
988368
Thu, Jul 30, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 431-440 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jasim A M, Aziz G. Efficacy of Swiss Ball Exercises on Motor Control and Defensive Blocking Handball Players With Hamstring Strain Injury. Iranian Rehabilitation Journal 2025; 23 (4) :431-440
URL: http://irj.uswr.ac.ir/article-1-2547-en.html
URL: http://irj.uswr.ac.ir/article-1-2547-en.html



1- Department of Sports Injury Rehabilitation, College of Physical Education and Sports Sciences, Al-Mustansiriyah University. Baghdad, Iraq.
2- Department of Sports Injury Rehabilitation, College of Science for Women, University of Baghdad, Baghdad, Iraq.
2- Department of Sports Injury Rehabilitation, College of Science for Women, University of Baghdad, Baghdad, Iraq.
Full-Text [PDF 1216 kb]
(754 Downloads)
| Abstract (HTML) (2214 Views)
Full-Text: (234 Views)
Introduction
In the last few decades, sports rehabilitation and sports medicine have been transformed by advances in biomechanics, technology, and interprofessional practices for injury management [1, 2]. Modern practices in contemporary rehabilitation are today aimed not only at speedy recovery but also at readmission of sportspersons to pre-injury level performance through evidence-based sport practice [3]. These advances have played a central role in balancing the complex interplay among mechanisms of injury, sport-specific prevention, and functional rehabilitation [4], particularly for sports with high injury risk like handball, where sudden deceleration changes, violent sprinting, and impact defensive maneuvers make the athlete susceptible to hamstring strain injury (HSI) [5, 6].
HSIs remain a current problem in handball, accounting for 12–15% of total sports injuries and tending to result in prolonged recovery and impact technical performance through ruptured training cycles [7, 8]. The physical stresses of handball, such as sudden decelerations and accelerations, and defense techniques, such as the block wall, expose the hamstring muscles to significant stress [9]. The block wall, a cornerstone of modern defensive play, relies on pinpoint coordination, explosive power, and dynamic stability to extinguish shots and initiate counterattacks. However, poor biomechanics or residual weakness from an injury can get in the way of this capacity, compromising personal and team performance [10].
Traditionally, rehabilitation programs have focused on the maintenance of muscle strength and range of motion (ROM), but more recent evidence indicates that balancing neuromuscular training to counter functional imbalances and avoid the risk of re-injury is necessary [10-12]. Recent technological and methodological advancements have revolutionized rehabilitation models, and Swiss ball exercises have become a cornerstone intervention to enhance neuromuscular control and functional rehabilitation in sports [13, 14]. The Swiss ball hamstring curl and wall squat are specific exercises aimed at improving hamstring strength, core stability, and dynamic balance by co-activating various muscles on unstable surfaces [15]. Experiments demonstrate that Swiss ball training can improve trunk extensor/flexor endurance, lower limb coordination, and control of the lumbopelvic region, which are crucial to prevent HSI and optimize sport-specific movement patterns, such as the block wall technique during handball [16, 17].
Although eccentric training was initially found useful in the prevention and rehabilitation of HSI, existing protocols fail to incorporate sport-specific neuromuscular training and biomechanical specificity, which are necessary for returning functional performance in defensive movements such as the block wall [18]. Swiss ball exercise, in its capacity to optimize eccentric-concentric activation of the muscles and dynamic stabilization [19].
By prioritizing hip joint mobility, hamstring strength, and lumbopelvic control, this intervention focuses on the performance demands of handball’s high-impact defensive maneuvers, which are commonly interrupted after injury [20]. In addition, the study’s focus on quantifying motor control adjustments and defensive blocking effectiveness is congruent with the increasing imperative to relate clinical outcomes to sport-specific performance measures.
Materials and Methods
This single-group pre-post prospective study adhered to the consolidated standards of reporting trials statement. The population was Baghdad Premier League club players, namely Al-Talaba, Al-Jaish, Al-Shurta, Al-Karkh, and Al-Hashd clubs. The assessment was conducted at the College of Physical Education and Sports Sciences from January 2023 to June 2024. The study was conducted per the principles of the Declaration of Helsinki. All eligible participants provided written informed consent and received a copy of their executed consent form for their personal records. The participants were informed that they could withdraw from the study at any point without obligation. Adverse effects (e.g. increased pain) were also noted.
Population
A priori power analysis (G*Power software, version 3.1.9.7) indicated a required sample size of n=28 to detect a medium effect size (d=0.6) in hamstring strength gains with 80% power (α=0.05). To allow for a 15% dropout, 32 participants were recruited.
The participants eligible for this study were athletes aged 18-35 years with a grade I hamstring injury diagnosis confirmed by magnetic resonance imaging (MRI) and clinical examination conducted by a physician. They had no prior history of recurrent hamstring injuries or surgical interventions and were engaged in professional or semi-professional handball. All participants provided written informed consent prior to the study [21]. The exclusion criteria included evidence of grade II or grade III hamstring injury, other lower limb musculoskeletal injuries affecting movement or performance, a history of neurological or orthopedic conditions impacting gait or balance, or an inability to comply with necessary procedures.
