
988368
Thu, Jul 30, 2026

Volume 23, Issue 3 (September 2025)
Iranian Rehabilitation Journal 2025, 23(3): 351-358 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hussein Abed F, Jihad S K. Anxiety Levels Among Patients Following Ischemic Stroke: A Cross-sectional Study. Iranian Rehabilitation Journal 2025; 23 (3) :351-358
URL: http://irj.uswr.ac.ir/article-1-2541-en.html
URL: http://irj.uswr.ac.ir/article-1-2541-en.html



1- Department of Mental and Psychological Health, College of Nursing, University of Babylon, Hillah, Iraq.
2- Department of Community Health, College of Nursing, University of Babylon, Hillah, Iraq.
2- Department of Community Health, College of Nursing, University of Babylon, Hillah, Iraq.
Full-Text [PDF 493 kb]
(570 Downloads)
| Abstract (HTML) (2176 Views)
Full-Text: (360 Views)
Introduction
Anxiety is an essential human emotion, for example, a sensation of alarm, fear, and physiological tension on perceiving threats in the absence of immediate danger [1]. The American Psychiatric Association describes anxiety as anticipation of future danger, with associated dysphoric mood and bodily symptoms of increased arousal or tension in muscles [2]. Despite its universality as the most prevalent mental illness on Earth, anxiety is not diagnosed due to social stigma, treatment denial, or inappropriate diagnosis by medical practitioners [3]. It is a mindset that is an adaptive response to situational danger and is governed by the experience an individual has in life, cognitive appraisal, and environmental stressors [4].
Ischemic stroke, responsible for approximately 85% of all strokes, results from thrombosis or embolic occlusion of cerebral blood flow and causes neurological dysfunction [5]. The pathophysiology of two significant regions is at issue: the ischemic core, which results in permanent damage to the neurons, and the penumbra, a recoverable region of compromised perfusion [6]. Survivors of ischemic stroke have multifaceted problems, including physical dysfunction, protracted recovery periods, and psychosocial consequences of altered self-concept, dependency on others, and encounters with the medical system [7].
Post-stroke psychological morbidity is startlingly common, with up to 72% of survivors suffering disabling fatigue and clinically significant impairments in quality of life [8]. Of these, post-stroke anxiety (PSA) develops in 20–25% of patients, becoming a major hindrance to rehabilitation [9]. Emotional distress is greatest in the initial month following stroke but often persists chronically, contributing to functional impairment and difficulties in social reintegration. Concerns regarding recurrence, loss of independence, and disruption of daily routines are determinants of chronic anxiety [8].
Since the ratio of PSA is highly extensive and adversely impacts recovery results, the current study investigated anxiety levels among survivors of ischemic stroke, residents of Babylon Governorate, Iraq. It explores correlations with demographic and clinical factors. The detection of such trends is required to incorporate mental health interventions into stroke rehabilitation programs and maximize integrated patient care.
Materials and Methods
Study design
A quantitative cross-sectional study was conducted to assess anxiety levels among post-ischemic stroke patients in Babylon Governorate, Iraq. Data were collected between December 22, 2024, and March 2, 2025, within the overall study duration from October 15, 2024, to July 1, 2025. The study design followed the strengthening the reporting of observational studies in epidemiology guidelines to ensure methodological rigor [10].
Study setting: Data were collected in two central locations: Al-Imam Al Sadiq Teaching Hospital and Babylon Specialized Medical Rehabilitation Center, which were selected based on their high volume of patients undergoing post-stroke rehabilitation treatment.
Sampling and participants
A convenience sample of 100 participants was recruited for this study. The inclusion criteria included adults ≥18 years, first-ever definitive ischemic stroke on neuroimaging (computed tomography [CT]/magnetic resonance imaging [MRI]) within the previous 6–12 months, and cognitive capacity to participate (excluding severe dementia or aphasia) [11]. The exclusion criteria included pre-existing psychiatric illnesses (e.g. depression and generalized anxiety disorder) and severe physical disabilities that prevented communication. The sample size was computed using the Equation 1:
where Z=1.96 (95% confidence level), P=0.5 (expected prevalence), and d=0.10 (margin of error), which produces a minimum of 97 participants [12].
Data collection
This study used a three-section standardized questionnaire:
1) Sociodemographic characteristics included age (years), sex (male/female), residence (urban/rural), marital status (single/married/divorced/widowed), educational level (illiterate, primary, secondary, diploma/above), and monthly income (as “enough,” “barely enough,” or “not enough”). 2) Clinical data: History of smoking (current/former/none) and chronic disease (e.g. diabetes mellitus, hyperlipidemia, hypertension, and atherosclerosis). 3) Anxiety scale: The Hamilton rating scale for anxiety (HAM-A) was culturally modified (e.g. “insight” items were changed). It comprises 14 domains (e.g. anxious mood, somatic symptoms, insomnia) that are rated on a 3-point Likert scale: 1=always, 2=sometimes, 3=never. Scores were summed to range from 14 to 42 and categorized as mild (14–20), moderate (21–27), and severe (≥28). The Arabic version was tested on 10 patients for cultural acceptability and understandability (Cronbach’s α=0.82) [13].
Patients were contacted on the day of routine follow-up. Informed written consent was obtained after explaining the study purpose, anonymity, and voluntariness. Two psychiatric nurses trained in interviewing conducted structured face-to-face interviews in a private, quiet room. The interviews lasted 10–15 minutes and were audio-taped (with permission). Double-entry daily and random re-interviews were conducted for 10% of the participants to verify reliability.
