
988368
Wed, Jul 29, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 363-374 |
Back to browse issues page


Ethics code: IR.USWR.REC.1401.132
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shakibamehr N, Pourmohamadreza-Tajrishi M, Adibsereshki N, Vahedi M. Oregan Model Parenting and Mothers' Mental Health vs Externalizing Problems in Motor-disabled Children. Iranian Rehabilitation Journal 2025; 23 (4) :363-374
URL: http://irj.uswr.ac.ir/article-1-2508-en.html
URL: http://irj.uswr.ac.ir/article-1-2508-en.html



1- Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Biostatistics and Epidemiology, Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Biostatistics and Epidemiology, Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Keywords: Oregon model parenting management (OMPM), Externalizing difficulties, Mother’s mental health, Motor disability
Full-Text [PDF 691 kb]
(417 Downloads)
| Abstract (HTML) (2129 Views)
Full-Text: (248 Views)
Introduction
Motor disability refers to an impairment that limits an individual’s ability to perform major life activities and hinders the effective use of their limbs. Globally, United Nations International Children's Emergency Fund (UNICEF) estimates that approximately 207.4 million children aged 5-17 years (12.5%) experience moderate to severe disabilities, based on household surveys assessing functional status [1]. In Iran, over one million individuals have at least one form of disability. These disabilities can arise from various causes, including congenital genetic factors and acquired injuries from traffic and non-traffic accidents [2].
Children with motor disabilities are particularly prone to behavioral challenges [3], which can adversely impact their developmental trajectory and overall quality of life (QoL). Considering the high prevalence of these disabilities, understanding their specific needs is essential for designing effective interventions and supportive services. Behavioral difficulties encompass actions that are socially or culturally unacceptable, pose safety risks, disrupt learning processes, and hinder healthy social interactions [4]. The persistence of such behaviors is often influenced by family environment and parenting practices. Caregiving for a child with a motor disability frequently results in caregiver stress and mental health issues for parents [5].
The presence of a child with motor impairment introduces new familial challenges, adversely affecting family dynamics and lifestyle. These children typically depend on caregivers, especially mothers, for daily activities. This dependency can generate emotional and behavioral stress within the family, impacting maternal mental health and, consequently, the child’s well-being [4]. Maternal approaches characterized by hostility, control, or punitive discipline can inadvertently foster maladaptive behaviors, irritability, and aggression in children [6].
Behavioral issues in children often reflect underlying familial mental health challenges, creating a cycle that exacerbates both child and maternal difficulties. Recent evidence underscores the necessity of appropriate programs and services aimed at promoting mental health in both mothers and children [7].
Parent management training (PMT) programs aim to improve parenting skills and child outcomes, employing various approaches. These programs focus on reinforcing positive behaviors and reducing problematic behaviors, helping parents acquire skills, such as encouraging desirable actions, setting boundaries, and monitoring activities to prevent or mitigate behavioral difficulties [8]. One prominent model is the Oregon model of parenting management (OMPM), which emphasizes three core components: 1) safety and behavioral strategies, equipping parents with skills to manage challenging behaviors; 2) self-management, teaching parents’ techniques to regulate their responses in difficult situations; and 3) reciprocal interactions, focusing on how parental behaviors influence child behaviors to promote healthier family dynamics [9].
Other approaches, including parenting programs, such as the positive parenting program (triple-P) [10] and stepping stones [11], vary in scope and methodology. The triple-P adopts a comprehensive, multi-level approach that emphasizes promoting positive reinforcement, reducing negative behaviors, and building parental confidence through adaptive skills training, making it suitable for a broad range of behavioral issues and prevention efforts [12]. In contrast, stepping stones is specifically designed for parents of children with behavioral and learning difficulties, focusing on targeted skill development to manage these special needs and foster emotional support through peer networks [11]. While both programs aim to improve parenting practices, their scope and primary focus differ. Triple-P offers a more general preventative framework, whereas stepping stones provides targeted interventions for complex cases. Understanding these distinctions is crucial to assess their relative suitability and expected outcomes compared to the current intervention for children with motor disabilities.
The distinguishing feature of OMPM lies in its focus on equipping parents, particularly mothers, with interactive management strategies that foster effective communication, which can reduce behavioral issues and enhance maternal mental health [13]. Since behavioral difficulties often originate early in childhood and children with motor disabilities require special care, paying attention to maternal behaviors, the quality of mother-child interactions, and implementing targeted interventions in these areas can contribute significantly to their well-being. Such approaches may prevent the escalation of psychological and behavioral problems later in life [14].
The article acknowledges the absence of local validation for the OMPM but does not explicitly detail how this study addresses this gap. Our research aims to evaluate the effectiveness of the OMPM within our specific cultural context, recognizing that cultural factors, such as familial norms, parenting practices, and social expectations, can influence the intervention’s outcomes. By assessing both maternal mental health and children’s externalizing behaviors, this study provides evidence of the model’s applicability and efficacy in our setting. Such validation is crucial, as cultural adaptations or considerations may be necessary to optimize the intervention’s relevance and effectiveness. Additionally, fostering positive mother-child relationships and strengthening family dynamics through programs like OMPM can establish a solid foundation for children’s active participation in school and society, promoting their independence and overall development. This foundation can alleviate the additional burdens children face due to reliance on caregivers, potentially preventing the emergence or deterioration of behavioral issues over time, while also improving maternal mental health. Overall, evaluating the model’s efficacy in our cultural context contributes to a broader understanding of how culturally sensitive parenting programs can be effectively implemented. Although the literature highlights the significance of maternal mental health and family dynamics in influencing child behavior, there remains a gap in research validating the OMPM in our specific cultural context. This study aims to fill this gap by evaluating the model’s effectiveness in promoting positive mother-child interactions and reducing behavioral difficulties among children with motor disabilities.
Materials and Methods
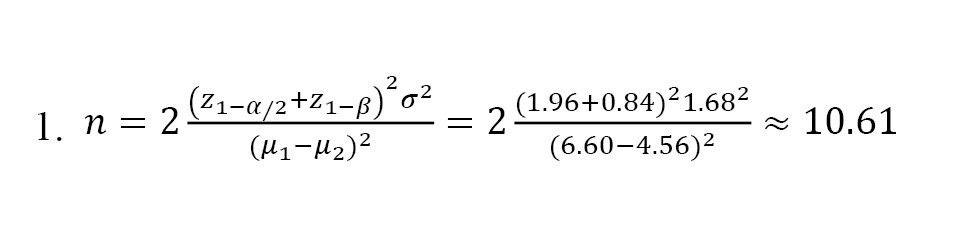
The present study employed a quasi-experimental design with a pre-test and post-test, incorporating a control group and a two-month follow-up. The target population consisted of boys aged 8 to 11 years with motor disabilities enrolled in special schools for children with physical and motor issues in Qazvin City during the 2023-2024 academic year. The decision to focus solely on boys was based on epidemiological data indicating a higher prevalence of motor disabilities among males, often with a male-to-female ratio of approximately 2:1 to 3:1 [15]. Additionally, boys tend to exhibit higher rates of externalizing behaviors, such as aggression and rule-breaking, which are often more prominent in this population [16]. A total of 30 participants and their mothers were selected through convenience sampling. The sample size was determined based on a similar study [17], with a type I error rate of 0.05, power of 0.8, and anticipated dropout rate of 25%. Using the sample size formula (Equation 1) and inclusion criteria, participants were randomly assigned to either the experimental or control group using simple randomization, resulting in 15 individuals in each group:
The inclusion criteria for the study were as follows: Both mothers and children had to be willing to cooperate; mothers needed to have at least a middle school certificate to complete written assignments during the intervention sessions; children should not have had any sensory impairments, such as vision or hearing problems, or neurological conditions, such as or attention deficit/hyperactivity disorder (based on parents’ reports), mothers should not have had mental disorders that could hinder their participation in the intervention sessions, as assessed through their own reports; and children had to have a T-score between 60 and 63 on the Achenbach child behavior checklist (ACBCL) to identify externalizing difficulties. Participants were excluded if they had participated in similar parent management programs within the previous six months or were currently involved in such programs. Additionally, incomplete questionnaire submissions also resulted in exclusion from the study.
The mental health inventory (MHI): The MHI is a 38-item instrument designed to measure well-being and mental distress, and has been validated in four large samples of participants aged 13 to 69 years across four large samples [18]. The purpose of this study was to evaluate participants’ overall mental health status, providing a reliable and valid tool for the Iranian population. The MHI’s psychometric properties, including high internal consistency and stability over time, support its suitability for this context. To streamline assessment, we used the shortened MHI-18 version, which assesses anxiety, depression, emotional ties, behavioral control, and positive affect—core components linked to mental well-being and distress [18]. The Persian MHI-18 has demonstrated excellent factorial validity, with two primary factors: Well-being (positive affect and emotional ties) and mental distress (depression, anxiety, and behavioral control), and a Cronbach’s α of 0.75, indicating good internal consistency. The use of the MHI-18 in this study was justified by its brevity, psychometric robustness, and established validity in Iranian samples [19].