Assessments
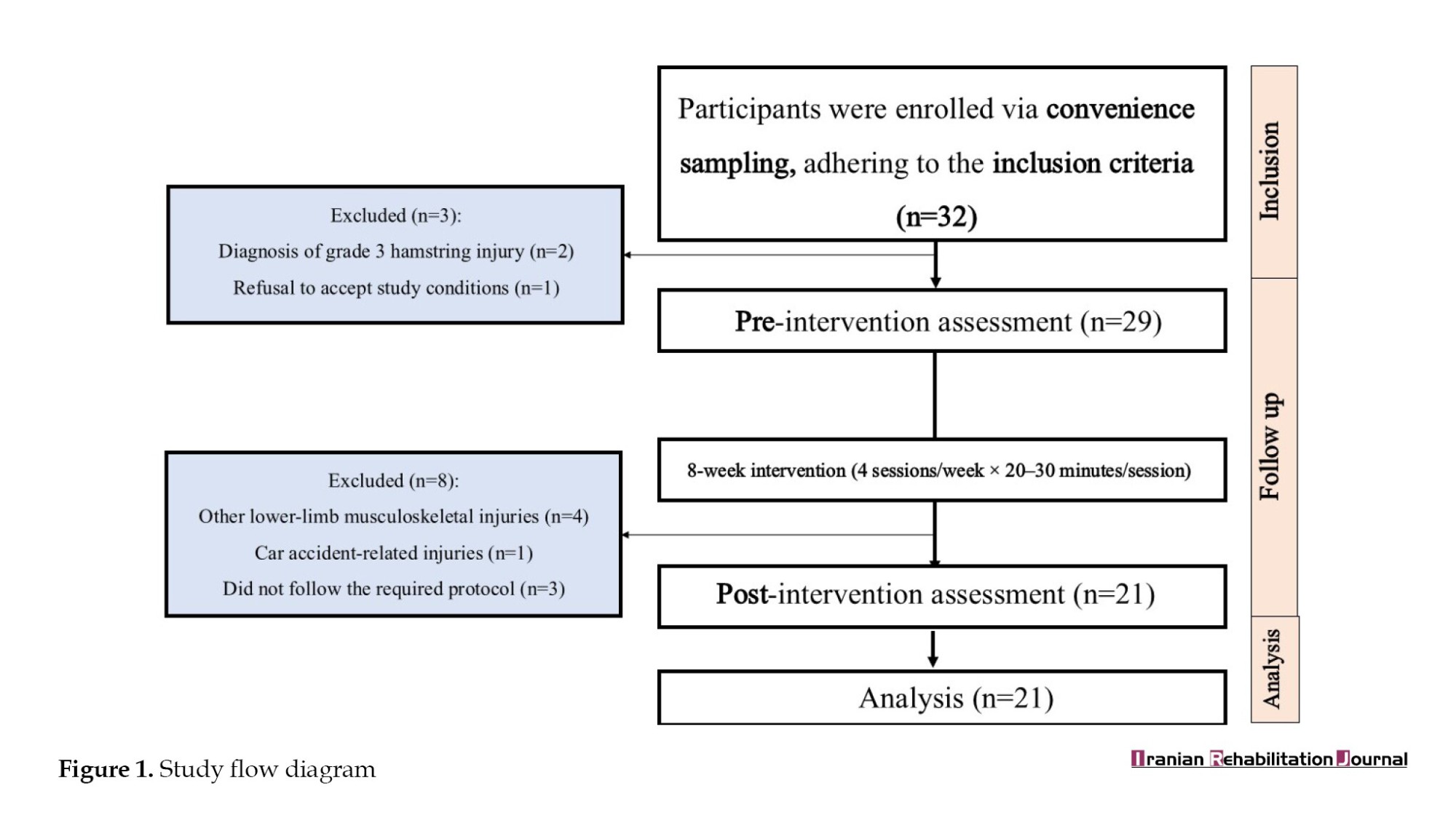
The participants were evaluated at two time points: Pre-intervention and post-intervention. They were recruited over eight weeks. After initial screening (demographic data collection, and physical examination), they were recruited for the study. The study outcomes were hip joint ROM, hamstring muscle strength, and defensive blocking performance in handball. The study flow diagram is shown in Figure 1.
The hip joint ROM was recorded following a protocol standardized for validation by expert consensus [22]. Measurements were taken 1–3 days post-injury to standardize acute-phase measurements. A Casio cinematic camera (Casio Computer Co., Ltd., Tokyo, Japan; 25 frames per second) mounted on a tripod was used to record the joint angles during active hip flexion and extension movements. Adhesive markers were placed on anatomical landmarks (lateral femoral condyle, greater trochanter, and anterior superior iliac spine) to enhance the precision of movement measurement [23].
Participants performed slow, controlled flexion and extension movements of the affected limb while supine on a medical examination table, moving to their maximum pain-free range. Video recordings were analyzed using Kinovea software (version 0.9.2; open-source software developed by Olivier Rossel, France) to measure hip joint angles (intraclass correlation coefficient [ICC]=0.79) [24]. Goniometric measurements were cross-referenced with a panel of three sports medicine experts to maintain adherence to accepted biomechanical criteria. A blinded examiner performed all measurements to limit measurement bias.
Hamstring muscle strength was measured using a handheld force sensor unit (MicroFET2 Dynamometer, Hoggan Scientific, Salt Lake City, USA), which is a valid measure of peak force production in Newtons. The participants were positioned prone on a medical examination table. During the relaxed condition test, the knee was kept in full extension to measure baseline muscle tone and passive resistance. The examiner placed the force sensor over the posterior distal femur and applied minimal pressure without eliciting any voluntary contraction from the participant [25].
For the tensed state test, the participants flexed their knees to approximately 30°, which was considered the optimum mid-range position for hamstring activation. Under these conditions, the participants were requested to maximally contract their hamstring muscles against the resistance of the force sensor. Three maximal voluntary isometric contractions (MVICs) were performed for each limb by each participant, with 30 seconds of rest between trials to minimize fatigue and ensure consistency of effort between repetitions (ICC=0.89 for relaxed and ICC=0.92 for tensed) [26].
Defensive blocking performance was evaluated using a standardized protocol adapted from validated handball-specific functional tests. The test evaluates an athlete’s ability to execute repetitive defensive blocks with technical precision, speed, and consistency in game-like conditions.
The test was conducted on a standard handball court. Two handballs were suspended from goalposts at a height of 2.6 meters, which could be adjusted downward for youth or female athletes. Adhesive tape markers were used to designate the 6-meter line, vertically aligned with the suspended balls, and two goalposts on the 8- to 9-meter line, 3 meters apart. A middle starting point was designated halfway between the two balls. Players began each trial from a stationary standing position at this location.
On a visual start signal, players performed a cycle consisting of a forward sprint, a jumping block to touch one of the balls with both hands, a controlled landing, and recovery to the starting position as fast as possible. This cycle was repeated as many times as possible within 15 s. All movements had to replicate real-game defense mechanics, including correct arm position, explosive jumping, and controlled direction changes.
Some performance criteria were utilized to uphold reliability and validity. Bilateral hand contact on the ball must be made on each block attempt. Each movement must be initiated from the established starting position, and any deviation invalidates that repetition. Attempts that did not meet these criteria (single-hand contact or a step outside the established area) were considered invalid and were not counted in the scoring. Scoring was based on the number of successful defensive blocks completed within 15 s [27].