Statistical analysis
Data were analyzed using SPSS software, version 23 and Microsoft Excel software, version 2010. Sociodemographic and clinical variables were described in terms of frequencies, percentages, Mean±SD. Inferential statistics comprised:
Chi-square tests to test the relationship between anxiety severity and categorical variables (e.g. smoking history, chronic disease). Multivariate logistic regression analysis to identify predictors of anxiety severity (e.g. age, income, comorbidities). The significance level was set at P<0.05 (two-tailed).
Results
Participant characteristics
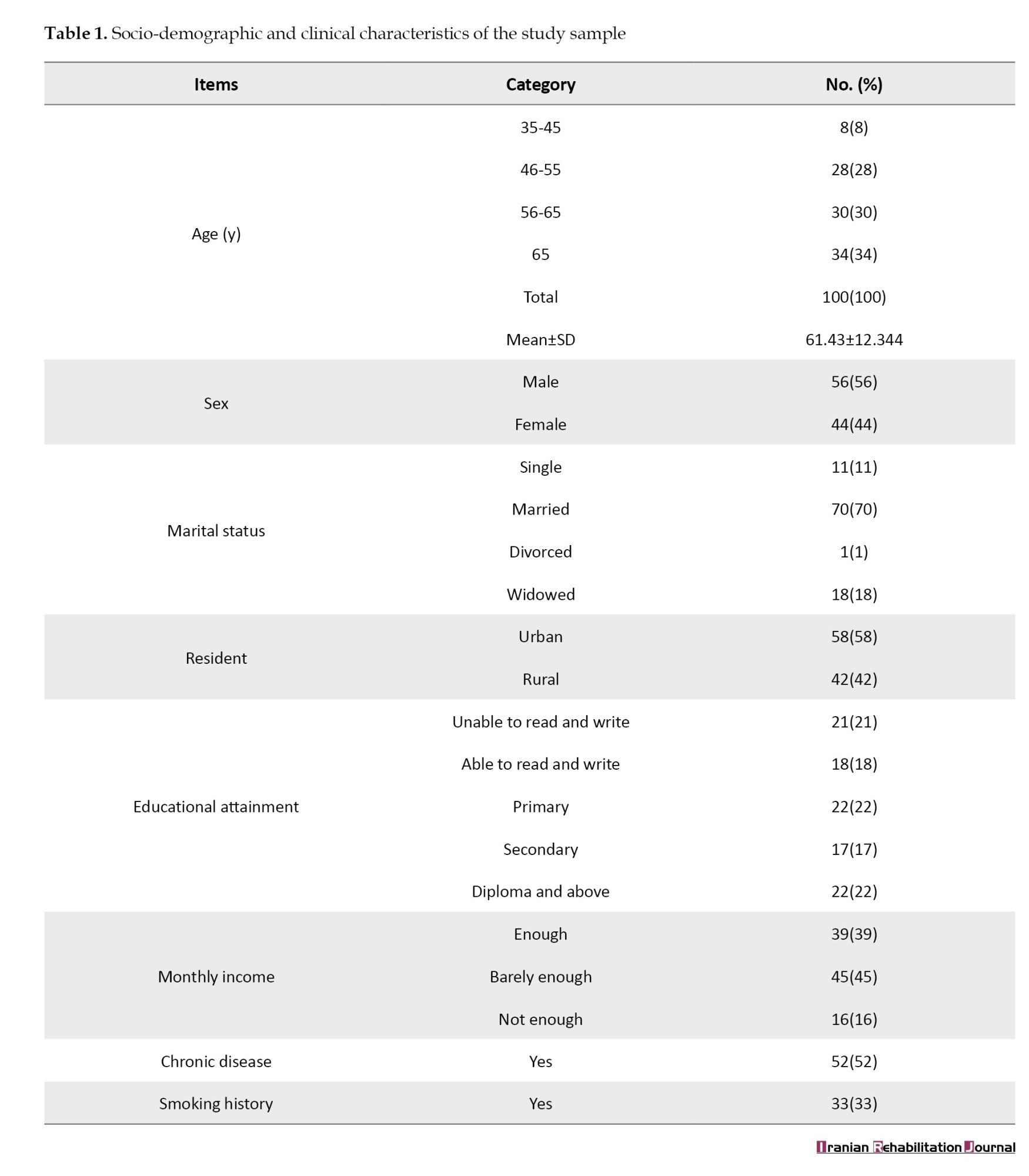
A total of 100 post-ischemic stroke patients participated in this study. Table 1 presents the demographic and clinical characteristics. The Mean±SD age was 61.43±12.34 years, and the majority (34.0%) were >65 years old. The sample consisted of 56% men, with two-thirds of the sample being married (70%) and residing in urban areas (58%). The education level was low, with 21% of the sample being illiterate, and 42.0% having received ≤ primary education. Income status revealed that 45.0% had just sufficient income, and 16.0% found their income to be too low.
