
988368
Thu, Jul 30, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 389-398 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghafoor A, Tariq F, Jawad S, Tariq N. Urdu Translation and Psychometric Properties of Spinal Cord Injury Spasticity Evaluation Tool. Iranian Rehabilitation Journal 2025; 23 (4) :389-398
URL: http://irj.uswr.ac.ir/article-1-2564-en.html
URL: http://irj.uswr.ac.ir/article-1-2564-en.html



1- Riphah College of Rehabilitation and Allied Health Sciences (RCRS), Faculty of Rehabilitation Sciences and Allied Health Sciences, Riphah International University, Lahore, Pakistan.
Keywords: Functional independence measure, Spinal cord injury (SCI), Spinal cord injury spasticity evaluation tool (SCI-SET), Reliability, Urdu translation, Validity
Full-Text [PDF 566 kb]
(402 Downloads)
| Abstract (HTML) (2087 Views)
Full-Text: (360 Views)
Introduction
Spinal cord injury (SCI) is a severe neurological condition that leads to physical dependence, morbidity, psychological stress, and significant financial burden [1]. Over the past 30 years, global prevalence has increased from 236 to 1298 cases per million, with an estimated 250000 to 500000 new cases annually [2, 3].
SCI progresses through two main stages: Primary and secondary injury. The primary injury occurs immediately following abrupt, serious spinal trauma and is frequently accompanied by fractures and displacements of the vertebrae. The main damage includes axonal network disruption, spinal joint rupture and neural stromal loss [4, 5]. The length of spinal cord entrapment and the degree of initial damage determine the severity of SCI [6]. Despite clinical manifestations suggesting complete functional loss, some axons may remain connected, indicating an incomplete injury [7]. Secondary injury begins with the primary injury and results in additional biochemical and biomechanical secondary injury to spinal tissues. This can cause neuronal excitotoxicity, leading to nucleic acid, protein, and phospholipid damage and consequent neurotoxicity [8].
A serious and complex medical illness, SCI affects 40 million people globally each year, with 2.1 to 130.7 million cases occurring in underdeveloped nations [9]. SCI places one of the biggest burdens on society, frequently resulting in severe impairment, reduced quality of life (QoL), and considerable emotional, financial, and social impacts on patients and their families [10]. In addition to major long-term medical consequences like exhaustion, discomfort, stiffness, and pressure sores, SCI can result in paralysis and sensory loss [11]. Males are two to five times more likely to experience it [12].
SCI often results in hip joint subluxation, lower leg paralysis, and autonomic dysreflexia (AD), which affects 48-60% of cases above the thoracic 6th vertebral level (T6), causing sudden high blood pressure. Understanding the SCI’s pathophysiology and recovery mechanisms is crucial for developing effective treatments [13]. Normal spinal cord function involves interactions among various cell types, which are disrupted post-injury, leading to impaired recovery [2].
After SCI, QoL is a crucial factor to consider. According to one source, spasticity contributes to a lower QoL. It can also cause pain, insomnia, pressure ulcers, and contractures [9, 14]. Numerous psychological aspects have been demonstrated to be associated with the degree of spasticity [15]. In addition, it may result in contractures, pressure ulcers, discomfort, and insomnia. Several physical therapy methods are recommended for the treatment of spasticity. These include heat, transcutaneous electric nerve stimulation, passive stretching, electromyography biofeedback, and other forms of exercise [16]. However, the effectiveness of any or all of these therapies is unknown [9]. From a therapeutic perspective, the knowledge that individuals with SCIs may have longer life expectancies following their lesions but may also experience a greater number of secondary health complications highlights the need to provide targeted care for particular secondary health complications and comorbidities [17].
In Pakistan, SCIs have not received significant attention in research. The nation’s 2005 northern earthquake was the only occasion on which the subject was brought up. Between 2011 and 2016, 1025 patients were admitted to the hospital. Compared to the corresponding female group, there were three times as many male patients. Ninety percent of patients have paraplegia [18, 19].
In the world, more than 300 million people speak Urdu, which is also Pakistan’s national language. However, the spasticity evaluation tool (SET) is challenging for Urdu-speaking patients with SCI to understand. It aimed to improve healthcare accessibility for Urdu-speaking individuals with SCI, ensuring they can accurately communicate their symptoms and experiences to healthcare professionals [20]. Ultimately, this study promises to improve the overall management and outcomes of spasticity in the Urdu-speaking SCI population. This study aimed to enhance the standard of care provided to patients with SCI, aiding in the accurate diagnosis, treatment, and monitoring of spasticity.
Materials and Methods
This cross-sectional study was conducted over ten months at the General Hospital in Lahore City, Pakistan, and the Riphah Rehabilitation Center. A pilot sample of 25 participants was used for testing the pre-final version of the questionnaire and was analyzed separately; these individuals were not included in the main reliability and validity analyses. The sample size was 175 people, selected using non-probability convenience sampling. Participants were aged 18 to 45, could read and write Urdu, suffered from SCI for at least six months, and scored at least 24 on the Mini-Mental State Examination (MMSE). Participants with cognitive, visual, auditory, or other neurological conditions (multiple sclerosis or Parkinson’s disease) were excluded. Data were collected using the spasticity evaluation assessment (SCI -SET), a 35-question self-administered assessment that evaluates the impact of spasticity on daily life [21], and the functional independence measure (FIM), an 18-item questionnaire that assesses impairment levels and care burden. The SCI-SET ratings ranged from -3 to +3, based on patient recollections from the previous week. In contrast, the FIM scores ranged from 1 (requiring total assistance) to 7 (full independence), with scores provided by a multidisciplinary team or a single expert.
Study participants were recruited through the rehabilitation clinics in Lahore City and the General Hospital, Lahore City. SCI-SETu was administered to patients with SCI who met the inclusion criteria. A sample of 175 patients was given the SCI-SETu at baseline and after 7 days assess test re-test reliability. Translation of the spasticity assessment tool for individuals with spinal column lesions into the Urdu version using the following steps as per Cosmin guidelines:
Stage 1: Initial translation
In the first phase, the instrument underwent two forward translations from English to Urdu. Bilingual translators with distinct backgroundscompleted the translations to ensure accuracy. Translator #1, a medical professional familiar with the questionnaire’s themes, and Translator #2, who had no medical training, performed these translations. A schematic of the cross-cultural adaptation process is presented in Figure 1.