Intervention
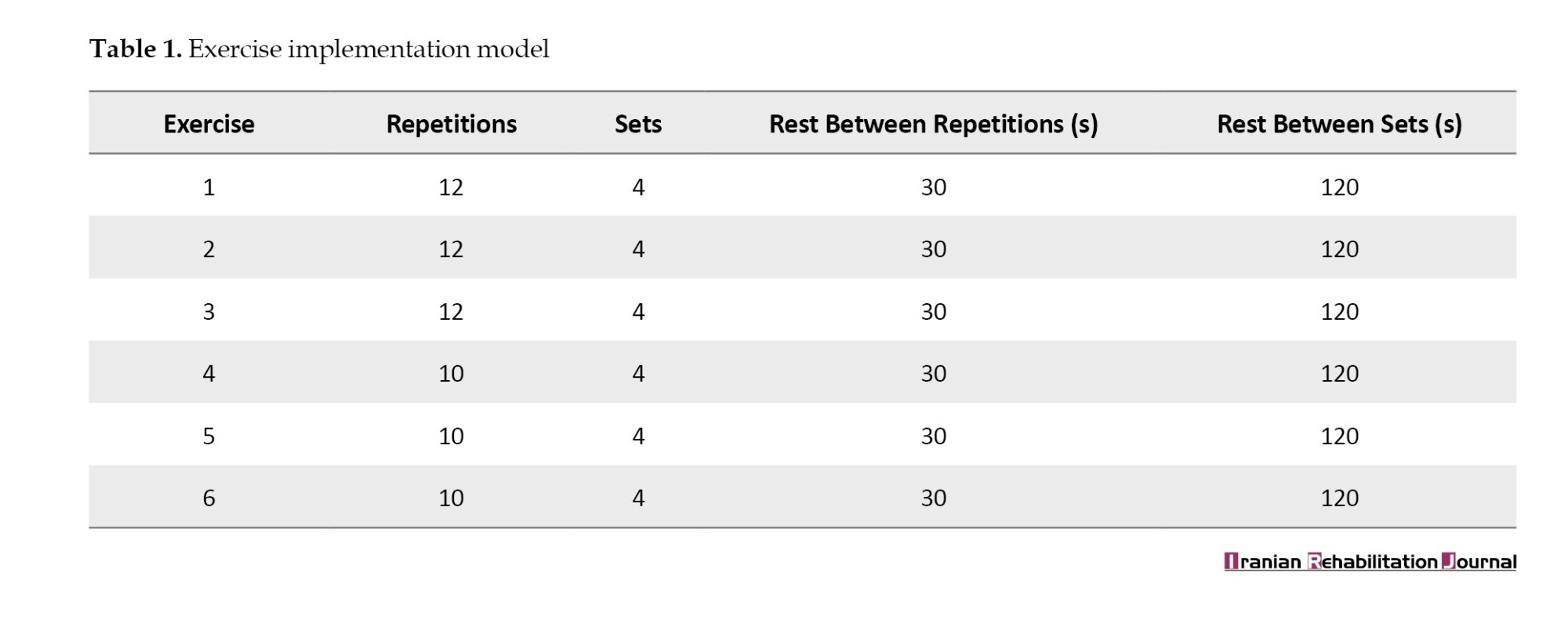
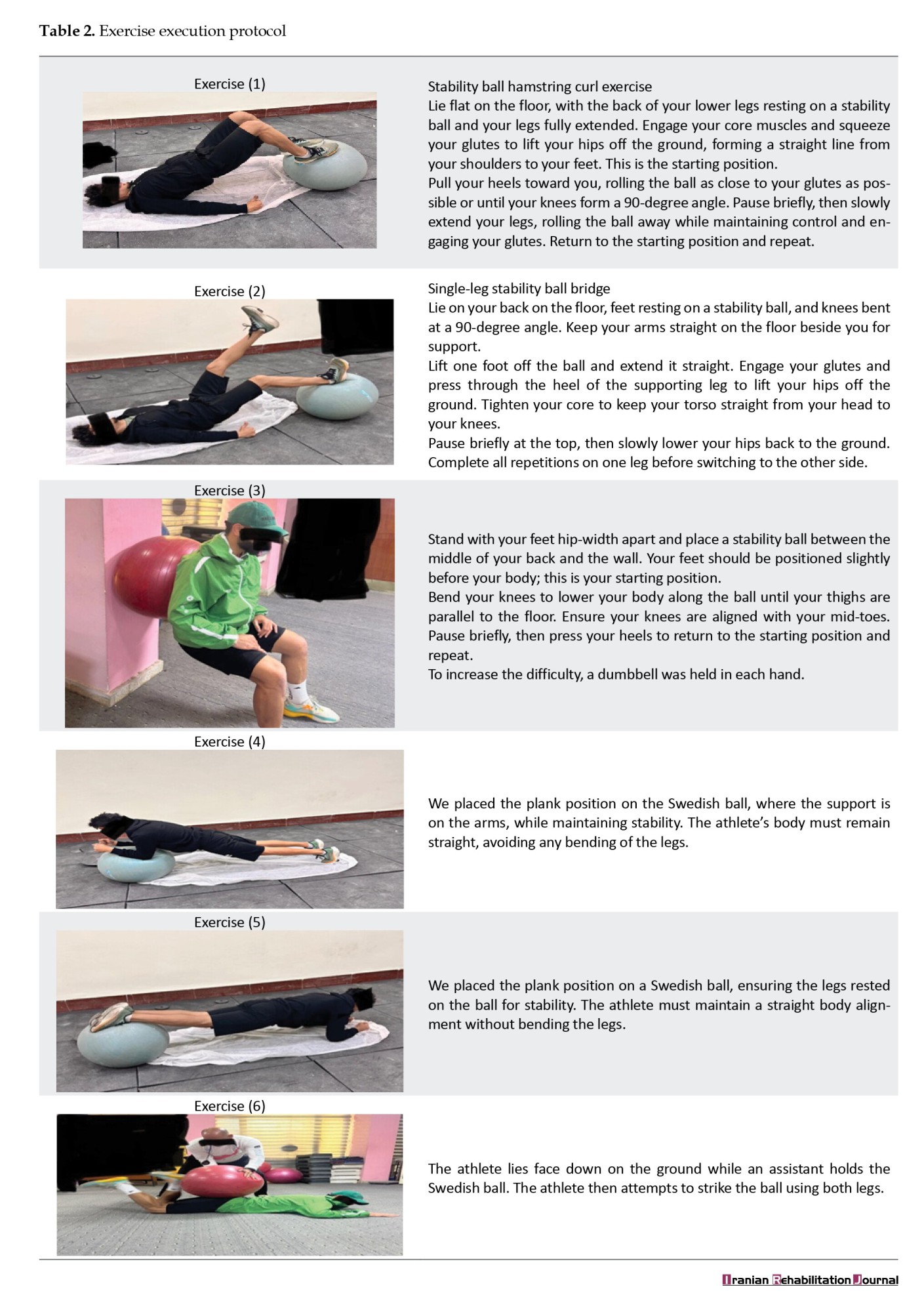
The rehabilitation program comprised Swiss ball exercises to improve hamstring flexibility, elasticity, and strength. The program lasted 8 weeks, with the participants attending four sessions per week, each lasting 20–30 minutes. The exercises were designed to progress from simple to complex movement patterns based on the functional demands of the participants. The sessions started with a warm-up, proceeded with the main Swiss ball exercises, and concluded with a cool-down phase [28]. Tables 1 and 2 present a detailed explanation of the model and exercise protocol.
Statistical analysis
Statistical analysis was performed using SPSS software, version 25 (IBM Corp., USA). Descriptive statistics were employed to describe the participants’ demographic and baseline characteristics. Normality test of data was conducted using the Shapiro-Wilk test. For variables in normal distribution, a paired t-test was utilized.
