights provided by this study, numerous barriers must be acknowledged. The cross-sectional design restricts the capacity to deduce causal relationships among boundaries, facilitators, and rehabilitative care outcomes. Additionally, data collection relied on self-reported measures, which may have introduced response bias. Even though adequate, the sample length may restrict generalizability to broader healthcare settings. Future studies should be longitudinal to establish causal pathways and contain objective measures of rehabilitative care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Kufa/Al-Furat Al-Awsat Technical University, Babylon, Iraq (Code: 2214, Dated: 5/10/2024).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Developing, supervising the concepts and data analysis: Mohammed Malih Radhi; Data collection, Investigating and writing the original draft: Salwan Abed Laftah and Kefah Zair Balat; Review and editing: Salwan Abed Laftah, Alaa Kadhim Abdul-Hameed, and Kefah Zair Balat.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The Health Authority of Babylon/Babylon Rehabilitation Center for Disabled, Iraq, approved all experimental protocols, and all permitted guidelines were adhered to during the data collection.
References
Full-Text: (364 Views)
IntroductionRehabilitative nursing care is crucial for enhancing the functional independence and exceptional lives of people with disabilities [1]. The World Health Organization (WHO) emphasizes the importance of rehabilitation as a critical healthcare issue, especially for individuals with physical, sensory, or cognitive impairments [2]. However, regardless of the growing recognition of its importance, numerous boundaries preclude the powerful implementation of rehabilitative nursing care, restricting patients’ capacity to achieve the most efficient healing outcomes. These barriers range from systemic healthcare barriers to person-nurse-related elements that affect the transport of rehabilitation offerings [3].
The existing literature has recognized multiple systemic and institutional barriers that impede rehabilitative nursing care. For instance, aid constraints, including insufficient staffing, lack of specialized rehabilitation schooling, and inadequate investment, are frequently pronounced as barriers in rehabilitation settings [4]. Furthermore, communication-demanding situations between healthcare professionals and patients with disabilities can negatively impact the affected person’s engagement and adherence to rehabilitative interventions [5]. These barriers are exacerbated by social determinants of health, including socioeconomic status, geographical location, and healthcare accessibility, which similarly affect the exceptional rehabilitation services acquired by individuals with disabilities [6].
In addition to systemic boundaries, nurse-associated elements play a pivotal role in the effectiveness of rehabilitative nursing care. Studies have proven that nurses’ attitudes, knowledge, and competencies appreciably affect the best rehabilitation services provided to patients with disabilities [7]. For example, nurses with a positive attitude toward incapacity and rehabilitation are likelier to implement patient-targeted care strategies and suggest complete rehabilitative interventions [8]. On the contrary, a lack of self-assurance or insufficient education in rehabilitative strategies can also cause suboptimal care transport and decreased affected person outcomes [9]. Furthermore, nurse-related elements, including job satisfaction, workload, and emotional resilience, also affect their capacity to provide effective rehabilitative care [10].
Facilitators of rehabilitative nursing care have also been extensively documented, with research emphasizing the significance of interdisciplinary collaboration, continuous expert development, and supportive healthcare regulations [11]. For instance, interdisciplinary teamwork among nurses, bodily therapists, occupational therapists, and physicians has improved rehabilitation results by ensuring holistic and coordinated care of clients with disabilities [1]. Moreover, ongoing schooling and education applications tailored to rehabilitative nursing can improve nurses’ abilities, increase self-assurance, and improve patient outcomes [12]. Additionally, healthcare policies that prioritizing rehabilitation services and allocating adequate resources to rehabilitation units can significantly enhance rehabilitative care delivery [1].
Given the interplay among systemic barriers, facilitators, and nurse-related factors in rehabilitative nursing care, comprehensive research is needed. This study aimed to investigate the barriers and facilitators of rehabilitative nursing care and nurse-related factors, including self-efficacy, organizational aid, and job empowerment, in influencing care results.
Materials and Methods
Study design and sitting
This study utilized a cross-sectional, descriptive-correlational design to investigate the barriers and facilitators of rehabilitative nursing care for clients with disabilities and the mediating roles of nurse-associated elements. The studies were conducted at the Babylon Center for the Rehabilitation of disabled persons in Babylon Governorate, Iraq, between November 3, 2024, and March 15, 2025. The center was chosen due to its pivotal function in providing rehabilitative services to a diverse population of clients with disabilities.