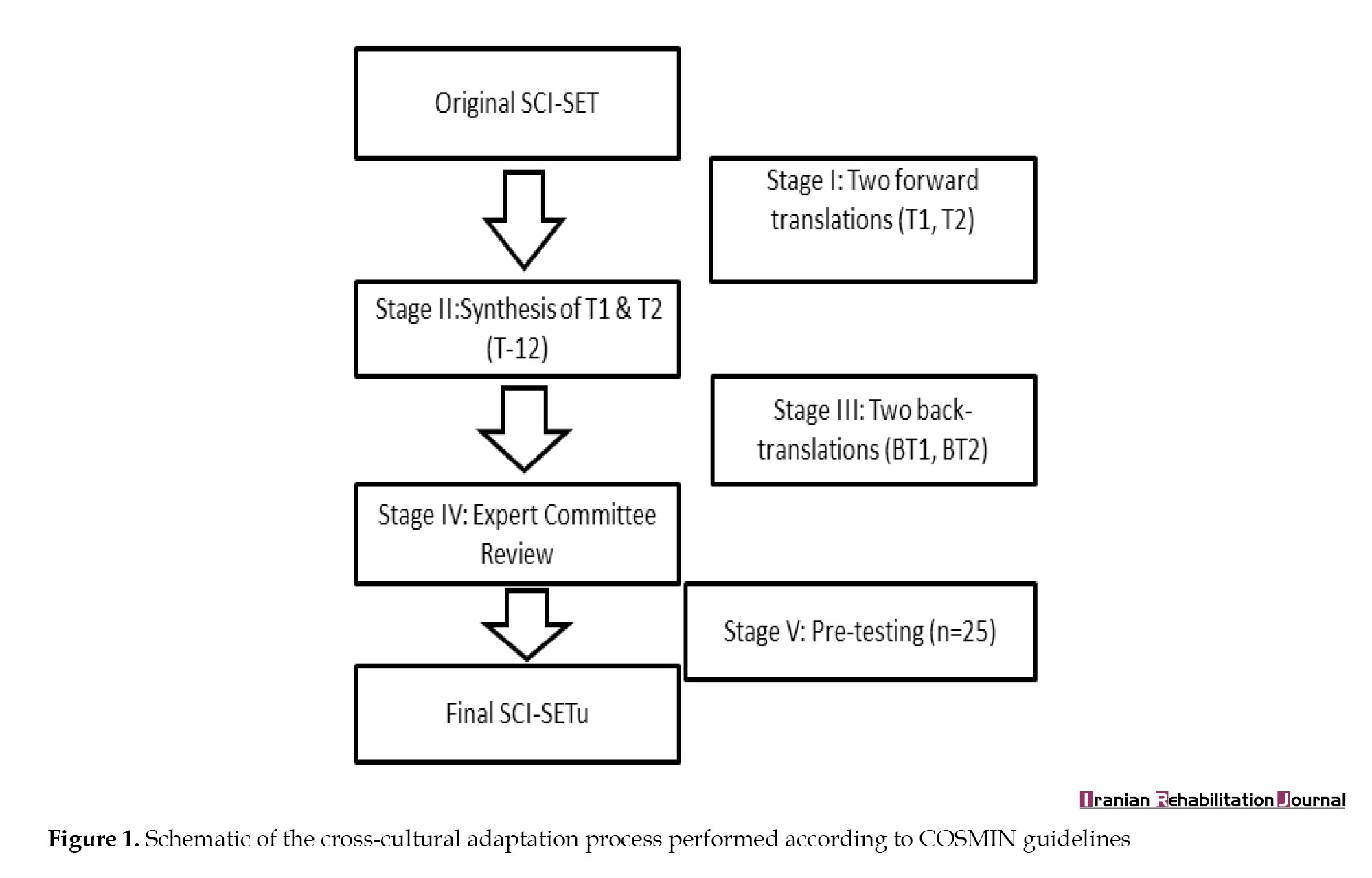
Stage II: Synthesis of these translations
In the second stage, a third impartial person synthesizes the two translations. The original questionnaire combines versions from Translators #1 and #2 to create a common translation (T12).
Stage III: Back translation
The third stage involves back-translating the questionnaire into the original language using the T-12 version. This validation method ensures that the translated version maintains the original information. Two additional back translations (BT1 and BT2) by native English speakers are conducted without revealing the scale’s concepts to prevent bias.
Stage IV: Expert committee
The expert committee works collaboratively, comprising methodologists, health professionals, linguists, and both forward and back translators. In constant contact with the questionnaire’s creators, the committee compiles all versions to create the pre-final questionnaire for field testing. Any discrepancies are addressed through consensus.
Stage V: Test of pre-final version
This stage assesses the viability of the pre-final Urdu version of the SCI-SETu. Twenty-five individuals independently complete the questionnaire and provide feedback on each topic and their responses, ensuring the modified version maintains equivalence in practical settings.
Stage VI: Submission of documentation to developers for appraisal
In the final phase of the adaptation process, the committee submits reports and forms. The committee ensures adherence to proposed stages and verifies that the reports accurately represent the adaptation process.
Pilot testing and adaptation
Subjects who met the inclusion criteria were included in the study. Written informed consent was obtained from all participants. After obtaining demographic data, all participants were asked to fill out the SCI-SETu questionnaire on the instructions, and it was scored on completion.
The analysis was conducted using SPSS for Windows software, version 21. Construct validity was determined by assessing the correlation between the SCI-SETu and FIM scores using Pearson’s correlation coefficients. The strength of correlation was interpreted as follows: Very high (0.90–1.00), strong (0.70–0.89), moderate (0.50–0.69), or weak (<0.50). For test re-test reliability, alongside the intra-class correlation coefficient (ICC), the SEM was calculated using the Equation 1:
1. SEM=SD √(1-ICC)
where SD is the standard deviation of the day 1 scores.
Internal consistency: Given the single assessment for patients, internal consistency was evaluated to gauge reliability. This was measured using Cronbach’s α coefficient, with a satisfactory threshold set at 0.7 or higher.
Test, re-test reliability: Reliability across repeated assessments were established using test re-test reliability. The ICC with 95% confidence intervals (CIs) was utilized for estimation. Internal consistency was also confirmed using Cronbach’s α.