To compare the outcome measures (i.e. ROM of the hip joint, hamstring strength, and defensive blocking performance) before and after the intervention, a paired-samples t-test was used. Statistical significance was set at P<0.05. Results were reported as Mean±SD, and effect sizes were calculated using Cohen’s d to allow for comparison of the size of change.
Results
Participant demographics
21 handball players (mean age: 24.6±3.2 years) with Grade I hamstring injuries were included in the study. Baseline demographic and injury-related characteristics are shown in Table 3. All subjects were competitive players in the Baghdad Premier League, with 6.5±2.1 years of competitive handball experience. Injuries were observed most frequently in the dominant limb (62.5%) in high-level defensive play or sprinting activities of play. Shapiro-Wilk test confirmed normal distribution of baseline data (P>0.05).
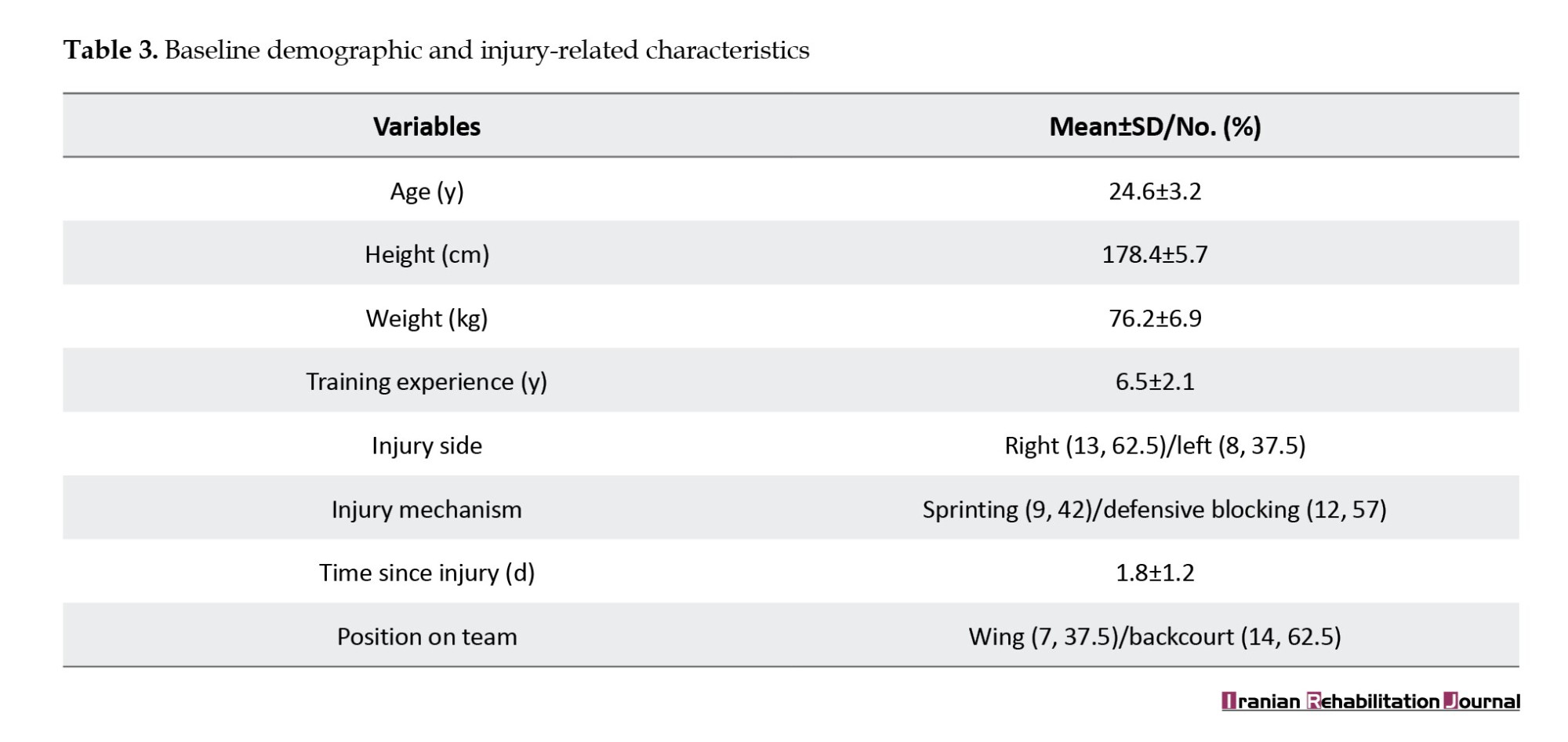
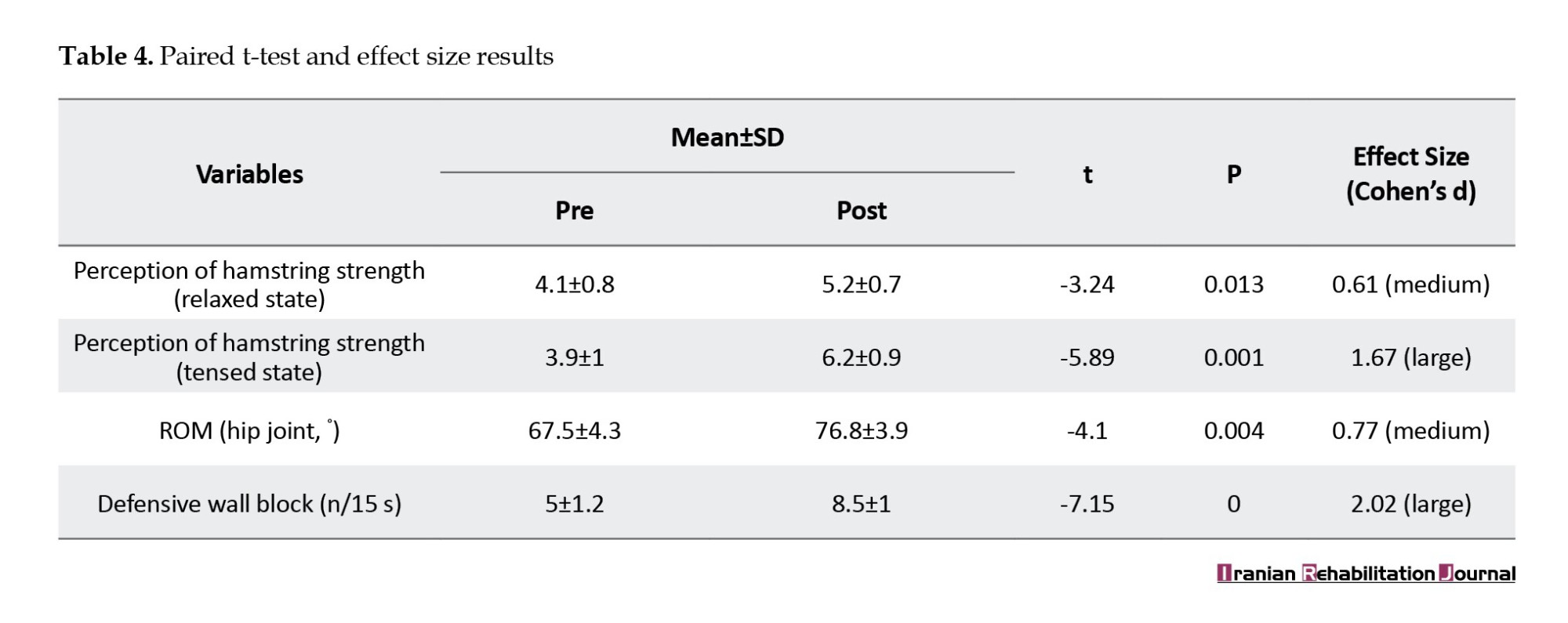
As seen from Table 3, all the variables improved statistically significantly (P<0.05) with different effect sizes ranging from medium to large, which illustrates variability in the responsiveness of clinical and functional measures. The Defensive Wall Block evidenced the largest effect size (d=2.02), illustrating that Swiss ball training effectively integrates hamstring strength, hip mobility, and sport-specific neuromuscular control in enhancing defensive ability. In contrast, perception of resting state hamstring strength (d=0.61) and range of hip joint motion (d=0.77) were affected mediumly.