Anxiety levels
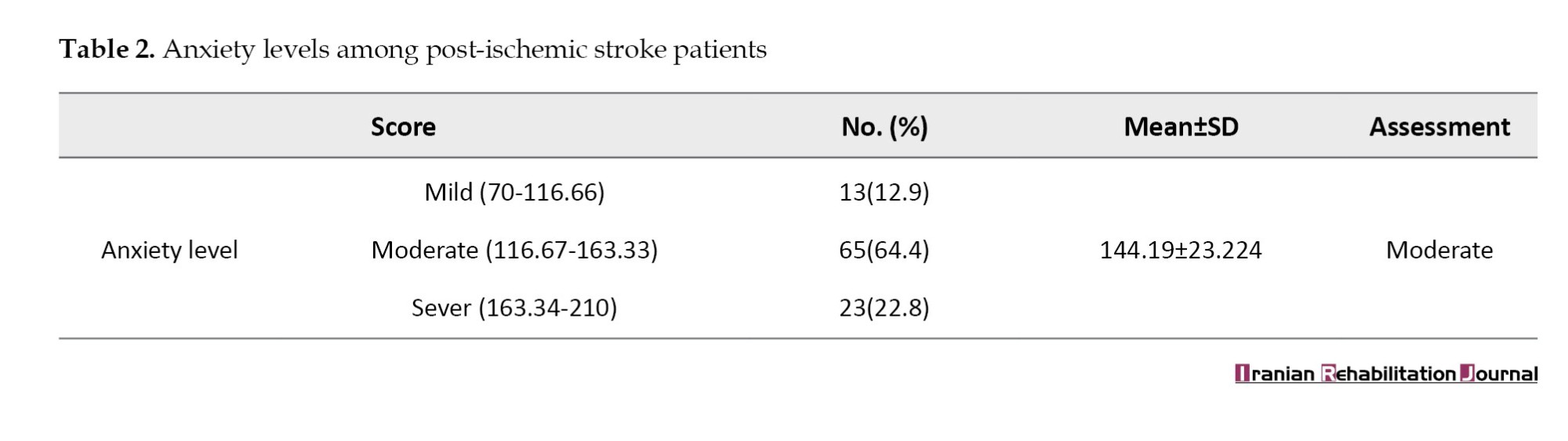
Table 2 presents the severity of anxiety, as assessed by the HAM-A.
The majority (64.4%) expressed moderate anxiety, while 22.8% expressed severe anxiety and 12.9% expressed mild anxiety. The overall mean HAM-A score was 144.19±23.22, indicating a considerable anxiety burden in this population.
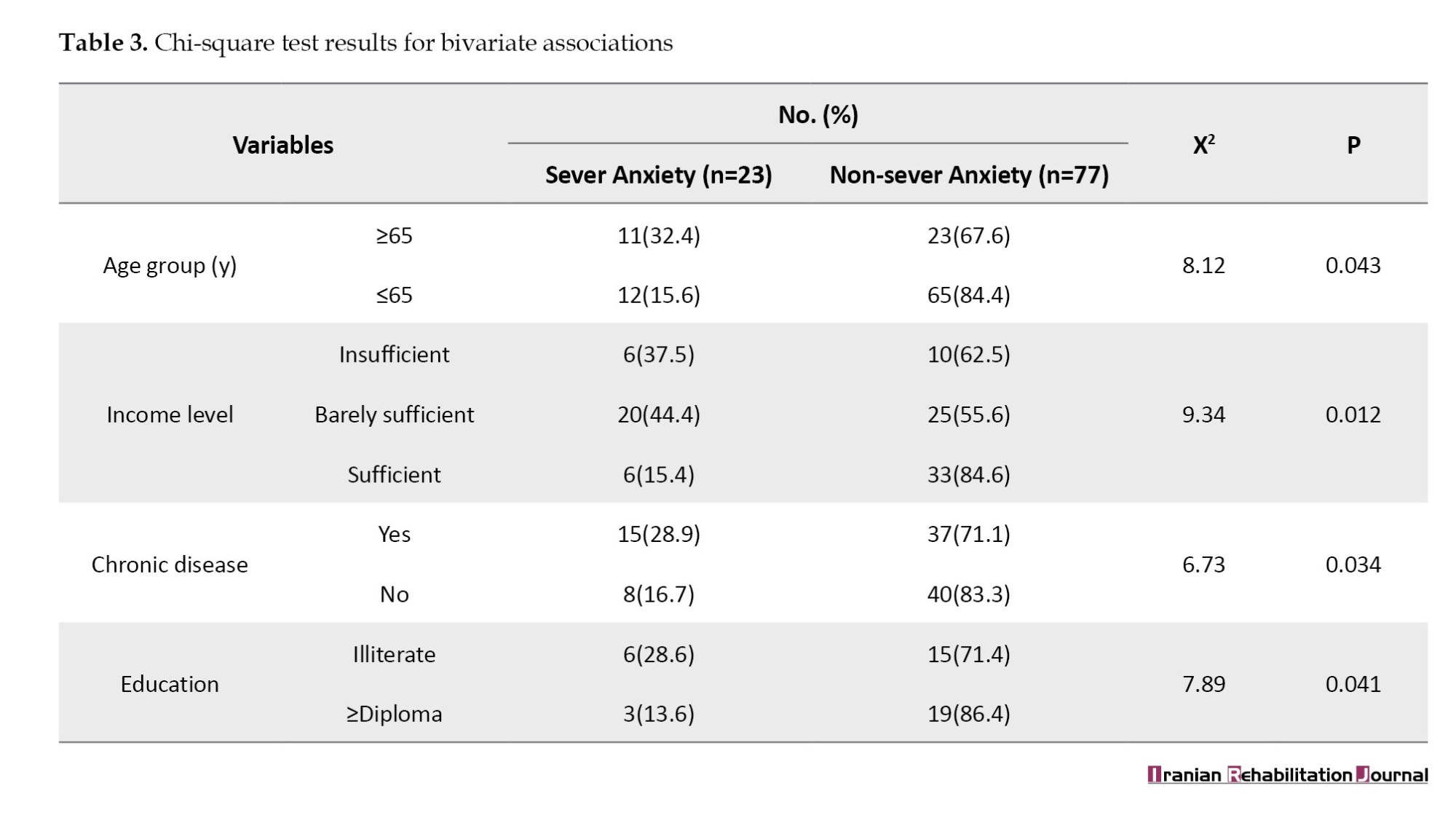
Bivariate associations
Table 3 presents the significant relationships between anxiety severity and sociodemographic/clinical variables. The outcomes suggested that 64.4% of patients had moderate anxiety (17 mean HAM-A score of 144.19±23.22), 22.8% had severe anxiety (163.34–210), and 12.9% had mild anxiety (70–116.66). Severe anxiety was correlated with age, low income, multiple chronic conditions, and less education. Severe anxiety was positively correlated with the predictors of old age (≥65 years), low income, and burden of chronic diseases, and less education, using multivariate analysis. Multivariate logistic regression revealed that patients with ≥2 comorbidities (odds ratio [OR]=3.21), lower-income (<satis-factory) OR=2.80), and older age (OR=1.04 per year) had increased odds of high anxiety.
