
988368
Thu, Jul 30, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 399-406 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hrefish Z A, Mohammed S H. Mental Health Literacy as a Mediator Between Stigma Among Caregivers and Medication Adherence of Psychotic Patients. Iranian Rehabilitation Journal 2025; 23 (4) :399-406
URL: http://irj.uswr.ac.ir/article-1-2602-en.html
URL: http://irj.uswr.ac.ir/article-1-2602-en.html



1- Department of Psychiatry and Mental Health Nursing, College of Nursing, University of Babylon, Babylon, Iraq.
Keywords: Mental health literacy (MHL), Caregiver stigma, Treatment adherence, Psychotic illnesses, Psychoeducation
Full-Text [PDF 542 kb]
(534 Downloads)
| Abstract (HTML) (2313 Views)
Full-Text: (311 Views)
Introduction
Psychotic illnesses, including schizophrenia and schizoaffective disorders, present profound challenges to patients, families, and healthcare systems. One of the most critical components in the management of psychotic disorders is ensuring consistent medication adherence, which is often disrupted by various psychosocial factors [1]. Research indicates that non-adherence to antipsychotic medications is prevalent, with rates ranging from 40% to 60% globally, leading to relapse, hospitalization, and worsening functional outcomes [2]. Caregivers play a crucial role in supporting adherence, especially when patients have limited insight or experience cognitive impairments. However, their attitudes, knowledge, and beliefs, particularly surrounding mental illness, can substantially influence treatment outcomes [3, 4].
Stigma is as a key obstacle among the many barriers to medication adherence. Caregivers may internalize societal stigma or experience public stigma due to their association with individuals diagnosed with psychotic illnesses. This “affiliate stigma” can cause psychological distress and lead to passive or avoidant care behaviors, ultimately undermining patient adherence [5]. Previous research studies have documented that caregivers experiencing higher levels of stigma often feel shame, reduce help-seeking behaviors, and may distance themselves from the patient, further weakening the support system necessary for long-term treatment compliance [6, 7]. In addition, stigma often correlates with misinformation and poor understanding of psychiatric conditions, thereby increasing the likelihood of negative caregiving outcomes [8].
Emerging literature suggests that mental health literacy (MHL) may be as a protective mediator in this dynamic. MHL refers to knowledge and beliefs about mental disorders that aid recognition, management, and prevention [9, 10]. Caregivers with higher MHL are more likely to adopt supportive, informed, and proactive attitudes toward their caregiving roles. Evidence shows that MHL reduces the impact of stigma and promotes help-seeking behavior, early identification of symptoms, and increased treatment compliance [11, 12]. Furthermore, MHL interventions have demonstrated measurable improvements in caregiver well-being and patient adherence among psychiatric populations [13].
Despite the growing body of research on the roles of stigma and MHL, few studies have explored how MHL mediates the relationship between caregiver stigma and patient medication adherence [13, 14]. Understanding this mediation pathway is critical for developing targeted educational and anti-stigma interventions. If MHL can buffer the adverse effects of caregiver stigma on adherence, public health efforts should prioritize mental health education as a strategic tool for improving psychiatric outcomes. Therefore, this study aimed to investigate the mediating role of MHL in the relationship between stigma among caregivers and medication adherence in patients with psychotic illnesses.
Materials and Methods
Study design and sitting
This study employed a cross-sectional, descriptive-correlational design to investigate the influence of MHL on the medication adherence of patients with psychotic illnesses. The research was conducted at a specialized psychiatric center in Baghdad City, Iraq, between March 1, 2025, and June 30, 2025. This center was selected due to its central role in providing outpatient psychiatric services and ongoing medication management for patients with chronic mental disorders, particularly those diagnosed with psychotic conditions. The location also served a demographically diverse population, making it suitable for exploring variations in caregiver literacy and patient adherence behaviors.
Study sample
A total of 150 caregivers participated in this study. The sample size was determined based on resource feasibility and the expected number of eligible participants during the data collection period. Participants were selected through purposive sampling, targeting primary informal caregivers of patients diagnosed with psychotic disorders, such as schizophrenia and schizoaffective disorder. Caregivers were eligible if they were aged 18 years or older, had been providing care for at least three months, could communicate in Arabic, and were able to provide informed consent. Caregivers were excluded if they had a diagnosed psychiatric illness that could interfere with their ability to respond accurately or if the patient under their care had a co-occurring substance use disorder, which might confound adherence patterns.
Study instruments
The first part of the tool was a demographic and clinical data questionnaire, developed by the researchers to collect background information on both caregivers and patients. The variables included caregiver age, gender, education level, relationship with the patient, and duration of caregiving, as well as patient diagnosis, illness duration, and frequency of clinical follow-up. Three validated instruments were used in this study:
To assess the relationship between caregivers’ stigma, MHL, and medication adherence among patients with psychotic illnesses, three validated instruments were employed. The MHL scale (MHLS), developed by O’Connor and Casey, is a 35-item tool used to evaluate knowledge and beliefs about mental disorders, including disorder recognition, risk factors, and help-seeking attitudes. This tool has demonstrated reliability in prior studies, with a Cronbach’s α of 0.88 [15]. The Arabic version used in this study was culturally adapted using standard forward–backward translation procedures and reviewed by mental health experts, showing excellent internal consistency (Cronbach’s α=0.87) in the pilot test.
The second instrument was the medication adherence rating scale (MARS), a 10-item scale originally developed by Thompson et al. to assess medication adherence behavior in psychiatric populations. This scale includes items on both behavior and attitudes toward medication and has shown high reliability in previous research, with a Cronbach’s α of 0.84 [16]. In the current study, caregivers completed the MARS to report observed patient medication behaviors. The Arabic version was previously validated and yielded strong reliability (intraclass correlation coefficient [ICC]=0.85) in the current context.
The third tool, the caregivers’ perceived stigma scale (CPMI), was utilized to measure the stigma experienced by caregivers of individuals with mental illness. This 22-item scale, adapted from the original tool by Chang et al. and modified for caregivers, covers domains such as discrimination, social withdrawal, and emotional burden. The tool has been previously validated, showing high reliability (Cronbach’s α=0.9) [17]. The Arabic version used in this study was translated and validated by a panel of bilingual mental health professionals. It demonstrated good internal consistency (Cronbach’s α=0.89) and stability (ICC=0.88) during the pilot testing phase.
