
988368
Wed, Jul 29, 2026

Volume 23, Issue 3 (September 2025)
Iranian Rehabilitation Journal 2025, 23(3): 339-350 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghanbarian K, Dalvand H, AlizadehKhoei M, Salmani F, Mehri A. Relationship of Executive Functions with Manual Dexterity and Instrumental Activities of Daily Living in Older Adults With and Without Mild Cognitive Impairment. Iranian Rehabilitation Journal 2025; 23 (3) :339-350
URL: http://irj.uswr.ac.ir/article-1-2539-en.html
URL: http://irj.uswr.ac.ir/article-1-2539-en.html



1- Department of Aging Health & Geriatric, School of Rehabilitation, Tehran University of Medical Sciences (TUMS), Tehran, Iran.
2- Department of Occupational Therapy, School of Rehabilitation, Tehran University of Medical Sciences (TUMS), Tehran, Iran. & Department of Occupational Therapy, School of Rehabilitation, Al-Subtain University, International Branch of TUMS, Karbala, Iraq.
3- Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences (TUMS), Tehran, Iran.
4- Geriatric Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
2- Department of Occupational Therapy, School of Rehabilitation, Tehran University of Medical Sciences (TUMS), Tehran, Iran. & Department of Occupational Therapy, School of Rehabilitation, Al-Subtain University, International Branch of TUMS, Karbala, Iraq.
3- Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences (TUMS), Tehran, Iran.
4- Geriatric Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
Keywords: Older adults, Instrumental activities of daily living (IADLs), Mild cognitive impairment (MCI), Executive functions (EFs), Manual dexterity
Full-Text [PDF 544 kb]
(959 Downloads)
| Abstract (HTML) (3178 Views)
Full-Text: (450 Views)
Introduction
Cognitive impairment is a major clinical concern, characterized by problems with memory, attention, and problem-solving skills. It significantly reduces the quality of life of older adults and their families [1], underscoring the need to identify contributing factors, such as executive functions (EFs). EFs are higher-level cognitive processes that manage thoughts and actions [2] and include key components such as inhibition in cognition status, planning, flexibility in attention, decision-making, and problem-solving [2].
Early assessment of EFs can help predict the onset of mild cognitive impairment (MCI) [3]. Strong EFs are critical for maintaining independence in daily life and assessing functional levels, particularly in instrumental activities of daily livings (IADLs) [4], even in the presence of cognitive impairments [5]. EF tests are commonly used during routine check-ups to obtain crucial information about cognitive abilities essential for managing daily activities [6].
Another crucial factor in maintaining independence in daily life is manual dexterity, the ability to skillfully manipulate objects using different grip hand patterns [7]. Impairments in either the dominant or non-dominant hand (or both) can severely limit functionality, especially in IADLs [8]. Unlike basic tasks (ADLs), IADLs demand higher cognitive processing, making individuals more vulnerable to cognitive decline. Consequently, older adults with MCI often struggle more than those without cognitive problems, needing extra time and making more errors during daily tasks, such as using public transportation, organizing items, or managing medications [9].
In this context, hand performance in tasks, such as gripping, lifting, and manipulating objects can significantly influence EFs, such as attention, problem-solving, planning, cognitive flexibility, and self-control [10]. Therefore, the ability to use hands effectively is essential for maintaining independence in older adults. Any decline in these abilities can impair the performance of IADLs, ultimately leading to greater dependence and a lower quality of life [4]. However,, understanding the relationship between EFs and IADLs is crucial for identifying individuals with MCI, as early interventions can manage the progression of cognitive decline [11]. Treatments aimed at improving EFs can help maintain independence [12]. Therefore, this study aimed to explore the relationships between EFs with manual dexterity and IADLs in older adults with MCI, and to compare these factors in those without cognitive impairment.
Materials and Methods
Subjects and sampling
In this case-control study, 64 older adults ≥60 years old (32 diagnosed with MCI and the remaining without cognitive impairment), who visited the geriatric clinic of Ziaeian Hospital at Tehran University of Medical Sciences and a day care center, were selected through a random sampling method, for face-to-face interviews from May to September, 2024. First, the assessor screened older adult outpatients for eligibility and willingness to participate in this study. The inclusion criteria included right-handed older adults without obvious physical impairments (e.g. speech disabilities, motor/physical difficulties), with normal or corrected vision and hearing, scoring <9 based on the geriatric depression scale (GDS)-15 tool (indicating no depression), and providing informed consent via signature or fingerprint. Outpatients who were not expected to continue their cooperation were excluded. Participants in the case group were included if they had been diagnosed with MCI using the Persian version of the clinical dementia rating (CDR) tool [13].
Background variables
Demographic data (age and sex) were collected. The Persian version of the GDS-15 [14] was employed to assess depression.
Cognition assessment measurement
The Persian version of the CDR tool was used to screen for cognitive status. This tool is one of the most reliable and effective screening tools for cognitive status, consisting of two main components: Memory and orientation. Memory includes remote, recent, immediate, and highly learned material, while orientation includes time, place, and person. A final score of 0 indicates no cognitive impairment, 0.5 signifies MCI, and 1 indicates dementia [13].
EFs assessment measurement
The Tower of London (ToL), Wisconsin card sorting test (WCST), and trail making test A and B (TMT-A and TMT-B) were used to assess EF of the participants in this study.
The computer version of the ToL was used in this study. The ToL was developed to evaluate at least two aspects of EFs: Strategic planning and problem-solving. The participants were presented with 12 challenges that required them to arrange the sample shape by moving colored plates (green, blue, and red) into the correct positions with the fewest necessary movements. Each challenge can be attempted up to three times. After a successful attempt (and if the challenge remains unsolved after three attempts), the next challenge is presented. The test was graded based on the total test time, total delay time, total number of errors, and total points [15].
In this study, a computer version of the WCST was used. In the WCST, the participant is presented with a deck of 64 cards, each featuring a shape with four symbols: a triangle, star, plus, and circle, in four colors: red, green, yellow, and blue. Naturally, no two cards are identical. Four cards, including “A red triangle, two green stars, three yellow pluses, and four blue circles,” served as the main cards. The participants’ task is to place the other cards under the main cards according to the rules governing them. After each response, participants received feedback indicating whether their answers were correct or incorrect. The desired pattern for the four main cards is color, form, and number, repeated twice (C, F, N, C, F, N). Once the participants provided a sufficient number of consecutive correct answers, the desired pattern changed, but the participants remained unaware of this change and must discover it independently. The test grading is based on the number of categories completed, the number of errors in persistence, the correct and incorrect responses, the duration of the test, and the conceptual level of responses. [16].
The TMT-A requires participants to draw lines that consecutively connect 25 circles on a piece of paper. The task requirements for the TMT-B are similar, except that the individual must alternate between numbers and letters (e.g. 1, A, 2, B, 3, C). The score for Part A reflected the time taken to complete the task, while for Part B, the total number of errors was recorded [17].
Manual dexterity assessment measurement
The Purdue Pegboard test (PPT) was used to assess the manual dexterity of the older adult participants in this study. The PPT consists of a rectangular board featuring two rows of holes (20-25 in number) on each side and three circular cups. The first cup contained pins, the second cup held washers, and the third cup had collars. A movable board covered all three cups. This test measured the speed and accuracy of the participants’ hand movements. The participant must remove the pins, washers, and collars one by one with the dominant hand (right), once with the non-dominant hand (left), and once with both hands simultaneously, placing them into the holes. The given time was 30 s, and at the end of this test, the number of pins placed in the holes was counted [18].
IADLs assessment measurement
The IADLs-Lawton tool was used for the IADLs assessment of the participants in this study. It comprises eight items: Telephone use, shopping, food preparation, house cleaning and laundry, transportation, medication management, and money management. Each item is scored as 0 (lower ability) or 1 (higher ability), with a total score of 8 reflecting full independent functioning [19].
Statistical analysis
Data were analyzed utilizing SPSS software, version 27. All analyses were considered statistically significant at P<0.05. Quantitative variables were described using central tendency and dispersion indices, while qualitative variables were represented using counts and percentages. The assumption of normality was assessed using the Shapiro-Wilk test. Spearman’s test is employed to examine the relationships between variables. The mean differences between the two groups were analyzed using the Mann-Whitney test.
