
988368
Sat, Jul 11, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 441-450 |
Back to browse issues page


Ethics code: IR.AJAUMS.REC.1402.176
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Teymouri S M, Dadarkhah A, Rezasoltani Z, Tabatabaee S M, Kazemi-Galougahi M H. Sagittal Alignment, Central Sensitization, and Psychosocial Factors in Military Personnel with Chronic Low Back Pain. Iranian Rehabilitation Journal 2025; 23 (4) :441-450
URL: http://irj.uswr.ac.ir/article-1-2573-en.html
URL: http://irj.uswr.ac.ir/article-1-2573-en.html
Seyed Mostafa Teymouri1 

 , Afsaneh Dadarkhah *1 , Zahra Rezasoltani1 , Seyed Morteza Tabatabaee1 , Mohammad Hassan Kazemi-Galougahi2
, Afsaneh Dadarkhah *1 , Zahra Rezasoltani1 , Seyed Morteza Tabatabaee1 , Mohammad Hassan Kazemi-Galougahi2
, Afsaneh Dadarkhah *1 , Zahra Rezasoltani1 , Seyed Morteza Tabatabaee1 , Mohammad Hassan Kazemi-Galougahi2
1- Clinical Biomechanics and Ergonomics Research Center, Aja University of Medical Sciences, Tehran, Iran.
2- Department of Social Medicine, Faculty of Medicine, AJA University of Medical Sciences, Tehran, Iran.
2- Department of Social Medicine, Faculty of Medicine, AJA University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 515 kb]
(439 Downloads)
| Abstract (HTML) (1615 Views)
Full-Text: (283 Views)
Introduction
Low back pain (LBP) is the most common musculoskeletal disorder and constitutes the largest portion of the global disability burden [1, 2]. In 2020, over 500 million individuals worldwide were affected by LBP, a number expected to rise to 800 million by 2050 [2]. The high prevalence of LBP has notable clinical, social, and economic consequences for individuals, healthcare systems, and society. A significant proportion of LBP cases are categorized as chronic non-specific LBP (CNLBP), where pain persists without a clear cause associated with a specific injury or medical condition [3]. CNLBP is a complex condition influenced by biophysical, psychosocial, genetic, and comorbid factors that can interact with one another to develop this condition [4].
Studies have demonstrated the importance of sagittal spinopelvic alignment in maintaining postural balance in healthy individuals [5, 6]. Altered spinal curvature and sagittal imbalance are commonly observed in individuals with CNLBP who also experience reduced range of motion (ROM) compared to asymptomatic individuals [7, 8]. However, the findings on sagittal spino-pelvic alignment in patients with LBP are inconsistent. While some studies reported substantial differences in alignment measures such as lumbar lordosis, sacral slope, and pelvic tilt between patients with LBP and asymptomatic individuals, others have found no significant differences [9-12]. There is also growing evidence that neuro-psychosocial factors play a significant role in the development and persistence of LBP [13-16]. Additionally, there is evidence of a relationship between postural balance and psychiatric disorders in individuals with CNLBP. Previous studies have shown that depressive disorders are strongly associated with increased thoracic kyphosis angle and elevated T1 slope, suggesting a potential psychosocial influence on sagittal alignment [17]. Psychological factors can also influence pain sensitivity and central nociceptive sensitization processes in patients with chronic LBP, as demonstrated by Steinmetz et al. for the first time [18].
LBP is a prevalent health issue in military personnel worldwide [19]. Military occupations often require exposure to physically demanding tasks and unpredictable environmental conditions. These factors, along with training loads and high-performance requirements, increase the risk of musculoskeletal conditions and LBP [20, 21]. Despite the high rate of CNLBP among military personnel, there is a notable gap in research on spinal alignment and ROM of the spine in this population. Moreover, the interplay between biomechanical factors and psychosocial properties, such as central sensitization, depression, and pressure pain threshold (PTT) remains poorly understood in patients with CNLBP. Therefore, this study aimed to evaluate sagittal spinal alignment and ROM in military personnel with CNLBP and to explore the correlations between these biomechanical parameters and factors such as central sensitization, disability and psychosocial factors.
Materials and Methods
Study design and ethics
This cross-sectional study was conducted on male military personnel affiliated with the Islamic Republic of Iran Army (AJA). Enrollment occurred between October 2023 and June 2024 at the Biomechanics Laboratory of the School of Medicine, AJA University of Medical Sciences, Tehran City, Iran. The two groups were recruited: One consisting of patients with CNLBP and the other of asymptomatic patients. Two groups were matched using a frequency matching method. Ethical approval was obtained from the Ethics Committee at AJA University of Medical Sciences. The participants received verbal and written descriptions of the study, and written informed consent was obtained.
Participants
Male military personnel aged 18-60 years, referred to the biomechanics laboratory at AJA University of Medical Sciences, were eligible for inclusion. All study participants were of the same ethnicity (Iranian/Middle Eastern). The study population consisted of two groups: one with CNLBP and one asymptomatic, which were matched using a frequency matching method based on age, BMI, and smoking habits. The CNLBP group was recruited first, followed by the control group. A total of 230 military personnel with CNLBP and 239 asymptomatic personnel were invited to participate. Of those invited, 49 individuals with CNLBP enrolled (response rate=21.3%). In the healthy control group, 63 individuals agreed to participate (initial response rate=26.4%); however, eight were excluded during frequency matching for age and military service duration, resulting in a final sample of 55 controls (final response rate=23.1%). Only male participants were included due to the predominantly male composition of the Iranian military. The inclusion criteria for the CNLBP group were as follows: Individuals who had experienced CNLBP for more than three months without any underlying pathology, aged between 18 and 60 years, and can perform forward flexion and extension movements unaided. Asymptomatic participants were screened to confirm no history of LBP or related symptoms. The exclusion criteria included any obvious deformity of the spine, pelvis, or lower extremities; rheumatologic or neurologic diseases; spinal fractures; a history of back surgery and history of medical and/or physiotherapeutic treatment within the last 12 weeks. The sample size was calculated based on Bujang et al. with an alpha of 0.05, power of 80%, R0=0.0, R1=0.4 resulting in a minimum of 46 participants per group [22]. We employed a convenience sampling method by recruiting participants by sending motivation letters to AJA personnel using the SMS system.
Variables
Spinal alignment and ROM: A spinal mouse® (Idiag, Volkerswill, Switzerland), which is a wireless electronic measurement device used to assess spinal mobility and posture in the sagittal plane. Before examination, the participants were registered in Spinal Mouse® software with their gender, age, and study codes. The participants were asked to undress their upper bodies. Then, the spinous processes were palpated, and specific vertebral landmarks (C7 and S3) were marked. All measurements were obtained in the following sequence: Upright position, maximum flexion in standing, and maximum extension in standing, to enhance reproducibility. The device’s mobile unit was slid along the spinous processes from C7 to S3 to capture skin contours and calculate sagittal spinal alignment by measuring the lumbar lordosis, sacral/hip, and inclination angles. The ROM was measured by repeating this process with participants in maximum flexion and extension.
Central sensitization inventory (CSI): Patients in the CNLBP and asymptomatic groups were assessed using the Persian translation of the CSI (CSI-Per). The CSI-Per showed strong validity and reliability (test re-test interclass correlation coefficient [ICC]=0.934, P<0.001; internal consistency Cronbach’s α=0.87) for assessing chronic pain symptoms in Persian-speaking patients [23].
PTT: Patients in the CNLBP and asymptomatic group were assessed using a Korean-made Algometer Device (SF model). This device, equipped with a one-centimeter disk, digitally displays the amount of pressure in Newtons and kilograms. A higher number on the screen indicates a greater pain tolerance in the patient, signifying less sensitivity. The algometer was applied at various points: 2 cm and 5 cm lateral to the first and third lumbar vertebrae, and 2 cm lateral to the fifth lumbar vertebra, on both sides [24]. The sensitivity threshold was measured three times, with a 30-second interval between each measurement. The mean of these measurements was calculated and recorded as the primary sensitivity data. This methodological approach ensured the accuracy and reliability of the data collected. Finally, the values measured on the right side and the values measured on the left side were added, and their average was expressed as the final number.