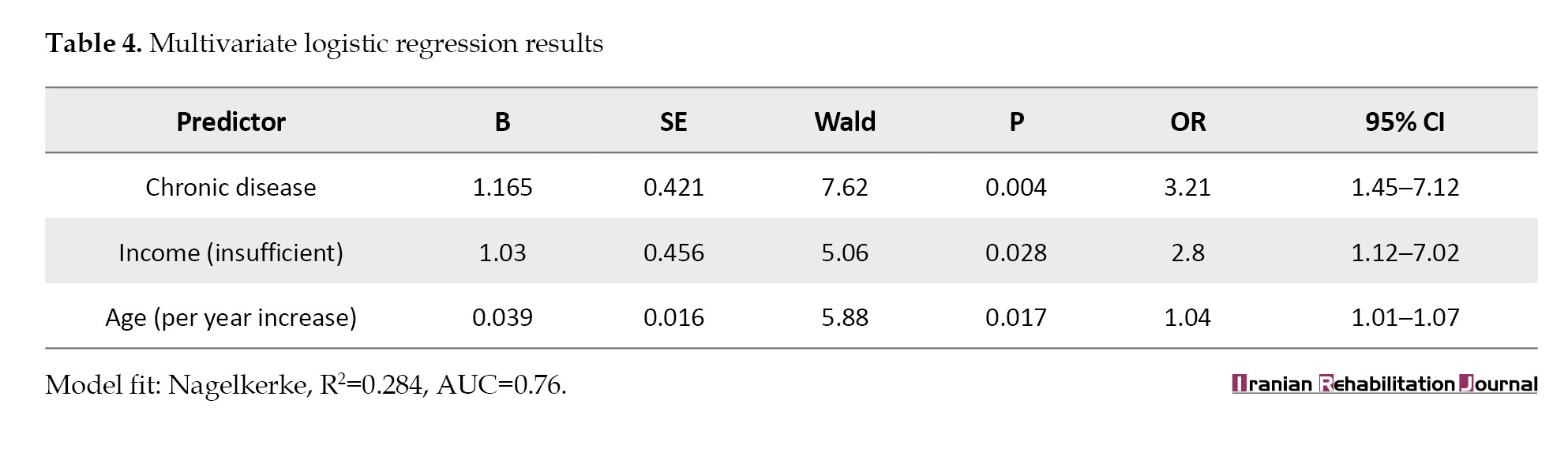
Predictors of severe anxiety
Table 4 presents the independent predictors of severe anxiety (HAM-A≥163.34). Table 4 demonstrates that chronic disease burden, financial inadequacy, and older age are independent predictors of severe anxiety (HAM-A≥163.34) in ischemic stroke survivors. Patients with ≥2 comorbid chronic illnesses were 3.21-fold more likely to experience severe anxiety (OR=3.21, 95% CI, 1.45%, 7.12%, P=0.004), demonstrating the cumulative physiological and psychological impact of multimorbidity. Patients with self-reported insufficient income had a 2.80-fold increased risk of severe anxiety (OR=2.80, 95% CI, 1.12%, 7.02%, P=0.028), suggesting socioeconomic heterogeneity in mental health recovery after stroke. Another year of age also raised the risk of severe anxiety by 4% (OR=1.04, 95% CI, 1.01%, 1.07%, P=0.017), in keeping with age-related risks, such as lost social support and heightened concern regarding recurrence. The model predicted 28.4% of the variance in anxiety severity (Nagelkerke R2=0.284) and demonstrated some discriminative power (area under the curve [AUC]=0.76).
Discussion
The findings of this study revealed a heavy psychological load in post-ischemic stroke survivors in Babylon Governorate, Iraq, with 64.4% experiencing moderate anxiety and 22.8% severe anxiety. These results align with global trends, wherein PSA affects 20–25% of survivors and tends to extend beyond the acute phase, hampering functional rehabilitation. In this paper, we situate these results within the existing literature, discuss the potential mechanisms, and provide clinical and research implications.