Discussion
Significant improvements were found in all measured outcomes following the 8-week Swiss ball rehabilitation program. As shown in Table 4, perceived hamstring strength increased in both relaxed (pre: 4.1±0.8 → post: 5.2±0.7; P=0.013) and tensed states (pre: 3.9±1.0 → post: 6.2±0.9; P=0.001), hip joint range of motion improved (67.5±4.3° → 76.8±3.9°; P=0.004), and defensive wall block showed the greatest gain (5.0±1.2 → 8.5±1.0; P<0.001). Effect sizes ranged from medium to large, indicating strong practical relevance. These outcomes reflect the effectiveness of the structured Swiss ball rehabilitation protocol in enhancing hamstring strength, flexibility, and functional performance through progressive exercises that promoted faster recovery and improved neuromuscular control.
Gains observed are consistent with biomechanical and neuromuscular benefits of unstable surface training. Swiss ball training, with dynamic stabilization, eccentric-concentric activation of the muscles, and proprioceptive feedback, most likely increased hamstring neuromuscular effectiveness and joint mobility [29]. The substantial overall effect size on defensive wall block performance suggests successful transfer of strength and flexibility adaptations to sport-specific performance, in particular reactive agility and explosive power—both crucial to handball defense [30].
Medium effects on passive hamstring qualities (relaxed-state strength sensation and range of motion) reflect the lagging adaptation of muscle stiffness and connective tissue compliance to dynamic training [29]. Passive flexibility gains may require longer interventions or adjunct therapy (e.g. foam rolling, static stretching) to achieve equivalent improvements to active neuromuscular outcomes. The findings provide further support to current evidence that unstable surface training provides increased prominence on neuromuscular coordination at the cost of passive tissue adaptation [31].
The diversity of rehabilitation exercises, their gradual progression from easy to difficult, and the commitment of the participants significantly contributed to the recovery process. When designing the rehabilitation exercises, the researcher should ensure a gradual approach to help the affected hamstring muscles adapt without causing pain, thereby facilitating effective recovery [7].
The researcher followed a gradual rehabilitation process for the hamstring muscles, yielding positive results. The principle of gradual progression serves as a safeguard against internal joint and muscle tendon disorders, preventing muscle spasms [7, 8]. The duration of treatment and rehabilitation varies depending on the injury type, location, and treatment methods used. It is crucial to complete the rehabilitation period to ensure full recovery [29].
Conclusion
This study highlights the Swiss ball rehabilitation program as a valuable method for recovering hamstring function, hip mobility, and defensive performance in handball players following injury. Despite the large effects of dynamic and neuromuscular measures, the medium effects of passive properties demonstrate the need for multimodal strategies to elicit tissue-level adaptations.
Study limitations
Single-group pre-post design: Without a control group, causal inferences about the intervention’s efficacy are extensive. Short-term follow-up: Retention of clinical gains over the long term and re-injury rates remain untested, limiting conclusions about sustained clinical relevance.
Future research recommendations
Randomized controlled trials: Compare Swiss ball rehabilitation with conventional protocols (e.g. eccentric training) to establish its unique benefits. Advanced biomechanical quantities: Use 3D motion analysis, muscle architecture imaging (e.g. MRI/ultrasound), and force plate kinetics to quantify passive and active adaptation.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Scientific Research Ethics Committee of Al-Mustansiriya University, College of Physical Education and Sports Sciences (Code: 35, April 28, 2023). Comprehensive ethical guidelines were adhered to, ensuring the safety and well-being of all participants. This includes obtaining informed consent from all participants and their legal guardians.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Alaa Mohammed Jasim; Methodology, data collection and data analysis: Ghufran Zaid Aziz; Writing the original draft and review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the College of Physical Education and Sports Sciences at Al-Mustansiriya University for their valuable support during this research.
References
In the last few decades, sports rehabilitation and sports medicine have been transformed by advances in biomechanics, technology, and interprofessional practices for injury management [1, 2]. Modern practices in contemporary rehabilitation are today aimed not only at speedy recovery but also at readmission of sportspersons to pre-injury level performance through evidence-based sport practice [3]. These advances have played a central role in balancing the complex interplay among mechanisms of injury, sport-specific prevention, and functional rehabilitation [4], particularly for sports with high injury risk like handball, where sudden deceleration changes, violent sprinting, and impact defensive maneuvers make the athlete susceptible to hamstring strain injury (HSI) [5, 6].
HSIs remain a current problem in handball, accounting for 12–15% of total sports injuries and tending to result in prolonged recovery and impact technical performance through ruptured training cycles [7, 8]. The physical stresses of handball, such as sudden decelerations and accelerations, and defense techniques, such as the block wall, expose the hamstring muscles to significant stress [9]. The block wall, a cornerstone of modern defensive play, relies on pinpoint coordination, explosive power, and dynamic stability to extinguish shots and initiate counterattacks. However, poor biomechanics or residual weakness from an injury can get in the way of this capacity, compromising personal and team performance [10].
Traditionally, rehabilitation programs have focused on the maintenance of muscle strength and range of motion (ROM), but more recent evidence indicates that balancing neuromuscular training to counter functional imbalances and avoid the risk of re-injury is necessary [10-12]. Recent technological and methodological advancements have revolutionized rehabilitation models, and Swiss ball exercises have become a cornerstone intervention to enhance neuromuscular control and functional rehabilitation in sports [13, 14]. The Swiss ball hamstring curl and wall squat are specific exercises aimed at improving hamstring strength, core stability, and dynamic balance by co-activating various muscles on unstable surfaces [15]. Experiments demonstrate that Swiss ball training can improve trunk extensor/flexor endurance, lower limb coordination, and control of the lumbopelvic region, which are crucial to prevent HSI and optimize sport-specific movement patterns, such as the block wall technique during handball [16, 17].
