
988368
Wed, Jul 1, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 1-10 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Putra M A D T, Akbar M F, Affaier A, Prasetia M V. Rehabilitation in Recurrent Ocular Myokymia: Trigger, Retraining, and Visual Ergonomics. Iranian Rehabilitation Journal 2026; 24 (1) :1-10
URL: http://irj.uswr.ac.ir/article-1-2625-en.html
URL: http://irj.uswr.ac.ir/article-1-2625-en.html
Muhammad Adib Dwi Tamma Putra *1 

 , Muhammad Fadill Akbar2 , Achmad Affaier2 , Muhammad Valdi Prasetia2
, Muhammad Fadill Akbar2 , Achmad Affaier2 , Muhammad Valdi Prasetia2
, Muhammad Fadill Akbar2 , Achmad Affaier2 , Muhammad Valdi Prasetia2
1- Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Universitas Sriwijaya, Palembang, Indonesia. & Doctoral Program, AMA University, Quezon, Philippines.
2- Faculty of Medicine, Universitas Sriwijaya, Palembang, Indonesia.
2- Faculty of Medicine, Universitas Sriwijaya, Palembang, Indonesia.
Keywords: Myokymia, Biofeedback, Psychology, Mindfulness, Computer vision syndrome (CVS), Botulinum toxins (botox)
Full-Text [PDF 597 kb]
(256 Downloads)
| Abstract (HTML) (1340 Views)
References
Full-Text: (64 Views)
Introduction
Recurrent ocular myokymia (ROM) is a benign, self-limiting condition characterized by fine, spontaneous contractions of the orbicularis oculi muscle, most commonly perceived by patients as eyelid twitching [1, 2]. Episodes usually last seconds to minutes, but when they become persistent or frequently recurrent, they may interfere with reading, screen use, social interaction, and sleep, and can provoke disproportionate concern about serious neurological disease [1-3]. This mismatch between low structural risk and potentially high subjective impact often leads to repeated medical consultations, underscoring the need for a structured management strategy that goes beyond simple reassurance.
The etiology of ROM is multifactorial. Consistently reported precipitating factors include psychophysiological stress, sleep deprivation, fatigue, excessive caffeine intake, and prolonged near work or visual strain [1, 2]. In contemporary environments dominated by screen-based tasks, digital eye strain (DES) has emerged as a particularly relevant contributor. A recent case-control study showed a significant association between prolonged daily digital screen exposure and chronic eyelid myokymia, suggesting that environmental and behavioral drivers are central to symptom persistence [3]. These findings support a model in which ROM reflects an interaction between neuromuscular hyperexcitability and modifiable behavioral, psychophysiological, and ergonomic triggers.
Conventional management emphasizes patient reassurance and avoidance of obvious triggers, grounded in the expectation that most cases resolve spontaneously [1, 2]. While this approach is appropriate for transient ROM, it may be insufficient for individuals with chronic, bilateral, or functionally limiting symptoms. In such patients, persistent hyperexcitability of facial motor pathways and impaired inhibitory control mechanisms analogous to those implicated in facial synkinesis, hemifacial spasm, and Bell’s palsy may require more active rehabilitation [4-6]. Neuromuscular retraining, biofeedback, mindfulness-based stress reduction (MBSR), lifestyle modification, and visual ergonomics have all demonstrated benefit in related neuromuscular or stress-linked conditions, but have not yet been integrated into a unified protocol specifically for ROM [3, 4, 7-12].
Existing ROM literature is largely descriptive, focusing on etiology, exclusion of secondary causes, and pharmacological approaches, such as botulinum toxin (botox) for refractory cases [1-3, 5, 13-15]. To our knowledge, no prior review has systematically synthesized neuromuscular, psychophysiological, and ergonomic interventions into a coherent, clinically applicable rehabilitation framework for ROM. The specific knowledge gap addressed by this review is the absence of a unified, rehabilitation-focused protocol for ROM that integrates neuromuscular, psychophysiological, and visual-ergonomic strategies.
This narrative review therefore aims to develop an integrated, evidence-informed rehabilitation framework for ROM that targets both neuromuscular dysfunction and modifiable behavioral triggers, and Discuss its clinical implications within contemporary rehabilitation medicine. Given the scarcity of ROM-specific intervention trials, this framework is explicitly presented as hypothesis-generating, drawing on direct data from ROM where available and on reasoned extrapolation from related conditions where ROM-specific evidence is lacking.
Materials and Methods
Study design and reporting approach
A narrative review methodology was chosen to permit integration of heterogeneous evidence from ophthalmology, neurology, rehabilitation, behavioral medicine, and ergonomics. The structure and reporting were guided by key domains of the scale for the assessment of narrative review articles (SANRA), with particular attention to Clear justification of the topic and its importance, explicit statement of objectives and the specific gap being addressed, transparent description of the literature search and selection process, and coherent presentation and critical discussion of the evidence.
Data sources and search strategy
A structured literature search was conducted in PubMed and Scopus for articles published between January 2015 and October 2025. The primary search block targeted ROM and related eyelid phenomena: (“eyelid myokymia” OR “ocular myokymia” OR “eyelid twitch*” OR “eye twitch*”).
This was combined with blocks representing rehabilitation and neuromuscular approaches:
AND (“rehabilitation” OR “neuromuscular retraining” OR “physical therapy” OR “physiotherapy” OR “biofeedback” OR “facial synkinesis” OR “hemifacial spasm” OR “Bell’s palsy”). To capture psychophysiological and ergonomic interventions relevant to ROM triggers, additional searches combined anxiety, mindfulness, and DES terms:
(“mindfulness-based stress reduction” OR “MBSR” OR “mindfulness” OR “stress reduction”) AND (“anxiety” OR “anxiety disorder”) (“digital eye strain” OR “computer vision syndrome”) AND (“20-20-20 rule” OR “microbreak*” OR “visual ergonomics” OR “blink rate”). Reference lists of key articles and reviews were screened for additional relevant studies. Where ROM-specific interventional data were sparse, the search was deliberately broadened to include:
Facial synkinesis, hemifacial spasm, and Bell’s palsy rehabilitation (neuromuscular and biofeedback), anxiety and stress-related disorders treated with MBSR or similar approaches, DES/computer vision syndrome (CVS) trials of visual ergonomics and microbreaks.
Eligibility criteria
The inclusion criteria were as follows:
Population
1) Adults or adolescents with eyelid/ocular myokymia, hemifacial spasm, facial synkinesis, or other focal facial motor hyperexcitability disorders with conceptual relevance to ROM. 2) Adults with anxiety disorders or DES/CVS where interventions were psychophysiological (e.g. MBSR) or visual-ergonomic and thus applicable to ROM triggers.
Interventions
1) Neuromuscular retraining, facial neuromuscular therapy, or EMG-based biofeedback. 2) Mindfulness-based or structured stress-reduction interventions, sleep optimization, and caffeine reduction. 3) Visual ergonomics and DES strategies (20-20-20 rule, microbreaks, blink training, workstation optimization). 4) Botox injections used to treat eyelid myokymia, hemifacial spasm, or sequelae of peripheral facial palsy.
Study design
1) Randomized controlled trials (RCTs), controlled clinical trials, cohort and case–control studies, case series, and well-documented case reports. 2) Clinical reviews or guidelines that informed red-flag identification or rehabilitation principles.
Outcomes
1) Symptom frequency or severity (e.g. twitch frequency, DES scores). 2) Objective neuromuscular markers (e.g. EMG activity, blink rate, facial grading). 3) Patient-reported functional or quality-of-life outcomes.
The exclusion criteria were as follows:
Non-human studies. Non-English language articles. Conditions without plausible conceptual transferability to ROM (e.g. generalized movement disorders). Purely tertiary online resources used only for background (e.g. EyeWiki and StatPearls) were not used as primary evidence but retained as clinical context references.
Study selection and data extraction
Titles and abstracts were screened for relevance to ROM, facial motor hyperexcitability, neuromuscular rehabilitation, psychophysiological interventions, or DES. Full texts of potentially eligible studies were then reviewed against the inclusion criteria. Disagreements regarding inclusion were resolved through discussion with a conservative bias toward including conceptually relevant studies.