The ACBCL: The ACBCL is a comprehensive tool designed to assess a wide range of behavioral and emotional problems in children aged 6 to 18. In this study, we used the Persian version to evaluate externalizing difficulties, specifically aggression and rule-breaking behaviors, as primary outcome measures. The ACBCL consists of 113 items rated on a three-point scale, completed by parents familiar with their child’s behavior. This study aimed to identify behavioral problems associated with internalizing and externalizing disorders, focusing on externalizing difficulties relevant to our intervention. The ACBCL has demonstrated good psychometric properties in the Iranian population, with reliability coefficients ranging from 0.48 to 0.85 for subscales [20]. The items cover various domains, such as withdrawal/depression, anxiety/depression, somatic complaints, social problems, thought problems, rule-breaking, attention problems, and aggressive behaviors. Factor analysis by Achenbach identified eight factors, with withdrawal, anxiety/depression, and somatic complaints reflecting internalizing difficulties, and rule-breaking and aggression indicating externalizing problems. Cronbach’s α for the scales ranged between 0.65 and 0.85, and for the eight subscales, it ranged from 0.48 to 0.75 [20]. In our study, we focused on evaluating externalizing difficulties, specifically aggression and rule-breaking behaviors, as these are crucial markers of outward behavioral issues. The Persian version of the ACBCL has been validated, with established cutoff scores of 60-63 and 63 and higher to identify borderline or clinical levels of these problems. The temporal stability of the scales was assessed using coefficients ranging from 0.32 to 0.67. In this study, only externalizing difficulties and their factors (aggression and rule-breaking behaviors) were evaluated as the primary outcome measures [21].
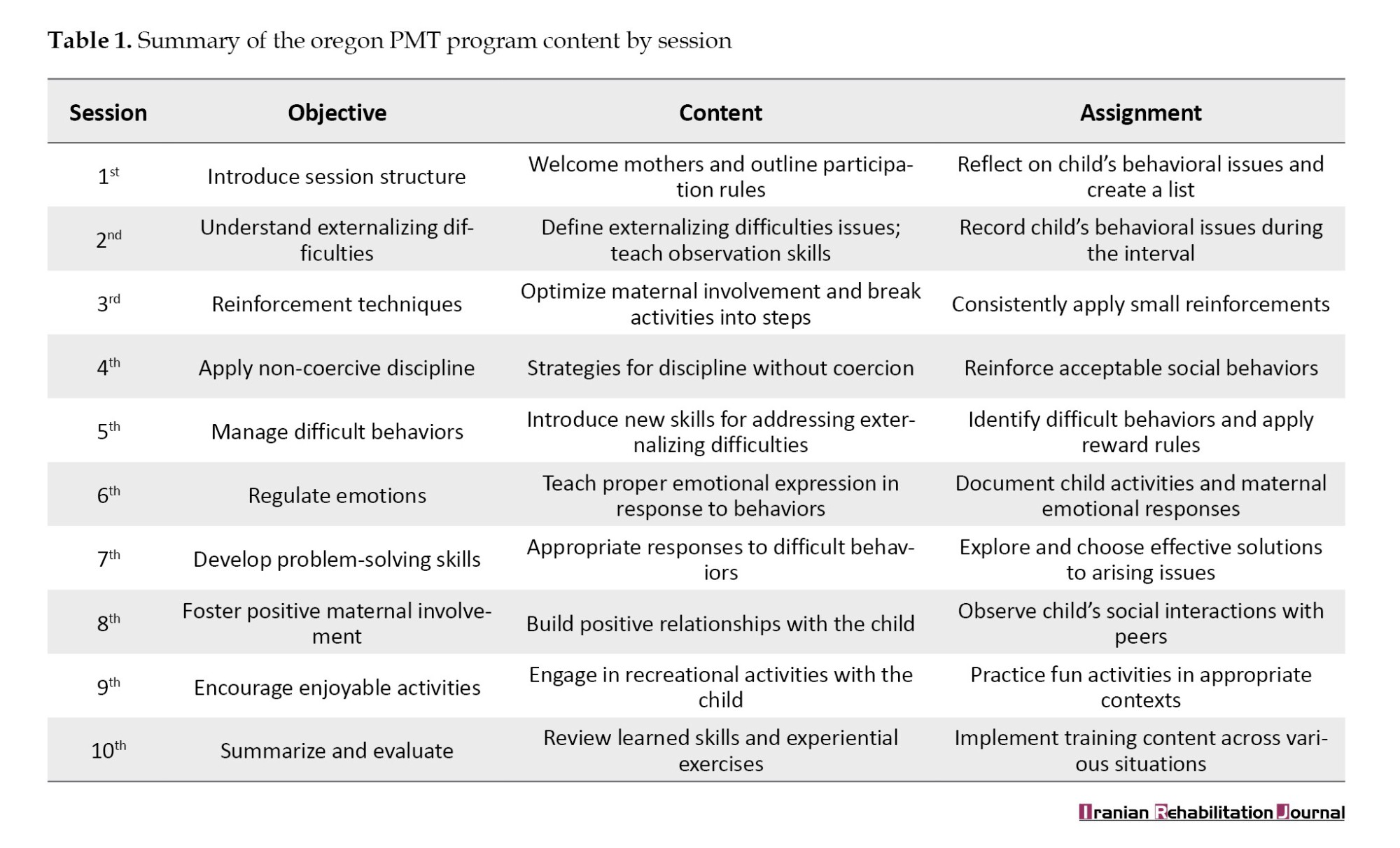
OMPM: The OMPM program is a type of therapeutic training that includes weekly sessions in which a therapist works with the parents of a family. The children do not participate in these sessions, and the intervention aims to replace parents’ coercive parenting methods with effective parenting strategies. Role-playing is an essential mechanism in the sessions, with the therapist using it to demonstrate good and bad examples and identify which parenting skills require attention, training, and practice. Once parents have practiced the parenting skills sufficiently, the therapist and parents select a specific situation for the next session, during which parents try to apply the newly acquired skills at home. Between sessions, the therapist contacted the parents to provide support and answer their questions. The duration of therapy depends on the family’s needs and progress during treatment, but it typically lasts for 10-15 weekly sessions. In the present study, parents received the intervention from two certified therapists who had completed a comprehensive 10-session parent management program [9] (Table 1).
Research procedure
After obtaining ethical approval, an introductory letter was prepared for the Exceptional Education Organization in Qazvin City. A meeting with relevant officials facilitated the identification of an educational center specializing in children with motor disabilities, and permission was obtained to access the facility. Following an explanation of the study’s objectives and procedures, written informed consent was obtained from mothers willing to participate. The mothers completed the ACBCL, and from the pool of children scoring between 60 and 63, 30 children were randomly selected and assigned to either the experimental or control group, with 15 children in each. To minimize measurement bias, assessors responsible for administering and scoring the questionnaires were blinded to the group assignments. The experimental group received the OMPM intervention in 10 training sessions, each lasting 90 minutes. Conversely, the control group participated in routine family education sessions at the center, designed to provide foundational parenting guidance without focusing on the specific content of the experimental program. The control group’s sessions, conducted over seven weekly meetings of approximately 30 minutes, covered topics, such as child growth and development, communication strategies, discipline techniques, and emotional support. The sessions combined lectures, interactive discussions, and informational resources to enhance general parenting skills. All mothers completed the MHI and the ACBCL at three intervals: pre-intervention, post-intervention, and two months after the intervention. The collected data were analyzed using chi-square tests, t-tests, and repeated-measures analysis of variance (ANOVA) in SPSS software, version 25.
Results
The participants’ Mean±SD ages 33.27±2.73 years for mothers and 9.70±0.87 years for children. The ages of children in the experimental and control groups were 9.77±0.85 and 9.63±0.89 years, respectively. Table 2 presents the demographic characteristics.
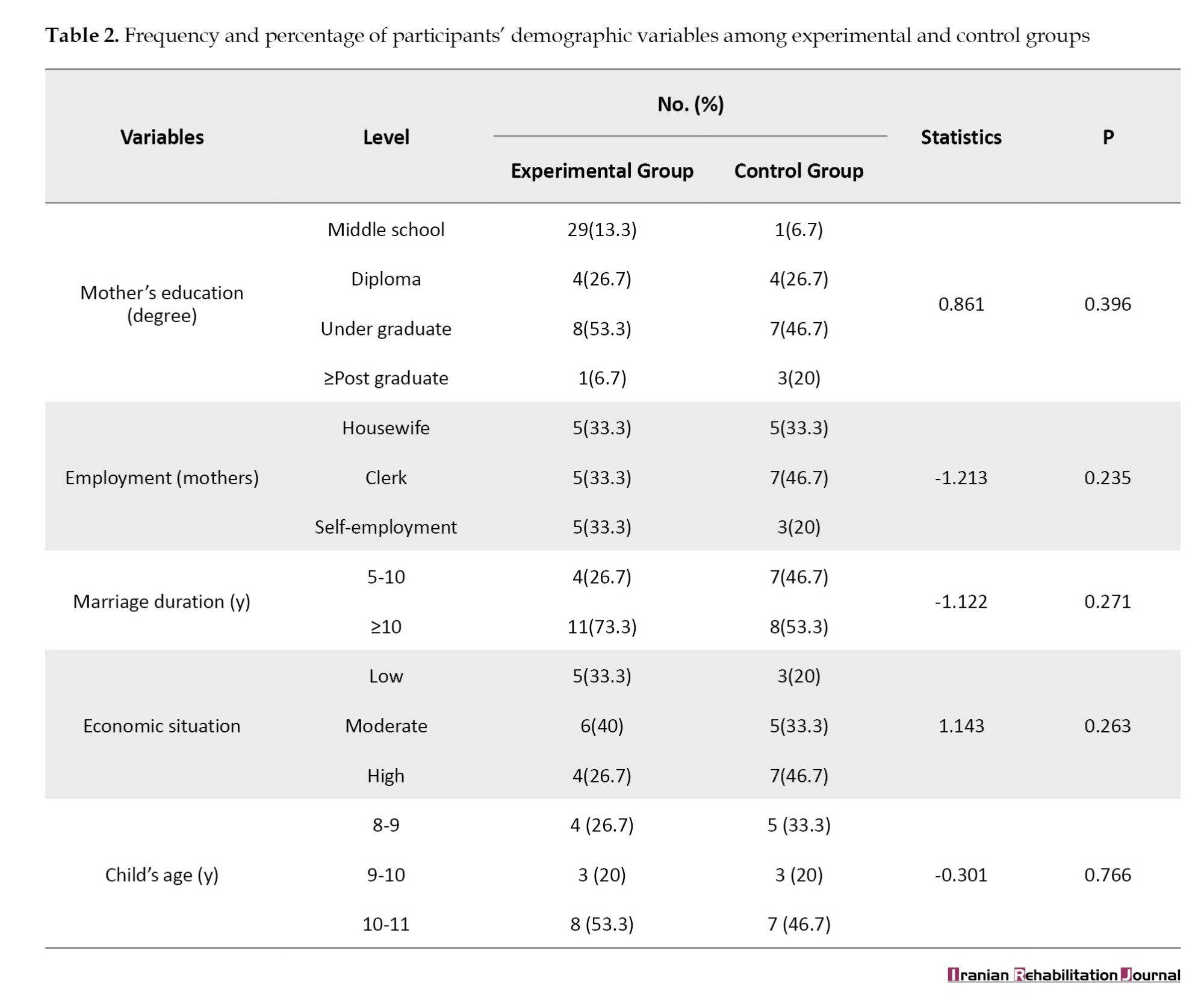
As indicated in Table 2 , the statistical analyses revealed no significant differences between the experimental and control groups concerning mothers’ educational levels, employment status, duration of marriage, family economic status, or children’s age (P>0.05).