Results
Sample description
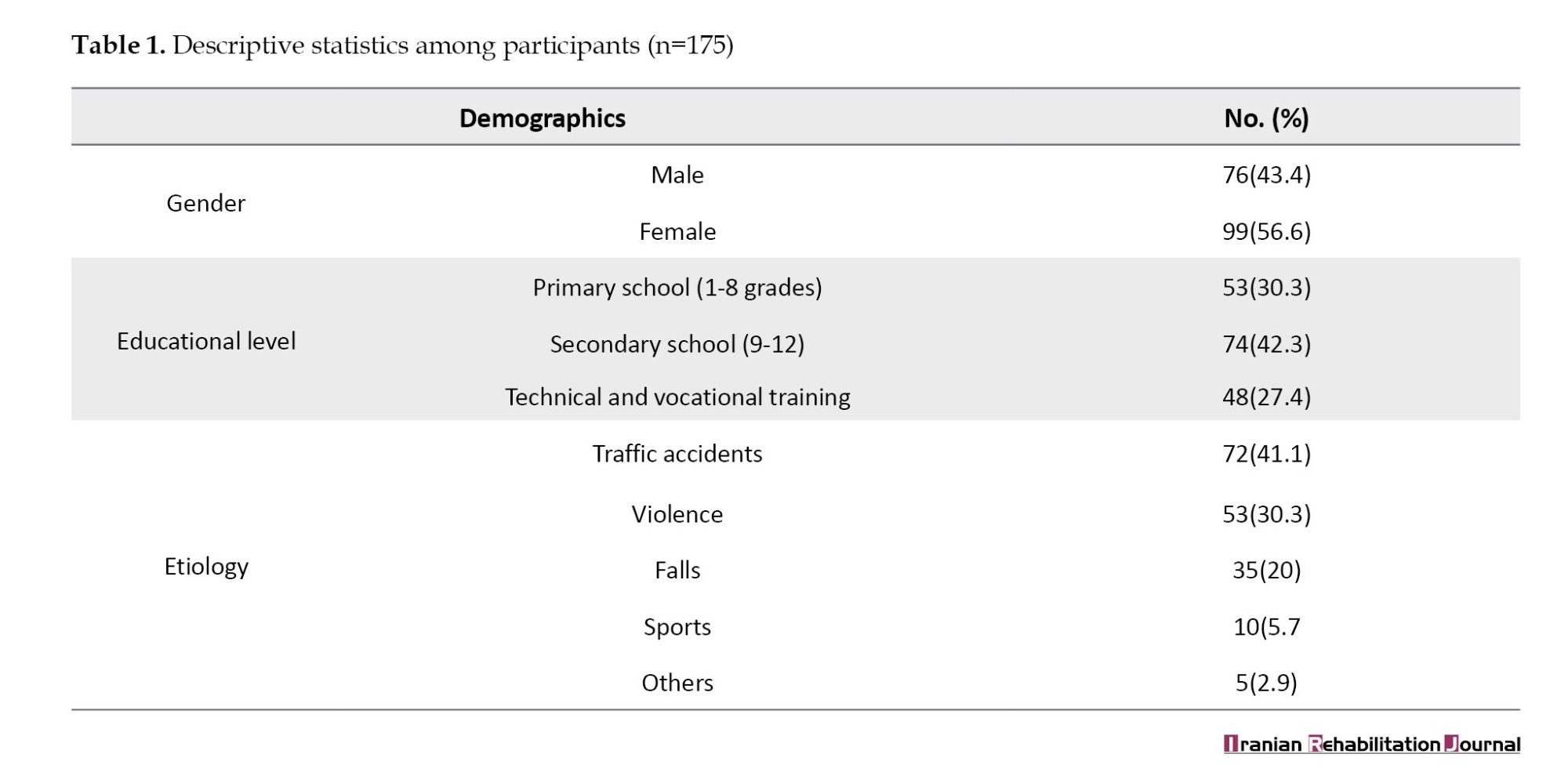
The mean age of the participants was 40.23±5.522 years (min 28 and max 45 years). The gender distribution was 76(43.4%) males and 99(56.6%) females. The etiology of SCI varies. Traffic accidents were the most common cause, 72(41.1%), and violence was the second most prevalent etiology, 53(30.3%). Falls contributed to 35(20%), while sports-related incidents comprised 10(5.7%). The educational level of the study participants was primary school education (1-8 grades) among 53 individuals (30.3%). Secondary school education (9-12 grades) was the most common, with 74 individuals (42.3%). Additionally, 48 individuals (27.4%) had undergone technical and vocational training (Table 1).
Day 1 reading
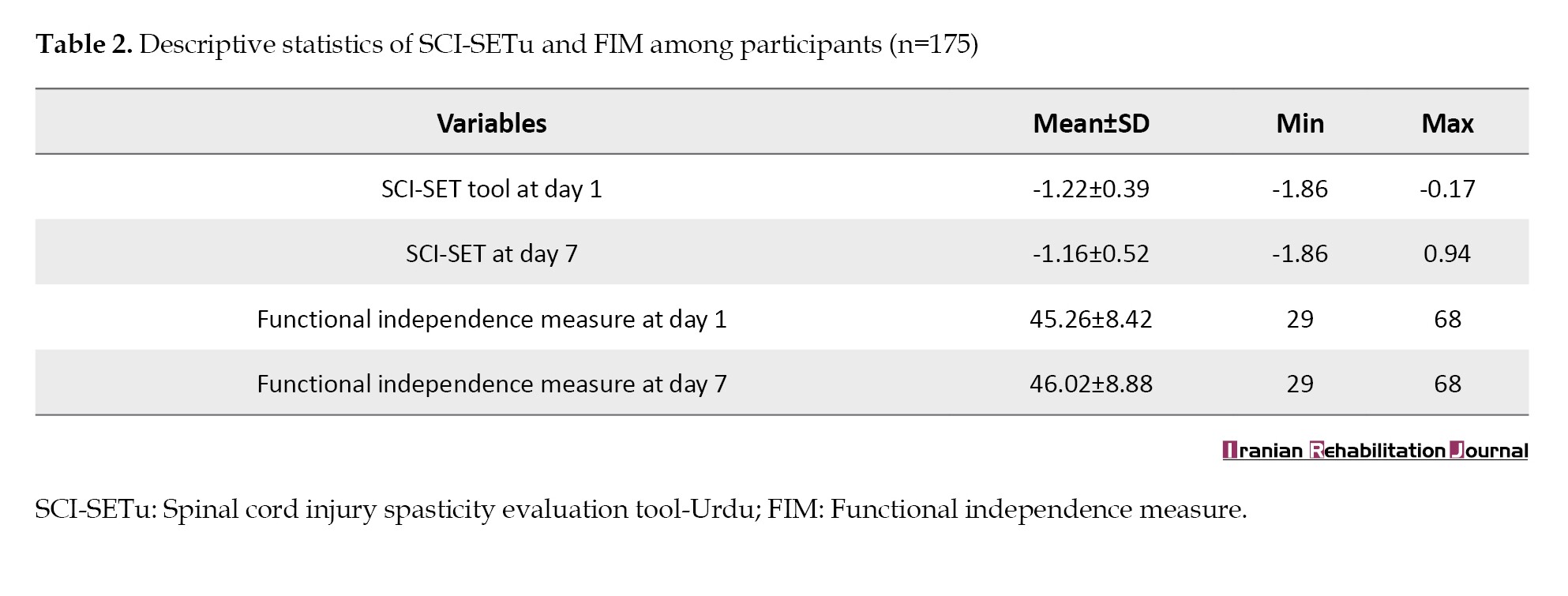
The descriptive statistics for SCI-SETu, on day 1, ranged from -1.86 to -0.17, with a mean of -1.22±0.39. The FIM scores on day 1 ranged from 29 to 68, with a mean of 45.26±8.42 (Table 2).
Day 2 reading
By day 7, the SCI-SETu scores ranged from -1.86 to 0.94, with a mean of -1.16±0.52. On day 7, the FIM scores ranged from 29 to 68, with an increased mean of 46.02±8.88 (Table 2).
Floor and ceiling effects
A floor or ceiling effect was considered present if more than 15% of participants achieved the lowest or highest possible score. Only one participant (0.6%) had the lowest score (-1.86), and one (0.6%) had the highest score (-0.17). No clustering of scores at the extremes was observed, confirming the absence of floor or ceiling effects.
