
988368
Wed, Jul 22, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 451-462 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ali Aqeel S, Lateef Muhe-Aldeen A. The Relationship Between Social Support and Psychological Well-being Among Chronic Hemodialysis Patients. Iranian Rehabilitation Journal 2025; 23 (4) :451-462
URL: http://irj.uswr.ac.ir/article-1-2579-en.html
URL: http://irj.uswr.ac.ir/article-1-2579-en.html



1- Department of Psychiatric and Mental Health Nursing, College of Nursing, University of Kirkuk, Kirkuk, Iraq.
Keywords: Social support, Psychological well-being, Renal dialysis, Kidney disease, Health personnel
Full-Text [PDF 510 kb]
(778 Downloads)
| Abstract (HTML) (2130 Views)
Full-Text: (349 Views)
Introduction
Chronic kidney disease (CKD) is a significant global health challenge, classified among the top 20 causes of mortality worldwide. This progressive, non-communicable condition affects approximately 600 million individuals globally, leading to an estimated 60,000+ fatalities annually due to its complications [1, 2]. The etiology of CKD is multifaceted, with various underlying diseases and comorbidities contributing to its development across all age demographics. A critical concern is the often-asymptomatic nature of early-stage CKD, underscoring the imperative for early detection and intervention. Historically, CKD has been misperceived as an inevitable consequence of aging or a condition impacting a limited segment of the population, rather than a prevalent, preventable, and treatable chronic illness [3, 4]. The psychological sequelae of chronic disease are substantial, frequently inducing feelings of guilt, a perceived loss of control, anger, grief, confusion, and fear among affected individuals [5].
Hemodialysis remains a cornerstone treatment modality for end-stage renal disease, a prevalent manifestation of advanced CKD. This life-sustaining procedure involves extracorporeal blood filtration to remove metabolic toxins and excess fluid, followed by reinfusion into the patient [6]. Despite its efficacy in prolonging survival, patients undergoing chronic hemodialysis face heightened mortality risks, particularly those with coexisting morbidities such as hypertension, cardiovascular disease, and type 2 diabetes mellitus [7]. The ongoing need for continuous hemodialysis therapy until the end of life profoundly impacts multiple dimensions of a patient’s existence, including their physical, psychological, financial, and social well-being [8].
The quality of an individual’s social connections is a well-established determinant of their capacity to manage stress and maintain overall well-being [9]. Empirical evidence consistently demonstrates that social support enhances health outcomes, with patients undergoing hemodialysis typically drawing support from their social networks, comprising family, friends, colleagues, and healthcare providers [10]. The specific social support needs of hemodialysis patients are heterogeneous, influenced by disease severity, the structure and quality of their social networks, and a range of individual psychosocial factors [11].
Emerging research suggests that psychological benefits may be derived from perceived social support among individuals undergoing chronic hemodialysis. However, a comprehensive review of the literature reveals a notable paucity of studies specifically investigating the intricate relationship between hemodialysis patients’ perceptions of social support and their mental health status. Therefore, this study aimed to elucidate the correlation between perceived social support and psychological well-being in this patient cohort.
Materials and Methods
Study design and setting
This quantitative study employed a descriptive correlational design to investigate the relationship between perceived social support and psychological well-being among hemodialysis patients. The study was conducted over six months, from November 20, 2024, to May 30, 2025. Data were collected at the AL-Amal Dialysis Center, located in Kirkuk city, in the northern region of Iraq. This setting was chosen due to its representative patient population undergoing regular hemodialysis treatment.
Sample size and sampling method
A non-probability purposive sampling technique was utilized to recruit a sample of 260 patients from the AL-Amal Dialysis Center. Purposive sampling was selected to ensure that participants met specific inclusion criteria relevant to the study objectives, thereby facilitating the collection of accurate and pertinent data. The inclusion criteria for participants included being an adult (>18 years), undergoing regular hemodialysis treatment at the center, communicating in the language of the questionnaire (Arabic/Kurdish), and providing informed consent to participate. Patients with severe cognitive impairment or those unable to provide consent were excluded.
Tools and instruments
Data were collected using a structured questionnaire comprising three sections:
Sociodemographic and hemodialysis-related variables questionnaire: This researcher-designed questionnaire was developed following an extensive review of relevant literature to capture essential demographic and clinical information.
Part 1: Sociodemographic characteristics: This section collected data on age (in years), sex, marital status, level of education, socioeconomic status, and area of residence (urban/rural).
Part 2: Hemodialysis-related variables: This section focused on clinical aspects pertinent to hemodialysis, including the duration of illness (years), the duration of hemodialysis treatment (years), the frequency of hemodialysis sessions per week, and the average duration of each hemodialysis session (hours).
General health questionnaire (GHQ-12): Williams and Goldberg [12] developed the general health questionnaire (GHQ-12), a widely recognized and validated instrument for screening psychological distress, including symptoms of depression, anxiety, and social dysfunction. This study utilized a version adapted for patients undergoing medical treatment. The instrument consists of 12 items, each rated on a four-point Likert scale: “Always,” “often,” “sometimes,” and “never.” Higher scores indicate a greater presence of psychological symptoms. The GHQ-12 was translated into Arabic to ensure comprehension among the study participants in Kirkuk City, Iraq. The instrument was translated into Arabic following a rigorous forward-backward translation procedure to maintain semantic and conceptual equivalence. Cultural adaptation was conducted in consultation with bilingual healthcare professionals to ensure clarity and appropriateness of items within the local context. Regarding the reliability, the internal consistency of the GHQ-12 was acceptable, with a Cronbach’s α coefficient of 0.86, while the perceived social support scale demonstrated a high level of internal consistency, yielding a Cronbach’s α of 0.91, indicating excellent reliability for both instruments in this sample. Additionally, the test re-test reliability was assessed using the intraclass correlation coefficient (ICC) over a one-week interval among a pilot sample of 30 hemodialysis patients, resulting in an ICC value of 0.88 for the GHQ-12 and 0.92 for the social support scale, both indicating strong temporal stability. The standard error of measurement (SEM) was calculated as Equation 1:
1. SEM=SD×√(1−ICC),
yielding an SEM of 1.38 for the GHQ-12 and 2.14 for the social support scale [12].
The perceived social support—healthcare provider scale, adapted from the original multidimensional scale of perceived social support (MSPSS) developed by Zimet et al. [13], was utilized in this study to specifically assess the level of support perceived by hemodialysis patients from their healthcare providers. The scale was translated into Arabic following a rigorous forward-backward translation process and cultural adaptation to ensure linguistic validity and contextual relevance for the study population in Kirkuk City. The final version consisted of 15 items, each rated on a five-point Likert scale ranging from “totally disagree” (1) to “totally agree” (5), with higher total scores indicating greater perceived social support from healthcare professionals. The scale’s reliability in the current sample was evaluated using Cronbach’s α coefficient, which yielded an excellent internal consistency value of 0.91. Additionally, test re-test reliability was assessed over a one-week interval in a pilot sample of 30 participants, resulting in an ICC of 0.92, indicating high temporal stability. The SEM was calculated as Equation 1, producing an SEM of 2.14, reflecting minimal measurement error and supporting the instrument’s precision in this study. These psychometric properties confirm the reliability and appropriateness of the adapted scale for use in the target population [13].
Ethical considerations
The study protocol received full ethical approval from the Ethics Committee of the College of Nursing at the University of Kirkuk. Prior to commencing data collection, official authorization was obtained from the Health Directorate of Kirkuk City. All participants were provided comprehensive information about the study’s purpose, procedures, potential risks, and benefits. Participation was voluntary, and each patient provided informed verbal consent before being included in the study. Confidentiality and anonymity were maintained throughout the research process; data were de-identified, and participants were assured that their responses would not affect their ongoing medical care.