Study sample
A stratified random sampling method was used to select members among the nurses and rehabilitation care beneficiaries. The center receives approximately 2052 registered visitors monthly, so a representative pattern was determined using Cochrane measures for the expected population. With a confidence level of 90% and a margin of error of 0.5, the survey included 385 participants. The sample included 192 nurses providing rehabilitation care and 193 patients receiving services. The inclusion criteria for nurses required at least six months of experience in rehabilitation nursing. At the same time, patients must be 18 years or older and have received rehabilitation care for at least one month.
Cochran’s method supports calculating the pattern length required to ensure the effects are statistically significant, with a 95% confidence level and a 0.5 margin of error. After calculating the system’s use, a sample size of 385 contributors (192 nurses and 193 clients) was determined. This sample size guarantees that the findings concerning barriers and facilitators in rehabilitative nursing care are strong and representative of the population at the Babylon Center for Rehabilitation of the Disabled.
Study instruments
Barriers and facilitators in rehabilitation nursing care
Three demonstrated instruments were applied to examine the barriers and facilitators of rehabilitation nursing care for individuals with disabilities. The barriers to providing patient-centered rehabilitation care scale (BPRCS) is a tool designed to evaluate the boundaries that healthcare carriers, especially rehabilitation nurses, face in delivering patient-centered care. This scale has been widely used in healthcare settings. It demonstrates sturdy reliability, with a Cronbach’s α of 0.87 [13] and an intraclass correlation coefficient (ICC) of 0.85, indicating excellent stability in evaluating barriers to patient-centered rehabilitation care. The facilitators and barriers scale measures elements that beautify care transport, including support systems, teamwork, and useful resource availability. This tool has been confirmed in previous studies, displaying true internal consistency (Cronbach’s α=0.91) [14]. This scale showed excellent reliability in the Arabic version, with an ICC of 0.89, confirming consistent measurements of facilitators and barriers in the nursing care environment. Additionally, the perceived organizational support (POS) scale was administered to evaluate the extent to which nurses experienced support from their establishments. The POS has been considerably demonstrated, with a Cronbach’s α of 0.88, and is a dependable degree of organizational support in healthcare settings [15]. The Arabic modification of the POS scale achieved an ICC of 0.86, reflecting high reliability in measuring POS among nurses.
Nurse-related factors (mediator variables)
Four scales were employed to explore the mediating roles of nurse-associated elements. The nurse self-efficacy for rehabilitation care (NSERC) scale was used to measure nurses’ self-belief in providing rehabilitation care. This scale has established strong reliability, with a Cronbach’s α of 0.89, and has been tested in numerous nursing populations [16]. The NSERC Arabic scale demonstrated an ICC of 0.88, demonstrating strong agreement in responses across repeated administrations and confirming its reliability for measuring nurse self-efficacy. The professional quality of life (ProQOL) scale assessed three key dimensions: Burnout, compassion, pleasure, and secondary disturbing pressure. The ProQOL is a properly mounted device with a Cronbach’s α ranging from 0.75 to 0.88 throughout its subscales [5]. The Arabic version of the ProQOL scale showed acceptable to excellent test re-test reliability, with ICC values ranging from 0.78 to 0.87 across the burnout, compassion satisfaction, and secondary psychological distress subscales. The nursing attitudes towards disability (NATD) scale assesses nurses’ attitudes towards individuals with disabilities. This scale has proven true reliability, with a Cronbach’s α of 0.85, and has been used in multiple studies to evaluate disability-associated attitudes among healthcare experts [17]. The Arabic NATD scale demonstrated an ICC of 0.83, consistently capturing nurses’ attitudes toward individuals with disabilities. Finally, the workplace empowerment scale (WES) was employed to assess nurses’ perceptions of empowerment in decision-making and resources access. The WES has been proven in nursing populations, with a Cronbach’s α of 0.82, indicating excellent reliability [18]. The Arabic version of the women’s WES showed an ICC of 0.81, supporting its reliability in assessing perceptions of workplace empowerment among rehabilitation nurses.
Validity and reliability
All measures used in this study were subjected to cultural modeling and linguistic translation to ensure the importance and suitability of monitoring devices in the Iraqi healthcare context. Most original instruments, including BPRCS, POS, and NATD scales, were originally developed in English. They were translated into Arabic using a standard forward and back translation system by bilingual professionals familiar with healthcare terminology and the Iraqi cultural context. The translated versions were then reviewed and improved by a committee of five rehabilitation nursing and health research specialists to ensure content equivalence, cultural relevance, and conceptual clarity. Where Arabic versions were already available and tested, they were used with minor modifications based on expert feedback. The pilot study, which involved 30 participants, demonstrated the readability and relevance of the translated instruments. These steps ensured the linguistic validity and cultural appropriateness of the tools used to assess barriers, facilitators, and nurse-related factors in the context of Iraq’s rehabilitative nursing care. Therefore, the tools were administered in Arabic to facilitate the experience and correct responses among the participants, most of whom were Arabic speakers.