Demographic and socioeconomic correlates
Age more than 65 years, urban dwelling, and low income emerged as predictors of anxiety severity in the present study. These findings are consistent with existing research on vulnerability in older stroke survivors due to reduced social support, fear of recurrence, and age-related decline in physical and cognitive resilience [14]. Urban living can signal disparities in access to psychosocial resources, as urban residents often face higher living costs and fractured social networks that exacerbate stress [15]. Economic adversity, characterized by 45% of participants as “barely sufficient” or “insufficient,” likely also enhances concern through constraints in access to healthcare, rehabilitation, and employment.
Notably, 58% of the patients had ≤ primary education, indicating the role of health literacy in mental health status following stroke. Lower educational attainment may limit patients’ understanding of their illness, treatment, and adaptation strategies, thereby promoting anxiety. This aligns with other research, in which socioeconomic disadvantages fuel psychological distress in stroke survivors [14].
Clinical and psychological implications
The prevalence of moderate-to-severe anxiety (87.2%) underscores the need to incorporate regular mental health screening into post-stroke care. The comorbidity of anxiety with chronic diseases describes a bidirectional effect: physiological stress of chronic illness may exacerbate anxiety, and anxiety itself can additionally destabilize metabolic and cardiovascular health, perpetuating a cycle of poor recovery. In addition, symptoms, such as muscle stiffness, agitation, and insomnia (as noted in the conclusions), are indicative of the somatic manifestation of anxiety, which can also affect mobility and rehabilitation adherence.
Comparisons with international literature reinforce the universality of PSA Studies reported that 66% of stroke survivors experienced moderate-to-severe anxiety within six months post-stroke, mirroring our findings [16]. Similarly, one study reported ongoing anxiety in over half of patients for up to one year, particularly in individuals with poor social support, a feature prevalent in our cohort [17].
Conclusion
The majority of sample post-ischemic stroke patients experienced moderate levels of anxiety, about a quarter of the sample had severe anxiety, and about half of the sample had mild anxiety. The most severe anxiety symptoms were observed in the somatic (muscular and gastrointestinal), autonomic, and behavioral domains at the interview, showing the highest levels of anxiety, with symptoms, such as stiffness, pallor, giddiness, and restlessness being particularly prevalent. Demographic Factors (younger, urban, married individuals, and those with lower income) had statistically significant impacts on anxiety levels. Significantly higher anxiety levels were found in patients with chronic illnesses, particularly those with hypertension, atherosclerosis, or multiple comorbidities. Moderate levels of anxiety were also found with intellectual problems (e.g. memory, concentration) and emotional problems (e.g. depression and insomnia), indicating a broad impact of PSA.
Strengths and limitations
The research strengths are that it targets a Middle Eastern population, where there is still a lack of mental health data after stroke, and that a validated tool (modified HAM-A) was used to measure anxiety. However, the following limitations should be noted. Cross-sectional design: Causality between anxiety and demographic/clinical factors cannot be established. Longitudinal studies are necessary to investigate temporal relationships. Convenience sampling: Results may not generalize to rural areas or non-Iraqi populations. Self-reported data: Potential biases in self-report of anxiety symptoms, partly overcome by structured interviews.
Recommendations
To improve the PSA, we suggest the following:
Multidisciplinary rehabilitation programs: Integration of mental health specialists (e.g. clinical psychologists and psychiatric nurses) into stroke care teams to provide counseling and cognitive-behavioral therapy. Targeted interventions: Prioritizing older patients, those with chronic illnesses, and those with financial hardships through subsidized treatments and community-based support. Health literacy programs: Educating patients and caregivers about anxiety management and rehabilitation strategies to improve adherence and reduce stigma.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Babylon, Hillah, Iraq (Code: 56). Administrative approvals were obtained from the hospital managers. Verbal and written informed consent emphasized voluntary entry, confidentiality (data anonymized using unique codes), and the right to withdraw.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and funding acquisition: Salma Kadhum Jihad; Methodology: Fatima Hussein Abed; Supervision, investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the participants and experts for their corporation. The authors thank Khamees Bandar, Nuhad Al-Douri, and Ali Ahmed Kadhum AL-Hattab University of Babylon, Hillah, Iraq, for their for their generous support.
References
Anxiety is an essential human emotion, for example, a sensation of alarm, fear, and physiological tension on perceiving threats in the absence of immediate danger [1]. The American Psychiatric Association describes anxiety as anticipation of future danger, with associated dysphoric mood and bodily symptoms of increased arousal or tension in muscles [2]. Despite its universality as the most prevalent mental illness on Earth, anxiety is not diagnosed due to social stigma, treatment denial, or inappropriate diagnosis by medical practitioners [3]. It is a mindset that is an adaptive response to situational danger and is governed by the experience an individual has in life, cognitive appraisal, and environmental stressors [4].
Ischemic stroke, responsible for approximately 85% of all strokes, results from thrombosis or embolic occlusion of cerebral blood flow and causes neurological dysfunction [5]. The pathophysiology of two significant regions is at issue: the ischemic core, which results in permanent damage to the neurons, and the penumbra, a recoverable region of compromised perfusion [6]. Survivors of ischemic stroke have multifaceted problems, including physical dysfunction, protracted recovery periods, and psychosocial consequences of altered self-concept, dependency on others, and encounters with the medical system [7].