Validity and reliability
To ensure linguistic and cultural relevance, all scales were translated into Arabic using the forward–backward translation method by bilingual mental health professionals. The translated instruments were reviewed by a panel of five experts in psychiatric nursing and psychology to ensure conceptual clarity and content validity. A pilot study was conducted with 30 caregivers who were not part of the final sample to evaluate the clarity, feasibility, and reliability. The pilot results demonstrated strong internal consistency for both the MHLS (Cronbach’s α=0.88) and MARS (Cronbach’s α=0.84), indicating the instruments were appropriate for use in the Iraqi caregiver population.
Data collection
Data were collected over four months during routine outpatient visits. Literate participants completed the questionnaires independently in a quiet room at the psychiatric center. At the same time, those with limited literacy received interviewer-administered surveys conducted by trained psychiatric nurses using a standardized script. Each session lasted approximately 20–30 minutes. Written informed consent was obtained from all participants prior to data collection. This study was approved by the Scientific Research Ethics Committee of the College of Nursing, University of Baghdad. Participants were assured of confidentiality, voluntary participation, and the right to withdraw from the study at any time without any impact on their or their patient’s care.
Data analysis
Data were analyzed using SPSS software, version version 27. Descriptive statistics, including frequencies, percentages, Mean±SD, were used to summarize the socio-demographic characteristics of caregivers and patients. Pearson’s correlation coefficient was employed to examine the relationships between caregiver stigma, MHL, and medication adherence. Multiple linear regression analysis was conducted to identify significant predictors of medication adherence, controlling for caregiver education levels. To assess the mediating role of MHL between stigma and medication adherence, a mediation analysis was performed using the bootstrapping method with 5000 samples to calculate the indirect effect and its 95% confidence interval (CI). The Sobel test was also applied to verify the significance of the mediation effect. Statistical significance was set at P<0.05 for all analyses.
Results
The study sample included 150 caregivers, and Table 1 showed that the average age was 51.49±13.35 years. Age groups were distributed as follows: 20–29 years (17.3%), 30–39 years (25.3%), 40–49 years (28%), 50–59 years (16%), and 60+ years (13.4%). Females comprised a slight majority (54.7%) compared to males (45.3%). Regarding education, most caregivers had a secondary school diploma or higher, with 22.7% secondary school, 20% diploma, 24% bachelor’s degree, and 13.3% postgraduate studies; 8% were illiterate, and 12% literate. Most caregivers were married (65.3%), while 20% were single, 5.3% separated, and 9.3% widowed. Housewives represented the largest group (38.7%), followed by employees (18.7%), students (14.7%), self-employed individuals (16%), and retired individuals (12%). Most lived in urban (60%) rather than rural areas (40%).
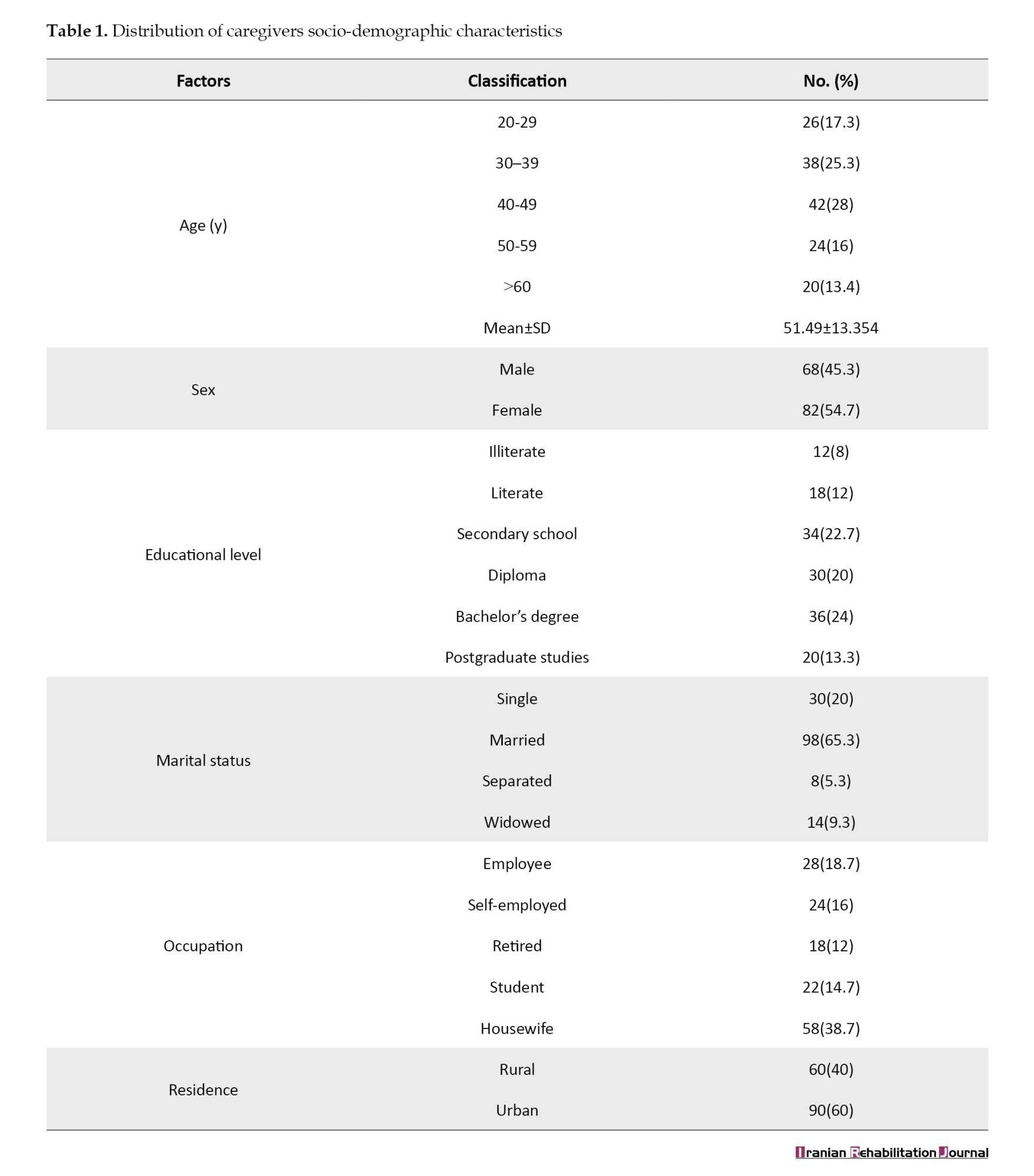
Table 2 presents the Pearson correlation coefficients between stigma, MHL, and medication adherence. The results indicated a significant negative correlation between stigma and both MHL (r=-0.48, P<0.01) and medication adherence (r=-0.52, P<0.01), suggesting that as perceived stigma increases, both mental health knowledge and adherence to medication decrease. Conversely, a strong positive correlation was found between MHL and medication adherence (r=0.58, P<0.01), indicating that caregivers with higher MHL are more likely to support better adherence to treatment among patients with psychotic illnesses.