Pain: To assess pain intensity (only in the CNLBP group), the visual analog scale (VAS) was used to mark a 10 cm line segment and provide the necessary explanations to the patient. The number 10 in this diagram indicates maximum pain, and the number zero indicates the pain-free point [25]. The patient was asked to indicate his average most severe pain in the past week on the chart.
Disability: Disability was measured using the Persian version of the Oswestry disability index (ODI) questionnaire in the CNLBP group [26].
Psychosocial occupational disability status: The Örebro musculoskeletal pain screening questionnaire (ÖMPSQ) is a widely used tool [27]. This questionnaire is a self-reported tool for the early identification of patients at risk of chronic musculoskeletal pain, particularly work-related LBP. It predicts work disability and assesses psychosocial risk factors affecting recovery and return to work. The validity and reliability of the Persian version of this questionnaire have been proven in the study of Sharafi et al. [27] in 2017 (ICC=0.82, Cronbach’s α=0.82).
Outcome measures
Measurements were conducted by the first author (Seyed Mostafa Teymouri), an MSc student in physical therapy with over four years of clinical experience treating patients with LBP. To mitigate the impact of diurnal variations in joint mechanics, all participants were assessed simultaneously (10 AM-1 PM). All assessments were conducted concurrently.
Statistical analysis
Descriptive statistics, including Mean±SD, frequencies, percentages, and interquartile ranges, were calculated to summarize the participant characteristics. The Kolmogorov-Smirnov test was employed to assess the normality of the data. Parametric tests were applied if the variables were normally distributed; otherwise, non-parametric tests were used. The independent t-tests were utilized for comparisons between groups. The chi-square test was used to compare qualitative variables. Spearman’s correlation coefficient was employed to examine the relationships between variables. All analyses were conducted using SPSS software, version 27 (IBM., Armonk, New York, USA), and the significance level for all tests was set at 0.05.
Results
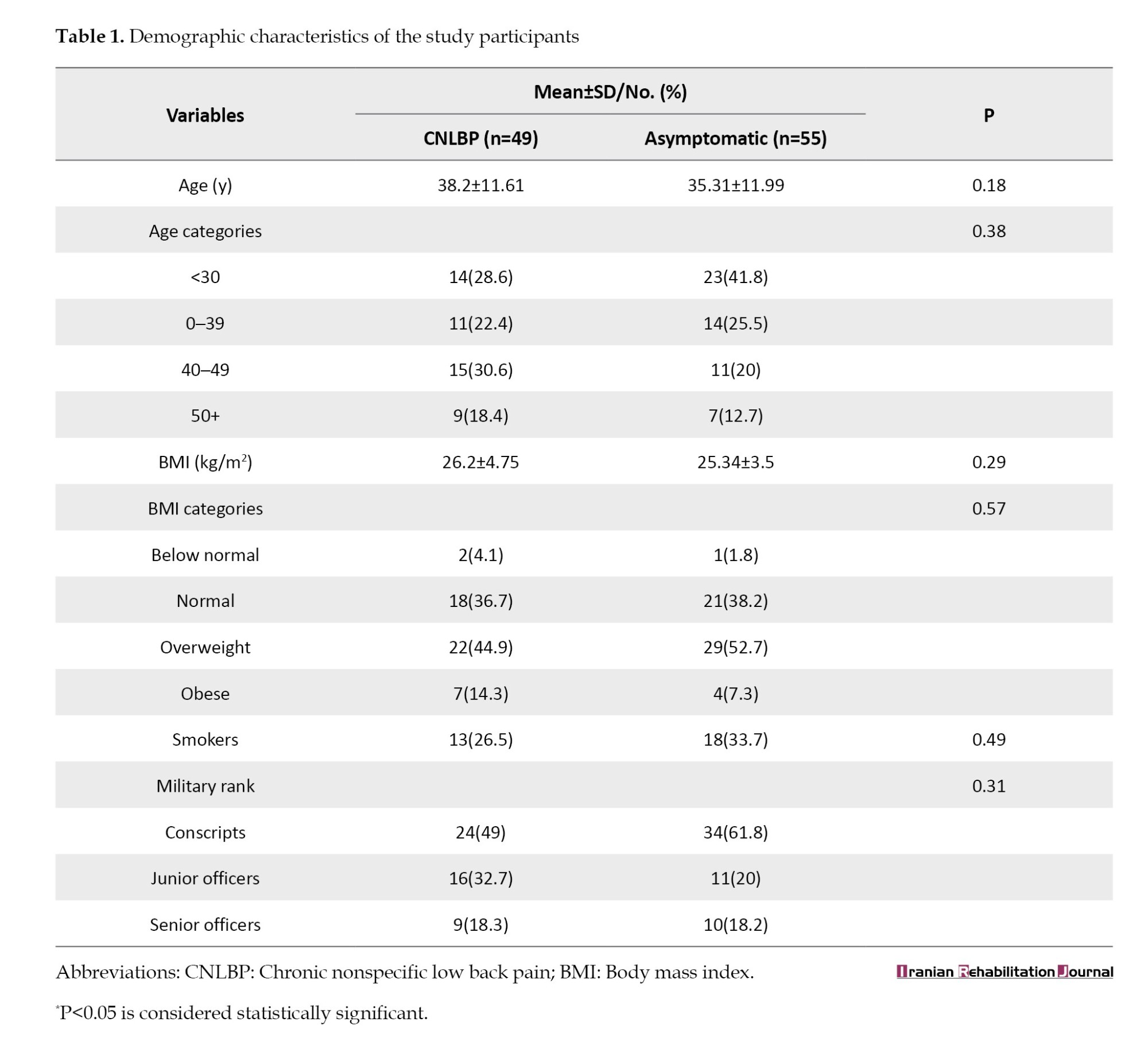
We recruited 104 participants, including 49 in the CNLBP group and 55 asymptomatic individuals. The mean age of the participants was 36.67±11.84 years, and the mean body mass index (BMI) was 25.72±4.13 kg/m². Table 1 presents the demographic information of the participants divided into two groups.