From each included study, the following data were extracted where available:
Study design and setting (e.g. RCT, case–control, case series). Sample size and population characteristics. Primary condition studied (ROM, hemifacial spasm, facial synkinesis, Bell’s palsy, anxiety, DES). Intervention type, dose, and duration. Comparator interventions or usual care when applicable. Primary and secondary outcomes, including symptom and functional measures. Adverse events and safety considerations.
Synthesis and classification of evidence
Given anticipated heterogeneity, no meta-analysis was attempted. Instead, studies were thematically organized into three primary rehabilitation domains:
Neuromuscular retraining and biofeedback (facial nerve rehabilitation and facial synkinesis).
Psychophysiological modulation and lifestyle optimization (MBSR and related stress-reduction strategies, sleep and caffeine). Visual ergonomics and DES management. Botulinum toxin therapy and red-flag recognition were treated as adjunctive and safety-oriented components.
For transparency, the strength of evidence supporting each domain was classified qualitatively by study design (e.g. RCT vs observational vs case report) and sample size, and mapped in Table 1 (evidence overview).
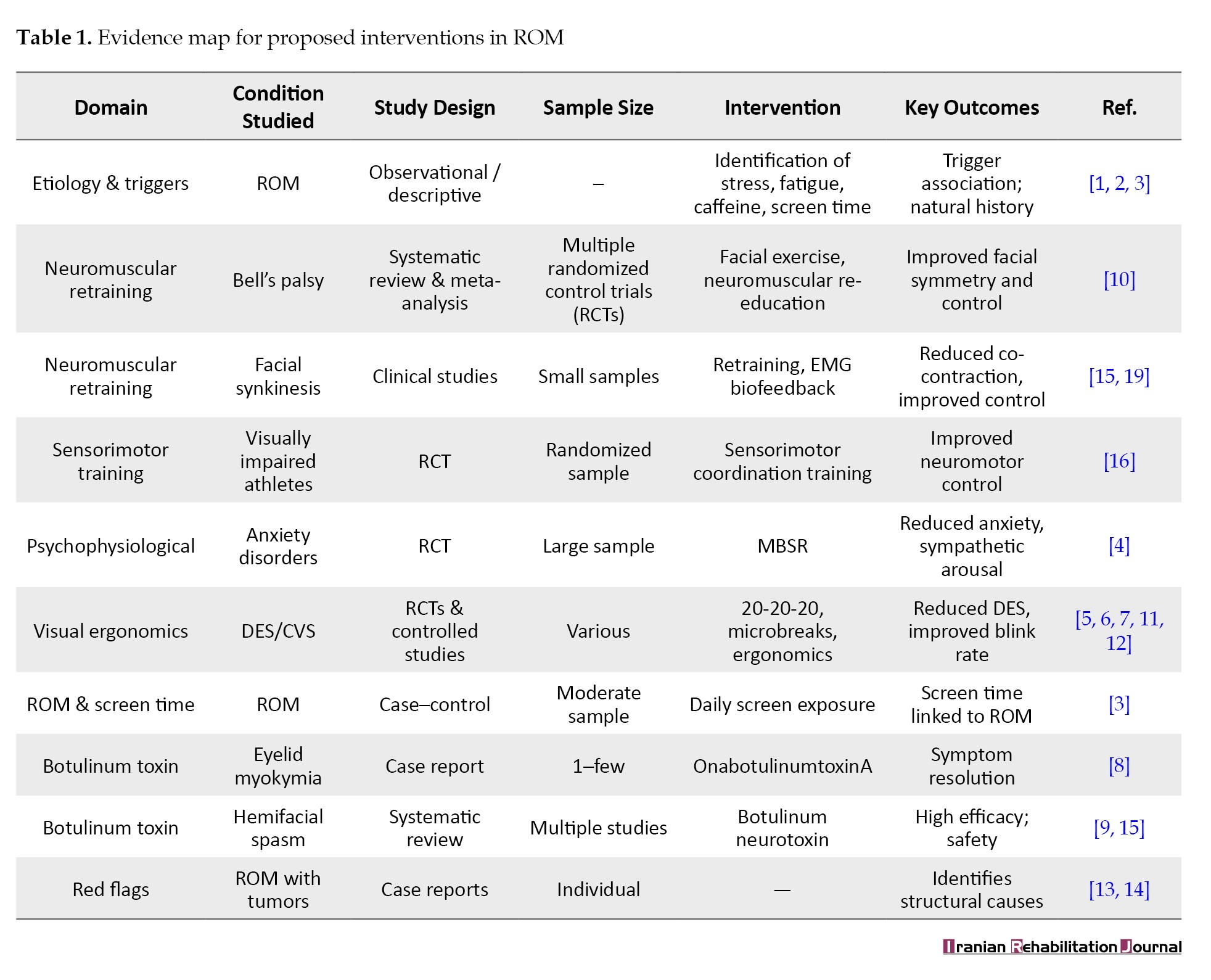
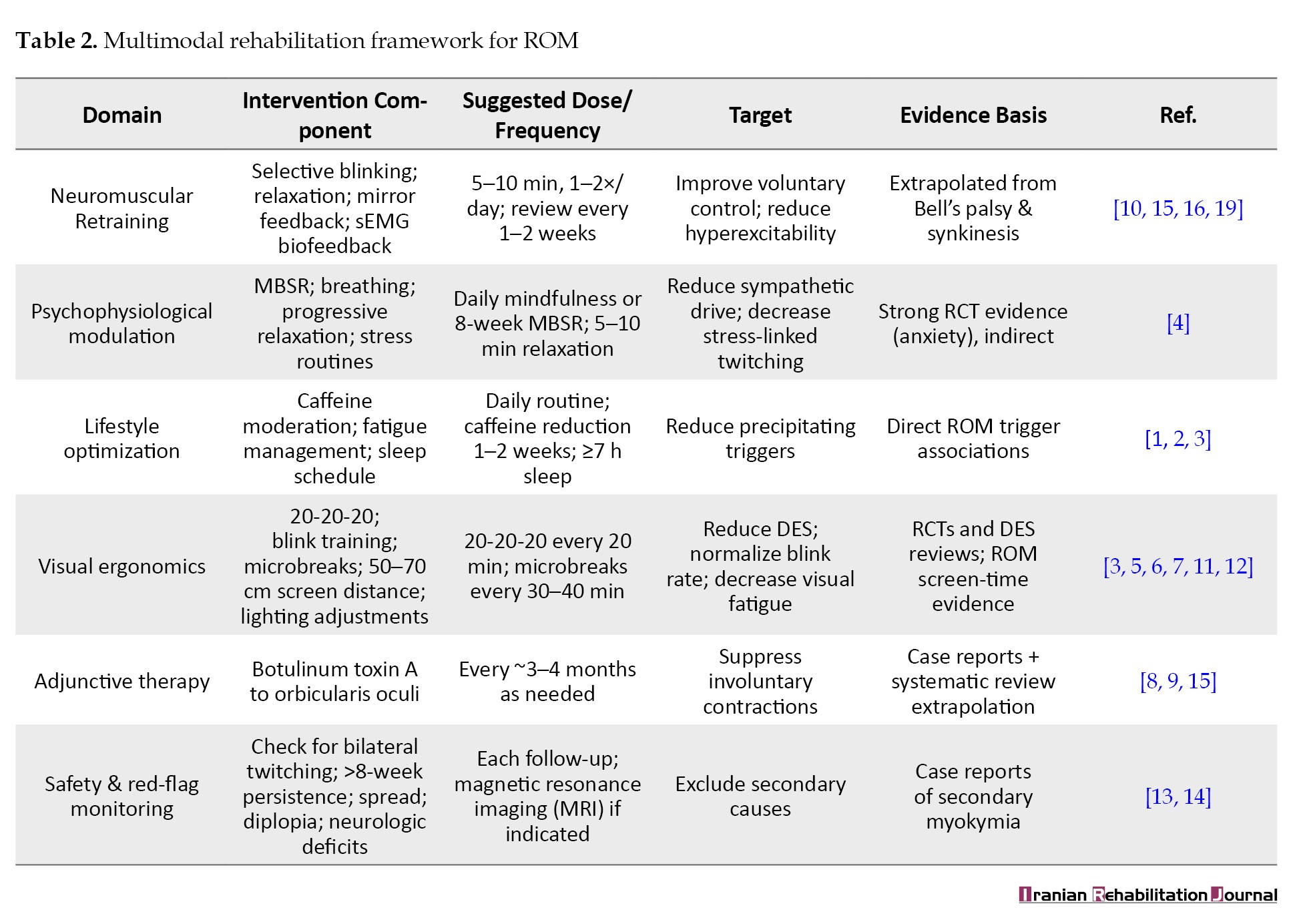
ROM-specific data are explicitly distinguished from extrapolated evidence derived from related conditions. The proposed multimodal rehabilitation framework is summarized in Table 2, detailing interventions, dosing, and evidence level.