Statistical analysis
All statistical analyses were performed using SPSS software, version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were employed to summarize the study sample’s characteristics. Categorical variables (e.g. sex, marital status, residence) were presented as frequencies and percentages. Continuous variables (e.g. age, duration of illness, GHQ-12 scores, and perceived social support scores) were expressed as the Mean±SD.
Inferential statistical methods were used to examine the relationships between variables and assess the psychometric properties of the instruments. The Kolmogorov–Smirnov test was used to assess the normality of the distribution of continuous variables. Spearman’s rank correlation coefficient was employed to analyze the relationship between ordinal variables and variables with non-normal distributions. The point-biserial correlation coefficient was used to examine the relationship between a dichotomous variable (e.g. sex, if dichotomized for specific analysis) and a continuous variable. Cronbach’s α coefficient was calculated to determine the internal consistency reliability of the GHQ-12 and the perceived social support scale within this specific study population.
Results
Sociodemographic characteristics
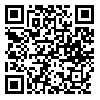
A total of 260 patients participated in this study. The demographic profile revealed that most participants were male (56.2%), with females constituting 43.8%. The most represented age group was 60-69 years (32.4%), followed by the 50-59 years group (21.9%). A significant proportion of patients were married (72.3%). Regarding educational attainment, 27.3% of the participants reported being unable to read or write, while 12.7% could read and write. Approximately 16.1% had completed intermediate education, and 13.5% had attained higher education. Most patients (83.8%) resided in urban areas, with a smaller percentage living in rural areas (16.2%) (Table 1).
Hemodialysis-related variables
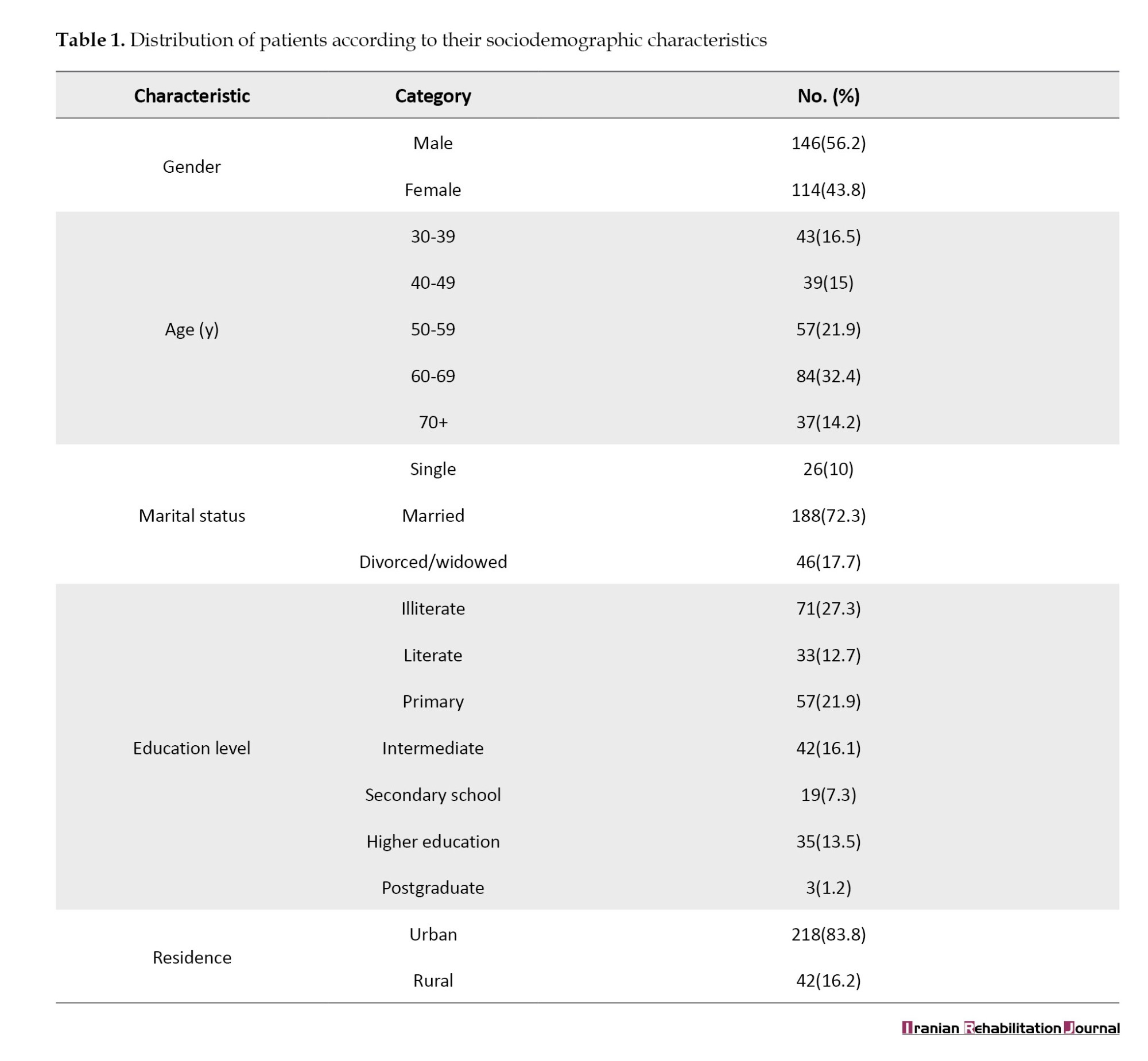
Table 2 presents the characteristics related to hemodialysis treatment. A substantial portion of patients (44.6%) reported having lived with their illness for five years or more. For the duration of hemodialysis treatment, the largest groups reported “less than one year” (30%) and “1-2 years” (30%). The standard treatment frequency for most patients was three times per week (65%). Regarding the duration of hemodialysis sessions, 63.8% of patients typically underwent three-hour sessions, while 36.2% had four-hour sessions.