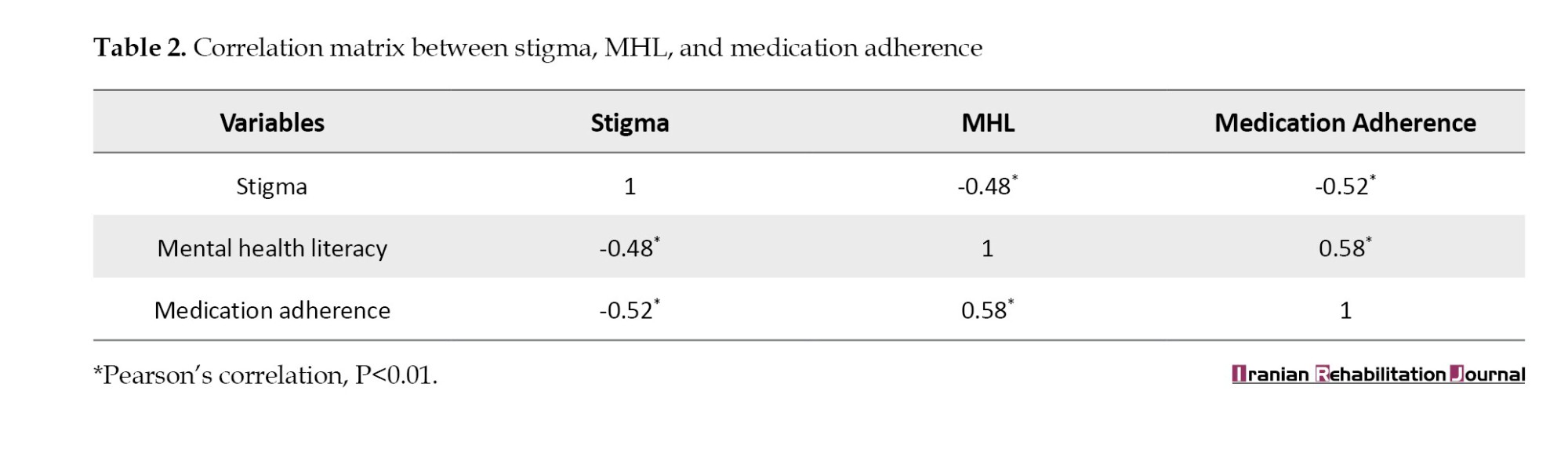
Table 3 presents the results of a multiple regression analysis examining the predictors of medication adherence. MHL (B=0.42, P<0.001) emerged as a strong positive predictor, while stigma (B=-0.31, P<0.001) was a significant negative predictor of adherence. Additionally, caregiver education levels showed a notable influence: those with secondary education (B=0.18, P=0.048) and those with a bachelor’s degree or higher (B=0.29, P=0.004) were more likely to promote higher adherence compared to illiterate caregivers. The model explained 46% of the variance in adherence (R²=0.46), and the overall model was statistically significant (F4, 145=31.04, P<0.001), highlighting the critical role of both literacy and stigma in shaping medication-taking behavior.
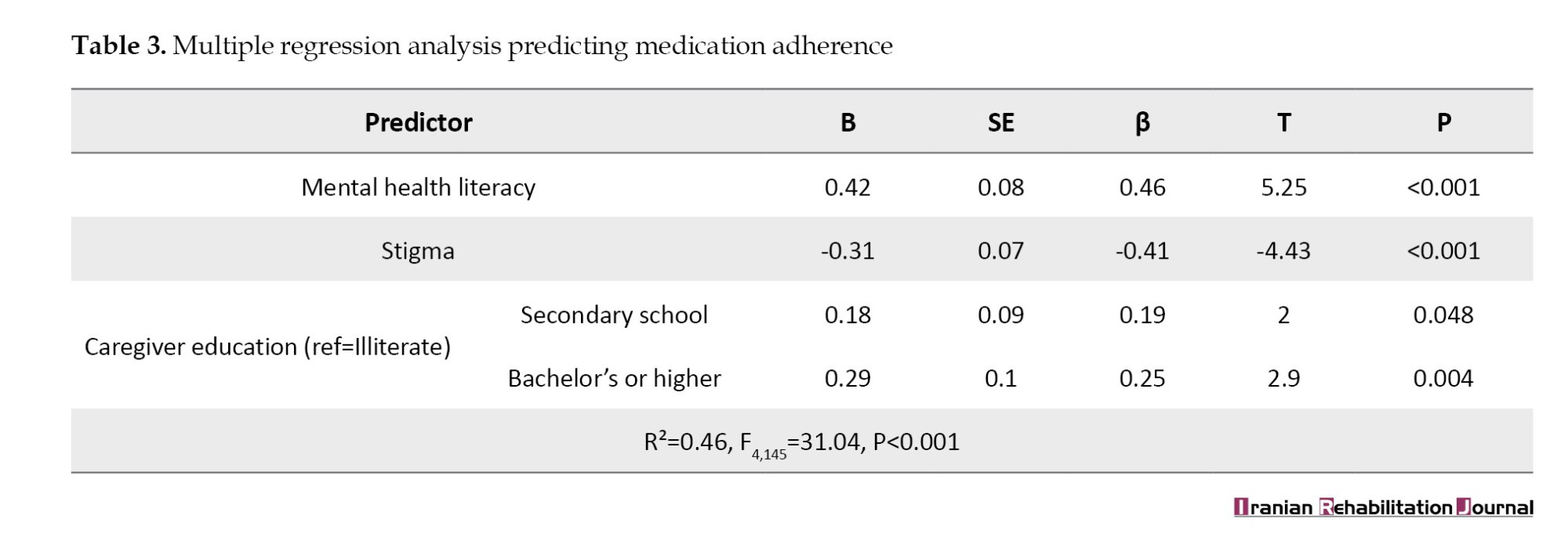
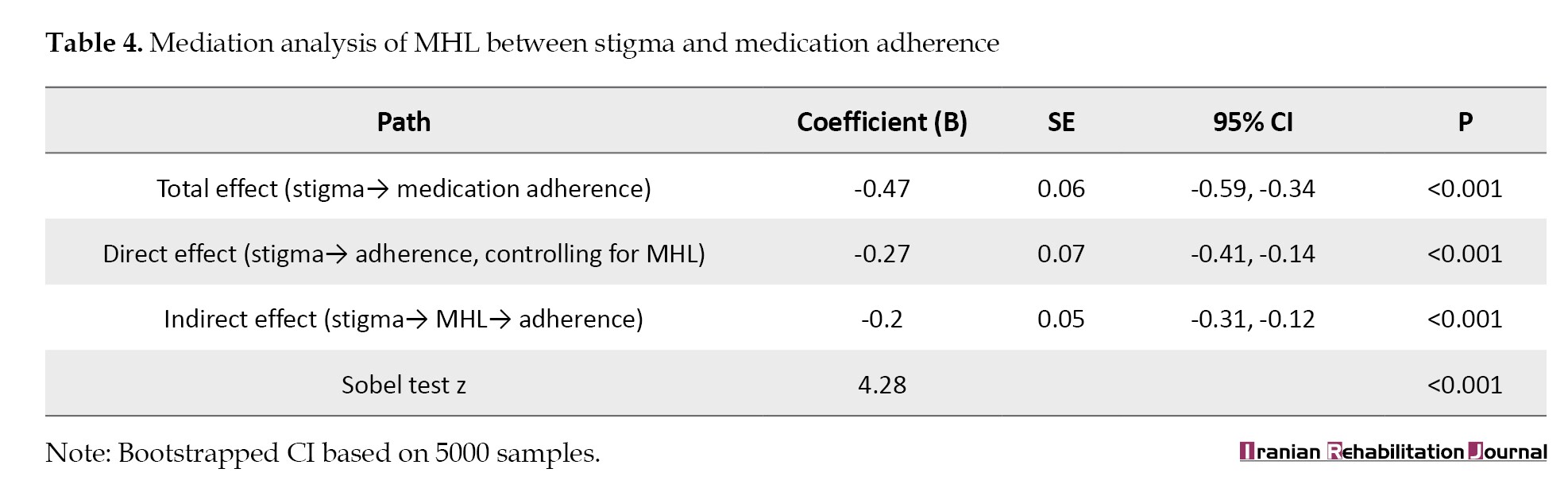
Table 4 presents a mediation analysis investigating whether MHL mediates the relationship between stigma and medication adherence. The total effect of stigma on adherence was significant and negative (B=-0.47, P<0.001). When MHL was included in the model, the direct effect of stigma was reduced but remained significant (B=-0.27, P<0.001), indicating partial mediation. The indirect effect of MHL was also significant (B=-0.2, 95% CI, -0.31%, -0.12%, P<0.001), supported by a significant Sobel test (z=4.28, P<0.001).
Discussion
Understanding the demographic profile of caregivers provides crucial context for interpreting the dynamics of stigma, MHL, and medication adherence. In this study, most caregivers were middle-aged females, with a substantial portion possessing secondary education or higher. This is consistent with previous research indicating that caregiving roles, especially in mental health contexts, are often assumed by middle-aged women with a moderate level of education [18, 19]. These sociodemographic factors can influence health beliefs, perceptions of stigma, and the ability to process mental health information [20].