Although eccentric training was initially found useful in the prevention and rehabilitation of HSI, existing protocols fail to incorporate sport-specific neuromuscular training and biomechanical specificity, which are necessary for returning functional performance in defensive movements such as the block wall [18]. Swiss ball exercise, in its capacity to optimize eccentric-concentric activation of the muscles and dynamic stabilization [19].
By prioritizing hip joint mobility, hamstring strength, and lumbopelvic control, this intervention focuses on the performance demands of handball’s high-impact defensive maneuvers, which are commonly interrupted after injury [20]. In addition, the study’s focus on quantifying motor control adjustments and defensive blocking effectiveness is congruent with the increasing imperative to relate clinical outcomes to sport-specific performance measures.
Materials and Methods
This single-group pre-post prospective study adhered to the consolidated standards of reporting trials statement. The population was Baghdad Premier League club players, namely Al-Talaba, Al-Jaish, Al-Shurta, Al-Karkh, and Al-Hashd clubs. The assessment was conducted at the College of Physical Education and Sports Sciences from January 2023 to June 2024. The study was conducted per the principles of the Declaration of Helsinki. All eligible participants provided written informed consent and received a copy of their executed consent form for their personal records. The participants were informed that they could withdraw from the study at any point without obligation. Adverse effects (e.g. increased pain) were also noted.
Population
A priori power analysis (G*Power software, version 3.1.9.7) indicated a required sample size of n=28 to detect a medium effect size (d=0.6) in hamstring strength gains with 80% power (α=0.05). To allow for a 15% dropout, 32 participants were recruited.
The participants eligible for this study were athletes aged 18-35 years with a grade I hamstring injury diagnosis confirmed by magnetic resonance imaging (MRI) and clinical examination conducted by a physician. They had no prior history of recurrent hamstring injuries or surgical interventions and were engaged in professional or semi-professional handball. All participants provided written informed consent prior to the study [21]. The exclusion criteria included evidence of grade II or grade III hamstring injury, other lower limb musculoskeletal injuries affecting movement or performance, a history of neurological or orthopedic conditions impacting gait or balance, or an inability to comply with necessary procedures.
Assessments
The participants were evaluated at two time points: Pre-intervention and post-intervention. They were recruited over eight weeks. After initial screening (demographic data collection, and physical examination), they were recruited for the study. The study outcomes were hip joint ROM, hamstring muscle strength, and defensive blocking performance in handball. The study flow diagram is shown in Figure 1.
The hip joint ROM was recorded following a protocol standardized for validation by expert consensus [22]. Measurements were taken 1–3 days post-injury to standardize acute-phase measurements. A Casio cinematic camera (Casio Computer Co., Ltd., Tokyo, Japan; 25 frames per second) mounted on a tripod was used to record the joint angles during active hip flexion and extension movements. Adhesive markers were placed on anatomical landmarks (lateral femoral condyle, greater trochanter, and anterior superior iliac spine) to enhance the precision of movement measurement [23].
Participants performed slow, controlled flexion and extension movements of the affected limb while supine on a medical examination table, moving to their maximum pain-free range. Video recordings were analyzed using Kinovea software (version 0.9.2; open-source software developed by Olivier Rossel, France) to measure hip joint angles (intraclass correlation coefficient [ICC]=0.79) [24]. Goniometric measurements were cross-referenced with a panel of three sports medicine experts to maintain adherence to accepted biomechanical criteria. A blinded examiner performed all measurements to limit measurement bias.
Hamstring muscle strength was measured using a handheld force sensor unit (MicroFET2 Dynamometer, Hoggan Scientific, Salt Lake City, USA), which is a valid measure of peak force production in Newtons. The participants were positioned prone on a medical examination table. During the relaxed condition test, the knee was kept in full extension to measure baseline muscle tone and passive resistance. The examiner placed the force sensor over the posterior distal femur and applied minimal pressure without eliciting any voluntary contraction from the participant [25].
For the tensed state test, the participants flexed their knees to approximately 30°, which was considered the optimum mid-range position for hamstring activation. Under these conditions, the participants were requested to maximally contract their hamstring muscles against the resistance of the force sensor. Three maximal voluntary isometric contractions (MVICs) were performed for each limb by each participant, with 30 seconds of rest between trials to minimize fatigue and ensure consistency of effort between repetitions (ICC=0.89 for relaxed and ICC=0.92 for tensed) [26].
Defensive blocking performance was evaluated using a standardized protocol adapted from validated handball-specific functional tests. The test evaluates an athlete’s ability to execute repetitive defensive blocks with technical precision, speed, and consistency in game-like conditions.
The test was conducted on a standard handball court. Two handballs were suspended from goalposts at a height of 2.6 meters, which could be adjusted downward for youth or female athletes. Adhesive tape markers were used to designate the 6-meter line, vertically aligned with the suspended balls, and two goalposts on the 8- to 9-meter line, 3 meters apart. A middle starting point was designated halfway between the two balls. Players began each trial from a stationary standing position at this location.
On a visual start signal, players performed a cycle consisting of a forward sprint, a jumping block to touch one of the balls with both hands, a controlled landing, and recovery to the starting position as fast as possible. This cycle was repeated as many times as possible within 15 s. All movements had to replicate real-game defense mechanics, including correct arm position, explosive jumping, and controlled direction changes.
Some performance criteria were utilized to uphold reliability and validity. Bilateral hand contact on the ball must be made on each block attempt. Each movement must be initiated from the established starting position, and any deviation invalidates that repetition. Attempts that did not meet these criteria (single-hand contact or a step outside the established area) were considered invalid and were not counted in the scoring. Scoring was based on the number of successful defensive blocks completed within 15 s [27].
Intervention
The rehabilitation program comprised Swiss ball exercises to improve hamstring flexibility, elasticity, and strength. The program lasted 8 weeks, with the participants attending four sessions per week, each lasting 20–30 minutes. The exercises were designed to progress from simple to complex movement patterns based on the functional demands of the participants. The sessions started with a warm-up, proceeded with the main Swiss ball exercises, and concluded with a cool-down phase [28]. Tables 1 and 2 present a detailed explanation of the model and exercise protocol.
Statistical analysis
Statistical analysis was performed using SPSS software, version 25 (IBM Corp., USA). Descriptive statistics were employed to describe the participants’ demographic and baseline characteristics. Normality test of data was conducted using the Shapiro-Wilk test. For variables in normal distribution, a paired t-test was utilized.