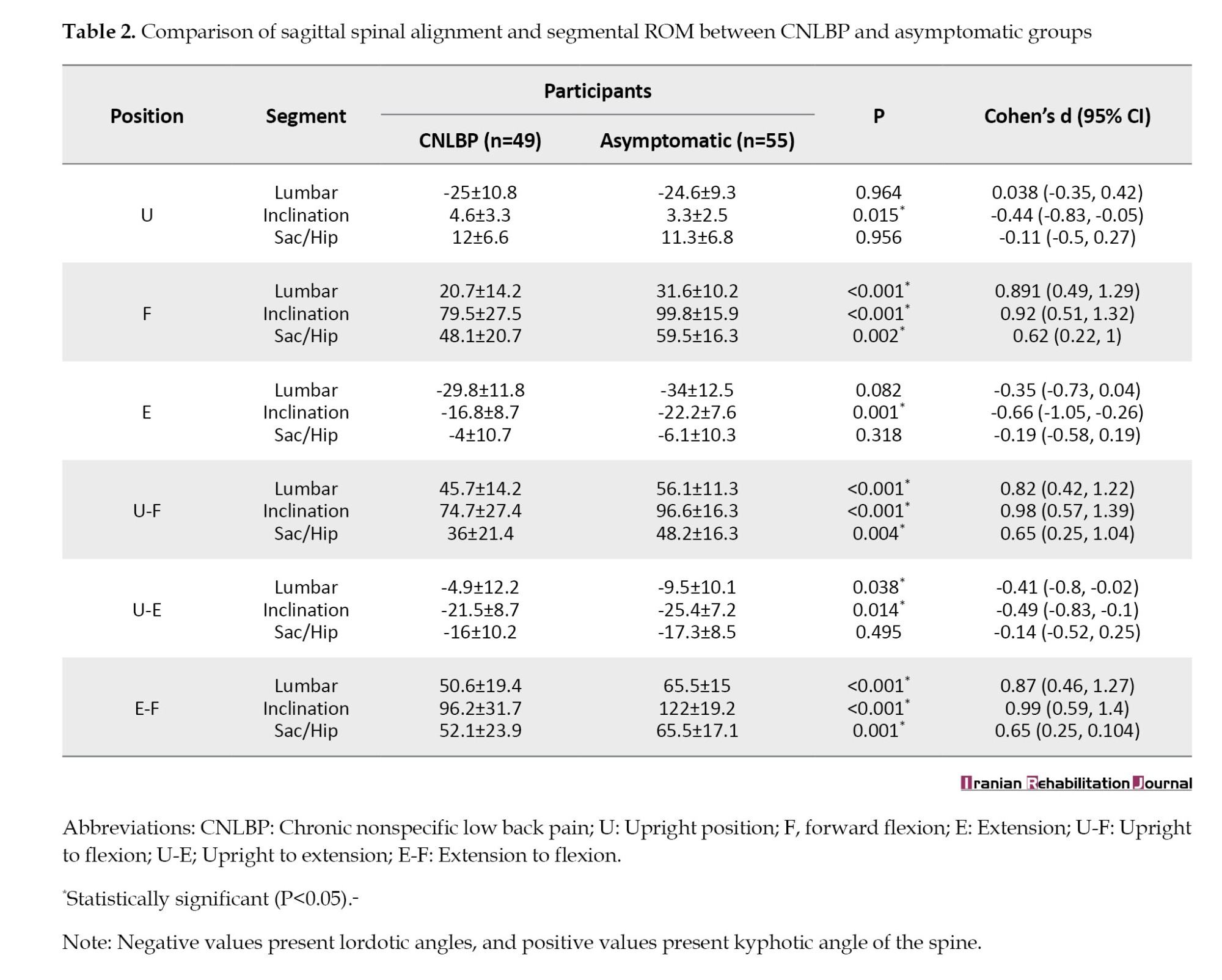
We measured lumbar, sacral/hip, and inclination segmental angles and segmental ROM using a Spinal Mouse; angles were recorded in three positions (upright, forward flexion, and extension), and ROM was analyzed across three motion directions (upright to flexion, upright to extension, and extension to flexion). Table 2 presents the Mean±SD values for CNLBP and asymptomatic participants, along with between-group effect sizes (Cohen’s d) and P. Significant differences were observed between the groups at all three positions. In the upright posture, participants with CNLBP had greater inclination angles compared to the asymptomatic group (P=0.015). During flexion, the inclination, sacral/hip, and lumbar angles were significantly lower in the CNLBP group (P<0.001, P=0.002, and P<0.001, respectively). Additionally, patients with CNLBP consistently exhibited higher sagittal inclination compared to the control group during extension (P=0.001). Analyzing the segments’ ROM revealed statistically significant differences in the lumbar angle and sagittal inclination in all motion directions. The difference in sacral/hip was statistically significant for both upright to flexion and extension to flexion (P=0.004 and P=0.001, respectively).
Next, CSI and PPT were measured in both CNLBP and asymptomatic participants, while VAS, ODI, and ÖMPSQ were assessed exclusively in the CNLBP group. Participants with CNLBP showed significantly higher CSI scores (28.51±11.92) compared to asymptomatic individuals (15.13±10.69), with a large effect size (Cohen’s d=-1.18, 95% confidence interval [CI] [-1.60, -0.77], P<0.001). PPT was lower in the CNLBP group (58.69±24.47) than in the asymptomatic group (82.07±29.52), indicating a significant difference (Cohen’s d=0.86, 95% CI, 0.45%, 1.26%, P<0.001). Among CNLBP participants, the Mean±SD values for VAS, ODI, and ÖMPSQ were 5.2±1.63, 23.67±11.74, and 94.47±24.01, respectively.
Table 3 presents the correlations between spinal segmental angles and neuro-psychosocial factors in the CNLBP group. In forward flexion, lumbar angle was negatively correlated with CSI (r=-0.27, 95% CI, -0.44%, -0.08%, P<0.05) and VAS (r=-0.44, 95% CI -0.65%, -0.17%, P<0.001). The inclination angle was also negatively correlated with CSI (r=-0.27, 95% CI, -0.44%, -0.08%, P<0.05), VAS (r=-0.34, 95% CI, -0.57%, -0.05%, P<0.05), ODI (r=-0.33, 95% CI, -0.56%, -0.04%, P<0.05), and ÖMPSQ (r=-0.41, 95% CI, -0.63%, -0.14%, P<0.001). The sacral/hip angle was negatively correlated with ÖMPSQ (r=-0.35, 95% CI, -0.58%, -0.07%, P<0.05). In extension, neither the lumbar angle nor the sacral/hip angle showed any significant correlations with VAS, ODI, or the psychosocial factors. However, the inclination angle was negatively correlated with ÖMPSQ (r=-0.39, 95% CI, -0.61%, -0.12%], P<0.001) and CSI (r=-0.21, 95% CI, -0.16%, -0.39%, P<0.05).
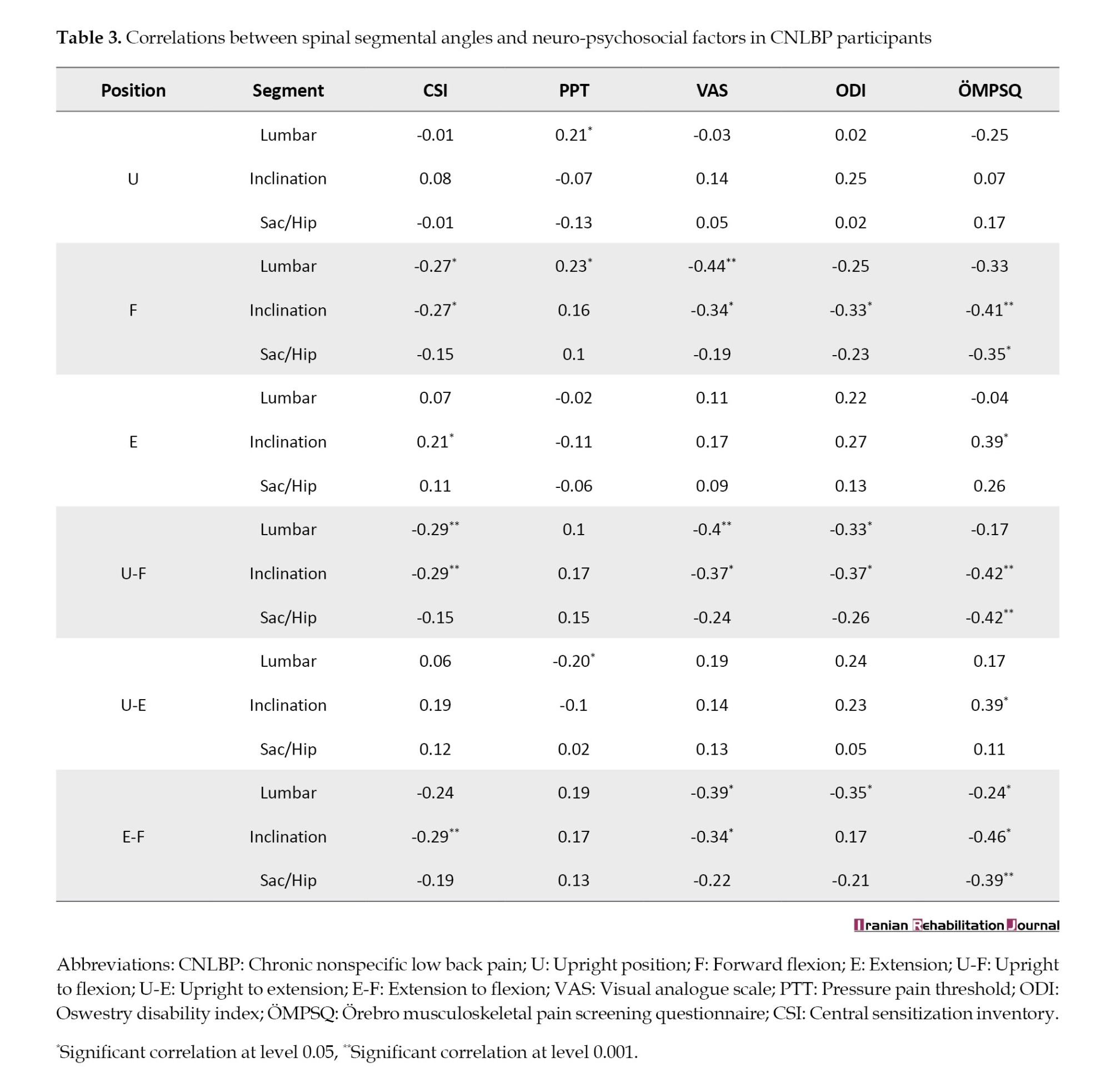
During upright to flexion motion, both lumbar inclination and inclination angle were negatively correlated with CSI (r=-0.29, 95% CI, -0.46%, -0.1%, P<0.001) and VAS (lumbar: r=-0.40, 95% CI, -0.62%, -0.13%, P<0.001; inclination: r=-0.37, 95% CI, -0.6%, -0.09%, P<0.05). Additionally, both the inclination angle and sacral/hip angle were negatively correlated with ÖMPSQ (r=-0.42, 95% CI, -0.63%, -0.15%, P<0.001). In the upright to extension transition, inclination angle was negatively correlated with ÖMPSQ (r=-0.39, 95% CI, -0.61%, -0.12%, P<0.05). Lastly, during extension to flexion motion, both lumbar angle and inclination angle were negatively correlated with the VAS score (lumbar: r=-0.39, 95% CI, -0.6%, -0.11%, P<0.05; inclination: r=-0.34, 95% CI, -0.57%, -0.05%, P<0.05). ÖMPSQ was negatively correlated with both sacral/hip angle (r=-0.39, 95% CI, -0.61%, -0.12%, P<0.001) and both lumbar and inclination angles. Table 3 presents a detailed presentation of all correlation coefficients and significance levels.