Construct validity
A strong positive correlation was found between the SCI-SETu and the FIM (r=0.788, P<0.01).
Internal consistency
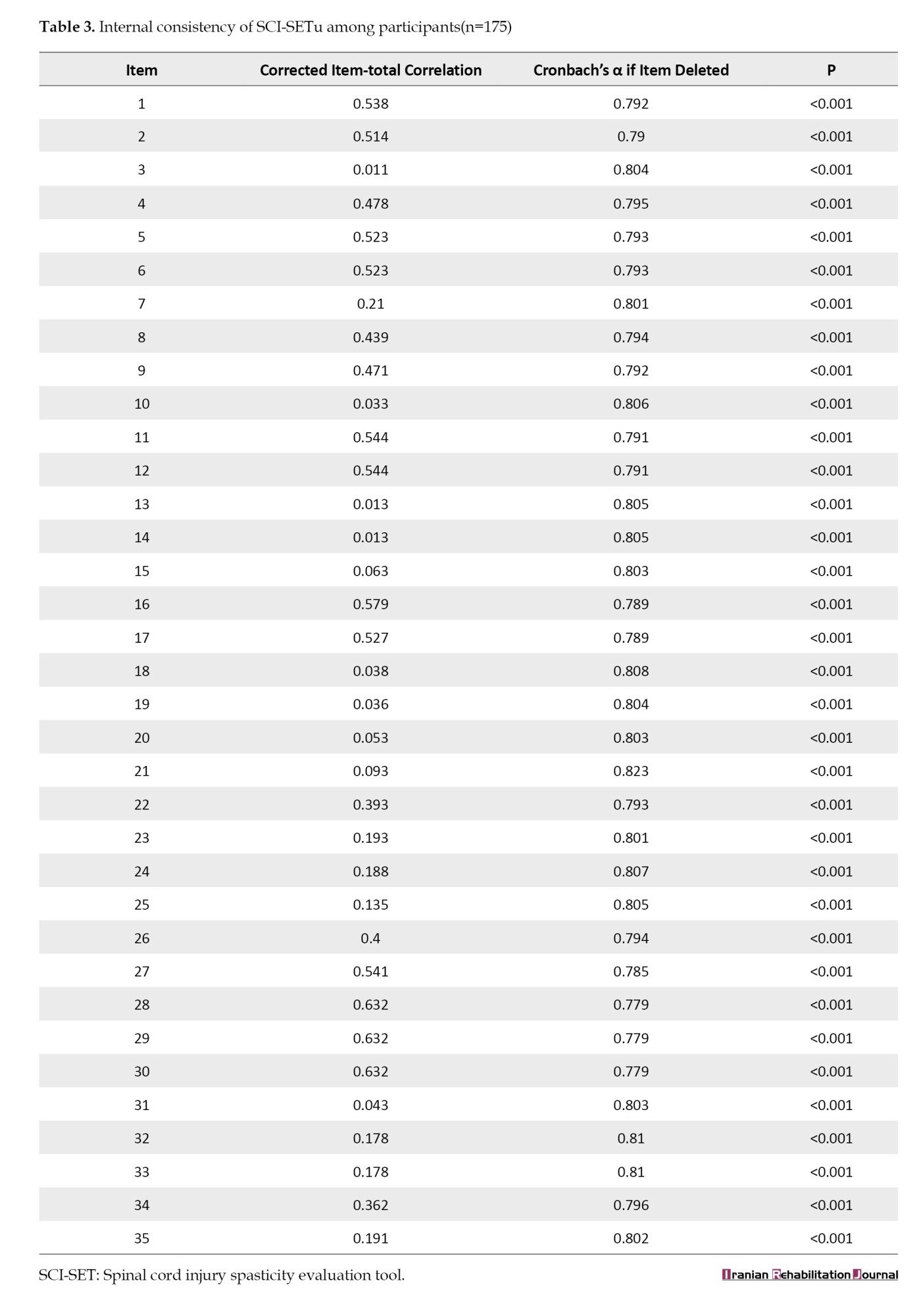
The overall Cronbach’s α for the SCI-SETu was 0.803 (95% CI, 0.759%, 0.842%). The corrected item-total correlations ranged from 0.011 to 0.632. Cronbach’s α if an item was deleted ranged from 0.779 to 0.823. All P were <0.001 (Table 3).
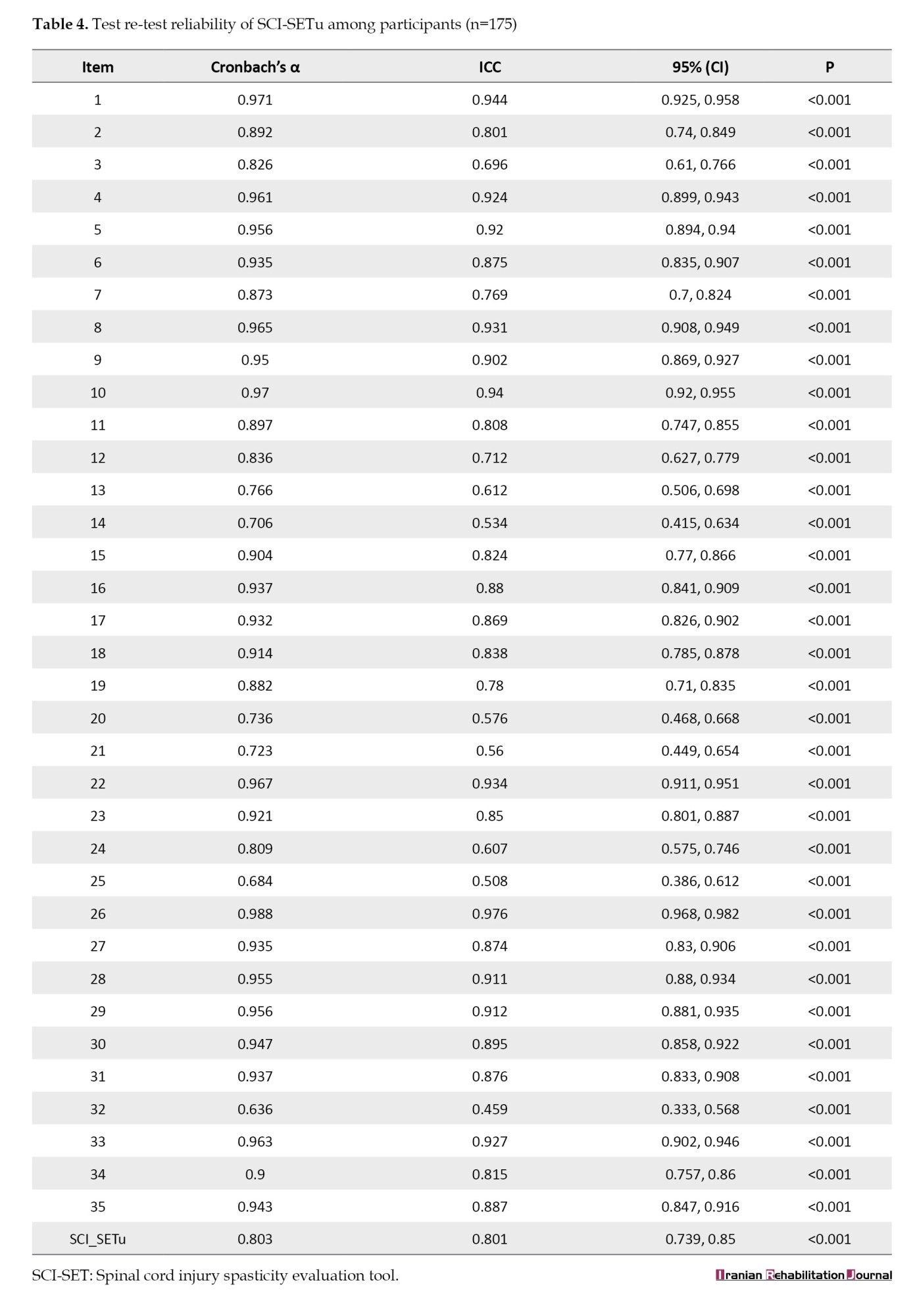
Test re-test reliability
The overall test re-test reliability for the SCI-SETu total score was excellent, with an ICC of 0.801 (95% CI, 0.739%, 0.85%). The SEM was 0.17. Item-level ICCs ranged from 0.459 to 0.976 (Table 4).