Results
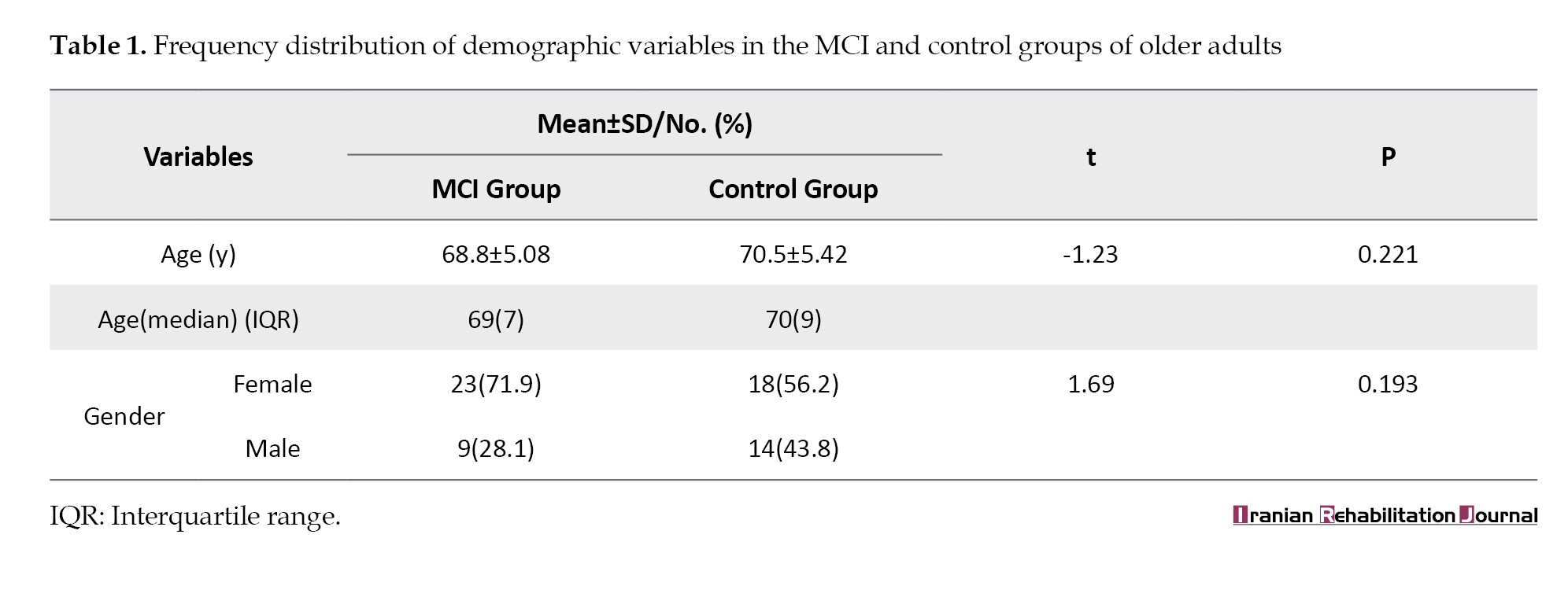
The mean age of the older adult participants in the MCI group was 68.88±5.08 years, while in the control group, it was 70.5±5.42 years. No significant differences in age were observed between the two groups (t=-1.23; P=0.221). In the MCI group, 71.9% (n=23) were female, and 28.1% (n=9) were male, whereas the control group consisted of 56.2% (n=18) females and 43.8% (n=14) males. No statistically significant differences in sex distribution were observed between the two groups (t=1.69; P=0.193) (Table 1).
EFs in older adults with and without MCI
The results of the independent-samples Mann-Whitney test showed statistically significant differences between the two groups for all components of the ToL test. The MCI group required more time to complete the test (t=5.7; P<0.001), made more errors (t=8.797; P<0.001), and ultimately obtained a lower overall score (t=-6.441; P<0.001) compared to the control group.
For the WCST, all measures showed a significant difference between the two groups, indicating that compared to the control group, the MCI group responded to fewer categories (t=-6.286; P<0.001), had more errors (t=6.822; P<0.001) and incorrect responses (t=6.544; P<0.001), and required more time to complete the test (t=4.014; P<0.001) (Table 2).
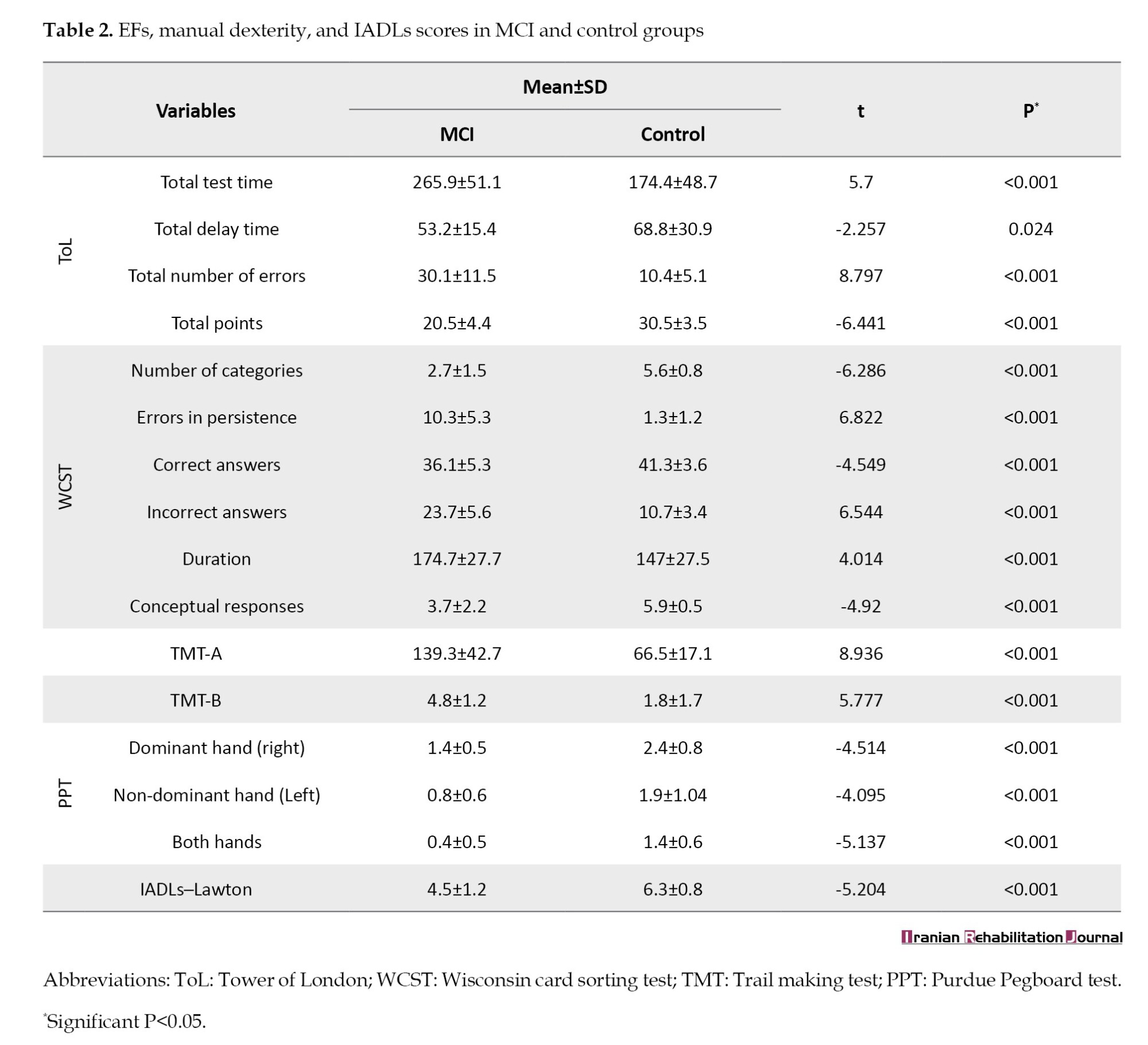
The results for the TMT showed a significant difference between the two groups. The MCI group took a longer time to complete the TMT-A (t=8.936; P<0.001) and also made more mistakes in TMT-B (t=5.777; P<0.001) compared to the control group (Table 2).
Manual dexterity in older adults with and without MCI
The results of the independent-samples Mann-Whitney test indicated statistically significant differences between the two groups for all PPT subtasks. This revealed that individuals with MCI placed fewer pins with their dominant (right) hand (t=-4.514; P<0.001), non-dominant (left) hand (t=-4.095; P<0.001) and both hands simultaneously (t=-5.137; P<0.001) in the holes compared to the control group (Table 2).
IADLs in older adults with and without MCI
The MCI group scored lower than the control group using the IADLs-Lawton tool (t=-5.204; P<0.001), showing that individuals with MCI may struggle with higher-level functional activities, which could impact their independence level and overall quality of life (Table 2).