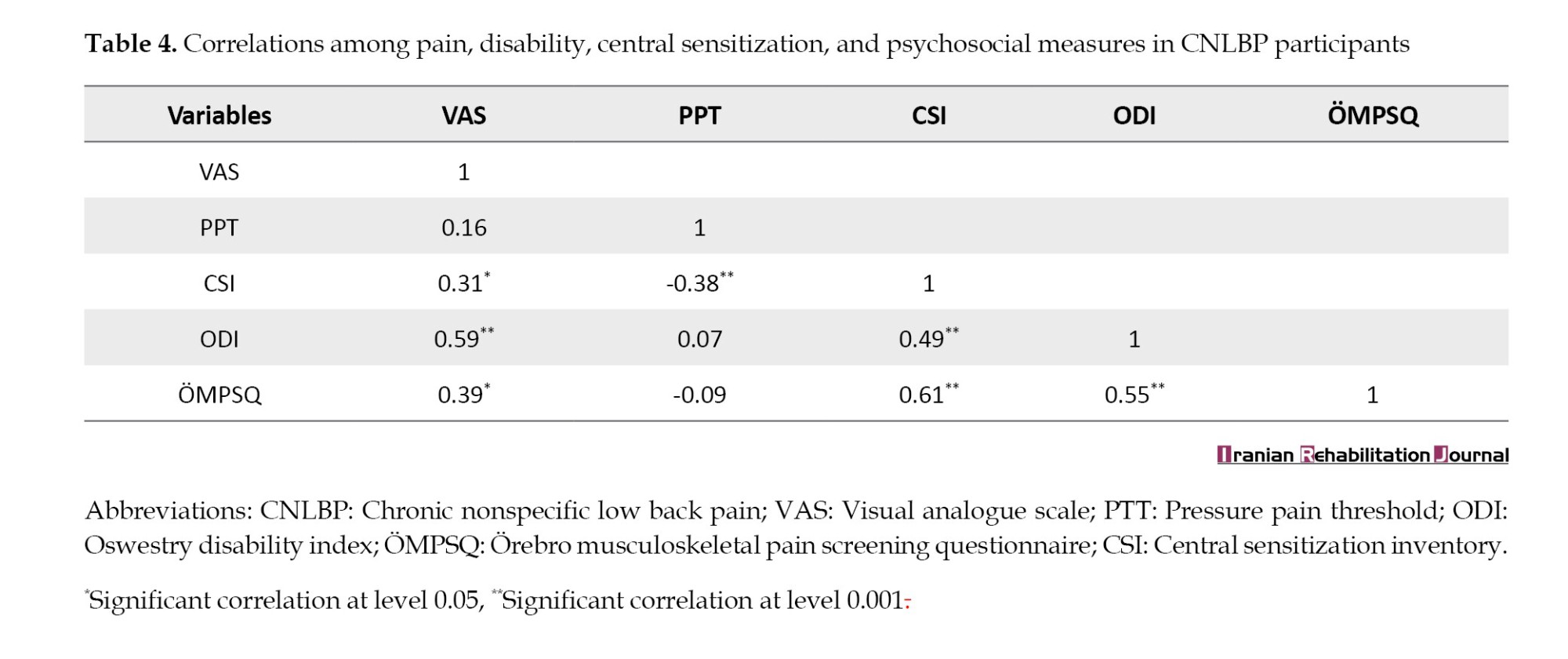
We further analyzed the correlations between CSI, PPT, VAS, and ÖMPSQ (Table 4). ÖMPSQ was significantly correlated with CSI (r=0.61, 95% CI, 0.4%, 0.77%, P<0.001), ODI (r=0.55, 95% CI, 0.31%, 0.72%, P<0.001), and VAS (r=0.39, 95% CI, 0.12%, 0.61%, P<0.05), indicating that higher levels of psychosocial distress were associated with increased central sensitization, disability, and pain intensity. Additionally, CSI was negatively correlated with PPT (r=-0.38, 95% CI, -0.54%, -0.2%, P<0.001), suggesting that greater central sensitization was associated with lower pain threshold. CSI was also positively correlated with VAS (r=0.31, 95% CI, 0.03%, 0.55%, P<0.05).
Discussion
This cross-sectional study investigated the relationships between sagittal spinal alignment, segmental ROM, and neuro-psychosocial factors in male military personnel with CNLBP. To our knowledge, this is the first study to comprehensively examine the relationships between spinal biomechanics and central sensitization, pain intensity, psychosocial factors, and disability in military populations.
Participants with CNLBP exhibited reduced lumbar flexion, altered sacral/hip and inclination angles across static and dynamic positions. Similar findings have been reported in patients with LBP, highlighting the relationship between restricted lumbar ROM, altered spinal posture, and LBP occurrence. For example, Feng et al. utilized a Spinal Mouse to evaluate spinal morphology in adolescents with and without CNLBP. They reported that a greater thoracic kyphosis angle and reduced lumbar ROM were correlated with the incidence of LBP [28]. Pourahmadi et al. found that participants with CNLBP presented decreased lumbar lordosis during sit-to-stand and stand-to-sit tasks compared to asymptomatic individuals [29]. The results from a systematic review that included 12 articles revealed that limited lumbar lordosis, unlike lumbar flexion and extension ROM, is associated with the development of LBP [30]. Although previous studies have also assessed spino-pelvic alignment in LBP and lumbar disk disease, the relationship between sagittal alignment and LBP remains unclear [9].
A key contribution of our study is the demonstration of robust associations between spinal biomechanical parameters and neuro-psychosocial variables. Our findings suggest a significant correlation between spinal morphology and ROM with psychosocial factors, disability, and pain intensity. Though statistically significant, these correlations were weak-to-moderate in magnitude, indicating that while mechanical dysfunction may play a role, other factors likely contribute to pain persistence, disability, and psychological burden [9]. Although psychological status is considered to be closely linked to LBP [31, 32], little is known about the relationship between a patient’s psychosocial profile and sagittal alignment. Therefore, comparing our results with existing literature is challenging. Collinet et al. demonstrated that depressive disorders in patients with CNLBP are associated with increased thoracic kyphosis [17]. Additionally, another study revealed a strong correlation between balance parameters and depression in patients with CNLBP. These findings highlight the importance of assessing psychosocial aspects as part of the interventions in patients with CNLBP [33].