Discussion
The translation and validation of assessment instruments are critical for ensuring accurate and meaningful measurements across diverse cultural and linguistic settings. This study aimed to translate the SCI-SET into Urdu (SCI-SETu) and assess its psychometric properties among patients with SCI. The current study shows that the SCI-SETu has strong concept validity, internal consistency, and test re-test reliability, which is consistent with previous studies conducted in Persian and Turkish contexts.
The translation of the SCI-SET into Persian (SCI-SETp) and validation process revealed strong psychometric qualities, with a Cronbach’s α of 0.862 and an ICC agreement for test re-test reliability of 0.84. These indicators demonstrate high internal stability and consistency over time. Our research found comparable results for the Urdu translation, with Cronbach’s α values ranging from 0.779-0.823 and ICCs ranging from 0.459-0.976. These findings indicate that the SCI-SETu is a valid instrument for assessing spasticity in patients with SCI, while retaining the original SCI-SET’s reliability and validity [20].
With an intraclass correlation coefficient (ICC) of 0.8, similar to the aforementioned studies, the cross-cultural validity and reliability of the Turkish version of the SCI-SET, known as the SCI-SETT, was confirmed as well. The vitality scores in the 12 items of the short form health survey (SF-36) and their significant relations to the total and domain scores of the SCI-SETT confirmed the SCI-SETT’s responsiveness in quantifying the impact of spasticity on QoL. Similarly, our investigation revealed a strong positive correlation (r=0.788, P<0.01) between the SCI-SETu and the functional independence measure (FIM), thereby improving its construct validity and applicability in evaluating the complex effects of spasticity on day-to-day functioning in Urdu-speaking patients with SCI [22].
With Cronbach’s α values of 0.862 and 0.8, respectively, the Persian and Turkish versions of the SCI-SET showed strong dependability regarding internal consistency. Similar internal consistency was shown by the SCI-SETu, whose Cronbach’s α values ranged from 0.636 to 0.988. Based on these findings, the Urdu version of the tool retains the other adjustments made to it and the original tool’s dependability, meaning that it assesses the construct of spasticity impact consistently across items [22].
Test re-test reliability is a crucial component of any assessment instrument since it ensures that it can consistently measure the same construct at multiple periods in time. The SCI-SETp had an ICC agreement of 0.84 and an ICC of 0.8. Our findings revealed that the SCI-SETu had ICCs ranging from 0.459 to 0.976, indicating high test re-test reliability. Besides, the absence of floor and ceiling effects in the present investigation suggests that the SCI-SETu is sensitive to mild to severe levels of spasticity among patients with SCI, providing a tool that enables the across-population assessment of patients [21].
Our sample characteristics provided further insights into the generalizability of our findings. The participants’ mean age was 40.23 years, and their gender distribution was balanced. Although there are many different causes of SCIs, the most frequent ones are related to traffic accidents, violence, falls, and sports-related mishaps. Although the participants’ educational backgrounds varied, most had completed secondary school. This demographic information highlights how the SCI-SETu can be used for various patients with SCI. With mean scores barely changing over a week, the descriptive statistics for the SCI-SETu scores demonstrated stability and reliability. Further supporting the construct validity of FIM is the substantial positive correlation (r=0.788, P<0.01) found between it and the SCI-SETu. When individual items were eliminated from the scale, Cronbach’s α coefficients indicated strong reliability, and the internal consistency analysis revealed corrected item-collective correlations ranging from 0.093 to 0.632 [21].
The psychometric properties of the SCI-SETu are strong and similar to those of its Turkish and Persian counterparts. This study adds to the increasing amount of data demonstrating the SCI-SET’s cross-cultural effectiveness and reliability in various linguistic and cultural contexts. The SCI-SETu has been successfully validated, providing researchers and physicians a useful tool to evaluate how spasticity affects the day-to-day activities of SCI patients who speak Urdu. This improves patient care, enables more focused therapies, and yields better results for a previously underserved population using reliable, culturally sensitive assessment methods.
This study has several limitations. First, using a convenience sampling method may limit the generalizability of the findings, as the participants may not be fully representative of the broader Urdu-speaking SCI population. Second, the validation relied on correlation with the FIM, a functional measure. However, it lacked an external criterion measure specifically for spasticity severity (e.g. clinician-rated Ashworth scale or Penn Spasm frequency scale). This would strengthen the validity of the argument. Third, the study was conducted in a single urban center (Lahore City); therefore, the generalizability of the SCI-SETu to other Urdu-speaking regions in Pakistan or other countries should be established through further multi-center research. Finally, the study did not stratify participants based on their injury or spasticity severity, which could have influenced the tool’s performance.
Conclusion
The Urdu version of the SCI-SETu has been shown to be a reliable tool for assessing spasticity in SCI patients. It is highly validity, test re-test reliability, and internally consistent, making it suitable for use in clinical and research settings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research and Ethical Review Committee of Riphah College of Rehab & Allied Health Sciences, Lahore, Pakistan (Code: REC.RCR&AHS.23.0270).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to everyone who helped with the research, including volunteers, team members, and everyone else who contributed.
References
Spinal cord injury (SCI) is a severe neurological condition that leads to physical dependence, morbidity, psychological stress, and significant financial burden [1]. Over the past 30 years, global prevalence has increased from 236 to 1298 cases per million, with an estimated 250000 to 500000 new cases annually [2, 3].