Results
Clinical features, triggers, and initial management
Narrative and review sources consistently describe ROM as a benign, self-limited neuromuscular phenomenon affecting the orbicularis oculi [1, 2]. Episodes typically present as unilateral, intermittent eyelid twitching without overt neurological deficits [1-3]. Persistent or chronic forms may cause functional inconvenience, insomnia, and anxiety, prompting repeated consultations [1-3].
Commonly reported precipitating factors include:
Psychophysiological stress and fatigue, sleep deprivation, excessive caffeine intake, and prolonged visual strain, especially during digital device use [1-3]. Güneş reported a significant association between longer daily digital screen time and chronic eyelid myokymia, reinforcing the role of DES as a modifiable environmental driver [3].
Initial management of ROM should include systematic identification and modification of known triggers (stress, sleep, caffeine, screen time [1-3], clear reassurance about the typically benign and self-limited course [1, 2], and vigilance for red flags such as bilateral involvement, spread beyond the eyelid, duration beyond 8 weeks, new visual symptoms, or additional neurological signs, which warrant neuroimaging and neurological evaluation to rule out secondary causes such as trigeminal schwannoma or intracranial tumors [1-3, 14, 15].
Evidence base by domain
The available evidence can be summarized as follows (and is detailed in Table 1).
ROM-specific evidence: Primarily observational descriptions and case reports on triggers, natural history, and rare structural causes, with isolated case reports onbotox response [1-3, 13-15].
Neuromuscular retraining and biofeedback: Systematic review and meta-analysis data on Bell’s palsy rehabilitation, and studies on facial synkinesis and facial nerve dysfunction, examining physical therapy, neuromuscular re-education, and biofeedback [4-6, 16].
Psychophysiological interventions: A high-quality RCT demonstrating that MBSR is non-inferior to escitalopram for anxiety disorders [7].
Visual ergonomics and DES: RCTs, controlled trials, and systematic reviews on DES, 20-20-20 rule, microbreaks, blink behavior, and ergonomic optimization [8-12].
Botulinum toxin: Case reports and systematic review data showing efficacy and safety in focal facial hyperkinesias, such as hemifacial spasm and sequelae of facial palsy, with limited but supportive case evidence in eyelid myokymia [5, 13, 17].
Overall, direct ROM-specific interventional evidence is limited, and much of the rehabilitation framework is extrapolated from related conditions with shared mechanisms of facial motor hyperexcitability.
Neuromuscular retraining and biofeedback (conceptual adaptation) aims to enhance selective voluntary control of the orbicularis oculi and improve the capacity to inhibit involuntary motor discharges. A systematic review and meta-analysis of physical therapy interventions in Bell’s palsy reported that tailored exercise programs and neuromuscular re-education improved facial symmetry and functional outcomes compared with minimal or no therapy [10]. These interventions commonly include:
1) Selective activation of facial muscles with deliberate relaxation phases, 2) mirror feedback to refine movement accuracy and symmetry, and 3) EMG-based biofeedback in some protocols to visualize muscle activation and support motor learning [4, 5, 16].
Sensorimotor training has also been shown to improve balance and coordination in visually impaired athletes, demonstrating the capacity of targeted training to drive functional neuroplastic changes despite sensory limitations [16].
Based on these principles, a hypothesis-generating ROM-oriented protocol could include:
1) Selective blinking and relaxation drills: slow, controlled blinks followed by conscious periocular relaxation, 10–15 repetitions, two to three times daily, 2) mirror feedback: To minimize co-activation of adjacent facial muscles and promote symmetric, precise movements, 3) SEMG biofeedback (where available): low-gain surface EMG over the orbicularis oculi to provide real-time feedback on contraction and relaxation, helping patients recognize and reduce overflow activation [4, 5], and 4) treatment dose: short sessions (5–10 min) once or twice daily, with clinical review every 1–2 weeks for refinement [4].
The efficacy of such protocols in ROM is not yet empirically proven, and their inclusion in this framework is based on mechanistic similarity with Bell’s palsy and facial synkinesis rather than direct ROM trials [4-6, 16]. These NMR and biofeedback strategies should therefore be clearly framed as low-risk, hypothesis-generating options.
Psychophysiological modulation and lifestyle optimization deal with stress, sleep disturbance, and excessive caffeine, that are well-recognized triggers for eyelid myokymia [1-3]. Elevated sympathetic arousal may increase excitatory neural drive, thereby promoting or prolonging twitching episodes.
A randomized, non-inferiority trial demonstrated that an 8-week MBSR program was non-inferior to escitalopram for reducing anxiety severity in adults with anxiety disorders [7]. The MBSR group showed significant improvements in anxiety scores and physiological stress markers, supporting its use as an evidence-based intervention for stress reduction [7]. Although ROM was not specifically studied, the mechanistic pathway reduced limbic and autonomic activation provides a plausible route by which MBSR could attenuate stress-related eyelid twitching.
Within a ROM rehabilitation program, psychophysiological strategies may therefore include:
1) Mindfulness-based interventions: standard MBSR or briefer mindfulness and relaxation protocols to reduce baseline stress and sympathetic tone [7], 2) Breathing and relaxation training: diaphragmatic breathing, progressive muscle relaxation, or guided imagery, particularly before periods of intensive visual work or at symptom onset, 3) sleep hygiene: Promoting ≥7 hours of sleep, regular sleep–wake schedules, and minimizing late-day caffeine [1-3], and 4) Caffeine moderation: progressive reduction of high caffeine intake, based on individualized assessment [1-3],
Education about the benign nature of ROM and the role of psychophysiological factors may reduce hypervigilance and catastrophic interpretation of symptoms, interrupting the cycle of anxiety and increased twitch awareness [1-3].
Evidence for these interventions in ROM is indirect, based primarily on their efficacy in anxiety disorders and the observational links between stress, fatigue, caffeine, and ROM [1-3, 7]. Recommendations in this domain are therefore hypothesis-generating but supported by level 1 evidence for anxiety and stress reduction [7].
Visual ergonomics and DES management are other important issues. DES, also known as CVS, is highly prevalent and associated with ocular discomfort, dryness, blurred vision, and reduced blink rate [8-12]. These factors may heighten orbicularis oculi excitability and predispose to or maintain eyelid twitching [3].
Evidence-based ergonomic strategies include:
1) 20-20-20 rule: looking at an object approximately 20 feet away for at least 20 seconds after every 20 minutes of screen use. In a trial of this rule, participants reported significant reductions in DES symptoms and accommodative stress [8]. 2) Viewing distance and screen positioning: Maintaining a 50–70 cm viewing distance and aligning the top of the screen at or just below eye level, with balanced ambient lighting to minimize glare [8-12], 3) blink-awareness training: Encouraging a blink rate of roughly 15–20 blinks per minute, supported by reminders (e.g. smartphone applications) and lubricating eye drops if required [8-12], 4) scheduled microbreaks: Short, regular breaks from near work which have been associated with reductions in DES symptoms in controlled studies [8-11], Güneş’ case-control study demonstrated that individuals with chronic eyelid myokymia had significantly longer daily screen exposure than controls, with a positive relationship between screen time and symptom burden [3]. This finding supports the centrality of visual ergonomics and screen-time management in ROM rehabilitation.