The association between central sensitization and CNLBP has been explored in prior studies [34, 35]. In our sample, CSI scores were substantially higher in the CNLBP group than in controls and were related to the extent of LBP [14]. This is the first study to examine the correlation between central sensitization and sagittal spinal morphology and segmental ROM. We observed weak, negative correlations between CSI scores and spinal biomechanical measures. In addition, CSI correlated with psychosocial burden (ÖMPSQ), disability (ODI), pain intensity (VAS), and lower lumbar PPT. Consistent with this pattern, another study reported that central sensitization in CNLBP is associated with psychosocial factors and higher ÖMPSQ scores [18]. These observations align with prior work: Dahmani et al. found higher CSI scores to be associated with greater disability, higher pain intensity, and elevated anxiety in CNLBP [36]. However, Mibu et al. reported no correlation between CSI and PPT [37, 38].
Conclusion
The findings of this study highlight that military personnel with CNLBP exhibit altered sagittal spinal alignment and reduced ROM across various positions, along with heightened central sensitization and greater psychosocial burden. These findings may inform the development of tailored interventions that combine targeted physical therapy with cognitive-behavioral strategies, addressing biomechanical and psychosocial contributors to CNLBP.
Limitations
This study has several limitations. First, our study has a cross-sectional design. Further longitudinal studies are needed to confirm the relationship between spinal parameters and neuro-psychosocial variables. Second, the sample was comprised exclusively of male Iranian military personnel, reflecting the predominantly male composition of the military personnel; therefore, generalizability to women and general population is limited. Moreover, cultural and organizational features of the Iranian military and distinct occupational demands may not mirror civilian contexts. Third, selection bias is possible due to convenience sampling and SMS-based recruitment, which may have preferentially enrolled individuals with a greater interest in spinal health or better digital access. Fourth, although the Spinal Mouse is validated, it lacks the precision of radiographic methods, and spinal alignment was assessed only in standing postures; seated and dynamic assessments may yield additional insights. Finally, we did not control for physical activity levels, fatigue, or occupational exposure, which could influence biomechanics and pain and introduce residual confounding. These limitations should be considered when interpreting the findings, and future studies are warranted to confirm and extend these results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the AJA University of Medical Sciences, Tehran, Iran (Code: IR.AJAUMS.REC.1402.176). The participants received verbal and written descriptions of the study, and written informed consent was obtained. All procedures adhered to the principles of the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Seyed Mostafa Teymouri, Afsaneh Dadarkhah, and Zahra Rezasoltani; Methodology: Seyed Mostafa Teymouri, Afsaneh Dadarkhah, and Mohammad Hassan Kazemi-Galougahi; Investigation: Seyed Mostafa Teymour; Writing the original draft: Seyed Mostafa Teymouri; Review and editing: Afsaneh Dadarkhah, Zahra Rezasoltani, Seyed Morteza Tabatabaee, and Mohammad Hassan Kazemi-Galougahi; Supervision: Afsaneh Dadarkhah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are profoundly grateful to the military personnel who volunteered their time despite of their demanding schedules.
References
Low back pain (LBP) is the most common musculoskeletal disorder and constitutes the largest portion of the global disability burden [1, 2]. In 2020, over 500 million individuals worldwide were affected by LBP, a number expected to rise to 800 million by 2050 [2]. The high prevalence of LBP has notable clinical, social, and economic consequences for individuals, healthcare systems, and society. A significant proportion of LBP cases are categorized as chronic non-specific LBP (CNLBP), where pain persists without a clear cause associated with a specific injury or medical condition [3]. CNLBP is a complex condition influenced by biophysical, psychosocial, genetic, and comorbid factors that can interact with one another to develop this condition [4].
Studies have demonstrated the importance of sagittal spinopelvic alignment in maintaining postural balance in healthy individuals [5, 6]. Altered spinal curvature and sagittal imbalance are commonly observed in individuals with CNLBP who also experience reduced range of motion (ROM) compared to asymptomatic individuals [7, 8]. However, the findings on sagittal spino-pelvic alignment in patients with LBP are inconsistent. While some studies reported substantial differences in alignment measures such as lumbar lordosis, sacral slope, and pelvic tilt between patients with LBP and asymptomatic individuals, others have found no significant differences [9-12]. There is also growing evidence that neuro-psychosocial factors play a significant role in the development and persistence of LBP [13-16]. Additionally, there is evidence of a relationship between postural balance and psychiatric disorders in individuals with CNLBP. Previous studies have shown that depressive disorders are strongly associated with increased thoracic kyphosis angle and elevated T1 slope, suggesting a potential psychosocial influence on sagittal alignment [17]. Psychological factors can also influence pain sensitivity and central nociceptive sensitization processes in patients with chronic LBP, as demonstrated by Steinmetz et al. for the first time [18].
LBP is a prevalent health issue in military personnel worldwide [19]. Military occupations often require exposure to physically demanding tasks and unpredictable environmental conditions. These factors, along with training loads and high-performance requirements, increase the risk of musculoskeletal conditions and LBP [20, 21]. Despite the high rate of CNLBP among military personnel, there is a notable gap in research on spinal alignment and ROM of the spine in this population. Moreover, the interplay between biomechanical factors and psychosocial properties, such as central sensitization, depression, and pressure pain threshold (PTT) remains poorly understood in patients with CNLBP. Therefore, this study aimed to evaluate sagittal spinal alignment and ROM in military personnel with CNLBP and to explore the correlations between these biomechanical parameters and factors such as central sensitization, disability and psychosocial factors.
Materials and Methods
Study design and ethics
This cross-sectional study was conducted on male military personnel affiliated with the Islamic Republic of Iran Army (AJA). Enrollment occurred between October 2023 and June 2024 at the Biomechanics Laboratory of the School of Medicine, AJA University of Medical Sciences, Tehran City, Iran. The two groups were recruited: One consisting of patients with CNLBP and the other of asymptomatic patients. Two groups were matched using a frequency matching method. Ethical approval was obtained from the Ethics Committee at AJA University of Medical Sciences. The participants received verbal and written descriptions of the study, and written informed consent was obtained.
Participants
Male military personnel aged 18-60 years, referred to the biomechanics laboratory at AJA University of Medical Sciences, were eligible for inclusion. All study participants were of the same ethnicity (Iranian/Middle Eastern). The study population consisted of two groups: one with CNLBP and one asymptomatic, which were matched using a frequency matching method based on age, BMI, and smoking habits. The CNLBP group was recruited first, followed by the control group. A total of 230 military personnel with CNLBP and 239 asymptomatic personnel were invited to participate. Of those invited, 49 individuals with CNLBP enrolled (response rate=21.3%). In the healthy control group, 63 individuals agreed to participate (initial response rate=26.4%); however, eight were excluded during frequency matching for age and military service duration, resulting in a final sample of 55 controls (final response rate=23.1%). Only male participants were included due to the predominantly male composition of the Iranian military. The inclusion criteria for the CNLBP group were as follows: Individuals who had experienced CNLBP for more than three months without any underlying pathology, aged between 18 and 60 years, and can perform forward flexion and extension movements unaided. Asymptomatic participants were screened to confirm no history of LBP or related symptoms. The exclusion criteria included any obvious deformity of the spine, pelvis, or lower extremities; rheumatologic or neurologic diseases; spinal fractures; a history of back surgery and history of medical and/or physiotherapeutic treatment within the last 12 weeks. The sample size was calculated based on Bujang et al. with an alpha of 0.05, power of 80%, R0=0.0, R1=0.4 resulting in a minimum of 46 participants per group [22]. We employed a convenience sampling method by recruiting participants by sending motivation letters to AJA personnel using the SMS system.
Variables
Spinal alignment and ROM: A spinal mouse® (Idiag, Volkerswill, Switzerland), which is a wireless electronic measurement device used to assess spinal mobility and posture in the sagittal plane. Before examination, the participants were registered in Spinal Mouse® software with their gender, age, and study codes. The participants were asked to undress their upper bodies. Then, the spinous processes were palpated, and specific vertebral landmarks (C7 and S3) were marked. All measurements were obtained in the following sequence: Upright position, maximum flexion in standing, and maximum extension in standing, to enhance reproducibility. The device’s mobile unit was slid along the spinous processes from C7 to S3 to capture skin contours and calculate sagittal spinal alignment by measuring the lumbar lordosis, sacral/hip, and inclination angles. The ROM was measured by repeating this process with participants in maximum flexion and extension.