Social support assessment
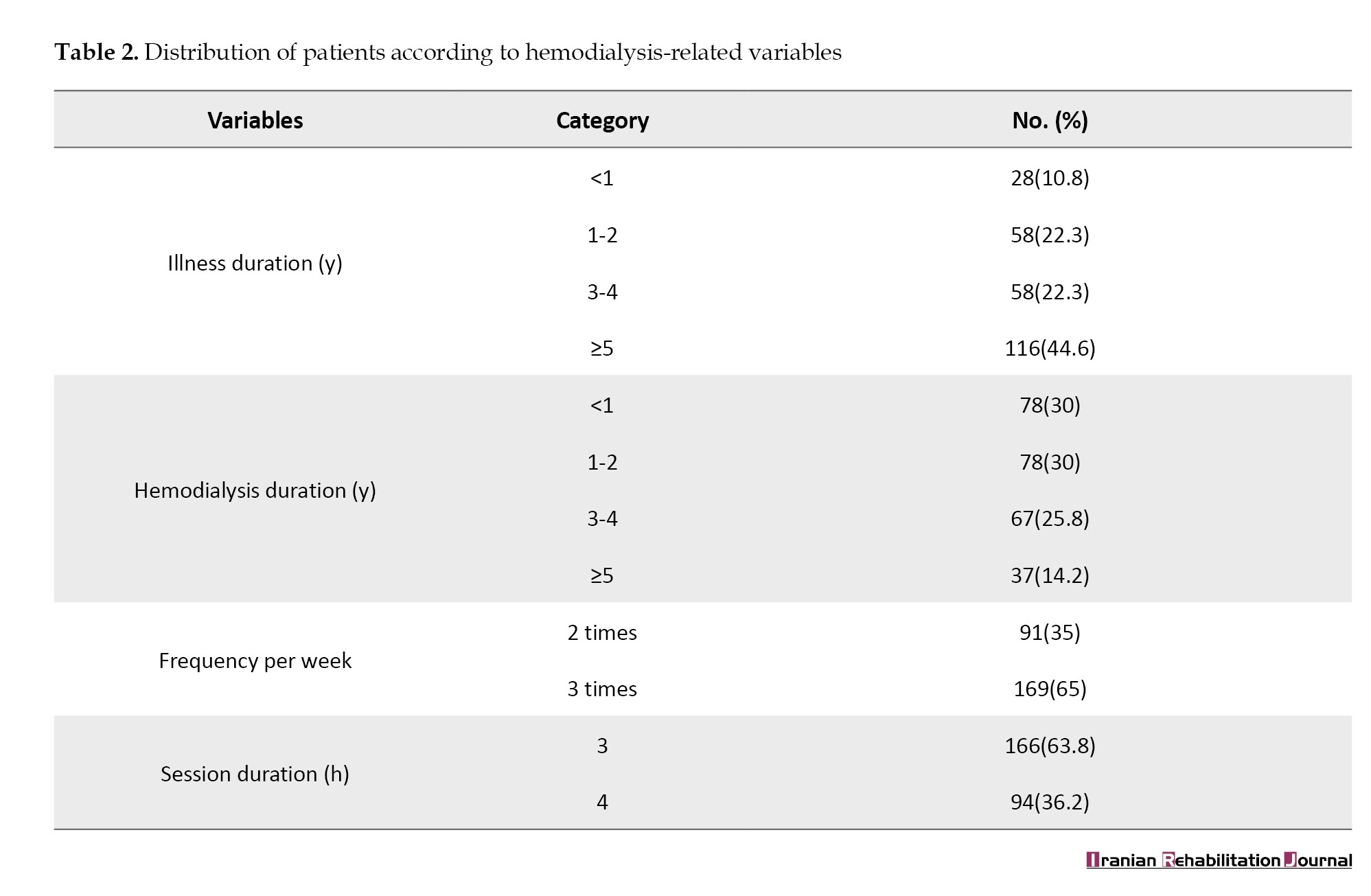
Table 3 presents the perceived social support from healthcare providers in various aspects of care. Patients reported high levels of perceived support in several domains, including receiving moral support (Mean±SD 4±1.01), feeling that providers were interested in them (Mean±SD 3.94±0.58), and experiencing openness in communication (Mean±SD 4.17±0.75). Patients also perceived high support for problem-solving assistance (Mean±SD 3.85±0.59) and positive interactions (Mean±SD 4.39±0.692). However, moderate levels of support were indicated in areas such as sensitivity to personal needs (Mean±SD 3.33±1) and reliance on providers for emotional support when feeling down (Mean±SD 3.01±0.95). A notably lower perceived support score was observed for providers sharing personal details (Mean±SD 2.38±1.14), suggesting limited reciprocal communication.
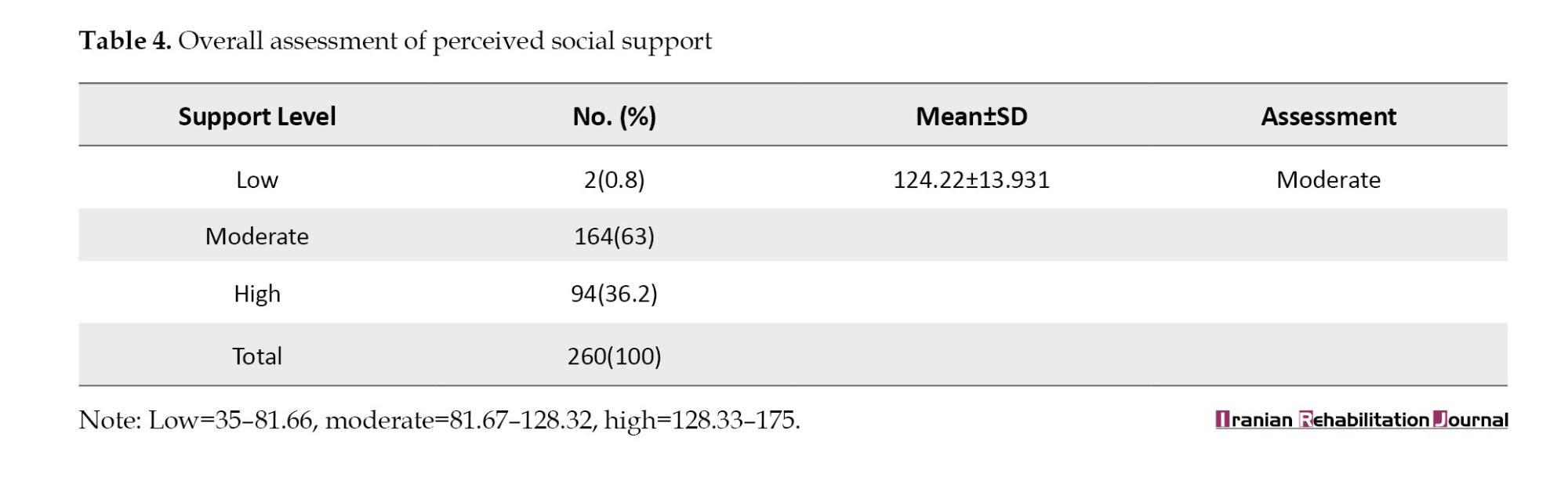
Table 4 presents the overall perceived social support. The findings indicated that most patients (63%) perceived moderate social support, while 36.2% perceived high social support. Only a small fraction (0.8%) reported low social support. The overall mean score for perceived social support was 124.22±13.931, which, according to the study’s classification, reflected a moderate level of overall social support.