Correlation analysis demonstrated that stigma was significantly and negatively associated with both MHL and medication adherence. This finding aligns with prior studies showing that high levels of stigma among caregivers can impede the acquisition of mental health knowledge and diminish their motivation or ability to support consistent medication use in psychotic patients [21, 22]. Conversely, MHL was positively correlated with medication adherence, suggesting that more knowledgeable caregivers are better equipped to understand psychiatric conditions and the importance of treatment adherence. This supports evidence from Lee et al. who emphasized that higher MHL is associated with improved care behaviors and health outcomes in psychiatric populations [23].
Regression analysis further reinforced these relationships. MHL emerged as a robust predictor of medication adherence, even after controlling for stigma and education. This aligns with the theory of planned behavior, which posits that knowledge and attitudes influence intentions and actions [24, 25]. Furthermore, the negative predictive role of stigma on adherence corroborates a body of literature suggesting that stigma contributes to avoidance, denial, or resentment toward psychiatric interventions among caregivers and patients [26, 27]. Importantly, caregiver education significantly predicted adherence, suggesting that educational attainment enhances the caregivers’ ability to process and implement health-related knowledge [28-30].
The mediation analysis confirmed that MHL significantly mediated the relationship between caregiver stigma and medication adherence. This indicates that stigma can impair medication adherence partly by reducing caregivers’ understanding of mental health. This pathway reflects the cognitive-behavioral model of stigma, which suggests that negative attitudes (stigma) reduce knowledge-seeking behavior (MHL), ultimately undermining caregiving efficacy. The partial mediation observed supports previous mediation models, such as that of O’Connor et al. who found that enhancing caregiver knowledge reduced the detrimental effects of stigma on treatment engagement [15].