Central sensitization inventory (CSI): Patients in the CNLBP and asymptomatic groups were assessed using the Persian translation of the CSI (CSI-Per). The CSI-Per showed strong validity and reliability (test re-test interclass correlation coefficient [ICC]=0.934, P<0.001; internal consistency Cronbach’s α=0.87) for assessing chronic pain symptoms in Persian-speaking patients [23].
PTT: Patients in the CNLBP and asymptomatic group were assessed using a Korean-made Algometer Device (SF model). This device, equipped with a one-centimeter disk, digitally displays the amount of pressure in Newtons and kilograms. A higher number on the screen indicates a greater pain tolerance in the patient, signifying less sensitivity. The algometer was applied at various points: 2 cm and 5 cm lateral to the first and third lumbar vertebrae, and 2 cm lateral to the fifth lumbar vertebra, on both sides [24]. The sensitivity threshold was measured three times, with a 30-second interval between each measurement. The mean of these measurements was calculated and recorded as the primary sensitivity data. This methodological approach ensured the accuracy and reliability of the data collected. Finally, the values measured on the right side and the values measured on the left side were added, and their average was expressed as the final number.
Pain: To assess pain intensity (only in the CNLBP group), the visual analog scale (VAS) was used to mark a 10 cm line segment and provide the necessary explanations to the patient. The number 10 in this diagram indicates maximum pain, and the number zero indicates the pain-free point [25]. The patient was asked to indicate his average most severe pain in the past week on the chart.
Disability: Disability was measured using the Persian version of the Oswestry disability index (ODI) questionnaire in the CNLBP group [26].
Psychosocial occupational disability status: The Örebro musculoskeletal pain screening questionnaire (ÖMPSQ) is a widely used tool [27]. This questionnaire is a self-reported tool for the early identification of patients at risk of chronic musculoskeletal pain, particularly work-related LBP. It predicts work disability and assesses psychosocial risk factors affecting recovery and return to work. The validity and reliability of the Persian version of this questionnaire have been proven in the study of Sharafi et al. [27] in 2017 (ICC=0.82, Cronbach’s α=0.82).
Outcome measures
Measurements were conducted by the first author (Seyed Mostafa Teymouri), an MSc student in physical therapy with over four years of clinical experience treating patients with LBP. To mitigate the impact of diurnal variations in joint mechanics, all participants were assessed simultaneously (10 AM-1 PM). All assessments were conducted concurrently.
Statistical analysis
Descriptive statistics, including Mean±SD, frequencies, percentages, and interquartile ranges, were calculated to summarize the participant characteristics. The Kolmogorov-Smirnov test was employed to assess the normality of the data. Parametric tests were applied if the variables were normally distributed; otherwise, non-parametric tests were used. The independent t-tests were utilized for comparisons between groups. The chi-square test was used to compare qualitative variables. Spearman’s correlation coefficient was employed to examine the relationships between variables. All analyses were conducted using SPSS software, version 27 (IBM., Armonk, New York, USA), and the significance level for all tests was set at 0.05.
Results
We recruited 104 participants, including 49 in the CNLBP group and 55 asymptomatic individuals. The mean age of the participants was 36.67±11.84 years, and the mean body mass index (BMI) was 25.72±4.13 kg/m². Table 1 presents the demographic information of the participants divided into two groups.
We measured lumbar, sacral/hip, and inclination segmental angles and segmental ROM using a Spinal Mouse; angles were recorded in three positions (upright, forward flexion, and extension), and ROM was analyzed across three motion directions (upright to flexion, upright to extension, and extension to flexion). Table 2 presents the Mean±SD values for CNLBP and asymptomatic participants, along with between-group effect sizes (Cohen’s d) and P. Significant differences were observed between the groups at all three positions. In the upright posture, participants with CNLBP had greater inclination angles compared to the asymptomatic group (P=0.015). During flexion, the inclination, sacral/hip, and lumbar angles were significantly lower in the CNLBP group (P<0.001, P=0.002, and P<0.001, respectively). Additionally, patients with CNLBP consistently exhibited higher sagittal inclination compared to the control group during extension (P=0.001). Analyzing the segments’ ROM revealed statistically significant differences in the lumbar angle and sagittal inclination in all motion directions. The difference in sacral/hip was statistically significant for both upright to flexion and extension to flexion (P=0.004 and P=0.001, respectively).
Next, CSI and PPT were measured in both CNLBP and asymptomatic participants, while VAS, ODI, and ÖMPSQ were assessed exclusively in the CNLBP group. Participants with CNLBP showed significantly higher CSI scores (28.51±11.92) compared to asymptomatic individuals (15.13±10.69), with a large effect size (Cohen’s d=-1.18, 95% confidence interval [CI] [-1.60, -0.77], P<0.001). PPT was lower in the CNLBP group (58.69±24.47) than in the asymptomatic group (82.07±29.52), indicating a significant difference (Cohen’s d=0.86, 95% CI, 0.45%, 1.26%, P<0.001). Among CNLBP participants, the Mean±SD values for VAS, ODI, and ÖMPSQ were 5.2±1.63, 23.67±11.74, and 94.47±24.01, respectively.
Table 3 presents the correlations between spinal segmental angles and neuro-psychosocial factors in the CNLBP group. In forward flexion, lumbar angle was negatively correlated with CSI (r=-0.27, 95% CI, -0.44%, -0.08%, P<0.05) and VAS (r=-0.44, 95% CI -0.65%, -0.17%, P<0.001). The inclination angle was also negatively correlated with CSI (r=-0.27, 95% CI, -0.44%, -0.08%, P<0.05), VAS (r=-0.34, 95% CI, -0.57%, -0.05%, P<0.05), ODI (r=-0.33, 95% CI, -0.56%, -0.04%, P<0.05), and ÖMPSQ (r=-0.41, 95% CI, -0.63%, -0.14%, P<0.001). The sacral/hip angle was negatively correlated with ÖMPSQ (r=-0.35, 95% CI, -0.58%, -0.07%, P<0.05). In extension, neither the lumbar angle nor the sacral/hip angle showed any significant correlations with VAS, ODI, or the psychosocial factors. However, the inclination angle was negatively correlated with ÖMPSQ (r=-0.39, 95% CI, -0.61%, -0.12%], P<0.001) and CSI (r=-0.21, 95% CI, -0.16%, -0.39%, P<0.05).
During upright to flexion motion, both lumbar inclination and inclination angle were negatively correlated with CSI (r=-0.29, 95% CI, -0.46%, -0.1%, P<0.001) and VAS (lumbar: r=-0.40, 95% CI, -0.62%, -0.13%, P<0.001; inclination: r=-0.37, 95% CI, -0.6%, -0.09%, P<0.05). Additionally, both the inclination angle and sacral/hip angle were negatively correlated with ÖMPSQ (r=-0.42, 95% CI, -0.63%, -0.15%, P<0.001). In the upright to extension transition, inclination angle was negatively correlated with ÖMPSQ (r=-0.39, 95% CI, -0.61%, -0.12%, P<0.05). Lastly, during extension to flexion motion, both lumbar angle and inclination angle were negatively correlated with the VAS score (lumbar: r=-0.39, 95% CI, -0.6%, -0.11%, P<0.05; inclination: r=-0.34, 95% CI, -0.57%, -0.05%, P<0.05). ÖMPSQ was negatively correlated with both sacral/hip angle (r=-0.39, 95% CI, -0.61%, -0.12%, P<0.001) and both lumbar and inclination angles. Table 3 presents a detailed presentation of all correlation coefficients and significance levels.