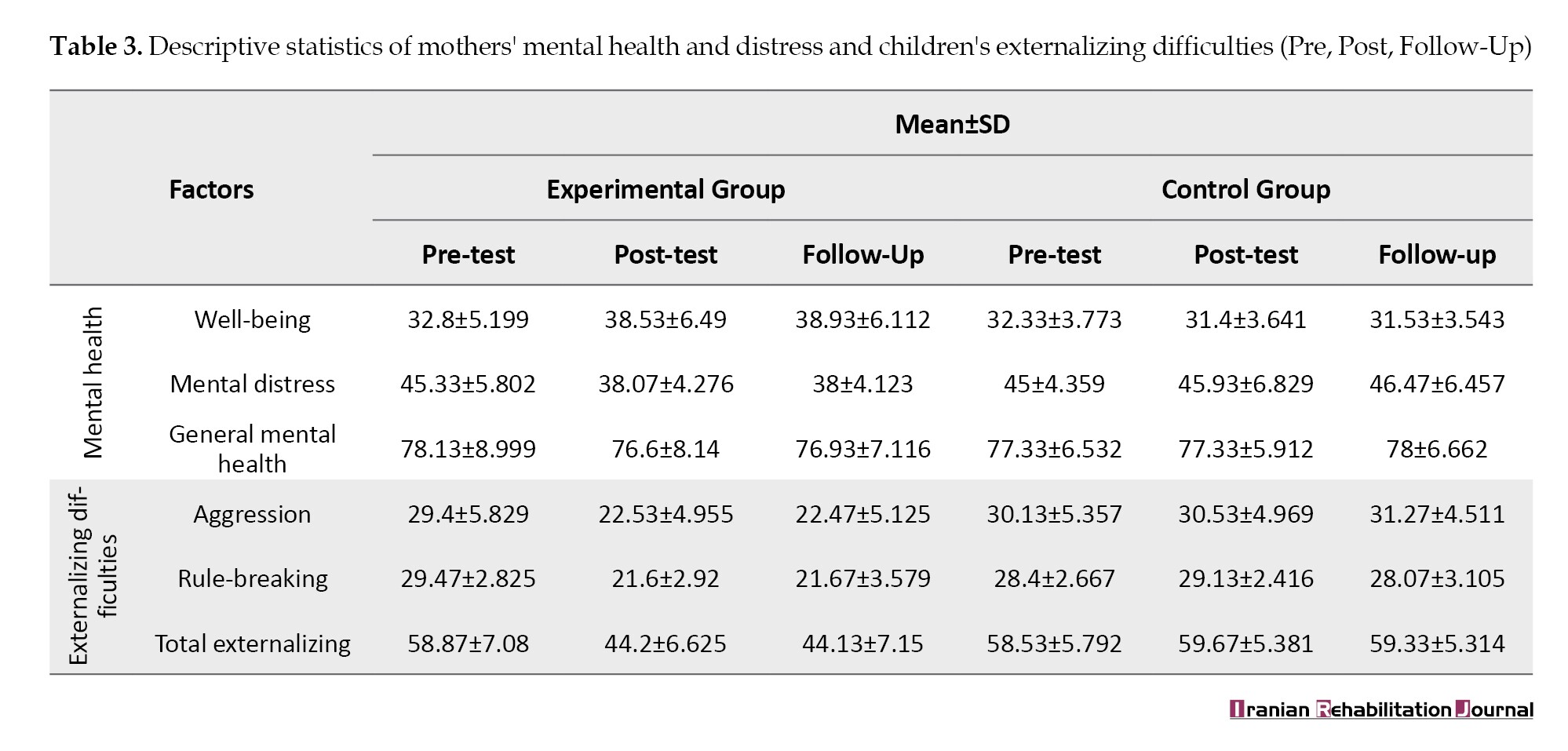
Table 3 presents descriptive statistics (Mean±SD) for the mental health factors (well-being and mental distress) of mothers and externalizing difficulties and their factors (aggression and rule-breaking behaviors) in children with motor disabilities, differentiated by the experimental and control groups at the pre-test, post-test, and follow-up stages.
Table 3 presents the descriptive statistics, Mean±SD for maternal mental health factors (well-being and mental distress) and children’s externalizing difficulties (including aggression and rule-breaking behaviors) across pre-test, post-test, and follow-up assessments, differentiated by group. The data indicated that the experimental group experienced significant improvements in maternal well-being and reductions in mental distress. Specifically, maternal well-being scores increased from a pre-intervention Mean±SD of 32.8±5.199 to 38.93±6.112 at post-test, while mental distress scores decreased correspondingly. The control group showed no significant changes over time. Similarly, externalizing difficulties in children, particularly aggression, showed marked improvement: mean scores declined from 29.4±5.829 pre-intervention to 22.47±5.125 at follow-up in the experimental group, whereas the control group’s scores remained relatively stable. These results underscore the positive impact of the intervention on both maternal mental health and children’s behavioral issues.
The assumptions underlying repeated-measures ANOVA, normal distribution, and absence of outliers, were verified, with no violations detected. Mauchly’s sphericity test indicated violations for some variables, necessitating the use of Greenhouse-Geisser corrections (Table 4).
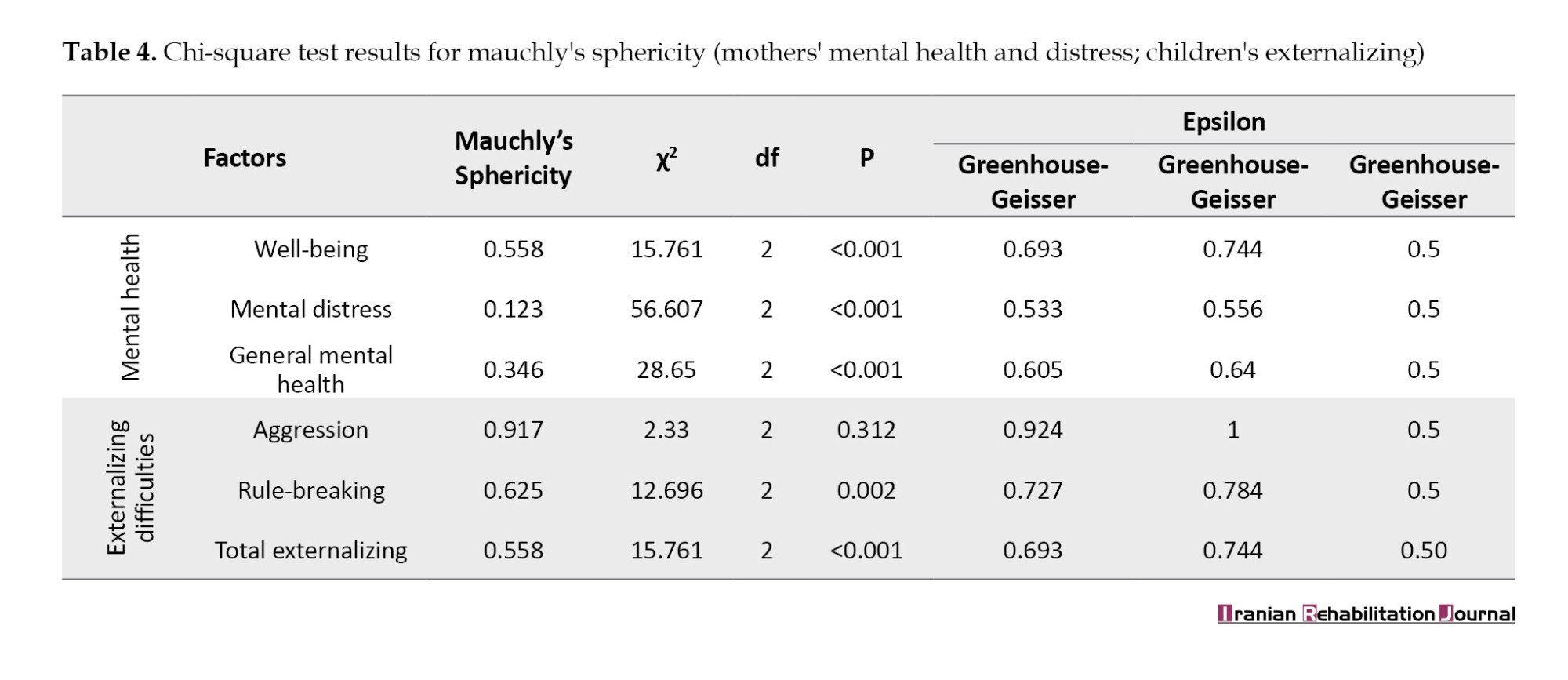
Table 4 presents the results of the chi-square test conducted to evaluate Mauchly’s sphericity assumption for mothers’ mental health factors, including well-being, mental distress, general mental health, as well as externalizing difficulties among children, focusing on aggression and rule-breaking. The findings indicate statistically significant results across various factors, with P<0.001 for well-being, mental distress, and general mental health, while rule-breaking showed a significant P of 0.002. The results of the chi-square test suggest that the variables exhibited significant differences that warranted the use of repeated-measures ANOVA to compare general mental health indicators and total externalizing difficulties between the experimental and control groups over the assessed time points (pre-test, post-test, and follow-up) (Table 5).