Relationships between EFs and manual dexterity
Spearman correlation in the MCI group revealed several associations with the third subtask of the PPT; ToL points correlated positively (r=0.529; P=0.002), indicating better PPT performance with higher ToL scores. Errors in persistence in WCST correlated negatively (r=-0.418; P=0.017), indicating that more errors were associated with poorer PPT performance. Correct answers in WCST showed a positive association (r=0.418; P=0.017), while incorrect answers in WCST had a negative correlation (r=-0.37; P=0.037), indicating better PPT performance with higher correct answers and lower incorrect answers. Longer TMT-A completion times were negatively associated with poorer PPT performance (r=-0.454; P=0.009), indicating a link between longer time and worse PPT performance (Table 3).
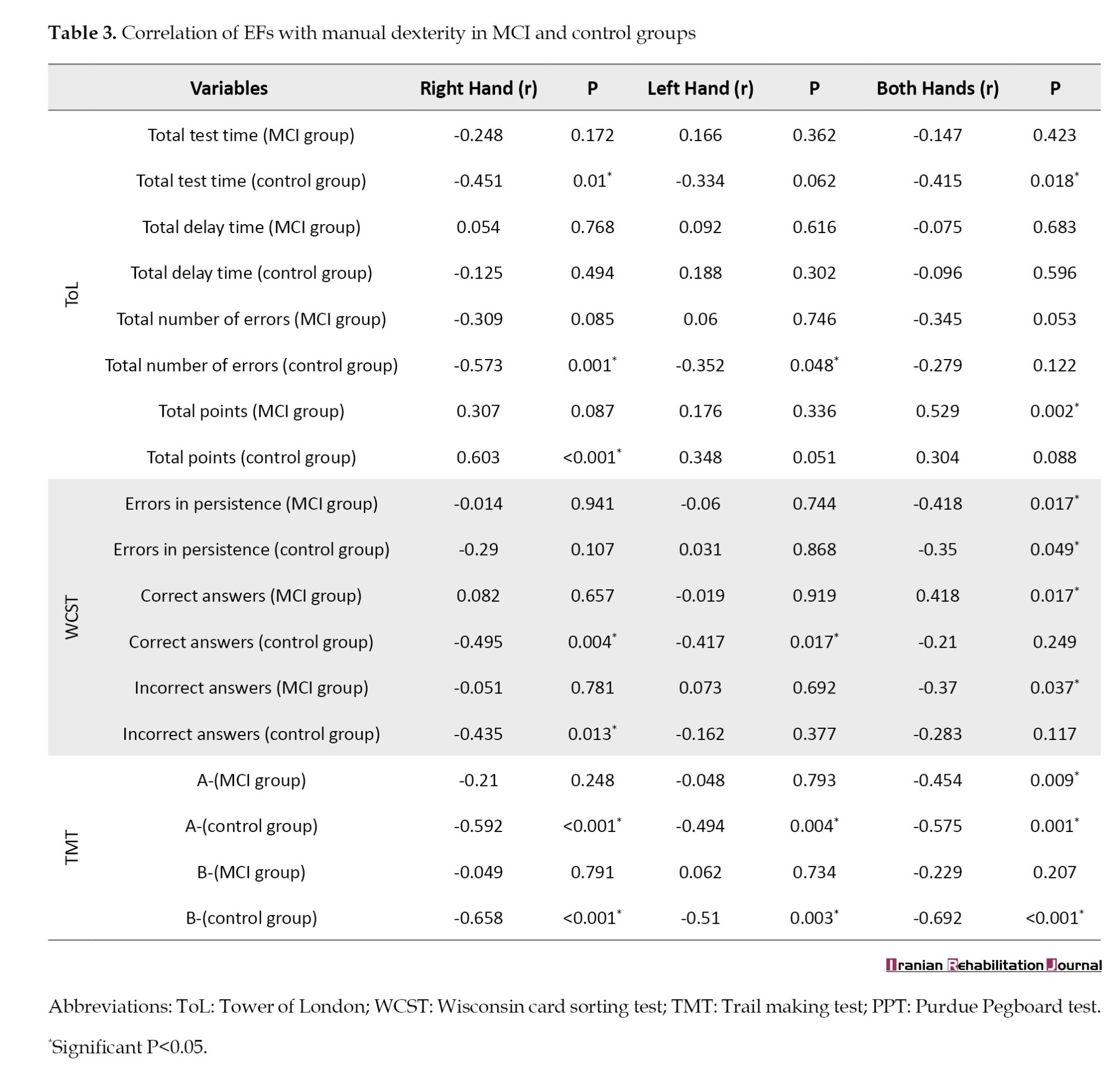
In the control group, the total test time in ToL negatively correlated with PPT subtasks one (r=-0.451; P=0.01) and three (r=-0.415; P=0.018), indicating slower ToL completion linked to poorer PPT performance. The total errors in the ToL were negatively correlated with PPT subtasks one (r=-0.573; P= 0.001) and two (r=-0.352; P=0.048), indicating that more errors were associated with poorer PPT performance. Higher total points in the ToL are associated with better performance in PPT subtask one (r=0.603; P<0.001). Errors in persistence in WCST negatively correlated with PPT subtask three (r=-0.35; P=0.049), and incorrect answers in WCST negatively correlated with PPT subtask one (r=-0.435; P=0.013), indicating more errors and incorrect answers linked to poorer PPT performance. TMT-A completion time negatively correlated with all PPT subtasks (subtask one: r=-0.592; P<0.001; subtask two: r=-0.494; P=0.004; subtask three: r=-0.575; P=0.001), and TMT-B errors negatively correlated with all PPT subtasks (subtask one: r=-0.658; P<0.001; subtask two: r=-0.51; P=0.003; subtask three: r=-0.692; P<0.001), showing higher completion time and errors in TMT associated with poorer PPT performance (Table 3).
Relationships between EFs and IADLs-Lawton
By performing Spearman correlation, it was shown that in the MCI group, total points were positively associated with the IADLs-Lawton score (r=0.425; P=0.015), indicating that the higher the total points participants had in the ToL, the higher their score in the IADLs. Persistence errors were negatively linked with the IADLs score (r=-0.538; P=0.002), indicating that the more individuals made perseveration errors in the WCST, the lower their score was in the IADLs. Correct answers were positively associated with the IADLs score (r=0.52; P=0.002), indicating that the more correct answers older adults had in the WCST, the higher their score in the IADLs. Incorrect answers were negatively correlated with the IADLs score (r=-0.454; P=0.009), indicating that the more individuals had incorrect answers in the WCST, the lower their score was in the IADLs. TMT-A performance was negatively associated with the IADLs score (r=-0.397; P=0.025), indicating that the more time participants spent completing the TMT-A, the lower their score was on the IADLs (Table 4).