Relationships between perceived social support and sociodemographic characteristics
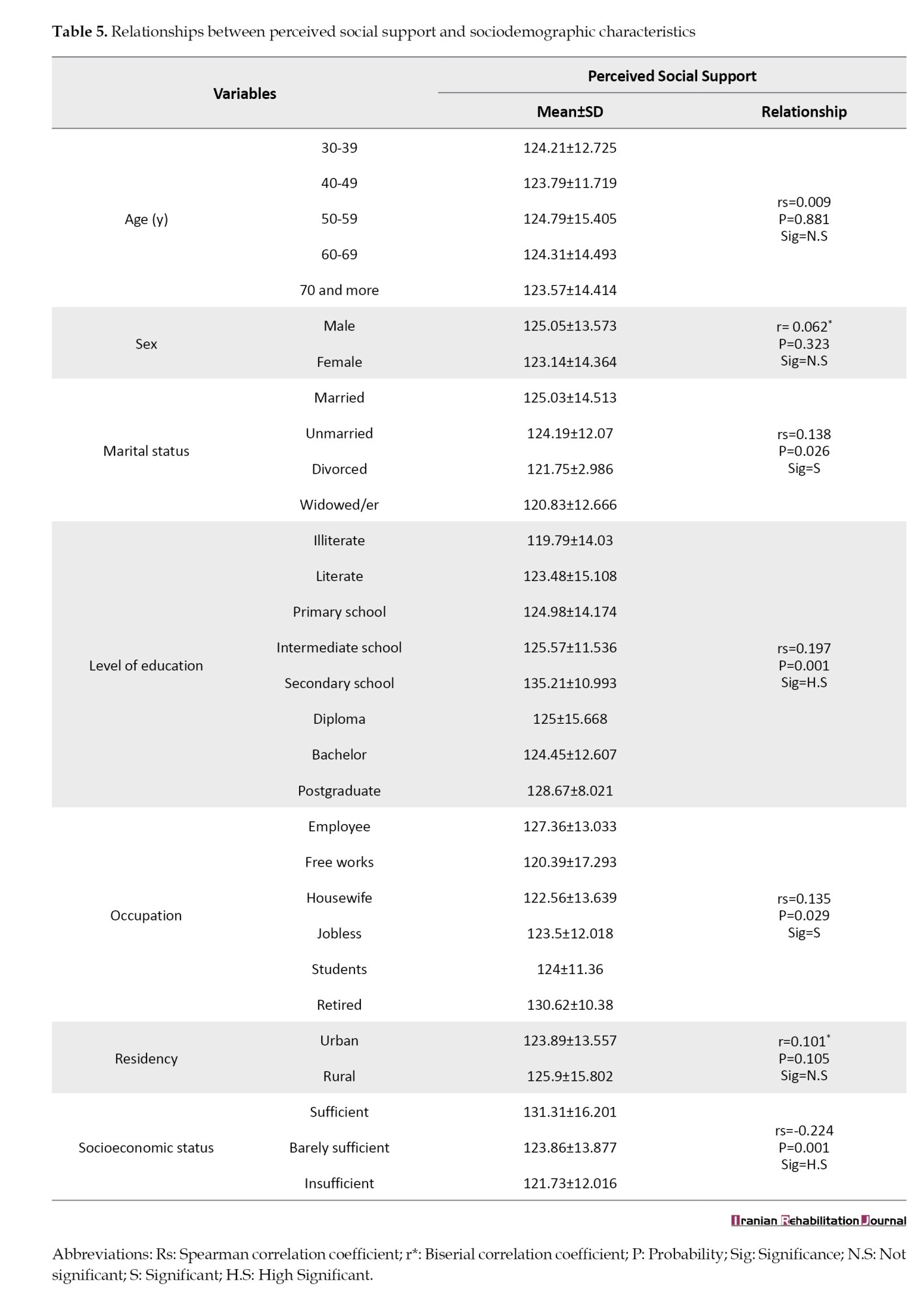
Table 5 presents the relationship between perceived social support and various sociodemographic factors. Significant relationships were found between marital status and education level. Married patients reported slightly higher perceived social support (mean=125.03) compared to unmarried or divorced/widowed groups, with this relationship being statistically significant (P=0.026). Education level demonstrated a strong, significant positive relationship with perceived social support (rs=0.197, P=0.001). Specifically, patients with secondary school education reported the highest mean perceived social support (M=135.21), indicating a trend in which higher education levels are associated with greater perceived support. Occupation also showed a significant relationship (rs=0.135, P=0.029), with retired individuals reporting higher support (M=130.62) compared to other occupational categories. Socioeconomic status was also significantly related (rs=-0.224, P=0.001), with those reporting “sufficient” socioeconomic status perceiving higher support than those with “barely sufficient” or “insufficient” status. In contrast, age, sex, and place of residence (urban vs rural) did not show statistically significant relationships with perceived social support in this study.
Correlation between social support and psychological well-being
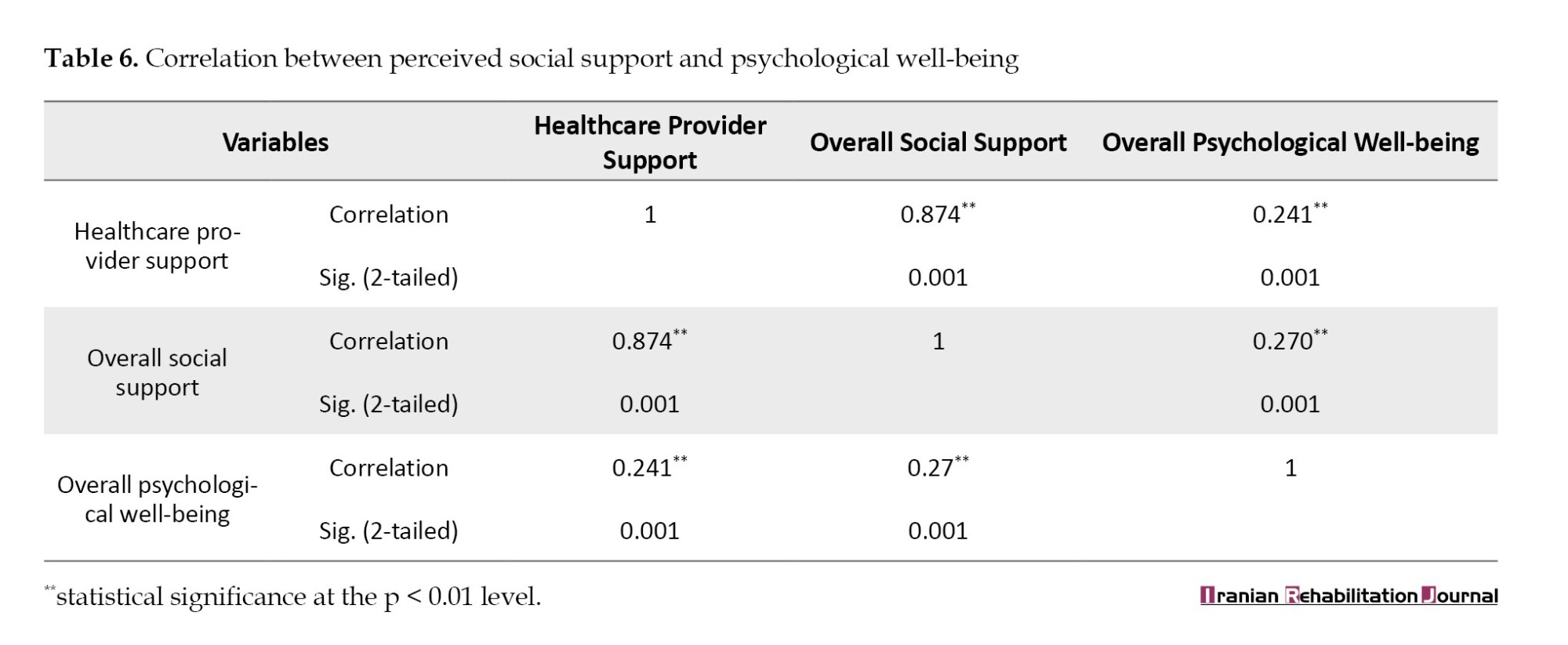
Table 6 presents the correlations between perceived social support and psychological well-being. A significant positive correlation was found between psychological well-being and overall perceived social support (r=0.27, P=0.001). This suggests that as perceived social support increases, hemodialysis patients’ psychological well-being tends to improve. Furthermore, healthcare provider support strongly correlated with overall psychological well-being (r=0.241, P=0.001). This indicates that the quality of support received from healthcare providers is a significant contributing factor to the psychological well-being of patients.
Discussion
This study aimed to assess the levels of psychological well-being and social support among individuals undergoing hemodialysis, and to investigate the correlation between social support and psychological well-being within this patient group. The demographic composition of the sample provided valuable insights into the characteristics of hemodialysis patients and their specific support needs.
The predominance of older adults in the sample, with the largest age group being 60-69 years (32.4%), aligns with established literature indicating an increased prevalence of chronic kidney failure with advancing age. This finding is consistent with studies in the United States [14], which reported that older dialysis patients, particularly those aged 60-69, tend to exhibit lower serum phosphorus levels and poorer nutritional status compared to their younger counterparts.