SCI progresses through two main stages: Primary and secondary injury. The primary injury occurs immediately following abrupt, serious spinal trauma and is frequently accompanied by fractures and displacements of the vertebrae. The main damage includes axonal network disruption, spinal joint rupture and neural stromal loss [4, 5]. The length of spinal cord entrapment and the degree of initial damage determine the severity of SCI [6]. Despite clinical manifestations suggesting complete functional loss, some axons may remain connected, indicating an incomplete injury [7]. Secondary injury begins with the primary injury and results in additional biochemical and biomechanical secondary injury to spinal tissues. This can cause neuronal excitotoxicity, leading to nucleic acid, protein, and phospholipid damage and consequent neurotoxicity [8].
A serious and complex medical illness, SCI affects 40 million people globally each year, with 2.1 to 130.7 million cases occurring in underdeveloped nations [9]. SCI places one of the biggest burdens on society, frequently resulting in severe impairment, reduced quality of life (QoL), and considerable emotional, financial, and social impacts on patients and their families [10]. In addition to major long-term medical consequences like exhaustion, discomfort, stiffness, and pressure sores, SCI can result in paralysis and sensory loss [11]. Males are two to five times more likely to experience it [12].
SCI often results in hip joint subluxation, lower leg paralysis, and autonomic dysreflexia (AD), which affects 48-60% of cases above the thoracic 6th vertebral level (T6), causing sudden high blood pressure. Understanding the SCI’s pathophysiology and recovery mechanisms is crucial for developing effective treatments [13]. Normal spinal cord function involves interactions among various cell types, which are disrupted post-injury, leading to impaired recovery [2].
After SCI, QoL is a crucial factor to consider. According to one source, spasticity contributes to a lower QoL. It can also cause pain, insomnia, pressure ulcers, and contractures [9, 14]. Numerous psychological aspects have been demonstrated to be associated with the degree of spasticity [15]. In addition, it may result in contractures, pressure ulcers, discomfort, and insomnia. Several physical therapy methods are recommended for the treatment of spasticity. These include heat, transcutaneous electric nerve stimulation, passive stretching, electromyography biofeedback, and other forms of exercise [16]. However, the effectiveness of any or all of these therapies is unknown [9]. From a therapeutic perspective, the knowledge that individuals with SCIs may have longer life expectancies following their lesions but may also experience a greater number of secondary health complications highlights the need to provide targeted care for particular secondary health complications and comorbidities [17].
In Pakistan, SCIs have not received significant attention in research. The nation’s 2005 northern earthquake was the only occasion on which the subject was brought up. Between 2011 and 2016, 1025 patients were admitted to the hospital. Compared to the corresponding female group, there were three times as many male patients. Ninety percent of patients have paraplegia [18, 19].
In the world, more than 300 million people speak Urdu, which is also Pakistan’s national language. However, the spasticity evaluation tool (SET) is challenging for Urdu-speaking patients with SCI to understand. It aimed to improve healthcare accessibility for Urdu-speaking individuals with SCI, ensuring they can accurately communicate their symptoms and experiences to healthcare professionals [20]. Ultimately, this study promises to improve the overall management and outcomes of spasticity in the Urdu-speaking SCI population. This study aimed to enhance the standard of care provided to patients with SCI, aiding in the accurate diagnosis, treatment, and monitoring of spasticity.
Materials and Methods
This cross-sectional study was conducted over ten months at the General Hospital in Lahore City, Pakistan, and the Riphah Rehabilitation Center. A pilot sample of 25 participants was used for testing the pre-final version of the questionnaire and was analyzed separately; these individuals were not included in the main reliability and validity analyses. The sample size was 175 people, selected using non-probability convenience sampling. Participants were aged 18 to 45, could read and write Urdu, suffered from SCI for at least six months, and scored at least 24 on the Mini-Mental State Examination (MMSE). Participants with cognitive, visual, auditory, or other neurological conditions (multiple sclerosis or Parkinson’s disease) were excluded. Data were collected using the spasticity evaluation assessment (SCI -SET), a 35-question self-administered assessment that evaluates the impact of spasticity on daily life [21], and the functional independence measure (FIM), an 18-item questionnaire that assesses impairment levels and care burden. The SCI-SET ratings ranged from -3 to +3, based on patient recollections from the previous week. In contrast, the FIM scores ranged from 1 (requiring total assistance) to 7 (full independence), with scores provided by a multidisciplinary team or a single expert.
Study participants were recruited through the rehabilitation clinics in Lahore City and the General Hospital, Lahore City. SCI-SETu was administered to patients with SCI who met the inclusion criteria. A sample of 175 patients was given the SCI-SETu at baseline and after 7 days assess test re-test reliability. Translation of the spasticity assessment tool for individuals with spinal column lesions into the Urdu version using the following steps as per Cosmin guidelines:
Stage 1: Initial translation
In the first phase, the instrument underwent two forward translations from English to Urdu. Bilingual translators with distinct backgroundscompleted the translations to ensure accuracy. Translator #1, a medical professional familiar with the questionnaire’s themes, and Translator #2, who had no medical training, performed these translations. A schematic of the cross-cultural adaptation process is presented in Figure 1.
Stage II: Synthesis of these translations
In the second stage, a third impartial person synthesizes the two translations. The original questionnaire combines versions from Translators #1 and #2 to create a common translation (T12).
Stage III: Back translation
The third stage involves back-translating the questionnaire into the original language using the T-12 version. This validation method ensures that the translated version maintains the original information. Two additional back translations (BT1 and BT2) by native English speakers are conducted without revealing the scale’s concepts to prevent bias.
Stage IV: Expert committee
The expert committee works collaboratively, comprising methodologists, health professionals, linguists, and both forward and back translators. In constant contact with the questionnaire’s creators, the committee compiles all versions to create the pre-final questionnaire for field testing. Any discrepancies are addressed through consensus.
Stage V: Test of pre-final version
This stage assesses the viability of the pre-final Urdu version of the SCI-SETu. Twenty-five individuals independently complete the questionnaire and provide feedback on each topic and their responses, ensuring the modified version maintains equivalence in practical settings.
Stage VI: Submission of documentation to developers for appraisal
In the final phase of the adaptation process, the committee submits reports and forms. The committee ensures adherence to proposed stages and verifies that the reports accurately represent the adaptation process.
Pilot testing and adaptation
Subjects who met the inclusion criteria were included in the study. Written informed consent was obtained from all participants. After obtaining demographic data, all participants were asked to fill out the SCI-SETu questionnaire on the instructions, and it was scored on completion.
The analysis was conducted using SPSS for Windows software, version 21. Construct validity was determined by assessing the correlation between the SCI-SETu and FIM scores using Pearson’s correlation coefficients. The strength of correlation was interpreted as follows: Very high (0.90–1.00), strong (0.70–0.89), moderate (0.50–0.69), or weak (<0.50). For test re-test reliability, alongside the intra-class correlation coefficient (ICC), the SEM was calculated using the Equation 1:
1. SEM=SD √(1-ICC)
where SD is the standard deviation of the day 1 scores.