Post-stroke psychological morbidity is startlingly common, with up to 72% of survivors suffering disabling fatigue and clinically significant impairments in quality of life [8]. Of these, post-stroke anxiety (PSA) develops in 20–25% of patients, becoming a major hindrance to rehabilitation [9]. Emotional distress is greatest in the initial month following stroke but often persists chronically, contributing to functional impairment and difficulties in social reintegration. Concerns regarding recurrence, loss of independence, and disruption of daily routines are determinants of chronic anxiety [8].
Since the ratio of PSA is highly extensive and adversely impacts recovery results, the current study investigated anxiety levels among survivors of ischemic stroke, residents of Babylon Governorate, Iraq. It explores correlations with demographic and clinical factors. The detection of such trends is required to incorporate mental health interventions into stroke rehabilitation programs and maximize integrated patient care.
Materials and Methods
Study design
A quantitative cross-sectional study was conducted to assess anxiety levels among post-ischemic stroke patients in Babylon Governorate, Iraq. Data were collected between December 22, 2024, and March 2, 2025, within the overall study duration from October 15, 2024, to July 1, 2025. The study design followed the strengthening the reporting of observational studies in epidemiology guidelines to ensure methodological rigor [10].
Study setting: Data were collected in two central locations: Al-Imam Al Sadiq Teaching Hospital and Babylon Specialized Medical Rehabilitation Center, which were selected based on their high volume of patients undergoing post-stroke rehabilitation treatment.
Sampling and participants
A convenience sample of 100 participants was recruited for this study. The inclusion criteria included adults ≥18 years, first-ever definitive ischemic stroke on neuroimaging (computed tomography [CT]/magnetic resonance imaging [MRI]) within the previous 6–12 months, and cognitive capacity to participate (excluding severe dementia or aphasia) [11]. The exclusion criteria included pre-existing psychiatric illnesses (e.g. depression and generalized anxiety disorder) and severe physical disabilities that prevented communication. The sample size was computed using the Equation 1:
where Z=1.96 (95% confidence level), P=0.5 (expected prevalence), and d=0.10 (margin of error), which produces a minimum of 97 participants [12].
Data collection
This study used a three-section standardized questionnaire:
1) Sociodemographic characteristics included age (years), sex (male/female), residence (urban/rural), marital status (single/married/divorced/widowed), educational level (illiterate, primary, secondary, diploma/above), and monthly income (as “enough,” “barely enough,” or “not enough”). 2) Clinical data: History of smoking (current/former/none) and chronic disease (e.g. diabetes mellitus, hyperlipidemia, hypertension, and atherosclerosis). 3) Anxiety scale: The Hamilton rating scale for anxiety (HAM-A) was culturally modified (e.g. “insight” items were changed). It comprises 14 domains (e.g. anxious mood, somatic symptoms, insomnia) that are rated on a 3-point Likert scale: 1=always, 2=sometimes, 3=never. Scores were summed to range from 14 to 42 and categorized as mild (14–20), moderate (21–27), and severe (≥28). The Arabic version was tested on 10 patients for cultural acceptability and understandability (Cronbach’s α=0.82) [13].
Patients were contacted on the day of routine follow-up. Informed written consent was obtained after explaining the study purpose, anonymity, and voluntariness. Two psychiatric nurses trained in interviewing conducted structured face-to-face interviews in a private, quiet room. The interviews lasted 10–15 minutes and were audio-taped (with permission). Double-entry daily and random re-interviews were conducted for 10% of the participants to verify reliability.
Statistical analysis
Data were analyzed using SPSS software, version 23 and Microsoft Excel software, version 2010. Sociodemographic and clinical variables were described in terms of frequencies, percentages, Mean±SD. Inferential statistics comprised:
Chi-square tests to test the relationship between anxiety severity and categorical variables (e.g. smoking history, chronic disease). Multivariate logistic regression analysis to identify predictors of anxiety severity (e.g. age, income, comorbidities). The significance level was set at P<0.05 (two-tailed).
Results
Participant characteristics
A total of 100 post-ischemic stroke patients participated in this study. Table 1 presents the demographic and clinical characteristics. The Mean±SD age was 61.43±12.34 years, and the majority (34.0%) were >65 years old. The sample consisted of 56% men, with two-thirds of the sample being married (70%) and residing in urban areas (58%). The education level was low, with 21% of the sample being illiterate, and 42.0% having received ≤ primary education. Income status revealed that 45.0% had just sufficient income, and 16.0% found their income to be too low.
Anxiety levels
Table 2 presents the severity of anxiety, as assessed by the HAM-A.
The majority (64.4%) expressed moderate anxiety, while 22.8% expressed severe anxiety and 12.9% expressed mild anxiety. The overall mean HAM-A score was 144.19±23.22, indicating a considerable anxiety burden in this population.
Bivariate associations
Table 3 presents the significant relationships between anxiety severity and sociodemographic/clinical variables. The outcomes suggested that 64.4% of patients had moderate anxiety (17 mean HAM-A score of 144.19±23.22), 22.8% had severe anxiety (163.34–210), and 12.9% had mild anxiety (70–116.66). Severe anxiety was correlated with age, low income, multiple chronic conditions, and less education. Severe anxiety was positively correlated with the predictors of old age (≥65 years), low income, and burden of chronic diseases, and less education, using multivariate analysis. Multivariate logistic regression revealed that patients with ≥2 comorbidities (odds ratio [OR]=3.21), lower-income (<satis-factory) OR=2.80), and older age (OR=1.04 per year) had increased odds of high anxiety.