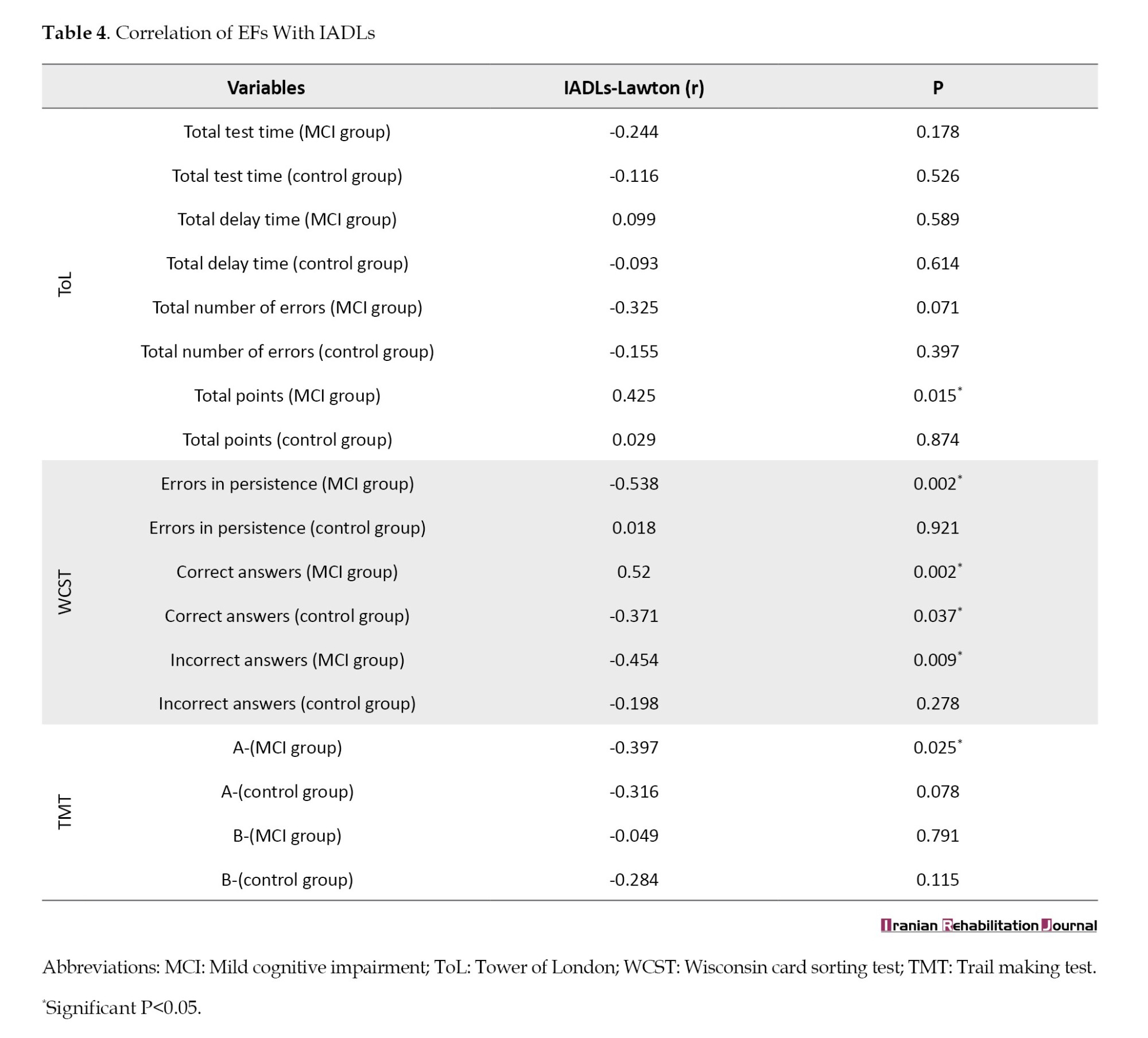
In the control group, correct answers were negatively associated with the IADLs score (r=-0.371; P=0.037), indicating that the more correct answers older adults had in the WCST, the lower their score was in the IADLs (Table 4).
Discussion
EFs in older adults with and without MCI
The findings of this study indicated that older adults with MCI exhibit significantly poorer EFs than cognitively healthy older adults. This is consistent with research indicating that individuals with MCI struggle with response inhibition, task switching, cognitive flexibility, and abstract reasoning—all key components of executive functioning. Additionally, studies have shown that individuals with MCI exhibited notable deficits in EFs, as measured by the Stroop test and the modified WCST (in terms of number of errors and perseverations), suggesting that these impairments reflect broader executive dysfunction in MCI [20, 21]. Another study demonstrated that patients with MCI show impairments in planning, problem-solving, and cognitive flexibility, as evidenced by their performance on the ToL and WCST [22]. This exhibition of poorer EFs in individuals with MCI results from structural brain atrophy, neurotransmitter deficits, disrupted neural networks, vascular damage, and failing compensatory mechanisms, which make it harder for MCI patients to perform tasks requiring planning, skill, working memory, and cognitive flexibility compared to cognitively healthy older adults [2, 23].
However, the results of a study revealed that older adults with amnestic MCI showed no significant differences from controls in performing certain executive tasks, such as the TMT-B. This may be attributed to the fact that amnestic MCI primarily affects memory-related brain regions (e.g. hippocampus and medial temporal lobes). At the same time, frontal lobe-dependent EFs may initially remain relatively unaffected [24]. Another study showed that individuals in the early stages of MCI performed normally on EFs tests. As the disease progresses, impairments in their EFs become apparent, which may be due to the early stages of MCI involving localized pathology (e.g. medial temporal atrophy), sparing frontal networks. However, as neurodegeneration spreads (e.g. extension to the prefrontal cortex), EFs decline [25].
Manual dexterity in older adults with and without MCI
The findings of this study showed that the MCI group performed worse in manual dexterity skills compared to the control group. A study indicated that patients with MCI exhibit deficits in fine motor control, as observed in their performance using the PPT in tasks involving picking up and inserting pins, which require precise finger and hand movements. The presence of these deficits was confirmed by a higher number of errors in the MCI group compared to the control group. Furthermore, errors such as dropping pins or incorrect pin selection were related to incorrect finger movements during task performance [26]. In another study [27], a decline in manual dexterity was observed in the MCI group using the PPT, which could indicate deterioration in the interactions between cognitive and motor functions. According to Rattanawan, this is due to neurodegeneration in individuals with MCI, which disrupts the integrative networks needed for skilled hand movements, particularly those involving executive-motor coordination [28].
However, the results of one study showed that performance based on manual dexterity tests (such as the Purdue Pegboard or grooved Pegboard) was similar in the MCI group and healthy older adults, especially in cases of amnestic MCI, which primarily affects memory and does not impact other cognitive domains. This may be due to the preservation of primary motor networks in the early stages of MCI; while motor impairments usually become apparent in more advanced stages [29].
IADLs in older adults with and without MCI
Based on the results of this study, the group with MCI performed worse on IADL activities compared to the control group, according to the IADLs-Lawton tool. Although studies confirm that patients with MCI have less ability to perform IADL activities compared to cognitively healthy individuals, the extent of this impairment may be too subtle for some measurement tools. For example, when assessing IADLs, the Lawton and Brody tools may lack sufficient sensitivity to detect minor but clinically significant changes [30]. Researchers [31] found that IADLs requiring greater cognitive resources are affected in individuals with MCI, and that MCI has a significant impact on IADLs, particularly in items related to financial management, use of transportation, and tasks related to household chores. This is because these complex activities require higher-level cognitive abilities such as planning, executive decision-making, and task switching, which are often impaired in patients with MCI. The findings of a decreased ability to perform IADLs highlight the need for early diagnosis and targeted interventions to maintain functional independence and optimize well-being in individuals with MCI [32].
Meanwhile, the results of the study [33] showed that compared to healthy older adult individuals, the group with amnestic MCI (those who only have memory impairment) did not exhibit a significant difference in IADLs performance. A significant decline in the ability to perform IADLs was observed only when MCI progressed to dementia.
Relationship between EFs and manual dexterity in older adults with and without MCI
In this study, a significant relationship was found between EFs and manual dexterity in both groups. A previous study [34] identified associations between hand function (measured by grip strength, finger tapping, and the Grooved Pegboard test) and cognitive abilities (EFs, attention, visuospatial skills, and processing speed) in older adults with MCI or dementia.
Moreover, studies have shown that weaker grip strength is associated with poorer cognitive performance, especially in processing speed and EFs [35, 36]. EFs are essential for manual skills, particularly for performing tasks that require fine motor control and coordination of both hands. The strong correlation between assessments of EFs and manual dexterity tests emphasizes the close relationship between cognitive and motor abilities in older adults. Impairments in EF (higher error rates, slower processing speed, and reduced cognitive flexibility) can lead to decreased movement accuracy and motor performance [37].
Although most studies confirm the relationship between EFs and manual dexterity in older adults with MCI, research [38] has reported that this relationship is weak or insignificant. Specifically, after controlling for diseases such as diabetes and arthritis, the association between EFs and manual dexterity in older adults with MCI decreased and became statistically insignificant, indicating that confounding variables, such as comorbid underlying diseases, influenced this relationship.
Relationship between EFs and IADLs in older adults with and without MCI
A significant relationship was observed between EFs and performing IADLs in both groups. The results of a study [33] showed that impairment in EFs is significantly associated with a reduced ability to perform IADLs, and this association is independent of disease diagnosis, cognitive impairment, memory function, and depression. Additionally, executive dysfunction was linearly related to a decline in IADL performance across each diagnostic group (healthy individuals, MCI, and mild Alzheimer’s), highlighting the crucial role of EFs in maintaining independence in daily life. Additionally, the researchers noted that [2] difficulties in problem-solving, cognitive flexibility, and processing speed can lead to challenges in managing complex daily activities, such as handling finances and performing household tasks.
In contrast, some studies have not reported a significant relationship between EFs and IADLs in healthy older adults or individuals with MCI. A study [39] found that in cognitively normal older adults, the relationship between EFs (such as planning and response inhibition) and IADL performance became weak and non-significant after controlling for age and education level. This could be attributed to greater cognitive reserve in older adults with higher education levels. Healthy older adults with higher education levels or those who engage in regular mental activities may utilize compensatory mechanisms that help maintain their ability to perform IADLs, even in the presence of mild decline in EF.