Adherence can be tracked via digital logs or simple symptom diaries, and outcomes monitored using instruments such as the CVS Questionnaire (CVS-Q) or other DES measures described in DES reviews [9-12].
Adjunctive therapies and safety considerations include the following items.
For refractory or functionally disabling ROM, botox type A may provide substantial relief. A case report described swallow-induced eyelid myokymia resolving after onabotulinumtoxinA injections into the orbicularis oculi [13]. Systematic review data and clinical series in hemifacial spasm and facial palsy sequelae show that botulinum neurotoxin is effective and generally safe in reducing focal facial hyperkinesias, with high response rates and manageable adverse events [5, 17].
Within the proposed framework, botox should be:
1) Reserved for refractory, functionally significant cases, 2) used only after exclusion of structural causes and after structured trials of conservative rehabilitation (neuromuscular, psychophysiological, ergonomic), and 3) Administered by clinicians experienced in periocular injection to minimize complications such as ptosis or diplopia [5, 13, 17].
Red-flag indicators, including bilateral symptoms, spread to other facial muscles, persistence beyond 8 weeks, visual changes, or other neurological signs should prompt timely neuroimaging and specialist referral [1-3, 14, 15].
Monitoring, outcomes, and practical framework include a pragmatic 6–8-week rehabilitation program. It might include follow-up every 2–4 weeks to assess
1) Frequency, duration, and situational triggers of eyelid twitching (patient diaries); 2) Perceived stress (e.g. using validated stress or anxiety scales as in analogous MBSR trials) [7]. 3) DES symptoms and functional impact using validated instruments described in the DES literature [9-12]. 3) Patient-defined goals and participation, in line with client-centered rehabilitation approaches [18, 19].
Adjustments to neuromuscular exercises, mindfulness and lifestyle strategies, and ergonomic prescriptions can then be made according to response and adherence.
Table 1 should summarize the supporting evidence by domain (condition, study design, sample size, intervention, key outcomes, and level of evidence: ROM-specific vs extrapolated), while Table 2 should outline the multimodal rehabilitation protocol (domain, specific intervention, dosing/frequency, primary targets, and supporting references).
Discussion
Pathophysiology and rationale for rehabilitation
ROM is thought to arise from spontaneous, intermittent discharges in facial nerve fibers innervating the orbicularis oculi, modulated by central excitatory drive, local neuromuscular conditions, and environmental stressors [1-3]. The condition shares mechanistic similarities with facial synkinesis, hemifacial spasm, and Bell’s palsy sequelae conditions in which aberrant reinnervation, synkinesis, and impaired cortical inhibition lead to involuntary contractions [4-6]. These parallels provide a physiological rationale for adapting neuromuscular retraining strategies to ROM, even though direct ROM trials are lacking.
Most idiopathic ROM is benign and functional rather than structural [1-3]. However, isolated eyelid myokymia can occasionally herald structural pathology, including trigeminal schwannoma or cerebral tumors [14, 15]. This finding underscores the importance of red-flag screening and appropriate imaging in atypical or persistent cases, after which a rehabilitative approach becomes both safe and appropriate.
Neuromuscular retraining and biofeedback
Evidence from Bell’s palsy rehabilitation indicates that targeted physical therapy including facial exercises, neuromuscular retraining, and biofeedback can improve facial function and symmetry [4-6]. These interventions draw on principles of motor relearning, repetitive practice, and sensorimotor feedback to strengthen cortical inhibitory circuits and refine motor output.
In ROM, structured exercises, such as selective blinking, graded relaxation, and EMG-guided control may plausibly help patients regain voluntary regulation over eyelid movement and attenuate motor hyperexcitability. However, in the absence of ROM-specific RCTs, this application must be considered exploratory and hypothesis-generating, supported by mechanistic analogy rather than direct efficacy data [4-6, 16].
Sensorimotor training in visually impaired athletes further supports the notion that carefully structured training can induce significant adaptations in neuromotor coordination even under sensory constraints [16]. This cross-modal evidence adds weight to the concept that cortical and subcortical plasticity can be harnessed to modify eyelid motor control.
Psychophysiological and lifestyle modulation
Stress, sleep deprivation, and excessive caffeine intake are repeatedly identified as ROM triggers [1-3]. The RCT demonstrating non-inferiority of MBSR versus escitalopram in anxiety disorders provides robust level 1 evidence that mindfulness-based interventions can significantly reduce both subjective anxiety and physiological stress responses [7]. Incorporating MBSR-style programs, or briefer, structured mindfulness and relaxation exercises, into ROM care is therefore scientifically reasonable, with the expectation that reduced autonomic arousal will diminish the propensity for stress-triggered twitching.
Coupling these strategies with sleep optimization and caffeine moderation directly addresses modifiable behavioral risk factors identified in clinical descriptions of eyelid myokymia [1-3]. Although empirical demonstration of their effect on ROM is lacking, the logic linking triggers, mechanisms, and interventions is coherent and consistent with biopsychosocial rehabilitation models [18, 20].
Visual ergonomics and DES
The DES literature demonstrates that visual ergonomics 20-20-20 rule, microbreaks, blink training, and workstation optimization can significantly reduce ocular discomfort and strain, with improved subjective comfort and visual function [8-12]. The association between prolonged screen exposure and eyelid myokymia in the case–control study by Güneş directly implicates digital behavior in ROM [3].
Within the proposed framework, visual ergonomics constitutes a core component rather than an adjunct. The comparatively strong evidence-base for DES interventions (including RCTs and systematic reviews) [8-12] supports recommending these strategies confidently as first-line measures for patients with ROM, especially those with high digital workloads.
Role of botox
Botox A is well established as an effective treatment for hemifacial spasm and sequelae of peripheral facial palsy, with systematic reviews documenting significant symptom reduction and generally favorable safety profiles [5, 17]. Case reports of eyelid myokymia responsive to botox further suggest potential utility in refractory ROM [13]. Within a ROM rehabilitation model, botox should be framed as a second-line adjunct for patients who remain significantly symptomatic despite structured conservative therapy, and only after structural causes have been excluded [5, 13-15, 17].
Strengths, limitations, and SANRA considerations
This review responds directly to SANRA domains by
Clearly articulating the clinical importance of ROM and the specific knowledge gap (lack of a unified rehabilitation protocol), explicitly describing the search strategy, databases, and eligibility criteria, distinguishing between direct ROM evidence and extrapolated data from related conditions, and proposing a structured framework and summarizing evidence in accompanying tables. However, several limitations must be acknowledged. The ROM-specific evidence base is limited, and much of the proposed framework is extrapolated from Bell’s palsy, hemifacial spasm, anxiety disorders, and DES [3-13, 16, 17].
As a narrative rather than systematic review, there is an inherent risk of selection bias despite efforts at transparent reporting. Tertiary clinical resources (EyeWiki, StatPearls) were used for background but not as primary evidence [1, 2].
Future research should therefore prioritize
Prospective observational studies evaluating the natural history of ROM under structured rehabilitative care, pilot and definitive RCTs of neuromuscular retraining, psychophysiological interventions, and ergonomic packages alone and in combination using ROM-specific outcomes, and standardized outcome sets (e.g. twitch frequency, EMG measures, DES questionnaires, quality-of-life indices) to facilitate comparison across studies [4-12, 16, 18, 20].
Clinical implications
Despite its limitations, this review offers a clinically pragmatic, biopsychosocial framework aligned with modern rehabilitation principles, which emphasize integrated, goal-oriented programs and active patient participation [6, 18-20]. By combining neuromuscular retraining, stress modulation, visual ergonomics, and selectively used botox, clinicians can move beyond simple reassurance toward a more proactive, structured approach to ROM.