Nevertheless, stigma retained a significant direct effect on adherence even after accounting for MHL, indicating that its influence extends beyond knowledge-related mechanisms. Stigma may also operate through emotional and psychological pathways; it can induce shame, social withdrawal, and distress in caregivers, which in turn erodes their confidence and self-efficacy in maintaining consistent care practices. Cognitive-behavioral perspectives suggest that these negative self-appraisals and emotions reinforce avoidance behaviors and reduce engagement with treatment, independently of literacy levels. Thus, while improving MHL is crucial, interventions solely targeting knowledge may be insufficient. Holistic approaches that integrate stigma-reduction strategies, emotional support, and caregiver empowerment programs are needed to address both the cognitive and affective dimensions of stigma and thereby maximize adherence [15].
Conclusion
The findings of this study conclude that MHL plays a significant mediating role in the relationship between caregiver stigma and medication adherence among patients with psychotic illnesses. Higher caregiver stigma levels were associated with reduced MHL and, subsequently, lower treatment adherence. Conversely, caregivers with greater MHL significantly supported better medication adherence, highlighting its pivotal role in improving treatment outcomes. These results underscore the importance of reducing stigma and enhancing MHL through targeted educational interventions. Healthcare systems should integrate caregiver-focused psychoeducation programs to improve understanding of psychotic disorders and reduce stigma-related barriers to treatment adherence.
Study limitation
This study has several limitations. First, its cross-sectional design limits the ability to infer causality between variables. Second, data were collected through self-reported questionnaires, which may be subject to social desirability and recall biases. Third, the sample was drawn from a single geographic region, potentially limiting the generalizability of the findings to the broader population. Finally, this study did not account for clinical severity or duration of illness, which may influence medication adherence and caregiver perceptions.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Research Ethics Committee of the College of Nursing, University of Babylon (No.: 78: dated 24/3/2025). The Health Authority of Baghdad/Baghdad Health Directorate, Iraq, approved all experimental protocols. During data collection, all permitted guidelines were adhered to.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, and data collection: Zaman Ahmed Hrefish; Writing the original draft: All authors; Data analysis, review and editing: Saja Hashem Mohammed.
Conflict of interest
The authors declared no conflict of interest.
References
Psychotic illnesses, including schizophrenia and schizoaffective disorders, present profound challenges to patients, families, and healthcare systems. One of the most critical components in the management of psychotic disorders is ensuring consistent medication adherence, which is often disrupted by various psychosocial factors [1]. Research indicates that non-adherence to antipsychotic medications is prevalent, with rates ranging from 40% to 60% globally, leading to relapse, hospitalization, and worsening functional outcomes [2]. Caregivers play a crucial role in supporting adherence, especially when patients have limited insight or experience cognitive impairments. However, their attitudes, knowledge, and beliefs, particularly surrounding mental illness, can substantially influence treatment outcomes [3, 4].
Stigma is as a key obstacle among the many barriers to medication adherence. Caregivers may internalize societal stigma or experience public stigma due to their association with individuals diagnosed with psychotic illnesses. This “affiliate stigma” can cause psychological distress and lead to passive or avoidant care behaviors, ultimately undermining patient adherence [5]. Previous research studies have documented that caregivers experiencing higher levels of stigma often feel shame, reduce help-seeking behaviors, and may distance themselves from the patient, further weakening the support system necessary for long-term treatment compliance [6, 7]. In addition, stigma often correlates with misinformation and poor understanding of psychiatric conditions, thereby increasing the likelihood of negative caregiving outcomes [8].
Emerging literature suggests that mental health literacy (MHL) may be as a protective mediator in this dynamic. MHL refers to knowledge and beliefs about mental disorders that aid recognition, management, and prevention [9, 10]. Caregivers with higher MHL are more likely to adopt supportive, informed, and proactive attitudes toward their caregiving roles. Evidence shows that MHL reduces the impact of stigma and promotes help-seeking behavior, early identification of symptoms, and increased treatment compliance [11, 12]. Furthermore, MHL interventions have demonstrated measurable improvements in caregiver well-being and patient adherence among psychiatric populations [13].
Despite the growing body of research on the roles of stigma and MHL, few studies have explored how MHL mediates the relationship between caregiver stigma and patient medication adherence [13, 14]. Understanding this mediation pathway is critical for developing targeted educational and anti-stigma interventions. If MHL can buffer the adverse effects of caregiver stigma on adherence, public health efforts should prioritize mental health education as a strategic tool for improving psychiatric outcomes. Therefore, this study aimed to investigate the mediating role of MHL in the relationship between stigma among caregivers and medication adherence in patients with psychotic illnesses.
Materials and Methods
Study design and sitting
This study employed a cross-sectional, descriptive-correlational design to investigate the influence of MHL on the medication adherence of patients with psychotic illnesses. The research was conducted at a specialized psychiatric center in Baghdad City, Iraq, between March 1, 2025, and June 30, 2025. This center was selected due to its central role in providing outpatient psychiatric services and ongoing medication management for patients with chronic mental disorders, particularly those diagnosed with psychotic conditions. The location also served a demographically diverse population, making it suitable for exploring variations in caregiver literacy and patient adherence behaviors.
Study sample
A total of 150 caregivers participated in this study. The sample size was determined based on resource feasibility and the expected number of eligible participants during the data collection period. Participants were selected through purposive sampling, targeting primary informal caregivers of patients diagnosed with psychotic disorders, such as schizophrenia and schizoaffective disorder. Caregivers were eligible if they were aged 18 years or older, had been providing care for at least three months, could communicate in Arabic, and were able to provide informed consent. Caregivers were excluded if they had a diagnosed psychiatric illness that could interfere with their ability to respond accurately or if the patient under their care had a co-occurring substance use disorder, which might confound adherence patterns.
Study instruments
The first part of the tool was a demographic and clinical data questionnaire, developed by the researchers to collect background information on both caregivers and patients. The variables included caregiver age, gender, education level, relationship with the patient, and duration of caregiving, as well as patient diagnosis, illness duration, and frequency of clinical follow-up. Three validated instruments were used in this study:
To assess the relationship between caregivers’ stigma, MHL, and medication adherence among patients with psychotic illnesses, three validated instruments were employed. The MHL scale (MHLS), developed by O’Connor and Casey, is a 35-item tool used to evaluate knowledge and beliefs about mental disorders, including disorder recognition, risk factors, and help-seeking attitudes. This tool has demonstrated reliability in prior studies, with a Cronbach’s α of 0.88 [15]. The Arabic version used in this study was culturally adapted using standard forward–backward translation procedures and reviewed by mental health experts, showing excellent internal consistency (Cronbach’s α=0.87) in the pilot test.