Predictors of severe anxiety
Table 4 presents the independent predictors of severe anxiety (HAM-A≥163.34). Table 4 demonstrates that chronic disease burden, financial inadequacy, and older age are independent predictors of severe anxiety (HAM-A≥163.34) in ischemic stroke survivors. Patients with ≥2 comorbid chronic illnesses were 3.21-fold more likely to experience severe anxiety (OR=3.21, 95% CI, 1.45%, 7.12%, P=0.004), demonstrating the cumulative physiological and psychological impact of multimorbidity. Patients with self-reported insufficient income had a 2.80-fold increased risk of severe anxiety (OR=2.80, 95% CI, 1.12%, 7.02%, P=0.028), suggesting socioeconomic heterogeneity in mental health recovery after stroke. Another year of age also raised the risk of severe anxiety by 4% (OR=1.04, 95% CI, 1.01%, 1.07%, P=0.017), in keeping with age-related risks, such as lost social support and heightened concern regarding recurrence. The model predicted 28.4% of the variance in anxiety severity (Nagelkerke R2=0.284) and demonstrated some discriminative power (area under the curve [AUC]=0.76).
Discussion
The findings of this study revealed a heavy psychological load in post-ischemic stroke survivors in Babylon Governorate, Iraq, with 64.4% experiencing moderate anxiety and 22.8% severe anxiety. These results align with global trends, wherein PSA affects 20–25% of survivors and tends to extend beyond the acute phase, hampering functional rehabilitation. In this paper, we situate these results within the existing literature, discuss the potential mechanisms, and provide clinical and research implications.
Demographic and socioeconomic correlates
Age more than 65 years, urban dwelling, and low income emerged as predictors of anxiety severity in the present study. These findings are consistent with existing research on vulnerability in older stroke survivors due to reduced social support, fear of recurrence, and age-related decline in physical and cognitive resilience [14]. Urban living can signal disparities in access to psychosocial resources, as urban residents often face higher living costs and fractured social networks that exacerbate stress [15]. Economic adversity, characterized by 45% of participants as “barely sufficient” or “insufficient,” likely also enhances concern through constraints in access to healthcare, rehabilitation, and employment.
Notably, 58% of the patients had ≤ primary education, indicating the role of health literacy in mental health status following stroke. Lower educational attainment may limit patients’ understanding of their illness, treatment, and adaptation strategies, thereby promoting anxiety. This aligns with other research, in which socioeconomic disadvantages fuel psychological distress in stroke survivors [14].
Clinical and psychological implications
The prevalence of moderate-to-severe anxiety (87.2%) underscores the need to incorporate regular mental health screening into post-stroke care. The comorbidity of anxiety with chronic diseases describes a bidirectional effect: physiological stress of chronic illness may exacerbate anxiety, and anxiety itself can additionally destabilize metabolic and cardiovascular health, perpetuating a cycle of poor recovery. In addition, symptoms, such as muscle stiffness, agitation, and insomnia (as noted in the conclusions), are indicative of the somatic manifestation of anxiety, which can also affect mobility and rehabilitation adherence.
Comparisons with international literature reinforce the universality of PSA Studies reported that 66% of stroke survivors experienced moderate-to-severe anxiety within six months post-stroke, mirroring our findings [16]. Similarly, one study reported ongoing anxiety in over half of patients for up to one year, particularly in individuals with poor social support, a feature prevalent in our cohort [17].
Conclusion
The majority of sample post-ischemic stroke patients experienced moderate levels of anxiety, about a quarter of the sample had severe anxiety, and about half of the sample had mild anxiety. The most severe anxiety symptoms were observed in the somatic (muscular and gastrointestinal), autonomic, and behavioral domains at the interview, showing the highest levels of anxiety, with symptoms, such as stiffness, pallor, giddiness, and restlessness being particularly prevalent. Demographic Factors (younger, urban, married individuals, and those with lower income) had statistically significant impacts on anxiety levels. Significantly higher anxiety levels were found in patients with chronic illnesses, particularly those with hypertension, atherosclerosis, or multiple comorbidities. Moderate levels of anxiety were also found with intellectual problems (e.g. memory, concentration) and emotional problems (e.g. depression and insomnia), indicating a broad impact of PSA.
Strengths and limitations
The research strengths are that it targets a Middle Eastern population, where there is still a lack of mental health data after stroke, and that a validated tool (modified HAM-A) was used to measure anxiety. However, the following limitations should be noted. Cross-sectional design: Causality between anxiety and demographic/clinical factors cannot be established. Longitudinal studies are necessary to investigate temporal relationships. Convenience sampling: Results may not generalize to rural areas or non-Iraqi populations. Self-reported data: Potential biases in self-report of anxiety symptoms, partly overcome by structured interviews.