The explicit mapping of evidence levels (Table 1) and operational outline of interventions (Table 2) may facilitate shared decision-making, helping patients prioritize low-risk, self-management strategies while understanding where evidence remains preliminary.
Conclusion
ROM is benign in prognosis but can be functionally and psychologically distressing when persistent or frequent. Traditional management focused on reassurance and trigger avoidance may not fully address the needs of patients with chronic or high-impact symptoms.
This narrative review proposes a multimodal, non-invasive rehabilitation framework for ROM that integrates neuromuscular retraining and biofeedback to improve voluntary control and dampen hyperexcitability, psychophysiological and lifestyle interventions (e.g. MBSR, sleep and caffeine optimization) to reduce sympathetic arousal and symptom vigilance, visual ergonomics and DES management to tackle a key environmental driver in contemporary digital lifestyles, and adjunctive botox therapy for carefully selected refractory cases after exclusion of secondary causes.
The framework is explicitly hypothesis-generating, grounded in a combination of direct ROM data and extrapolated evidence from related neuromuscular, stress, and ergonomics research. Future controlled trials should validate this integrated approach using standardized neuromuscular and patient-reported outcomes. Until such data are available, the proposed model and accompanying evidence tables provide a structured, biopsychosocial lens through which clinicians can manage ROM more proactively, support patient self-efficacy, and potentially reduce the burden of recurrent consultations driven by persistent eyelid twitching.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, funding acquisition, project administration and investigation: Muhammad Adib Dwi Tamma Putra and Muhammad Fadill Akbar; Methodology and writing the original draft: Muhammad Adib Dwi Tamma Putra, Achmad Affaier; Data curation: Muhammad Adib Dwi Tamma Putra, Muhammad Fadill Akbar, and Muhammad Valdi Prasetia; Formal analysis: Muhammad Fadill Akbar and Achmad Affaier; Review and editing: Muhammad Adib Dwi Tamma Putra, Muhammad Fadill Akbar, Muhammad Valdi Prasetia; Supervision: Muhammad Adib Dwi Tamma Putra.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all colleagues who contributed significant insights throughout the study’s planning and execution phases, and who also offered assistance in analyzing and interpreting the data.
Recurrent ocular myokymia (ROM) is a benign, self-limiting condition characterized by fine, spontaneous contractions of the orbicularis oculi muscle, most commonly perceived by patients as eyelid twitching [1, 2]. Episodes usually last seconds to minutes, but when they become persistent or frequently recurrent, they may interfere with reading, screen use, social interaction, and sleep, and can provoke disproportionate concern about serious neurological disease [1-3]. This mismatch between low structural risk and potentially high subjective impact often leads to repeated medical consultations, underscoring the need for a structured management strategy that goes beyond simple reassurance.
The etiology of ROM is multifactorial. Consistently reported precipitating factors include psychophysiological stress, sleep deprivation, fatigue, excessive caffeine intake, and prolonged near work or visual strain [1, 2]. In contemporary environments dominated by screen-based tasks, digital eye strain (DES) has emerged as a particularly relevant contributor. A recent case-control study showed a significant association between prolonged daily digital screen exposure and chronic eyelid myokymia, suggesting that environmental and behavioral drivers are central to symptom persistence [3]. These findings support a model in which ROM reflects an interaction between neuromuscular hyperexcitability and modifiable behavioral, psychophysiological, and ergonomic triggers.
Conventional management emphasizes patient reassurance and avoidance of obvious triggers, grounded in the expectation that most cases resolve spontaneously [1, 2]. While this approach is appropriate for transient ROM, it may be insufficient for individuals with chronic, bilateral, or functionally limiting symptoms. In such patients, persistent hyperexcitability of facial motor pathways and impaired inhibitory control mechanisms analogous to those implicated in facial synkinesis, hemifacial spasm, and Bell’s palsy may require more active rehabilitation [4-6]. Neuromuscular retraining, biofeedback, mindfulness-based stress reduction (MBSR), lifestyle modification, and visual ergonomics have all demonstrated benefit in related neuromuscular or stress-linked conditions, but have not yet been integrated into a unified protocol specifically for ROM [3, 4, 7-12].
Existing ROM literature is largely descriptive, focusing on etiology, exclusion of secondary causes, and pharmacological approaches, such as botulinum toxin (botox) for refractory cases [1-3, 5, 13-15]. To our knowledge, no prior review has systematically synthesized neuromuscular, psychophysiological, and ergonomic interventions into a coherent, clinically applicable rehabilitation framework for ROM. The specific knowledge gap addressed by this review is the absence of a unified, rehabilitation-focused protocol for ROM that integrates neuromuscular, psychophysiological, and visual-ergonomic strategies.
This narrative review therefore aims to develop an integrated, evidence-informed rehabilitation framework for ROM that targets both neuromuscular dysfunction and modifiable behavioral triggers, and Discuss its clinical implications within contemporary rehabilitation medicine. Given the scarcity of ROM-specific intervention trials, this framework is explicitly presented as hypothesis-generating, drawing on direct data from ROM where available and on reasoned extrapolation from related conditions where ROM-specific evidence is lacking.
Materials and Methods
Study design and reporting approach
A narrative review methodology was chosen to permit integration of heterogeneous evidence from ophthalmology, neurology, rehabilitation, behavioral medicine, and ergonomics. The structure and reporting were guided by key domains of the scale for the assessment of narrative review articles (SANRA), with particular attention to Clear justification of the topic and its importance, explicit statement of objectives and the specific gap being addressed, transparent description of the literature search and selection process, and coherent presentation and critical discussion of the evidence.
Data sources and search strategy
A structured literature search was conducted in PubMed and Scopus for articles published between January 2015 and October 2025. The primary search block targeted ROM and related eyelid phenomena: (“eyelid myokymia” OR “ocular myokymia” OR “eyelid twitch*” OR “eye twitch*”).
This was combined with blocks representing rehabilitation and neuromuscular approaches:
AND (“rehabilitation” OR “neuromuscular retraining” OR “physical therapy” OR “physiotherapy” OR “biofeedback” OR “facial synkinesis” OR “hemifacial spasm” OR “Bell’s palsy”). To capture psychophysiological and ergonomic interventions relevant to ROM triggers, additional searches combined anxiety, mindfulness, and DES terms:
(“mindfulness-based stress reduction” OR “MBSR” OR “mindfulness” OR “stress reduction”) AND (“anxiety” OR “anxiety disorder”) (“digital eye strain” OR “computer vision syndrome”) AND (“20-20-20 rule” OR “microbreak*” OR “visual ergonomics” OR “blink rate”). Reference lists of key articles and reviews were screened for additional relevant studies. Where ROM-specific interventional data were sparse, the search was deliberately broadened to include:
Facial synkinesis, hemifacial spasm, and Bell’s palsy rehabilitation (neuromuscular and biofeedback), anxiety and stress-related disorders treated with MBSR or similar approaches, DES/computer vision syndrome (CVS) trials of visual ergonomics and microbreaks.
Eligibility criteria
The inclusion criteria were as follows:
Population
1) Adults or adolescents with eyelid/ocular myokymia, hemifacial spasm, facial synkinesis, or other focal facial motor hyperexcitability disorders with conceptual relevance to ROM. 2) Adults with anxiety disorders or DES/CVS where interventions were psychophysiological (e.g. MBSR) or visual-ergonomic and thus applicable to ROM triggers.
Interventions
1) Neuromuscular retraining, facial neuromuscular therapy, or EMG-based biofeedback. 2) Mindfulness-based or structured stress-reduction interventions, sleep optimization, and caffeine reduction. 3) Visual ergonomics and DES strategies (20-20-20 rule, microbreaks, blink training, workstation optimization). 4) Botox injections used to treat eyelid myokymia, hemifacial spasm, or sequelae of peripheral facial palsy.
Study design
1) Randomized controlled trials (RCTs), controlled clinical trials, cohort and case–control studies, case series, and well-documented case reports. 2) Clinical reviews or guidelines that informed red-flag identification or rehabilitation principles.