Data collection
Data were collected using self-administered questionnaires for nurses and interviewer-supported surveys for clients to assess literacy boundaries. Participants were approached during their routine visits to the rehabilitation center, and written informed consent was obtained before participation. The study lasted three months, from December 1, 2024, to February 26, 2025.
Data evaluation
Data were analyzed using SPSS software, version 27. Descriptive records, including Mean±SD, were used to summarize the demographic and examine the variables. Pearson’s correlation coefficient was used to examine the relationships among barriers, facilitators, and nurse-associated factors. Structural equation modeling (SEM) was used to check the mediating position of nurse-associated elements within the relationship among barriers, facilitators, and rehabilitative nursing care consequences. Statistical significance was set at a P<0.05.
Results
Table 1 presents the socio-demographic traits of the nurses and clients involved in the study. The implied age of nurses (Mean±SD) was 34.6±7.5 years, while the Mean±SD age of clients was 42.3±11.2 years. The nurses have a Mean±SD of 24.3±8.9 months of experience in rehabilitation. Key scales were also supplied, together with BPRCS, which had a Mean±SD of 3.85±0.68, and facilitators of care, with a Mean±SD of 4.12±0.75. Additionally, they assessed POS, NSERC, professional first-class of life (ProQOL), NATD, and administrative center empowerment WES, with scores ranging from 3.45 to 4.20, indicating diverse ranges of perception and involvement in these elements of nursing practice.
Table 2 presents the correlation analysis between barriers, facilitators, and nurse-related factors. Complete negative correlations were observed between BPRCS and each facilitator (-0.60), and numerous nurse-associated factors, including POS (-0.45), NSERC (0.53), ProQOL (-0.33), NATD (-0.40), and WES (-0.42). Conversely, facilitators displayed fine correlations with these equal factors, such as a sturdy advantageous correlation with POS (0.55) and NSERC (0.47). These correlations confirm that as facilitators increase, the positive factors associated with the nurse also improve, while barriers tend to negatively impact these factors.
Table 3 presents the SEM path evaluation results, including course coefficients and significance values. The analysis revealed that barriers significantly negatively impacted rehabilitative care outcomes, with a route coefficient of -0.45 (P<0.01), which means that barriers strongly restricted care outcomes. In assessment, facilitators greatly impact care results (coefficient=0.60, P<0.01). NSERC (coefficient=0.35, P=0.02) and POS (coefficient=0.42, P<0.01) positively influenced rehabilitative care consequences. The mediator impact of nurse-related factors was sizeable, with a coefficient of 0.38 (P<0.01), indicating that these factors were key in mediating the relationship between barriers/facilitators and care consequences.
Table 4 presents the bootstrapped self-assurance periods for the mediation analysis, which examines the oblique outcomes of nurse-associated elements (self-efficacy and organizational support) within the relationship between obstacles/facilitators and rehabilitative care outcomes. The route from boundaries to effects, mediated by nurse-associated factors, indicates a considerable terrible effect (-0.13), with the 95% self-belief confidence interval from -0.25 to -0.03 and a P of 0.02, indicating a statistically significant indirect impact. Conversely, the path from facilitators to outcomes, mediated with the aid of the identical elements, demonstrated a considerable impact (0.18), with the confidence interval programming language between 0.10 and 0.30 and a P much less than 0.01, confirming a strong indirect effect. Additionally, the mediator’s direct effect on effects was vast (0.35), with a confidence interval ranging between 0.22 and 0.50, providing strong evidence of the mediating role of nurse-related elements in improving care effects. This mediation analysis reinforces the importance of nurse-related factors in influencing rehabilitative care outcomes and highlights their important position in the limitations and facilitators frameworks.