Internal consistency: Given the single assessment for patients, internal consistency was evaluated to gauge reliability. This was measured using Cronbach’s α coefficient, with a satisfactory threshold set at 0.7 or higher.
Test, re-test reliability: Reliability across repeated assessments were established using test re-test reliability. The ICC with 95% confidence intervals (CIs) was utilized for estimation. Internal consistency was also confirmed using Cronbach’s α.
Results
Sample description
The mean age of the participants was 40.23±5.522 years (min 28 and max 45 years). The gender distribution was 76(43.4%) males and 99(56.6%) females. The etiology of SCI varies. Traffic accidents were the most common cause, 72(41.1%), and violence was the second most prevalent etiology, 53(30.3%). Falls contributed to 35(20%), while sports-related incidents comprised 10(5.7%). The educational level of the study participants was primary school education (1-8 grades) among 53 individuals (30.3%). Secondary school education (9-12 grades) was the most common, with 74 individuals (42.3%). Additionally, 48 individuals (27.4%) had undergone technical and vocational training (Table 1).
Day 1 reading
The descriptive statistics for SCI-SETu, on day 1, ranged from -1.86 to -0.17, with a mean of -1.22±0.39. The FIM scores on day 1 ranged from 29 to 68, with a mean of 45.26±8.42 (Table 2).
Day 2 reading
By day 7, the SCI-SETu scores ranged from -1.86 to 0.94, with a mean of -1.16±0.52. On day 7, the FIM scores ranged from 29 to 68, with an increased mean of 46.02±8.88 (Table 2).
Floor and ceiling effects
A floor or ceiling effect was considered present if more than 15% of participants achieved the lowest or highest possible score. Only one participant (0.6%) had the lowest score (-1.86), and one (0.6%) had the highest score (-0.17). No clustering of scores at the extremes was observed, confirming the absence of floor or ceiling effects.
Construct validity
A strong positive correlation was found between the SCI-SETu and the FIM (r=0.788, P<0.01).
Internal consistency
The overall Cronbach’s α for the SCI-SETu was 0.803 (95% CI, 0.759%, 0.842%). The corrected item-total correlations ranged from 0.011 to 0.632. Cronbach’s α if an item was deleted ranged from 0.779 to 0.823. All P were <0.001 (Table 3).
Test re-test reliability
The overall test re-test reliability for the SCI-SETu total score was excellent, with an ICC of 0.801 (95% CI, 0.739%, 0.85%). The SEM was 0.17. Item-level ICCs ranged from 0.459 to 0.976 (Table 4).
Discussion
The translation and validation of assessment instruments are critical for ensuring accurate and meaningful measurements across diverse cultural and linguistic settings. This study aimed to translate the SCI-SET into Urdu (SCI-SETu) and assess its psychometric properties among patients with SCI. The current study shows that the SCI-SETu has strong concept validity, internal consistency, and test re-test reliability, which is consistent with previous studies conducted in Persian and Turkish contexts.
The translation of the SCI-SET into Persian (SCI-SETp) and validation process revealed strong psychometric qualities, with a Cronbach’s α of 0.862 and an ICC agreement for test re-test reliability of 0.84. These indicators demonstrate high internal stability and consistency over time. Our research found comparable results for the Urdu translation, with Cronbach’s α values ranging from 0.779-0.823 and ICCs ranging from 0.459-0.976. These findings indicate that the SCI-SETu is a valid instrument for assessing spasticity in patients with SCI, while retaining the original SCI-SET’s reliability and validity [20].
With an intraclass correlation coefficient (ICC) of 0.8, similar to the aforementioned studies, the cross-cultural validity and reliability of the Turkish version of the SCI-SET, known as the SCI-SETT, was confirmed as well. The vitality scores in the 12 items of the short form health survey (SF-36) and their significant relations to the total and domain scores of the SCI-SETT confirmed the SCI-SETT’s responsiveness in quantifying the impact of spasticity on QoL. Similarly, our investigation revealed a strong positive correlation (r=0.788, P<0.01) between the SCI-SETu and the functional independence measure (FIM), thereby improving its construct validity and applicability in evaluating the complex effects of spasticity on day-to-day functioning in Urdu-speaking patients with SCI [22].
With Cronbach’s α values of 0.862 and 0.8, respectively, the Persian and Turkish versions of the SCI-SET showed strong dependability regarding internal consistency. Similar internal consistency was shown by the SCI-SETu, whose Cronbach’s α values ranged from 0.636 to 0.988. Based on these findings, the Urdu version of the tool retains the other adjustments made to it and the original tool’s dependability, meaning that it assesses the construct of spasticity impact consistently across items [22].
Test re-test reliability is a crucial component of any assessment instrument since it ensures that it can consistently measure the same construct at multiple periods in time. The SCI-SETp had an ICC agreement of 0.84 and an ICC of 0.8. Our findings revealed that the SCI-SETu had ICCs ranging from 0.459 to 0.976, indicating high test re-test reliability. Besides, the absence of floor and ceiling effects in the present investigation suggests that the SCI-SETu is sensitive to mild to severe levels of spasticity among patients with SCI, providing a tool that enables the across-population assessment of patients [21].
Our sample characteristics provided further insights into the generalizability of our findings. The participants’ mean age was 40.23 years, and their gender distribution was balanced. Although there are many different causes of SCIs, the most frequent ones are related to traffic accidents, violence, falls, and sports-related mishaps. Although the participants’ educational backgrounds varied, most had completed secondary school. This demographic information highlights how the SCI-SETu can be used for various patients with SCI. With mean scores barely changing over a week, the descriptive statistics for the SCI-SETu scores demonstrated stability and reliability. Further supporting the construct validity of FIM is the substantial positive correlation (r=0.788, P<0.01) found between it and the SCI-SETu. When individual items were eliminated from the scale, Cronbach’s α coefficients indicated strong reliability, and the internal consistency analysis revealed corrected item-collective correlations ranging from 0.093 to 0.632 [21].
The psychometric properties of the SCI-SETu are strong and similar to those of its Turkish and Persian counterparts. This study adds to the increasing amount of data demonstrating the SCI-SET’s cross-cultural effectiveness and reliability in various linguistic and cultural contexts. The SCI-SETu has been successfully validated, providing researchers and physicians a useful tool to evaluate how spasticity affects the day-to-day activities of SCI patients who speak Urdu. This improves patient care, enables more focused therapies, and yields better results for a previously underserved population using reliable, culturally sensitive assessment methods.
This study has several limitations. First, using a convenience sampling method may limit the generalizability of the findings, as the participants may not be fully representative of the broader Urdu-speaking SCI population. Second, the validation relied on correlation with the FIM, a functional measure. However, it lacked an external criterion measure specifically for spasticity severity (e.g. clinician-rated Ashworth scale or Penn Spasm frequency scale). This would strengthen the validity of the argument. Third, the study was conducted in a single urban center (Lahore City); therefore, the generalizability of the SCI-SETu to other Urdu-speaking regions in Pakistan or other countries should be established through further multi-center research. Finally, the study did not stratify participants based on their injury or spasticity severity, which could have influenced the tool’s performance.