Outcomes
1) Symptom frequency or severity (e.g. twitch frequency, DES scores). 2) Objective neuromuscular markers (e.g. EMG activity, blink rate, facial grading). 3) Patient-reported functional or quality-of-life outcomes.
The exclusion criteria were as follows:
Non-human studies. Non-English language articles. Conditions without plausible conceptual transferability to ROM (e.g. generalized movement disorders). Purely tertiary online resources used only for background (e.g. EyeWiki and StatPearls) were not used as primary evidence but retained as clinical context references.
Study selection and data extraction
Titles and abstracts were screened for relevance to ROM, facial motor hyperexcitability, neuromuscular rehabilitation, psychophysiological interventions, or DES. Full texts of potentially eligible studies were then reviewed against the inclusion criteria. Disagreements regarding inclusion were resolved through discussion with a conservative bias toward including conceptually relevant studies.
From each included study, the following data were extracted where available:
Study design and setting (e.g. RCT, case–control, case series). Sample size and population characteristics. Primary condition studied (ROM, hemifacial spasm, facial synkinesis, Bell’s palsy, anxiety, DES). Intervention type, dose, and duration. Comparator interventions or usual care when applicable. Primary and secondary outcomes, including symptom and functional measures. Adverse events and safety considerations.
Synthesis and classification of evidence
Given anticipated heterogeneity, no meta-analysis was attempted. Instead, studies were thematically organized into three primary rehabilitation domains:
Neuromuscular retraining and biofeedback (facial nerve rehabilitation and facial synkinesis).
Psychophysiological modulation and lifestyle optimization (MBSR and related stress-reduction strategies, sleep and caffeine). Visual ergonomics and DES management. Botulinum toxin therapy and red-flag recognition were treated as adjunctive and safety-oriented components.
For transparency, the strength of evidence supporting each domain was classified qualitatively by study design (e.g. RCT vs observational vs case report) and sample size, and mapped in Table 1 (evidence overview).
ROM-specific data are explicitly distinguished from extrapolated evidence derived from related conditions. The proposed multimodal rehabilitation framework is summarized in Table 2, detailing interventions, dosing, and evidence level.
Results
Clinical features, triggers, and initial management
Narrative and review sources consistently describe ROM as a benign, self-limited neuromuscular phenomenon affecting the orbicularis oculi [1, 2]. Episodes typically present as unilateral, intermittent eyelid twitching without overt neurological deficits [1-3]. Persistent or chronic forms may cause functional inconvenience, insomnia, and anxiety, prompting repeated consultations [1-3].
Commonly reported precipitating factors include:
Psychophysiological stress and fatigue, sleep deprivation, excessive caffeine intake, and prolonged visual strain, especially during digital device use [1-3]. Güneş reported a significant association between longer daily digital screen time and chronic eyelid myokymia, reinforcing the role of DES as a modifiable environmental driver [3].
Initial management of ROM should include systematic identification and modification of known triggers (stress, sleep, caffeine, screen time [1-3], clear reassurance about the typically benign and self-limited course [1, 2], and vigilance for red flags such as bilateral involvement, spread beyond the eyelid, duration beyond 8 weeks, new visual symptoms, or additional neurological signs, which warrant neuroimaging and neurological evaluation to rule out secondary causes such as trigeminal schwannoma or intracranial tumors [1-3, 14, 15].
Evidence base by domain
The available evidence can be summarized as follows (and is detailed in Table 1).
ROM-specific evidence: Primarily observational descriptions and case reports on triggers, natural history, and rare structural causes, with isolated case reports onbotox response [1-3, 13-15].
Neuromuscular retraining and biofeedback: Systematic review and meta-analysis data on Bell’s palsy rehabilitation, and studies on facial synkinesis and facial nerve dysfunction, examining physical therapy, neuromuscular re-education, and biofeedback [4-6, 16].
Psychophysiological interventions: A high-quality RCT demonstrating that MBSR is non-inferior to escitalopram for anxiety disorders [7].
Visual ergonomics and DES: RCTs, controlled trials, and systematic reviews on DES, 20-20-20 rule, microbreaks, blink behavior, and ergonomic optimization [8-12].
Botulinum toxin: Case reports and systematic review data showing efficacy and safety in focal facial hyperkinesias, such as hemifacial spasm and sequelae of facial palsy, with limited but supportive case evidence in eyelid myokymia [5, 13, 17].
Overall, direct ROM-specific interventional evidence is limited, and much of the rehabilitation framework is extrapolated from related conditions with shared mechanisms of facial motor hyperexcitability.
Neuromuscular retraining and biofeedback (conceptual adaptation) aims to enhance selective voluntary control of the orbicularis oculi and improve the capacity to inhibit involuntary motor discharges. A systematic review and meta-analysis of physical therapy interventions in Bell’s palsy reported that tailored exercise programs and neuromuscular re-education improved facial symmetry and functional outcomes compared with minimal or no therapy [10]. These interventions commonly include:
1) Selective activation of facial muscles with deliberate relaxation phases, 2) mirror feedback to refine movement accuracy and symmetry, and 3) EMG-based biofeedback in some protocols to visualize muscle activation and support motor learning [4, 5, 16].
Sensorimotor training has also been shown to improve balance and coordination in visually impaired athletes, demonstrating the capacity of targeted training to drive functional neuroplastic changes despite sensory limitations [16].
Based on these principles, a hypothesis-generating ROM-oriented protocol could include:
1) Selective blinking and relaxation drills: slow, controlled blinks followed by conscious periocular relaxation, 10–15 repetitions, two to three times daily, 2) mirror feedback: To minimize co-activation of adjacent facial muscles and promote symmetric, precise movements, 3) SEMG biofeedback (where available): low-gain surface EMG over the orbicularis oculi to provide real-time feedback on contraction and relaxation, helping patients recognize and reduce overflow activation [4, 5], and 4) treatment dose: short sessions (5–10 min) once or twice daily, with clinical review every 1–2 weeks for refinement [4].
The efficacy of such protocols in ROM is not yet empirically proven, and their inclusion in this framework is based on mechanistic similarity with Bell’s palsy and facial synkinesis rather than direct ROM trials [4-6, 16]. These NMR and biofeedback strategies should therefore be clearly framed as low-risk, hypothesis-generating options.
Psychophysiological modulation and lifestyle optimization deal with stress, sleep disturbance, and excessive caffeine, that are well-recognized triggers for eyelid myokymia [1-3]. Elevated sympathetic arousal may increase excitatory neural drive, thereby promoting or prolonging twitching episodes.
A randomized, non-inferiority trial demonstrated that an 8-week MBSR program was non-inferior to escitalopram for reducing anxiety severity in adults with anxiety disorders [7]. The MBSR group showed significant improvements in anxiety scores and physiological stress markers, supporting its use as an evidence-based intervention for stress reduction [7]. Although ROM was not specifically studied, the mechanistic pathway reduced limbic and autonomic activation provides a plausible route by which MBSR could attenuate stress-related eyelid twitching.
Within a ROM rehabilitation program, psychophysiological strategies may therefore include:
1) Mindfulness-based interventions: standard MBSR or briefer mindfulness and relaxation protocols to reduce baseline stress and sympathetic tone [7], 2) Breathing and relaxation training: diaphragmatic breathing, progressive muscle relaxation, or guided imagery, particularly before periods of intensive visual work or at symptom onset, 3) sleep hygiene: Promoting ≥7 hours of sleep, regular sleep–wake schedules, and minimizing late-day caffeine [1-3], and 4) Caffeine moderation: progressive reduction of high caffeine intake, based on individualized assessment [1-3],
Education about the benign nature of ROM and the role of psychophysiological factors may reduce hypervigilance and catastrophic interpretation of symptoms, interrupting the cycle of anxiety and increased twitch awareness [1-3].
Evidence for these interventions in ROM is indirect, based primarily on their efficacy in anxiety disorders and the observational links between stress, fatigue, caffeine, and ROM [1-3, 7]. Recommendations in this domain are therefore hypothesis-generating but supported by level 1 evidence for anxiety and stress reduction [7].