The SEM route model illustrates the relationships between barriers, facilitators, and rehabilitative care outcomes, incorporating nurse-related elements as mediators. Barriers negatively impacted the effects of rehabilitative care (β=-0.45, P<0.01), while facilitators had a robust and significant effect (β=0.60, P<0.01). Nurse-related factors, including nurse self-efficacy (β=0.35, P=0.02) and POS (β=0.42, P<0.01), affect rehabilitative care outcomes. These nurse-associated elements mediate the relationship (β=0.38, P<0.01), emphasizing their vital function in enhancing rehabilitative nursing care. Figure 1 underscores the significance of decreasing barriers, strengthening facilitators, and supporting nurses to improve outcomes for affected individuals.
Discussion
The results of this study highlight the critical role of each barrier and facilitator in rehabilitative nursing care for clients with disabilities, while emphasizing the mediating impact of nurse-related elements. The socio-demographic characteristics show that the nurses in the study had an average of 24.3 months of rehabilitation experience, suggesting personnel with moderate exposure to rehabilitative care. This enjoyment stage is applicable, as previous studies have implied that expert exposure and experience significantly affect nurses’ ability to provide good rehabilitative care [19-21].
The correlation analysis showed that boundaries to affected person-targeted care (BPRCS) were negatively related to facilitators (-0.6) and numerous nurse-associated factors, along with POS (-0.45) and administrative center empowerment (-0.42). These results align with earlier research indicating that institutional and systemic barriers, including a lack of resources and administrative guidance, obstruct the capacity of nurses to provide the best care [22]. Furthermore, the negative correlation between BPRCS and professional quality of existence (-0.33) indicates that nurses with more boundaries experience decreased activity pride and better ranges of burnout, consistent with earlier studies highlighting the emotional toll of rehabilitative nursing [23].
Conversely, facilitators showed robust positive correlations with nurse-related factors, POS (0.55), and nurse self-efficacy (0.47). This indicates that supportive work environments, adequate training, and empowerment techniques enhance the nurses’ ability to provide powerful care. Prior literature confirms that nurses who perceive better organizational support are likelier to interact in proactive patient care, demonstrate resilience, and preserve long-term commitment to rehabilitation [24]. Additionally, the superb correlation between facilitators and nursing attitudes closer to incapacity (0.45) shows that supportive environments contribute to extra-inclusive, patient-centered care.
The SEM results enhance these findings by demonstrating that boundaries significantly preclude rehabilitative care effects (-0.45, P<0.01), while facilitators positively contribute to stepped-forward results (0.60, P<0.01). Nurse self-efficacy (0.35, P=0.02) and perceived organizational aid (0.42, P<0.01) positively influenced care results, supporting previous studies that emphasize the importance of confidence and institutional support in enhancing nursing performance [25]. The mediating impact of nurse-related factors (0.38, P<0.01) confirms that these variables function as essential mechanisms through which barriers and facilitators impact rehabilitative care.
Social cognitive theory (SCT), based on Bandura (1986), which emphasizes the interaction between personal, environmental, and behavioral elements in influencing human actions is an appropriate theoretical framework for this SEM scheme. Social cognitive theory (SCT) is especially applicable as it highlights the role of self-efficacy, a key mediating issue in the version, in which nurses’ self-belief in their capability to offer rehabilitative care substantially influences patient outcomes [26]. The theory also aligns with the effect of POS, as environmental factors, such as workplace resources and institutional backing, affect nurses’ behaviors and overall performance in delivering care.
Research supports that self-efficacy and organizational support improve healthcare vendors’ performance and patient results. For instance, Cherniss discusses the function of self-efficacy in expert settings [27], while Rubel et al. emphasize how POS fosters dedication and overall performance in healthcare [28]. This theoretical foundation justifies the mediating roles within the SEM model and provides a lens to improve rehabilitative nursing care.
These results have vast implications for healthcare policymakers. Addressing boundaries that include inadequate resources, schooling, and organizational constraints may enhance the effects of rehabilitative care [29, 30]. Simultaneously, improving facilitators, such as business empowerment, professional development, and psychological support, may also optimize nursing performance and affect personal consequences. Future studies should explore intervention techniques to strengthen facilitators while mitigating barriers to enhance the overall effectiveness of rehabilitative nursing care.
Conclusion
This study highlighted the main barriers and influencing factors in the rehabilitative nursing care of patients with disabilities, where nurse-related elements were mediating. The results showed that barriers negatively impacted care outcomes, while facilitating factors, such as organizational support, self-efficacy, and workplace empowerment, significantly improved nursing performance. Nurse-related factors, such as attitudes toward disability and professional well-being, strengthened these relationships, emphasizing their importance in improving care delivery. To improve rehabilitative nursing care, healthcare organizations should strengthen organizational support, provide focused education to improve nurses’ self-efficacy, and implement rules that promote empowerment and positive attitudes toward disability care.