The gender distribution, with a majority of male participants (56.2%), mirrors the findings of studies conducted in Iran [15] that explored the impact of perceived social support, spiritual well-being, health literacy, and resilience on the quality of life (QoL) of hemodialysis patients. This male-predominant pattern appears consistent across various cultural contexts.
Analysis of marital status revealed that most patients (72.3%) were married. This observation resonates with research from Iran [16], which identified marital status as a significant factor influencing the achievement of therapeutic goals. Married individuals demonstrated superior adherence to treatment protocols compared to single or widowed patients, suggesting that the presence of a spouse offers critical emotional and practical support throughout the demanding hemodialysis treatment process.
The residential distribution, with most patients residing in urban areas (83.8%), is consistent with studies from Kenya [17]. It indicates a higher concentration of patients in metropolitan regions compared to rural settings. Urban residence may be correlated with improved access to dialysis facilities and healthcare services.
Regarding educational attainment, over a quarter of the patients (27.3%) were illiterate. This finding supports studies conducted in Kirkuk [18], which also reported a significant proportion of patients with low literacy levels. Educational level emerged as a significant predictor of perceived social support, with patients possessing a secondary school education reporting higher support levels than those with lower educational attainment.
Occupational status analysis indicated that a notable percentage of patients were housewives, a finding echoed in research from Southern Ethiopia [19]. This study highlighted that an individual’s employment status significantly impacts their QoL, social engagement, and treatment adherence. Occupational status not only influences financial stability but also shapes social relationships and a sense of purpose.
An examination of socioeconomic status revealed that nearly half of the patients (49.2%) perceived their financial situation as “barely sufficient.” This result is comparable to findings from Taiwan [20], underscoring the influence of socioeconomic status on patient health outcomes. Financial constraints can pose significant barriers to accessing healthcare, nutritious food, and maintaining a good QoL.
Regarding hemodialysis-related factors, the study indicated that 44.6% of patients had been undergoing treatment for “5 years or more.” This aligns with research from Ethiopia [21], where the median duration of illness was reported to be 65 months (approximately 5 years). The chronicity of illness can influence a patient’s adaptation to treatment and their coping mechanisms for managing a long-term health condition.
A distribution of 30% of patients having been on hemodialysis for “less than a year” and another 30% for “1-2 years” is comparable to findings from the United States [22] concerning the duration of hemodialysis and its impact on patient outcomes. A substantial number of patients (approximately two-thirds) on hemodialysis for less than a year suggests that a significant portion of the sample was in the early stages of adapting to the treatment regimen.
The finding that approximately 65% of patients underwent hemodialysis treatments “three days a week,” with 63.8% having sessions lasting “three hours,” is consistent with a study from China [23]. This treatment frequency (three times a week) is often associated with better outcomes and reduced mortality rates in hemodialysis patients.
The study’s social support assessment revealed that 63% of patients perceived moderate social support. This finding aligns with research indicating that hemodialysis patients experience comparable levels of social support to those with other chronic illnesses [24]. Furthermore, individuals who perceived higher social support reported less fatigue, pain, depression, and anxiety, emphasizing the crucial role of robust support networks in enhancing patient outcomes.
The positive relationship between marital status, education level, and perceived social support indicates that married patients and those with higher education levels tend to receive greater social support. This finding corroborates earlier research from Turkey [25] and Poland [26], identifying social support as a predictive factor for QoL in hemodialysis patients. Marital status significantly influences the availability of emotional and informational support, while educational level affects the patient’s ability to access and utilize support resources.
The positive correlation (r=0.270, P=0.001) between social support and mental health signifies that hemodialysis patients with greater perceived social support generally exhibit better mental health. Direct assistance from healthcare providers plays a vital role in enhancing psychological well-being, highlighting the importance of healthcare professionals offering medical care and emotional and social support. This outcome is consistent with previous research demonstrating a strong positive correlation between perceived social support and overall psychological resilience in dialysis patients [27, 28], where increased social support is associated with improved coping capabilities.
Conclusion
This study provides valuable insights into the influence of social support on the psychological well-being of chronic hemodialysis patients in Kirkuk City. The findings indicate that most patients experience moderate levels of both perceived social support and psychological well-being. The study identified that certain sociodemographic factors, namely marital status and educational attainment, are significantly associated with perceived social support and psychological well-being.
The positive correlation between social support and mental health underscores the critical importance of robust support systems for hemodialysis patients. Healthcare providers play a pivotal role in fostering mental health among these individuals. This study demonstrates that patients who receive adequate social support from various sources, including healthcare providers, family, and friends, are better equipped to manage their chronic illness and maintain a higher QoL.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Research Ethics Committee of the College of Nursing, University of Kirkuk, Kirkuk, Iraq on November 24, 2024 (Code: 8).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, investigation, writing the original draft, data collection and data analysis: Sumaya Ali Aqeel; Supervision, methodology, review & editing: Abbas Lateef Muhe-Aldeen.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their sincere gratitude to the staff of the Al-Amal Dialysis Center in Kirkuk City for their invaluable cooperation and support in facilitating data collection.
References
Chronic kidney disease (CKD) is a significant global health challenge, classified among the top 20 causes of mortality worldwide. This progressive, non-communicable condition affects approximately 600 million individuals globally, leading to an estimated 60,000+ fatalities annually due to its complications [1, 2]. The etiology of CKD is multifaceted, with various underlying diseases and comorbidities contributing to its development across all age demographics. A critical concern is the often-asymptomatic nature of early-stage CKD, underscoring the imperative for early detection and intervention. Historically, CKD has been misperceived as an inevitable consequence of aging or a condition impacting a limited segment of the population, rather than a prevalent, preventable, and treatable chronic illness [3, 4]. The psychological sequelae of chronic disease are substantial, frequently inducing feelings of guilt, a perceived loss of control, anger, grief, confusion, and fear among affected individuals [5].
Hemodialysis remains a cornerstone treatment modality for end-stage renal disease, a prevalent manifestation of advanced CKD. This life-sustaining procedure involves extracorporeal blood filtration to remove metabolic toxins and excess fluid, followed by reinfusion into the patient [6]. Despite its efficacy in prolonging survival, patients undergoing chronic hemodialysis face heightened mortality risks, particularly those with coexisting morbidities such as hypertension, cardiovascular disease, and type 2 diabetes mellitus [7]. The ongoing need for continuous hemodialysis therapy until the end of life profoundly impacts multiple dimensions of a patient’s existence, including their physical, psychological, financial, and social well-being [8].
The quality of an individual’s social connections is a well-established determinant of their capacity to manage stress and maintain overall well-being [9]. Empirical evidence consistently demonstrates that social support enhances health outcomes, with patients undergoing hemodialysis typically drawing support from their social networks, comprising family, friends, colleagues, and healthcare providers [10]. The specific social support needs of hemodialysis patients are heterogeneous, influenced by disease severity, the structure and quality of their social networks, and a range of individual psychosocial factors [11].
Emerging research suggests that psychological benefits may be derived from perceived social support among individuals undergoing chronic hemodialysis. However, a comprehensive review of the literature reveals a notable paucity of studies specifically investigating the intricate relationship between hemodialysis patients’ perceptions of social support and their mental health status. Therefore, this study aimed to elucidate the correlation between perceived social support and psychological well-being in this patient cohort.
Materials and Methods
Study design and setting
This quantitative study employed a descriptive correlational design to investigate the relationship between perceived social support and psychological well-being among hemodialysis patients. The study was conducted over six months, from November 20, 2024, to May 30, 2025. Data were collected at the AL-Amal Dialysis Center, located in Kirkuk city, in the northern region of Iraq. This setting was chosen due to its representative patient population undergoing regular hemodialysis treatment.