Visual ergonomics and DES management are other important issues. DES, also known as CVS, is highly prevalent and associated with ocular discomfort, dryness, blurred vision, and reduced blink rate [8-12]. These factors may heighten orbicularis oculi excitability and predispose to or maintain eyelid twitching [3].
Evidence-based ergonomic strategies include:
1) 20-20-20 rule: looking at an object approximately 20 feet away for at least 20 seconds after every 20 minutes of screen use. In a trial of this rule, participants reported significant reductions in DES symptoms and accommodative stress [8]. 2) Viewing distance and screen positioning: Maintaining a 50–70 cm viewing distance and aligning the top of the screen at or just below eye level, with balanced ambient lighting to minimize glare [8-12], 3) blink-awareness training: Encouraging a blink rate of roughly 15–20 blinks per minute, supported by reminders (e.g. smartphone applications) and lubricating eye drops if required [8-12], 4) scheduled microbreaks: Short, regular breaks from near work which have been associated with reductions in DES symptoms in controlled studies [8-11], Güneş’ case-control study demonstrated that individuals with chronic eyelid myokymia had significantly longer daily screen exposure than controls, with a positive relationship between screen time and symptom burden [3]. This finding supports the centrality of visual ergonomics and screen-time management in ROM rehabilitation.
Adherence can be tracked via digital logs or simple symptom diaries, and outcomes monitored using instruments such as the CVS Questionnaire (CVS-Q) or other DES measures described in DES reviews [9-12].
Adjunctive therapies and safety considerations include the following items.
For refractory or functionally disabling ROM, botox type A may provide substantial relief. A case report described swallow-induced eyelid myokymia resolving after onabotulinumtoxinA injections into the orbicularis oculi [13]. Systematic review data and clinical series in hemifacial spasm and facial palsy sequelae show that botulinum neurotoxin is effective and generally safe in reducing focal facial hyperkinesias, with high response rates and manageable adverse events [5, 17].
Within the proposed framework, botox should be:
1) Reserved for refractory, functionally significant cases, 2) used only after exclusion of structural causes and after structured trials of conservative rehabilitation (neuromuscular, psychophysiological, ergonomic), and 3) Administered by clinicians experienced in periocular injection to minimize complications such as ptosis or diplopia [5, 13, 17].
Red-flag indicators, including bilateral symptoms, spread to other facial muscles, persistence beyond 8 weeks, visual changes, or other neurological signs should prompt timely neuroimaging and specialist referral [1-3, 14, 15].
Monitoring, outcomes, and practical framework include a pragmatic 6–8-week rehabilitation program. It might include follow-up every 2–4 weeks to assess
1) Frequency, duration, and situational triggers of eyelid twitching (patient diaries); 2) Perceived stress (e.g. using validated stress or anxiety scales as in analogous MBSR trials) [7]. 3) DES symptoms and functional impact using validated instruments described in the DES literature [9-12]. 3) Patient-defined goals and participation, in line with client-centered rehabilitation approaches [18, 19].
Adjustments to neuromuscular exercises, mindfulness and lifestyle strategies, and ergonomic prescriptions can then be made according to response and adherence.
Table 1 should summarize the supporting evidence by domain (condition, study design, sample size, intervention, key outcomes, and level of evidence: ROM-specific vs extrapolated), while Table 2 should outline the multimodal rehabilitation protocol (domain, specific intervention, dosing/frequency, primary targets, and supporting references).
Discussion
Pathophysiology and rationale for rehabilitation
ROM is thought to arise from spontaneous, intermittent discharges in facial nerve fibers innervating the orbicularis oculi, modulated by central excitatory drive, local neuromuscular conditions, and environmental stressors [1-3]. The condition shares mechanistic similarities with facial synkinesis, hemifacial spasm, and Bell’s palsy sequelae conditions in which aberrant reinnervation, synkinesis, and impaired cortical inhibition lead to involuntary contractions [4-6]. These parallels provide a physiological rationale for adapting neuromuscular retraining strategies to ROM, even though direct ROM trials are lacking.
Most idiopathic ROM is benign and functional rather than structural [1-3]. However, isolated eyelid myokymia can occasionally herald structural pathology, including trigeminal schwannoma or cerebral tumors [14, 15]. This finding underscores the importance of red-flag screening and appropriate imaging in atypical or persistent cases, after which a rehabilitative approach becomes both safe and appropriate.
Neuromuscular retraining and biofeedback
Evidence from Bell’s palsy rehabilitation indicates that targeted physical therapy including facial exercises, neuromuscular retraining, and biofeedback can improve facial function and symmetry [4-6]. These interventions draw on principles of motor relearning, repetitive practice, and sensorimotor feedback to strengthen cortical inhibitory circuits and refine motor output.
In ROM, structured exercises, such as selective blinking, graded relaxation, and EMG-guided control may plausibly help patients regain voluntary regulation over eyelid movement and attenuate motor hyperexcitability. However, in the absence of ROM-specific RCTs, this application must be considered exploratory and hypothesis-generating, supported by mechanistic analogy rather than direct efficacy data [4-6, 16].
Sensorimotor training in visually impaired athletes further supports the notion that carefully structured training can induce significant adaptations in neuromotor coordination even under sensory constraints [16]. This cross-modal evidence adds weight to the concept that cortical and subcortical plasticity can be harnessed to modify eyelid motor control.
Psychophysiological and lifestyle modulation
Stress, sleep deprivation, and excessive caffeine intake are repeatedly identified as ROM triggers [1-3]. The RCT demonstrating non-inferiority of MBSR versus escitalopram in anxiety disorders provides robust level 1 evidence that mindfulness-based interventions can significantly reduce both subjective anxiety and physiological stress responses [7]. Incorporating MBSR-style programs, or briefer, structured mindfulness and relaxation exercises, into ROM care is therefore scientifically reasonable, with the expectation that reduced autonomic arousal will diminish the propensity for stress-triggered twitching.
Coupling these strategies with sleep optimization and caffeine moderation directly addresses modifiable behavioral risk factors identified in clinical descriptions of eyelid myokymia [1-3]. Although empirical demonstration of their effect on ROM is lacking, the logic linking triggers, mechanisms, and interventions is coherent and consistent with biopsychosocial rehabilitation models [18, 20].
Visual ergonomics and DES
The DES literature demonstrates that visual ergonomics 20-20-20 rule, microbreaks, blink training, and workstation optimization can significantly reduce ocular discomfort and strain, with improved subjective comfort and visual function [8-12]. The association between prolonged screen exposure and eyelid myokymia in the case–control study by Güneş directly implicates digital behavior in ROM [3].
Within the proposed framework, visual ergonomics constitutes a core component rather than an adjunct. The comparatively strong evidence-base for DES interventions (including RCTs and systematic reviews) [8-12] supports recommending these strategies confidently as first-line measures for patients with ROM, especially those with high digital workloads.
Role of botox
Botox A is well established as an effective treatment for hemifacial spasm and sequelae of peripheral facial palsy, with systematic reviews documenting significant symptom reduction and generally favorable safety profiles [5, 17]. Case reports of eyelid myokymia responsive to botox further suggest potential utility in refractory ROM [13]. Within a ROM rehabilitation model, botox should be framed as a second-line adjunct for patients who remain significantly symptomatic despite structured conservative therapy, and only after structural causes have been excluded [5, 13-15, 17].
Strengths, limitations, and SANRA considerations
This review responds directly to SANRA domains by
Clearly articulating the clinical importance of ROM and the specific knowledge gap (lack of a unified rehabilitation protocol), explicitly describing the search strategy, databases, and eligibility criteria, distinguishing between direct ROM evidence and extrapolated data from related conditions, and proposing a structured framework and summarizing evidence in accompanying tables. However, several limitations must be acknowledged. The ROM-specific evidence base is limited, and much of the proposed framework is extrapolated from Bell’s palsy, hemifacial spasm, anxiety disorders, and DES [3-13, 16, 17].