Study limitation
Despite the valuable insights provided by this study, numerous barriers must be acknowledged. The cross-sectional design restricts the capacity to deduce causal relationships among boundaries, facilitators, and rehabilitative care outcomes. Additionally, data collection relied on self-reported measures, which may have introduced response bias. Even though adequate, the sample length may restrict generalizability to broader healthcare settings. Future studies should be longitudinal to establish causal pathways and contain objective measures of rehabilitative care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Kufa/Al-Furat Al-Awsat Technical University, Babylon, Iraq (Code: 2214, Dated: 5/10/2024).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Developing, supervising the concepts and data analysis: Mohammed Malih Radhi; Data collection, Investigating and writing the original draft: Salwan Abed Laftah and Kefah Zair Balat; Review and editing: Salwan Abed Laftah, Alaa Kadhim Abdul-Hameed, and Kefah Zair Balat.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The Health Authority of Babylon/Babylon Rehabilitation Center for Disabled, Iraq, approved all experimental protocols, and all permitted guidelines were adhered to during the data collection.
References
- Radhi MM, Al-Eqabi QA, Hindi NK. Rehabilitation problems of people with motor disabilities at Babylon center for rehabilitation of the disabled. Medical Journal of Babylon. 2023; 20(4):838-43. [DOI:10.4103/MJBL.MJBL_674_23]
- World Health Organization. Rehabilitation in health systems. Geneva: World Health Organization; 2021. [Link]
- Elzeni BM, Soliman S, Boughdady A. Assessment of communication barriers between nurses and elderly patients. Mansoura Nursing Journal. 2023; 10(1):251-69. [DOI:10.21608/mnj.2023.320390]
- Similä H, Immonen M, Toska-Tervola J, Enwald H, Keränen N, Kangas M, et al. Feasibility of mobile mental wellness training for older adults. Geriatric Nursing. 2018; 39(5):499-505. [DOI:10.1016/j.gerinurse.2018.02.001] [PMID]
- Balat KZ, Laftah SA, Radhi M. The relationship between psychological distress and quality of life among women undergoing Mastectomy in Iraq: A descriptive correlational study. National Journal of Community Medicine. 2025; 16(01):20-7. [DOI:10.55489/njcm.160120254716]
- Dyer S, van den Berg M, Barnett K, Brown A, Johnstone G, Laver K, et al. Review of innovative models of aged care: Report prepared for the Royal Commission into Aged Care Quality and Safety. Adelaide: Flinders University; 2019. [Link]
- Fiorini J, Venturini G, Conti F, Funaro E, Caruso R, Kangasniemi M, et al. Vessel health and preservation: An integrative review. Journal of Clinical Nursing. 2019 ; 28(7-8):1039-49. [DOI:10.1111/jocn.14707] [PMID]
- Von Walden F, Gidlund EK, Liu C, Ramstrand N, Norrbom J, Von Wachenfelt N, et al. Effect of acute transcranial magnetic stimulation on intracellular signalling in human skeletal muscle. Journal of Rehabilitation Medicine. 2020; 52(2):jrm00022. [DOI:10.2340/16501977-2643] [PMID]
- Al-Eqabi QA, Niazy SM, Radhi MM. Amputation-related factors influencing activities of daily living among amputees. Iranian Journal of War and Public Health. 2024; 16(2):123-9. [Link]
- Oh WO, Shim KW, Yeom I, Park IT, Heo Y. Features and diversity of symptoms of moyamoya disease in adolescents: A cluster analysis. Journal of Advanced Nursing. 2021; 77(5):2319-27. [DOI:10.1111/jan.14723] [PMID]
- Juma Elywy G, Radhi MM, Khyoosh Al-Eqabi QA. Social Support and Its Association With the Quality of Life (QoL) of Amputees. Iranian Rehabilitation Journal. 2022; 20(2):253-60. [DOI:10.32598/irj.20.2.1784.1]
- Radhi MM, Faris HI. Roles of nursing skills in improving quality of rehabilitative health services for patients with chronic conditions. History of Medicine. 2023; 9(1):831-7. [Link]
- Rodrigues IB, Adachi JD, Beattie KA, MacDermid JC. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskeletal Disorders. 2017; 18(1):540. [DOI:10.1186/s12891-017-1914-5] [PMID]