Sample size and sampling method
A non-probability purposive sampling technique was utilized to recruit a sample of 260 patients from the AL-Amal Dialysis Center. Purposive sampling was selected to ensure that participants met specific inclusion criteria relevant to the study objectives, thereby facilitating the collection of accurate and pertinent data. The inclusion criteria for participants included being an adult (>18 years), undergoing regular hemodialysis treatment at the center, communicating in the language of the questionnaire (Arabic/Kurdish), and providing informed consent to participate. Patients with severe cognitive impairment or those unable to provide consent were excluded.
Tools and instruments
Data were collected using a structured questionnaire comprising three sections:
Sociodemographic and hemodialysis-related variables questionnaire: This researcher-designed questionnaire was developed following an extensive review of relevant literature to capture essential demographic and clinical information.
Part 1: Sociodemographic characteristics: This section collected data on age (in years), sex, marital status, level of education, socioeconomic status, and area of residence (urban/rural).
Part 2: Hemodialysis-related variables: This section focused on clinical aspects pertinent to hemodialysis, including the duration of illness (years), the duration of hemodialysis treatment (years), the frequency of hemodialysis sessions per week, and the average duration of each hemodialysis session (hours).
General health questionnaire (GHQ-12): Williams and Goldberg [12] developed the general health questionnaire (GHQ-12), a widely recognized and validated instrument for screening psychological distress, including symptoms of depression, anxiety, and social dysfunction. This study utilized a version adapted for patients undergoing medical treatment. The instrument consists of 12 items, each rated on a four-point Likert scale: “Always,” “often,” “sometimes,” and “never.” Higher scores indicate a greater presence of psychological symptoms. The GHQ-12 was translated into Arabic to ensure comprehension among the study participants in Kirkuk City, Iraq. The instrument was translated into Arabic following a rigorous forward-backward translation procedure to maintain semantic and conceptual equivalence. Cultural adaptation was conducted in consultation with bilingual healthcare professionals to ensure clarity and appropriateness of items within the local context. Regarding the reliability, the internal consistency of the GHQ-12 was acceptable, with a Cronbach’s α coefficient of 0.86, while the perceived social support scale demonstrated a high level of internal consistency, yielding a Cronbach’s α of 0.91, indicating excellent reliability for both instruments in this sample. Additionally, the test re-test reliability was assessed using the intraclass correlation coefficient (ICC) over a one-week interval among a pilot sample of 30 hemodialysis patients, resulting in an ICC value of 0.88 for the GHQ-12 and 0.92 for the social support scale, both indicating strong temporal stability. The standard error of measurement (SEM) was calculated as Equation 1:
1. SEM=SD×√(1−ICC),
yielding an SEM of 1.38 for the GHQ-12 and 2.14 for the social support scale [12].
The perceived social support—healthcare provider scale, adapted from the original multidimensional scale of perceived social support (MSPSS) developed by Zimet et al. [13], was utilized in this study to specifically assess the level of support perceived by hemodialysis patients from their healthcare providers. The scale was translated into Arabic following a rigorous forward-backward translation process and cultural adaptation to ensure linguistic validity and contextual relevance for the study population in Kirkuk City. The final version consisted of 15 items, each rated on a five-point Likert scale ranging from “totally disagree” (1) to “totally agree” (5), with higher total scores indicating greater perceived social support from healthcare professionals. The scale’s reliability in the current sample was evaluated using Cronbach’s α coefficient, which yielded an excellent internal consistency value of 0.91. Additionally, test re-test reliability was assessed over a one-week interval in a pilot sample of 30 participants, resulting in an ICC of 0.92, indicating high temporal stability. The SEM was calculated as Equation 1, producing an SEM of 2.14, reflecting minimal measurement error and supporting the instrument’s precision in this study. These psychometric properties confirm the reliability and appropriateness of the adapted scale for use in the target population [13].
Ethical considerations
The study protocol received full ethical approval from the Ethics Committee of the College of Nursing at the University of Kirkuk. Prior to commencing data collection, official authorization was obtained from the Health Directorate of Kirkuk City. All participants were provided comprehensive information about the study’s purpose, procedures, potential risks, and benefits. Participation was voluntary, and each patient provided informed verbal consent before being included in the study. Confidentiality and anonymity were maintained throughout the research process; data were de-identified, and participants were assured that their responses would not affect their ongoing medical care.
Statistical analysis
All statistical analyses were performed using SPSS software, version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were employed to summarize the study sample’s characteristics. Categorical variables (e.g. sex, marital status, residence) were presented as frequencies and percentages. Continuous variables (e.g. age, duration of illness, GHQ-12 scores, and perceived social support scores) were expressed as the Mean±SD.
Inferential statistical methods were used to examine the relationships between variables and assess the psychometric properties of the instruments. The Kolmogorov–Smirnov test was used to assess the normality of the distribution of continuous variables. Spearman’s rank correlation coefficient was employed to analyze the relationship between ordinal variables and variables with non-normal distributions. The point-biserial correlation coefficient was used to examine the relationship between a dichotomous variable (e.g. sex, if dichotomized for specific analysis) and a continuous variable. Cronbach’s α coefficient was calculated to determine the internal consistency reliability of the GHQ-12 and the perceived social support scale within this specific study population.
Results
Sociodemographic characteristics
A total of 260 patients participated in this study. The demographic profile revealed that most participants were male (56.2%), with females constituting 43.8%. The most represented age group was 60-69 years (32.4%), followed by the 50-59 years group (21.9%). A significant proportion of patients were married (72.3%). Regarding educational attainment, 27.3% of the participants reported being unable to read or write, while 12.7% could read and write. Approximately 16.1% had completed intermediate education, and 13.5% had attained higher education. Most patients (83.8%) resided in urban areas, with a smaller percentage living in rural areas (16.2%) (Table 1).
Hemodialysis-related variables
Table 2 presents the characteristics related to hemodialysis treatment. A substantial portion of patients (44.6%) reported having lived with their illness for five years or more. For the duration of hemodialysis treatment, the largest groups reported “less than one year” (30%) and “1-2 years” (30%). The standard treatment frequency for most patients was three times per week (65%). Regarding the duration of hemodialysis sessions, 63.8% of patients typically underwent three-hour sessions, while 36.2% had four-hour sessions.
Social support assessment
Table 3 presents the perceived social support from healthcare providers in various aspects of care. Patients reported high levels of perceived support in several domains, including receiving moral support (Mean±SD 4±1.01), feeling that providers were interested in them (Mean±SD 3.94±0.58), and experiencing openness in communication (Mean±SD 4.17±0.75). Patients also perceived high support for problem-solving assistance (Mean±SD 3.85±0.59) and positive interactions (Mean±SD 4.39±0.692). However, moderate levels of support were indicated in areas such as sensitivity to personal needs (Mean±SD 3.33±1) and reliance on providers for emotional support when feeling down (Mean±SD 3.01±0.95). A notably lower perceived support score was observed for providers sharing personal details (Mean±SD 2.38±1.14), suggesting limited reciprocal communication.
Table 4 presents the overall perceived social support. The findings indicated that most patients (63%) perceived moderate social support, while 36.2% perceived high social support. Only a small fraction (0.8%) reported low social support. The overall mean score for perceived social support was 124.22±13.931, which, according to the study’s classification, reflected a moderate level of overall social support.