The second instrument was the medication adherence rating scale (MARS), a 10-item scale originally developed by Thompson et al. to assess medication adherence behavior in psychiatric populations. This scale includes items on both behavior and attitudes toward medication and has shown high reliability in previous research, with a Cronbach’s α of 0.84 [16]. In the current study, caregivers completed the MARS to report observed patient medication behaviors. The Arabic version was previously validated and yielded strong reliability (intraclass correlation coefficient [ICC]=0.85) in the current context.
The third tool, the caregivers’ perceived stigma scale (CPMI), was utilized to measure the stigma experienced by caregivers of individuals with mental illness. This 22-item scale, adapted from the original tool by Chang et al. and modified for caregivers, covers domains such as discrimination, social withdrawal, and emotional burden. The tool has been previously validated, showing high reliability (Cronbach’s α=0.9) [17]. The Arabic version used in this study was translated and validated by a panel of bilingual mental health professionals. It demonstrated good internal consistency (Cronbach’s α=0.89) and stability (ICC=0.88) during the pilot testing phase.
Validity and reliability
To ensure linguistic and cultural relevance, all scales were translated into Arabic using the forward–backward translation method by bilingual mental health professionals. The translated instruments were reviewed by a panel of five experts in psychiatric nursing and psychology to ensure conceptual clarity and content validity. A pilot study was conducted with 30 caregivers who were not part of the final sample to evaluate the clarity, feasibility, and reliability. The pilot results demonstrated strong internal consistency for both the MHLS (Cronbach’s α=0.88) and MARS (Cronbach’s α=0.84), indicating the instruments were appropriate for use in the Iraqi caregiver population.
Data collection
Data were collected over four months during routine outpatient visits. Literate participants completed the questionnaires independently in a quiet room at the psychiatric center. At the same time, those with limited literacy received interviewer-administered surveys conducted by trained psychiatric nurses using a standardized script. Each session lasted approximately 20–30 minutes. Written informed consent was obtained from all participants prior to data collection. This study was approved by the Scientific Research Ethics Committee of the College of Nursing, University of Baghdad. Participants were assured of confidentiality, voluntary participation, and the right to withdraw from the study at any time without any impact on their or their patient’s care.
Data analysis
Data were analyzed using SPSS software, version version 27. Descriptive statistics, including frequencies, percentages, Mean±SD, were used to summarize the socio-demographic characteristics of caregivers and patients. Pearson’s correlation coefficient was employed to examine the relationships between caregiver stigma, MHL, and medication adherence. Multiple linear regression analysis was conducted to identify significant predictors of medication adherence, controlling for caregiver education levels. To assess the mediating role of MHL between stigma and medication adherence, a mediation analysis was performed using the bootstrapping method with 5000 samples to calculate the indirect effect and its 95% confidence interval (CI). The Sobel test was also applied to verify the significance of the mediation effect. Statistical significance was set at P<0.05 for all analyses.
Results
The study sample included 150 caregivers, and Table 1 showed that the average age was 51.49±13.35 years. Age groups were distributed as follows: 20–29 years (17.3%), 30–39 years (25.3%), 40–49 years (28%), 50–59 years (16%), and 60+ years (13.4%). Females comprised a slight majority (54.7%) compared to males (45.3%). Regarding education, most caregivers had a secondary school diploma or higher, with 22.7% secondary school, 20% diploma, 24% bachelor’s degree, and 13.3% postgraduate studies; 8% were illiterate, and 12% literate. Most caregivers were married (65.3%), while 20% were single, 5.3% separated, and 9.3% widowed. Housewives represented the largest group (38.7%), followed by employees (18.7%), students (14.7%), self-employed individuals (16%), and retired individuals (12%). Most lived in urban (60%) rather than rural areas (40%).
Table 2 presents the Pearson correlation coefficients between stigma, MHL, and medication adherence. The results indicated a significant negative correlation between stigma and both MHL (r=-0.48, P<0.01) and medication adherence (r=-0.52, P<0.01), suggesting that as perceived stigma increases, both mental health knowledge and adherence to medication decrease. Conversely, a strong positive correlation was found between MHL and medication adherence (r=0.58, P<0.01), indicating that caregivers with higher MHL are more likely to support better adherence to treatment among patients with psychotic illnesses.
Table 3 presents the results of a multiple regression analysis examining the predictors of medication adherence. MHL (B=0.42, P<0.001) emerged as a strong positive predictor, while stigma (B=-0.31, P<0.001) was a significant negative predictor of adherence. Additionally, caregiver education levels showed a notable influence: those with secondary education (B=0.18, P=0.048) and those with a bachelor’s degree or higher (B=0.29, P=0.004) were more likely to promote higher adherence compared to illiterate caregivers. The model explained 46% of the variance in adherence (R²=0.46), and the overall model was statistically significant (F4, 145=31.04, P<0.001), highlighting the critical role of both literacy and stigma in shaping medication-taking behavior.
Table 4 presents a mediation analysis investigating whether MHL mediates the relationship between stigma and medication adherence. The total effect of stigma on adherence was significant and negative (B=-0.47, P<0.001). When MHL was included in the model, the direct effect of stigma was reduced but remained significant (B=-0.27, P<0.001), indicating partial mediation. The indirect effect of MHL was also significant (B=-0.2, 95% CI, -0.31%, -0.12%, P<0.001), supported by a significant Sobel test (z=4.28, P<0.001).
Discussion
Understanding the demographic profile of caregivers provides crucial context for interpreting the dynamics of stigma, MHL, and medication adherence. In this study, most caregivers were middle-aged females, with a substantial portion possessing secondary education or higher. This is consistent with previous research indicating that caregiving roles, especially in mental health contexts, are often assumed by middle-aged women with a moderate level of education [18, 19]. These sociodemographic factors can influence health beliefs, perceptions of stigma, and the ability to process mental health information [20].