Another study found that in the early stages of MCI, the decline in IADL performance is more strongly associated with impairments in memory and processing speed rather than EFs, as many IADLs (such as medication management) rely more on episodic memory (remembering timing and details) and processing speed (responding quickly to changes) rather than complex planning (EFs) [2].
The first limitation of this study was that, due to its cross-sectional design, it could not predict the long-term outcomes of cognitive impairment on motor function in older adults. The second limitation was the use of numerous tools to assess EFs, which could introduce bias into the results by causing fatigue in the participants, particularly in the MCI group. Third, since part of the sample was collected from a geriatric clinic, older adults often attended with their caregivers, and as a result, caregivers sometimes answered the questions on behalf of the older adults during the interviews.
Conclusion
This study demonstrated that older adults with MCI, compared to cognitively healthy peers, performed worse on EFs and manual dexterity tests and scored lower on the IADLs-Lawton tool. The significant correlation between EFs and manual dexterity indicated that, in general, the more time individuals spent completing EF tests and the more errors they made, the poorer their performance was on the manual dexterity test. Additionally, the significant correlation between EFs and IADLs showed that having a higher number of incorrect responses and lower scores on EF tests was associated with lower scores on the IADLs-Lawton tool. These results highlight the importance of assessing cognitive and motor abilities to facilitate early interventions and support to achieve independence. Combining cognitive and motor education programs with caregiver training can effectively address these challenges.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.MEDICINE.REC.1403.058). Regarding ethical considerations, eligible older adult participants who agreed to contribute to the study signed or fingerprinted an informed consent form. To further protect participants, interviews were conducted privately, and their rights and confidentiality were respected.
Funding
This study was extracted from the master's thesis of Kosar Ghanbarian, approved by the Department of Aging Health & Geriatric, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. This study was financially supported by Tehran University of Medical Science, Tehran, Iran.
Authors' contributions
Conceptualization, supervision and methodology: Hamid Dalvand and Mahtab Alizadeh-Khoei; Investigation: Fatemeh Salmani; Writing the original draft: Kosar Ghanbarian; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors gratefully acknowledge the contributions of the medical team at Geriatric Clinic of Ziaeian Hospital and the community staff at Day Care Center for their support in participant recruitment and data collection. Their cooperation was essential to the success of this study. The authors also thank the participants who generously contributed their time to this study.
References
Cognitive impairment is a major clinical concern, characterized by problems with memory, attention, and problem-solving skills. It significantly reduces the quality of life of older adults and their families [1], underscoring the need to identify contributing factors, such as executive functions (EFs). EFs are higher-level cognitive processes that manage thoughts and actions [2] and include key components such as inhibition in cognition status, planning, flexibility in attention, decision-making, and problem-solving [2].
Early assessment of EFs can help predict the onset of mild cognitive impairment (MCI) [3]. Strong EFs are critical for maintaining independence in daily life and assessing functional levels, particularly in instrumental activities of daily livings (IADLs) [4], even in the presence of cognitive impairments [5]. EF tests are commonly used during routine check-ups to obtain crucial information about cognitive abilities essential for managing daily activities [6].
Another crucial factor in maintaining independence in daily life is manual dexterity, the ability to skillfully manipulate objects using different grip hand patterns [7]. Impairments in either the dominant or non-dominant hand (or both) can severely limit functionality, especially in IADLs [8]. Unlike basic tasks (ADLs), IADLs demand higher cognitive processing, making individuals more vulnerable to cognitive decline. Consequently, older adults with MCI often struggle more than those without cognitive problems, needing extra time and making more errors during daily tasks, such as using public transportation, organizing items, or managing medications [9].
In this context, hand performance in tasks, such as gripping, lifting, and manipulating objects can significantly influence EFs, such as attention, problem-solving, planning, cognitive flexibility, and self-control [10]. Therefore, the ability to use hands effectively is essential for maintaining independence in older adults. Any decline in these abilities can impair the performance of IADLs, ultimately leading to greater dependence and a lower quality of life [4]. However,, understanding the relationship between EFs and IADLs is crucial for identifying individuals with MCI, as early interventions can manage the progression of cognitive decline [11]. Treatments aimed at improving EFs can help maintain independence [12]. Therefore, this study aimed to explore the relationships between EFs with manual dexterity and IADLs in older adults with MCI, and to compare these factors in those without cognitive impairment.
Materials and Methods
Subjects and sampling
In this case-control study, 64 older adults ≥60 years old (32 diagnosed with MCI and the remaining without cognitive impairment), who visited the geriatric clinic of Ziaeian Hospital at Tehran University of Medical Sciences and a day care center, were selected through a random sampling method, for face-to-face interviews from May to September, 2024. First, the assessor screened older adult outpatients for eligibility and willingness to participate in this study. The inclusion criteria included right-handed older adults without obvious physical impairments (e.g. speech disabilities, motor/physical difficulties), with normal or corrected vision and hearing, scoring <9 based on the geriatric depression scale (GDS)-15 tool (indicating no depression), and providing informed consent via signature or fingerprint. Outpatients who were not expected to continue their cooperation were excluded. Participants in the case group were included if they had been diagnosed with MCI using the Persian version of the clinical dementia rating (CDR) tool [13].
Background variables
Demographic data (age and sex) were collected. The Persian version of the GDS-15 [14] was employed to assess depression.
Cognition assessment measurement
The Persian version of the CDR tool was used to screen for cognitive status. This tool is one of the most reliable and effective screening tools for cognitive status, consisting of two main components: Memory and orientation. Memory includes remote, recent, immediate, and highly learned material, while orientation includes time, place, and person. A final score of 0 indicates no cognitive impairment, 0.5 signifies MCI, and 1 indicates dementia [13].
EFs assessment measurement
The Tower of London (ToL), Wisconsin card sorting test (WCST), and trail making test A and B (TMT-A and TMT-B) were used to assess EF of the participants in this study.
The computer version of the ToL was used in this study. The ToL was developed to evaluate at least two aspects of EFs: Strategic planning and problem-solving. The participants were presented with 12 challenges that required them to arrange the sample shape by moving colored plates (green, blue, and red) into the correct positions with the fewest necessary movements. Each challenge can be attempted up to three times. After a successful attempt (and if the challenge remains unsolved after three attempts), the next challenge is presented. The test was graded based on the total test time, total delay time, total number of errors, and total points [15].
In this study, a computer version of the WCST was used. In the WCST, the participant is presented with a deck of 64 cards, each featuring a shape with four symbols: a triangle, star, plus, and circle, in four colors: red, green, yellow, and blue. Naturally, no two cards are identical. Four cards, including “A red triangle, two green stars, three yellow pluses, and four blue circles,” served as the main cards. The participants’ task is to place the other cards under the main cards according to the rules governing them. After each response, participants received feedback indicating whether their answers were correct or incorrect. The desired pattern for the four main cards is color, form, and number, repeated twice (C, F, N, C, F, N). Once the participants provided a sufficient number of consecutive correct answers, the desired pattern changed, but the participants remained unaware of this change and must discover it independently. The test grading is based on the number of categories completed, the number of errors in persistence, the correct and incorrect responses, the duration of the test, and the conceptual level of responses. [16].
The TMT-A requires participants to draw lines that consecutively connect 25 circles on a piece of paper. The task requirements for the TMT-B are similar, except that the individual must alternate between numbers and letters (e.g. 1, A, 2, B, 3, C). The score for Part A reflected the time taken to complete the task, while for Part B, the total number of errors was recorded [17].
Manual dexterity assessment measurement
The Purdue Pegboard test (PPT) was used to assess the manual dexterity of the older adult participants in this study. The PPT consists of a rectangular board featuring two rows of holes (20-25 in number) on each side and three circular cups. The first cup contained pins, the second cup held washers, and the third cup had collars. A movable board covered all three cups. This test measured the speed and accuracy of the participants’ hand movements. The participant must remove the pins, washers, and collars one by one with the dominant hand (right), once with the non-dominant hand (left), and once with both hands simultaneously, placing them into the holes. The given time was 30 s, and at the end of this test, the number of pins placed in the holes was counted [18].
IADLs assessment measurement
The IADLs-Lawton tool was used for the IADLs assessment of the participants in this study. It comprises eight items: Telephone use, shopping, food preparation, house cleaning and laundry, transportation, medication management, and money management. Each item is scored as 0 (lower ability) or 1 (higher ability), with a total score of 8 reflecting full independent functioning [19].