As a narrative rather than systematic review, there is an inherent risk of selection bias despite efforts at transparent reporting. Tertiary clinical resources (EyeWiki, StatPearls) were used for background but not as primary evidence [1, 2].
Future research should therefore prioritize
Prospective observational studies evaluating the natural history of ROM under structured rehabilitative care, pilot and definitive RCTs of neuromuscular retraining, psychophysiological interventions, and ergonomic packages alone and in combination using ROM-specific outcomes, and standardized outcome sets (e.g. twitch frequency, EMG measures, DES questionnaires, quality-of-life indices) to facilitate comparison across studies [4-12, 16, 18, 20].
Clinical implications
Despite its limitations, this review offers a clinically pragmatic, biopsychosocial framework aligned with modern rehabilitation principles, which emphasize integrated, goal-oriented programs and active patient participation [6, 18-20]. By combining neuromuscular retraining, stress modulation, visual ergonomics, and selectively used botox, clinicians can move beyond simple reassurance toward a more proactive, structured approach to ROM.
The explicit mapping of evidence levels (Table 1) and operational outline of interventions (Table 2) may facilitate shared decision-making, helping patients prioritize low-risk, self-management strategies while understanding where evidence remains preliminary.
Conclusion
ROM is benign in prognosis but can be functionally and psychologically distressing when persistent or frequent. Traditional management focused on reassurance and trigger avoidance may not fully address the needs of patients with chronic or high-impact symptoms.
This narrative review proposes a multimodal, non-invasive rehabilitation framework for ROM that integrates neuromuscular retraining and biofeedback to improve voluntary control and dampen hyperexcitability, psychophysiological and lifestyle interventions (e.g. MBSR, sleep and caffeine optimization) to reduce sympathetic arousal and symptom vigilance, visual ergonomics and DES management to tackle a key environmental driver in contemporary digital lifestyles, and adjunctive botox therapy for carefully selected refractory cases after exclusion of secondary causes.
The framework is explicitly hypothesis-generating, grounded in a combination of direct ROM data and extrapolated evidence from related neuromuscular, stress, and ergonomics research. Future controlled trials should validate this integrated approach using standardized neuromuscular and patient-reported outcomes. Until such data are available, the proposed model and accompanying evidence tables provide a structured, biopsychosocial lens through which clinicians can manage ROM more proactively, support patient self-efficacy, and potentially reduce the burden of recurrent consultations driven by persistent eyelid twitching.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, funding acquisition, project administration and investigation: Muhammad Adib Dwi Tamma Putra and Muhammad Fadill Akbar; Methodology and writing the original draft: Muhammad Adib Dwi Tamma Putra, Achmad Affaier; Data curation: Muhammad Adib Dwi Tamma Putra, Muhammad Fadill Akbar, and Muhammad Valdi Prasetia; Formal analysis: Muhammad Fadill Akbar and Achmad Affaier; Review and editing: Muhammad Adib Dwi Tamma Putra, Muhammad Fadill Akbar, Muhammad Valdi Prasetia; Supervision: Muhammad Adib Dwi Tamma Putra.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all colleagues who contributed significant insights throughout the study’s planning and execution phases, and who also offered assistance in analyzing and interpreting the data.
References
- EyeWiki. Eyelid myokymia [Internet]. 2025 [Updated 2026 February 26]. Available from: [Link]
- Patel BC, Chardoub AAJ. Eyelid myokymia. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. [Link]
- Güneş IB. Association between eyelid twitching and digital screen time. Cureus. 2024; 16(9):e69249. [DOI:10.7759/cureus.69249]
- Khan AJ, Heikkinen A, Taylor R, Thompson TL, Chatzikonstantinou E, O’Connell NE. Physical therapy interventions for bell’s palsy: A systematic review and meta-analysis. Clinical Rehabilitation. 2022; 36(10):1143-1154. [DOI:10.1177/02692155221110727] [PMID]
- Wang B, Wei X, Qi H, Bao X, Hu M, Ma J. Efficacy and safety of botulinum neurotoxin in the treatment of hemifacial spasm: A systematic review and meta-analysis. BMC Neurology. 2024; 24:420. [DOI:10.1186/s12883-024-03883-x] [PMID]
- Peitersen E. Bell’s Palsy: The spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Oto-Laryngologica, Supplement. 2002; (549):4-30. [DOI:10.1080/000164802760370736]
- Hoge EA, Bui E, Palitz SA, Schwarz NR, Owens ME, Johnston JM, et al. Mindfulness-based stress reduction vs escitalopram for anxiety disorders: A randomized noninferiority trial. JAMA Psychiatry. 2023; 80(1):13-21. [DOI:10.1001/jamapsychiatry.2022.3679] [PMID]
- Talens-Estarelles C, García-Lázaro S, Cerviño A, Albarrán-Diego C. Testing the 20-20-20 rule to alleviate digital eye strain. Contact Lens and Anterior Eye. 2023; 46(4):101744. [DOI:10.1016/j.clae.2022.101744] [PMID]
- Pucker AD, Tichenor AA. Digital eye strain updated perspectives. Clinical Optometry. 2024; 16:89-104. [DOI:10.2147/OPTO.S412382] [PMID]
- Kaur K, Gurnani B, Agarwal T, Goyal N, Singhal D, Singh S, et al. Digital eye strain: A comprehensive review. Ophthalmology and Therapy. 2022; 11(3):1065-85. [DOI:10.1007/s40123-022-00540-9] [PMID]
- Sheppard AL, Wolffsohn JS. Digital eye strain: Prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018; 3(1):e000146. [DOI:10.1136/bmjophth-2018-000146] [PMID]
- Rosenfield M. Computer vision syndrome: A review of ocular causes and potential treatments. Computers in Human Behavior. 2015; 51:244-51. [DOI:10.1016/j.chb.2015.04.073]
- Vuppala AAD, Miller NR, Subramanian PS. Swallow-induced eyelid myokymia: A synkinetic variant responsive to onabotulinumtoxina. Neuro-Ophthalmology. 2020; 44(5):291-3. [DOI:10.1080/01658107.2019.1587637] [PMID]
- Ito E, Uemura K, Yokoyama K, Otsuki M. Trigeminal schwannoma presenting as isolated eyelid myokymia: A case report. Clinical Case Reports. 2023; 11(2):e7086. [DOI:10.1002/ccr3.7086] [PMID]
- Abdolrahimi M, Bahrami E, Tabibzadeh M. Eyelid myokymia secondary to cerebral tumor: A case report. Neuro-Ophthalmology. 2018; 42(2):113-6. [DOI:10.1080/01658107.2017.1350195] [PMID]
- Wahlström EK, Holmström A, Fagergren A, Törnhage CJ, Nordström A. Sensorimotor training improves balance and coordination in visually impaired athletes: A randomized controlled trial. Clinical Rehabilitation. 2025; 39(2):123-131. [DOI:10.1177/02646196251322125]
- Carré F, Amar J, Tankéré F, Foirest C. Botulinum toxin injections to manage sequelae of peripheral facial palsy. Toxins. 2024; 16(3):161. [DOI:10.3390/toxins16030161] [PMID]
- Wade DT, de Jong BA. Recent advances in rehabilitation. BMJ. 2000; 320(7246):1385-8. [DOI:10.1136/bmj.320.7246.1385] [PMID]
- Wressle E, Eeg-Olofsson AM, Marcusson J, Henriksson C. Improved client participation in the rehabilitation process using a client-centred goal formulation structure. Journal of Rehabilitation Medicine. 2002;34(1):5-11. [DOI:10.1080/165019702317242640] [PMID]
- Donker-Cools BH, Wind H, Frings-Dresen MH. Return to work after acquired brain injury: A systematic review. Brain Injury. 2018: 32(4); 357-82. [DOI: 10.3109/02699052.2015.1090014] [PMID]
Article type: Reviews |
Subject:
Physical Medicine and Rehabilitation
Received: 2025/09/27 | Accepted: 2025/12/3 | Published: 2026/03/1
Received: 2025/09/27 | Accepted: 2025/12/3 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