We further analyzed the correlations between CSI, PPT, VAS, and ÖMPSQ (Table 4). ÖMPSQ was significantly correlated with CSI (r=0.61, 95% CI, 0.4%, 0.77%, P<0.001), ODI (r=0.55, 95% CI, 0.31%, 0.72%, P<0.001), and VAS (r=0.39, 95% CI, 0.12%, 0.61%, P<0.05), indicating that higher levels of psychosocial distress were associated with increased central sensitization, disability, and pain intensity. Additionally, CSI was negatively correlated with PPT (r=-0.38, 95% CI, -0.54%, -0.2%, P<0.001), suggesting that greater central sensitization was associated with lower pain threshold. CSI was also positively correlated with VAS (r=0.31, 95% CI, 0.03%, 0.55%, P<0.05).
Discussion
This cross-sectional study investigated the relationships between sagittal spinal alignment, segmental ROM, and neuro-psychosocial factors in male military personnel with CNLBP. To our knowledge, this is the first study to comprehensively examine the relationships between spinal biomechanics and central sensitization, pain intensity, psychosocial factors, and disability in military populations.
Participants with CNLBP exhibited reduced lumbar flexion, altered sacral/hip and inclination angles across static and dynamic positions. Similar findings have been reported in patients with LBP, highlighting the relationship between restricted lumbar ROM, altered spinal posture, and LBP occurrence. For example, Feng et al. utilized a Spinal Mouse to evaluate spinal morphology in adolescents with and without CNLBP. They reported that a greater thoracic kyphosis angle and reduced lumbar ROM were correlated with the incidence of LBP [28]. Pourahmadi et al. found that participants with CNLBP presented decreased lumbar lordosis during sit-to-stand and stand-to-sit tasks compared to asymptomatic individuals [29]. The results from a systematic review that included 12 articles revealed that limited lumbar lordosis, unlike lumbar flexion and extension ROM, is associated with the development of LBP [30]. Although previous studies have also assessed spino-pelvic alignment in LBP and lumbar disk disease, the relationship between sagittal alignment and LBP remains unclear [9].
A key contribution of our study is the demonstration of robust associations between spinal biomechanical parameters and neuro-psychosocial variables. Our findings suggest a significant correlation between spinal morphology and ROM with psychosocial factors, disability, and pain intensity. Though statistically significant, these correlations were weak-to-moderate in magnitude, indicating that while mechanical dysfunction may play a role, other factors likely contribute to pain persistence, disability, and psychological burden [9]. Although psychological status is considered to be closely linked to LBP [31, 32], little is known about the relationship between a patient’s psychosocial profile and sagittal alignment. Therefore, comparing our results with existing literature is challenging. Collinet et al. demonstrated that depressive disorders in patients with CNLBP are associated with increased thoracic kyphosis [17]. Additionally, another study revealed a strong correlation between balance parameters and depression in patients with CNLBP. These findings highlight the importance of assessing psychosocial aspects as part of the interventions in patients with CNLBP [33].
The association between central sensitization and CNLBP has been explored in prior studies [34, 35]. In our sample, CSI scores were substantially higher in the CNLBP group than in controls and were related to the extent of LBP [14]. This is the first study to examine the correlation between central sensitization and sagittal spinal morphology and segmental ROM. We observed weak, negative correlations between CSI scores and spinal biomechanical measures. In addition, CSI correlated with psychosocial burden (ÖMPSQ), disability (ODI), pain intensity (VAS), and lower lumbar PPT. Consistent with this pattern, another study reported that central sensitization in CNLBP is associated with psychosocial factors and higher ÖMPSQ scores [18]. These observations align with prior work: Dahmani et al. found higher CSI scores to be associated with greater disability, higher pain intensity, and elevated anxiety in CNLBP [36]. However, Mibu et al. reported no correlation between CSI and PPT [37, 38].
Conclusion
The findings of this study highlight that military personnel with CNLBP exhibit altered sagittal spinal alignment and reduced ROM across various positions, along with heightened central sensitization and greater psychosocial burden. These findings may inform the development of tailored interventions that combine targeted physical therapy with cognitive-behavioral strategies, addressing biomechanical and psychosocial contributors to CNLBP.
Limitations
This study has several limitations. First, our study has a cross-sectional design. Further longitudinal studies are needed to confirm the relationship between spinal parameters and neuro-psychosocial variables. Second, the sample was comprised exclusively of male Iranian military personnel, reflecting the predominantly male composition of the military personnel; therefore, generalizability to women and general population is limited. Moreover, cultural and organizational features of the Iranian military and distinct occupational demands may not mirror civilian contexts. Third, selection bias is possible due to convenience sampling and SMS-based recruitment, which may have preferentially enrolled individuals with a greater interest in spinal health or better digital access. Fourth, although the Spinal Mouse is validated, it lacks the precision of radiographic methods, and spinal alignment was assessed only in standing postures; seated and dynamic assessments may yield additional insights. Finally, we did not control for physical activity levels, fatigue, or occupational exposure, which could influence biomechanics and pain and introduce residual confounding. These limitations should be considered when interpreting the findings, and future studies are warranted to confirm and extend these results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the AJA University of Medical Sciences, Tehran, Iran (Code: IR.AJAUMS.REC.1402.176). The participants received verbal and written descriptions of the study, and written informed consent was obtained. All procedures adhered to the principles of the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Seyed Mostafa Teymouri, Afsaneh Dadarkhah, and Zahra Rezasoltani; Methodology: Seyed Mostafa Teymouri, Afsaneh Dadarkhah, and Mohammad Hassan Kazemi-Galougahi; Investigation: Seyed Mostafa Teymour; Writing the original draft: Seyed Mostafa Teymouri; Review and editing: Afsaneh Dadarkhah, Zahra Rezasoltani, Seyed Morteza Tabatabaee, and Mohammad Hassan Kazemi-Galougahi; Supervision: Afsaneh Dadarkhah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are profoundly grateful to the military personnel who volunteered their time despite of their demanding schedules.
References
- Li Y, Zou C, Guo W, Han F, Fan T, Zang L, et al. Global burden of low back pain and its attributable risk factors from 1990 to 2021: A comprehensive analysis from the global burden of disease study 2021. Frontiers in Public Health. 2024; 12:1480779. [DOI:10.3389/fpubh.2024.1480779] [PMID]
- Ferreira ML, de Luca K, Haile LM, Steinmetz JD, Culbreth GT, Cross M, et al. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: A systematic analysis of the global burden of disease study 2021. The Lancet Rheumatology. 2023; 5(6):e316-29. [DOI:10.2139/ssrn.4318392]
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017; 389(10070):736-47. [DOI:10.1016/S0140-6736(16)30970-9] [PMID]
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018; 391(10137):2356-67. [DOI:10.1016/S0140-6736(18)30480-X] [PMID]
- Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. Journal of Spinal Disorders & Techniques. 2005; 18(1):40-7. [DOI:10.1097/01.bsd.0000117542.88865.77] [PMID]