Correlation analysis demonstrated that stigma was significantly and negatively associated with both MHL and medication adherence. This finding aligns with prior studies showing that high levels of stigma among caregivers can impede the acquisition of mental health knowledge and diminish their motivation or ability to support consistent medication use in psychotic patients [21, 22]. Conversely, MHL was positively correlated with medication adherence, suggesting that more knowledgeable caregivers are better equipped to understand psychiatric conditions and the importance of treatment adherence. This supports evidence from Lee et al. who emphasized that higher MHL is associated with improved care behaviors and health outcomes in psychiatric populations [23].
Regression analysis further reinforced these relationships. MHL emerged as a robust predictor of medication adherence, even after controlling for stigma and education. This aligns with the theory of planned behavior, which posits that knowledge and attitudes influence intentions and actions [24, 25]. Furthermore, the negative predictive role of stigma on adherence corroborates a body of literature suggesting that stigma contributes to avoidance, denial, or resentment toward psychiatric interventions among caregivers and patients [26, 27]. Importantly, caregiver education significantly predicted adherence, suggesting that educational attainment enhances the caregivers’ ability to process and implement health-related knowledge [28-30].
The mediation analysis confirmed that MHL significantly mediated the relationship between caregiver stigma and medication adherence. This indicates that stigma can impair medication adherence partly by reducing caregivers’ understanding of mental health. This pathway reflects the cognitive-behavioral model of stigma, which suggests that negative attitudes (stigma) reduce knowledge-seeking behavior (MHL), ultimately undermining caregiving efficacy. The partial mediation observed supports previous mediation models, such as that of O’Connor et al. who found that enhancing caregiver knowledge reduced the detrimental effects of stigma on treatment engagement [15].
Nevertheless, stigma retained a significant direct effect on adherence even after accounting for MHL, indicating that its influence extends beyond knowledge-related mechanisms. Stigma may also operate through emotional and psychological pathways; it can induce shame, social withdrawal, and distress in caregivers, which in turn erodes their confidence and self-efficacy in maintaining consistent care practices. Cognitive-behavioral perspectives suggest that these negative self-appraisals and emotions reinforce avoidance behaviors and reduce engagement with treatment, independently of literacy levels. Thus, while improving MHL is crucial, interventions solely targeting knowledge may be insufficient. Holistic approaches that integrate stigma-reduction strategies, emotional support, and caregiver empowerment programs are needed to address both the cognitive and affective dimensions of stigma and thereby maximize adherence [15].
Conclusion
The findings of this study conclude that MHL plays a significant mediating role in the relationship between caregiver stigma and medication adherence among patients with psychotic illnesses. Higher caregiver stigma levels were associated with reduced MHL and, subsequently, lower treatment adherence. Conversely, caregivers with greater MHL significantly supported better medication adherence, highlighting its pivotal role in improving treatment outcomes. These results underscore the importance of reducing stigma and enhancing MHL through targeted educational interventions. Healthcare systems should integrate caregiver-focused psychoeducation programs to improve understanding of psychotic disorders and reduce stigma-related barriers to treatment adherence.
Study limitation
This study has several limitations. First, its cross-sectional design limits the ability to infer causality between variables. Second, data were collected through self-reported questionnaires, which may be subject to social desirability and recall biases. Third, the sample was drawn from a single geographic region, potentially limiting the generalizability of the findings to the broader population. Finally, this study did not account for clinical severity or duration of illness, which may influence medication adherence and caregiver perceptions.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Research Ethics Committee of the College of Nursing, University of Babylon (No.: 78: dated 24/3/2025). The Health Authority of Baghdad/Baghdad Health Directorate, Iraq, approved all experimental protocols. During data collection, all permitted guidelines were adhered to.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, and data collection: Zaman Ahmed Hrefish; Writing the original draft: All authors; Data analysis, review and editing: Saja Hashem Mohammed.
Conflict of interest
The authors declared no conflict of interest.
References
- Patel KP, Oroszi TL. Schizophrenia management approaches: A look at progress and challenges. World Journal of Neuroscience. 2024; 15(1):13-34. [DOI:10.4236/wjns.2025.151003]
- Abdullah-Koolmees H, Nawzad S, Egberts TC, Vuyk J, Gardarsdottir H, Heerdink ER. The effect of non-adherence to antipsychotic treatment on rehospitalization in patients with psychotic disorders. Therapeutic Advances in Psychopharmacology. 2021; 11:20451253211027449. [DOI:10.1177/20451253211027449] [PMID]
- Balat KZ, Laftah SA, Radhi M. The relationship between psychological distress and quality of life among women undergoing mastectomy in Iraq: A descriptive correlational study. National Journal of Community Medicine. 2025; 16(1):20-7. [DOI:10.55489/njcm.160120254716]
- Radhi MM, Al-Eqabi QA, Hindi NK. Rehabilitation problems of people with motor disabilities at Babylon center for rehabilitation of the disabled. Medical Journal of Babylon. 2023; 20(4):838-43. [DOI:10.4103/MJBL.MJBL_674_23]
- Alasmee N. Primary caregivers experience of anti-psychotic medication: A qualitative study. Archives of Psychiatric Nursing. 2020; 34(6):520-8. [DOI:10.1016/j.apnu.2020.09.002] [PMID]