Statistical analysis
Data were analyzed utilizing SPSS software, version 27. All analyses were considered statistically significant at P<0.05. Quantitative variables were described using central tendency and dispersion indices, while qualitative variables were represented using counts and percentages. The assumption of normality was assessed using the Shapiro-Wilk test. Spearman’s test is employed to examine the relationships between variables. The mean differences between the two groups were analyzed using the Mann-Whitney test.
Results
The mean age of the older adult participants in the MCI group was 68.88±5.08 years, while in the control group, it was 70.5±5.42 years. No significant differences in age were observed between the two groups (t=-1.23; P=0.221). In the MCI group, 71.9% (n=23) were female, and 28.1% (n=9) were male, whereas the control group consisted of 56.2% (n=18) females and 43.8% (n=14) males. No statistically significant differences in sex distribution were observed between the two groups (t=1.69; P=0.193) (Table 1).
EFs in older adults with and without MCI
The results of the independent-samples Mann-Whitney test showed statistically significant differences between the two groups for all components of the ToL test. The MCI group required more time to complete the test (t=5.7; P<0.001), made more errors (t=8.797; P<0.001), and ultimately obtained a lower overall score (t=-6.441; P<0.001) compared to the control group.
For the WCST, all measures showed a significant difference between the two groups, indicating that compared to the control group, the MCI group responded to fewer categories (t=-6.286; P<0.001), had more errors (t=6.822; P<0.001) and incorrect responses (t=6.544; P<0.001), and required more time to complete the test (t=4.014; P<0.001) (Table 2).
The results for the TMT showed a significant difference between the two groups. The MCI group took a longer time to complete the TMT-A (t=8.936; P<0.001) and also made more mistakes in TMT-B (t=5.777; P<0.001) compared to the control group (Table 2).
Manual dexterity in older adults with and without MCI
The results of the independent-samples Mann-Whitney test indicated statistically significant differences between the two groups for all PPT subtasks. This revealed that individuals with MCI placed fewer pins with their dominant (right) hand (t=-4.514; P<0.001), non-dominant (left) hand (t=-4.095; P<0.001) and both hands simultaneously (t=-5.137; P<0.001) in the holes compared to the control group (Table 2).
IADLs in older adults with and without MCI
The MCI group scored lower than the control group using the IADLs-Lawton tool (t=-5.204; P<0.001), showing that individuals with MCI may struggle with higher-level functional activities, which could impact their independence level and overall quality of life (Table 2).
Relationships between EFs and manual dexterity
Spearman correlation in the MCI group revealed several associations with the third subtask of the PPT; ToL points correlated positively (r=0.529; P=0.002), indicating better PPT performance with higher ToL scores. Errors in persistence in WCST correlated negatively (r=-0.418; P=0.017), indicating that more errors were associated with poorer PPT performance. Correct answers in WCST showed a positive association (r=0.418; P=0.017), while incorrect answers in WCST had a negative correlation (r=-0.37; P=0.037), indicating better PPT performance with higher correct answers and lower incorrect answers. Longer TMT-A completion times were negatively associated with poorer PPT performance (r=-0.454; P=0.009), indicating a link between longer time and worse PPT performance (Table 3).
In the control group, the total test time in ToL negatively correlated with PPT subtasks one (r=-0.451; P=0.01) and three (r=-0.415; P=0.018), indicating slower ToL completion linked to poorer PPT performance. The total errors in the ToL were negatively correlated with PPT subtasks one (r=-0.573; P= 0.001) and two (r=-0.352; P=0.048), indicating that more errors were associated with poorer PPT performance. Higher total points in the ToL are associated with better performance in PPT subtask one (r=0.603; P<0.001). Errors in persistence in WCST negatively correlated with PPT subtask three (r=-0.35; P=0.049), and incorrect answers in WCST negatively correlated with PPT subtask one (r=-0.435; P=0.013), indicating more errors and incorrect answers linked to poorer PPT performance. TMT-A completion time negatively correlated with all PPT subtasks (subtask one: r=-0.592; P<0.001; subtask two: r=-0.494; P=0.004; subtask three: r=-0.575; P=0.001), and TMT-B errors negatively correlated with all PPT subtasks (subtask one: r=-0.658; P<0.001; subtask two: r=-0.51; P=0.003; subtask three: r=-0.692; P<0.001), showing higher completion time and errors in TMT associated with poorer PPT performance (Table 3).
Relationships between EFs and IADLs-Lawton
By performing Spearman correlation, it was shown that in the MCI group, total points were positively associated with the IADLs-Lawton score (r=0.425; P=0.015), indicating that the higher the total points participants had in the ToL, the higher their score in the IADLs. Persistence errors were negatively linked with the IADLs score (r=-0.538; P=0.002), indicating that the more individuals made perseveration errors in the WCST, the lower their score was in the IADLs. Correct answers were positively associated with the IADLs score (r=0.52; P=0.002), indicating that the more correct answers older adults had in the WCST, the higher their score in the IADLs. Incorrect answers were negatively correlated with the IADLs score (r=-0.454; P=0.009), indicating that the more individuals had incorrect answers in the WCST, the lower their score was in the IADLs. TMT-A performance was negatively associated with the IADLs score (r=-0.397; P=0.025), indicating that the more time participants spent completing the TMT-A, the lower their score was on the IADLs (Table 4).
In the control group, correct answers were negatively associated with the IADLs score (r=-0.371; P=0.037), indicating that the more correct answers older adults had in the WCST, the lower their score was in the IADLs (Table 4).
Discussion
EFs in older adults with and without MCI
The findings of this study indicated that older adults with MCI exhibit significantly poorer EFs than cognitively healthy older adults. This is consistent with research indicating that individuals with MCI struggle with response inhibition, task switching, cognitive flexibility, and abstract reasoning—all key components of executive functioning. Additionally, studies have shown that individuals with MCI exhibited notable deficits in EFs, as measured by the Stroop test and the modified WCST (in terms of number of errors and perseverations), suggesting that these impairments reflect broader executive dysfunction in MCI [20, 21]. Another study demonstrated that patients with MCI show impairments in planning, problem-solving, and cognitive flexibility, as evidenced by their performance on the ToL and WCST [22]. This exhibition of poorer EFs in individuals with MCI results from structural brain atrophy, neurotransmitter deficits, disrupted neural networks, vascular damage, and failing compensatory mechanisms, which make it harder for MCI patients to perform tasks requiring planning, skill, working memory, and cognitive flexibility compared to cognitively healthy older adults [2, 23].
However, the results of a study revealed that older adults with amnestic MCI showed no significant differences from controls in performing certain executive tasks, such as the TMT-B. This may be attributed to the fact that amnestic MCI primarily affects memory-related brain regions (e.g. hippocampus and medial temporal lobes). At the same time, frontal lobe-dependent EFs may initially remain relatively unaffected [24]. Another study showed that individuals in the early stages of MCI performed normally on EFs tests. As the disease progresses, impairments in their EFs become apparent, which may be due to the early stages of MCI involving localized pathology (e.g. medial temporal atrophy), sparing frontal networks. However, as neurodegeneration spreads (e.g. extension to the prefrontal cortex), EFs decline [25].
Manual dexterity in older adults with and without MCI
The findings of this study showed that the MCI group performed worse in manual dexterity skills compared to the control group. A study indicated that patients with MCI exhibit deficits in fine motor control, as observed in their performance using the PPT in tasks involving picking up and inserting pins, which require precise finger and hand movements. The presence of these deficits was confirmed by a higher number of errors in the MCI group compared to the control group. Furthermore, errors such as dropping pins or incorrect pin selection were related to incorrect finger movements during task performance [26]. In another study [27], a decline in manual dexterity was observed in the MCI group using the PPT, which could indicate deterioration in the interactions between cognitive and motor functions. According to Rattanawan, this is due to neurodegeneration in individuals with MCI, which disrupts the integrative networks needed for skilled hand movements, particularly those involving executive-motor coordination [28].
However, the results of one study showed that performance based on manual dexterity tests (such as the Purdue Pegboard or grooved Pegboard) was similar in the MCI group and healthy older adults, especially in cases of amnestic MCI, which primarily affects memory and does not impact other cognitive domains. This may be due to the preservation of primary motor networks in the early stages of MCI; while motor impairments usually become apparent in more advanced stages [29].
IADLs in older adults with and without MCI
Based on the results of this study, the group with MCI performed worse on IADL activities compared to the control group, according to the IADLs-Lawton tool. Although studies confirm that patients with MCI have less ability to perform IADL activities compared to cognitively healthy individuals, the extent of this impairment may be too subtle for some measurement tools. For example, when assessing IADLs, the Lawton and Brody tools may lack sufficient sensitivity to detect minor but clinically significant changes [30]. Researchers [31] found that IADLs requiring greater cognitive resources are affected in individuals with MCI, and that MCI has a significant impact on IADLs, particularly in items related to financial management, use of transportation, and tasks related to household chores. This is because these complex activities require higher-level cognitive abilities such as planning, executive decision-making, and task switching, which are often impaired in patients with MCI. The findings of a decreased ability to perform IADLs highlight the need for early diagnosis and targeted interventions to maintain functional independence and optimize well-being in individuals with MCI [32].