To compare the outcome measures (i.e. ROM of the hip joint, hamstring strength, and defensive blocking performance) before and after the intervention, a paired-samples t-test was used. Statistical significance was set at P<0.05. Results were reported as Mean±SD, and effect sizes were calculated using Cohen’s d to allow for comparison of the size of change.
Results
Participant demographics
21 handball players (mean age: 24.6±3.2 years) with Grade I hamstring injuries were included in the study. Baseline demographic and injury-related characteristics are shown in Table 3. All subjects were competitive players in the Baghdad Premier League, with 6.5±2.1 years of competitive handball experience. Injuries were observed most frequently in the dominant limb (62.5%) in high-level defensive play or sprinting activities of play. Shapiro-Wilk test confirmed normal distribution of baseline data (P>0.05).
As seen from Table 3, all the variables improved statistically significantly (P<0.05) with different effect sizes ranging from medium to large, which illustrates variability in the responsiveness of clinical and functional measures. The Defensive Wall Block evidenced the largest effect size (d=2.02), illustrating that Swiss ball training effectively integrates hamstring strength, hip mobility, and sport-specific neuromuscular control in enhancing defensive ability. In contrast, perception of resting state hamstring strength (d=0.61) and range of hip joint motion (d=0.77) were affected mediumly.
Discussion
Significant improvements were found in all measured outcomes following the 8-week Swiss ball rehabilitation program. As shown in Table 4, perceived hamstring strength increased in both relaxed (pre: 4.1±0.8 → post: 5.2±0.7; P=0.013) and tensed states (pre: 3.9±1.0 → post: 6.2±0.9; P=0.001), hip joint range of motion improved (67.5±4.3° → 76.8±3.9°; P=0.004), and defensive wall block showed the greatest gain (5.0±1.2 → 8.5±1.0; P<0.001). Effect sizes ranged from medium to large, indicating strong practical relevance. These outcomes reflect the effectiveness of the structured Swiss ball rehabilitation protocol in enhancing hamstring strength, flexibility, and functional performance through progressive exercises that promoted faster recovery and improved neuromuscular control.
Gains observed are consistent with biomechanical and neuromuscular benefits of unstable surface training. Swiss ball training, with dynamic stabilization, eccentric-concentric activation of the muscles, and proprioceptive feedback, most likely increased hamstring neuromuscular effectiveness and joint mobility [29]. The substantial overall effect size on defensive wall block performance suggests successful transfer of strength and flexibility adaptations to sport-specific performance, in particular reactive agility and explosive power—both crucial to handball defense [30].
Medium effects on passive hamstring qualities (relaxed-state strength sensation and range of motion) reflect the lagging adaptation of muscle stiffness and connective tissue compliance to dynamic training [29]. Passive flexibility gains may require longer interventions or adjunct therapy (e.g. foam rolling, static stretching) to achieve equivalent improvements to active neuromuscular outcomes. The findings provide further support to current evidence that unstable surface training provides increased prominence on neuromuscular coordination at the cost of passive tissue adaptation [31].
The diversity of rehabilitation exercises, their gradual progression from easy to difficult, and the commitment of the participants significantly contributed to the recovery process. When designing the rehabilitation exercises, the researcher should ensure a gradual approach to help the affected hamstring muscles adapt without causing pain, thereby facilitating effective recovery [7].
The researcher followed a gradual rehabilitation process for the hamstring muscles, yielding positive results. The principle of gradual progression serves as a safeguard against internal joint and muscle tendon disorders, preventing muscle spasms [7, 8]. The duration of treatment and rehabilitation varies depending on the injury type, location, and treatment methods used. It is crucial to complete the rehabilitation period to ensure full recovery [29].
Conclusion
This study highlights the Swiss ball rehabilitation program as a valuable method for recovering hamstring function, hip mobility, and defensive performance in handball players following injury. Despite the large effects of dynamic and neuromuscular measures, the medium effects of passive properties demonstrate the need for multimodal strategies to elicit tissue-level adaptations.
Study limitations
Single-group pre-post design: Without a control group, causal inferences about the intervention’s efficacy are extensive. Short-term follow-up: Retention of clinical gains over the long term and re-injury rates remain untested, limiting conclusions about sustained clinical relevance.
Future research recommendations
Randomized controlled trials: Compare Swiss ball rehabilitation with conventional protocols (e.g. eccentric training) to establish its unique benefits. Advanced biomechanical quantities: Use 3D motion analysis, muscle architecture imaging (e.g. MRI/ultrasound), and force plate kinetics to quantify passive and active adaptation.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Scientific Research Ethics Committee of Al-Mustansiriya University, College of Physical Education and Sports Sciences (Code: 35, April 28, 2023). Comprehensive ethical guidelines were adhered to, ensuring the safety and well-being of all participants. This includes obtaining informed consent from all participants and their legal guardians.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Alaa Mohammed Jasim; Methodology, data collection and data analysis: Ghufran Zaid Aziz; Writing the original draft and review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the College of Physical Education and Sports Sciences at Al-Mustansiriya University for their valuable support during this research.