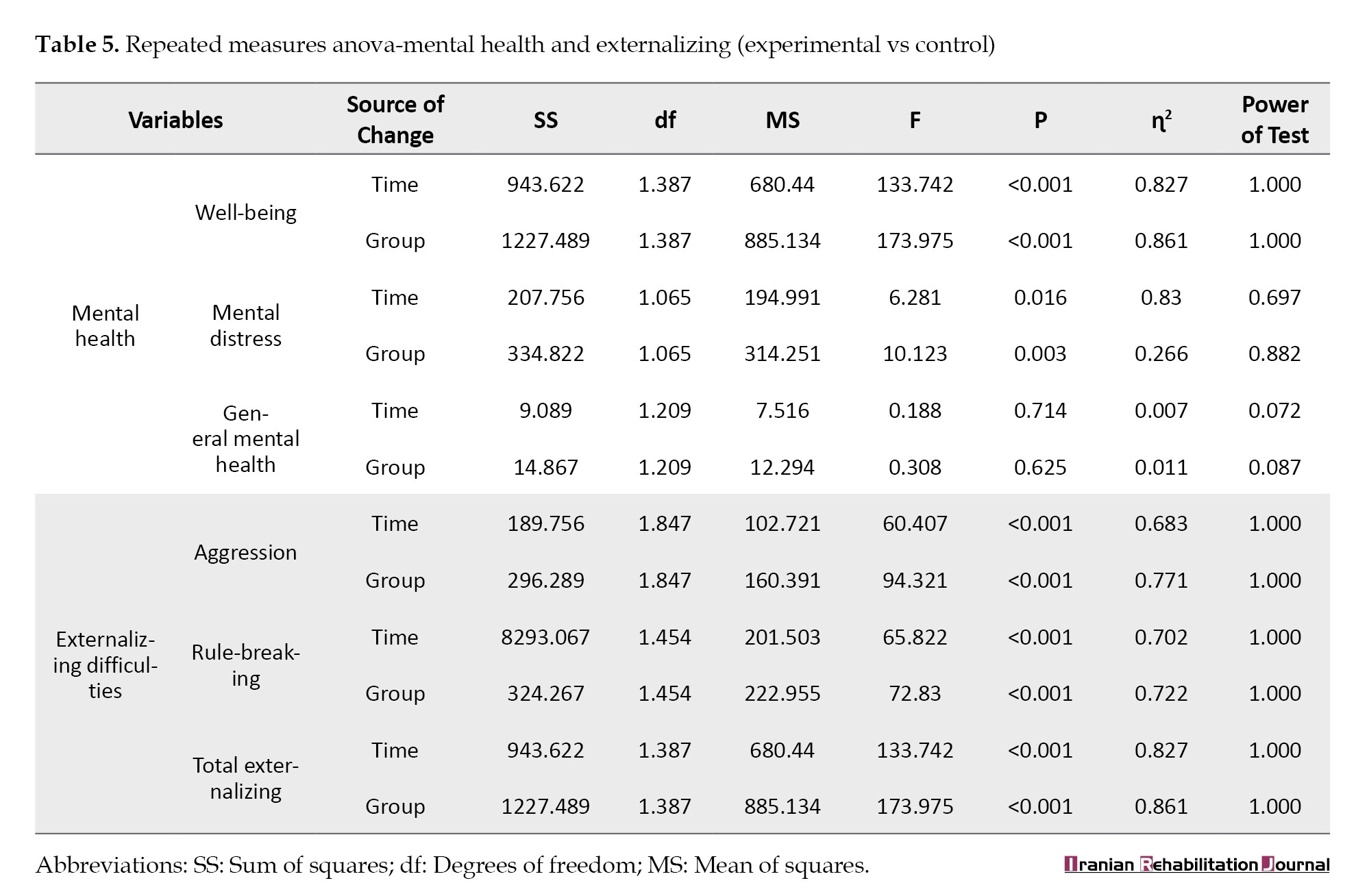
Table 5 summarizes the findings from repeated-measures ANOVA, indicating significant effects of time and group on maternal mental health (well-being and mental distress) and children’s externalizing behaviors. The experimental group demonstrated significant improvements over time: Such as, well-being (F [1, df], P<0.001, η²=0.861) and reduction in mental distress (F [1, df], P<0.016, η²=0.266). Similarly, there were significant decreases in aggression (F [1, df], P<0.001, η²=0.771) and rule-breaking behaviors (F [1, df], P<0.001, η²=0.722). The effect sizes indicate a strong impact of the intervention on these outcomes.
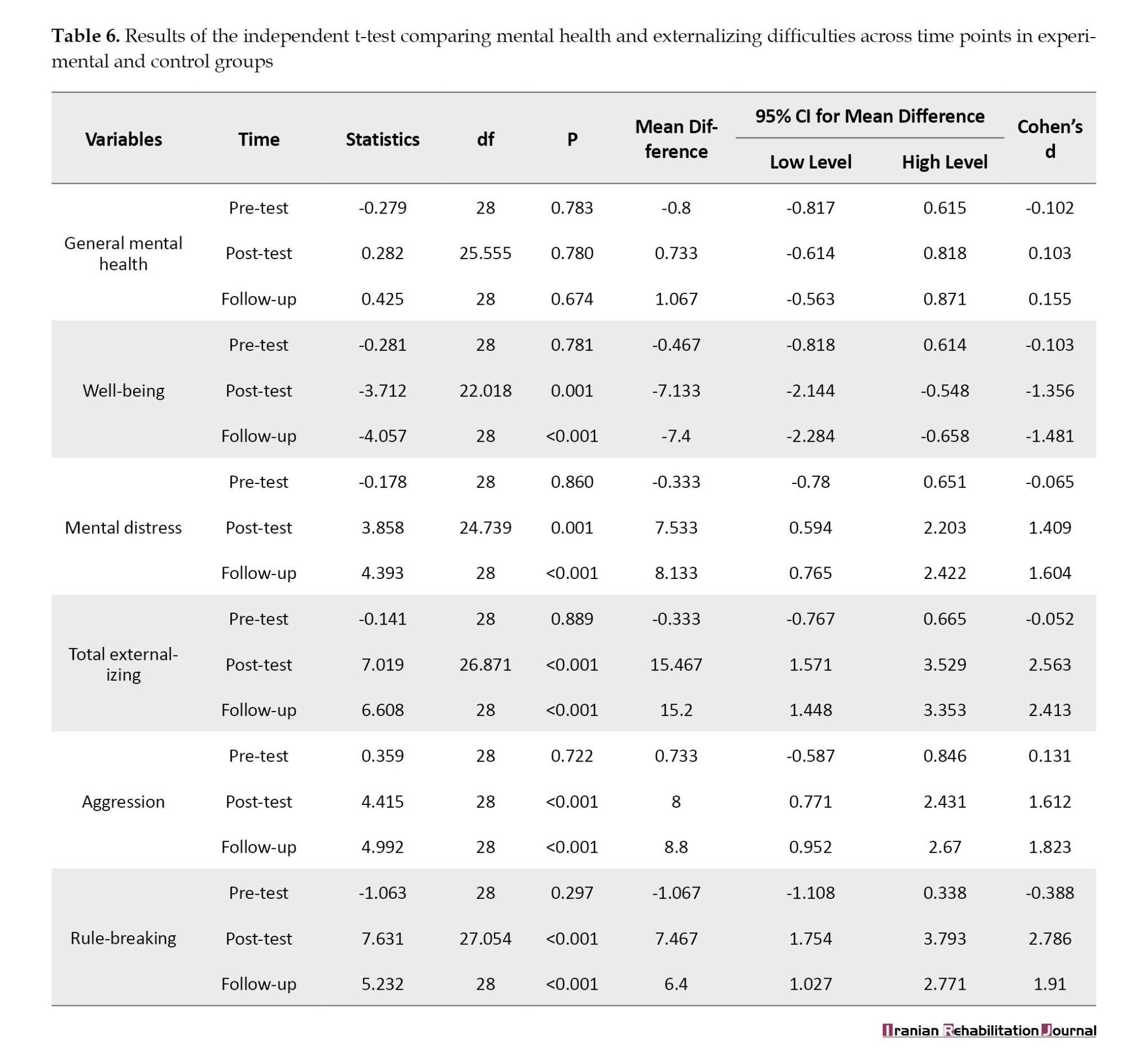
Finally, Table 6 presents independent t-tests comparing the groups at each time point. Pre-test comparisons across groups showed no statistically significant differences in any measure (P>0.05), with effect sizes being minimal (Cohen’s d≈-0.1 to 0.13), indicating negligible baseline differences in mental health and externalizing behaviors. However, at post-test, the experimental group demonstrated substantial improvements across most variables, with effect sizes ranging from large to very large: Well-being (d≈-1.36; 95% CI supporting this magnitude), total externalizing behaviors (d≈2.56), aggression (d≈1.61), and rule-breaking (d≈2.79). These effect sizes, exceeding the threshold for large effects (d≥0.8), indicate meaningful and practically significant changes. Furthermore, the effect persisted at follow-up, with effect sizes remaining large (d>1.9), underscoring the durable impact of the intervention on enhancing children’s mental health and reducing externalizing difficulties.