Meanwhile, the results of the study [33] showed that compared to healthy older adult individuals, the group with amnestic MCI (those who only have memory impairment) did not exhibit a significant difference in IADLs performance. A significant decline in the ability to perform IADLs was observed only when MCI progressed to dementia.
Relationship between EFs and manual dexterity in older adults with and without MCI
In this study, a significant relationship was found between EFs and manual dexterity in both groups. A previous study [34] identified associations between hand function (measured by grip strength, finger tapping, and the Grooved Pegboard test) and cognitive abilities (EFs, attention, visuospatial skills, and processing speed) in older adults with MCI or dementia.
Moreover, studies have shown that weaker grip strength is associated with poorer cognitive performance, especially in processing speed and EFs [35, 36]. EFs are essential for manual skills, particularly for performing tasks that require fine motor control and coordination of both hands. The strong correlation between assessments of EFs and manual dexterity tests emphasizes the close relationship between cognitive and motor abilities in older adults. Impairments in EF (higher error rates, slower processing speed, and reduced cognitive flexibility) can lead to decreased movement accuracy and motor performance [37].
Although most studies confirm the relationship between EFs and manual dexterity in older adults with MCI, research [38] has reported that this relationship is weak or insignificant. Specifically, after controlling for diseases such as diabetes and arthritis, the association between EFs and manual dexterity in older adults with MCI decreased and became statistically insignificant, indicating that confounding variables, such as comorbid underlying diseases, influenced this relationship.
Relationship between EFs and IADLs in older adults with and without MCI
A significant relationship was observed between EFs and performing IADLs in both groups. The results of a study [33] showed that impairment in EFs is significantly associated with a reduced ability to perform IADLs, and this association is independent of disease diagnosis, cognitive impairment, memory function, and depression. Additionally, executive dysfunction was linearly related to a decline in IADL performance across each diagnostic group (healthy individuals, MCI, and mild Alzheimer’s), highlighting the crucial role of EFs in maintaining independence in daily life. Additionally, the researchers noted that [2] difficulties in problem-solving, cognitive flexibility, and processing speed can lead to challenges in managing complex daily activities, such as handling finances and performing household tasks.
In contrast, some studies have not reported a significant relationship between EFs and IADLs in healthy older adults or individuals with MCI. A study [39] found that in cognitively normal older adults, the relationship between EFs (such as planning and response inhibition) and IADL performance became weak and non-significant after controlling for age and education level. This could be attributed to greater cognitive reserve in older adults with higher education levels. Healthy older adults with higher education levels or those who engage in regular mental activities may utilize compensatory mechanisms that help maintain their ability to perform IADLs, even in the presence of mild decline in EF.
Another study found that in the early stages of MCI, the decline in IADL performance is more strongly associated with impairments in memory and processing speed rather than EFs, as many IADLs (such as medication management) rely more on episodic memory (remembering timing and details) and processing speed (responding quickly to changes) rather than complex planning (EFs) [2].
The first limitation of this study was that, due to its cross-sectional design, it could not predict the long-term outcomes of cognitive impairment on motor function in older adults. The second limitation was the use of numerous tools to assess EFs, which could introduce bias into the results by causing fatigue in the participants, particularly in the MCI group. Third, since part of the sample was collected from a geriatric clinic, older adults often attended with their caregivers, and as a result, caregivers sometimes answered the questions on behalf of the older adults during the interviews.
Conclusion
This study demonstrated that older adults with MCI, compared to cognitively healthy peers, performed worse on EFs and manual dexterity tests and scored lower on the IADLs-Lawton tool. The significant correlation between EFs and manual dexterity indicated that, in general, the more time individuals spent completing EF tests and the more errors they made, the poorer their performance was on the manual dexterity test. Additionally, the significant correlation between EFs and IADLs showed that having a higher number of incorrect responses and lower scores on EF tests was associated with lower scores on the IADLs-Lawton tool. These results highlight the importance of assessing cognitive and motor abilities to facilitate early interventions and support to achieve independence. Combining cognitive and motor education programs with caregiver training can effectively address these challenges.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.MEDICINE.REC.1403.058). Regarding ethical considerations, eligible older adult participants who agreed to contribute to the study signed or fingerprinted an informed consent form. To further protect participants, interviews were conducted privately, and their rights and confidentiality were respected.
Funding
This study was extracted from the master's thesis of Kosar Ghanbarian, approved by the Department of Aging Health & Geriatric, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. This study was financially supported by Tehran University of Medical Science, Tehran, Iran.
Authors' contributions
Conceptualization, supervision and methodology: Hamid Dalvand and Mahtab Alizadeh-Khoei; Investigation: Fatemeh Salmani; Writing the original draft: Kosar Ghanbarian; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors gratefully acknowledge the contributions of the medical team at Geriatric Clinic of Ziaeian Hospital and the community staff at Day Care Center for their support in participant recruitment and data collection. Their cooperation was essential to the success of this study. The authors also thank the participants who generously contributed their time to this study.
References
- Ben Ayed I, Ammar A, Boujelbane MA, Salem A, Naija S, Amor SB, et al. Acute effect of simultaneous exercise and cognitive tasks on cognitive functions in elderly individuals with mild cognitive impairment. Diseases. 2024; 12(7):148.[DOI:10.3390/diseases12070148] [PMID]
- Corbo I, Casagrande M. Higher-Level executive functions in healthy elderly and mild cognitive impairment: A systematic review. Journal of Clinical Medicine. 2022; 11(5):1204. [DOI:10.3390/jcm11051204] [PMID]
- García-García-Patino R, Benito-León J, Mitchell AJ, Pastorino-Mellado D, García García R, Ladera-Fernández V, et al. Memory and executive dysfunction predict complex activities of daily living impairment in amnestic multi-domain mild cognitive impairment. Journal of Alzheimer's Disease. 2020; 75(3):1061-9. [DOI:10.3233/JAD-191263] [PMID]
- Mansbach WE, Mace RA. Predicting functional dependence in mild cognitive impairment: Differential contributions of memory and executive functions. The Gerontologist. 2019; 59(5):925-35. [DOI:10.1093/geront/gny097] [PMID]
- Hunter EG, Kearney PJ. Occupational therapy interventions to improve performance of instrumental activities of daily living for community-dwelling older adults: A systematic review. The American Journal of Occupational Therapy. 2018; 72(4):7204190050p1-7204190050p9. [DOI:10.5014/ajot.2018.031062] [PMID]
- Punitha P, Jessy J. Effect of meta-cognitive strategy-based activities on executive functioning, social networking, and instrumental activities of daily living among women. Cureus. 2024; 16(4):e58698. [PMID]
- Jiménez-Barrios M, González-Bernal J, Santamaría-Peláez M, Collazo-Riobo C, Cubo E, Gabriel-Galán JMT, et al. Impact of a dynamic orthosis on manual dexterity among people with Parkinson’s disease: A randomized trial. The American Journal of Occupational Therapy. 2025; 79(1): 7901205110. [DOI:10.5014/ajot.2025.050723]