References
- Khaliliyan H, Ansari M, Bahramizadeh M, Batra K, Afolabi A, Ghaffari F,et al. Changes in postural control due to electrical stimulation therapy for ankle instability: A systematic review. Journal of Rehabilitation Sciences & Research. 2024; 11(3):117-26. [DOI:10.30476/jrsr.2024.102704.1486]
- Khaliliyan H, Sharafatvaziri A, Safaeepour Z, Bahramizadeh M. Gait and muscle activity measures after biomechanical device therapy in subjects with ankle instability: A systematic review. The Foot. 2024; 59:102083. [DOI:10.1016/j.foot.2024.102083] [PMID]
- Evans TA, Lam KC. Clinical outcomes assessment in sport rehabilitation. Journal of Sport Rehabilitation. 2011; 20(1):8-16. [DOI:10.1123/jsr.20.1.8] [PMID]
- Bahramizadeh M, Khaliliyan H, Sharafatvaziri A, Sadeghi-Demneh E, Szarpak L, Pruc M, et al. Postural control measures after lateral ankle sprain while wearing ankle orthoses: A systematic review. Iranian Rehabilitation Journal. 2024; 22(1):1-4. [DOI:10.32598/irj.22.1.1719.3]
- Prentice W. Rehabilitation techniques for sports medicine and athletic training. New York: Routledge; 2024. [DOI:10.4324/9781003526308]
- Jiang Y. Combination of wearable sensors and internet of things and its application in sports rehabilitation. Computer Communications. 2020; 150:167-76. [DOI:10.1016/j.comcom.2019.11.021]
- Prior M, Guerin M, Grimmer K. An evidence-based approach to hamstring strain injury: A systematic review of the literature. Sports Health. 2009; 1(2):154-64. [DOI:10.1177/1941738108324962] [PMID]
- Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. Journal of Orthopaedic & Sports Physical Therapy. 2010; 40(2):67-81. [DOI:10.2519/jospt.2010.3047] [PMID]
- da Silva Miranda RM, Lopes KJ, Fragata MB, Boaes DC, Ramos MS, Borges GF. Muscle Skeletal Disorders and Factors of Stress in Handball Athletes. Journal of Health Sciences. 2019; 21(2):144-8. [DOI:10.17921/2447-8938.2019v21n2p144-148]
- García-Sánchez C, Navarro RM, Karcher C, de la Rubia A. Physical demands during official competitions in elite handball: A systematic review. International Journal of Environmental Research and Public Health. 2023; 20(4):3353. [DOI:10.3390/ijerph20043353] [PMID]
- Michalsik LB, Aagaard P. Physical demands in elite team handball: Comparisons between male and female players. The Journal of Sports Medicine and Physical Fitness. 2015; 55(9):878-91. [PMID]
- Sharifi G, Najafabadi AB, Ghashghaei FE. Oxidative stress and total antioxidant capacity in handball players. Advanced Biomedical Research. 2014; 3(1):181. [DOI:10.4103/2277-9175.139538] [PMID]
- Brandão FM, Duarte TS, Cunha VF, Werneck FZ, Bara Filho MG. Physical demands and psychophysiological stress in young athletes team sports. Journal of Physical Education. 2023; 34:e3440. [DOI:10.4025/jphyseduc.v34i1.3440]
- Cunniffe B, Fallan C, Yau A, Evans GH, Cardinale M. Assessment of physical demands and fluid balance in elite female handball players during a 6-day competitive tournament. International Journal of Sport Nutrition and Exercise Metabolism. 2015; 25(1):78-96. [DOI:10.1123/ijsnem.2013-0210] [PMID]
- Vurgun H, Edis Ç. Only swiss ball core exercises can improve of functional movement screen score and core muscle endurance?. International Journal of Applied Exercise Physiology. 2020; 9(10):181-7. [Link]
- Manchado C, García-Ruiz J, Cortell-Tormo JM, Tortosa-Martínez J. Effect of core training on male handball players’ throwing velocity. Journal of Human Kinetics. 2017; 56:177. [DOI:10.1515/hukin-2017-0035] [PMID]
- Alhenawy S. Influence of swiss ball crunches on the technical performance of swallow skills on rings for under 14 years-old gymnastics team. International Journal of Sports Science and Arts. 2024; 26(1):20-52. [DOI:10.21608/eijssa.2024.284077.1225]
- Petruzela J, Papla M, Stastny P. Conditioning strategies for improving handball throwing velocity: A systematic review and meta-analyses. Journal of human kinetics. 2023; 87:189. [DOI:10.5114/jhk/162017] [PMID]
- Anderson KG. Muscle and force characteristics in stable and unstable exercise protocols [master thesis]. St. John's: Memorial University of Newfoundland. [Link]
- Yan Y, Seoyoung P, Seomyeong H, Zhao Y. The effect of 12-week combined balance and plyometric training on dynamic balance and lower extremity injury risk in college dancers. Frontiers in Physiology. 2025; 16:1501828. [DOI:10.3389/fphys.2025.1501828] [PMID]
- Edouard P, Branco P, Alonso JM. Muscle injury is the principal injury type and hamstring muscle injury is the first injury diagnosis during top-level international athletics championships between 2007 and 2015. British Journal of Sports Medicine. 2016; 50(10):619-30. [DOI:10.1136/bjsports-2015-095559] [PMID]
- Moreside JM, McGill SM. Hip joint range of motion improvements using three different interventions. The Journal of Strength & Conditioning Research. 2012; 26(5):1265-73. [DOI:10.1519/JSC.0b013e31824f2351] [PMID]
- Yamazaki K. A logic of the firm without center technology a case study of casio computer co., ltd in the digital camera industry. Paper presented at: The Proceedings of the 4th European Conference on Entrepreneurship and Innovation. 11 September 2009; Antwerp, Belgium. [Link]
- Yazdani S, Homayouni S, Eftekhari H, Yazdani S. Kinovea program for assessment of female student’s knee joint proprioception in closed kinetic chain: Emphasis on validity and reliability. Journal of Advanced Sport Technology. 2023; 7(2):56-64. [DOI:10.22098/jast.2023.2473]
- Claudino JG, Cardoso Filho CA, Bittencourt NF, Gonçalves LG, Couto CR, Quintão RC, et al. Eccentric strength assessment of hamstring muscles with new technologies: A systematic review of current methods and clinical implications. Sports Medicine-Open. 2021; 7(1):10. [DOI:10.1186/s40798-021-00298-7] [PMID]
- Reurink G, Goudswaard GJ, Moen MH, Tol JL, Verhaar JA, Weir A. Strength measurements in acute hamstring injuries: Intertester reliability and prognostic value of handheld dynamometry. Journal of Orthopaedic & Sports Physical Therapy. 2016; 46(8):689-96. [DOI:10.2519/jospt.2016.6363] [PMID]
- García-de-Alcaraz A, Ortega E, Palao JM. Technical-tactical performance profile of the block and dig according to competition category in men’s volleyball. Motriz: Revista de Educação Física. 2016; 22(2):102-9. [DOI:10.1590/S1980-6574201600020013]
- Rusdiawan A, Kusuma DA, Firmansyah A, Wismanadi H, Cemal Ö, Wicahyani S, et al. A combination of swissball hamstring curl and stiff-leg deadlift training on agility, hamstring asymmetry, and leg power in badminton athletes with hamstring asymmetry conditions. Retos. 2024; 2024(59):666-73. [DOI:10.47197/retos.v59.107995]
- Escamilla RF, Lewis C, Bell D, Bramblet G, Daffron J, Lambert S, et al. Core muscle activation during Swiss ball and traditional abdominal exercises. Journal of Orthopaedic & Sports Physical Therapy. 2010; 40(5):265-76. [DOI:10.2519/jospt.2010.3073] [PMID]
- Biz C, Nicoletti P, Baldin G, Bragazzi NL, Crimi A, Ruggieri P. Hamstring strain injury (HSI) prevention in professional and semi-professional football teams: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8272. [DOI:10.3390/ijerph18168272] [PMID]
- Wiriawan O, Rusdiawan A, Kusuma DA, Firmansyah A, García-Jiménez JV, Zein MI, et al. Unilateral hamstring muscle strengthening exercises can improve hamstring asymmetry and increase jumping performance in sub-elite badminton athletes. Retos. 2024; 2024(54):761-70. [DOI:10.47197/retos.v54.103783]
Article type: Original Research Articles |
Subject:
Sport rehabilitation
Received: 2025/06/11 | Accepted: 2025/07/21 | Published: 2025/12/1
Received: 2025/06/11 | Accepted: 2025/07/21 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