Discussion
This study investigated the effectiveness of the OMPM program on the mental health of Iranian mothers caring for children with motor disabilities and externalizing behavioral difficulties. The primary hypothesis was that the OMPM would enhance effective parenting skills, thereby alleviating maternal mental health problems and reducing externalizing behaviors in children.
Initial findings demonstrated that participation in the OMPM significantly improved maternal well-being and decreased mental distress, with these benefits maintained at two-month follow-up. These results are consistent with prior research [5, 17, 22], suggesting that the program enhances emotional awareness, enabling mothers to respond more consciously and calmly to their children’s challenging behaviors. Such improvements facilitate closer mother-child interactions, promote emotional regulation, and diminish impulsive reactions rooted in prior stressors [22, 23].
The mechanisms underlying these outcomes involve mothers learning strategies that help them disengage from automatic, reactive responses, thereby encouraging more rational decision-making amid emotionally charged situations. As mothers become more aware of their emotional reactions, they tend to regulate their responses more effectively, which enhances both their emotional well-being and capacity to cope with daily stressors [3]. Increased emotional awareness further fosters empathy for children’s feelings, encourages reflective pauses before reacting, and contributes to sustained improvements in maternal mental health [5].
Although the intervention successfully mitigated maternal mental distress, it did not significantly influence broader measures of mental health. This aligns with existing literature emphasizing the complex bidirectional relationship between maternal mental health and child behavioral challenges. Maternal depressive symptoms and low self-efficacy are associated with greater behavioral issues in children [24]. However, these factors are influenced by persistent mental health challenges that may not be entirely alleviated through brief intervention alone. It should be noted that this study relied on self-report measures, which, while valuable, may be subject to bias and may not fully capture the nuanced dynamics of maternal mental health. Future interventions should aim to include targeted mental health support alongside parenting programs to foster more comprehensive improvements. It is also important to acknowledge that this study relied on self-reported assessments of mental well-being and distress from the mothers involved. While these self-reported measures may reveal positive therapeutic effects, improvements in mental health could be attributed to various factors outside the intervention itself. Nonetheless, it is plausible to argue that the mental health inventory utilized in this study sufficiently captured mothers’ health-related responses and experiences [25]. Future interventions should focus on enhancing maternal skills to better support mothers facing significant mental distress, rather than expecting that participation in the OMPM program alone will yield substantial improvements in general mental health outcomes.
Regarding children’s externalizing behaviors, the OMPM yielded significant reductions in aggression, rule-breaking, and overall externalizing difficulties, consistent with previous literature findings [26]. The intervention appeared to primarily influence behaviors within the home environment, as teachers did not report similar improvements, indicating possible contextual limitations of generalizability outside the family setting.
The core premise of the OMPM suggests that improvements in maternal parenting skills translate into decreased externalizing difficulties. Mothers learn to avoid negative reactions and employ more effective discipline strategies, which are critical in managing externalizing problems [10, 24]. Effect size analyses indicated that reductions in aggression, rule-breaking, and total externalizing behaviors were meaningful, although the small sample size limited subgroup analyses, particularly for children with more severe issues. It is plausible that children with higher initial severity may benefit the most from such interventions [25].
To elucidate potential mediators, factors, such as maternal education, consistency in parenting practices, and children’s emotional regulation should be explored in future research [27]. The sustained improvement observed at follow-up suggests that mothers felt more confident and effective post-intervention, which may have created a positive feedback loop, improving both their mental health and their children’s behaviors [28].
Despite these encouraging results, several limitations must be considered. The small sample size of 30 participants (15 per group), recruited via convenience sampling, constrains the statistical power and limits the generalizability of the results to broader populations. This sampling approach may also introduce selection bias, further affecting the external validity. Although the sample size was comparable to prior research [17], further studies should aim for larger, randomly selected samples to facilitate more comprehensive subgroup analyses and confirm the robustness of these findings. It is important to note that this study focused exclusively on boys, primarily because epidemiological data indicate a higher prevalence of motor disabilities among males and the tendency for boys to exhibit more externalizing behaviors, such as aggression, which are often linked to such disabilities. While this focus provides valuable insights into this subgroup, it limits the applicability of the findings to girls. Including both genders in future research would enhance the generalizability and allow exploration of potential gender-specific responses to interventions. A notable limitation of this study is the reliance on self-report questionnaires to assess maternal mental health and child behavior. This method is susceptible to various biases, such as social desirability and recall bias, which can affect data accuracy. Furthermore, the quasi-experimental design lacking randomization restricts causal inferences, and the absence of long-term follow-up prevents evaluation of the sustainability of intervention effects over time. To address these limitations, future research should incorporate larger, more diverse samples, utilize objective assessment measures alongside self-reports, and adopt longitudinal designs. Including data from fathers and other caregivers may also provide a more comprehensive understanding of familial influences on child outcomes.
Conclusion
Based on the findings, it can be concluded that OMPM intervention has a positive impact on the two factors of mental health (well-being and mental distress) of mothers and externalizing difficulties in children with motor disabilities, with effects persisting even after a two-month follow-up. As OMPM is a cost-effective approach, policymakers and therapists can utilize the results of this study to inform decisions that benefit children with motor disabilities and their families. Given the individual, familial, and societal costs associated with externalizing difficulties in childhood, there has been increasing attention on risk factors for the development of these difficulties and the effectiveness of intervention services. Parenting management programs are well-established based on theories and research highlighting the link between ineffective parenting and children’s externalizing difficulties. However, many children with externalizing difficulties are also clinically challenged by internalizing problems that may manifest as externalizing difficulties.
This area of research—whether (PMT) programs addressing ineffective parenting practices also positively affect childhood internalizing issues—has received less attention. Nonetheless, based on the current findings, several hypotheses can be proposed. First, designing and implementing PMT programs that include changes in warmth, hostility, and behavior control may effectively address both externalizing and internalizing difficulties. Therefore, concurrently examining internalizing issues in children is recommended, given the complex interactions among parenting behaviors, internalizing, and externalizing difficulties. Second, there is a strong association between maternal hostility and child behavioral outcomes, suggesting that non-hostile maternal behavior should be explicitly targeted in management programs, despite being indirectly addressed in most interventions. Third, mothers alone cannot fully resolve or reduce their children’s externalizing difficulties (as indicated by effect sizes); thus, interventions must be broader than just mother management training, incorporating elements, such as teaching self-regulation to children and reducing family stress.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.132). Informed consent was obtained from all mothers of children included in the study.
Funding
This study was extracted from the master's thesis of Narjes Shakibamehr, approved by the Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. This study was supported in part by the Deputy of Research and Technology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization: Narjes Shakibamehr, Masoume Pourmohamadreza-Tajrishi, and Mohsen Vahedi; Supervision, methodology, validation, analysis and writing the original draft: Masoume Pourmohamadreza-Tajrishi and Mohsen Vahedi; Investigation: Narjes Shakibamehr; Review and editing: Masoume Pourmohamadreza-Tajrishi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to all mothers and their children with motor disabilities for participating in this study.
References
Motor disability refers to an impairment that limits an individual’s ability to perform major life activities and hinders the effective use of their limbs. Globally, United Nations International Children's Emergency Fund (UNICEF) estimates that approximately 207.4 million children aged 5-17 years (12.5%) experience moderate to severe disabilities, based on household surveys assessing functional status [1]. In Iran, over one million individuals have at least one form of disability. These disabilities can arise from various causes, including congenital genetic factors and acquired injuries from traffic and non-traffic accidents [2].
Children with motor disabilities are particularly prone to behavioral challenges [3], which can adversely impact their developmental trajectory and overall quality of life (QoL). Considering the high prevalence of these disabilities, understanding their specific needs is essential for designing effective interventions and supportive services. Behavioral difficulties encompass actions that are socially or culturally unacceptable, pose safety risks, disrupt learning processes, and hinder healthy social interactions [4]. The persistence of such behaviors is often influenced by family environment and parenting practices. Caregiving for a child with a motor disability frequently results in caregiver stress and mental health issues for parents [5].