Relationships between perceived social support and sociodemographic characteristics
Table 5 presents the relationship between perceived social support and various sociodemographic factors. Significant relationships were found between marital status and education level. Married patients reported slightly higher perceived social support (mean=125.03) compared to unmarried or divorced/widowed groups, with this relationship being statistically significant (P=0.026). Education level demonstrated a strong, significant positive relationship with perceived social support (rs=0.197, P=0.001). Specifically, patients with secondary school education reported the highest mean perceived social support (M=135.21), indicating a trend in which higher education levels are associated with greater perceived support. Occupation also showed a significant relationship (rs=0.135, P=0.029), with retired individuals reporting higher support (M=130.62) compared to other occupational categories. Socioeconomic status was also significantly related (rs=-0.224, P=0.001), with those reporting “sufficient” socioeconomic status perceiving higher support than those with “barely sufficient” or “insufficient” status. In contrast, age, sex, and place of residence (urban vs rural) did not show statistically significant relationships with perceived social support in this study.
Correlation between social support and psychological well-being
Table 6 presents the correlations between perceived social support and psychological well-being. A significant positive correlation was found between psychological well-being and overall perceived social support (r=0.27, P=0.001). This suggests that as perceived social support increases, hemodialysis patients’ psychological well-being tends to improve. Furthermore, healthcare provider support strongly correlated with overall psychological well-being (r=0.241, P=0.001). This indicates that the quality of support received from healthcare providers is a significant contributing factor to the psychological well-being of patients.
Discussion
This study aimed to assess the levels of psychological well-being and social support among individuals undergoing hemodialysis, and to investigate the correlation between social support and psychological well-being within this patient group. The demographic composition of the sample provided valuable insights into the characteristics of hemodialysis patients and their specific support needs.
The predominance of older adults in the sample, with the largest age group being 60-69 years (32.4%), aligns with established literature indicating an increased prevalence of chronic kidney failure with advancing age. This finding is consistent with studies in the United States [14], which reported that older dialysis patients, particularly those aged 60-69, tend to exhibit lower serum phosphorus levels and poorer nutritional status compared to their younger counterparts.
The gender distribution, with a majority of male participants (56.2%), mirrors the findings of studies conducted in Iran [15] that explored the impact of perceived social support, spiritual well-being, health literacy, and resilience on the quality of life (QoL) of hemodialysis patients. This male-predominant pattern appears consistent across various cultural contexts.
Analysis of marital status revealed that most patients (72.3%) were married. This observation resonates with research from Iran [16], which identified marital status as a significant factor influencing the achievement of therapeutic goals. Married individuals demonstrated superior adherence to treatment protocols compared to single or widowed patients, suggesting that the presence of a spouse offers critical emotional and practical support throughout the demanding hemodialysis treatment process.
The residential distribution, with most patients residing in urban areas (83.8%), is consistent with studies from Kenya [17]. It indicates a higher concentration of patients in metropolitan regions compared to rural settings. Urban residence may be correlated with improved access to dialysis facilities and healthcare services.
Regarding educational attainment, over a quarter of the patients (27.3%) were illiterate. This finding supports studies conducted in Kirkuk [18], which also reported a significant proportion of patients with low literacy levels. Educational level emerged as a significant predictor of perceived social support, with patients possessing a secondary school education reporting higher support levels than those with lower educational attainment.
Occupational status analysis indicated that a notable percentage of patients were housewives, a finding echoed in research from Southern Ethiopia [19]. This study highlighted that an individual’s employment status significantly impacts their QoL, social engagement, and treatment adherence. Occupational status not only influences financial stability but also shapes social relationships and a sense of purpose.
An examination of socioeconomic status revealed that nearly half of the patients (49.2%) perceived their financial situation as “barely sufficient.” This result is comparable to findings from Taiwan [20], underscoring the influence of socioeconomic status on patient health outcomes. Financial constraints can pose significant barriers to accessing healthcare, nutritious food, and maintaining a good QoL.
Regarding hemodialysis-related factors, the study indicated that 44.6% of patients had been undergoing treatment for “5 years or more.” This aligns with research from Ethiopia [21], where the median duration of illness was reported to be 65 months (approximately 5 years). The chronicity of illness can influence a patient’s adaptation to treatment and their coping mechanisms for managing a long-term health condition.
A distribution of 30% of patients having been on hemodialysis for “less than a year” and another 30% for “1-2 years” is comparable to findings from the United States [22] concerning the duration of hemodialysis and its impact on patient outcomes. A substantial number of patients (approximately two-thirds) on hemodialysis for less than a year suggests that a significant portion of the sample was in the early stages of adapting to the treatment regimen.
The finding that approximately 65% of patients underwent hemodialysis treatments “three days a week,” with 63.8% having sessions lasting “three hours,” is consistent with a study from China [23]. This treatment frequency (three times a week) is often associated with better outcomes and reduced mortality rates in hemodialysis patients.
The study’s social support assessment revealed that 63% of patients perceived moderate social support. This finding aligns with research indicating that hemodialysis patients experience comparable levels of social support to those with other chronic illnesses [24]. Furthermore, individuals who perceived higher social support reported less fatigue, pain, depression, and anxiety, emphasizing the crucial role of robust support networks in enhancing patient outcomes.
The positive relationship between marital status, education level, and perceived social support indicates that married patients and those with higher education levels tend to receive greater social support. This finding corroborates earlier research from Turkey [25] and Poland [26], identifying social support as a predictive factor for QoL in hemodialysis patients. Marital status significantly influences the availability of emotional and informational support, while educational level affects the patient’s ability to access and utilize support resources.
The positive correlation (r=0.270, P=0.001) between social support and mental health signifies that hemodialysis patients with greater perceived social support generally exhibit better mental health. Direct assistance from healthcare providers plays a vital role in enhancing psychological well-being, highlighting the importance of healthcare professionals offering medical care and emotional and social support. This outcome is consistent with previous research demonstrating a strong positive correlation between perceived social support and overall psychological resilience in dialysis patients [27, 28], where increased social support is associated with improved coping capabilities.
Conclusion
This study provides valuable insights into the influence of social support on the psychological well-being of chronic hemodialysis patients in Kirkuk City. The findings indicate that most patients experience moderate levels of both perceived social support and psychological well-being. The study identified that certain sociodemographic factors, namely marital status and educational attainment, are significantly associated with perceived social support and psychological well-being.
The positive correlation between social support and mental health underscores the critical importance of robust support systems for hemodialysis patients. Healthcare providers play a pivotal role in fostering mental health among these individuals. This study demonstrates that patients who receive adequate social support from various sources, including healthcare providers, family, and friends, are better equipped to manage their chronic illness and maintain a higher QoL.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Research Ethics Committee of the College of Nursing, University of Kirkuk, Kirkuk, Iraq on November 24, 2024 (Code: 8).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, investigation, writing the original draft, data collection and data analysis: Sumaya Ali Aqeel; Supervision, methodology, review & editing: Abbas Lateef Muhe-Aldeen.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their sincere gratitude to the staff of the Al-Amal Dialysis Center in Kirkuk City for their invaluable cooperation and support in facilitating data collection.