- Mac-Thiong JM, Labelle H, Berthonnaud E, Betz RR, Roussouly P. Sagittal spinopelvic balance in normal children and adolescents. European Spine Journal. 2007; 16(2):227-34. [DOI:10.1007/s00586-005-0013-8] [PMID]
- Tüzün C, Yorulmaz I, Cindaş A, Vatan S. Low back pain and posture. Clinical Rheumatology. 1999; 18(4):308-12. [DOI:10.1007/s100670050107] [PMID]
- Errabity A, Calmels P, Han WS, Bonnaire R, Pannetier R, Convert R, et al. The effect of low back pain on spine kinematics: A systematic review and meta-analysis. Clinical biomechanics. 2023; 108:106070. [DOI:10.1016/j.clinbiomech.2023.106070] [PMID]
- Chaléat-Valayer E, Mac-Thiong JM, Paquet J, Berthonnaud E, Siani F, Roussouly P. Sagittal spino-pelvic alignment in chronic low back pain. European Spine Journal. 2011; 20(Suppl 5):634-40. [DOI:10.1007/s00586-011-1931-2] [PMID]
- Chun SW, Lim CY, Kim K, Hwang J, Chung SG. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine Journal. 2017; 17(8):1180-91. [DOI:10.1016/j.spinee.2017.04.034] [PMID]
- Habibi Z, Maleki F, Meybodi AT, Mahdavi A, Saberi H. Lumbosacral sagittal alignment in association to intervertebral disc diseases. Asian Spine Journal. 2014; 8(6):813-9. [DOI:10.4184/asj.2014.8.6.813] [PMID]
- Hansen BB, Bendix T, Grindsted J, Bliddal H, Christensen R, Hansen P, et al. Effect of lumbar disc degeneration and low-back pain on the lumbar lordosis in supine and standing: A cross-sectional MRI study. Spine. 2015; 40(21):1690-6. [DOI:10.1097/BRS.0000000000001120] [PMID]
- Ivo R, Nicklas A, Dargel J, Sobottke R, Delank KS, Eysel P, Weber B. Brain structural and psychometric alterations in chronic low back pain. European Spine Journal. 2013; 22(9):1958-64. [DOI:10.1007/s00586-013-2692-x] [PMID]
- Akeda K, Takegami N, Yamada J, Fujiwara T, Nishimura A, Sudo A. Central sensitization in chronic low back pain: A population-based study of a Japanese mountain village. Journal of Pain Research. 2021; 14:1271-80. [DOI:10.2147/JPR.S301924] [PMID]
- Takegami N, Akeda K, Yamada J, Nishimura A, Sudo A. Association between low back pain and psychological stress response in a Japanese population-based study. Journal of Orthopaedic Science. 2024; 29(3):749-54. [DOI:10.1016/j.jos.2023.04.001] [PMID]
- Nava-Bringas TI, Macías-Hernández SI, Vásquez-Ríos JR, Coronado-Zarco R, Miranda-Duarte A, Cruz-Medina E, et al. Fear-avoidance beliefs increase perception of pain and disability in Mexicans with chronic low back pain. Revista Brasileira de Reumatologia. 2017; 57(4):306-10. [DOI:10.1016/j.rbre.2016.11.003] [PMID]
- Collinet A, Ntilikina Y, Romani A, Schuller S, Sauleau EA, Charles YP. Psychopathological profile and sagittal alignment in low-back pain. Orthopaedics & Traumatology, Surgery & Research. 2023; 109(2):103474. [DOI:10.1016/j.otsr.2022.103474] [PMID]
- Steinmetz A, Hacke F, Delank KS. Pressure pain thresholds and central sensitization in relation to psychosocial predictors of chronicity in low back pain. Diagnostics. 2023; 13(4):786. [DOI:10.3390/diagnostics13040786] [PMID]
- Xing WY, Zhang YH, Yang QH, Wang XQ. Prevalence and risk factors of low back pain in military personnel: A systematic review. EFORt Open Reviews. 2024; 9(10):1002-12. [DOI:10.1530/EOR-22-0113] [PMID]
- Abt JP, Perlsweig K, Nagai T, Sell TC, Wirt MD, Lephart SM. Effects of age and military service on strength and physiological characteristics of U.S. army soldiers. Military Medicine. 2016; 181(2):173-9. [DOI:10.7205/MILMED-D-15-00036] [PMID]
- Ernat J, Knox J, Orchowski J, Owens B. Incidence and risk factors for acute low back pain in active duty infantry. Military Medicine. 2012; 177(11):1348-51. [DOI:10.7205/MILMED-D-12-00183] [PMID]
- Bujang MA, Baharum N. Sample size guideline for correlation analysis. World Journal of Social Science Research. 2016; 3(1):37. [DOI:10.22158/wjssr.v3n1p37]
- Noorollahzadeh K, Kahrizi S, Fesharaki MG, Heidarian M, Neblett R, Behzadipour S. Cross-cultural adaptation and psychometric validation of the Persian version of the central sensitization inventory. Musculoskeletal Science & Practice. 2021; 51:102314. [DOI:10.1016/j.msksp.2020.102314] [PMID]
- Vučinić N, Erić M, Tomašević-Todorović S, Milekić B. Application of algometry in patients with cervical and lumbar radiculopathy. Journal of Back and Musculoskeletal Rehabilitation. 2018; 31(3):567-75. [DOI:10.3233/BMR-170965] [PMID]
- Williams ACC, Craig KD. Updating the definition of pain. Pain. 2016; 157(11):2420-3. [DOI:10.1097/j.pain.0000000000000613] [PMID]
- Mousavi SJ, Parnianpour M, Mehdian H, Montazeri A, Mobini B. The oswestry disability index, the roland-morris disability questionnaire, and the quebec back pain disability scale: Translation and validation studies of the Iranian versions. Spine. 2006; 31(14):E454-9. [DOI:10.1097/01.brs.0000222141.61424.f7] [PMID]
- Sharafi SE, Hafizi S, Shahi MH, Kordi R, Noorbala AA, Arbabi M, et al. The Persian version of örebro musculoskeletal pain screening questionnaire: Translation and evaluation of its psychometric properties. International Journal of Preventive Medicine. 2017; 8:14. [DOI:10.4103/2008-7802.201658] [PMID]
- Feng Q, Jiang C, Zhou Y, Huang Y, Zhang M. Relationship between spinal morphology and function and adolescent non-specific back pain: A cross-sectional study. Journal of back and Musculoskeletal Rehabilitation. 2017; 30(3):625-33. [DOI:10.3233/BMR-160544] [PMID]
- Pourahmadi M, Takamjani IE, Sarrafzadeh J, Mohsenifar H, Fazeli SH, Bagheri R, et al. Effect of chronic low back pain on lumbar spine lordosis during sit-to-stand and stand-to-sit. Journal of Manipulative and Physiological Therapeutics. 2020; 43(2):79-92. [DOI:10.1016/j.jmpt.2018.11.028] [PMID]
- Sadler SG, Spink MJ, Ho A, De Jonge XJ, Chuter VH. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskeletal Disorders. 2017; 18(1):179. [DOI:10.1186/s12891-017-1534-0] [PMID]
- Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: A systematic review. Spine Journal. 2014; 14(5):816-36.[DOI:10.1016/j.spinee.2013.09.036] [PMID]
- Singhal K, Muliyala KP, Pakhare AP, Behera P, Santoshi JA. Do patients of chronic low back pain have psychological comorbidities? Avicenna Journal of Medicine. 2021; 11(3):145-51. [DOI:10.1055/s-0041-1734385] [PMID]
- Mingorance JA, Montoya P, Vivas Miranda JG, Riquelme I. Differences in postural balance, pain sensitivity and depression between individuals with acute and chronic back pain. Journal of Clinical Medicine. 2022;11(10). [DOI:10.3390/jcm11102700] [PMID]
- Gräper PJ, Hartvigsen J, Scafoglieri A, Clark JR, van Trijffel E, Hallegraeff JM. Sensory profiles and their role in the persistence of central sensitization symptoms in low back pain. A prospective cohort study. Physiotherapy Theory and Practice. 2024; 41(2):317-26. [DOI:10.1080/09593985.2024.2326592] [PMID]
- Moriki K, Tushima E, Ogihara H, Endo R, Sato T, Ikemoto Y. Combined effects of lifestyle and psychosocial factors on central sensitization in patients with chronic low back pain: A cross-sectional study.Journal of Orthopaedic Science. 2022; 27(6):1185-9. [DOI:10.1016/j.jos.2021.07.012] [PMID]
- Dahmani D, Taik FZ, Berrichi I, Fourtassi M, Abourazzak FE. Impact of central sensitization on pain, disability and psychological distress in patients with knee osteoarthritis and chronic low back pain. BMC Musculoskeletal Disorders. 2023; 24(1):877. [DOI:10.1186/s12891-023-07019-z] [PMID]
- Mibu A, Nishigami T, Tanaka K, Manfuku M, Yono S. Difference in the impact of central sensitization on pain-related symptoms between patients with chronic low back pain and knee osteoarthritis. Journal of Pain Research. 2019; 12:1757-65. [DOI:10.2147/JPR.S200723] [PMID]
- Tran TH, Van MP. Effects of cognitive behavioral therapy combined with physical therapy on improving outcomes in chronic low back pain. Journal of Physical Therapy Science. 2025; 37(6):291-7. [Link]
Article type: Original Research Articles |
Subject:
Physical Medicine and Rehabilitation
Received: 2025/07/20 | Accepted: 2025/09/9 | Published: 2025/12/1
Received: 2025/07/20 | Accepted: 2025/09/9 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