The presence of a child with motor impairment introduces new familial challenges, adversely affecting family dynamics and lifestyle. These children typically depend on caregivers, especially mothers, for daily activities. This dependency can generate emotional and behavioral stress within the family, impacting maternal mental health and, consequently, the child’s well-being [4]. Maternal approaches characterized by hostility, control, or punitive discipline can inadvertently foster maladaptive behaviors, irritability, and aggression in children [6].
Behavioral issues in children often reflect underlying familial mental health challenges, creating a cycle that exacerbates both child and maternal difficulties. Recent evidence underscores the necessity of appropriate programs and services aimed at promoting mental health in both mothers and children [7].
Parent management training (PMT) programs aim to improve parenting skills and child outcomes, employing various approaches. These programs focus on reinforcing positive behaviors and reducing problematic behaviors, helping parents acquire skills, such as encouraging desirable actions, setting boundaries, and monitoring activities to prevent or mitigate behavioral difficulties [8]. One prominent model is the Oregon model of parenting management (OMPM), which emphasizes three core components: 1) safety and behavioral strategies, equipping parents with skills to manage challenging behaviors; 2) self-management, teaching parents’ techniques to regulate their responses in difficult situations; and 3) reciprocal interactions, focusing on how parental behaviors influence child behaviors to promote healthier family dynamics [9].
Other approaches, including parenting programs, such as the positive parenting program (triple-P) [10] and stepping stones [11], vary in scope and methodology. The triple-P adopts a comprehensive, multi-level approach that emphasizes promoting positive reinforcement, reducing negative behaviors, and building parental confidence through adaptive skills training, making it suitable for a broad range of behavioral issues and prevention efforts [12]. In contrast, stepping stones is specifically designed for parents of children with behavioral and learning difficulties, focusing on targeted skill development to manage these special needs and foster emotional support through peer networks [11]. While both programs aim to improve parenting practices, their scope and primary focus differ. Triple-P offers a more general preventative framework, whereas stepping stones provides targeted interventions for complex cases. Understanding these distinctions is crucial to assess their relative suitability and expected outcomes compared to the current intervention for children with motor disabilities.
The distinguishing feature of OMPM lies in its focus on equipping parents, particularly mothers, with interactive management strategies that foster effective communication, which can reduce behavioral issues and enhance maternal mental health [13]. Since behavioral difficulties often originate early in childhood and children with motor disabilities require special care, paying attention to maternal behaviors, the quality of mother-child interactions, and implementing targeted interventions in these areas can contribute significantly to their well-being. Such approaches may prevent the escalation of psychological and behavioral problems later in life [14].
The article acknowledges the absence of local validation for the OMPM but does not explicitly detail how this study addresses this gap. Our research aims to evaluate the effectiveness of the OMPM within our specific cultural context, recognizing that cultural factors, such as familial norms, parenting practices, and social expectations, can influence the intervention’s outcomes. By assessing both maternal mental health and children’s externalizing behaviors, this study provides evidence of the model’s applicability and efficacy in our setting. Such validation is crucial, as cultural adaptations or considerations may be necessary to optimize the intervention’s relevance and effectiveness. Additionally, fostering positive mother-child relationships and strengthening family dynamics through programs like OMPM can establish a solid foundation for children’s active participation in school and society, promoting their independence and overall development. This foundation can alleviate the additional burdens children face due to reliance on caregivers, potentially preventing the emergence or deterioration of behavioral issues over time, while also improving maternal mental health. Overall, evaluating the model’s efficacy in our cultural context contributes to a broader understanding of how culturally sensitive parenting programs can be effectively implemented. Although the literature highlights the significance of maternal mental health and family dynamics in influencing child behavior, there remains a gap in research validating the OMPM in our specific cultural context. This study aims to fill this gap by evaluating the model’s effectiveness in promoting positive mother-child interactions and reducing behavioral difficulties among children with motor disabilities.
Materials and Methods
The present study employed a quasi-experimental design with a pre-test and post-test, incorporating a control group and a two-month follow-up. The target population consisted of boys aged 8 to 11 years with motor disabilities enrolled in special schools for children with physical and motor issues in Qazvin City during the 2023-2024 academic year. The decision to focus solely on boys was based on epidemiological data indicating a higher prevalence of motor disabilities among males, often with a male-to-female ratio of approximately 2:1 to 3:1 [15]. Additionally, boys tend to exhibit higher rates of externalizing behaviors, such as aggression and rule-breaking, which are often more prominent in this population [16]. A total of 30 participants and their mothers were selected through convenience sampling. The sample size was determined based on a similar study [17], with a type I error rate of 0.05, power of 0.8, and anticipated dropout rate of 25%. Using the sample size formula (Equation 1) and inclusion criteria, participants were randomly assigned to either the experimental or control group using simple randomization, resulting in 15 individuals in each group:
The inclusion criteria for the study were as follows: Both mothers and children had to be willing to cooperate; mothers needed to have at least a middle school certificate to complete written assignments during the intervention sessions; children should not have had any sensory impairments, such as vision or hearing problems, or neurological conditions, such as or attention deficit/hyperactivity disorder (based on parents’ reports), mothers should not have had mental disorders that could hinder their participation in the intervention sessions, as assessed through their own reports; and children had to have a T-score between 60 and 63 on the Achenbach child behavior checklist (ACBCL) to identify externalizing difficulties. Participants were excluded if they had participated in similar parent management programs within the previous six months or were currently involved in such programs. Additionally, incomplete questionnaire submissions also resulted in exclusion from the study.
The mental health inventory (MHI): The MHI is a 38-item instrument designed to measure well-being and mental distress, and has been validated in four large samples of participants aged 13 to 69 years across four large samples [18]. The purpose of this study was to evaluate participants’ overall mental health status, providing a reliable and valid tool for the Iranian population. The MHI’s psychometric properties, including high internal consistency and stability over time, support its suitability for this context. To streamline assessment, we used the shortened MHI-18 version, which assesses anxiety, depression, emotional ties, behavioral control, and positive affect—core components linked to mental well-being and distress [18]. The Persian MHI-18 has demonstrated excellent factorial validity, with two primary factors: Well-being (positive affect and emotional ties) and mental distress (depression, anxiety, and behavioral control), and a Cronbach’s α of 0.75, indicating good internal consistency. The use of the MHI-18 in this study was justified by its brevity, psychometric robustness, and established validity in Iranian samples [19].
The ACBCL: The ACBCL is a comprehensive tool designed to assess a wide range of behavioral and emotional problems in children aged 6 to 18. In this study, we used the Persian version to evaluate externalizing difficulties, specifically aggression and rule-breaking behaviors, as primary outcome measures. The ACBCL consists of 113 items rated on a three-point scale, completed by parents familiar with their child’s behavior. This study aimed to identify behavioral problems associated with internalizing and externalizing disorders, focusing on externalizing difficulties relevant to our intervention. The ACBCL has demonstrated good psychometric properties in the Iranian population, with reliability coefficients ranging from 0.48 to 0.85 for subscales [20]. The items cover various domains, such as withdrawal/depression, anxiety/depression, somatic complaints, social problems, thought problems, rule-breaking, attention problems, and aggressive behaviors. Factor analysis by Achenbach identified eight factors, with withdrawal, anxiety/depression, and somatic complaints reflecting internalizing difficulties, and rule-breaking and aggression indicating externalizing problems. Cronbach’s α for the scales ranged between 0.65 and 0.85, and for the eight subscales, it ranged from 0.48 to 0.75 [20]. In our study, we focused on evaluating externalizing difficulties, specifically aggression and rule-breaking behaviors, as these are crucial markers of outward behavioral issues. The Persian version of the ACBCL has been validated, with established cutoff scores of 60-63 and 63 and higher to identify borderline or clinical levels of these problems. The temporal stability of the scales was assessed using coefficients ranging from 0.32 to 0.67. In this study, only externalizing difficulties and their factors (aggression and rule-breaking behaviors) were evaluated as the primary outcome measures [21].
OMPM: The OMPM program is a type of therapeutic training that includes weekly sessions in which a therapist works with the parents of a family. The children do not participate in these sessions, and the intervention aims to replace parents’ coercive parenting methods with effective parenting strategies. Role-playing is an essential mechanism in the sessions, with the therapist using it to demonstrate good and bad examples and identify which parenting skills require attention, training, and practice. Once parents have practiced the parenting skills sufficiently, the therapist and parents select a specific situation for the next session, during which parents try to apply the newly acquired skills at home. Between sessions, the therapist contacted the parents to provide support and answer their questions. The duration of therapy depends on the family’s needs and progress during treatment, but it typically lasts for 10-15 weekly sessions. In the present study, parents received the intervention from two certified therapists who had completed a comprehensive 10-session parent management program [9] (Table 1).
Research procedure
After obtaining ethical approval, an introductory letter was prepared for the Exceptional Education Organization in Qazvin City. A meeting with relevant officials facilitated the identification of an educational center specializing in children with motor disabilities, and permission was obtained to access the facility. Following an explanation of the study’s objectives and procedures, written informed consent was obtained from mothers willing to participate. The mothers completed the ACBCL, and from the pool of children scoring between 60 and 63, 30 children were randomly selected and assigned to either the experimental or control group, with 15 children in each. To minimize measurement bias, assessors responsible for administering and scoring the questionnaires were blinded to the group assignments. The experimental group received the OMPM intervention in 10 training sessions, each lasting 90 minutes. Conversely, the control group participated in routine family education sessions at the center, designed to provide foundational parenting guidance without focusing on the specific content of the experimental program. The control group’s sessions, conducted over seven weekly meetings of approximately 30 minutes, covered topics, such as child growth and development, communication strategies, discipline techniques, and emotional support. The sessions combined lectures, interactive discussions, and informational resources to enhance general parenting skills. All mothers completed the MHI and the ACBCL at three intervals: pre-intervention, post-intervention, and two months after the intervention. The collected data were analyzed using chi-square tests, t-tests, and repeated-measures analysis of variance (ANOVA) in SPSS software, version 25.