- Chen MD, I JH, Pellegrini CA, Chen HF, Su CY, Chang YC. The facilitators and barriers to physical activity scale for people with mental illness in Taiwan: Development and validation. Disability and Rehabilitation. 2022; 44(17):4879-87. [DOI:10.1080/09638288.2021.1916627] [PMID]
- Eisenberger R, Huntington R, Hutchison S, Sowa D. Perceived organizational support. Journal of Applied Psychology. 1986; 71(3):500-7. [DOI:10.1037//0021-9010.71.3.500]
- Everett B, Salamonson Y, Davidson PM. Bandura’s exercise self-efficacy scale: validation in an Australian cardiac rehabilitation setting. International Journal of Nursing Studies. 2009; 46(6):824-9. [DOI:10.1016/j.ijnurstu.2009.01.016] [PMID]
- Polikandrioti M, Govina O, Vasilopoulos G, Adamakidou T, Plakas S, Kalemikerakis I, et al. Nursing students’ attitudes towards people with disabilities. International Journal of Caring Sciences. 2020; 13(1):480-8. [Link]
- Matthews RA, Michelle Diaz W, Cole SG. The organizational empowerment scale. Personnel Review. 2003; 32(3):297-318. [DOI:10.1108/00483480310467624]
- Radhi MM. Degree of disease acceptance and health seeking behaviors for type 2 diabetic patients at diabetic center in Hilla City. Medico-Legal Update. 2020; 20(2):853-8. [DOI:10.37506/mlu.v20i2.1347]
- Al-Eqabi QA, Niazy SM, Radhi MM. Effectiveness of digital health interventions in managing glycated haemoglobin: A randomized controlled trial. National Journal of Community Medicine. 2024; 15(09):747-53. [DOI:10.55489/njcm.150920244442]
- Malih Radhi M, Zair Balat K. Health literacy and its association with medication adherence in patients with hypertension: A mediating role of social support. Iranian Rehabilitation Journal. 2024; 22(1):117-28. [DOI:10.32598/irj.22.1.1989.1]
- Malih Radhi M, Juma Elywy G, Abbas Khyoosh Al-Eqabi Q. Burdens among wives of disabled people in the light of some social variables. Iranian Rehabilitation Journal. 2023; 21(3):473-84. [DOI:10.32598/irj.21.3.1765.3]
- Elywy GJ, Radhi MM, AlEqabi QA. Relationship between social support and self-hardiness among breast cancer women in Nasiriyah, Iraq. Journal of the Pakistan Medical Association. 2023; 73(9):S9-14. [Link]
- Lin LC, Huang YC, Carter P, Zuniga J. Resilience among nurses in long term care and rehabilitation settings. Applied Nursing Research. 2021; 62:151518. [DOI:10.1016/j.apnr.2021.151518] [PMID]
- Astutik WS. The role of evidence-based management in enhancing nursing performance and patient care outcomes. The Journal of Academic Science. 2024 ;1(5):541-52. [Link]
- Marks DF. The health psychology reader. California: SAGE Publications; 2002. [Link]
- Cherniss C. Role of professional self-efficacy in the etiology and amelioration of burnout. In: Schaufeli WB, Maslach Ch, Marek T, editors. Professional burnout. London: Routledge; 2017. [DOI:10.4324/9781315227979-11]
- Rubel MR, Hung Kee DM, Rimi NN. High-performance work practices and medical professionals’ work outcomes: The mediating effect of perceived organizational support. Journal of Advances in Management Research. 2021; 18(3):368-91. [DOI:10.1108/JAMR-05-2020-0076]
- Yasir AA, Elywy GJ, Radhi MM. Assessment the Development of Social Responsibility among Sample of (Kut Technical Institute, Iraq) Students and its Relation to Social Media Network Sites. Research Journal of Pharmacy and Technology. 2018; 11(10):4426-30. [DOI:10.5958/0974-360X.2018.00810.7]
- Qassim WJ, Yasir AA, Radhi MM. Assessment of Self Hardness and its Relationship to Treatment Acceptance for Patients with Diabetes Mellitus at Diabetic Center in Hilla City/Iraq. Journal of Pharmaceutical Sciences and Research. 2018; 10(1):142-5. [Link]
Article type: Original Research Articles |
Subject:
Nursing
Received: 2025/03/27 | Accepted: 2025/04/21 | Published: 2025/06/1
Received: 2025/03/27 | Accepted: 2025/04/21 | Published: 2025/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