- Manesh AE, Dalvandi A, Zoladl M. The experience of stigma in family caregivers of people with schizophrenia spectrum disorders: A meta-synthesis study. Heliyon. 2023; 9(3):e14333. [DOI:10.1016/j.heliyon.2023.e14333] [PMID]
- Brigiano M, Calabrese L, Chirico I, Trolese S, Quartarone M, Forte L, et al. Within my walls, i escape being underestimated: A systematic review and thematic synthesis of stigma and help-seeking in dementia. Behavioral Sciences. 2025; 15(6):774. [DOI:10.3390/bs15060774] [PMID]
- Radu M, Ciucă A, Crișan CA, Pintea S, Predescu E, Șipos R, et al. The impact of psychiatric disorders on caregivers: An integrative predictive model of burden, stigma, and well‐being. Perspectives in Psychiatric Care. 2022; 58(4):2372. [DOI:10.1111/ppc.13071] [PMID]
- Zeng S, Bailey R, Peng S, Chen X. Defining mental health literacy: A systematic literature review and educational inspiration. Journal of Public Mental Health. 2024; 23(3):189-204. [DOI:10.1108/JPMH-04-2024-0055]
- He X, Chen S, Zhang Q, He S, Yang L, Ma J. Mental health literacy and professional psychological help-seeking attitudes among primary healthcare workers: The mediating role of social support and mental illness stigma. Risk Management and Healthcare Policy. 2025; 18:703-18. [DOI:10.2147/RMHP.S512458] [PMID]
- Elywy GJ, Radhi MM, AlEqabi QA. Relationship between social support and self-hardiness among breast cancer women in Nasiriyah, Iraq. Journal of the Pakistan Medical Association. 2023; 73(9):S9-14. [DOI:10.47391/JPMA.IQ-02]
- Malih Radhi M, Juma Elywy G, Abbas Khyoosh Al-Eqabi Q. Burdens among wives of disabled people in the light of some social variables. Iranian Rehabilitation Journal. 2023; 21(3):473-84. [DOI:10.32598/irj.21.3.1765.3]
- Andrade C, Tavares M, Soares H, Coelho F, Tomás C. Positive mental health and mental health literacy of informal caregivers: A scoping review. International Journal of Environmental Research and Public Health. 2022; 19(22):15276. [DOI:10.3390/ijerph192215276] [PMID]
- Sakız H, Kaçan H. Resilience and mental health literacy mediate the effect of caregiver burden on internalized stigma among mothers of children with disabilities. Children’s Health Care. 2023; 54(4):1-24. [DOI:10.1080/02739615.2023.2290264]
- O’Connor M, Casey L. The Mental Health Literacy Scale (MHLS): A new scale-based measure of mental health literacy. Psychiatry Research. 2015; 229(1-2):511-6. [DOI:10.1016/j.psychres.2015.05.064] [PMID]
- Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new medication adherence rating scale (MARS) for the psychoses. Schizophrenia Research. 2000; 42(3):241-7. [DOI:10.1016/S0920-9964(99)00130-9] [PMID]
- Chang CC, Su JA, Chang KC, Lin CY, Koschorke M, Thornicroft G. Perceived stigma of caregivers: Psychometric evaluation for Devaluation of Consumer Families Scale. International Journal of Clinical and Health Psychology. 2018; 18(2):170-8. [DOI:10.1016/j.ijchp.2017.12.003] [PMID]
- Radhi MM, Niazy SM, Abed SN. Individual-related factors associated with treatment adherence among hypertensive patients. Journal of Public Health in Africa. 2023; 14(6):2466. [DOI:10.4081/jphia.2023.2466] [PMID]
- Abed Laftah S, Kadhim Abdul-Hameed A, Zair Balat K, Malih Radhi M. Barriers and facilitators in rehabilitative nursing care for disabilities and mediating roles of nurse-related factors. Iranian Rehabilitation Journal. 2025; 23(2):165-74. [DOI:10.32598/irj.23.2.1989.4]
- Alwatify SS, Radhi MM. Diabetes self-management and its association with medication adherence in diabetic patients. Iranian Journal of War and Public Health. 2025; 17(1):17-22. [DOI:10.58209/ijwph.17.1.17]
- Niazy SM, Abadi NN, Radhi MM, Al-Eqabi QA, AL-Thabhawee GD. Impact of digital health literacy on quality of life among people with physical disabilities. Iranian Journal of War and Public Health. 2025; 17(2):197-203. [DOI:10.58209/ijwph.17.2.197]
- Klinpiboon P, Chanthapasa K. The medication use issues and challenges of mental illness exacerbation in patients with schizophrenia: A qualitative study in Thailand. Patient Preference and Adherence. 2023; 17:2927-37. [DOI:10.2147/PPA.S420973] [PMID]
- Lee HY, Hwang J, Ball JG, Lee J, Albright DL. Is health literacy associated with mental health literacy? Findings from Mental Health Literacy Scale. Perspectives in Psychiatric Care. 2020; 56(2):393-400. [DOI:10.1111/ppc.12447] [PMID]
- Amoako GK, Dzogbenuku RK, Abubakari A. Do green knowledge and attitude influence the youth’s green purchasing? Theory of planned behavior. International Journal of Productivity and Performance Management. 2020; 69(8):1609-26. [DOI:10.1108/IJPPM-12-2019-0595]
- Rodrigues JM, Cruz AS, Queirós C. Understanding stigma in mental illness: A novel literature-based model of development. Psychiatry International. 2025; 6(1):21. [DOI:10.3390/psychiatryint6010021]
- El-Saifi N, Moyle W, Jones C, Alston-Knox C. Determinants of medication adherence in older people with dementia from the caregivers’ perspective. International Psychogeriatrics. 2019; 31(3):331-9. [DOI:10.1017/S1041610218000583] [PMID]
- Niazy SM, Al-Eqabi QA, Radhi MM, AL-Thabhawee GD. Nutritional status in community-dwelling older adults and geriatric home. Iranian Journal of War and Public Health. 2025; 17(1):83-7. [DOI:10.58209/ijwph.17.1.83]
- Radhi MM. Degree of disease acceptance and health seeking behaviors for type 2 diabetic patients at diabetic center in Hilla City. Medico Legal Update. 2020; 20(2):853-8. [DOI:10.37506/mlu.v20i2.1347]
- Yasir AA, Qassim WJ, Radhi MM. Assessment the feeling of psychological loneliness among wives of martyrs in the light of some social variables in Babylon Governorate/Iraq. Journal of Pharmaceutical Sciences and Research. 2018; 10(1):40-4. [Link]
- Qassim WJ, Yasir AA, Radhi MM. Assessment of self hardness and its relationship to treatment acceptance for patients with diabetes mellitus at diabetic center in Hilla City/Iraq. Journal of Pharmaceutical Sciences and Research. 2018; 10(1):142-5. [Link]
Article type: Original Research Articles |
Subject:
Nursing
Received: 2025/07/18 | Accepted: 2025/08/30 | Published: 2025/12/1
Received: 2025/07/18 | Accepted: 2025/08/30 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