Results
The participants’ Mean±SD ages 33.27±2.73 years for mothers and 9.70±0.87 years for children. The ages of children in the experimental and control groups were 9.77±0.85 and 9.63±0.89 years, respectively. Table 2 presents the demographic characteristics.
As indicated in Table 2 , the statistical analyses revealed no significant differences between the experimental and control groups concerning mothers’ educational levels, employment status, duration of marriage, family economic status, or children’s age (P>0.05).
Table 3 presents descriptive statistics (Mean±SD) for the mental health factors (well-being and mental distress) of mothers and externalizing difficulties and their factors (aggression and rule-breaking behaviors) in children with motor disabilities, differentiated by the experimental and control groups at the pre-test, post-test, and follow-up stages.
Table 3 presents the descriptive statistics, Mean±SD for maternal mental health factors (well-being and mental distress) and children’s externalizing difficulties (including aggression and rule-breaking behaviors) across pre-test, post-test, and follow-up assessments, differentiated by group. The data indicated that the experimental group experienced significant improvements in maternal well-being and reductions in mental distress. Specifically, maternal well-being scores increased from a pre-intervention Mean±SD of 32.8±5.199 to 38.93±6.112 at post-test, while mental distress scores decreased correspondingly. The control group showed no significant changes over time. Similarly, externalizing difficulties in children, particularly aggression, showed marked improvement: mean scores declined from 29.4±5.829 pre-intervention to 22.47±5.125 at follow-up in the experimental group, whereas the control group’s scores remained relatively stable. These results underscore the positive impact of the intervention on both maternal mental health and children’s behavioral issues.
The assumptions underlying repeated-measures ANOVA, normal distribution, and absence of outliers, were verified, with no violations detected. Mauchly’s sphericity test indicated violations for some variables, necessitating the use of Greenhouse-Geisser corrections (Table 4).
Table 4 presents the results of the chi-square test conducted to evaluate Mauchly’s sphericity assumption for mothers’ mental health factors, including well-being, mental distress, general mental health, as well as externalizing difficulties among children, focusing on aggression and rule-breaking. The findings indicate statistically significant results across various factors, with P<0.001 for well-being, mental distress, and general mental health, while rule-breaking showed a significant P of 0.002. The results of the chi-square test suggest that the variables exhibited significant differences that warranted the use of repeated-measures ANOVA to compare general mental health indicators and total externalizing difficulties between the experimental and control groups over the assessed time points (pre-test, post-test, and follow-up) (Table 5).
Table 5 summarizes the findings from repeated-measures ANOVA, indicating significant effects of time and group on maternal mental health (well-being and mental distress) and children’s externalizing behaviors. The experimental group demonstrated significant improvements over time: Such as, well-being (F [1, df], P<0.001, η²=0.861) and reduction in mental distress (F [1, df], P<0.016, η²=0.266). Similarly, there were significant decreases in aggression (F [1, df], P<0.001, η²=0.771) and rule-breaking behaviors (F [1, df], P<0.001, η²=0.722). The effect sizes indicate a strong impact of the intervention on these outcomes.
Finally, Table 6 presents independent t-tests comparing the groups at each time point. Pre-test comparisons across groups showed no statistically significant differences in any measure (P>0.05), with effect sizes being minimal (Cohen’s d≈-0.1 to 0.13), indicating negligible baseline differences in mental health and externalizing behaviors. However, at post-test, the experimental group demonstrated substantial improvements across most variables, with effect sizes ranging from large to very large: Well-being (d≈-1.36; 95% CI supporting this magnitude), total externalizing behaviors (d≈2.56), aggression (d≈1.61), and rule-breaking (d≈2.79). These effect sizes, exceeding the threshold for large effects (d≥0.8), indicate meaningful and practically significant changes. Furthermore, the effect persisted at follow-up, with effect sizes remaining large (d>1.9), underscoring the durable impact of the intervention on enhancing children’s mental health and reducing externalizing difficulties.
Discussion
This study investigated the effectiveness of the OMPM program on the mental health of Iranian mothers caring for children with motor disabilities and externalizing behavioral difficulties. The primary hypothesis was that the OMPM would enhance effective parenting skills, thereby alleviating maternal mental health problems and reducing externalizing behaviors in children.
Initial findings demonstrated that participation in the OMPM significantly improved maternal well-being and decreased mental distress, with these benefits maintained at two-month follow-up. These results are consistent with prior research [5, 17, 22], suggesting that the program enhances emotional awareness, enabling mothers to respond more consciously and calmly to their children’s challenging behaviors. Such improvements facilitate closer mother-child interactions, promote emotional regulation, and diminish impulsive reactions rooted in prior stressors [22, 23].
The mechanisms underlying these outcomes involve mothers learning strategies that help them disengage from automatic, reactive responses, thereby encouraging more rational decision-making amid emotionally charged situations. As mothers become more aware of their emotional reactions, they tend to regulate their responses more effectively, which enhances both their emotional well-being and capacity to cope with daily stressors [3]. Increased emotional awareness further fosters empathy for children’s feelings, encourages reflective pauses before reacting, and contributes to sustained improvements in maternal mental health [5].
Although the intervention successfully mitigated maternal mental distress, it did not significantly influence broader measures of mental health. This aligns with existing literature emphasizing the complex bidirectional relationship between maternal mental health and child behavioral challenges. Maternal depressive symptoms and low self-efficacy are associated with greater behavioral issues in children [24]. However, these factors are influenced by persistent mental health challenges that may not be entirely alleviated through brief intervention alone. It should be noted that this study relied on self-report measures, which, while valuable, may be subject to bias and may not fully capture the nuanced dynamics of maternal mental health. Future interventions should aim to include targeted mental health support alongside parenting programs to foster more comprehensive improvements. It is also important to acknowledge that this study relied on self-reported assessments of mental well-being and distress from the mothers involved. While these self-reported measures may reveal positive therapeutic effects, improvements in mental health could be attributed to various factors outside the intervention itself. Nonetheless, it is plausible to argue that the mental health inventory utilized in this study sufficiently captured mothers’ health-related responses and experiences [25]. Future interventions should focus on enhancing maternal skills to better support mothers facing significant mental distress, rather than expecting that participation in the OMPM program alone will yield substantial improvements in general mental health outcomes.
Regarding children’s externalizing behaviors, the OMPM yielded significant reductions in aggression, rule-breaking, and overall externalizing difficulties, consistent with previous literature findings [26]. The intervention appeared to primarily influence behaviors within the home environment, as teachers did not report similar improvements, indicating possible contextual limitations of generalizability outside the family setting.
The core premise of the OMPM suggests that improvements in maternal parenting skills translate into decreased externalizing difficulties. Mothers learn to avoid negative reactions and employ more effective discipline strategies, which are critical in managing externalizing problems [10, 24]. Effect size analyses indicated that reductions in aggression, rule-breaking, and total externalizing behaviors were meaningful, although the small sample size limited subgroup analyses, particularly for children with more severe issues. It is plausible that children with higher initial severity may benefit the most from such interventions [25].
To elucidate potential mediators, factors, such as maternal education, consistency in parenting practices, and children’s emotional regulation should be explored in future research [27]. The sustained improvement observed at follow-up suggests that mothers felt more confident and effective post-intervention, which may have created a positive feedback loop, improving both their mental health and their children’s behaviors [28].
Despite these encouraging results, several limitations must be considered. The small sample size of 30 participants (15 per group), recruited via convenience sampling, constrains the statistical power and limits the generalizability of the results to broader populations. This sampling approach may also introduce selection bias, further affecting the external validity. Although the sample size was comparable to prior research [17], further studies should aim for larger, randomly selected samples to facilitate more comprehensive subgroup analyses and confirm the robustness of these findings. It is important to note that this study focused exclusively on boys, primarily because epidemiological data indicate a higher prevalence of motor disabilities among males and the tendency for boys to exhibit more externalizing behaviors, such as aggression, which are often linked to such disabilities. While this focus provides valuable insights into this subgroup, it limits the applicability of the findings to girls. Including both genders in future research would enhance the generalizability and allow exploration of potential gender-specific responses to interventions. A notable limitation of this study is the reliance on self-report questionnaires to assess maternal mental health and child behavior. This method is susceptible to various biases, such as social desirability and recall bias, which can affect data accuracy. Furthermore, the quasi-experimental design lacking randomization restricts causal inferences, and the absence of long-term follow-up prevents evaluation of the sustainability of intervention effects over time. To address these limitations, future research should incorporate larger, more diverse samples, utilize objective assessment measures alongside self-reports, and adopt longitudinal designs. Including data from fathers and other caregivers may also provide a more comprehensive understanding of familial influences on child outcomes.
Conclusion
Based on the findings, it can be concluded that OMPM intervention has a positive impact on the two factors of mental health (well-being and mental distress) of mothers and externalizing difficulties in children with motor disabilities, with effects persisting even after a two-month follow-up. As OMPM is a cost-effective approach, policymakers and therapists can utilize the results of this study to inform decisions that benefit children with motor disabilities and their families. Given the individual, familial, and societal costs associated with externalizing difficulties in childhood, there has been increasing attention on risk factors for the development of these difficulties and the effectiveness of intervention services. Parenting management programs are well-established based on theories and research highlighting the link between ineffective parenting and children’s externalizing difficulties. However, many children with externalizing difficulties are also clinically challenged by internalizing problems that may manifest as externalizing difficulties.