Conclusion
The Urdu version of the SCI-SETu has been shown to be a reliable tool for assessing spasticity in SCI patients. It is highly validity, test re-test reliability, and internally consistent, making it suitable for use in clinical and research settings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research and Ethical Review Committee of Riphah College of Rehab & Allied Health Sciences, Lahore, Pakistan (Code: REC.RCR&AHS.23.0270).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to everyone who helped with the research, including volunteers, team members, and everyone else who contributed.
References
- Hu X, Xu W, Ren Y, Wang Z, He X, Huang R, et al. Spinal cord injury: Molecular mechanisms and therapeutic interventions. Signal Transduction and Targeted Therapy. 20236; 8(1):245. [DOI:10.1038/s41392-023-01477-6] [PMID]
- Sturm C, Gutenbrunner CM, Egen C, Geng V, Lemhöfer C, Kalke YB, et al. Which factors have an association to the quality of life (QoL) of people with acquired spinal cord injury (SCI)? A cross-sectional explorative observational study. Spinal Cord. 2021; 59(8):925-932. [DOI:10.1038/s41393-021-00663-z] [PMID]
- Wecht JM, Krassioukov AV, Alexander M, Handrakis JP, McKenna SL, Kennelly M, et al. International standards to document autonomic function following SCI (ISAFSCI): Second edition. Topics in Spinal Cord Injury Rehabilitation. 2021; 27(2):23-49. [DOI:10.46292/sci2702-23] [PMID]
- Bhagwani A, Chopra M, Kumar H. Spinal cord injury provoked neuropathic pain and spasticity, and their GABaergic connection. Neurospine. 2022; 19(3):646-68. [DOI:10.14245/ns.2244368.184] [PMID]
- Stampas A, Hook M, Korupolu R, Jethani L, Kaner MT, Pemberton E, et al. Evidence of treating spasticity before it develops: A systematic review of spasticity outcomes in acute spinal cord injury interventional trials. Therapeutic Advances in Neurological Disorders. 2022; 15:17562864211070657. [DOI:10.1177/17562864211070657] [PMID]
- Rupp R, Biering-Sørensen F, Burns SP, Graves DE, Guest J, Jones L, et al. International standards for neurological classification of spinal cord injury: Revised 2019. Topics in Spinal Cord Injury Rehabilitation. 2021; 27(2):1-22. [DOI:10.46292/sci2702-1] [PMID]
- Sangari S, Perez MA. Prevalence of spasticity in humans with spinal cord injury with different injury severity. Journal of Neurophysiology. 2022; 128(3):470-9. [DOI:10.1152/jn.00126.2022] [PMID]
- DiPiro ND, Murday D, Corley EH, Krause JS. The primary and secondary causes of hospitalizations during the first five years after spinal cord injury. Spinal Cord. 2022; 60(6):574-9. [DOI:10.1038/s41393-022-00750-9] [PMID]
- Barbosa PHFA, Glinsky JV, Fachin-Martins E, Harvey LA. Physiotherapy interventions for the treatment of spasticity in people with spinal cord injury: A systematic review. Spinal Cord. 2021; 59(3):236-47. [DOI:10.1038/s41393-020-00610-4] [PMID]
- Zhang Y, Al Mamun A, Yuan Y, Lu Q, Xiong J, Yang S, et al. Acute spinal cord injury: Pathophysiology and pharmacological intervention (Review). Molecular Medicine Reports. 2021; 23(6):417. [DOI:10.3892/mmr.2021.12056] [PMID]
- Nas K, Yazmalar L, Şah V, Aydın A, Öneş K. Rehabilitation of spinal cord injuries. World Journal of Orthopedics. 2015; 6(1):8-16. [DOI:10.5312/wjo.v6.i1.1] [PMID]
- Quadri SA, Farooqui M, Ikram A, Zafar A, Khan MA, Suriya SS, et al. Recent update on basic mechanisms of spinal cord injury. Neurosurgical Review. 2020; 43(2):425-41. [DOI:10.1007/s10143-018-1008-3] [PMID]
- Lorach H, Galvez A, Spagnolo V, Martel F, Karakas S, Intering N, et al. Walking naturally after spinal cord injury using a brain-spine interface. Nature. 2023; 618(7963):126-33. [DOI:10.1038/s41586-023-06094-5] [PMID]
- Bryce TN, Huang V, Escalon MX. Spinal cord injury. In: Cifu DX, editor. Braddom’s physical medicine and rehabilitation (sixth edition). Philadelphia: Elsevier; 2021. [DOI:10.1016/B978-0-323-62539-5.00049-7]
- Westerkam D, Saunders LL, Krause JS. Association of spasticity and life satisfaction after spinal cord injury. Spinal Cord. 2011; 49(9):990-4. [DOI:10.1038/sc.2011.49] [PMID]
- Ding W, Hu S, Wang P, Kang H, Peng R, Dong Y, et al. Spinal cord injury: The global incidence, prevalence, and disability from the global burden of disease study 2019. Spine. 2022; 47(21):1532-40. [DOI:10.1097/BRS.0000000000004417] [PMID]
- Pili R, Gaviano L, Pili L, Petretto DR. Ageing, disability, and spinal cord injury: Some issues of analysis. Current Gerontology and Geriatrics Research. 2018; 2018:4017858. [DOI:10.1155/2018/4017858] [PMID]
- Darain H, Ilyas SM, Zeb A, Ullah I, Muhammad DJPM, Rehabilitationsmedizin, Kurortmedizin. Epidemiology of spinal cord injury in Pakistan: A retrospective study. Wissenschaft und Forschung. 2017; 27(02):106-9. [DOI:10.1055/s-0042-124356]
- Benavente A, Palazón R, Tamayo R, Morán E, Alaejos J, Alcaraz A. Assessment of disability in spinal cord injury. Disability and Rehabilitation. 2003; 25(18):1065-70. [DOI:10.1080/0963828031000137775] [PMID]
- Ansari NN, Kashi M, Naghdi S. The spinal cord injury spasticity evaluation tool: A Persian adaptation and validation study. The Journal of Spinal Cord Medicine. 2017; 40(4):380-8. [DOI:10.1080/10790268.2016.1195941] [PMID]
- Adams MM, Ginis KA, Hicks AL. The spinal cord injury spasticity evaluation tool: Development and evaluation. Archives of Physical Medicine and Rehabilitation. 2007; 88(9):1185-92. [DOI:10.1016/j.apmr.2007.06.012] [PMID]
- Akpinar P, Atici A, Kurt KN, Ozkan FU, Aktas I, Kulcu DG. Reliability and cross-cultural adaptation of the turkish version of the spinal cord injury spasticity evaluation tool. International Journal of Rehabilitation Research. 2017; 40(2):152-7. [DOI:10.1097/MRR.0000000000000223] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2025/07/7 | Accepted: 2025/09/3 | Published: 2025/12/1
Received: 2025/07/7 | Accepted: 2025/09/3 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