Recommendations
To improve the PSA, we suggest the following:
Multidisciplinary rehabilitation programs: Integration of mental health specialists (e.g. clinical psychologists and psychiatric nurses) into stroke care teams to provide counseling and cognitive-behavioral therapy. Targeted interventions: Prioritizing older patients, those with chronic illnesses, and those with financial hardships through subsidized treatments and community-based support. Health literacy programs: Educating patients and caregivers about anxiety management and rehabilitation strategies to improve adherence and reduce stigma.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Babylon, Hillah, Iraq (Code: 56). Administrative approvals were obtained from the hospital managers. Verbal and written informed consent emphasized voluntary entry, confidentiality (data anonymized using unique codes), and the right to withdraw.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and funding acquisition: Salma Kadhum Jihad; Methodology: Fatima Hussein Abed; Supervision, investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the participants and experts for their corporation. The authors thank Khamees Bandar, Nuhad Al-Douri, and Ali Ahmed Kadhum AL-Hattab University of Babylon, Hillah, Iraq, for their for their generous support.
References
- Akiskal HS. Anxiety: Definition, relationship to depression, and proposal for an integrative model. In: Tuma AH, Maser JD, editors. Anxiety and the anxiety disorders. New York: Routledge; 2019. [DOI:10.4324/9780203728215-56]
- Simon N, Hollander E, Rothbaum BO, Stein DJ. The American psychiatric association publishing textbook of anxiety, trauma, and ocd-related disorders. Washington: American Psychiatric Pub; 2020. [DOI:10.1176/appi.books.9781615379378]
- Najm Abd H, Dakhil Nawam S. The relationship between verbal violence and psychological stress among nurses. Iranian Rehabilitation Journal. 2025; 23(1):53-64. [DOI:10.32598/irj.23.1.1619.8]
- Abed Laftah S, Kadhim Abdul-Hameed A, Zair Balat K, Malih Radhi M. Barriers and facilitators in rehabilitative nursing care for clients with disabilities: A mediating roles of nurse-related factors. Iranian Rehabilitation Journal. 2025; 23(2):165-74. [DOI:10.32598/irj.23.2.1989.4]
- Feske SK. Ischemic stroke. The American Journal of Medicine. 2021; 134(12):1457-64. [DOI:10.1016/j.amjmed.2021.07.027]
- Mendelson SJ, Prabhakaran S. Diagnosis and management of transient ischemic attack and acute ischemic stroke: A review. JAMA. 2021; 325(11):1088-98. [DOI:10.1001/jama.2020.26867] [PMID]
- Siegler JE, Boehme AK, Kumar AD, Gillette MA, Albright KC, Martin-Schild S. What change in the National Institutes of Health Stroke Scale should define neurologic deterioration in acute ischemic stroke? Journal of Stroke and Cerebrovascular Diseases. 2013; 22(5):675-82. [DOI:10.1016/j.jstrokecerebrovasdis.2012.04.012] [PMID]
- D'Aniello GE, Scarpina F, Mauro A, Mori I, Castelnuovo G, Bigoni M, et al. Characteristics of anxiety and psychological well-being in chronic post-stroke patients. Journal of The Neurological Sciences. 2014; 338(1-2):191-6. [DOI:10.1016/j.jns.2014.01.005] [PMID]
- Ahmadizadeh Z, Samaei SA, Alibakhshi H, Pahlevanian A, Binesh M. Factors associated with occupational performance in older people with stroke. Iranian Rehabilitation Journal. 2024; 22(4):673-80. [DOI:10.32598/irj.22.4.2080.1]
- Cuschieri S. The STROBE guidelines. Saudi Journal of Anaesthesia. 2019; 13(Suppl 1):S31-4. [DOI:10.4103/sja.SJA_543_18] [PMID]
- Zehra A, Ahmer Z, Qadri U, Ovais M. Depression, anxiety and stress in formal and informal caregivers of Autistic Children in Karachi. Iranian Rehabilitation Journal. 2024; 22(2):277-84. [DOI:10.32598/irj.22.2.2025.1]
- Cumming TB, Blomstrand C, Skoog I, Linden T. The high prevalence of anxiety disorders after stroke. The American Journal of Geriatric Psychiatry. 2016; 24(2):154-60. [DOI:10.1016/j.jagp.2015.06.003] [PMID]
- Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occupational Medicine. 2015; 65(7):601. [DOI:10.1093/occmed/kqv054] [PMID]
- Rafsten L, Danielsson A, Sunnerhagen KS. Anxiety after stroke: A systematic review and meta-analysis. Journal of Rehabilitation Medicine. 2018; 50(9):769-78. [DOI:10.2340/16501977-2384] [PMID]
- Chun HY, Whiteley WN, Dennis MS, Mead GE, Carson AJ. Anxiety After Stroke: The Importance of Subtyping. Stroke. 2018; 49(3):556-64. [DOI:10.1161/STROKEAHA.117.020078] [PMID]
- Campbell Burton CA, Murray J, Holmes J, Astin F, Greenwood D, et al. Frequency of anxiety after stroke: A systematic review and meta-analysis of observational studies. International Journal of Stroke. 2013; 8(7):545-59. [DOI:10.1111/j.1747-4949.2012.00906.x] [PMID]
- Lincoln NB, Brinkmann N, Cunningham S, Dejaeger E, De Weerdt W, Jenni W, et al. Anxiety and depression after stroke: A 5 year follow-up. Disability and Rehabilitation. 2013; 35(2):140-5. [DOI:10.3109/09638288.2012.691939] [PMID]
Article type: Original Research Articles |
Subject:
Nursing
Received: 2025/05/1 | Accepted: 2025/06/11 | Published: 2025/09/1
Received: 2025/05/1 | Accepted: 2025/06/11 | Published: 2025/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