This area of research—whether (PMT) programs addressing ineffective parenting practices also positively affect childhood internalizing issues—has received less attention. Nonetheless, based on the current findings, several hypotheses can be proposed. First, designing and implementing PMT programs that include changes in warmth, hostility, and behavior control may effectively address both externalizing and internalizing difficulties. Therefore, concurrently examining internalizing issues in children is recommended, given the complex interactions among parenting behaviors, internalizing, and externalizing difficulties. Second, there is a strong association between maternal hostility and child behavioral outcomes, suggesting that non-hostile maternal behavior should be explicitly targeted in management programs, despite being indirectly addressed in most interventions. Third, mothers alone cannot fully resolve or reduce their children’s externalizing difficulties (as indicated by effect sizes); thus, interventions must be broader than just mother management training, incorporating elements, such as teaching self-regulation to children and reducing family stress.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.132). Informed consent was obtained from all mothers of children included in the study.
Funding
This study was extracted from the master's thesis of Narjes Shakibamehr, approved by the Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. This study was supported in part by the Deputy of Research and Technology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization: Narjes Shakibamehr, Masoume Pourmohamadreza-Tajrishi, and Mohsen Vahedi; Supervision, methodology, validation, analysis and writing the original draft: Masoume Pourmohamadreza-Tajrishi and Mohsen Vahedi; Investigation: Narjes Shakibamehr; Review and editing: Masoume Pourmohamadreza-Tajrishi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to all mothers and their children with motor disabilities for participating in this study.
References
- Olusanya BO, Kancherla V, Shaheen A, Ogbo FA, Davis AC. Global and regional prevalence of disabilities among children and adolescents: Analysis of findings from global health databases. Frontiers in Public Health. 2022; 10:977453. [DOI:10.3389/fpubh.2022.977453] [PMID]
- Veisani Y, Delpisheh A, Moradi G, Hassanzadeh J, Sayehmiri K. Inequality in addiction and mental disorders in 6818 suicide attempts: Determine of positive contribution of determinants by decomposition method. Iranian Journal of Public Health. 2017; 46(6):796. [Link]
- Pourmohamadreza Tajrishi M, Tarrah Hamed Nezam R, Movallali G. Effect of a behavioral support program on the social skills of male children with biomotor disabilities. Archives of Rehabilitation. 2019; 20(2):98-113. [DOI:10.32598/rj.20.2.98]
- Mattson G, Kuo DZ, Committee on Psychosocial Aspects of Child and Family Health, Council on Children With Disabilities, Yogman M, Baum R, et al. Psychosocial factors in children and youth with special health care needs and their families. Pediatrics. 2019; 143(1):e20183171. [DOI:10.1542/9781610023658-part07-psychosocial_factors]
- Shiri E, Behzadpoor S. The effectiveness of family-based behavior therapy on behavioral excesses of iranian young children with autism via telehealth. Practice in Clinical Psychology. 2025; 13(1):57-70. [DOI:10.32598/jpcp.13.1.987.1]
- Thijssen J, Vink G, Muris P, de Ruiter C. The effectiveness of parent management training-oregon model in clinically referred children with externalizing behavior problems in the Netherlands. Child Psychiatry and Human Development. 2017; 48(1):136-150. [DOI:10.1007/s10578-016-0660-5] [PMID]
- Marquis SM, McGrail K, Hayes M. Mental health of parents of children with a developmental disability in British Columbia, Canada. Journal of Epidemiology and Community Health. 2020; 74(2):173-8. [DOI:10.1136/jech-2018-211698] [PMID]
- Amaral S, Dinarte-Diaz L, Dominguez P, Perez-Vincent SM. Helping families help themselves: The (Un) intended impacts of a digital parenting program. Journal of Development Economics. 2024; 166:103181. [DOI:10.1016/j.jdeveco.2023.103181]
- Forgatch MS, Gewirtz AH. The evolution of the oregon model of parent management training. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York: The Guilford Press; 2017. [Link]
- Pourmohamadreza-Tajrishi M, Ashouri M, Afrooz GA, Arjmandnia AA, Ghobari-Bonab B. [The effectiveness of positive parenting program (triple-P) training on interaction of mother-child with intellectual disability (Persian)]. Rehabilitation. 2015; 16(2):128-37. [Link]
- Tellegen CL, Sanders MR. Stepping stones triple P-positive parenting program for children with disability: A systematic review and meta-analysis. Research in Developmental Disabilities. 2013; 34(5):1556-71. [DOI:10.1016/j.ridd.2013.01.022] [PMID]
- Ashori M, Afrooz GA, Arjmandnia AA, Pourmohamadreza-Tajrishi M, Ghobari-Bonab B. Group positive parenting program (triple-P) and the relationships of mother-child with intellectual disability. Practice in Clinical Psychology. 2015; 3(1):31-8. [Link]
- Preiß J, Lang A, Hauser T, Angerer M, Schernhardt P, Schabus M. Maternal characteristics and their relation to early mother-child interaction and cognitive development in toddlers. Plos One. 2025; 20(1):e0301876. [DOI:10.1371/journal.pone.0301876] [PMID]
- Aghakeshmiri A, Soleimanian AA, Golpich Z. An integrative parenting program for adoptive families: A mixed-method study. Practice in Clinical Psychology. 2024; 12(2):137-52. [DOI:10.32598/jpcp.12.2.924.1]
- Tsai CF, Guo HR, Tseng YC, Lai DC. Sex and geographic differences in the prevalence of reported childhood motor disability and their trends in Taiwan. BioMed Research International. 2018; 2018:6754230. [DOI:10.1155/2018/6754230] [PMID]
- Petersen MK. Gender differences in preshool conduct disorder symptoms across one-year [master thesis]. Lexington: University of Kentucky; 2024. [Link]
- Kajbaf MB, Shirazi Tehrani AR, Mirdrikvand F, Mazaheri M. [The effectiveness of parent behavioral management training on general health of mothers with hyperactivity children (Persian)]. Journal of Family Research. 2015; 11(1):103-22. [Link]
- Veit CT, Ware JE Jr. The structure of psychological distress and well-being in general populations. Journal of Consulting and Clinical Psychology. 1983; 51(5):730-42. [DOI:10.1037/0022-006X.51.5.730] [PMID]
- Meybodi FA, Saeedi Z, Behjati Z, Noorbala F, Dastbaravardec A, Enjedany E. Reliability and validity of a Farsi version of 18-item Mental Health Inventory. Procedia-Social and Behavioral Sciences. 2011; 30:1425-9. [DOI:10.1016/j.sbspro.2011.10.277]
- Achenbach TM. Child behavior checklist. In: Kreutzer JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. New York: Springer; 2011. [DOI:10.1007/978-0-387-79948-3_1529]
- Minaee A. [Adaptation and standardization of child behavior checklist, youth self-report, and teacher’s report forms (Persian)]. Journal of Exceptional Children. 2006; 6(1):529-58. [Link]
- Kosari F, Sabahi P, Makvand Hosseini S. Comparative effects of parent management training combined with ACT and mindful parenting on parent-child relationship. Journal of Research and Health. 2024; 14(2):177-88. [DOI:10.32598/JRH.14.2.1543.2]
- Shokri A, Kazemi R, Narimani M, Taklavi S. Comparison of the effectiveness of mother’s mindfulness-based cognitive therapy and cognitive emotion regulation training on externalizing disorder and self-efficacy of aggressive children. Practice in Clinical Psychology. 2020; 8(2):85-98. [DOI:10.32598/jpcp.8.2.677.1]
- Ahun MN, Ali NB, Hentschel E, Jeong J, Franchett E, Yousafzai AK. A meta-analytic review of the implementation characteristics in parenting interventions to promote early child development. Annals of the New York Academy of Sciences. 2024; 1533(1):99-144. [DOI:10.1111/nyas.15110] [PMID]
- Al Sager A, Goodman SH, Jeong J, Bain PA, Ahun MN. Effects of multi-component parenting and parental mental health interventions on early childhood development and parent outcomes: A systematic review and meta-analysis. Lancet Child Adolesc Health. 2024; 8(9):656-69. [DOI:10.1016/S2352-4642(24)00134-2] [PMID]
- Hermanns JM, Asscher JJ, Zijlstra BJ, Hoffenaar PJ, Dekovič M. Long-term changes in parenting and child behavior after the Home-Start family support program. Children and Youth Services Review. 2013; 35(4):678-84. [DOI:10.1016/j.childyouth.2013.01.017]
- Salma J, Febriana A, Ikasari FS. The role of communication and family parenting patterns in preventing bullying behavior. Holistic Journal of Nursing Studies. 2025; 1(1):36-43. [DOI:10.64621/hjns.v1i1.27]
- Rademacher A, Zumbach J, Koglin U. Parenting style and child aggressive behavior from preschool to elementary school: The mediating effect of emotion dysregulation. Early Childhood Education Journal. 2025; 53(1):63-72. [DOI:10.1007/s10643-023-01560-1]
Article type: Original Research Articles |
Subject:
Psychology
Received: 2025/04/18 | Accepted: 2025/07/29 | Published: 2025/12/1
Received: 2025/04/18 | Accepted: 2025/07/29 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