- Bouscaren N, Yildiz H, Dartois L, Vercambre MN, Boutron-Ruault MC. Decline in instrumental activities of daily living over 4-year: the association with hearing, visual and dual sensory impairments among non-institutionalized women. The Journal of Nutrition, Health & Aging. 2019; 23(8):687-93. [DOI:10.1007/s12603-019-1231-9] [PMID]
- Osman A, Radman D, Belchior P, Gélinas I. A systematic review of psychometric properties of questionnaires assessing activities of daily living among older adults with neurocognitive disorders. Australian Occupational Therapy Journal. 2025; 72(1):e13013. [DOI:10.1111/1440-1630.13013] [PMID]
- Ávila RT, de Paula JJ, Bicalho MA, Moraes EN, Nicolato R, Malloy-Diniz LF, et al. Working memory and cognitive flexibility mediates visuoconstructional abilities in older adults with heterogeneous cognitive ability. Journal of The International Neuropsychological Society. 2015; 21(5):392-8. [DOI:10.1017/S135561771500034X] [PMID]
- Zhao X, Liang W, Maes JHR. Associations between self- and informant-reported abilities of instrumental activities of daily living and cognitive functions in older adults with mild cognitive impairment. Archives of Clinical Neuropsychology. 2021; 36(5):723-33. [DOI:10.1093/arclin/acaa110] [PMID]
- Lahav O, Katz N. Independent older adult's IADL and executive function according to cognitive performance. OTJR: Occupation, Participation and Health. 2020; 40(3):183-9. [DOI:10.1177/1539449220905813] [PMID]
- Sharifi K. [Diagnostic accuracy comparison between the Persian versions of clinical dementia rating (P-CDR) and cognitive state test (P-COST) in the elderly dementia screening (Persian)]. Nursing And Midwifery Journal. 2016; 14(6):551-61. [Link]
- Malakouti SK, Fatollahi P, Mirabzadeh A, Salavati M, Zandi T. Reliability, validity and factor structure of the GDS-15 in Iranian elderly. International Journal of Geriatric Psychiatry. 2006; 21(6):588-93. [DOI:10.1002/gps.1533] [PMID]
- Hudon C, St-Hilaire A, Landry M, Belzile F, Macoir J. Normative data for the Tower of London (Drexel version) in the Quebec-French population aged between 50 and 88 years. Applied Neuropsychology. Adult. 2025; 32(4):953-9. [DOI:10.1080/23279095.2023.2227382] [PMID]
- Kopp B, Lange F, Steinke A. The reliability of the Wisconsin card sorting test in clinical practice. Assessment. 2021; 28(1):248-63. [DOI:10.1177/1073191119866257] [PMID]
- Simfukwe C, Youn YC, Kim SY, An SS. Digital trail making test-black and white: Normal vs MCI. Applied Neuropsychology. Adult. 2022; 29(6):1296-303. [DOI:10.1080/23279095.2021.1871615] [PMID]
- Rodríguez-Aranda C, Mittner M, Vasylenko O. Association between executive functions, working memory, and manual dexterity in young and healthy older adults: An exploratory study. Perceptual and Motor Skills. 2016; 122(1):165-92. [DOI:10.1177/0031512516628370] [PMID]
- Hassani Mehraban A, Soltanmohamadi Y, Akbarfahimi M, Taghizadeh G. Validity and reliability of the Persian version of Lawton instrumental activities of daily living scale in patients with dementia. Medical Journal of The Islamic Republic of Iran. 2014; 28:25. [PMID]
- Rattanavichit Y, Chaikeeree N, Boonsinsukh R, Kitiyanant K. The age differences and effect of mild cognitive impairment on perceptual-motor and executive functions. Frontiers in Psychology. 2022; 13:906898. [DOI:10.3389/fpsyg.2022.906898] [PMID]
- Guarino A, Forte G, Giovannoli J, Casagrande M. Executive functions in the elderly with mild cognitive impairment: a systematic review on motor and cognitive inhibition, conflict control and cognitive flexibility. Aging & Mental Health. 2020; 24(7):1028-45. [DOI:10.1080/13607863.2019.1584785] [PMID]
- Kobayashi-Cuya KE, Sakurai R, Sakuma N, Suzuki H, Yasunaga M, et al. Hand dexterity, not handgrip strength, is associated with executive function in Japanese community-dwelling older adults: A cross-sectional study. BMC Geriatrics. 2018; 18(1):192. [PMID]
- Corbo I, Troisi G, Marselli G, Casagrande M. The role of cognitive flexibility on higher level executive functions in mild cognitive impairment and healthy older adults. BMC Psychology. 2024; 12(1):317. [DOI:10.1186/s40359-024-01807-5] [PMID]
- Pagen LHG, van de Ven VG, Gronenschild EHBM, Priovoulos N, Verhey FRJ, Jacobs HIL. Contributions of cerebro-cerebellar default mode connectivity patterns to memory performance in mild cognitive impairment. Journal of Alzheimer's Disease. 2020; 75(2):633-47. [DOI:10.3233/JAD-191127] [PMID]
- Jobson DD, Hase Y, Clarkson AN, Kalaria RN. The role of the medial prefrontal cortex in cognition, ageing and dementia. Brain Communications. 2021; 3(3):fcab125. [DOI:10.1093/braincomms/fcab125] [PMID]
- Vasylenko O, Gorecka MM, Waterloo K, Rodríguez-Aranda C. Reduction in manual asymmetry and decline in fine manual dexterity in right-handed older adults with mild cognitive impairment. Laterality. 2022; 27(6):581-604. [DOI:10.1080/1357650X.2022.2111437] [PMID]
- Alfeo F, Lanciano T, Abbatantuono C, Gintili G, De Caro MF, Curci A, et al. Cognitive, emotional, and daily functioning domains involved in decision-making among patients with mild cognitive impairment: A systematic review. Brain Sciences. 2024; 14(3):278. [DOI:10.3390/brainsci14030278] [PMID]
- Rattanawan P. Correlations between hand dexterity and bimanual coordination on the activities of daily living in older adults with mild cognitive impairment. Dementia and Geriatric Cognitive Disorders Extra. 2022; 12(1):24-32. [DOI:10.1159/000521644] [PMID]
- Heintz Walters B, Huddleston WE, O’Connor K, Wang J, Hoeger Bement M, Keenan KG. The role of eye movements, attention, and hand movements on age-related differences in pegboard tests. Journal of Neurophysiology. 2021; 126(5):1710-22. [DOI:10.1152/jn.00629.2020] [PMID]
- Bahureksa L, Najafi B, Saleh A, Sabbagh M, Coon D, Mohler MJ, et al. The impact of mild cognitive impairment on gait and balance: A systematic review and meta-analysis of studies using instrumented assessment. Gerontology. 2017; 63(1):67-83. [DOI:10.1159/000445831] [PMID]
- Jekel K, Damian M, Wattmo C, Hausner L, Bullock R, Connelly PJ, et al. Mild cognitive impairment and deficits in instrumental activities of daily living: A systematic review. Alzheimer’s Research & Therapy. 2015; 7(1):17. [DOI:10.1186/s13195-015-0099-0]
- Wilson G. Functional adaptations to strength training in older adults: the influence of genetic variation, health status and physical characteristics [PhD dissertation]. Sydney: The University of Sydney; 2021. [Link]
- Ginsberg TB, Powell L, Emrani S, Wasserman V, Higgins S, Chopra A, et al. Instrumental activities of daily living, neuropsychiatric symptoms, and neuropsychological impairment in mild cognitive impairment. The Journal of the American Osteopathic Association. 2019; 119(2):96-101. [DOI:10.7556/jaoa.2019.015] [PMID]
- Hesseberg K, Tangen GG, Pripp AH, Bergland A. Associations between cognition and hand function in older people diagnosed with mild cognitive impairment or dementia. Dementia and Geriatric Cognitive Disorders Extra. 2020; 10(3):195-204. [DOI:10.1159/000510382]
- Hooghiemstra AM, Ramakers IHGB, Sistermans N, Pijnenburg YAL, Aalten P, Hamel REG, et al. Gait speed and grip strength reflect cognitive impairment and are modestly related to incident cognitive decline in memory clinic patients with subjective cognitive decline and mild cognitive impairment: Findings from the 4C study. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2017; 72(6):846-54. [DOI:10.1093/gerona/glx003] [PMID]
- Miyano I, Bae S, Lee S, Shimada H, Kitaoka H. Association between simple test assessing hand dexterity and mild cognitive impairment in independent older adults. International Journal of Geriatric Psychiatry. 2023; 38(1):e5862. [DOI:10.1002/gps.5862]
- Vasylenko O, Gorecka MM, Rodríguez‐Aranda C. Manual dexterity in young and healthy older adults. 2. Association with cognitive abilities. Developmental Psychobiology. 2018; 60(4):428-39. [DOI:10.1002/dev.21618] [PMID]
- Kiper P, Richard M, Stefanutti F, Pierson-Poinsignon R, Cacciante L, Perin C, et al. Combined motor and cognitive rehabilitation: the impact on motor performance in patients with mild cognitive impairment. Systematic review and meta-analysis. Journal of Personalized Medicine. 2022; 12(2):276. [DOI:10.3390/jpm12020276] [PMID]
- Mohammad N, Rezapour T, Kormi-Nouri R, Abdekhodaie E, Ghamsari AM, Ehsan HB, et al. The effects of different proxies of cognitive reserve on episodic memory performance: Aging study in Iran. International Psychogeriatrics. 2020; 32(1):25-34. [DOI:10.1017/S1041610219001613] [PMID]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2025/05/6 | Accepted: 2025/06/11 | Published: 2025/09/1
Received: 2025/05/6 | Accepted: 2025/06/11 | Published: 2025/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