References
- Noce A, Marrone G, Urciuoli S, Di Daniele F, Di Lauro M, Pietroboni Zaitseva A, et al. Usefulness of extra virgin olive oil minor polar compounds in the management of chronic kidney disease patients. Nutrients. 2021; 13(2):581. [DOI:10.3390/nu13020581] [PMID]
- Alemayehu YH, Seylania K, Bahramnezhad F. The relationship between health literacy and quality of life among hemodialysis patients: An integrative review. Human Antibodies. 2020; 28(1):75-81. [DOI:10.3233/HAB-190394] [PMID]
- Abd HA, Ahmed AMK. Quantitative determination of trace elements (Zn, Cu, and Mg) in serum for chronic renal failure using graphite furnace atomic absorption (GFAAS). Pakistan Journal of Life and Social Sciences. 2024; 22(1):1679-87. [DOI:10.57239/PJLSS-2024-22.1.00117]
- Shawkat EA, Abdulrahman SJ, Bakr BA. Assessment the role of erythropoietin, hepcidin and albumin in patients with chronic kidney disease in Kirkuk-Iraq. Kirkuk Journal of Science. 2023; 18(3):7-12. [DOI:10.32894/kujss.2023.141071.1104]
- Muhe-Aldeen AL, Shakor JA, Mustafa DY. Post-traumatic stress disorders among cancer patients in Kirkuk City. Indian Journal of Public Health Research and Development. 2019; 10(2):951. [DOI:10.5958/0976-5506.2019.00419.4]
- Sanyaolu A, Okorie C, Annan R, Turkey H, Akhtar N, Gray F, et al. Epidemiology and management of chronic renal failure: A global public health problem. Biostatistics Epidemiology International Journal. 2020; 1(1):13-8. [Link]
- Muhaldeen FF, Raoof AA. SARS-CoV-2 related morbidity and mortality in patients undergoing hemodialysis at The Kirkuk Hemodialysis Center. Kirkuk Journal of Medical Sciences. 2024; 12(1):49-54. [DOI:10.32894/kjms.2024.144739.1080]
- Kerr M, Jaure A, Stephens JH, Kim S, Cutler R, Cashmore B, et al. Experiences of indigenous patients receiving dialysis: Systematic review of qualitative studies. American Journal of Kidney Diseases. 2023; 83(2):139-50. [DOI:10.1053/j.ajkd.2023.07.014] [PMID]
- Grevenstein D, Bluemke M, Schweitzer J, Aguilar-Raab C. Better family relationships-higher well-being: The connection between relationship quality and health related resources. Mental Health & Prevention. 2019; 14:200160. [DOI:10.1016/j.mph.2019.200160]
- Pan KC, Hung SY, Chen CI, Lu CY, Shih ML, Huang CY. Social support as a mediator between sleep disturbances, depressive symptoms, and health-related quality of life in patients undergoing hemodialysis. Plos One. 2019; 14(4):e0216045. [DOI:10.1371/journal.pone.0216045] [PMID]
- Thong MS, Kaptein AA, Krediet RT, Boeschoten EW, Dekker FW. Social support predicts survival in dialysis patients. Nephrology, Dialysis, Transplantation. 2019; 22(3):847-52. [DOI:10.1093/ndt/gfl700] [PMID]
- Williams P, Goldberg DP. A user’s guide to the General Health Questionnaire. Berkshire: NFER, Nelson; 1988. [Link]
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. Journal of Personality Assessment. 1988; 52(1):30-41. [DOI:10.1207/s15327752jpa5201_2]
- Rhee CM, Zhou M, Woznick R, Mullon C, Anger MS, Ficociello LH. A real-world analysis of the influence of age on maintenance hemodialysis patients: Managing serum phosphorus with sucroferric oxyhydroxide as part of routine clinical care. International Urology and Nephrology. 2022; 55(2):377-87. [DOI:10.1007/s11255-022-03327-w] [PMID]
- Hassani F, Zarea K, Gholamzadeh Jofreh M, Dashtebozorgi Z, Chan SWC. Effect of perceived social support, spiritual well-being, health literacy, and resilience on quality of life in patients undergoing hemodialysis: A structural equation model. Jundishapur Journal of Chronic Disease Care. 2022; 11(2):e123080. [DOI:10.5812/jjcdc.123080]
- Mazdeh M, Nozari B, Hatmi Z, Zamyadi M, Mahdavi A. The impact of gender and marital status on therapeutic outcomes of maintenance hemodialysis patients. Nephro-Urology Monthly. 2009; 1(2):124-8. [Link]
- Opiyo RO, Nyasulu PS, Olenja J, Zunza M, Nguyen KA, Bukania Z, et al. Factors associated with adherence to dietary prescription among adult patients with chronic kidney disease on hemodialysis in national referral hospitals in Kenya: A mixed-methods survey. Renal Replacement Therapy. 2019; 5(1):s41100-019-0237-4. [DOI:10.1186/s41100-019-0237-4] [PMID]
- Abdullah Mohammed A, Salah Mohammad Salih H. Effectiveness of nutritional instructional program on knowledge among hemodialysis patients in Kirkuk general hospital. Migration Letters. 2023; 20(S2):206-11. [Link]
- Kirkeskov L, Carlsen RK, Lund T, Buus NH. Employment of patients with kidney failure treated with dialysis or kidney transplantation-A systematic review and meta-analysis. BMC Nephrology. 2021; 22(1):348. [DOI:10.1186/s12882-021-02552-2] [PMID]
- Jankowska-Polanska B, Uchmanowicz I, Wysocka A, Uchmanowicz B, Lomper K, Fal AM. Factors affecting the quality of life of chronic dialysis patients. European Journal of Public Health. 2017; 27(2):262-7. [DOI:10.1093/eurpub/ckw193] [PMID]
- AlRowaie F, Alaryni A, AlGhamdi A, Alajlan R, Alabdullah R, Alnutaifi R, et al. Quality of life among peritoneal and hemodialysis patients: A cross-sectional study. Clinics and Practice. 2023; 13(5):1215-26. [DOI:10.3390/clinpract13050109] [PMID]
- Betiru EA, Mamo E, Boneya DJ, Adem A, Abebaw D. Survival analysis and its predictors among hemodialysis patients at Saint Paul hospital millennium medical college and myungsung christian medical center in Addis Ababa, Ethiopia, 2021. International Journal of Nephrology and Renovascular Disease. 2023; 16:59-71. [DOI:10.2147/IJNRD.S401022] [PMID]
- Rayner HC, Zepel L, Fuller DS, Morgenstern H, Karaboyas A, Culleton BF, et al. Recovery time, quality of life, and mortality in hemodialysis patients: The dialysis outcomes and practice patterns study (DOPPS). American Journal of Kidney Diseases. 2014; 64(1):86-94. [DOI:10.1053/j.ajkd.2014.01.014]
- Hu L, Wang Z, He X. Hemodialysis dose and frequency should be considered in subgroup analysis. Cardiovascular Diabetology. 2024; 23(1):416. [DOI:10.1186/s12933-024-02482-x] [PMID]
- Erickson SJ, Yabes JG, Han Z, Roumelioti ME, Rollman BL, Weisbord SD, et al. Associations between Social Support and Patient-Reported Outcomes in Patients Receiving Hemodialysis: Results from the TACcare Study. Kidney360. 2024; 5(6):860-9. [DOI:10.34067/KID.0000000000000456] [PMID]
- Ozdemir N. The relationship between perceived social support, psychological resilience and happiness levels of hemodialysis patients. Annals of Medical Research. 2019; 26(10):2286. [DOI:10.5455/annalsmedres.2019.09.523]
- Sułkowski L, Matyja A, Matyja M. Social support and quality of life in hemodialysis patients: A comparative study with healthy controls. Medicina. 2024; 60(11):1732. [DOI:10.3390/medicina60111732] [PMID]
- Karami H, Rahmati M, Abbasi P. Investigating the relationship between perceived social support and resilience in patients undergoing hemodialysis: A cross-sectional study. BMC Nephrology. 2025; 26(1):278. [DOI:10.1186/s12882-025-04204-1] [PMID]
Article type: Original Research Articles |
Subject:
Social Welfare
Received: 2025/07/10 | Accepted: 2025/08/16 | Published: 2025/12/1
Received: 2025/07/10 | Accepted: 2025/08/16 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
